Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
|
|
|
- David Atkins
- 5 years ago
- Views:
Transcription

1 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
2 Talk Overview Background Assessment and Classification Surgical therapy Medical therapy
3 Types of Fistulas in Crohn s Disease Perianal 54% Entero-enteric 21% Rectovaginal 9% Enterocutaneous 6% Enterovesical 3% Entero-intraabdominal 3%
4 Perianal Fistula Prevalence Overall prevalence Population based 21-23% Referral center 14-38% Surgical patients 17-28% Based on GI tract disease Ileal 12% Ileocolonic 15% Colon w/o rectal dz 41% Colon + rectal dz 92%
5 Perianal Disease at Diagnosis Predicts Poor Outcomes Retrospective cohort of 1123 patients 3 factors at diagnosis were independently predictive of a disabling CD course in the 5-year period after diagnosis: Factor OR (95% CI) Initial requirement for steroids 3.1 ( ) Age < 40 years 2.1 ( ) Perianal disease at diagnosis 1.8 ( ) Beaugerie L et al. Gastroenterology 2006;130:650-6
6 Assessment & Classification

7 Abscess

8 Fistula: Park s Classification Supra-sphincteric Extra-sphincteric Intersphincteric Trans-sphincteric
9 AGA Classification 2003 Simple Fistula Complex Fistula External opening Single Several Other complications No perianal abscess No rectal stenosis No proctitis No connection to vagina or bladder Perianal abscess Rectal stenosis Overt proctitis Connection to vagina or bladder Locations Low superficial Low inter-sphincteric Low intra-sphincteric Inter-sphincteric Trans-sphincteric Supra-sphincteric Extra-sphincteric AGA medical position statement: Perianal Crohn s disease. Gastroenterology 2003;125:1503
10 Evaluation Modality Options Fistulography- painful and low accuracy Pelvic CT- limited by poor spatial resolution Pelvic MRI Rectal EUS Examination under anesthesia
11 Assessment of Perianal Disease Prospective, blinded study compared EUS, MRI and EUA in 32 patients with suspected perianal Crohn s disease All 3 methods had excellent accuracy: EUS 91% (95% CI = 75-98%) EUA 91% (95% CI = 75-98%) MRI 87% (95% CI = 69-96%) Combining either EUS or MRI with EUA increased accuracy to 100% Schwartz DA et al. Gastroenterology. 2001;121:
12 SURGICAL TREATMENT
13 Surgery for Crohn s Perianal Disease Treatment goal: Eliminate sepsis with the least amount of functional derangement ASCRS Practice Parameters: The primary treatment for perianal Crohn s fistulas is medical Surgery is reserved for the control of sepsis and occasionally as an adjunct for cure. Dis Colon Rectum 2011;54:
14 Crohn s Perianal Fistulas: Surgical Options Fistulotomy- for simple, low fistulas. Setons- for complex fistulas; prevent recurrent sepsis Collagen plug, fibrin glue Rectal mucosal advancement flap Diverting ileostomy Proctectomy/colectomy % will require this
15 Fistulotomy Use for symptomatic simple fistulas- low fistula and no rectal inflammation Healing in % Minor incontinence in 6-12% Skill of operating surgeon significant factor


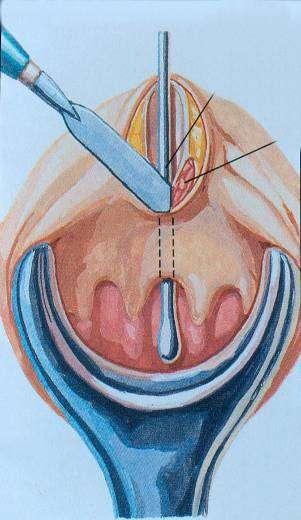
16 Fistulotomy Images courtesy of T Hull, MD

17


18 Courtesy of Victor Fazio, MD

19
20 Advancement Flap If rectal mucosa is grossly normal Sometimes done in conjunction with defunctioning stoma Success rates: Short term % Long term- 50%

21 Advancement Flap Slide courtesy of Victor Fazio, MD
22 MEDICAL TREATMENT
23 Antibiotics Most are small case series using 2-4 months of: Metronidazole mg/day Ciprofloxacin 1000 mg/day Combination General results: Initial improvement after 6-8 weeks Rarely complete closure of the fistula Prompt recurrence upon discontinuation Benefit for abscesses Bernstein LH et al. Gastroenterology 1980; 79: Jakobovits J, et al. Am J Gastroenterol 1984; 79: Brandt LJ et al. Gastroenterology 1982; 83: Turunen U et al. Scand J Gastroenterol 1989; 24 suppl: 144. Solomon MJ, et al. Can J Gastroenterol 1993; 7:
24 RCT with Antibiotics 25 patients X 10 weeks Ciprofloxacin (10) Metronidazole (7) Placebo (8) Response: 50% reduction in the number of draining fistulas Ciprofloxacin Metronidazole Placebo Response 40% 14% 12.5% Remission 30% 0% 12.5% Termination of the trial prior to week 10 10% 71%* 12% Thia KT et al. Inflamm Bowel Dis 2009;15:17-24
25 Meta-Analysis of Antibiotics for Perianal Fistulas OR = 0.80 (0.66, 0.98); NNT = 5 Khan KT et al. Am J Gastroenterol 2011;106:661-73
26 Azathioprine and 6-mercaptopurine Meta-analysis of trials in which perianal fistula healing was a secondary endpoint Azathioprine/6-MP N = 41 Placebo N = 29 Response* 22 (54%) 6 (21%) OR 4.44 ( ) * complete healing or decreased discharge Pearson DC et al. Ann Intern Med 1995;123:
27 % Patients Tacrolimus RCT 40 * 43% Tacrolimus 0.2mg/kg/d Placebo % 10% 8% Partial Complete Sandborn et al Gastroenterology 2003;125:380 8.
28
29 Cyclosporine NO controlled trials 10 case series- 64 patients total: 4 mg/kg/d IV for 7 days, then po Overall response rate: 83% Relapse rate: 62%
30 Anti-TNF Engineered Antibodies Chimeric monoclonal antibody Human recombinant antibody Humanized Fab fragment VL VH Mouse Human No Fc PEG CH 1 IgG1 IgG1 PEG PEG = Polyethylene glycol Infliximab Adalimumab Certolizumab pegol
31 Infliximab for Fistulizing Crohn s: Initial Induction RCT 94 patients with single or multiple enterocutaneous fistula(s) draining for at least three months Randomized to placebo, 5 or 10 mg/kg of infliximab at 0, 2, and 6 weeks Primary endpoint: 50% reduction in the number of draining fistulas for at least two consecutive evaluation visits (at least one month) Fistula considered closed when not draining despite gentle compression Patients followed at 2, 6, 10, 14, and 18 weeks Present D, et al. N Engl J Med. 1999;340:

32 Infliximab for Fistulizing Crohn s Primary Endpoint: 50% Reduction in Draining Fistulas P=0.021 P=0.002 Present D, et al. N Engl J Med. 1999;340:

33 Infliximab for Fistulizing Crohn s Complete Response: All Fistulas Closed P<0.001 P=0.04 Present D, et al. N Engl J Med. 1999;340:
34 ACCENT II Study Design Infusion Week 0 Week 2 Week 6 Week 14 Responders n=195 (69%) All Patients, n=306 Infliximab 5 mg/kg 24 patients discontinued Nonresponders n=87 (31%) Week 22 Week 30 Week 38 Week 46 Placebo Maintenance n=99 Infliximab 5 mg/kg q 8 weeks Infliximab 5 mg/kg Maintenance n=96 Infliximab 10 mg/kg q 8 weeks Evaluation at Week 54
35 Draining Fistulas at Baseline By Location All Randomized Patients Placebo maintenance 5 mg/kg maintenance Total Patients Randomized Number (%) Patients with: Abdominal fistulas 24 (17.3%) 14 (10.4%) 38 (13.9%) Perianal fistulas 118 (84.9%) 120 (89.6%) 238 (87.2%) Rectovaginal fistulas 11 (7.9%) 12 (9.0%) 23 (8.4%)

36 Patients Who Had Not Lost Response (%) ACCENT II 36 Time to Loss of Response Among Patients Responding at Weeks 10 and 14 P=0.001
37 Patients in Response (%) ACCENT II 37 Fistula Response at Week 54 Among Patients Responding at Weeks 10 and P=0.002 P= % % 23% 40% 0 24/89 41/83 24/89 41/83 Fistula Response Complete Response Placebo maintenance 5 mg/kg infliximab maintenance
38 Adalimumab for Treatment of Crohn s Related Fistulas Secondary endpoint in CHARM trial: 2 doses of adalimumab (80 mg 40 mg) and then randomized to placebo or 2 treatment arms 117 patients had draining fistulas at screening and baseline visits- 97% had perianal fistulas Fistula response also assessed as part of open label extension (ADHERE trial) Colombel JF et al. Gut 2009;58:940-8
39 Adalimumab for Fistula Healing *P < 0.05 Colombel JF et al. Gut 2009;58:940-8
40 Adalimumab for Fistula Healing Fistula response NOT affected by: Baseline immunosuppressant or antibiotic use Prior anti-tnf therapy 90% of those with healed fistulas at end of CHARM maintained closure after 1 additional year of therapy Colombel JF et al. Gut 2009;58:940-8
41 Certolizumab for Fistulas: Subgroup Analysis from PRECiSE 2 Among patients received open-label induction with certolizumab (400 mg at weeks 0, 2 & 4), 108 patients had draining fistulas at baseline 58/108 with draining fistulas were responders (by CDAI) at week 6 randomised to certolizumab 400 mg (n = 28) or placebo (n = 30) q 4 weeks from weeks Fistula closure was evaluated throughout the study, with a final assessment at week 26.
42 % Patients Certolizumab for Fistulas: Subgroup Analysis from PRECiSE P=0.069 Closure & > 50% maintenance P= /13 11/15 4/13 10/15 Closure & 100% maintenance Placebo Certolizumab Schreiber S et al. Aliment Pharmacol Ther 2011;33:185-93
43 Take Home Points Perianal disease is associated with more aggressive course of Crohn s Management of perianal Crohn s requires combination of surgical and medical therapy Medical tx- infliximab is the best studied agent but also some proof for benefit with: Antibiotics- short term 6-MP/azathioprine Adalimumab Tacrolimus
44 PE + Flex sig?eua/mri/eus?gi tract evaluation Simple Fistula Complex Fistula Antibiotics +/- Fistulotomy Control of sepsis/seton Follow Response No response 6-MP/Aza Anti-TNF Antibiotics + Anti-TNF, 6-MP/Aza

45 Thank You
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Epidemiology / Morbidity
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc. Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Konservative Behandlungsmöglichkeiten?
 PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
Perianal Fistula of Crohn s Disease
 Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Corporate Presentation
 Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions
: Future Directions") Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cx601 ADMIRE-CD Top-Line Results Webcast. 24 August 2015
 Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy
 Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Special Authorization Drug Products with
 Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series
 CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Management of complex perianal Crohn s disease
 REVIEW ARTICLE Annals of Gastroenterology (2017) 30, 1-12 Management of complex perianal Crohn s disease Lara Aguilera-Castro, Carlos Ferre-Aracil, Ana Garcia-Garcia-de-Paredes, Enrique Rodriguez-de-Santiago,
REVIEW ARTICLE Annals of Gastroenterology (2017) 30, 1-12 Management of complex perianal Crohn s disease Lara Aguilera-Castro, Carlos Ferre-Aracil, Ana Garcia-Garcia-de-Paredes, Enrique Rodriguez-de-Santiago,
Practical Risk Management Tools for Patients with IBD. Garth Swanson MD Rush University Medical Center
 Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review)
") Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Practice Parameters for the management of perianal abscess and fistula-in-ano(1)
") New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Κατανοώντας τα περιεδρικά συρίγγια στη νόσο Crohn: παρελθόν και μέλλον. Ι. Γ. Παπακωνσταντίνου Αναπλ. Καθηγητής Χειρουργικής
 Κατανοώντας τα περιεδρικά συρίγγια στη νόσο Crohn: παρελθόν και μέλλον Ι. Γ. Παπακωνσταντίνου Αναπλ. Καθηγητής Χειρουργικής Epidemiology, Burden of Disease and Pathophysiology Epidemiology of Perianal
Κατανοώντας τα περιεδρικά συρίγγια στη νόσο Crohn: παρελθόν και μέλλον Ι. Γ. Παπακωνσταντίνου Αναπλ. Καθηγητής Χειρουργικής Epidemiology, Burden of Disease and Pathophysiology Epidemiology of Perianal
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Research Article Temporary Fecal Diversion in the Management of Colorectal and Perianal Crohn s Disease
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Emerging g therapies for IBD: A practical approach to positioning. Sequential Therapies for IBD
 Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study
 ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL
 INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
Op#mizing)Management)in)IBD:) Mucosal)Healing)
Management)in)IBD:) Mucosal)Healing)") Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma: a pilot study
 Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
BEYOND MOLECULAR BIOLOGY: IMPROVING QUALITY OF LIFE IN PATIENTS WITH CROHN S DISEASE. Stephen B. Hanauer, MD*
 BEYOND MOLECULAR BIOLOGY: IMPROVING QUALITY OF LIFE IN PATIENTS WITH CROHN S DISEASE Stephen B. Hanauer, MD* ABSTRACT *Professor of Medicine and Clinical Pharmacology; Chief, Section of Gastroenterology,
BEYOND MOLECULAR BIOLOGY: IMPROVING QUALITY OF LIFE IN PATIENTS WITH CROHN S DISEASE Stephen B. Hanauer, MD* ABSTRACT *Professor of Medicine and Clinical Pharmacology; Chief, Section of Gastroenterology,
Of Treatment For Inflammatory Bowel Diseases
 Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: , 2016
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 1939-1945, 2016 Similar outcomes for anti-tumor necrosis factor-α antibody and immunosuppressant following seton drainage in patients with Crohn's disease-related
EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 1939-1945, 2016 Similar outcomes for anti-tumor necrosis factor-α antibody and immunosuppressant following seton drainage in patients with Crohn's disease-related
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis
 Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
Once Daily Dosing for Induction and Maintenance of Remission in Ulcerative Colitis John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University JKM 2014 Svartz N. Acta Med Scand
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Review Article Practical Medical Management of Crohn s Disease
 ISRN Gastroenterology Volume 2013, Article ID 208073, 12pages http://dx.doi.org/10.1155/2013/208073 Review Article Practical Medical Management of Crohn s Disease Bulent Baran 1 and Cetin Karaca 2 1 Van
ISRN Gastroenterology Volume 2013, Article ID 208073, 12pages http://dx.doi.org/10.1155/2013/208073 Review Article Practical Medical Management of Crohn s Disease Bulent Baran 1 and Cetin Karaca 2 1 Van
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases
 Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
Biologics, Novel Therapeutic Approaches in Inflammatory Bowel Diseases Walter Reinisch Univ-Klinik für Innere Medizin III Abt. Gastroenterologie & Hepatologie AKH Wien The Biologic s evolution From availabilitydriven
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
et al.. Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab..
 Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab. Guillaume Bouguen, Laurent Siproudhis, Emmanuel Gizard, Timothée Wallenhorst, Vincent Billioud, Jean-François Bretagne,
Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab. Guillaume Bouguen, Laurent Siproudhis, Emmanuel Gizard, Timothée Wallenhorst, Vincent Billioud, Jean-François Bretagne,
Optimal care during pregnancy and delivery
 Oxford Inflammatory Bowel Disease MasterClass Optimal care during pregnancy and delivery Professor Catherine Nelson-Piercy, London, UK Oxford Inflammatory Bowel Disease MasterClass Therapeutic goals in
Oxford Inflammatory Bowel Disease MasterClass Optimal care during pregnancy and delivery Professor Catherine Nelson-Piercy, London, UK Oxford Inflammatory Bowel Disease MasterClass Therapeutic goals in
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: May 1, 2018 Last Revised: April 18, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: May 1, 2018 Last Revised: April 18, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Name of Policy: Plugs for Fistula Repair
 Name of Policy: Plugs for Fistula Repair Policy #: 399 Latest Review Date: November 2013 Category: Surgical Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Plugs for Fistula Repair Policy #: 399 Latest Review Date: November 2013 Category: Surgical Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Selection and use of the non-anti- TNF biological therapies: Who? When? How?
 Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula
 Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Conflict of Interest. Inflammatory Bowel Disease. Road Map. Scope of the Disorder (United States) Age-Specific Incidence of IBD*
 Age-Specific Incidence of IBD*") Inflammatory Bowel Disease Conflict of Interest No conflicts of interest Sonia Friedman, M.D. Assistant Professor of Medicine Gastroenterology Division Brigham and Women s Hospital Road Map Background
Inflammatory Bowel Disease Conflict of Interest No conflicts of interest Sonia Friedman, M.D. Assistant Professor of Medicine Gastroenterology Division Brigham and Women s Hospital Road Map Background
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Surgery in Inflammatory Bowel Disease. Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh
 Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at: