Medical Management of Intestinal Strictures
|
|
|
- Homer Hampton
- 6 years ago
- Views:
Transcription





1 Medical Management of Intestinal Strictures Subrata Ghosh, FRCP, FRCPE, FRCPC, AGAF, FCAHS Professor of Translational Medicine Director of the Institute of Translational Medicine University of Birmingham, United Kingdom Adjunct Professor & past chairman of Medicine University of Calgary, Canada
2 Stricturing Crohn s Disease Up to one third of patients with CD develop strictures within 10 years of diagnosis and most commonly affect the distal ileum or the surgical anastomotic site (Cosnes et al. 2002). Small bowel CD is an independent predictor of a shorter time to complications (2.12 ( ) (Siegel et al 2016). A number of risk factors have been identified for stricture development, such as disease duration, smoking, ileal disease and NOD2/CARD15 genetic mutations, though only a limited number have been robustly replicated.
3 Treating Biologic Refractory Crohn s disease The traditional paradigms are getting challenged. The concept of optimum Therapeutic Drug levels are getting challenged. The transition to out of class therapeutic agents (with reference to anti-tnf) is getting challenged. We need more studies in stenotic CD concepts are evolving
4 JAK2 OR NOD2 p.1007insc NOD2 overall NOD2 p.1007insc NOD2 overall IL23R NOD2 p.1007insc NOD2 overall NOD2 p.1007insc NOD2 overall NOD2 p.1007insc NOD2 overall LOC Genetic factors conferring an increased susceptibility to develop Crohn s disease (CD) also influence disease phenotype: Results from the IBDchip European project OR of association and 95% CI for single nucleotide polymorphisms (SNPs) that passed Bonferroni correction for each outcome Ileal involvement (L1+L3) Colonic involvement (L1+L3) Bowel stenosis SNPs Bowel resection Complicated 4 Cleynen I, et al. Gut 2013;62:

5 Kaplan Meier Curves smokers and non smokers Grey = smokers Black = non-smokers Nunes T et. al. APT 2013;38:752.

 Caecum Ascending colon")





6 LI is a quantitative tool to assess cumulative structural bowel damage in CD Region Upper GI tract Small bowel Colon and rectum Anus Segment Oesophagus Stomach Duodenum n segments of 20 cm (up to 20) Caecum Ascending colon Transverse colon Descending colon Sigmoid colon Rectum Anus Entire GI tract evaluated for damage (stricturing, penetrating lesions, surgery) Divided into 4 regions, and subdivided into segments Lesions and surgery in each segment scored 0-3 according to severity Composite region and overall index score calculated LI used to assess damage progression, and to evaluate treatment strategy Potential endpoint for diseasemodification trials Pariente B, et al. Inflamm Bowel Dis 2011;17: Pariente B, et al. Gastroenterology 2015;148:52 63; Fiorini G, et al. J Crohns Colitis 2016:
7 Pro or Anti-fibrogenic effect on Myofibroblasts Lawrence, Rogler et al. JCC 2015
8 Process of tissue repair and fibrosis Lawrence, Rogler et al. JCC 2015
9 Cellular Immune Response and Fibrosis
10 Paediatric Inception Cohort: Development of Stricturing or Penetrating Complications at FU Kugathasan et al Lancet 2017

11 Comparative effectiveness study on early intervention in paediatric IBD Walters T, et al. Gastroenterology 2014;146:
12 Cumulative Probability of Abdominal Surgery Crohn s disease Phenotype at anti-tnf start B1= inflammatory; B2= stricturing; B3=penetrating. L1=terminal ileal Moran GW et. al. Clin Gastroenterol Hepatol 2015

13 LPL GATA3 expression and anti-tnf response in CD Sa1969 DDW Gene Expression of Matrix Metalloproteinase-3 in Lamina Propria Mononuclear Cells Predicts Response to TNF Inhibitors in Colonic Inflammatory Bowel Disease Christina Hirota, Ji Li, Miriam Fort Gasia, Mailin Deane, Aito Ueno, Paul L. Beck, Marietta Iacucci, Xianyong Gui, Subrata Ghosh Ji Li et al. IBD 2016;22:
14 Paediatric Inception Cohort: Ileal Gene Signatures Associated With Disease Complications Kugathasan S et al. Lancet 2017 Ileal Gene Signatures predict B2 > B3
15 Probability of complication-free survival Anti-TNF use within 90 days reduces internal penetrating complication-free survival 100 Stricturing behaviour (B2) Penetrating behavior (B3) Age at diagnosis HR p value HR p value 1.13 ( ) ( ) days Race 1.25 ( ) ( ) Isolated ileal location (L1) 1.66 ( ) ( ) 0.72 ASCA IgA ( ) ( ) 0.18 CBir ( ) ( ) Early anti-tnf 1.13 ( ) ( ) B2 (no early TNFα) B2 (early TNFα) B3 (no early TNFα) B3 (early TNFα) p=0.75 p= years BUT NOT STRICTURING DISEASE Time to event (days) Kugathasan S, et al. Lancet 2017;389:
16 ILEAL VERSUS COLONIC CROHN S DISEASE STRICTURE COMPARISON (Chen W et al JCC 2016) Ileal (n = 37) Colonic (n = 11) Mean SEM Mean SEM I. Mucosa Active inflammation Chronic inflammation Fibrosis Muscular Hyperplasia 83.33*** *** 8.52 Space volume expansion II. Submucosa Active inflammation Chronic inflammation Fibrosis 40.09** ** 7.04 Muscular Hyperplasia 75.23** ** 7.87 Adipocyte proliferation Neuronal hypertrophy Space volume expansion III. Muscularis propria Active inflammation Chronic inflammation Fibrosis 0.90* * 3.03 Muscular Hypertrophy 78.83* * 9.87 Neuronal hypertrophy Adipocyte proliferation Space volume expansion

17 Contrast Enhanced Ultrasound Reduced Blood Volume and Blood Flow in Patients with Fibrotic Disease Nylund K et al. Ultrasound in Med & Biol 2013;39:1197


18 Severe CD NTI Incomplete mechanical bowel obstruction NTI, neo-terminal ileum


19 Stricture localised perforation with inflammatory mass


20 MR-Enterography: extent of disease Assessment of extent/severity of disease Assessment of complications Thickened narrowed terminal ileum Assessment of treatment response
21 Model to predict complications of CD 16-year-old girl, small bowel and perianal disease, QSS group= No treatment Risk of complication Early anti-tnf treatment Years from presentation Early IM treatment Overall HR Benefits of therapy 0.18 Personal Characteristics Input age at Dx 16 Gender input UT input CBir1 input SNP12 input Months since Dx PA input OmpC input SNP13 input 0 Immunomodulators 1 Disease Location SB input 1 LB input 1 Treatment Options Anti-TNF 0 Treatment option=1: treatment within 90 days from diagnosis. Serological Inputs ASCA A input 118 ASCA G input 18 panca input 11 Corticosteroids 0 Genetic Inputs Genetic information 0 SNP8 input Treatment option=2: treatment after 90 days from diagnosis. 0 Dx, diagnosis; SB, small bowel; LB, large bowel; UT, upper tract; PA, perianal; anti-cbir1, anti-flagellin; OmpC, anti-outer-membrane porin C of E. coli; panca, perinuclear antineutrophil antibody; QSS, quartile sum score; SNP, single nucleotide polymorphism. Siegel CA, et al. Inflamm Bowel Dis 2011;17:


22 POCER PostOperative Crohn s Endoscopic Recurrence Khanna R, et al. Lancet 2015;386;
 No endoscopy (Standard arm) 1/3 of patients All")
23 SURGERY: Curative resection Randomisation 1:2 18 month colonoscopy POCER: study design Randomised, multicentre study in Australia and New Zealand Standard care with best drug therapy versus endoscopic monitoring with treatment step up in postoperative CD High/low risk stratification (High risk: smoker, 2 surgeries, perforating disease) No endoscopy (Standard arm) 1/3 of patients All patients: Metronidazole: 0 3 months Low risk: No further treatment High risk: Thiopurine or adalimumab if thiopurine intolerant 2/3 of patients Endoscopic intervention (Active arm) Risk driven by best drug therapy 6-month colonoscopy Step up treatment if i2 on Rutgeerts scale * *To thiopurine (low-risk patients), adalimumab 40 mg eow (high-risk patients on thiopurine), or adalimumab 40 mg ew (high-risk thiopurine-intolerant patients) De Cruz P, et al. Lancet 2015;385:
24 Percentage of patients POCER: endoscopic outcomes at 18 months Remission (Rutgeerts i0 i1) and recurrence (Rutgeerts i2 i4) 100 Primary endpoint p= % 60 51% 49% 40 33% 20 0 Remission Recurrence Remission Recurrence Active arm (n=122) Standard arm (n=52) De Cruz P, et al. Lancet 2015;385:
 and mucosal lesions (Rutgeerts i1 i4) p=0.")
 Standard arm (n=52) De Cruz P, et al.")
25 Percentage of patients POCER: mucosal healing at 18 months Complete mucosal healing (Rutgeerts i0) and mucosal lesions (Rutgeerts i1 i4) p= % 92% % 8% 0 Complete healing Lesions Complete healing Lesions Active arm (n=122) Standard arm (n=52) De Cruz P, et al. Lancet 2015;385:
26 PREVENT Study Clinical Endpoints Regueiro M et al. Gastroenterology 2016;150:
27 PREVENT Study endoscopic recurrence Regueiro M et al. Gastroenterology 2016;150:
28 POST- OPERATIVE Anti-TNF Strategy Colonoscopy 6-12 months after resection and introduction of TNFi in patients with endoscopic recurrence with or without immunosuppressive drugs would appear to be a pragmatic therapeutic strategy in most patients. Risk attenuation such as cessation of smoking should always be encouraged. Ghosh S, D Haens G. Editorial Gastroenterology 2016;150:
29 RESECTION IMMUNOHISTOLOGICAL RECURRENCE COLONOSCOPIC RECURRENCE SYMPTOMATIC RECURRENCE TIME

30 Stages of Postoperative Recurrence Immunohistological recurrence Endoscopic recurrence Symptomatic recurrence INDEX SURGERY Complications Surgery TIME SINCE SURGERY Ghosh S, D Haens G. Gastroenterology 2016;150:1521
31 Anti-fibrotic strategies in Crohn s disease Early effective treatment before fibrosis happens. Arrest stenosis by anti-inflammatory therapy Use specific targeted therapies in development: Anti-MMP9 Anti-IL36 Small molecule oral kinase inhibitors Inhibit TGF-beta mediated collagen deposition
32 Filgotinib: JAK 1 inhibitor in CD Endpoint Placebo (n=44) % Filgotinib 200mg (n=128) % Clinical remission (CDAI<150) Clinical response (100 point CDAI) IBDQ All endpoints statistically significant Lancet 2017;389:
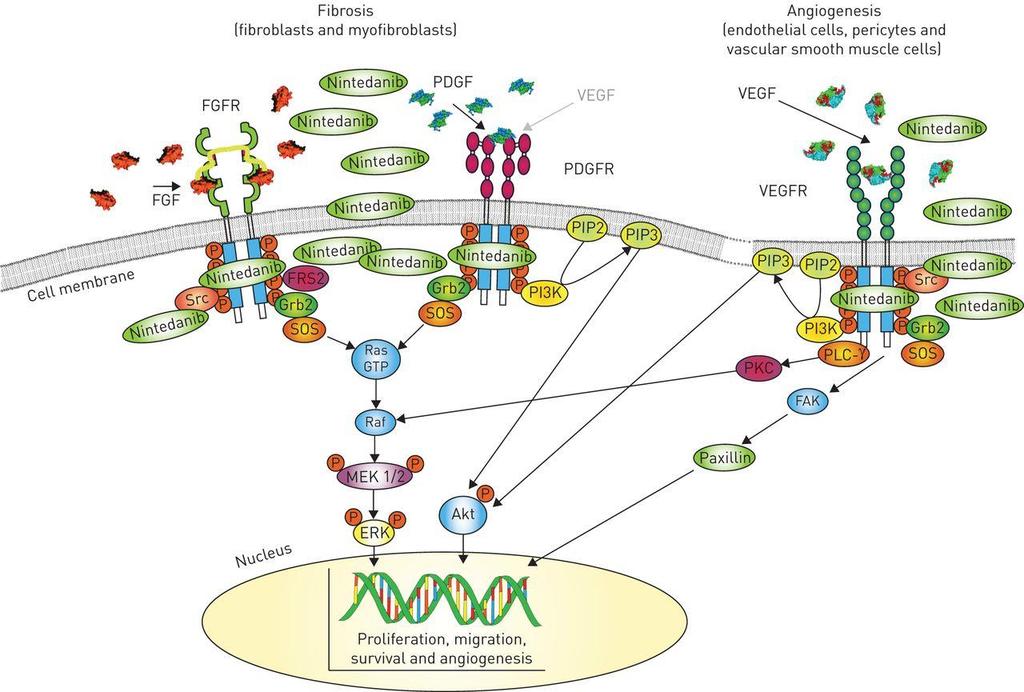
33 Nintedanib

34 Pirfenidone - MoA
35 Medical Management of Intestinal Strictures Pre-stricture Established stricture Assess risk factors Assessment for inflammation Micropenetrating disease etc Commence on Disease modification Effective therapy for inflammation Objectively assess Resolution of inflammation Assess for residual stenosis Aim to resolve inflammation Within 6 months
36 T2T recommendations in CD Composite endpoint Clinical/PRO remission AND Endoscopic remission Defined as resolution of abdominal pain and normalisation of bowel habit Assessed at minimum of 3 months during active disease Patients individual goals should also be addressed Defined as resolution of ulceration Should be assessed within 6 9 months after start of therapy When endoscopy cannot adequately evaluate inflammation, assess resolution of inflammation by cross-sectional imaging Adjunctive measures Biomarkers: CRP and faecal calprotectin are adjunctive measures of inflammation, not targets, for monitoring CD Histology: histologic remission is not considered a target CRP, C-reactive protein; PRO, patient-reported outcome Peyrin-Biroulet L, et al. Am J Gastroenterol 2015;110:
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Fibrotic complications of inflammatory bowel disease
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fibrotic complications of inflammatory bowel disease Gerhard Rogler, Department of Gastroenterology
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Strategies for changing the course of Crohn s disease
 Strategies for changing the course of Crohn s disease Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Where we are now and where we want to be Diagnosis (usually endoscopy)
Strategies for changing the course of Crohn s disease Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Where we are now and where we want to be Diagnosis (usually endoscopy)
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Disease behavior in adult patients- are there predictors for stricture or fistula formation?
 Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
Disease behavior in adult patients- are there predictors for stricture or fistula formation? Falk Symposium 168, Madrid, Spain Iris Dotan, M.D., Head, IBD Center, Department of Gastroenterology and Liver
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL
 INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The future of IBD therapeutic research
 The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
The future of IBD therapeutic research Jean-Frederic Colombel, MD Director Susan and Leonard Feinstein IBD Clinical Center Icahn School of Medicine, Mount Sinai Hospital New York J-F Colombel has served
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Towards Precision Medicine in Inflammatory Bowel Diseases
 Precision Medicine and Biomarkers Leaders Summit. Munich September 13-14, 2018 Towards Precision Medicine in Inflammatory Bowel Diseases ANDRÉS HURTADO-LORENZO, Ph.D. SENIOR DIRECTOR OF TRANSLATIONAL RESEARCH
Precision Medicine and Biomarkers Leaders Summit. Munich September 13-14, 2018 Towards Precision Medicine in Inflammatory Bowel Diseases ANDRÉS HURTADO-LORENZO, Ph.D. SENIOR DIRECTOR OF TRANSLATIONAL RESEARCH
Crohn s Disease: A New Approach to an Old Problem
 Management of Postoperative Crohn s Disease: A New Approach to an Old Problem Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center
Management of Postoperative Crohn s Disease: A New Approach to an Old Problem Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv
 Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv University 1 SHARE study My year Collaboration between gastroenterology
Guided by Dr. Michal Amitai Head of Abdominal Imaging Department of Diagnostic Imaging Sheba Medical Center Sackler School of Medicine, Tel Aviv University 1 SHARE study My year Collaboration between gastroenterology
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Prevention and Management of Postoperative Crohn s disease
 Prevention and Management of Postoperative Crohn s disease Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center Director, Gastroenterology,
Prevention and Management of Postoperative Crohn s disease Miguel Regueiro, M.D. Associate Professor of Medicine Associate Chief for Education Clinical Head and Co-Director, IBD Center Director, Gastroenterology,
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence
 Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence Sharon Dudley-Brown, PHD, FNP-BC, FAAN Assistant Professor Johns Hopkins University Baltimore, MD sdudley2@jhmi.edu Disclosures
Challenges in IBD: The Post-Op IBD Patient: Preventing Pouchitis & Recurrence Sharon Dudley-Brown, PHD, FNP-BC, FAAN Assistant Professor Johns Hopkins University Baltimore, MD sdudley2@jhmi.edu Disclosures
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Impact of endoscopic monitoring in postoperative Crohn s disease patients already receiving pharmacological prevention of recurrence
 1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Clinical Trials in IBD. Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases
 Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art
 Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
IBD Tools to Aid in the Accurate Diagnosis of Inflammatory Bowel Disease
 IBD Tools to Aid in the Accurate Diagnosis of Inflammatory Bowel Disease Inflammatory Bowel Disease Experts in Autoimmunity Inova Diagnostics offers a complete array of methods to aid in the diagnosis
IBD Tools to Aid in the Accurate Diagnosis of Inflammatory Bowel Disease Inflammatory Bowel Disease Experts in Autoimmunity Inova Diagnostics offers a complete array of methods to aid in the diagnosis
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
AVX-470, an Orally Delivered Anti-TNF Antibody for Treatment of Acute Ulcerative Colitis: Results of a First-in- Human Trial
 AVX-470, an Orally Delivered Anti-TNF Antibody for Treatment of Acute Ulcerative Colitis: Results of a First-in- Human Trial M Scott Harris 1, Deborah Hartman 1, Sharon Spence 1, Sally Kennedy 1, Theodore
AVX-470, an Orally Delivered Anti-TNF Antibody for Treatment of Acute Ulcerative Colitis: Results of a First-in- Human Trial M Scott Harris 1, Deborah Hartman 1, Sharon Spence 1, Sally Kennedy 1, Theodore
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Biologic Therapy for Ulcerative Colitis in 2015
 5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
Op#mizing)Management)in)IBD:) Mucosal)Healing)
Management)in)IBD:) Mucosal)Healing)") Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Op#mizing)Management)in)IBD:) Mucosal)Healing) Vipul&Jairath&MD&PhD& Associate&Professor&of&Medicine,&Epidemiology&and& Biosta=s=cs& Western&University&&& Division&of&Gastroenterology,&& London&Health&Sciences&Network&
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
4/16/2018. Updates in Crohn s Disease. Disclosures. Learning Objectives. Crohn s Disease is Progressive and Destructive
 4/16/218 Disclosures Updates in Crohn s Disease David T. Rubin, MD Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition University of Chicago Consultant
4/16/218 Disclosures Updates in Crohn s Disease David T. Rubin, MD Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition University of Chicago Consultant
Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152
 Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Understanding clinical aspects of Crohn s disease and ulcerative colitis: Implications for the basic scientist
 Understanding clinical aspects of Crohn s disease and ulcerative colitis: Implications for the basic scientist Scott Plevy, MD Associate Professor of Medicine, Microbiology & Immunology UNC School of Medicine
Understanding clinical aspects of Crohn s disease and ulcerative colitis: Implications for the basic scientist Scott Plevy, MD Associate Professor of Medicine, Microbiology & Immunology UNC School of Medicine
A Case of Inflammatory Bowel Disease
 A Case of Inflammatory Bowel Disease Dr Barrie Rathbone www.le.ac.uk 26 year old Polish woman Admitted as emergency under surgeons RUQ and RIF pain Abdominal pain had occurred intermittently for a few
A Case of Inflammatory Bowel Disease Dr Barrie Rathbone www.le.ac.uk 26 year old Polish woman Admitted as emergency under surgeons RUQ and RIF pain Abdominal pain had occurred intermittently for a few
Jonathan R. Dillman, MD, MSc. Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center
 MR Enterography in Children: Interpretation & Value-Added Jonathan R. Dillman, MD, MSc Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center Disclosures Crohn s disease
MR Enterography in Children: Interpretation & Value-Added Jonathan R. Dillman, MD, MSc Associate Professor Department of Radiology Cincinnati Children s Hospital Medical Center Disclosures Crohn s disease
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease
 Mark Lazarev, MD November 14, 2013 Assistant Professor of Medicine, Johns Hopkins University School of Medicine Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease 1 Talk outline
Mark Lazarev, MD November 14, 2013 Assistant Professor of Medicine, Johns Hopkins University School of Medicine Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease 1 Talk outline
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis
 doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
doi: 10.2169/internalmedicine.1607-18 http://internmed.jp CASE REPORT A Case of Crohn s Disease with Mesalazine Allergy that was Difficult to Differentiate from Comorbid Ulcerative Colitis Rumiko Tsuboi,
Referring to Part of Dossier: Volume: Page:
 Synopsis Abbott Laboratories Name of Study Drug: Adalimumab Name of Active Ingredient: Adalimumab Title of Study: Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority
Synopsis Abbott Laboratories Name of Study Drug: Adalimumab Name of Active Ingredient: Adalimumab Title of Study: Individual Study Table Referring to Part of Dossier: Volume: Page: (For National Authority
KEEP CALM AND TREAT TO TARGET IN INFLAMMATORY BOWEL DISEASE
 KEEP CALM AND TREAT TO TARGET IN INFLAMMATORY BOWEL DISEASE This symposium took place on 30 th October 2017, as part of the 25th United European Gastroenterology (UEG) Week in Barcelona, Spain Chairperson
KEEP CALM AND TREAT TO TARGET IN INFLAMMATORY BOWEL DISEASE This symposium took place on 30 th October 2017, as part of the 25th United European Gastroenterology (UEG) Week in Barcelona, Spain Chairperson
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Approximately 80% of patients with Crohn s disease
 CLINICAL REVIEW Postoperative Recurrent Luminal Crohn s Disease: A Systematic Review Peter De Cruz, MD, Michael A. Kamm, PhD, Lani Prideaux, MD, Patrick B. Allen, MD, and Paul V. Desmond, MD Abstract:
CLINICAL REVIEW Postoperative Recurrent Luminal Crohn s Disease: A Systematic Review Peter De Cruz, MD, Michael A. Kamm, PhD, Lani Prideaux, MD, Patrick B. Allen, MD, and Paul V. Desmond, MD Abstract:
Oxford Inflammatory Bowel Disease MasterClass. What is early IBD? Prof. Laurent Peyrin-Biroulet Head, IBD Unit Nancy University Hospital, France
 Oxford Inflammatory Bowel Disease MasterClass What is early IBD? Prof. Laurent Peyrin-Biroulet Head, IBD Unit Nancy University Hospital, France Disclosures Consulting and/or lecture fees from Merck, Abbott,
Oxford Inflammatory Bowel Disease MasterClass What is early IBD? Prof. Laurent Peyrin-Biroulet Head, IBD Unit Nancy University Hospital, France Disclosures Consulting and/or lecture fees from Merck, Abbott,
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura
 Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura") Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease
 Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease Vinna An, Ashwinna Asairinachan, Michael Johnston, James Keck, Paul Salama, Steven Brown, Rodney Woods Department of Colorectal
Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease Vinna An, Ashwinna Asairinachan, Michael Johnston, James Keck, Paul Salama, Steven Brown, Rodney Woods Department of Colorectal
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Cancer Risk with IBD Therapies How to Discuss with your Patients?
 Cancer Risk with IBD Therapies How to Discuss with your Patients? Douglas L Nguyen, MD Assistant Clinical Professor of Medicine University of California, Irvine Medical Center H.H. Chao Comprehensive Digestive
Cancer Risk with IBD Therapies How to Discuss with your Patients? Douglas L Nguyen, MD Assistant Clinical Professor of Medicine University of California, Irvine Medical Center H.H. Chao Comprehensive Digestive
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
Guideline on the development of new medicinal products for the treatment of Crohn s Disease
 28 June 2018 CPMP/EWP/2284/99 Rev. 2 Committee for Medicinal Products for Human Use (CHMP) Guideline on the development of new medicinal products for the treatment of Crohn s Draft agreed by Efficacy Working
28 June 2018 CPMP/EWP/2284/99 Rev. 2 Committee for Medicinal Products for Human Use (CHMP) Guideline on the development of new medicinal products for the treatment of Crohn s Draft agreed by Efficacy Working
IBD What s in it for you?
 Addenbrooke s NHS Trust IBD What s in it for you? Dr Miles Parkes Consultant Gastroenterologist Cambridge What is IBD? - inflammatory bowel disease Ulcerative colitis + Crohn s disease = main forms Incidence
Addenbrooke s NHS Trust IBD What s in it for you? Dr Miles Parkes Consultant Gastroenterologist Cambridge What is IBD? - inflammatory bowel disease Ulcerative colitis + Crohn s disease = main forms Incidence
Genetics. Environment. You Are Only 10% Human. Pathogenesis of IBD. Advances in the Pathogenesis of IBD: Genetics Leads to Function IBD
 Advances in the Pathogenesis of IBD: Genetics Leads to Function Pathogenesis of IBD Environmental Factors Microbes Scott Plevy, MD Associate Professor of Medicine, Microbiology & Immunology UNC School
Advances in the Pathogenesis of IBD: Genetics Leads to Function Pathogenesis of IBD Environmental Factors Microbes Scott Plevy, MD Associate Professor of Medicine, Microbiology & Immunology UNC School
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
Diagnostics and disease monitoring in IBD: State of the art 2011
 Diagnostics and disease monitoring in IBD: State of the art 2011 David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University of Chicago Medical Center The
Diagnostics and disease monitoring in IBD: State of the art 2011 David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University of Chicago Medical Center The
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Predictors of recurrence of Crohn s disease after ileocolectomy: A review
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i39.14393 World J Gastroenterol 2014 October 21; 20(39): 14393-14406 ISSN 1007-9327
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i39.14393 World J Gastroenterol 2014 October 21; 20(39): 14393-14406 ISSN 1007-9327
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Highlights of DDW 2015: Crohn s disease
 Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Highlights of DDW 2015: Crohn s disease Mark S. Silverberg, MD, PhD, FRCPC Associate Professor of Medicine, University of Toronto Staff Gastroenterologist, Mount Sinai Hospital Senior Investigator, Lunenfeld-Tanenbaum
Selective leucocyte trafficking inhibitors for treatment of IBD
 Selective leucocyte trafficking inhibitors for treatment of IBD Séverine Vermeire MD, PhD Department of Gastroenterology University Hospitals Leuven Belgium Migration of Leucocytes plays a key role in
Selective leucocyte trafficking inhibitors for treatment of IBD Séverine Vermeire MD, PhD Department of Gastroenterology University Hospitals Leuven Belgium Migration of Leucocytes plays a key role in
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 5 2016 Article 4 Isolated Jejunal Crohn s Disease, A Diagnostic Dilemma Elise Biesboer BS Lacey Stelle MD Michelle M. Olson MD, MACM Paul Tender MD University
World Journal of Colorectal Surgery Volume 6, Issue 5 2016 Article 4 Isolated Jejunal Crohn s Disease, A Diagnostic Dilemma Elise Biesboer BS Lacey Stelle MD Michelle M. Olson MD, MACM Paul Tender MD University
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Inflammatory Bowel Disease: Updates and Controversies CASE #1 CASE #1 8/6/2015. What is the most likely diagnosis?
 Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Inflammatory Bowel Disease: Updates and Controversies Tehttp://192.185.93.102/~paulkeij/wpcontent/uploads/2013/07/collaboration.jpgxt August 7, 2015 Meagan M Costedio, MD; Colorectal Surgery; Cleveland
Anus,Rectum and Colon
 JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp ORIGINAL RESEARCH ARTICLE Risk factors for recurrence of Crohn s disease requiring surgery in patients receiving post-operative anti-tumor necrosis
JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp ORIGINAL RESEARCH ARTICLE Risk factors for recurrence of Crohn s disease requiring surgery in patients receiving post-operative anti-tumor necrosis
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency London, 22 February 2007 Doc. Ref. CPMP/EWP/2284/99 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON THE DEVELOPMENT OF NEW MEDICINAL PRODUCTS FOR
European Medicines Agency London, 22 February 2007 Doc. Ref. CPMP/EWP/2284/99 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON THE DEVELOPMENT OF NEW MEDICINAL PRODUCTS FOR
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University