High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease
|
|
|
- Charlotte Arnold
- 5 years ago
- Views:
Transcription

1 Accepted Manuscript High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease Shailja C. Shah, Joren R. ten Hove, Daniel Castaneda, Carolina Palmela, Erik Mooiweer, Jean-Frédéric Colombel, Noam Harpaz, Thomas A. Ullman, Ad A. van Bodegraven, Jeroen M. Jansen, Nofel Mahmmod, Andrea E. van der Meulen-de Jong, Cyriel Y. Ponsioen, Christine J. van der Woude, Bas Oldenburg, Steven H. Itzkowitz, Joana Torres PII: S (18) DOI: /j.cgh Reference: YJCGH To appear in: Clinical Gastroenterology and Hepatology Accepted Date: 12 January 2018 Please cite this article as: Shah SC, ten Hove JR, Castaneda D, Palmela C, Mooiweer E, Colombel J-F, Harpaz N, Ullman TA, van Bodegraven AA, Jansen JM, Mahmmod N, van der Meulen-de Jong AE, Ponsioen CY, van der Woude CJ, Oldenburg B, Itzkowitz SH, Torres J, High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease, Clinical Gastroenterology and Hepatology (2018), doi: /j.cgh This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 Manuscript Number: CGH Title: High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease Authors: Shailja C. Shah 1,2 *, Joren R. ten Hove 3 *, Daniel Castaneda 1, Carolina Palmela 1, Erik Mooiweer 3, Jean-Frédéric Colombel 1, Noam Harpaz 1, Thomas A. Ullman 1, Ad A. van Bodegraven 4, Jeroen M. Jansen 5, Nofel Mahmmod 6, Andrea E. van der Meulen-de Jong 7, Cyriel Y. Ponsioen 8, Christine J. van der Woude 9, Bas Oldenburg 3, Steven H. Itzkowitz 1, Joana Torres 1,10. *These two authors contributed equally to this work. Institutions: 1) The Henry D. Janowitz Division of Gastroenterology, Icahn School of Medicine at Mount Sinai, New York, NY, USA. 2) Department of Gastroenterology and Hepatology, Vanderbilt University Medical Center, Nashville, Tennessee. 3) Department of Gastroenterology and Hepatology, University Medical Center Utrecht, Utrecht, The Netherlands. 4) Department of Gastroenterology and Hepatology, Vrije Universiteit Medical Center Amsterdam, Amsterdam, The Netherlands. 5) Department of Gastroenterology and Hepatology, Onze Lieve Vrouwe Gasthuis Amsterdam, Amsterdam, The Netherlands 6) Department of Gastroenterology and Hepatology, St Antonius Hospital Nieuwegein, Nieuwegein, The Netherlands 7) Department of Gastroenterology and Hepatology, Leiden University Medical Center, Leiden, The Netherlands. 8) Department of Gastroenterology and Hepatology, Amsterdam Medical Center, Amsterdam, The Netherlands. 9) Department of Gastroenterology and Hepatology, Erasmus Medical Center Rotterdam, Rotterdam, The Netherlands. 10) Surgical Department, Gastroenterology Division, Hospital Beatriz Ângelo, Loures, Portugal Grant Support: None Disclosures/Conflict of interest statement: The authors have no potential conflicts (financial, professional, nor personal) that are relevant to this manuscript. Writing assistance: No additional writing assistance was used for this manuscript Author contributions: JRtH, SCS and JT: study concept and design, data acquisition, data analysis and interpretation, manuscript writing; DC, CP, EM, NH, AAvB, JMJ, NM, AvdM, CYP, CJvdW: data acquisition, review of final manuscript; JFC, TAU, BO, SHI: study concept and design, data interpretation, critical revision of the manuscript for important intellectual content 1
3 Corresponding Author: Joana Torres, MD 1468 Madison Avenue Annenberg Building, 5 th Floor, Room 5-12 Box 1069 New York, NY USA Ph: joanatorres00@gmail.com 2
4 Abstract: Background & Aims: Patients with inflammatory bowel disease (IBD) and primary sclerosing cholangitis (PSC, termed PSC-IBD) are at increased risk for colorectal cancer (CRC), but their risk following a diagnosis of low-grade dysplasia (LGD) is not well described. We aimed to determine the rate of advanced colorectal neoplasia (acrn), defined as high-grade dysplasia and/or colorectal cancer, following a diagnosis of indefinite dysplasia or LGD in this population. Methods: We performed a retrospective, longitudinal study of 1911 patients with colonic IBD (293 with PSC and 1618 without PSC) who underwent more than 2 surveillance colonoscopies from 2000 through 2015 in the Netherlands or the United States (9265 patient-years of follow up). We collected data on clinical and demographic features of patients, as well as data from each surveillance colonoscopy and histologic reports. For each surveillance colonoscopy, the severity of active inflammation was documented. The primary outcome was a diagnosis of acrn during follow up. We also investigated factors associated with acrn in patients with or without a prior diagnosis of indefinite dysplasia or LGD. Results: Patients with PSC-IBD had a 2-fold higher risk of developing acrn than patients with IBD only. Mean inflammation scores did not differ significantly between patients with PSC-IBD (0.55) vs patients with only IBD (0.56) (P=0.89), nor did proportions of patients with LGD (21% of patients with PSC-IBD vs 18% of patients with only IBD) differ significantly (P=0.37). However, the rate of acrn following a diagnosis of LGD was significantly higher in patients with PSC-IBD (8.4 per 100 patient-years) than patients with only IBD (3.0 per 100 patient-years) (P=0.01). PSC (adjusted hazard ratio [ahr], 2.01; 95% CI, ), increasing age (ahr 1.03; 95% CI, ), and active inflammation (ahr, 2.39; 95% CI, ) were independent risk factors for acrn. Dysplasia was more often endoscopically invisible in patients with PSC-IBD than in patients with only IBD. Conclusion: In a longitudinal study of almost 2000 patients with colonic IBD, PSC remained a strong independent risk factor for acrn. Once LGD is detected, acrn develops at a higher rate in patients with PSC and is more often endoscopically invisible than in patients with only IBD. 3
5 Our findings support recommendations for careful annual colonoscopic surveillance for patients with IBD and PSC, and consideration of colectomy once LGD is detected. KEY WORDS: surveillance; colon cancer; Crohn s disease; ulcerative colitis 4
6 87 Introduction 88 Patients with inflammatory bowel disease (IBD) are at an increased risk of developing colorectal cancer (CRC). 1,2 The co-occurrence of primary sclerosing cholangitis (PSC) 1,3, a chronic liver disease characterized by progressive inflammation and fibrosis of the bile ducts 4, increases this risk substantially. 5 While an estimated 70% of patients with PSC have a concomitant diagnosis of IBD (termed PSC-IBD) 6, only 3-5% of patients with IBD have concomitant PSC, with the diagnosis more common in patients with ulcerative colitis (UC). 7,5 The PSC-IBD phenotype is often characterized by extensive colitis with rectal sparing and backwash ileitis, albeit with a mild and often asymptomatic clinical course. 8,9,10,11,12,13 However, despite their mild clinical colitis, patients with PSC-IBD compared to patients with only IBD colitis have a 3- to 5-fold higher risk of CRC, and the cancers more often occur in the right colon. 14,15 As such, current guidelines recommend that patients with PSC-IBD be enrolled in a CRC surveillance program with annual colonoscopy from the time of PSC diagnosis, regardless of their duration of IBD. This is in contrast to those with IBD colitis and no PSC (non-psc IBD), where CRC surveillance is recommended after 8 years of colonic disease. 5,16,17,18 The development of neoplasia in IBD colitis follows a multistep sequence from chronic inflammation and no dysplasia or indefinite dysplasia (IND) to low grade-dysplasia (LGD) and high-grade dysplasia (HGD) prior to final malignant transformation to adenocarcinoma. As such, the presence and grade of dysplasia remain the best current indicators of cancer risk in IBD. There is an increasing tendency to keep patients with LGD on intensive surveillance instead of recommending proctocolectomy. 19,20 However, very few studies have described the risk of acrn 108 in patients with PSC-IBD following a diagnosis of IND and/or LGD. 21,22 Further, the studies that 5
7 do report on the risk of neoplasia in patients with PSC-IBD were performed in an era where imaging enhanced endoscopy and high-resolution endoscopy were not routinely used The aims of the present study were to report on the risk of acrn in a well-characterized cohort of patients with PSC-IBD enrolled in a surveillance program in the modern endoscopic era, and to describe the rate of acrn after a diagnosis of IND and/or LGD in these patients compared to patients with non-psc IBD and longstanding IBD colitis also undergoing surveillance. Methods Study population and case identification Patients with established IBD colitis undergoing colonoscopic surveillance between were retrospectively identified from two databases: a Dutch database inclusive of 2 secondary and 6 tertiary centers and the Mount Sinai Hospital database in New York City inclusive of one tertiary IBD referral center. Cases were identified by query of the electronic health record (EHR)-linked database utilizing both ICD-9 and -10 codes and free text searches for cases of IBD and also free text searches for PSC. Patient selection (inclusion and exclusion criteria) After initial identification through the EHR query, individual charts were reviewed. For patients with PSC-IBD, a clinical diagnosis of PSC had to be confirmed by distinctive features on cholangiography or liver biopsy (for those with small-duct PSC). Additional inclusion criteria were: 1) diagnosis of IBD (UC, CD, IBD undifferentiated [IBD-U]) with colonic involvement confirmed endoscopically and histologically; 2) confirmed colonic disease duration of at least 8 years for patients with non-psc IBD or any colonic disease duration for patients 6
8 with PSC-IBD; 3) enrollment in a surveillance program and 4) at least left-sided colitis (UC or IBD-U) or involvement of >30% of the colonic surface (CD or IBD-U). Patients with a history of colectomy prior to enrollment or history of acrn prior to or at the index colonoscopy during the defined study period were excluded. Surveillance procedures were defined as colonoscopies in which either segmental random biopsies or chromoendoscopy were employed. Colonoscopies with other indications, e.g. medically refractory disease, were excluded. The index colonoscopy was defined as the first surveillance colonoscopy performed within the study period ( ). Data collection Database coding was identical for all study populations. The date of study entry was set at the first surveillance colonoscopy in the database. The time of onset of PSC or IBD was determined from EHR review. The date of the last colonoscopy was set as the last day of followup. The following baseline demographic and clinical data were abstracted: date of birth, sex, date of PSC diagnosis (if applicable), date of IBD diagnosis, IBD type, maximum disease extent, and date of prior diagnosis of IND and/or LGD (if applicable). Maximum disease extent was defined as the maximum documented extent of endoscopic disease on any colonoscopy and was coded as follows: extensive/pancolitis (>50%) or intermediate/left-sided (30-50%). Medication exposure (at least one prescription) was recorded for 5-aminosalicylates (5-ASA), thiopurines, and biologics. Data from each surveillance colonoscopy was recorded, including date of exam, quality of bowel preparation (adequate or inadequate), most proximal extent examined, use of chromoendoscopy, presence and severity of endoscopic inflammation, presence of post- 7
9 inflammatory polyps ( pseudopolyps ), stricture(s) and visible lesions. Endoscopically detected neoplastic lesions were categorized based on morphology (polypoid/non-polypoid) Endoscopically invisible neoplasia was defined as neoplasia detected in a random biopsy with no corresponding morphologic lesion seen on endoscopy. Right-sided lesions were defined as those proximal to the splenic flexure. Because this was a retrospective study, there was no a priori protocol in place to record endoscopic activity in a uniform way. Thus, for each surveillance colonoscopy, severity of active endoscopic inflammation was scored on a 4-point scale for each colonic segment visualized to allow for standardization: 0 (no inflammation/remission), 1 (mild inflammation), 2 (moderate inflammation) or 3 (severe inflammation). A mean inflammatory severity score per patient and per colonoscopy was calculated by dividing the sum of inflammatory severity scores by the total number of colonic segments visualized per colonoscopy and then by the total number of surveillance colonoscopies. Histology Dysplasia was recorded as indefinite (IND), low-grade (LGD), or high-grade (HGD). All histologic diagnoses were as reported in the original pathology report; no specimens were rereviewed or altered for this study. Of note, it is routine clinical practice at each participating institution that all pathology concerning for colorectal neoplasia is reviewed at the time of diagnosis and agreed upon by at least two pathologists. Primary and secondary outcomes The primary outcome was a diagnosis of acrn, defined as HGD or CRC, during follow up. Secondary outcomes were a diagnosis of IND and/or LGD during follow-up and the development of acrn following a diagnosis of IND and/or LGD. Factors associated with a 8
10 diagnosis of acrn in patients with PSC-IBD or patients with non-psc IBD with or without a prior diagnosis of IND and/or LGD were explored Statistical analysis Basic descriptive statistics were generated for patients meeting inclusion criteria. Chisquare and Fisher s exact tests were used to compare categorical variables and dichotomous outcomes, while the Student s t-test and Mann-Whitney U-test were used for analyzing continuous data. Incidence rates were calculated as the number of cases per 100 patient-years (pty) of follow-up. Univariate and multivariate Cox-regression modeling was used to identify factors associated with acrn. The proportional hazards assumption of time-static covariates was assessed using log-log plots and Schoenfeld residuals. Because inflammatory scores were not stable over time, these were inputted as time-changing covariates into the models. Mean inflammation scores were re-calculated at every time-point for each patient to correct for the also variable number of colonoscopies. A p-value of 0.10 was used as the cutoff for selecting variables for the multivariate analysis. Kaplan-Meier survival curves were generated to compare cumulative incidence rates. Follow-up data were censored at the last point of colonoscopic follow-up, acrn diagnosis, or colectomy. All data analyses were performed using SPSS version 22 (Armonk, NY: IBM Corp.). Study Oversight The Institutional Review Board (IRB) for each of the included sites approved the creation and analysis of a longitudinal retrospective cohort database of patients with colonic IBD 197 undergoing surveillance
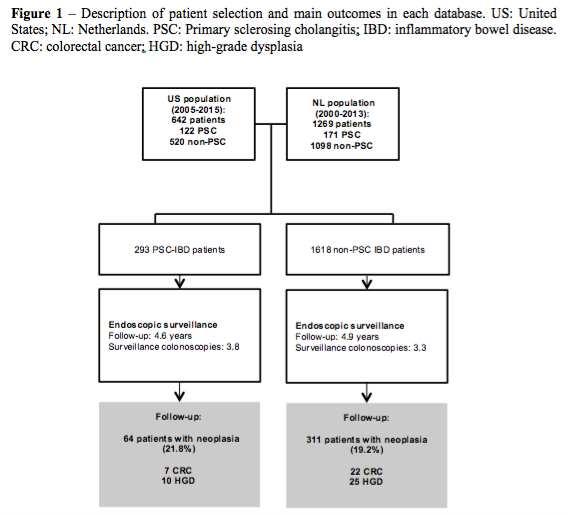
11 199 Results 200 Baseline demographic and clinical characteristics Of 1,911 patients with colonic IBD in the combined database meeting inclusion criteria, 293 patients were confirmed to have PSC-IBD; the remaining 1,618 patients with non-psc IBD served as the comparison group (Figure 1). Main demographic and clinical features of the cohort are detailed in Table 1. Compared with the non-psc IBD group, patients with PSC-IBD were more often male and younger at study entry, although the age of IBD diagnosis was similar between groups (p=0.11). As expected, UC was the predominant IBD type in the PSC-IBD group. Patients with PSC-IBD were less frequently exposed to IBD therapy compared to patients with non-psc IBD. In 151 patients (51.5%), the PSC diagnosis was established after the IBD diagnosis, while in 36 (12.3%) PSC was established before the IBD diagnosis. For the remainder, PSC and IBD were diagnosed within the same year or the sequence of diagnoses was not recorded. The mean follow-up for the total cohort was 4.8 (±3.0) years, with a total of 9,265 patient-years of follow-up; there was no difference in follow-up time between patients with PSC- IBD and patients with non-psc IBD. The number of surveillance colonoscopies performed within the study period was higher in patients with PSC-IBD compared to patients with non- PSC IBD (3.8 vs. 3.3, p<0.01). Inflammatory activity The endoscopic severity of inflammation on surveillance exams was similar between patients with PSC-IBD and patients with non-psc IBD (Supplementary Table 1). The proportion of procedures in which extensive active disease was observed in patients with PSC-IBD vs 10
12 patients with non-psc IBD patients was 27% vs 12% (p<0.01), 23% vs 10% (p<0.01), and 27% vs 10% (p<0.01) for the first, second and third surveillance colonoscopy, respectively. The proportion of patients in endoscopic remission on each of their surveillance colonoscopies during the entire study period was higher in patients with non-psc IBD compared to patients with PSC- IBD (p=0.02). Occurrence of acrn and associated risk factors Among patients with PSC-IBD, acrn was diagnosed in 17 patients (5.8%), with CRC in 7 (2.4%) and HGD in 10 patients (3.4%) (Table 2). The frequency of acrn during follow-up was significantly lower in patients with non-psc IBD (2.9%), with CRC and HGD diagnosed in 1.4% and 1.5% patients respectively (p=0.01). The incidence rate of acrn in patients with PSC- IBD compared to patients with non-psc IBD was significantly higher (1.3 vs. 0.6/100pty, p<0.01) (Figure 2). While acrn was more often right-sided in patients with PSC-IBD compared to patients with non-psc IBD, this was not statistically significant (53% vs. 31%, p=0.12). Among 40 patients with PSC-IBD (14%) where the diagnosis of PSC was newly established within the study period, three cases of acrn occurred, with a mean duration of 4.0 years (±2.5) between the PSC diagnosis and acrn occurrence. The primary outcomes stratified by study site are detailed in Supplementary Table 2. On multivariate Cox-regression analysis, PSC (adjusted HR (ahr) 2.01, 95%CI: ), increasing age (ahr 1.03, 95% CI: ), and active inflammation (ahr 2.39, 95%CI: ) remained independent predictors of acrn diagnosis during follow-up (Table ). Correcting for geography (US vs. Netherlands) did not affect these findings (Supplementary Table 3) 11
13 243 Risk of acrn following a diagnosis of IND and/or LGD 244 The number of patients in the total cohort with at least one diagnosis of IND was (7.7%). In 101 patients (5.3%) no additional dysplasia was detected. Among patients with a diagnosis of IND, the rate of developing acrn following detection of IND was higher in patients with PSC-IBD compared to patients with non-psc IBD (p=0.02, Supplementary Figure 1). However, when patients with a synchronous or metachronous diagnosis of LGD (n=46) were excluded from this analysis (i.e. no grade of dysplasia higher than IND), this difference was no longer significant. The occurrence of at least one LGD-containing lesion during the study period was similar for both patients with PSC-IBD and patients with non-psc IBD (21% vs. 18%, p=0.37). Despite a similar proportion of patients with LGD, the rate of developing acrn following detection of LGD was almost 3-fold higher in patients with PSC-IBD compared to patients with non-psc IBD (8.4 vs. 3.0/100pty, p=0.01, Figure 3). For the subgroup of patients with LGD, the number of patients in whom endoscopically invisible LGD was detected over the course of surveillance was higher in patients with PSC-IBD (38% vs. 22%, p=0.01). The proportion of invisible LGD cases among the total number of LGD cases (per-colonoscopy analysis) was also higher. In a sub-analysis of the Netherlands population, we corrected for the total number of random biopsies taken (107,745 biopsies in total); the number of random biopsies needed to detect invisible dysplasia was 826 in patients with PSC-IBD compared to 1,703 in patients with non-psc IBD On univariate Cox regression analysis, only PSC and multifocal dysplasia were associated with higher risk of acrn diagnosis following LGD detection, while polypoid 12
14 morphology of the lesion (vs. nonpolypoid or invisible) was associated with a lower risk. On multivariate analysis, only polypoid morphology remained significant and was associated with a reduced risk of acrn (ahr 0.31, 95%CI: ) following LGD detection compared to nonpolypoid or endoscopically invisible lesions (Supplementary Table 4). Discussion In this large, multicenter, cross-national longitudinal cohort study of patients with confirmed IBD colitis undergoing colonoscopic CRC surveillance, we report a higher risk of acrn in patients with concomitant PSC as compared to those without PSC, in the current era of improved endoscopic technology and more effective medical therapy for inflammation. While these findings corroborate previous studies, we further expand knowledge in the field by reporting an even higher risk of acrn following detection of LGD (but not IND alone). That LGD was more often endoscopically invisible in patients with PSC-IBD compared to patients with non-psc IBD justifies the more intensive management considerations for this population. Our findings suggest that while continued meticulous CRC surveillance with annual colonoscopy is indicated in the absence of dysplasia for patients with PSC-IBD, the detection of LGD or higher-grade pathology should lead to a careful weighting of the pros and cons of more aggressive therapeutic management, including colectomy. In our well-characterized surveillance cohort, which to our knowledge is the largest published cohort of patients with PSC-IBD undergoing surveillance, we found that having PSC- IBD is associated with a 2-fold higher risk of acrn. This risk is slightly lower than prior studies and a recent meta-analysis of 16 studies that reported a 3.4 fold higher odds for colorectal neoplasia in patients with PSC-IBD. 23 Importantly, the increased risk in our study remained after 13
15 correcting for active endoscopic inflammation over time (which was employed as a time- changing covariate rather than a mean overall score). Endoscopic activity assessed during subsequent colonoscopies was strongly associated with the risk of future acrn, congruent with studies in the population with non-psc IBD. 24,25,26 Whether the outcomes of endoscopic inflammation compared to histologic inflammation are distinct remains a question for future investigation. The increased risk of CRC in patients with PSC and concomitant colonic IBD has firmly been established, although the underlying mechanisms remain unclear. 27,28,3,29,30 The nearly 3- fold higher rate of acrn (HGD and/or CRC) diagnosis following LGD detection, as well as the difference in location, morphology, and endoscopic conspicuousness of dysplasia in patients with PSC-IBD compared to patients with non-psc IBD suggests nuances in the pathogenesis of neoplasia between these groups. Several authors have proposed a role for altered colonic bile composition in carcinogenesis. A right-sided predominance of neoplasia reinforces this hypothesis, as well as several studies directly measuring the bile acid composition in both animals and humans. 31,29,32 There is also evidence supporting the notion that patients with PSC have an altered colonic microbiome irrespective of concurrent IBD or UDCA treatment. 33 Still, whether these bacterial alterations are a cause or a consequence of the disease characteristics specific to PSC remains to be clarified. Patients with PSC also share a distinct genotype 34, which may further predispose them to neoplastic progression. More likely, the underlying etiologies are multifactorial with roles for gene-environment interactions, the microbiome, and epigenetic modifications. Further investigations will hopefully open new avenues for novel therapeutic 308 discovery and primary and secondary prevention. 14
16 All told, because the mechanisms underlying PSC as an independent risk factor for CRC in the setting of IBD colitis are unclear, the best strategy for CRC prevention in patients with PSC-IBD remains frequent, attentive surveillance colonoscopy. An important observation from our study that distinguishes patients with PSC-IBD from patients with non-psc IBD, is that dysplasia was more often detected in random biopsies. While previous retrospective studies have shown a low overall yield for dysplasia with random biopsies as opposed to only targeted biopsies of visible lesions, there was higher yield for dysplasia on random biopsy in those with concurrent PSC. 35,36 Our data further add to this body of evidence, and it can therefore be questioned whether the current recommendation, based on the results of prospective studies, to move away from random biopsies as part of CRC surveillance should preclude patients with PSC-IBD. 37,38 During surveillance examinations, particular attention should be paid to the proximal colon as right-sided cancers seem to be more common in patients with PSC-IBD compared to patients with non-psc IBD colitis. 32 While the proportion of right-sided acrn was higher in the PSC-IBD subgroup, this difference was not statistically significant in the present study and may be due to insufficient power; it may also reflect selection bias since one of our inclusion criteria for the non-psc IBD subgroup was at least left-sided disease extent or more than 30% involvement, and thus may not represent the overall IBD population. Our study confirms that the date of PSC diagnosis is particularly relevant when risk-stratifying patients, since it seems that the risk of neoplastic progression is highest within the first few years of the PSC diagnosis. 39 Thus, while CRC surveillance is recommended after disease duration of 8 years in patients with colonic IBD and no PSC 40, CRC surveillance at the time of diagnosis in the 330 setting of PSC is recommended and further corroborated by our findings. 15
17 Our study has several strengths. In addition to being perhaps the largest IBD surveillance cohort in the modern era, our cohort is particularly robust since each patient was confirmed to have colonic IBD and to be actively enrolled in a colonoscopic CRC surveillance program. Comprehensive data on disease history and endoscopic findings during surveillance allowed for more accurate neoplastic risk assessment, particularly with respect to measurement of inflammatory burden over time. Importantly, detailed information on inflammatory activity at each colonoscopy was incorporated into the analysis for more accurate assessment of acrn development in patients with PSC-IBD. Our study also has some limitations, most notably the retrospective design. Despite the large size of our PSC-IBD cohort, additional sub-analyses, such as stratification according to IBD type or medication use, yielded insufficient power to permit meaningful conclusions. Although we combined surveillance cohorts from two different countries, we predefined the inclusion/exclusion criteria, variables to be assessed, and definitions of outcomes. Combining these two cohorts enhanced not only our power to detect meaningful differences, but also the generalizability of our findings given that our study population included patients from affiliated community-based sites as well as tertiary IBD referral centers. That said, there may be unmeasured differences in care pathways between the Netherlands and US leading to heterogeneity in our study results. It is important to note, however, that after adjusting for study site and clinical-demographic differences between the Netherlands and US cohorts, our results remained significant (supplementary table 3). The lack of standardized guidelines for the use of chromoendoscopy for CRC surveillance in patients with IBD colitis unfortunately precluded a meaningful analysis of its impact on dysplasia detection since 10% of exams were performed with chromoendoscopy. Finally, while no samples were re-reviewed by pathologists for the 16
18 purposes of this study, it is routine practice at all institutions participating in this study that whenever there is a diagnosis of CRN, that the specimen is reviewed by two pathologists and consensus reached before final reporting. In summary, using a large well-characterized cohort of patients with confirmed colonic IBD undergoing surveillance between , we substantiated prior smaller reports of the increased risk of acrn in patients with concurrent PSC-IBD compared to patients with only IBD colitis undergoing surveillance. Novel findings of our study include the significantly higher rate of acrn diagnosis following a diagnosis of LGD in the setting of PSC complicating IBD. This finding together with a higher risk of invisible dysplasia in patients with PSC-IBD highlights the need for an ongoing strict CRC surveillance program in these patients and a low threshold to advise colectomy once LGD is detected in this select population. 17
19 367 References: Lutgens MWMD, van Oijen MGH, van der Heijden GJMG, et al. Declining risk of colorectal cancer in inflammatory bowel disease: an updated meta-analysis of populationbased cohort studies. Inflamm Bowel Dis 19: Jess T, Rungoe C, Peyrin Biroulet L. Risk of Colorectal Cancer in Patients With Ulcerative Colitis: A Meta-analysis of Population-Based Cohort Studies. Clin Gastroenterol Hepatol 2012;10: Claessen MMH, Vleggaar FP, Tytgat KMAJ, et al. High lifetime risk of cancer in primary sclerosing cholangitis. J Hepatol 2009;50: Horsley-Silva JL, Carey EJ, Lindor KD. Advances in primary sclerosing cholangitis. Lancet Gastroenterol Hepatol 2016;1: Torres J, Pineton de Chambrun G, Itzkowitz S, et al. Review article: colorectal neoplasia in patients with primary sclerosing cholangitis and inflammatory bowel disease. Aliment Pharmacol Ther 2011;34: Weismüller TJ, Trivedi PJ, Bergquist A, et al. Patient Age, Sex, and Inflammatory Bowel Disease Phenotype Associate With Course of Primary Sclerosing Cholangitis. Gastroenterology March Olsson R, Danielsson A, Järnerot G, et al. Prevalence of primary sclerosing cholangitis in patients with ulcerative colitis. Gastroenterology 1991;100: Boonstra K, van Erpecum KJ, van Nieuwkerk KMJ, et al. Primary sclerosing cholangitis is associated with a distinct phenotype of inflammatory bowel disease. Inflamm Bowel Dis 2012;18: O Toole A, Alakkari A, Keegan D, et al. Primary Sclerosing Cholangitis and Disease Distribution in Inflammatory Bowel Disease. Clin Gastroenterol Hepatol 2012;10: Penna C, Dozois R, Tremaine W, et al. Pouchitis after ileal pouch-anal anastomosis for ulcerative colitis occurs with increased frequency in patients with associated primary sclerosing cholangitis. Gut 1996;38: Loftus E V, Harewood GC, Loftus CG, et al. PSC-IBD: a unique form of inflammatory bowel disease associated with primary sclerosing cholangitis. Gut 2005;54: De Vries AB, Janse M, Blokzijl H, et al. Distinctive inflammatory bowel disease phenotype in primary sclerosing cholangitis. World J Gastroenterol 2015;21:
20 Sinakos E, Samuel S, Enders F, et al. Inflammatory Bowel Disease in Primary Sclerosing Cholangitis. Inflamm Bowel Dis 2013;19: Lundqvist K, Broomé U. Differences in colonic disease activity in patients with ulcerative colitis with and without primary sclerosing cholangitis: a case control study. Dis Colon Rectum 1997;40: Soetikno RM, Lin OS, Heidenreich PA, et al. Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and ulcerative colitis: a meta-analysis. Gastrointest Endosc 2002;56: Farraye FA, Odze RD, Eaden J, et al. AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology 2010;138: Annese V, Daperno M, Rutter MD, et al. European evidence based consensus for endoscopy in inflammatory bowel disease. J Crohns Colitis 2013;7: Broomé U, Löfberg R, Lundqvist K, et al. Subclinical time span of inflammatory bowel disease in patients with primary sclerosing cholangitis. Dis Colon Rectum 1995;38: Pekow JR, Hetzel JT, Rothe JA, et al. Outcome after surveillance of low-grade and indefinite dysplasia in patients with ulcerative colitis. Inflamm Bowel Dis 2010;16: Fumery M, Dulai PS, Gupta S, et al. Incidence, Risk Factors, and Outcomes of Colorectal Cancer in Patients with Ulcerative Colitis with Low-Grade Dysplasia: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol December Venkatesh PGK, Jegadeesan R, Gutierrez NG, et al. Natural history of low grade dysplasia in patients with primary sclerosing cholangitis and ulcerative colitis. J Crohn s Colitis 2013;7: Eaton JE, Smyrk TC, Imam M, et al. The fate of indefinite and low-grade dysplasia in ulcerative colitis and primary sclerosing cholangitis colitis before and after liver transplantation. Aliment Pharmacol Ther 2013;38: Zheng H-H, Jiang X-L. Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and inflammatory bowel disease. Eur J Gastroenterol Hepatol 2016;28: Rutter M, Saunders B, Wilkinson K, et al. Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology 2004;126:
21 Rubin DT, Huo D, Kinnucan JA, et al. Inflammation is an independent risk factor for colonic neoplasia in patients with ulcerative colitis: a case-control study. Clin Gastroenterol Hepatol 2013;11: e1-e Gupta RB, Harpaz N, Itzkowitz S, et al. Histologic inflammation is a risk factor for progression to colorectal neoplasia in ulcerative colitis: a cohort study. Gastroenterology 2007;133: ; quiz Broomé U, Löfberg R, Veress B, et al. Primary sclerosing cholangitis and ulcerative colitis: evidence for increased neoplastic potential. Hepatology 1995;22: Kornfeld D, Ekbom A, Ihre T. Is there an excess risk for colorectal cancer in patients with ulcerative colitis and concomitant primary sclerosing cholangitis? A population based study. Gut 1997;41: Shetty K, Rybicki L, Brzezinski A, et al. The risk for cancer or dysplasia in ulcerative colitis patients with primary sclerosing cholangitis. Am J Gastroenterol 1999;94: Navaneethan U, Venkatesh PGK, Lashner BA, et al. Temporal trends in colon neoplasms in patients with primary sclerosing cholangitis and ulcerative colitis. J Crohn s Colitis 2012;6: Barrasa JI, Olmo N, Lizarbe MA, et al. Bile acids in the colon, from healthy to cytotoxic molecules. Toxicol In Vitro 2013;27: Claessen MMH, Lutgens MWMD, van Buuren HR, et al. More right-sided IBDassociated colorectal cancer in patients with primary sclerosing cholangitis. Inflamm Bowel Dis 2009;15: Sabino J, Vieira-Silva S, Machiels K, et al. Primary sclerosing cholangitis is characterised by intestinal dysbiosis independent from IBD. Gut 2016;65: Ji S-G, Juran BD, Mucha S, et al. Genome-wide association study of primary sclerosing cholangitis identifies new risk loci and quantifies the genetic relationship with inflammatory bowel disease. Nat Genet December Navaneethan U, Kochhar G, Venkatesh PGK, et al. Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary sclerosing cholangitis and ulcerative colitis. J Crohns Colitis 2013;7: Van den Broek FJC, Stokkers PCF, Reitsma JB, et al. Random biopsies taken during colonoscopic surveillance of patients with longstanding ulcerative colitis: low yield and absence of clinical consequences. Am J Gastroenterol 2014;109:
22 Moussata D, Allez M, Cazals-Hatem D, et al. Are random biopsies still useful for the detection of neoplasia in patients with IBD undergoing surveillance colonoscopy with chromoendoscopy? Gut 2017:gutjnl Watanabe T, Ajioka Y, Mitsuyama K, et al. Comparison of Targeted vs Random Biopsies for Surveillance of Ulcerative Colitis-associated Colorectal Cancer. Gastroenterology August Navaneethan U, Kochhar G, Venkatesh PGK, et al. Duration and severity of primary sclerosing cholangitis is not associated with risk of neoplastic changes in the colon in patients with ulcerative colitis. Gastrointest Endosc 2012;75: e Lutgens MWMD, Vleggaar FP, Schipper MEI, et al. High frequency of early colorectal cancer in inflammatory bowel disease. Gut 2008;57: Figure Legends (Main): Figure 1 Description of patient selection and main outcomes in each database. Figure 2 Kaplan-Meier time-to-event (acrn) analysis, all patients since study entry. Figure 3 Kaplan-Meier time-to-event (acrn) analysis, patients with LGD only. 21
23 Table 1: Baseline characteristics of the study population. PSC: Primary sclerosing cholangitis; IBD: inflammatory bowel disease. PSC-IBD (n=293) Non-PSC IBD (n=1618) p-value Male (%) 205 (70.0%) 796 (49.2%) <0.001 Age at study inclusion, years, mean (standard deviation (SD)) IBD type - Ulcerative colitis - Crohn s colitis - Indeterminate colitis Disease extent - Not specified - Limited extent/proctitis - Intermediate/Left-sided - Extensive/pancolitis Age at IBD diagnosis, years, mean (SD) 39 (14) 45 (13) < (69.3%) 76 (25.9%) 14 (4.8%) 34 (11.8%) 13 (4.5%) 41 (14.2%) 201 (69.6%) 912 (56.4%) 661 (40.9%) 45 (2.8%) 154 (9.6%) 49 (3.1%) 572 (35.8%) 823 (51.5%) <0.001 < (13) 28 (12) 0.11 IBD duration, years, mean (SD) 12 (10) 17 (9) <0.001 Age at PSC diagnosis, years, mean (SD) Medication use - 5-aminosalicylates - Thiopurines - Biologicals Duration of follow-up after index colonoscopy, years - mean (SD) - median Number of surveillance colonoscopies (mean) 32 (14) (75.4%) 93 (31.7%) 38 (13.0%) 4.6 (3.2) (81.3%) 825 (51.0%) 402 (24.8%) 4.9 (3.0) <0.001 < <0.001
24 Table 2: Description of the outcomes during the study period. CRC=colorectal cancer, HGD=high-grade dysplasia, LGD=low-grade dysplasia, AN=advanced neoplasia, y=years Advanced neoplasia (acrn) - CRC - HGD LGD (patients with 1 LGD lesion) IND (patients with IND as highest grade lesion) Time from IBD diagnosis to acrn diagnosis, years, mean Time from database entry to acrn diagnosis, years, mean Time from LGD to acrn diagnosis, years, mean PSC-IBD (n=293) 17 (5.8%) 7 (2.4%) 10 (3.4%) Non-PSC IBD (n=1618) 47 (2.9%) 22 (1.4%) 25 (1.5%) p-value (20.5%) 295 (18.2%) (9.2%) 74 (4.6%)
25 Table 3: Uni- and multivariate Cox-regression analysis for the overall risk of acrn (all patients). Univariate Multivariate Variable HR 95% CI P-value ahr 95% CI P-value Age, years Age at IBD diagnosis Sex (reference: male) PSC Inflammation severity, mean [0-3]* < <0.001 IBD type (reference: UC) Maximum disease extent (reference: pancolitis) Thiopurine exposure Biological exposure aminosalicylate exposure Number of surveillance procedures *entered as time-changing covariate; 0 (no inflammation/remission), 1 (mild), 2 (moderate), 3 (severe)
26
27
28
29 Supplementary Table 1: Inflammatory parameters during surveillance. *=corrected for total number of surveillance colonoscopies per patient PSC-IBD Non-PSC IBD Severity of active inflammation, mean [0-3]* p-value Extent of active inflammation, mean [0-3]* Activity ratio for all surveillance colonoscopies (active:inactive) No inflammation on ALL surveillance colonoscopies Inflammation extent (1 st colonoscopy) - No activity - Limited - Intermediate - Extensive/pancolitis Inflammation extent (2 nd colonoscopy) - No activity - Limited - Intermediate - Extensive/pancolitis Inflammation extent (3 rd colonoscopy) - No activity - Limited - Intermediate - Extensive/pancolitis Endoscopic inflammation severity (1 st colonoscopy) - No activity - Mild - Moderate - Severe Endoscopic inflammation severity (2 nd colonoscopy) - No activity - Mild - Moderate - Severe Endoscopic inflammation severity (3 rd colonoscopy) - No activity - Mild - Moderate - Severe 45% 41% (27.1%) 546 (34.1%) (53.6%) 7 (3.0%) 38 (16.0%) 65 (27.4%) 125 (55.3%) 9 (4.0%) 40 (17.7%) 52 (23.0%) 102 (57.3%) 6 (3.4%) 22 (12.4%) 48 (27.0%) 160 (57.1%) 100 (35.7%) 19 (6.8%) 1 (0.4%) 125 (53.6%) 89 (38.2%) 16 (6.9%) 3 (1.3%) 864 (57.9%) 89 (6.0%) 363 (24.3%) 176 (11.8%) 866 (61.2%) 109 (7.7%) 297 (21.0%) 141 (10.0%) 584 (63.6%) 79 (8.6%) 164 (17.9%) 92 (9.9%) 924 (57.8%) 495 (30.9%) 131 (8.2%) 50 (3.1%) 864 (59.3%) 445 (30.5%) 101 (6.9%) 48 (3.3%) <0.001 < (55.4%) 63 (34.2%) 13 (7.1%) 6 (3.3%) 583 (61.6%) 276 (29.2%) 64 (6.8%) 23 (2.4%) 0.17
30 Supplementary Table 2: Database characteristics: comparison Netherlands (NL)-United States (US) NL (n=1269) US (n=642) p-value Male (%) 674 (53.1%) 327 (50.9%) 0.37 Age at study inclusion, mean (Standard deviation [SD]) 45 (12) 41 (15) <0.001 Age at IBD diagnosis, mean (SD) 29 (12) 26 (14) <0.001 Primary sclerosing cholangitis (PSC) 171 (13.5%) 122 (19.0%) Age at PSC diagnosis, mean (SD) 33 (12) 32 (16) 0.37 IBD type - Ulcerative colitis - Crohn s colitis - Indeterminate colitis 800 (63.0%) 434 (34.2%) 35 (2.8%) 315 (49.1%) 303 (47.2%) 24 (3.7%) <0.001 Extensive disease / pancolitis 686 (54.1%) 338 (52.6%) 0.56 Medication use - 5-aminosalicylates - Thiopurines - Biologicals Number of surveillance colonoscopies (mean) Interval between surveillance colonoscopies, years (mean) Neoplasia Outcomes: 999 (78.7%) 556 (43.8%) 156 (12.3%) 543 (83.8%) 362 (56.4%) 284 (44.2%) <0.001 < <0.001 Colorectal cancer (CRC) 17 (1.3%) 12 (1.9%) 0.37 High-grade dysplasia (HGD) 15 (1.2%) 20 (3.1%) Low-grade dysplasia (LGD) 264 (20.8%) 88 (13.7%) <0.001
31 Supplementary Table 3: Uni- and multivariate Cox-regression analysis for the overall risk of acrn* (all patients), corrected for study site. Univariate Multivariate Variable HR 95% CI p-value ahr 95% CI p-value PSC Inflammation (severity [0-3])** < <0.001 Sex (reference: male) IBD type (reference: UC) Maximum disease extent (reference: pancolitis) Age at IBD diagnosis Age (years) Thiopurine exposure Biological exposure aminosalicylate exposure Number of surveillance procedures Population (reference: US) < *advanced colorectal neoplasia, acrn: defined as colorectal cancer and/or high-grade dysplasia **entered as time-changing covariate; 0 (no inflammation/remission), 1 (mild), 2 (moderate), 3 (severe)
32 Supplementary Table 4: Uni- and multivariate Cox-regression analysis for the risk of acrn* following detection of low-grade dysplasia (LGD). Univariate Multivariate Variable HR 95% CI p-value ahr 95% CI p-value PSC Sex (reference: male) Thiopurine exposure Biological exposure aminosalicylate exposure Dysplasia characteristics Distal location Multifocality Polypoid morphology Invisible dysplasia Nonpolypoid morphology *advanced colorectal neoplasia, acrn: defined as colorectal cancer and/or high-grade dysplasia
33 Supplementary Figure 1 Kaplan-Meier time-to-event (acrn*) analysis for patients with indeterminate dysplasia (IND); time from first IND within study interval to event. (p=0.02, logrank test). Survival free of HGD/CRC *advanced colorectal neoplasia, acrn: defined as colorectal cancer (CRC) and/or high-grade dysplasia (HGD)
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Patients with longstanding ulcerative colitis (UC) or
 or") ORIGINAL ARTICLE Misclassification of Dysplasia in Patients with Inflammatory Bowel Disease: Consequences for Progression Rates to Advanced Neoplasia Fiona D.M. van Schaik, MD,* Fiebo J.W. ten Kate, MD,
ORIGINAL ARTICLE Misclassification of Dysplasia in Patients with Inflammatory Bowel Disease: Consequences for Progression Rates to Advanced Neoplasia Fiona D.M. van Schaik, MD,* Fiebo J.W. ten Kate, MD,
Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary sclerosing cholangitis and ulcerative colitis
 Journal of Crohn's and Colitis (2013) 7, 974 981 Available online at www.sciencedirect.com ScienceDirect Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary
Journal of Crohn's and Colitis (2013) 7, 974 981 Available online at www.sciencedirect.com ScienceDirect Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
Diagnostic techniques for surveillance of dysplasia
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Comparison of outcomes for patients with primary sclerosing cholangitis associated with ulcerative colitis and Crohn s disease
 Gastroenterology Report, 4(1), 2016, 43 49 doi: 10.1093/gastro/gou074 Advance Access Publication Date: 29 October 2014 Original article ORIGINAL ARTICLE Comparison of outcomes for patients with primary
Gastroenterology Report, 4(1), 2016, 43 49 doi: 10.1093/gastro/gou074 Advance Access Publication Date: 29 October 2014 Original article ORIGINAL ARTICLE Comparison of outcomes for patients with primary
Primary sclerosing cholangitis (PSC) is a chronic, cholestatic
 is a chronic, cholestatic") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:540 546 Progressive Primary Sclerosing Cholangitis Requiring Liver Transplantation Is Associated With Reduced Need for Colectomy in Patients With Ulcerative
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:540 546 Progressive Primary Sclerosing Cholangitis Requiring Liver Transplantation Is Associated With Reduced Need for Colectomy in Patients With Ulcerative
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA
 Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Patients with long-standing, extensive ulcerative colitis (UC) Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine
 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1225 1230 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine THOMAS ULLMAN,* VICTORIA CROOG,* NOAM HARPAZ, SABERA HOSSAIN, ASHER
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1225 1230 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine THOMAS ULLMAN,* VICTORIA CROOG,* NOAM HARPAZ, SABERA HOSSAIN, ASHER
Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K.
 UvA-DARE (Digital Academic Repository) Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K. Link to publication Citation for published version
CRC and Dysplasia in IBD: Objectives of Talk. Colorectal Cancer and Dysplasia in IBD: A Case-Based Approach. Page 1
 Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
P rimary sclerosing cholangitis (PSC) is a chronic cholestatic
 is a chronic cholestatic") 91 INFLAMMATORY BOWEL DISEASE PSC-IBD: a unique form of inflammatory bowel disease associated with primary sclerosing cholangitis E V Loftus Jr, G C Harewood, C G Loftus, W J Tremaine, W S Harmsen, A R
91 INFLAMMATORY BOWEL DISEASE PSC-IBD: a unique form of inflammatory bowel disease associated with primary sclerosing cholangitis E V Loftus Jr, G C Harewood, C G Loftus, W J Tremaine, W S Harmsen, A R
Colorectal Cancer in Inflammatory Bowel Disease
 Gut and Liver, Vol. 2, No. 2, September 2008, pp. 61-73 review Colorectal Cancer in Inflammatory Bowel Disease Jonathan Potack and Steven H. Itzkowitz Division of Gastroenterology, Department of Medicine,
Gut and Liver, Vol. 2, No. 2, September 2008, pp. 61-73 review Colorectal Cancer in Inflammatory Bowel Disease Jonathan Potack and Steven H. Itzkowitz Division of Gastroenterology, Department of Medicine,
IBD high risk groups
 IBD high risk groups Ulcerative colitis Value (95% CI) CRC prevalence (%) 3.7 (3.2-4.2) Overall annual CRC incidence (%) 0.3 (0.2-0.4) Annual CRC incidence in first decade of UC (%) 0.2 (0.1-0.2) Annual
IBD high risk groups Ulcerative colitis Value (95% CI) CRC prevalence (%) 3.7 (3.2-4.2) Overall annual CRC incidence (%) 0.3 (0.2-0.4) Annual CRC incidence in first decade of UC (%) 0.2 (0.1-0.2) Annual
When and How to use Chromoendoscopy in IBD
 When and How to use Chromoendoscopy in IBD Samir A. Shah, MD, FACG, FASGE, AGAF Clinical Professor of Medicine, Brown University Chief of Gastroenterology, The Miriam Hospital Gastroenterology Associates,
When and How to use Chromoendoscopy in IBD Samir A. Shah, MD, FACG, FASGE, AGAF Clinical Professor of Medicine, Brown University Chief of Gastroenterology, The Miriam Hospital Gastroenterology Associates,
Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1015 1021 Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine SIERRA MATULA,* VICTORIA CROOG,* STEVEN ITZKOWITZ,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1015 1021 Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine SIERRA MATULA,* VICTORIA CROOG,* STEVEN ITZKOWITZ,*
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy - Should It Be Standard of Care in IBD?
 Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Increased Risk of Primary Sclerosing Cholangitis and Ulcerative Colitis in First-Degree Relatives of Patients With Primary Sclerosing Cholangitis
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:939 943 Increased Risk of Primary Sclerosing Cholangitis and Ulcerative Colitis in First-Degree Relatives of Patients With Primary Sclerosing Cholangitis
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:939 943 Increased Risk of Primary Sclerosing Cholangitis and Ulcerative Colitis in First-Degree Relatives of Patients With Primary Sclerosing Cholangitis
Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease
 Aliment Pharmacol Ther 23; 18 (Suppl. 2): 1 5. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease P. MUNKHOLM Department of Medical Gastroenterology, Hvidovre
Aliment Pharmacol Ther 23; 18 (Suppl. 2): 1 5. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease P. MUNKHOLM Department of Medical Gastroenterology, Hvidovre
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease
 Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
White Rose Research Online URL for this paper: Version: Accepted Version
 This is a repository copy of Patients with Endoscopically Visible Polypoid Adenomatous Lesions Within the Extent of Ulcerative Colitis Have an Increased Risk of Colorectal Cancer Despite Endoscopic Resection.
This is a repository copy of Patients with Endoscopically Visible Polypoid Adenomatous Lesions Within the Extent of Ulcerative Colitis Have an Increased Risk of Colorectal Cancer Despite Endoscopic Resection.
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
High frequency of early colorectal cancer in inflammatory bowel disease
 See Commentary, p 1194 1 Department of Hepatology, University Medical Center, Utrecht, The Netherlands; 2 Department of Pathology, University Medical Center, Utrecht, The Netherlands; 3 Department of Hepatology,
See Commentary, p 1194 1 Department of Hepatology, University Medical Center, Utrecht, The Netherlands; 2 Department of Pathology, University Medical Center, Utrecht, The Netherlands; 3 Department of Hepatology,
Accepted Manuscript. Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess
 Accepted Manuscript Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess PII: S1542-3565(19)30153-3 DOI: https://doi.org/10.1016/j.cgh.2019.02.013 Reference:
Accepted Manuscript Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess PII: S1542-3565(19)30153-3 DOI: https://doi.org/10.1016/j.cgh.2019.02.013 Reference:
Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
 nature publishing group ORIGINAL CONTRIBUTIONS 1461 CME see related editorial on page 1473 Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
nature publishing group ORIGINAL CONTRIBUTIONS 1461 CME see related editorial on page 1473 Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
Accepted Manuscript. En bloc resection for mm polyps to reduce post-colonoscopy cancer and surveillance. C. Hassan, M. Rutter, A.
 Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:303 308 Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis BARBARA BRADEN,* JOHNNY HALLIDAY,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:303 308 Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis BARBARA BRADEN,* JOHNNY HALLIDAY,*
IBD and Cancer: Myths and Facts
 IBD and Cancer: Myths and Facts Thomas A. Ullman, MD Medical Director, Faculty Prac>ce Department of Medicine Icahn School of Medicine at Mount Sinai New York, USA Risk of Colorectal Cancer in UC Eaden
IBD and Cancer: Myths and Facts Thomas A. Ullman, MD Medical Director, Faculty Prac>ce Department of Medicine Icahn School of Medicine at Mount Sinai New York, USA Risk of Colorectal Cancer in UC Eaden
Quality in Endoscopy: Can We Do Better?
 Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Advances in Ulcerative Colitis - Volume 3 CME
 1 de 12 22/01/2008 04:46 p.m. More: Advances in Ulcerative Colitis Advances in Ulcerative Colitis - Volume 3 CME Complete author affiliations and disclosures are at the end of this activity. Release Date:
1 de 12 22/01/2008 04:46 p.m. More: Advances in Ulcerative Colitis Advances in Ulcerative Colitis - Volume 3 CME Complete author affiliations and disclosures are at the end of this activity. Release Date:
Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients with high risk of colorectal cancer
 ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.264 Intest Res 2016;14(3):264-269 Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients
ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.264 Intest Res 2016;14(3):264-269 Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts
 Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
The variable risk of colorectal cancer in patients with inflammatory bowel disease.
 The variable risk of colorectal cancer in patients with inflammatory bowel disease. Lindgren, Stefan Published in: European Journal of Internal Medicine DOI: 10.1016/j.ejim.2004.12.001 Published: 2005-01-01
The variable risk of colorectal cancer in patients with inflammatory bowel disease. Lindgren, Stefan Published in: European Journal of Internal Medicine DOI: 10.1016/j.ejim.2004.12.001 Published: 2005-01-01
Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines
 INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-8 Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines Vicent Hernández a, Juan Clofent b Complexo Hospitalario
INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-8 Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines Vicent Hernández a, Juan Clofent b Complexo Hospitalario
Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease
 Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease Francis A. Farraye, MD, MSc Clinical Director, Section of Gastroenterology, Boston Medical Center Professor of Medicine,
Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease Francis A. Farraye, MD, MSc Clinical Director, Section of Gastroenterology, Boston Medical Center Professor of Medicine,
Inflammatory bowel disease (IBD), which includes ulcerative
, which includes ulcerative") Chromoendoscopy and Dysplasia Surveillance in Inflammatory Bowel Disease: Past, Present, and Future Steven Naymagon, MD, and Thomas A. Ullman, MD Dr Naymagon is an assistant professor of medicine and Dr
Chromoendoscopy and Dysplasia Surveillance in Inflammatory Bowel Disease: Past, Present, and Future Steven Naymagon, MD, and Thomas A. Ullman, MD Dr Naymagon is an assistant professor of medicine and Dr
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
Cost-effectiveness of adenoma surveillance - the Dutch guidelines -
 Cost-effectiveness of adenoma surveillance - the Dutch guidelines - WEO working group adenoma surveillance 20 May, 2016 Iris Lansdorp-Vogelaar, PhD On behalf of the SAP study-group Introduction Adenoma
Cost-effectiveness of adenoma surveillance - the Dutch guidelines - WEO working group adenoma surveillance 20 May, 2016 Iris Lansdorp-Vogelaar, PhD On behalf of the SAP study-group Introduction Adenoma
Adherence to surveillance guidelines for dysplasia and colorectal carcinoma in ulcerative and Crohn s colitis patients in the Netherlands
 Online Submissions: wjg.wjgnet.com World J Gastroenterol 9 January 14; 15(2): 226-23 wjg@wjgnet.com World Journal of Gastroenterology ISSN 17-9327 doi:1.3748/wjg.15.226 9 The WJG Press and Baishideng.
Online Submissions: wjg.wjgnet.com World J Gastroenterol 9 January 14; 15(2): 226-23 wjg@wjgnet.com World Journal of Gastroenterology ISSN 17-9327 doi:1.3748/wjg.15.226 9 The WJG Press and Baishideng.
Chromoendoscopy as an Adjunct to Colonoscopy
 Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps
 Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps Full guideline Draft for consultation, May 00 0 This guideline
Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps Full guideline Draft for consultation, May 00 0 This guideline
PATIENTS WITH LONG-STANDING inflammatory
 Digestive Endoscopy 2016; 28: 266 273 doi: 10.1111/den.12634 Review Paradigm Shift in the Surveillance and Management of Dysplasia in Inflammatory Bowel Disease (West) Roy Soetikno, 1 Tonya Kaltenbach,
Digestive Endoscopy 2016; 28: 266 273 doi: 10.1111/den.12634 Review Paradigm Shift in the Surveillance and Management of Dysplasia in Inflammatory Bowel Disease (West) Roy Soetikno, 1 Tonya Kaltenbach,
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Novel Optical Research at UPMC
 Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Malignancy in ulcerative colitis (UC) is believed to ORIGINAL ARTICLES
 is believed to ORIGINAL ARTICLES") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:534 541 ORIGINAL ARTICLES Long-term Follow-up After Polypectomy Treatment for Adenoma-Like Dysplastic Lesions in Ulcerative Colitis ROBERT D. ODZE,* FRANCIS
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:534 541 ORIGINAL ARTICLES Long-term Follow-up After Polypectomy Treatment for Adenoma-Like Dysplastic Lesions in Ulcerative Colitis ROBERT D. ODZE,* FRANCIS
Primary Sclerosing Cholangitis with Inflammatory Bowel Disease in Korean Children
 pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2015.18.4.268 Pediatr Gastroenterol Hepatol Nutr 2015 December 18(4):268-275 Original Article PGHN Primary Sclerosing Cholangitis with Inflammatory
pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2015.18.4.268 Pediatr Gastroenterol Hepatol Nutr 2015 December 18(4):268-275 Original Article PGHN Primary Sclerosing Cholangitis with Inflammatory
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Patients with inflammatory bowel disease (IBD) carry a higher
 carry a higher") Advances in the Diagnosis and Management of Colonic Dysplasia in Patients With Inflammatory Bowel Disease Shirley Cohen-Mekelburg, MD, Yecheskel Schneider, MD, Stephanie Gold, MD, Ellen Scherl, MD, and
Advances in the Diagnosis and Management of Colonic Dysplasia in Patients With Inflammatory Bowel Disease Shirley Cohen-Mekelburg, MD, Yecheskel Schneider, MD, Stephanie Gold, MD, Ellen Scherl, MD, and
Microbiome, Inflammation and Cancer
 Microbiome, Inflammation and Cancer Anita Afzali MD, MPH, FACG Medical Director, OSU Inflammatory Bowel Disease Center Abercrombie & Fitch Endowed Chair in Inflammatory Bowel Disease 4 th Annual Cancer
Microbiome, Inflammation and Cancer Anita Afzali MD, MPH, FACG Medical Director, OSU Inflammatory Bowel Disease Center Abercrombie & Fitch Endowed Chair in Inflammatory Bowel Disease 4 th Annual Cancer
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
CANCER SCREENING IN IBD David T. Rubin, MD, FACG
 1C: Advances in Inflammatory Bowel Disease CANCER SCREENING IN IBD David T. Rubin, MD, FACG Risk Factors for Neoplasia in Chronic Colitis An increasing amount of evidence has provided a link between chronically
1C: Advances in Inflammatory Bowel Disease CANCER SCREENING IN IBD David T. Rubin, MD, FACG Risk Factors for Neoplasia in Chronic Colitis An increasing amount of evidence has provided a link between chronically
RE: Title: Practical fecal calprotectin cut-off value for Japanese patients with ulcerative colitis
 September 10, 2018 Professor Xue-Jiao Wang, MD Science Editor Editorial Office 'World Journal of Gastroenterology' RE: 40814 Title: Practical fecal calprotectin cut-off value for Japanese patients with
September 10, 2018 Professor Xue-Jiao Wang, MD Science Editor Editorial Office 'World Journal of Gastroenterology' RE: 40814 Title: Practical fecal calprotectin cut-off value for Japanese patients with
The pathology of IBD and its modification by liver disease. Roger Feakins ESP/H-ECCO
 The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
The pathology of IBD and its modification by liver disease Roger Feakins ESP/H-ECCO Enterprise Interest None IBD UC [IBDU] Crohn s IBD: distribution of disease Ulcerative colitis continuous Crohn s colitis
Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R.
 UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K.
 UvA-DARE (Digital Academic Repository) Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Primary sclerosing cholangitis and primary biliary cirrhosis: epidemiology, risk factors, and outcome Boonstra, K. Link to publication Citation for published version
There is a well-established association between inflammatory
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1346 1350 Aminosalicylate Therapy in the Prevention of Dysplasia and Colorectal Cancer in Ulcerative Colitis DAVID T. RUBIN, ANDELKA LOSAVIO, NICOLE YADRON,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2006;4:1346 1350 Aminosalicylate Therapy in the Prevention of Dysplasia and Colorectal Cancer in Ulcerative Colitis DAVID T. RUBIN, ANDELKA LOSAVIO, NICOLE YADRON,
POST TRANSPLANT OUTCOMES IN PSC
 POST TRANSPLANT OUTCOMES IN PSC Kidist K. Yimam, MD Medical Director, Autoimmune Liver Disease Program Division of Hepatology and Liver Transplantation California Pacific Medical Center (CPMC) PSC Partners
POST TRANSPLANT OUTCOMES IN PSC Kidist K. Yimam, MD Medical Director, Autoimmune Liver Disease Program Division of Hepatology and Liver Transplantation California Pacific Medical Center (CPMC) PSC Partners
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Accepted Manuscript. Improving Outcomes in Patients with Inflammatory Bowel Disease through Integrated Multi-Disciplinary Care the Future of IBD Care
 Accepted Manuscript Improving Outcomes in Patients with Inflammatory Bowel Disease through Integrated Multi-Disciplinary Care the Future of IBD Care Kaci Christian, MD, Raymond K. Cross, MD, MS PII: S1542-3565(18)30746-8
Accepted Manuscript Improving Outcomes in Patients with Inflammatory Bowel Disease through Integrated Multi-Disciplinary Care the Future of IBD Care Kaci Christian, MD, Raymond K. Cross, MD, MS PII: S1542-3565(18)30746-8
AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
Childhood onset inflammatory bowel disease and risk of cancer: a Swedish nationwide cohort study
 Childhood onset inflammatory bowel disease and risk of cancer: a Swedish nationwide cohort study 6- O Olén,,, J Askling, MC Sachs, P Frumento, M Neovius, KE Smedby, A Ekbom, P Malmborg,,5 JF Ludvigsson
Childhood onset inflammatory bowel disease and risk of cancer: a Swedish nationwide cohort study 6- O Olén,,, J Askling, MC Sachs, P Frumento, M Neovius, KE Smedby, A Ekbom, P Malmborg,,5 JF Ludvigsson
Masato Kusunoki Editor. Colitis-Associated Cancer
 Masato Kusunoki Editor Colitis-Associated Cancer 123 Colitis-Associated Cancer ThiS is a FM Blank Page Masato Kusunoki Editor Colitis-Associated Cancer Editor Masato Kusunoki Mie University Graduate School
Masato Kusunoki Editor Colitis-Associated Cancer 123 Colitis-Associated Cancer ThiS is a FM Blank Page Masato Kusunoki Editor Colitis-Associated Cancer Editor Masato Kusunoki Mie University Graduate School
Accepted Manuscript. Correlation or Causation: Sex Hormones and Microscopic Colitis. Baldeep Pabla, Reid M. Ness
 Accepted Manuscript Correlation or Causation: Sex Hormones and Microscopic Colitis Baldeep Pabla, Reid M. Ness PII: S0016-5085(18)35216-8 DOI: https://doi.org/10.1053/j.gastro.2018.11.007 Reference: YGAST
Accepted Manuscript Correlation or Causation: Sex Hormones and Microscopic Colitis Baldeep Pabla, Reid M. Ness PII: S0016-5085(18)35216-8 DOI: https://doi.org/10.1053/j.gastro.2018.11.007 Reference: YGAST
MINI-REVIEW. Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer. Lin-Lin Ren, Jing-Yuan Fang * Abstract.
 Should we Sound the Alarm?- Dysplasia and Colitis-associated Colorectal Cancer MINI-REVIEW Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer Lin-Lin Ren, Jing-Yuan Fang * Abstract
Should we Sound the Alarm?- Dysplasia and Colitis-associated Colorectal Cancer MINI-REVIEW Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer Lin-Lin Ren, Jing-Yuan Fang * Abstract
Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
 1022 ORIGINAL CONTRIBUTIONS nature publishing group see related editorial on page 1035 Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
1022 ORIGINAL CONTRIBUTIONS nature publishing group see related editorial on page 1035 Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews
 Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews DR. NILESH CHANDE COORDINATING EDITOR, IBD REVIEW GROUP; UNIVERSITY OF WESTERN ONTARIO, LONDON, ON CANADA An international organisation
Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews DR. NILESH CHANDE COORDINATING EDITOR, IBD REVIEW GROUP; UNIVERSITY OF WESTERN ONTARIO, LONDON, ON CANADA An international organisation
Objec-ve. Case Presenta-ons and Ques-ons to Panel. Dysplasia case 11/13/11
 Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Recurrence and survival rates of inflammatory bowel disease-associated colorectal cancer following postoperative chemotherapy: a comparative study
 Gastroenterology Report, 5(1), 2017, 57 61 doi: 10.1093/gastro/gow016 Advance Access Publication Date: 8 June 2016 Original article ORIGINAL ARTICLE Recurrence and survival rates of inflammatory bowel
Gastroenterology Report, 5(1), 2017, 57 61 doi: 10.1093/gastro/gow016 Advance Access Publication Date: 8 June 2016 Original article ORIGINAL ARTICLE Recurrence and survival rates of inflammatory bowel
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients
 Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients Tamás Molnár 1, Klaudia Farkas 1, Tibor Nyári 2, Zoltán Szepes 1, Ferenc Nagy 1,
Response to First Intravenous Steroid Therapy Determines the Subsequent Risk of Colectomy in Ulcerative Colitis Patients Tamás Molnár 1, Klaudia Farkas 1, Tibor Nyári 2, Zoltán Szepes 1, Ferenc Nagy 1,
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Inflammatory Bowel Disease and Primary Sclerosing Cholangitis: A Review of the Phenotype and Associated Specific Features
 Gut and Liver, Vol. 12, No. 1, January 2018, pp. 17-29 Review Inflammatory Bowel Disease and Primary Sclerosing Cholangitis: A Review of the Phenotype and Associated Specific Features Carolina Palmela
Gut and Liver, Vol. 12, No. 1, January 2018, pp. 17-29 Review Inflammatory Bowel Disease and Primary Sclerosing Cholangitis: A Review of the Phenotype and Associated Specific Features Carolina Palmela
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Title: Crohn s disease and cystic fibrosis: there is still a lot to learn
 Title: Crohn s disease and cystic fibrosis: there is still a lot to learn Authors: Claudio Trigo Salado, Eduardo Leo Carnerero, María Dolores de la Cruz Ramírez DOI: 10.17235/reed.2018.5725/2018 Link:
Title: Crohn s disease and cystic fibrosis: there is still a lot to learn Authors: Claudio Trigo Salado, Eduardo Leo Carnerero, María Dolores de la Cruz Ramírez DOI: 10.17235/reed.2018.5725/2018 Link:
HLA TYPING AND EXPRESSION: POTENTIAL MARKER FOR IDENTIFYING EARLY DYSPLASIA AND STRATIFYING THE RISK FOR IBD-CANCER
 HLA TYPING AND EXPRESSION: POTENTIAL MARKER FOR IDENTIFYING EARLY DYSPLASIA AND STRATIFYING THE RISK FOR IBD-CANCER Megan Garrity, S. Breanndan Moore, M.D., William Sandborn, M.D., Vernon Pankratz, Ph.D.,
HLA TYPING AND EXPRESSION: POTENTIAL MARKER FOR IDENTIFYING EARLY DYSPLASIA AND STRATIFYING THE RISK FOR IBD-CANCER Megan Garrity, S. Breanndan Moore, M.D., William Sandborn, M.D., Vernon Pankratz, Ph.D.,
DIVISION OF GASTROENTEROLOGY
 DR. Lloyd Mayer T H E H E N R Y D. J A N O W I T Z DIVISION OF GASTROENTEROLOGY Mount Sinai is consistently ranked among the top five gastroenterology centers in the nation. The irresistible combination
DR. Lloyd Mayer T H E H E N R Y D. J A N O W I T Z DIVISION OF GASTROENTEROLOGY Mount Sinai is consistently ranked among the top five gastroenterology centers in the nation. The irresistible combination
Colorectal cancer surveillance in inflammatory bowel diseases
 Turkish Journal of Cancer Volume 34, No.2, 2004 55 Colorectal cancer surveillance in inflammatory bowel diseases MURAT TÖRÜNER Ankara University Medical School, Department of Gastroenterology, Ankara-Turkey
Turkish Journal of Cancer Volume 34, No.2, 2004 55 Colorectal cancer surveillance in inflammatory bowel diseases MURAT TÖRÜNER Ankara University Medical School, Department of Gastroenterology, Ankara-Turkey
As clinicians we would all agree that the goal for our
 CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
CURRENT CONTROVERSIES: PRO, CON, AND BALANCE Controversies in Mucosal Healing in Ulcerative Colitis Sunanda Kane, MD,* Frances Lu, MD, Asher Kornbluth, MD, Dahlia Awais, MD, and Peter D.R. Higgins, MD,
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
C olorectal cancer (CRC) is one of the most feared
 is one of the most feared") 1573 INFLAMMATORY BOWEL DISEASE 5-Aminosalicylate use and colorectal cancer risk in inflammatory bowel disease: a large epidemiological study T P van Staa, T Card, R F Logan, H G M Leufkens... See end
1573 INFLAMMATORY BOWEL DISEASE 5-Aminosalicylate use and colorectal cancer risk in inflammatory bowel disease: a large epidemiological study T P van Staa, T Card, R F Logan, H G M Leufkens... See end
Screening for Colorectal Cancer in the Elderly. The Broad Perspective
 Screening for Colorectal Cancer in the Elderly Charles J. Kahi, MD, MSCR Indiana University School of Medicine Richard L. Roudebush VA Medical Center Indianapolis, Indiana ACG Regional Midwest Course Symposium
Screening for Colorectal Cancer in the Elderly Charles J. Kahi, MD, MSCR Indiana University School of Medicine Richard L. Roudebush VA Medical Center Indianapolis, Indiana ACG Regional Midwest Course Symposium
NIH Public Access Author Manuscript Inflamm Bowel Dis. Author manuscript; available in PMC 2013 December 01.
 NIH Public Access Author Manuscript Published in final edited form as: Inflamm Bowel Dis. 2012 December ; 18(12): 2240 2246. doi:10.1002/ibd.22912. Prospective Study of the Progression of Low-Grade Dysplasia
NIH Public Access Author Manuscript Published in final edited form as: Inflamm Bowel Dis. 2012 December ; 18(12): 2240 2246. doi:10.1002/ibd.22912. Prospective Study of the Progression of Low-Grade Dysplasia
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
available at
 Journal of Crohn's and Colitis (2010) 4, 661 668 available at www.sciencedirect.com A short course of corticosteroids prior to surveillance colonoscopy to decrease mucosal inflammation in inflammatory
Journal of Crohn's and Colitis (2010) 4, 661 668 available at www.sciencedirect.com A short course of corticosteroids prior to surveillance colonoscopy to decrease mucosal inflammation in inflammatory
 associated with severe symptoms and impaired quality of life. UC may affect all ages and medical treatment depends on disease severity and extent. In the case of intractable disease, colectomy may be indicated.
associated with severe symptoms and impaired quality of life. UC may affect all ages and medical treatment depends on disease severity and extent. In the case of intractable disease, colectomy may be indicated.
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
Inflammatory Bowel Disease: Clinical updates. Dr Jeff Chao Princess Alexandra Hospital
 Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
Inflammatory Bowel Disease: Clinical updates Dr Jeff Chao Princess Alexandra Hospital Inflammatory bowel disease 2017 Clinical updates and future directions Pathogenesis Treatment targets Therapeutic agents
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two