When and How to use Chromoendoscopy in IBD
|
|
|
- Clemence Andrews
- 5 years ago
- Views:
Transcription

1 When and How to use Chromoendoscopy in IBD Samir A. Shah, MD, FACG, FASGE, AGAF Clinical Professor of Medicine, Brown University Chief of Gastroenterology, The Miriam Hospital Gastroenterology Associates, Inc 44 West River Street, Providence RI
2 Patients Concerns About Ulcerative Colitis Primary concerns Patients (%) Developing cancer 23 Uncertainty of disease progression 22 Losing bowel control 18 Energy level 12 Ostomy bag 8 Using steroids 7 Medication effects 5 Surgery 4 Other 1 Loftus EV. Inflamm Bowel Dis 2006;12:
3 Learning Objectives Understand the increased risk of CRC in IBD Specific risk factors Risk stratify for surveillance Recognize limitations of conventional colonoscopy and random biopsy Describe the indications for the usage of chromoendoscopy to detect dysplasia in patients with IBD Shah, Rubin, Farraye. Curr Gastroenterol Rep (2014) 16:407 Soetikno, R et al. Gastroenterology. 2013;144: Kiesslich&Neurath. Chromoendoscopy in inflammatory bowel disease. Gastroenterology Clinics of North America 41.2 (2012): Laine L, Kaltenbach T, Barkun A, et al. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology 2015;148: Shergill A, et al. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc May;81(5):
4 Take home points Increased risk of colon cancer in IBD But, not as high as we used to think Risk stratification Polyps in IBD patients: treat like non-ibd Nomenclature: Paris classification, Border, ulcer Chromoendoscopy Yes: increases yield May decrease incidence/mortality of CRC ASGE Guidelines, SCENIC Consensus Confirmed dysplasia = colectomy HGD, endoscopically unresectable dysplasia LGD* controversial
5 Cumulative Risk (%) NESGNA Risk of CRC in IBD is Less Than Previously Reported: Evidence of Successful Prevention? 48 studies included in the metaanalysis Included both population-based (259,266 person-years at risk) and referral center studies (29,799 patient-years at risk) Cumulative risk in IBD patients Overall Population based Referral center Overall cumulative risk at 10, 20 and >20 years is 1%, 3% and 7% 30 Rate higher in referral centers and in patients with extensive disease 20 Risk is still almost 2x higher in Crohn s and ulcerative colitis compared with general population years 20 years >20 years Lutgens MW, et al. Inflamm Bowel Dis. 2013;19:
6 Cumulative Incidence of Colorectal Cancer (%) Cumulative Incidence of Colorectal Cancer (%) NESGNA Cumulative Risk of CRC Among IBD Patients From Olmsted County, Minnesota, CRC in patients with UC (n=378) comparison with expected incidence from SEER data, Iowa whites, (P=0.55, log rank) year cancer risk: 2.0% (vs. 2.3% expected based on Iowa SEER rates) (P=0.55, log-rank test). Observed Expected CRC in patients with CD (n=314) comparison with expected incidence from SEER data, Iowa whites, (P=0.66, log rank) year cancer risk: 2.4% (vs. 1.6% expected based on Iowa SEER rates) (P=0.66, log-rank test). Observed Expected Years from Diagnosis Years from Diagnosis No. at risk cancers diagnosed within 30 days of IBD diagnosis excluded. No. at risk cancers diagnosed within 30 days of IBD diagnosis excluded. Jess T, et al. Gastroenterology. 2006;130:
7 Cancer Risk Factors in IBD Extensive disease No increase in proctitis patients, intermediate risk in left sided UC and highest risk in in pancolitis Disease duration/age at diagnosis Family history of colorectal cancer Highest risk if FDR with CRC < 50 Primary sclerosing cholangitis Histologic Disease activity Previous dysplasia Pseudopolyps, strictures, forshortened colon Probable risk factors Poor compliance with medical therapy Male Sex Lewis et al. Gastroenterol Clin N Am 1999;28:459 Askling J, et al. Gastroenterology Rutter, et al. Gastroenterology, 2004 Farraye FA, Odze R, et al Gastroenterology 2010; 138: Jess T, et al. Risk of colorectal cancer in patients with ulcerative colitis: a meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2012;10:
8 1. Rutter MD, et al. Gastroenterology. 2004;126: Rutter MD, et al. Gut. 2004;53: Gupta RB, et al. Gastroenterology. 2007;133: Rubin DT, et al. Clin Gastroenterol Hepatol. 2013;11: NESGNA Potential Relationship Between Chronic Inflammation and Risk of Colorectal Cancer in IBD 2004 analysis: the only risk factor for developing CRC in patients with long-standing, extensive UC was an increased histologic inflammation score (OR 4.69, 95% CI , P<0.001) 1 With macroscopically normal mucosa, 5-year cancer risk returned to level of general population 1, study: prolonged histologic inflammation was a risk factor for progression to advanced neoplasia in patients with long-standing UC 3 Every unit increase in cumulative mean histologic inflammation score 3-fold increase in risk of advanced neoplasia case-control study: >3-fold increase in neoplasia with each 1- unit increase in histologic inflammatory activity score; risk increased to 7-fold with higher degrees of inflammation 4
9 Cancer Surveillance in Colitis Inflammation Dysplasia Cancer Death Initiate screening and surveillance Intervention to prevent further progression: surgery
10 Is Surveillance Effective? Choi 1993: Patients who underwent surveillance presented with a significantly earlier stage of cancer 5 year survival higher in surveillance group Karlen 1998: Relative CRC risk decline with increasing number of colonoscopies Eaden 2000: OR for CRC decreased with increasing number of colonoscopies Velayos 2006: OR for CRC decreased with increasing number of colonoscopies 1. Choi PM, et al. Gut. 1994; 35: Karlen P, et al. Gastroenterology. 1998;115: Eaden JA, et al. Aliment Pharmacol Ther. 2000;14: Velayos FS, et al. Gastroenterology. 2006;130:
11 Surveillance Colonoscopy in IBD Retrospective study of 6823 patients with IBD (2764 with a recent colonoscopy, 4059 without a recent colonoscopy) seen and followed for at least 3 years at 2 tertiary referral hospitals (MGH & BWH) in Boston, Massachusetts The incidence of CRC among patients with and without a recent colonoscopy were 1.6% and 2.7% respectively (OR, 0.56; 95%, CI ) Among patients with CRC, a colonoscopy within 6 to 36 months before diagnosis was associated with a reduced mortality rate (OR, 0.34; 95% CI ) Conclusion: A recent colonoscopy (within 36 months) is associated with a reduced incidence of CRC in patients with IBD, and lower mortality rates in those diagnosed with CRC Ananthakrishnan AN, et al. Colonoscopy is associated with a reduced risk for colon cancer and mortality in patients with inflammatory bowel diseases. Clin Gastroenterol Hepatol Feb;13(2):
12 Increased Risk of CRC in IBD Study of 55,008 Medicare patients, 15% of IBD patients with a diagnosis of CRC ( ) had undergone surveillance colonoscopy in the previous 3 years Compared with non-ibd patients, IBD patients were 3 times more likely (15.5% vs. 5.8%) to have had a colonoscopy within 6 to 36 months before the CRC diagnosis (CD: OR, 3.07; 95% CI, ; UC: OR, 3.05; 95% CI, ) 62.5% of CD and 38.5% of UC patients with interval CRC had advanced (stage III or IV) CRC at diagnosis Conclusions: dysplasia may be often missed or unrecognized with standard (old) colonoscopic surveillance techniques Wang YR, Cangemi JR, Loftus EV, Picco MF. Use of surveillance colonoscopy in medicare patients with inflammatory bowel disease prior to colorectal cancer diagnosis. Digestion. 2014;90(1):58-62.
13 Biopsy Recommendations for Cancer Screening in IBD 90% Confidence 95% Confidence Dysplasia Cancer Dysplasia or Cancer For patients with extensive disease, a minimum of 33 biopsies are recommended 2 4-quadrant biopsies every 10 cm throughout the colon Studies done pre HD scopes Evidence suggests that recommendations are frequently not observed 3 1. Rubin CE, et al. Gastroenterology. 1992;103: Itzkowitz SH, et al. Inflamm Bowel Dis. 2005;11: Itzkowitz SH, et al. Gastroenterology. 2004;126:
14 <0.1% Surface Area Colon Surface Area Random Biopsied SA 100% 2000cm 2 colon SA vs 1.32cm 2 random SA 33 random biopsies sample <0.1% of the bowel
 10% of dysplasia RB, 90% targeted van den Broek Am J Gastroenterol 2011 Rutter MD. J Gastroenterol. 2011;46 SCENIC Gastroenterology 2015;148:639 651.")
15 466 surveillance colonoscopies (167 pt) 11,772 biopsies 1 LGD = positive on random biopsies (all others were targeted biopsies) Rutter: 1/1266 random bx SCENIC: 39/48,522 (0.08%) 10% of dysplasia RB, 90% targeted van den Broek Am J Gastroenterol 2011 Rutter MD. J Gastroenterol. 2011;46 SCENIC Gastroenterology 2015;148:
16 Colectomy for Dysplasia in UC Low grade dysplasia 20% cancer High grade dysplasia 42% cancer DALM 43% cancer The finding of dysplasia of any grade should be confirmed by a pathologist with special expertise in gastrointestinal pathology Confirmed dysplasia = colectomy Bernstein et al, Lancet 1994;334:71
17 Progression Probability NESGNA Progression of Neoplasia in UC: Chicago 35 patients in analysis 2 with IND and 2 with LGD developed HGD or CRC over mean duration of 49.8 months Incident rate for advanced neoplasia for all patients was 2.7 cases of HGD or CRC per 100 person-years at risk Conclusion : a low rate of progression to HGD or CRC in patients with LGD or IND under surveillance Polypoid dysplasia showed less risk of progression than flat dysplasia Years from Index Date Kaplan-Meier curve of progression to high-grade dysplasia or colorectal cancer in patients with low grade or indefinite dysplasia. IND=indefinite dysplasia Pekow JR, et al. Inflamm Bowel Dis. 2010;16:
18 Fate of Dysplasia at Colectomy Ullman, 2003 Gastroenterology Dysplasia found with random bx Low definition, White light Colectomy performed 7/46 (15%) had synchronous CRC 53% of the flat LGD by random bx HGD or CRC over 5 years Specificity: = 68% Marion, 2016 CGH Dysplasia found with High definition WL & Chromo Colectomy performed 0/10 (0%) had synchronous CRC Unknown if any of the LGD detected by Chromo would progress to HGD or CRC Specificity 0% so far Dysplasia found by Chromoendoscopy is not the same as dysplasia found in earlier times by random biopsy and low definition. Chromo: Greater sensitivity for lower speficiity Ullman T, et al. Gastroenterology 2003; 125: Marion JF, et al. CGH 2016;14:
19 The Case for Chromoendoscopy

20 Chromoendoscopy in Inflammatory Bowel Disease Ralf Kiesslich, Markus F. Neurath, MD Author Year Country Dye Staining Endoscopy Design No. of pts. Pts. with dysplasia Outcome chromo vs. standard Kiesslich et al Germany MB Pancolonic Magnification Randomized 1: vs. 10 dysplastic lesions Matsumoto et al. Rutter et al Japan IC Pancolonic WLE Prospective cohort 2004 UK IC Pancolonic WLE Prospective cohort % vs. 38% sensitivity vs. 2 dysplastic lesions Hurlstone et al. Kiesslich et al UK IC Targeted Magnification Prospective cohort 2007 Germany MB Pancolonic CLE Randomized 1: vs. 24 dysplastic lesions vs. 4 dysplastic lesions Marion et al. Günther et al. Hlavaty et al US MB Pancolonic WLE Tandem colonoscopy 2011 Germany IC Pancolonic CE Randomized 1:1: Slovakia IC Pancolonic CE Tandem colonoscopy vs. 3 patients with dysplastic lesions (2+ CEM4) vs. 0 patients with dysplastic lesions vs. 2 dysplastic lesions Evaluating Inflammatory Bowel Disease, GCNA, June 2012, Editors: Shah, Harris, Feller
21 Chromoendoscopy: Which Dye? Indigo carmine (0.03%-0.4%) Contrast stain neither reacts or is absorbed by the colonic mucosa Pools in mucosal grooves allowing better definition of small or flat lesions as well as alterations in mucosal architecture Can be washed off the mucosa Methylene blue ( %) Vital dye taken up by colonic mucosa within 1-2 minutes staining noninflamed mucosa but is poorly taken up by dysplastic tissue or inflamed mucosa No published studies comparing indigo carmine to methylene blue in patients with IBD. Other dyes: FD&C#2 Blue Farraye FA, Schroy P. Chromoendoscopy: A new vision for colonoscopic surveillance in IBD. Gastroenterology 2006;131:
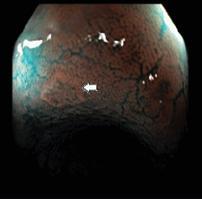
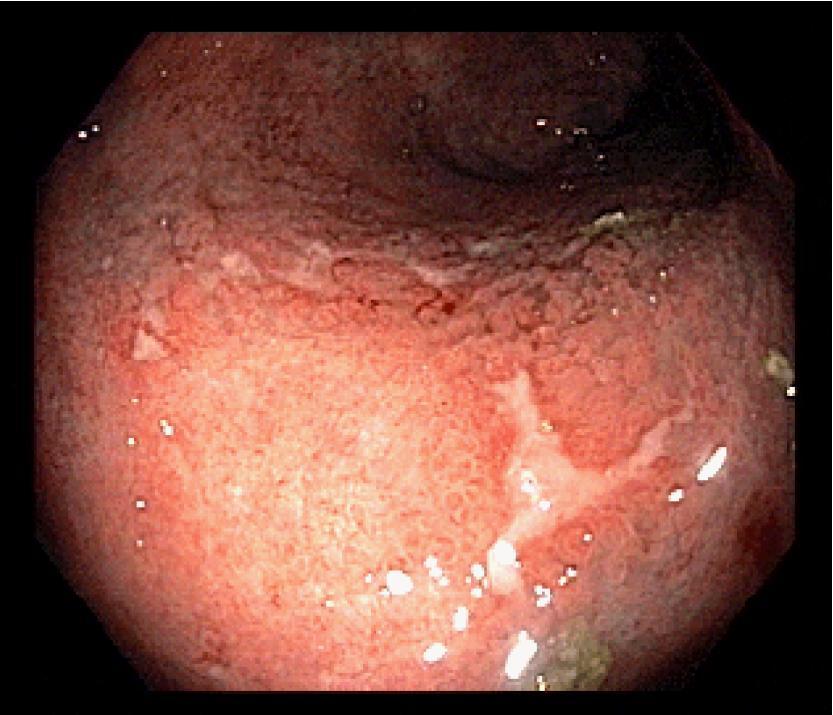
 Examples of type I (left) and type IV (right) lesions before and after chromoendoscopy. Kiesslich, R et al.")
22 Pit Pattern Classification (Kudo) The typical crypt architecture of types I-V are indicated (A). (B) Examples of type I (left) and type IV (right) lesions before and after chromoendoscopy. Kiesslich, R et al. Gut 2004;53:
23 Chromoendoscopy Videos
24 Chromoendoscopy: pseudopolyps

25 Adenoma found in a sea of pseudopolyps
26 Chromo with IC using flushing device
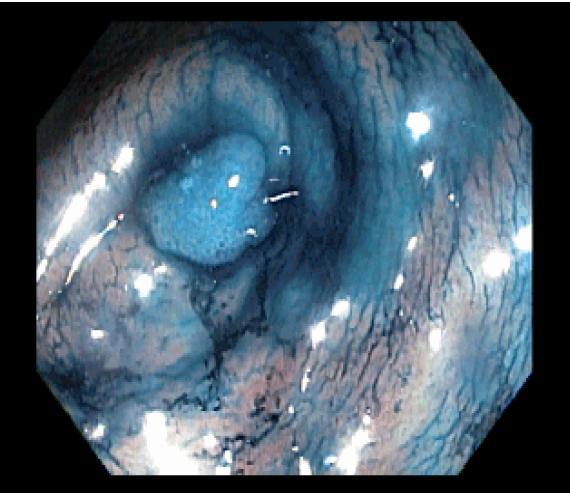
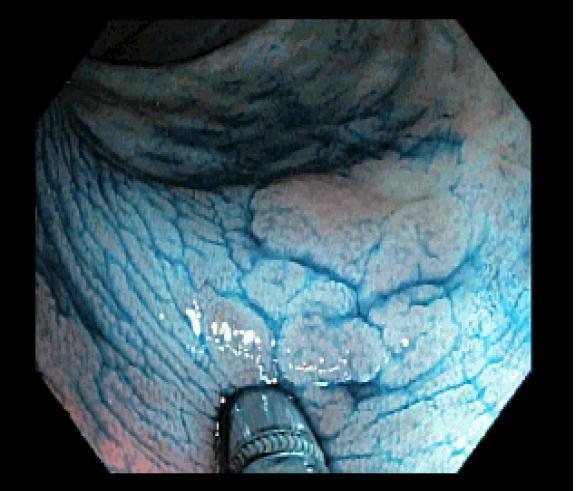
27 Chromoendoscopy: pt with longstanding Crohn s colitis

28

29
30
31 Can one do chromoendoscopy in a busy clinical practice? Time: not an issue (Flusher, targeted biopsies. But schedule for 1 hour) Training (15-20 cases); online resources Technique: Flusher vs spray catheter Does it work in a private practice: yes! 2005: started: recorded on op note whether lesion seen with chromo or not Selection bias in patients chosen for Chromo
32 Chromoendoscopy in practice Single physician experience / scopes; 118pts, mean age 51.4 years Chromo - IC (64 scopes) WLE (120 scopes) 38.8 minutes 20.5 minutes 42.0 bx (13 jars) 34.8 bx (10 jars) 157 polyps (2.45/scope) 87 polyps (0.725/scope) 25/64 (39.1%) dys polyps 8/120 (6.9%) dys polyps (p<0.001) *flat dysplasia on one random biopsy: doing well, no colectomy, annual colonoscopy with chromo since Jatsukar N, Reinert S, Resnick M, Shah SA. IBD Advances, 2012 Shah, Rubin, Farraye. Curr Gastroenterol Rep (2014) 16:407
33 Is it recommended? BSG, ECCO, ESGE, CAG, APAG, JGES: endorse Chromo as preferred! CCFA/ASGE/AGA: endorse chromoendoscopy SCENIC CONSENSUS STATEMENT ACG: not enough data to endorse Ok to do if have expertise, HD scope with random biopsies ok too Though increase in yield of dysplastic lesions, does this translate to less cancer (DoDo Bird analogy- Dr Peter Higgins). Need to show decrease in CRC/mortality


34 Two non-profit charitable foundations (Maxine and Jack Zarrow Family Foundation and the William Warren Foundation), provided unrestricted gifts supporting the guideline development process
35 SCENIC Nomenclature Dysplasia is either visible or invisible Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology 2015;148:

36 SCENIC Nomenclature Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:
37 SCENIC Nomenclature It is recommended that the terms dysplasia-associated lesion or mass (DALM) and adenoma-like or non-adenoma-like DALM be abandoned Use the preferred term endoscopically resectable which indicates that: distinct margins of the lesion could be identified the lesion appears to be completely removed on visual inspection after endoscopic resection histologic examination of the resected specimen is consistent with complete removal biopsy specimens taken from mucosa immediately adjacent to the resection site are free of dysplasia on histologic examination All other lesions are endoscopically unresectable Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:
38 Shergill A, et al. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc May;81(5):
39 ASGE Guidelines All patients with UC or Crohn s colitis are recommended to undergo a screening colonoscopy 8 years after disease onset to (1) re-evaluate extent of disease and (2) initiate surveillance for colorectal neoplasia (Grade: Moderate) Surveillance colonoscopy is recommended every 1 to 3 years beginning after 8 years of disease in patients with UC with macroscopic or histologic evidence of inflammation proximal to and including the sigmoid colon and for patients with Crohn s colitis with greater than one-third of colon involvement (Grade: Moderate) Shergill A, et al. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc May;81(5):
40 ASGE: How to Perform Surveillance Chromoendoscopy with targeted biopsies is recommended as the preferred surveillance technique to maximize dysplasia detection (Grade: Moderate) Chromoendoscopy-targeted biopsies are sufficient for dysplasia surveillance in patients with IBD and that consideration should be given to taking two biopsies from each colon segment for histologic staging to assess extent and severity of inflammation (Grade: Low) Random biopsies with targeted biopsies of any suspicious appearing lesions remain a reasonable alternative for dysplasia surveillance if the yield of chromoendoscopy is reduced by significant underlying inflammation, significant pseudopolyposis, or poor preparation or if chromoendoscopy is not available (Grade: Low) Shergill A, et al. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc May;81(5):
41 ASGE: After Polypectomy Patients with IBD whose polypoid dysplastic lesions have been removed completely receive endoscopic surveillance at 1 to 6 months and at 12 months, with yearly surveillance thereafter (Grade: Moderate) Patients with IBD whose non-polypoid dysplastic lesions have been removed completely receive endoscopic surveillance at 1 to 6 months and at 12 months, with yearly surveillance thereafter (Grade: Low) Proctocolectomy in patients with IBD if a detected lesion is not endoscopically resectable, if there is evidence of dysplasia at the base of the lesion, or if endoscopically invisible HGD or multifocal LGD is found in the colon during a high-quality chromoendoscopy examination (Grade: Moderate)
42 SCENIC: Detection of Dysplasia on Surveillance Colonoscopy High definition is recommended rather than standard definition colonoscopy (Strong recommendation) Chromoendoscopy is recommended rather than standard-definition white-light colonoscopy (Strong recommendation) Chromoendoscopy is suggested rather than white-light colonoscopy when performing surveillance with high-definition colonoscopy (Conditional recommendation) Narrow band is not recommended as alternative to standard definition or high definition white light endoscopy or chromoendoscopy (Conditional recommendation) Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:
43 SURFACE: guidelines chromo Strict patient selection. Unmask the mucosal surface. Reduce peristaltic waves. Full length staining of the colon. Augmented detection with dyes. Crypt architecture analysis. Endoscopic targeted biopsies. Kiesslich&Neurath. Chromoendoscopy in inflammatory bowel disease. Gastroenterology Clinics of North America 41.2 (2012):

44 Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:
45 What I Do: Chromo for all IBD Surveillance. Targeted biopsies In our AEC: 0.1% IC (food coloring grade) Mixed that morning of in 1 liter H20. Clean further on way in. Flusher starting in the cecum, panchromoendoscopy by section. Suction pools carefully No significant inflammation. Targeted biopsies only. I book 45 min. (usually takes me 30 min) 0.02% MB in hospital (One 10ml vial of MB in 500 cc sterile water) Otherwise same protocol If IC available, Soetikno protocol 1hour booking in hospital Wear scrubs and old sneakers(otherwise your clothes will be stained blue!)


46 Chromo in Practice Mix to 0.1% to 0.4%

47 Chromo in the Hospital
48 Should You Continue to Obtain Random Biopsies When Using Chromoendoscopy? Continue random biopsies in high risk patients such as those with PSC or a previous history of dysplasia Use random biopsies as alternative to CE or in patients with poor prep and/or multiple pseudopolyps Continue to take several biopsies to document extent and severity of disease
 Patient preferences Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus")
49 Invisible Dysplasia If invisible dysplasia is detected and confirmed by a second expert pathologist, management must be individualized and is dependent on: Low grade dysplasia vs high grade dysplasia Unifocal vs multifocal Patients risk factors (PSC, duration and extent of disease, FH of CRC, etc) Patient preferences Laine L, Kaltenbach T, Barkun A, et al and SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148:
50 Summary: Management of Dysplasia Dysplasia should be confirmed by a second expert pathologist Polypoid and nonpolypoid dysplasia can be managed endoscopically if the lesion can be completely resected and there is no adjacent invisible dysplasia; otherwise surgery is required Advanced endoscopic techniques may be needed for resection and referral to an experienced endoscopist appropriate

51 Sanduleanu S, Kaltenbach T, Barkun A, et al. A roadmap to the implementation of chromoendoscopy in inflammatory bowel disease colonoscopy surveillance practice. Gastrointest Endosc Jan;83(1):
52 Endoscopy Resources Soetikno R, Subramanian V, Kaltenbach T, et al. The detection of nonpolypoid (flat and depressed) colorectal neoplasms in patients with inflammatory bowel disease. Gastroenterology. 2013;144: Soetikno R, Sanduleanu S, Kaltenbach T. An atlas of the nonpolypoid colorectal neoplasms in IBD. Gastrointest Endosc Clin N Am Jul;24(3): Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease. Gastrointestinal Endoscopy Clinics of North America. Volume 24, Issue 3, Pages (July 2014). Google: youtube ASGE Chromoendoscopy

53
54 Post SCENIC Studies Author/year Choi UK, 2015 Mooiweer Dutch, 2015 Marion US, 2015 Gasia Canada, 2016 Deepak US, 2016 Rubin US, 2016 Parakkal US, 2016 Study Period Study Design Cohort Dysplastic Lesions Bottom Line Retrospective Surveillance 267 CE Superior Retrospective Surveillance 401 CE no difference Retrospective Longitudinal Surveillance 44 CE Superior Retrospective Surveillance 74 CE no difference Retrospective Dysplasia 95 CE Superior Retrospective Dysplasia 85 CE Superior Retrospective 95 (78 UC) Dysplasia 40 CE Superior FD&C#2 Blue
55 Chromoendoscopy superior to Standard in Long Term Surveillance Marion JF, et al. Clinical Gastroenterology and Hepatology 2016;14:
56 Ashwin Says Chromo is Better


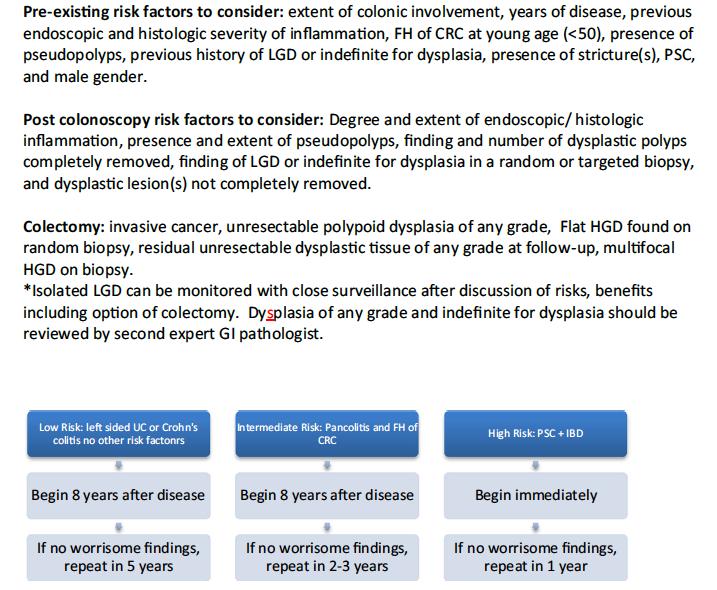
57 British Society Guidelines 2010 Screening colonoscopy at 10 years (preferably in remission, pancolonic dye-spray) Lower Risk Extensive colitis with NO ACTIVE endoscopic/histological inflammation OR left-sided colitis OR Crohn s colitis of <50% colon Intermediate Risk Extensive colitis with MILD ACTIVE endoscopic/histological inflammation OR post-inflammatory polyps OR family history CRC in FDR aged 50+ Higher Risk Extensive colitis with MODERATE/SEVERE ACTIVE endoscopic/histological inflammation OR stricture in past 5 years OR dysplasia in past 5 years declining surgery OR PSC / transplant for PSC OR family history CRC in FDR aged <50 5 Years 3 Years 1 Year Pancolonic dye spraying with targeted biopsy of abnormal areas is recommended, otherwise 2 4 random biopsies from every 10 cm of the colorectum should be taken Other Considerations Patient preference, multiple postinflammatory polyps, age and comorbidity, accuracy and completeness of examination FDR, first-degree relative; PSC, primary sclerosing cholangitis Cairns SR et al. Gut 2010;56:666.
58
59 Stool DNA as Adjunct to Endoscopy Pilot studies have demonstrated that methylated DNA markers ( BMP3, Vimentin, EYA4, NDRG4) can be detected in stool of IBD patients with dysplasia or CRC DNA Chip: N=338, ROC=0.93, Sensitivity 92%, Specificity 94% Kisiel JB, et al. Stool DNA testing for the of colorectal neoplasia in patients with inflammatory bowel disease. Aliment Pharmacol Ther Mar;37(5): Kisiel JB, et al. DDW 2016
60 Chemoprevention Equivocal data on folic acid, 5-ASA Emerging data on Statins 47% CRC (95% CI: 26-62%) 94% IBD-CRC (n=55) (95% CI: 45-99%) Atorvastatin indcuces apoptosis in CRC cells, slows colon tumor xenograft growth in mice Poynter J, Higgins PDR, et al. NEJM 2005;352: Johnson LA, Higgins PDR. DDS 2010;55:
61 Chemoprevention 11,001 IBD patients Boston area from , CRC diagnosis validated 1376 pts (12.5%) on statins vs 9,625 not Controlled for age, gender, smoking, PSC, CRP, ESR, surveill colonoscopy within 3 yr Statin use associated with 58% reduction in IBD-CRC (95% CI: 38-72%) 2% of statin users developed CRC 3% of nonstatin users developed CRC Ananthakrishnan A, et al. DDW 2016
62 Summary The absolute risk of CRC in IBD is limited Stratify for high risk: Extensive disease, long duration, uncontrolled inflammation, FH of CRC and patients with PSC carry a greater risk of CRC To prevent IBD related CRC, the goal is to minimize severity and extent of inflammation, whereas the methods used to do this (regular follow-up, medical treatment, chemoprevention, surveillance, and surgery) act in common and not as single cancer-preventive factors Random biopsies have extremely low yield Chromoendoscopy detects more dysplasia than HD white light endoscopy We need prospective data that chromoendoscopy prevents development of CRC in IBD patients
63 Why Chromoendoscopy? Increases yield of important findings No increased risk Safe, easy to learn and perform Takes more time*: but isn t your patient worth it? Don t you take your time on screening colons for high ADR? Potential for cost saving (less frequent scopes, no need for random biopsies) Important in the MACRA/MIPS era! Should be standard for surveillance in IBD (in my opinion). Negative chromocolonoscopy associated with good long term colectomy free survival Long term data needed. Risk stratify with Stool DNA? Chemoprevention with statins? *Increased time is negligible if stop random biopsies and use flusher
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Chromoendoscopy - Should It Be Standard of Care in IBD?
 Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Diagnostic techniques for surveillance of dysplasia
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
CRC and Dysplasia in IBD: Objectives of Talk. Colorectal Cancer and Dysplasia in IBD: A Case-Based Approach. Page 1
 Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
Colorectal Cancer and in IBD: A Case-Based Approach Fernando Velayos MD MPH Associate Director of Translational Research University of California, San Francisco Center for Crohn s s and Colitis CRC and
PATIENTS WITH LONG-STANDING inflammatory
 Digestive Endoscopy 2016; 28: 266 273 doi: 10.1111/den.12634 Review Paradigm Shift in the Surveillance and Management of Dysplasia in Inflammatory Bowel Disease (West) Roy Soetikno, 1 Tonya Kaltenbach,
Digestive Endoscopy 2016; 28: 266 273 doi: 10.1111/den.12634 Review Paradigm Shift in the Surveillance and Management of Dysplasia in Inflammatory Bowel Disease (West) Roy Soetikno, 1 Tonya Kaltenbach,
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Quality in Endoscopy: Can We Do Better?
 Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Random biopsy is recommended in the US to detect
 Gastroenterology in Motion Ralf Kiesslich and Thomas D. Wang, Section Editors The Detection of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Patients With Inflammatory Bowel Disease ROY SOETIKNO,
Gastroenterology in Motion Ralf Kiesslich and Thomas D. Wang, Section Editors The Detection of Nonpolypoid (Flat and Depressed) Colorectal Neoplasms in Patients With Inflammatory Bowel Disease ROY SOETIKNO,
Chromoendoscopy as an Adjunct to Colonoscopy
 Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
IBD high risk groups
 IBD high risk groups Ulcerative colitis Value (95% CI) CRC prevalence (%) 3.7 (3.2-4.2) Overall annual CRC incidence (%) 0.3 (0.2-0.4) Annual CRC incidence in first decade of UC (%) 0.2 (0.1-0.2) Annual
IBD high risk groups Ulcerative colitis Value (95% CI) CRC prevalence (%) 3.7 (3.2-4.2) Overall annual CRC incidence (%) 0.3 (0.2-0.4) Annual CRC incidence in first decade of UC (%) 0.2 (0.1-0.2) Annual
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/CT Colonography Chromoendoscopy as an Adjunct to Colonoscopy
FEP Medical Policy Manual Effective Date: April 15, 2018 Related Policies: 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/CT Colonography Chromoendoscopy as an Adjunct to Colonoscopy
Description. Section: Medicine Effective Date: July 15, Subsection: Original Policy Date: September 13, 2012 Subject: Page: 1 of 17
 Page: 1 of 17 Last Review Status/Date: June 2016 Description Chromoendoscopy refers to the application of dyes or stains during endoscopy to enhance tissue differentiation or characterization. When used
Page: 1 of 17 Last Review Status/Date: June 2016 Description Chromoendoscopy refers to the application of dyes or stains during endoscopy to enhance tissue differentiation or characterization. When used
Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients with high risk of colorectal cancer
 ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.264 Intest Res 2016;14(3):264-269 Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients
ORIGINAL ARTICLE pissn 1598-9100 eissn 2288-1956 http://dx.doi.org/10.5217/ir.2016.14.3.264 Intest Res 2016;14(3):264-269 Role of random biopsies in surveillance of dysplasia in ulcerative colitis patients
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease
 An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Colorectal Cancer in Inflammatory Bowel Disease
 Gut and Liver, Vol. 2, No. 2, September 2008, pp. 61-73 review Colorectal Cancer in Inflammatory Bowel Disease Jonathan Potack and Steven H. Itzkowitz Division of Gastroenterology, Department of Medicine,
Gut and Liver, Vol. 2, No. 2, September 2008, pp. 61-73 review Colorectal Cancer in Inflammatory Bowel Disease Jonathan Potack and Steven H. Itzkowitz Division of Gastroenterology, Department of Medicine,
Chromoendoscopy is an image-enhanced endoscopic technique
 The Role of Chromoendoscopy in Evaluating Colorectal Dysplasia Anna M. Buchner, MD, PhD Dr Buchner is an assistant professor of medicine in the Division of Gastroenterology at the University of Pennsylvania
The Role of Chromoendoscopy in Evaluating Colorectal Dysplasia Anna M. Buchner, MD, PhD Dr Buchner is an assistant professor of medicine in the Division of Gastroenterology at the University of Pennsylvania
Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease
 Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease Francis A. Farraye, MD, MSc Clinical Director, Section of Gastroenterology, Boston Medical Center Professor of Medicine,
Diagnosis and Management of Flat and Polypoid Dysplasia in Inflammatory Bowel Disease Francis A. Farraye, MD, MSc Clinical Director, Section of Gastroenterology, Boston Medical Center Professor of Medicine,
Patients with longstanding ulcerative colitis (UC) or
 or") ORIGINAL ARTICLE Misclassification of Dysplasia in Patients with Inflammatory Bowel Disease: Consequences for Progression Rates to Advanced Neoplasia Fiona D.M. van Schaik, MD,* Fiebo J.W. ten Kate, MD,
ORIGINAL ARTICLE Misclassification of Dysplasia in Patients with Inflammatory Bowel Disease: Consequences for Progression Rates to Advanced Neoplasia Fiona D.M. van Schaik, MD,* Fiebo J.W. ten Kate, MD,
White Rose Research Online URL for this paper: Version: Accepted Version
 This is a repository copy of Patients with Endoscopically Visible Polypoid Adenomatous Lesions Within the Extent of Ulcerative Colitis Have an Increased Risk of Colorectal Cancer Despite Endoscopic Resection.
This is a repository copy of Patients with Endoscopically Visible Polypoid Adenomatous Lesions Within the Extent of Ulcerative Colitis Have an Increased Risk of Colorectal Cancer Despite Endoscopic Resection.
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts
 Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Endoscopy in IBD. F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M.
 Frankfurt/M.") F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
F.Hartmann K.Kasper-Kliniken (St.Marienkrankenhaus) Frankfurt/M. F.Hartmann@em.uni-frankfurt.de Indications for endoscopy Diagnosis Management Surveillance Diagnosis Single most valuable tool: ileocolonoscopy
Inflammatory bowel disease (IBD), which includes ulcerative
, which includes ulcerative") Chromoendoscopy and Dysplasia Surveillance in Inflammatory Bowel Disease: Past, Present, and Future Steven Naymagon, MD, and Thomas A. Ullman, MD Dr Naymagon is an assistant professor of medicine and Dr
Chromoendoscopy and Dysplasia Surveillance in Inflammatory Bowel Disease: Past, Present, and Future Steven Naymagon, MD, and Thomas A. Ullman, MD Dr Naymagon is an assistant professor of medicine and Dr
Advances in Endoscopic Imaging
 Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Advances in Endoscopic Imaging SGNA meeting February 20, 2010 Amar R. Deshpande, MD Asst Professor of Medicine Division of Gastroenterology University of Miami Miller School of Medicine Objectives To recognize
Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
 nature publishing group ORIGINAL CONTRIBUTIONS 1461 CME see related editorial on page 1473 Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
nature publishing group ORIGINAL CONTRIBUTIONS 1461 CME see related editorial on page 1473 Low-Grade Dysplasia in Ulcerative Colitis: Risk Factors for Developing High-Grade Dysplasia or Colorectal Cancer
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Patients with inflammatory bowel disease (IBD) carry a higher
 carry a higher") Advances in the Diagnosis and Management of Colonic Dysplasia in Patients With Inflammatory Bowel Disease Shirley Cohen-Mekelburg, MD, Yecheskel Schneider, MD, Stephanie Gold, MD, Ellen Scherl, MD, and
Advances in the Diagnosis and Management of Colonic Dysplasia in Patients With Inflammatory Bowel Disease Shirley Cohen-Mekelburg, MD, Yecheskel Schneider, MD, Stephanie Gold, MD, Ellen Scherl, MD, and
Objec-ve. Case Presenta-ons and Ques-ons to Panel. Dysplasia case 11/13/11
 Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Adherence to surveillance guidelines for dysplasia and colorectal carcinoma in ulcerative and Crohn s colitis patients in the Netherlands
 Online Submissions: wjg.wjgnet.com World J Gastroenterol 9 January 14; 15(2): 226-23 wjg@wjgnet.com World Journal of Gastroenterology ISSN 17-9327 doi:1.3748/wjg.15.226 9 The WJG Press and Baishideng.
Online Submissions: wjg.wjgnet.com World J Gastroenterol 9 January 14; 15(2): 226-23 wjg@wjgnet.com World Journal of Gastroenterology ISSN 17-9327 doi:1.3748/wjg.15.226 9 The WJG Press and Baishideng.
Corporate Medical Policy
 Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
Corporate Medical Policy Chromoendoscopy as an Adjunct to Colonoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: chromoendoscopy_as_an_adjunct_to_colonoscopy 7/2012 11/2017
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls. Disclosures: None. CRC: still a major public health problem
 Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls Disclosures: None Jonathan P. Terdiman, M.D. Professor of Clinical Medicine University of California, San Francisco CRC: still a major public
Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls Disclosures: None Jonathan P. Terdiman, M.D. Professor of Clinical Medicine University of California, San Francisco CRC: still a major public
Endoscopic Therapeutic Approach for Dysplasia in Inflammatory Bowel Disease
 FOCUSED REVIEW SERIES: Current Status of Endoscopy in the Management of Inflammatory Bowel Disease Clin Endosc 2017;50:437-445 https://doi.org/10.5946/ce.2017.132 Print ISSN 2234-2400 On-line ISSN 2234-2443
FOCUSED REVIEW SERIES: Current Status of Endoscopy in the Management of Inflammatory Bowel Disease Clin Endosc 2017;50:437-445 https://doi.org/10.5946/ce.2017.132 Print ISSN 2234-2400 On-line ISSN 2234-2443
Confocal Laser Endomicroscopy
 Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Confocal Laser Endomicroscopy Policy Number: 2.01.87 Last Review: 3/2018 Origination: 3/2013 Next Review: 9/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for
Improving you ADR. Robert Enns Colonoscopy Education Day October 2018
 Improving you ADR Robert Enns Colonoscopy Education Day October 2018 ADR Applying to CSP Assume 50% ADR in FIT positive patients Out of 40 patients only 20 will have polyps Out of 20 likely 15 will be
Improving you ADR Robert Enns Colonoscopy Education Day October 2018 ADR Applying to CSP Assume 50% ADR in FIT positive patients Out of 40 patients only 20 will have polyps Out of 20 likely 15 will be
Post-colonoscopy colorectal cancers in Lynch syndrome
 Post-colonoscopy colorectal cancers in Lynch syndrome Francesc Balaguer, MD PhD High Risk Colorectal Cancer Clinic Head of the Gastroenterology Department Hospital Clínic de Barcelona fprunes@clinic.cat
Post-colonoscopy colorectal cancers in Lynch syndrome Francesc Balaguer, MD PhD High Risk Colorectal Cancer Clinic Head of the Gastroenterology Department Hospital Clínic de Barcelona fprunes@clinic.cat
Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease
 Aliment Pharmacol Ther 23; 18 (Suppl. 2): 1 5. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease P. MUNKHOLM Department of Medical Gastroenterology, Hvidovre
Aliment Pharmacol Ther 23; 18 (Suppl. 2): 1 5. Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease P. MUNKHOLM Department of Medical Gastroenterology, Hvidovre
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease
 Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
Title: Serrated polyposis syndrome associated with long-standing inflammatory bowel disease Authors: Jesús Castro, Miriam Cuatrecasas, Francesc Balaguer, Elena Ricart, María Pellisé DOI: 10.17235/reed.2017.5068/2017
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
I n 1925, Crohn and Rosenberg first observed that ulcerative
 256 INFLAMMATORY BOWEL DISEASE Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis M D Rutter, B P Saunders, G Schofield, A Forbes, A B Price, I C Talbot... See
256 INFLAMMATORY BOWEL DISEASE Pancolonic indigo carmine dye spraying for the detection of dysplasia in ulcerative colitis M D Rutter, B P Saunders, G Schofield, A Forbes, A B Price, I C Talbot... See
Advances in Ulcerative Colitis - Volume 3 CME
 1 de 12 22/01/2008 04:46 p.m. More: Advances in Ulcerative Colitis Advances in Ulcerative Colitis - Volume 3 CME Complete author affiliations and disclosures are at the end of this activity. Release Date:
1 de 12 22/01/2008 04:46 p.m. More: Advances in Ulcerative Colitis Advances in Ulcerative Colitis - Volume 3 CME Complete author affiliations and disclosures are at the end of this activity. Release Date:
Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary sclerosing cholangitis and ulcerative colitis
 Journal of Crohn's and Colitis (2013) 7, 974 981 Available online at www.sciencedirect.com ScienceDirect Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary
Journal of Crohn's and Colitis (2013) 7, 974 981 Available online at www.sciencedirect.com ScienceDirect Random biopsies during surveillance colonoscopy increase dysplasia detection in patients with primary
Finding and Removing Difficult Polyps (safely)
") Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Where a licence is displayed above, please note the terms and conditions of the licence govern your use of this document.
 A Randomized Trial Comparing High Definition Colonoscopy Alone With High Definition Dye Spraying and Electronic Virtual Chromoendoscopy for Detection of Colonic Neoplastic Lesions During IBD Surveillance
A Randomized Trial Comparing High Definition Colonoscopy Alone With High Definition Dye Spraying and Electronic Virtual Chromoendoscopy for Detection of Colonic Neoplastic Lesions During IBD Surveillance
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA
 Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Can We Predict the Natural History of Ulcerative Colitis? Edward V Loftus, Jr, MD Professor of Medicine Mayo Clinic Rochester, Minnesota, USA Endpoints Overview Hospitalization Surgery Colorectal cancer
Colon Cancer Screening with Image-Enhanced Endoscopy
 FOCUSED REVIEW SERIES: Endoscopic Screening and Surveillance for Gastrointestinal Cancer Clin Endosc 2014;47:504-508 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.6.504
FOCUSED REVIEW SERIES: Endoscopic Screening and Surveillance for Gastrointestinal Cancer Clin Endosc 2014;47:504-508 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2014.47.6.504
Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps
 Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps Full guideline Draft for consultation, May 00 0 This guideline
Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn s disease and polyps Full guideline Draft for consultation, May 00 0 This guideline
Colorectal cancer surveillance in inflammatory bowel diseases
 Turkish Journal of Cancer Volume 34, No.2, 2004 55 Colorectal cancer surveillance in inflammatory bowel diseases MURAT TÖRÜNER Ankara University Medical School, Department of Gastroenterology, Ankara-Turkey
Turkish Journal of Cancer Volume 34, No.2, 2004 55 Colorectal cancer surveillance in inflammatory bowel diseases MURAT TÖRÜNER Ankara University Medical School, Department of Gastroenterology, Ankara-Turkey
Endoscopic monitoring of IBD patients for healing and dysplasia in 2018
 Endoscopic monitoring of IBD patients for healing and dysplasia in 2018 Marietta Iacucci, MD, PhD, FASGE Senior Associate Professor(Reader) University of Birmingham, UK Adjunct Associate Professor of Medicine
Endoscopic monitoring of IBD patients for healing and dysplasia in 2018 Marietta Iacucci, MD, PhD, FASGE Senior Associate Professor(Reader) University of Birmingham, UK Adjunct Associate Professor of Medicine
The variable risk of colorectal cancer in patients with inflammatory bowel disease.
 The variable risk of colorectal cancer in patients with inflammatory bowel disease. Lindgren, Stefan Published in: European Journal of Internal Medicine DOI: 10.1016/j.ejim.2004.12.001 Published: 2005-01-01
The variable risk of colorectal cancer in patients with inflammatory bowel disease. Lindgren, Stefan Published in: European Journal of Internal Medicine DOI: 10.1016/j.ejim.2004.12.001 Published: 2005-01-01
Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
 1022 ORIGINAL CONTRIBUTIONS nature publishing group see related editorial on page 1035 Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
1022 ORIGINAL CONTRIBUTIONS nature publishing group see related editorial on page 1035 Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
Missed Lesions at Endoscopy. Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand
 Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Patients with long-standing, extensive ulcerative colitis (UC) Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine
 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1225 1230 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine THOMAS ULLMAN,* VICTORIA CROOG,* NOAM HARPAZ, SABERA HOSSAIN, ASHER
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2008;6:1225 1230 Progression to Colorectal Neoplasia in Ulcerative Colitis: Effect of Mesalamine THOMAS ULLMAN,* VICTORIA CROOG,* NOAM HARPAZ, SABERA HOSSAIN, ASHER
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Benchmarking For Colonoscopy. Technology and Technique to Improve Adenoma Detection
 Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
Malignancy in ulcerative colitis (UC) is believed to ORIGINAL ARTICLES
 is believed to ORIGINAL ARTICLES") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:534 541 ORIGINAL ARTICLES Long-term Follow-up After Polypectomy Treatment for Adenoma-Like Dysplastic Lesions in Ulcerative Colitis ROBERT D. ODZE,* FRANCIS
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:534 541 ORIGINAL ARTICLES Long-term Follow-up After Polypectomy Treatment for Adenoma-Like Dysplastic Lesions in Ulcerative Colitis ROBERT D. ODZE,* FRANCIS
Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines
 INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-8 Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines Vicent Hernández a, Juan Clofent b Complexo Hospitalario
INVITED REVIEW Annals of Gastroenterology (2012) 25, 1-8 Intestinal cancer in inflammatory bowel disease: natural history and surveillance guidelines Vicent Hernández a, Juan Clofent b Complexo Hospitalario
Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:303 308 Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis BARBARA BRADEN,* JOHNNY HALLIDAY,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:303 308 Risk for Colorectal Neoplasia in Patients With Colonic Crohn s Disease and Concomitant Primary Sclerosing Cholangitis BARBARA BRADEN,* JOHNNY HALLIDAY,*
Technology and Interventions to Improve ADR
 Technology and Interventions to Improve ADR Aasma Shaukat, MD MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of
Technology and Interventions to Improve ADR Aasma Shaukat, MD MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of
Tips to Improve ADRs during Colonoscopy
 Tips to Improve ADRs during Colonoscopy Aasma Shaukat, MD, MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of high-quality
Tips to Improve ADRs during Colonoscopy Aasma Shaukat, MD, MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of high-quality
AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease
 GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
GASTROENTEROLOGY 2010;138:746 774 AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease AGA Podcast interview: www.gastro.org/gastropodcast. Learning
MINI-REVIEW. Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer. Lin-Lin Ren, Jing-Yuan Fang * Abstract.
 Should we Sound the Alarm?- Dysplasia and Colitis-associated Colorectal Cancer MINI-REVIEW Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer Lin-Lin Ren, Jing-Yuan Fang * Abstract
Should we Sound the Alarm?- Dysplasia and Colitis-associated Colorectal Cancer MINI-REVIEW Should we Sound the Alarm? Dysplasia and Colitis-associated Colorectal Cancer Lin-Lin Ren, Jing-Yuan Fang * Abstract
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS
 SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
SURGICAL MANAGEMENT OF ULCERATIVE COLITIS Cary B. Aarons, MD Associate Professor of Surgery Division of Colon & Rectal Surgery University of Pennsylvania AGENDA Background Diagnosis/Work-up Medical Management
Devices To Improve Colon Polyp Detection
 Devices To Improve Colon Polyp Detection ACG/VGS Regional Postgraduate Course Sep 10-11, 2016 Williamsburg, VA VIVEK KAUL, MD, FACG Segal-Watson Professor of Medicine Chief, Division of Gastroenterology
Devices To Improve Colon Polyp Detection ACG/VGS Regional Postgraduate Course Sep 10-11, 2016 Williamsburg, VA VIVEK KAUL, MD, FACG Segal-Watson Professor of Medicine Chief, Division of Gastroenterology
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Improving Your Adenoma Detection Rate
 Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1015 1021 Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine SIERRA MATULA,* VICTORIA CROOG,* STEVEN ITZKOWITZ,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1015 1021 Chemoprevention of Colorectal Neoplasia in Ulcerative Colitis: The Effect of 6-Mercaptopurine SIERRA MATULA,* VICTORIA CROOG,* STEVEN ITZKOWITZ,*
Medical Policy. MP Confocal Laser Endomicroscopy
 Medical Policy BCBSA Ref. Policy: 2.01.87 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
Medical Policy BCBSA Ref. Policy: 2.01.87 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.80 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Presence of pseudopolyps in ulcerative colitis is associated with a higher risk for treatment escalation Dimitrios S. Politis a, Konstantinos
EXPERT WORKING GROUP Surveillance after neoplasia removal. Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum
 EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
Microbiome, Inflammation and Cancer
 Microbiome, Inflammation and Cancer Anita Afzali MD, MPH, FACG Medical Director, OSU Inflammatory Bowel Disease Center Abercrombie & Fitch Endowed Chair in Inflammatory Bowel Disease 4 th Annual Cancer
Microbiome, Inflammation and Cancer Anita Afzali MD, MPH, FACG Medical Director, OSU Inflammatory Bowel Disease Center Abercrombie & Fitch Endowed Chair in Inflammatory Bowel Disease 4 th Annual Cancer
Novel Optical Research at UPMC
 Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Novel Optical Research at UPMC Randall Brand, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Pittsburgh Medical Center Background Patients with UC and CD of
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis
 Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
Alimentary Pharmacology and Therapeutics Randomised clinical trial: delayed-release oral mesalazine 4.8 g day vs. 2.4 g day in endoscopic mucosal healing ASCEND I and II combined analysis G. R. Lichtenstein*,
IBD and Cancer: Myths and Facts
 IBD and Cancer: Myths and Facts Thomas A. Ullman, MD Medical Director, Faculty Prac>ce Department of Medicine Icahn School of Medicine at Mount Sinai New York, USA Risk of Colorectal Cancer in UC Eaden
IBD and Cancer: Myths and Facts Thomas A. Ullman, MD Medical Director, Faculty Prac>ce Department of Medicine Icahn School of Medicine at Mount Sinai New York, USA Risk of Colorectal Cancer in UC Eaden
Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
CANCER SCREENING IN IBD David T. Rubin, MD, FACG
 1C: Advances in Inflammatory Bowel Disease CANCER SCREENING IN IBD David T. Rubin, MD, FACG Risk Factors for Neoplasia in Chronic Colitis An increasing amount of evidence has provided a link between chronically
1C: Advances in Inflammatory Bowel Disease CANCER SCREENING IN IBD David T. Rubin, MD, FACG Risk Factors for Neoplasia in Chronic Colitis An increasing amount of evidence has provided a link between chronically
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
Masato Kusunoki Editor. Colitis-Associated Cancer
 Masato Kusunoki Editor Colitis-Associated Cancer 123 Colitis-Associated Cancer ThiS is a FM Blank Page Masato Kusunoki Editor Colitis-Associated Cancer Editor Masato Kusunoki Mie University Graduate School
Masato Kusunoki Editor Colitis-Associated Cancer 123 Colitis-Associated Cancer ThiS is a FM Blank Page Masato Kusunoki Editor Colitis-Associated Cancer Editor Masato Kusunoki Mie University Graduate School
High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease
 Accepted Manuscript High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease Shailja C. Shah, Joren R. ten Hove, Daniel Castaneda,
Accepted Manuscript High Risk of Advanced Colorectal Neoplasia in Patients With Primary Sclerosing Cholangitis Associated With Inflammatory Bowel Disease Shailja C. Shah, Joren R. ten Hove, Daniel Castaneda,
Meta-analysis: cancer risk of low-grade dysplasia in chronic ulcerative colitis
 Alimentary Pharmacology & Therapeutics Meta-analysis: cancer risk of low-grade dysplasia in chronic ulcerative colitis T. THOMAS*, K. A. ABRAMS, R.J.ROBINSON*&J.F.MAYBERRY* *Department of Gastroenterology,
Alimentary Pharmacology & Therapeutics Meta-analysis: cancer risk of low-grade dysplasia in chronic ulcerative colitis T. THOMAS*, K. A. ABRAMS, R.J.ROBINSON*&J.F.MAYBERRY* *Department of Gastroenterology,