SURGICAL SITE INFECTIONS SURVEILLANCE & PREVENTION
|
|
|
- Sara May Watson
- 5 years ago
- Views:
Transcription


1 SURGICAL SITE INFECTIONS SURVEILLANCE & PREVENTION
2 Objectives List evidence based prevention strategies Define Surgical Site Infections based on NHSN definitions Describe surveillance tips
3 Facts According to 2018 Patient Safety Movement Foundation: There are approximately 300,000 SSIs annually. 17% of all HAIs, second only to UTIs. SSIs occur in 2%-5% of patients undergoing inpatient surgery The SSI mortality rate is 3% with a 2-11% times higher risk of death versus other infections. 75% of deaths among patients with SSI are directly attributable to the SSI. Long term disabilities can result from SSIs, resulting in life-altering disabilities and associated financial burdens.
4 So what s reportable in Texas?
5
6 Prevention of SSI Pre-operative Skin cleansing with CHG and educate patients on how to apply/bathe/shower & shampoo prior to surgery Pre-operative screening for patients at risk for SSI. Nasal screening for Staphylococcus aureus in patients undergoing cardiac and elective orthopedic surgery Decolonize protocol for carriers with intranasal meds.
7 Educate patients & families on SSI prevention. Stop smoking affects wound healing Proper nutrition Diabetes needs to be controlled Identify skin irritations and hypersensitivity & any new skin abrasions Post-op wound healing techniques used Proper Hand Hygiene Proper hair removal (NO SHAVING or RAZORS, clipping only those areas needed).
8 Appropriate timing, selection and duration of prophylactic antibiotics Maintain normothermia with forced air blankets, pre-op, during surgery and in PACU. Use warmed IV fluids for IVs and flushes Traffic control in the OR Protect primary closure incisions with sterile dressing for hours post-op Discontinue ABX within 24 hours after surgery unless s/s of infection are present.
9 NHSN Operative Procedure that is included in the ICD-10-PCS or CPT NHSN operative procedure code mapping AND takes place during an operation where at least one incision (including laparoscopic approach and cranial Burr holes) is made through the skin or mucous membrane, or reoperation via an incision that was left open during a prior operative procedure AND takes place in an operating room (OR), defined as a patient care area that met the Facilities Guidelines Institute s (FGI) or American Institute of Architects (AIA) criteria for an operating room when it was constructed or renovated11. This may include an operating room, C-section room, interventional radiology room, or a cardiac catheterization lab.
10 NHSN Inpatient Operative Procedure NHSN Inpatient Operative Procedure: An NHSN operative procedure performed on a patient whose date of admission to the healthcare facility and the date of discharge are different calendar days.
11 NHSN Outpatient Operative Procedure NHSN Outpatient Operative Procedure: An NHSN operative procedure performed on a patient whose date of admission to the healthcare facility and date of discharge are the same calendar day.

12
13 Primary Closure Primary Closure = closure of the skin level during the original surgery, regardless of the presence of wires, wicks, drains, or other devices or objects extruding through the incision, includes surgeries where the skin is closed by some means. Thus, if any portion of the incision is closed at the skin level, by any manner, a designation of primary closure should be assigned to the surgery. NOTE: If a procedure has multiple incision/laparoscopic trocar sites and any of the incisions are closed primarily, then the procedure is entered as having been closed primarily. This change removed the phrase all tissue levels from the definition. This definition will be easier to apply and is closer to definitions used by other surgical professional groups.

14
15 Non- Primary Closure Skin level is left completely open during the original surgery Deep tissue layers may be closed by some means (with the skin level left open), or the deep and superficial layers may both be left completely open. Wounds with non-primary closure may or may not be described as "packed with gauze or other material, and may or may not be covered with plastic, wound vacs, or other synthetic devices or materials. For example: a laparotomy in which the incision was closed to the level of the deep tissue layers, sometimes called fascial layers or deep fascia, but the skin level was left open. For example: an open abdomen case in which the abdomen is left completely open after the surgery.

16

17
18 Case 1 A patient is admitted with a ruptured diverticulum and a COLO procedure is performed in the inpatient OR. Case is entered as a wound class 3 Specimen is obtained in the OR which later returns (+) for E. coli The skin incision was closed at 4 locations with staples with gauze packing in between.
19 Is this procedure primarily closed? 1. Yes 2. No
20 Is this procedure primarily closed? 1. Yes 2. No
21 Case 1 -Rationale The skin is closed at some points along the skin incision. Thus, if any portion of the incision is closed at the skin level, by any manner, a designation of primary closure should be assigned to the surgery.
22 If you are following COLO in your monthly reporting plan should this case be entered into your denominator data? 1.Yes 2.No
23 If you are following COLO in your monthly reporting plan should this case be entered into your denominator data? 1.Yes 2.No
24 Surveillance Surveillance of SSIs with feedback of appropriate data to surgeons has been shown to be an important component of strategies to reduce SSI risk. A successful surveillance program includes the use of epidemiologically sound infection definitions and effective surveillance methods stratification of SSI rates according to risk factors associated with SSI development data feedback A new CDC and Healthcare Infection Control Practices Advisory Committee guideline for the Prevention of Surgical Site Infection has been published in 2017 and has replaced the previous Guideline for Prevention of Surgical Site Infection, 1999
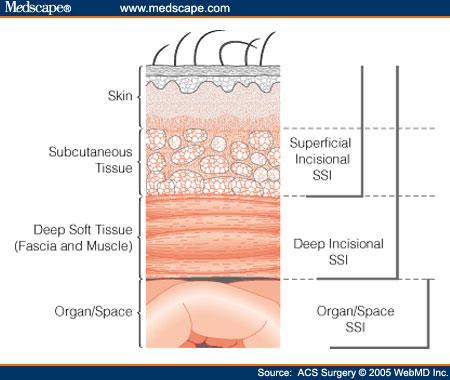
25 CDC Definitions NHSN manual from Jan pdf 3 Types Superficial Incisional SSI Deep Incisional SSI Organ/ Organ Space
26 Sources of Data for Finding SSI Microbiology reports Infection control rounds on nursing units Pharmacy reports for antimicrobial use Operating room report of surgeries Use post-discharge surveillance methods for SSI Electronic Surveillance Programs ER Diagnosis List Case Managers IPs in your community!
27 Important Information! Please note that key terms that have been defined in other NHSN trainings (e.g. CLABSI, CAUTI) including Infection Window Period, Present on Admission (POA), Healthcareassociated Infection (HAI), and Repeat Infection Timeframe (RIT) DO NOT apply to SSI!
28 Date of Event Date of event (DOE): For an SSI the date of event is the date when the first element used to meet the SSI infection criterion occurs for the first time during the surveillance period. The date of event must fall within the SSI surveillance period to meet SSI criteria.
29 DOE for SSIs that progress to a deeper level during surveillance period SSIs are always reported at the deepest level that they occur within the surveillance period. If during the surveillance period a patient s initial SSI meets criteria for a deeper level, then the date of event should be the date for the deepest level.
30
31 Example For example: Day 1 COLO procedure Day 6 DOE for meeting a superficial incisional SSI Day 25 DOE for the meeting an organ space IAB SSI Only report one SSI with the DOE for the organ space IAB
32 Pathogen Assignment The Pathogen Assignment Guidance found in Chapter 2 Identifying HAIs is based on Repeat Infection Timeframes (RIT) which is not used with SSIs SSI are procedure based and have long surveillance periods (30 to 90 days) SSIs can progress to a deeper level during a surveillance period and a new pathogen can be found. Pathogen Assignment for SSI has not changed.
33 BSI Secondary to an SSI Secondary BSI Attribution Period: The secondary BSI attribution period for SSI is a 17-day period that includes the date of SSI event, 3 days prior & 13 days after. For other HAIs the Secondary BSI attribution period is determined by using: Infection Window Period Repeat Infection Timeframe. These two definitions do not apply to SSI.

34
35 Any blood culture that occurs during the SSI Secondary BSI attribution period will be assessed using Appendix B in the BSI protocol to determine if the blood meets Secondary BSI criteria. If a (+) blood culture occurs after the SSI secondary BSI attribution period it should be fully evaluated to see if at that time it is meeting criteria to be secondary to an ongoing SSI.
.")
36 PATOS- Infection present at time of surgery Infection present at time of surgery (PATOS) denotes there is evidence of an infection/abscess at the time of the start of or during the index surgical procedure (present pre-operatively). This field is a required field and it is found on the SSI event form not on the denominator for procedure form.
37 Only select PATOS = YES if it applies to the depth of SSI that is being attributed to the procedure IF: a patient had evidence of an intra-abdominal infection at the time of surgery and then later returns with an organ space SSI the PATOS field would be selected as a YES. If the patient returned with a superficial or deep incisional SSI the PATOS field would be selected as a NO.

38 The patient does not have to meet the NHSN definition of an SSI at the time of the primary procedure but there must be notation that there is evidence of infection or abscess present at the time of surgery.
39 All of the SSI SIR reports that use the new 2015 SSI baseline will exclude SSIs that are reported as present at time of surgery from both the numerator and denominator. Meaning the PATOS event is excluded in the numerator of the SIR and the procedure from which the event occurred is excluded in the denominator of the SIR.
40 Case 2 Patient was admitted with an acute abdomen, to OR for XLAP with findings of an abscess due to ruptured appendix and an APPY is performed. Patient returns 2 weeks later and meets criteria for an organ space IAB SSI.
41 Does this patient meet the criteria for PATOS? 1. PATOS= NO 2. PATOS= YES
42 Does this patient meet the criteria for PATOS? 1. PATOS= NO 2. PATOS= YES
43 Since this SSI is related to an infection that was PATOS it does not have to be reported to NHSN. 1. True 2. False
44 Since this SSI is related to an infection that was PATOS it does not have to be reported to NHSN. 1. True 2. False
45 Case 2 -Rationale The PATOS field would be selected as YES since there was evidence of infection at the time of surgery and the subsequent SSI developed at the same level. Infections that meet SSI criteria and have the PATOS field as a YES are reported to NHSN.

46

47

48
49 Reporting Instruction -24 Hour Rule (SSI Protocol 9-20) If the wound class has changed, report the higher wound class. If the ASA class has changed, report the higher ASA class. Note: When the patient returns to the OR within 24 hours of the end of the first procedure assign the surgical wound closure technique that applies when the patient leaves the OR from the first operative procedure.
50 Same NHSN operative procedure via separate incisions For operative procedures performed via separate incisions during same trip to operating room (i.e., AMP, BRST, CEA, FUSN, FX, HER, HPRO, KPRO, LAM, NEPH, OVRY, PVBY, REFUSN), separate Denominator Procedure forms are completed. To document the duration of the procedures, indicate the procedure/surgery start time to procedure/surgery finish time for each procedure separately alternatively, take the total time for the procedures and split it evenly between procedures. OR SSI Chapter : Denominator Data Reporting Instructions
51 Case 3 A patient had bilateral knee prostheses (KPRO) implanted during a single trip to the OR. Left KPRO PST at 8:30 am there was no note of a finish time for this knee Right KPRO PF time was at 11:30 am
52 Which Statement is correct? 1. One KPRO procedure should be reported with a combined duration of 3hrs 0 min 2. Two Separate KPRO procedures should be reported, each with a duration of 1hr 30 min 3. Two separate KPRO should be entered, each with a duration of 3hrs 0 min
53 Which Statement is correct? 1. One KPRO procedure should be reported with a combined duration of 3hrs 0 min 2. Two Separate KPRO procedures should be reported, each with a duration of 1hr 30 min 3. Two separate KPRO should be entered, each with a duration of 3hrs 0 min

54
55 Procedures that can never be coded as clean wound class The procedures that can never be entered as clean are: APPY, BILI, CHOL, COLO, REC, SB and VHYS. In the application, clean is not on the drop down menu. A CSEC, HYST, or OVRY can be a clean wound class based on the particular events and findings of an individual case. Wound class should be set by someone who is part of the surgical team based on the findings of each specific case.

56

57

58

59

60
61 Diabetes NHSN has added another option for users to answer the question of diabetes on the denominator for procedure form. The ICD-10-CM diagnosis codes that reflect the diagnosis of diabetes are also acceptable for use to answer YES to the diabetes field question on the denominator for procedure entry if they are documented during the admission where the procedure is performed Definition includes those with diagnosis of diabetes requiring management with insulin or a non-insulin anti-diabetic agent. Definition excludes people who receive insulin for perioperative glucose control but have no diagnosis of diabetes.
62
63

64

65

66
67 Reporting Instruction : Labor Length of time from beginning of active labor as an inpatient to delivery of the infant, expressed in hours No labor, hours = 0 Check for documentation in the chart May be defined by your hospital s policies and procedures but should reflect the onset of regular contractions or induction that leads to delivery during this admission
68 HPRO and KPRO Revisions If performed, evaluate whether any diagnoses indicating possible infection (acquired absence of hip or knee joint, with or without the presence of an antibiotic-impregnated spacer) or any procedures such as insertion or replacement of cement spacer or removal of cement spacer were coded in the 90 days prior to and including the index HPRO or KPRO revision. This field will only open on the application if the case has been entered as a HPRO or KPRO revision.

69
70 CDC Definitions Superficial (Primary or Secondary) Infection occurs within 30 days after NHSN operative procedure And Infection involves only skin or subcutaneous tissue of the incision And patient has at least one of the following: a) Purulent drainage from superficial incision b) Organisms identified from an aseptically-obtained specimen from the superficial incision or subcutaneous tissue by a culture or non-culture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment (e.g., not Active Surveillance Culture/Testing (ASC/AST) c) Superficial incision that is deliberately opened by a surgeon, attending physician or other designee and culture or non-culture based testing is not performed AND Patient has at least one of the following signs or symptoms: pain or tenderness; localized swelling; erythema; or heat. d) Diagnosis of a superficial incisional SSI by the surgeon or attending physician or other designee
71 Superficial Incisional SSI Reporting Diagnosis/treatment of cellulitis (redness/warmth/swelling), by itself, does not meet criterion d for superficial incisional SSI. Conversely, an incision that is draining or that has organisms identified by culture or non-culture based testing is not considered a cellulitis. A stitch abscess alone (minimal inflammation and discharge confined to the points of suture penetration) is not considered an SSI. A localized stab wound or pin site infection. While it would be considered either a skin (SKIN) or soft tissue (ST) infection, depending on its depth, it is not reportable under this module. Note: a laparoscopic trocar site for an NHSN operative procedure is not considered a stab wound.

72

73

74
75 Case 4 2/15-62 year-old female admitted and underwent a total knee arthroplasty (KPRO) 2/17 -Patient discharged 3/9 -Patient is seen in the physician office after the patient tripped and fell at home. There is drainage noted from the superficial incision. A culture is collected from the drainage. The culture grows coagulase-negative staphylococci (CoNS).
76 What would be reported? 1. SSI SIP attributable to the KPRO 2. SSI DIP attributable to the KPRO 3. Nothing. The wound culture grew common skin flora only. 4. Nothing. The patient fell at home, therefore you cannot attribute an SSI to the KPRO procedure.
77 Rationale Common commensals are not excluded from SSI determination. Culture results of mixed flora or mixed cutaneous flora cannot be reported to NHSN as there is no such pathogen option in this list of pathogens. Numerator Reporting Instruction #12: An SSI that otherwise meets the NHSN definitions should be reported to NHSN without regard to post-operative accidents, falls, inappropriate showering or bathing practices, or other occurrences that may or may not be attributable to patients intentional or unintentional postoperative actions.

78 Table 4 NHSN Principal Operative Procedure Category Selection Lists
79 Deep Incisional SSI An Infection occurs within 30 or 90 days after the NHSN operative procedure (where day 1 = the procedure date) according to the procedure list AND Involves deep soft tissues of the incision (e.g. fascial and muscle layers) AND
80 Patient has at least one of the following: a. Purulent drainage from the deep incision. b. a deep incision that spontaneously dehisces, or is deliberately opened or aspirated by a surgeon, attending physician** or other designee and organism is identified by a culture or nonculture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment (e.g., not Active Surveillance Culture/Testing (ASC/AST) or culture or non-culture based microbiologic testing method is not performed AND patient has at least one of the following signs or symptoms: fever (>38 C); localized pain or tenderness. A culture or nonculture based test that has a negative finding does not meet this criterion. c. an abscess or other evidence of infection involving the deep incision that is detected on gross anatomical or histopathologic exam, or imaging test

81
82 Case 5 11/1 -Patient is admitted to the hospital for an HPRO revision. No evidence of infection at the time of the surgery. 11/4 -Postoperative course is unremarkable; patient discharged. 11/18-Patient is readmitted with complaints of pain and swelling since 11/16. To OR for left hip I&D. Serous fluid was cultured from the fascial layer. 11/19 -Culture result returned and is positive for Staph epidermidis in broth only.
83 Is this an SSI? 1. Yes, meets criteria 2. No, colonized with MRSA so this was POA
84 What infection should be reported? 1. SSI-SIP 2. SSI-SIS 3. SSI-DIP 4. SSI-DIS 5. SSI-IAB
85
86 Organ/Space SSI Infection Infection occurs within 30 or 90 days after the NHSN operative procedure (where day 1= procedure date) according to the procedure list AND Infection involves any part of the body deeper than the fascial/muscle layers, that is opened or manipulated during the operative procedure AND
87 Patient has at least one of the following: Purulent drainage from a drain that is placed into the organ/space (e.g. closed suction drainage system, open drain, T-tube, CT Guided drainage). Organisms isolated from an aseptically-obtained fluid or tissue in the organ/space by a culture or non-culture based microbiologic testing method (not ASC/AST). An abscess or other evidence of infection involving the organ/space that is detected on gross anatomical or histopathologic exam, or imaging test evidence suggestive of infection AND Meets at least one criterion for a specific organ/space infection site listed. These criteria are in the Surveillance Definitions for Specific Types of Infections Chapter.

88
89 Organ Space SSI 2 different criteria must be met for Organ/Space SSI SSI organ/space criteria AND Those of the specific site of the organ/space operated on SSI event form Table of Instructions

90 Table 3 Specific Sites of an Organ/Space SSI.

91
92 Reporting Instruction Attributing SSI to an NHSN procedure when there is evidence of infection at the time of the primary surgery: POA definition does not apply to the SSI protocol. If there was evidence of infection at the time of the procedure and then later in the surveillance period the patient develops an infection that meets the NHSN SSI criteria, it is attributed to the procedure. A high level wound class is not an exclusion for a patient later meeting criteria for an SSI.
93 Case 6 On 2/1 -Patient presents to ED with acute abdomen and is admitted to the OR on the same day for colon resection (COLO). Peritoneal abscess noted at time of surgery. Abdominal abscesses drained and thorough abdominal washout, incision loosely closed with some packing between staples and a JP drain is placed in an adjacent stab wound. 2/4 -Patient discharged, wounds healing well. 2/8 -Patient presents to ED with fever, abdominal pain, and sent to CT for CT guided drainage of an abscess.
94 Case 6 This is reported as an SSI-IAB (meets IAB criterion b and 3a.) The PATOS field would be entered as a YES
95 If during the post-operative period the surgical site has an invasive manipulation/accession for diagnostic or therapeutic purposes (e.g., needle aspiration, accession of ventricular shunts, accession of breast expanders ) and there is no evidence of an infection at that time, if an SSI develops following this manipulation/accession, the infection is not attributed to the operation. This reporting instruction does NOT apply to closed manipulation (e.g., closed reduction of a dislocated hip after an orthopedic procedure). Invasive manipulation does not include wound packing, changing of wound packing materials or staple removal as part of postoperative care.

96
97 Different operative procedure categories performed via same incision during same trip to the OR: First, attempt to determine the procedure that is thought to be associated with the infection. Example: If the patient had a CBGC and CARD-AVR done at the same time and returns and meets criteria with an infected valve, then the SSI will be linked to the CARD-AVR. If it s not clear (as in the case of a superficial incisional SSI), use the NHSN Principal Operative Procedure Selection Lists to select which operative procedure to report. Categories with the highest risk of SSI are listed before those with lower risks
98 Case 7 10/8 -Patient admitted and underwent laparoscopic hysterectomy (HYST). Wound class 2. 10/15 -Readmitted with abdominal pain. CT showed fluid and air in pelvis. To OR for COLO where purulence was noted in the deep pelvic area.
99 Does this patient meet criteria for an organ space SSI? 1. Yes 2. No
100
101 What site specific SSI does this patient have? SSI-DIP SSI-IAB SSI-OREP Not an SSI
102 OREP-Deep pelvic tissue infection or other infection of the male or female reproductive tract (epididymis, testes, prostate, vagina, ovaries, uterus, chorioamnionitis, excluding vaginitis, endometritis or vaginal cuff infections) OREP Criterion 2: Patient has an abscess or other evidence of infection of affected site on gross anatomic or histopathologic exam.
, spleen, pancreas, peritoneum,")
103 Why isn t this an SSI-IAB? IAB Intraabdominal, not specified elsewhere including gallbladder, bile ducts, liver (excluding viral hepatitis), spleen, pancreas, peritoneum, subphrenicor subdiaphragmaticspace, or other intraabdominal tissue or area not specified elsewhere Site Définitions Chapter; Chapter 17
104 Case 8 3/9 49 year-old patient goes to OR for a XLAP and COLO procedure. 3/17 Patient complains of new abdominal pain. 3/18 Temperature noted of CT of abdomen findings: severe colon thickening -correlate with enteritis/colitis. Blood cultures obtained. Physician initiates and documents antimicrobial treatment for gastrointestinal tract infection. 3/20 Blood cultures return positive P. aeruginosa.
105 Does this patient meet criteria for an SSI? 1. Does not meet SSI criteria 2. SSI Organ/Space, specific site GIT, with a secondary BSI 3. SSI Organ/Space, specific site IAB, with a secondary BSI 4. SSI Organ/Space, specific site GIT without secondary BSI
106 Rationale Case 8-GIT Criterion 2d Patient has at least two of the following signs or symptoms compatible with infection of the organ or tissue involved: fever (>38.0 C), nausea*, vomiting*, pain*or tenderness*, odynophagia*, or dysphagia* And at least one of the following: d. imaging test evidence suggestive of infection (e.g., endoscopic exam, MRI, CT scan), which if equivocal is supported by clinical correlation (i.e., physician documentation of antimicrobial treatment for gastrointestinal tract infection). *With no other recognized cause P. aeruginosa is not an MBI organism must investigate blood cx as secondary to another source or as primary LCBI
107 Case 8 -Rationale Why not IAB Intraabdominal infection as the specific site of SSI? The infection is in the gastrointestinal tract and not involving the intraabdominal space GIT focuses on infections of the gastrointestinal tract Therefore, GIT is the appropriate choice site of SSI in this case Site Definitions Chapter; Chapter 17


108 Questions?
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION
 SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Facts There were an estimated 157,500 surgical site infections associated with inpatient surgeries in 2011. SSIs were the most common healthcare-associated
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Facts There were an estimated 157,500 surgical site infections associated with inpatient surgeries in 2011. SSIs were the most common healthcare-associated
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION
 SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Disclosures: I have No conflicts of interest No commercial support No specific product will be endorsed during this presentation Facts There were an
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Disclosures: I have No conflicts of interest No commercial support No specific product will be endorsed during this presentation Facts There were an
SURGICAL SITE INFECTIONS. National Healthcare Safety Network (NHSN)
") SURGICAL SITE INFECTIONS National Healthcare Safety Network (NHSN) KEY TERMS In-plan surveillance means that you have committed to following the NHSN surveillance protocol, in its entirety, for that particular
SURGICAL SITE INFECTIONS National Healthcare Safety Network (NHSN) KEY TERMS In-plan surveillance means that you have committed to following the NHSN surveillance protocol, in its entirety, for that particular
Building Confidence in NHSN. Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network
 Building Confidence in NHSN Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network Objectives Identify resources to improve reporting Examine
Building Confidence in NHSN Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network Objectives Identify resources to improve reporting Examine
SURGICAL SITE INFECTIONS. National Healthcare Safety Network (NHSN)
") SURGICAL SITE INFECTIONS National Healthcare Safety Network (NHSN) 2018 SSI UPDATES Definition for Date of Event (DOE): added additional guidance surrounding DOE and tissue level as well as timeframe for
SURGICAL SITE INFECTIONS National Healthcare Safety Network (NHSN) 2018 SSI UPDATES Definition for Date of Event (DOE): added additional guidance surrounding DOE and tissue level as well as timeframe for
RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017
 NOVEMBER 2017") RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017 Welcome to this training resource. It has been designed for all healthcare workers involved in coordinating SSI surveillance, SSI surveillance data
RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017 Welcome to this training resource. It has been designed for all healthcare workers involved in coordinating SSI surveillance, SSI surveillance data
APIC NHSN Webinar 9/8/2015. Topic Overview. Overall Learning Objectives
 APIC NHSN Webinar Janet Brooks, Cindy Gross, Denise Leaptrot, & Eileen Scalise Subject Matter Experts September 9, 2015 National Center for Emerging and Zoonotic Infectious Diseases Place Descriptor Here
APIC NHSN Webinar Janet Brooks, Cindy Gross, Denise Leaptrot, & Eileen Scalise Subject Matter Experts September 9, 2015 National Center for Emerging and Zoonotic Infectious Diseases Place Descriptor Here
Schematic of diagnosing surgical site infections
 Schematic of diagnosing surgical site infections Infection occurred within 30 days after an operation if no implant is in place within one year if an implant is in place eg. hip replacement Do NOT report
Schematic of diagnosing surgical site infections Infection occurred within 30 days after an operation if no implant is in place within one year if an implant is in place eg. hip replacement Do NOT report
Validation of HAI Reporting in New Hampshire Hospitals: Data from
 Validation of HAI Reporting in New Hampshire Hospitals: Data from 2014-15 Nancy Reinhalter, RN CCRC JSI Research & Training Institute, Inc. February 22, 2017 ACKNOWLEDGEMENTS JSI Team Priscilla Davis Paddy
Validation of HAI Reporting in New Hampshire Hospitals: Data from 2014-15 Nancy Reinhalter, RN CCRC JSI Research & Training Institute, Inc. February 22, 2017 ACKNOWLEDGEMENTS JSI Team Priscilla Davis Paddy
Form C KNHSS Operative Procedure Categories Codes
 Form C KNHSS Operative Procedure Categories Codes NHSN Operative Procedure Category Mappings to ICD-9-CM Codes and CPT Codes CPT codes are to be used for outpatient surgery cases only. KNHSS Code NHSN
Form C KNHSS Operative Procedure Categories Codes NHSN Operative Procedure Category Mappings to ICD-9-CM Codes and CPT Codes CPT codes are to be used for outpatient surgery cases only. KNHSS Code NHSN
NHSN and Public Reporting. Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_
 1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
AFL REVISION NOTICE. Please delete previous copies of this AFL and replace with the April 27, 2011 revised version.
 State of California Health and Human Services Agency California Department of Public Health HOWARD BACKER, MD, MPH Interim Director EDMUND G. BROWN JR. Governor AFL REVISION NOTICE Subject: Requirements
State of California Health and Human Services Agency California Department of Public Health HOWARD BACKER, MD, MPH Interim Director EDMUND G. BROWN JR. Governor AFL REVISION NOTICE Subject: Requirements
Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care
 National Quality Strategy Domain: Effective Clinical Care") Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Percentage
Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Percentage
Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition
 Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition") 1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
Surgical Site Infection (SSI) Reporting Through NHSN: Tips, Trips and Best Practices
 Reporting Through NHSN: Tips, Trips and Best Practices") Surgical Site Infection (SSI) Reporting Through NHSN: Tips, Trips and Best Practices Kathy Allen-Bridson RN, BSN, MScPH, CIC Nurse Consultant Division of Healthcare Quality Promotion Centers for Disease
Surgical Site Infection (SSI) Reporting Through NHSN: Tips, Trips and Best Practices Kathy Allen-Bridson RN, BSN, MScPH, CIC Nurse Consultant Division of Healthcare Quality Promotion Centers for Disease
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH
 National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
Basics of Epidemiology Answer Key
 Basics of Epidemiology Answer Key Pre-Quiz Question (slide 4) Q, A reservoir is the habitat where an infectious disease lives, multiplies and grows. Which of these could be a reservoir? A. Chronic carrier
Basics of Epidemiology Answer Key Pre-Quiz Question (slide 4) Q, A reservoir is the habitat where an infectious disease lives, multiplies and grows. Which of these could be a reservoir? A. Chronic carrier
Surveillance will occur in all inpatient locations in Kuwait Ministry of Health hospitals.
 Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] Non-Catheter-Associated Urinary Tract Infection [UTI]) Other Urinary System Infection [USI]) Events Settings: Surveillance will
Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CAUTI] Non-Catheter-Associated Urinary Tract Infection [UTI]) Other Urinary System Infection [USI]) Events Settings: Surveillance will
Surveillance and Surveillance Definitions NHSN. Jo Ellen Walton, BSN, RN, CIC
 Surveillance and Surveillance Definitions NHSN Jo Ellen Walton, BSN, RN, CIC Surveillance in Acute Care Facilities Central Line Associated Bloodstream Infections (CLABSIs) Catheter Associated Urinary Tract
Surveillance and Surveillance Definitions NHSN Jo Ellen Walton, BSN, RN, CIC Surveillance in Acute Care Facilities Central Line Associated Bloodstream Infections (CLABSIs) Catheter Associated Urinary Tract
Catheter Associated Urinary Tract Infection
 Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS
 NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
Infection Control: Surgical Site Infections
 Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
Catheter Associated Urinary Tract Infection
 Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
2016 National Healthcare Safety Network (NHSN) Definition Update. Peg Gilbert, RN, MS, CIC. Quality Improvement Advisor, Regional Lead.
 Definition Update. Peg Gilbert, RN, MS, CIC. Quality Improvement Advisor, Regional Lead.") 2016 National Healthcare Safety Network (NHSN) Definition Update Peg Gilbert, RN, MS, CIC Quality Improvement Advisor, Regional Lead Objectives Relate the changes in the NHSN surveillance definitions for
2016 National Healthcare Safety Network (NHSN) Definition Update Peg Gilbert, RN, MS, CIC Quality Improvement Advisor, Regional Lead Objectives Relate the changes in the NHSN surveillance definitions for
Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries)
 Surveillance Update (with special reference to Colorectal Surgeries)") Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries) Where we started and where we re going Anjum Khan MBBS MSc CIC Infection Control Professional Department
Surgical Site Infection (SSI) Surveillance Update (with special reference to Colorectal Surgeries) Where we started and where we re going Anjum Khan MBBS MSc CIC Infection Control Professional Department
Categorizing Wound Infections: A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database
 : A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database Luke V. Selby MD, Daniel D. Sjoberg MS, Danielle Cassella MA, Mindy Sovel MPH MS, David R. Jones MD, Vivian E. Strong
: A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database Luke V. Selby MD, Daniel D. Sjoberg MS, Danielle Cassella MA, Mindy Sovel MPH MS, David R. Jones MD, Vivian E. Strong
Prevention of CAUTI is discussed in the CDC/HICPAC document, Guideline for Prevention of Catheter-associated Urinary Tract Infection 4.
 Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
NHSN Catheter-Associated Urinary Tract Infection Surveillance in 2016
 NHSN Catheter-Associated Urinary Tract Infection Surveillance in 2016 Presented by: Susan Steeves MSN, RN, CNL, CIC June 28,2016 Taken from: NHSN Training 2016 March 3, 2016 Eileen Scalise, MSN, RN Nurse
NHSN Catheter-Associated Urinary Tract Infection Surveillance in 2016 Presented by: Susan Steeves MSN, RN, CNL, CIC June 28,2016 Taken from: NHSN Training 2016 March 3, 2016 Eileen Scalise, MSN, RN Nurse
Prevention of CAUTI is discussed in the CDC/HICPAC document, Guideline for Prevention of Catheter-associated Urinary Tract Infection.
 Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY
 Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY December 29, 2016 FINAL Working Group: Bonita Lee (Chair), Joanne Langley,
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY December 29, 2016 FINAL Working Group: Bonita Lee (Chair), Joanne Langley,
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI. CPT. Pasri Maharom MD, MPH Dec 15, 2015
 Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
BEST PRACTICES FOR SURGICAL SITE INFECTION (SSI) Janet Sullivan RN, BSN, CIC November 20, 2013
 Janet Sullivan RN, BSN, CIC November 20, 2013") BEST PRACTICES FOR SURGICAL SITE INFECTION (SSI) Janet Sullivan RN, BSN, CIC November 20, 2013 LEARNING OBJECTIVES Discuss the impact of SSIs on patient safety and the cost of healthcare Describe the CDC
BEST PRACTICES FOR SURGICAL SITE INFECTION (SSI) Janet Sullivan RN, BSN, CIC November 20, 2013 LEARNING OBJECTIVES Discuss the impact of SSIs on patient safety and the cost of healthcare Describe the CDC
Annex 4. Case definitions of infections
 Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
Arteriovenostomy for renal dialysis 39.27, 39.42
 Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Surgery categories NHSN Surgery codes (Reference: NHSN Operative Procedure Category Mappings to ICD-9-CM Codes, October 2010 www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf) Operative aortic aneurysm
Sustained CAUTI and CLABSI Improvements Using a Bundled Approach
 Sustained CAUTI and CLABSI Improvements Using a Bundled Approach Experiences of a Level 1 Trauma Center Angela Booth-Jones, PHD, MS, CIC Director, Infection Prevention 1 2 3 Miami Valley Hospital MVH has
Sustained CAUTI and CLABSI Improvements Using a Bundled Approach Experiences of a Level 1 Trauma Center Angela Booth-Jones, PHD, MS, CIC Director, Infection Prevention 1 2 3 Miami Valley Hospital MVH has
Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review
 Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review Disclosures The following individuals have no actual or potential conflicts of interest in relation to this
Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review Disclosures The following individuals have no actual or potential conflicts of interest in relation to this
Infection prevention in the OR: A close examination of interventions
 Infection prevention in the OR: A close examination of interventions Kim Delahanty BSN, PHN, MBA/HCM, CIC, FAPIC kboyntondelahanty@ucsd.edu 1 Objectives Describe the clinical and economic impact of SSIs
Infection prevention in the OR: A close examination of interventions Kim Delahanty BSN, PHN, MBA/HCM, CIC, FAPIC kboyntondelahanty@ucsd.edu 1 Objectives Describe the clinical and economic impact of SSIs
None of the authors has any disclosures or conflicts of interest to report
 None of the authors has any disclosures or conflicts of interest to report The Effect OF PATOS (Present At the Time Of Surgery) On The Calculation of SSI Rates for Appendectomy and Colectomy: Is PATOS
None of the authors has any disclosures or conflicts of interest to report The Effect OF PATOS (Present At the Time Of Surgery) On The Calculation of SSI Rates for Appendectomy and Colectomy: Is PATOS
Data Collection Help Sheet
 Global Outcomes in Surgery Collaboration GlobalSurg II: Determining the worldwide epidemiology of surgical site infections after gastrointestinal surgery Data Collection Help Sheet Introduction This document
Global Outcomes in Surgery Collaboration GlobalSurg II: Determining the worldwide epidemiology of surgical site infections after gastrointestinal surgery Data Collection Help Sheet Introduction This document
Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015
 Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015 Scenario 1: Postoperative SSI A 16 year-old patient Principal Operative Procedure: Incision and Drainage for monoarticular
Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015 Scenario 1: Postoperative SSI A 16 year-old patient Principal Operative Procedure: Incision and Drainage for monoarticular
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
CASE SCENARIO EXERCISE
 påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
Catheter-Associated Urinary Tract Infection () Event Introduction: Urinary tract infections (UTIs) are tied with pneumonia as the second most common type of healthcare-associated infection, second only
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Surveillance and Epidemiological Investigation
 Surveillance and Epidemiological Investigation Objectives The participant will be able to identify at least 4 types of data used for surveillance of infections. The participant will be able to define outbreak.
Surveillance and Epidemiological Investigation Objectives The participant will be able to identify at least 4 types of data used for surveillance of infections. The participant will be able to define outbreak.
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Process audit for SSI. CME on Infection Prevention & Control Breach Candy Hospital Trust
 Process audit for SSI CME on Infection Prevention & Control Breach Candy Hospital Trust Introduction SSIs are the most common healthcare-associated infection, accounting for 31% of all HAIs among hospitalized
Process audit for SSI CME on Infection Prevention & Control Breach Candy Hospital Trust Introduction SSIs are the most common healthcare-associated infection, accounting for 31% of all HAIs among hospitalized
Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection?
 ANNALS OF SURGERY Vol. 237, No. 3, 358 362 2003 Lippincott Williams & Wilkins, Inc. Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection? Chesley Richards,
ANNALS OF SURGERY Vol. 237, No. 3, 358 362 2003 Lippincott Williams & Wilkins, Inc. Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection? Chesley Richards,
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project
 Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement Indwelling Urinary Catheters Insertion,
Quality Improvement Updates Foley Discontinuation Protocol Surgical Care Improvement Project Barbara J Martin, RN, MBA Quality Consultant, Center for Clinical Improvement Indwelling Urinary Catheters Insertion,
Modifiable Risk Factors in Orthopaedic Infections
 Modifiable Risk Factors in Orthopaedic Infections AAOS Patient Safety Committee Burden US Surgical Site Infections (SSI) by the Numbers ~300,000 SSIs/yr (17% of all HAI; second to UTI) 2%-5% of patients
Modifiable Risk Factors in Orthopaedic Infections AAOS Patient Safety Committee Burden US Surgical Site Infections (SSI) by the Numbers ~300,000 SSIs/yr (17% of all HAI; second to UTI) 2%-5% of patients
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Tied with pneumonia as the second most common type of healthcareassociated
 Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
INFECTION PREVENTION AND CONTROL
 INFECTION PREVENTION AND CONTROL Health Care-Associated Infection (HAI) Definitions May 28, 2012 The Capital Health Infection Prevention Control (IPAC) department conducts ongoing surveillance reports
INFECTION PREVENTION AND CONTROL Health Care-Associated Infection (HAI) Definitions May 28, 2012 The Capital Health Infection Prevention Control (IPAC) department conducts ongoing surveillance reports
Presented by: Phenelle Segal, RN CIC President, Infection Control Consulting Services, LLC
 Catheter-associated Urinary Tract Infection (CAUTI) in Long-Term Care Settings Presented by: Phenelle Segal, RN CIC President, Infection Control Consulting Services, LLC Presenter has no financial disclosures
Catheter-associated Urinary Tract Infection (CAUTI) in Long-Term Care Settings Presented by: Phenelle Segal, RN CIC President, Infection Control Consulting Services, LLC Presenter has no financial disclosures
MBSAQIP Complex Clinical Scenarios & Variable Review
 MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida
 Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Surgical Site Infections: the international guidelines for best practices and effective actions
 Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Activity C: ELC Prevention Collaboratives
 Surgical Site Infection (SSI) Toolkit Activity C: ELC Prevention Collaboratives S.I. Berríos-Torres, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Draft - 12/21/09
Surgical Site Infection (SSI) Toolkit Activity C: ELC Prevention Collaboratives S.I. Berríos-Torres, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention Draft - 12/21/09
Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC
 Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC Tel: +973 172 80 8 50 Mobile: +973 343 58 323 Fax: +973 a 11446 Address: BMMI Tower, Office 1423, 14 th Floor,
Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC Tel: +973 172 80 8 50 Mobile: +973 343 58 323 Fax: +973 a 11446 Address: BMMI Tower, Office 1423, 14 th Floor,
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January December 2009
 Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2009 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Contents
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2009 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Contents
PREVENTING SURGICAL SITE INFECTIONS
 PREVENTING SURGICAL SITE INFECTIONS Surgical site infections (SSIs) are costly for the NHS and the patient increasing the length of hospital stay and the need for further treatment. This article examines
PREVENTING SURGICAL SITE INFECTIONS Surgical site infections (SSIs) are costly for the NHS and the patient increasing the length of hospital stay and the need for further treatment. This article examines
The Michigan Trauma Quality Improvement Program. Ann Arbor, MI June 7, 2011
 The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
Pediatric SC/SCR Education Session: Difficult Definitions. NSQIP Annual Meeting July 26, 2014
 Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
SSI. Ren yu Zhang MD
 Ren yu Zhang MD 3 27 2014 1 SSI 16 million operative procedures in 2010. Overall SSI rate 1.9% for 2006 8. Accounts 31% of healthcare associated infection. Leads to further morbidity and mortality. Economic
Ren yu Zhang MD 3 27 2014 1 SSI 16 million operative procedures in 2010. Overall SSI rate 1.9% for 2006 8. Accounts 31% of healthcare associated infection. Leads to further morbidity and mortality. Economic
Chapter 14 8/23/2016. Surgical Wound Care. Wound Classifications. Wound Healing. Classified According to. Phases
 Chapter 14 Surgical Wound Care All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Wound Classifications Classified According to Cause Incision
Chapter 14 Surgical Wound Care All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Wound Classifications Classified According to Cause Incision
Healthcare-associated infections and antimicrobial use in European long-term care facilities (HALT-3) RESIDENT QUESTIONNAIRE
 RESIDENT QUESTIONNAIRE") Healthcare-associated infections and antimicrobial use in European long-term care facilities (HALT-3) RESIDENT QUESTIONNAIRE RESIDENT DATA GENDER Male Female BIRTH YEAR (YYYY) LENGTH OF STAY IN THE FACILITY
Healthcare-associated infections and antimicrobial use in European long-term care facilities (HALT-3) RESIDENT QUESTIONNAIRE RESIDENT DATA GENDER Male Female BIRTH YEAR (YYYY) LENGTH OF STAY IN THE FACILITY
CDC/NHSN Surveillance Definitions for Specific Types of Infections
 CDC/NHSN Surveillance Definitions for Specific Types of Infections INTRODUCTION This chapter contains the CDC/NHSN surveillance definitions and criteria for all specific types of infections. This chapter
CDC/NHSN Surveillance Definitions for Specific Types of Infections INTRODUCTION This chapter contains the CDC/NHSN surveillance definitions and criteria for all specific types of infections. This chapter
HAAD JAWDA Quality Performance monthly KPI Profile (specialized and general hospitals)
") HAAD JAWDA Quality Performance monthly KPI Profile (specialized and general hospitals) June 2017 Page 1 of 159 Executive Summary The Health Authority Abu Dhabi (HAAD) is the regulative body of the Healthcare
HAAD JAWDA Quality Performance monthly KPI Profile (specialized and general hospitals) June 2017 Page 1 of 159 Executive Summary The Health Authority Abu Dhabi (HAAD) is the regulative body of the Healthcare
Sébastien LUSTIG MD, PhD, Prof *,** Tristan Ferry ** Frederic Laurent ** *Albert Trillat Center- Lyon, **CRIOA Lyon
 SICOT Meeting Roma September 2016 Risk factors of periprosthetic infection and my experience of how to prevent an infection Sébastien LUSTIG MD, PhD, Prof *,** Tristan Ferry ** Frederic Laurent ** *Albert
SICOT Meeting Roma September 2016 Risk factors of periprosthetic infection and my experience of how to prevent an infection Sébastien LUSTIG MD, PhD, Prof *,** Tristan Ferry ** Frederic Laurent ** *Albert
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Measure #165 (NQF 0130): Coronary Artery Bypass Graft (CABG): Deep Sternal Wound Infection Rate National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #165 (NQF 0130): Coronary Artery Bypass Graft (CABG): Deep Sternal Wound Infection Rate National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Overview of the WHO global guidelines for the prevention of surgical site infection
 Overview of the WHO global guidelines for the prevention of surgical site infection Dr. Mohamed Abbas, MD, MS Semmelweiss CEE Conference Budapest 08.03.2017 Outline of presentation General background Burden
Overview of the WHO global guidelines for the prevention of surgical site infection Dr. Mohamed Abbas, MD, MS Semmelweiss CEE Conference Budapest 08.03.2017 Outline of presentation General background Burden
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida
 Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Presentation at ACS NSQIP National Conference in July Surgical Site Infection Reduction Strategies
 Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Appendicitis. Diagnosis and Surgery
 Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
2018 CNISP HAI Surveillance Case definitions
 2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
Tennessee s Tenth Report on Healthcare-Associated Infections: Overview of Report, Methodology, and Format
 Tennessee s Tenth Report on Healthcare-Associated Infections: Overview of Report, Methodology, and Format TDH HAI Team September 3, 2015 Acknowledgements THA/TCPS for hosting this webinar TDH HAI Team
Tennessee s Tenth Report on Healthcare-Associated Infections: Overview of Report, Methodology, and Format TDH HAI Team September 3, 2015 Acknowledgements THA/TCPS for hosting this webinar TDH HAI Team
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Infection Control: Meeting the Challenge
 22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
Appendix G Explanation/Clarification Summary
 Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
Appendix G Explanation/Clarification Summary Summary of Changes for Recommendations Alignment of measures with VBP by fiscal year Measures and service dates were adjusted to be consistent with the FY2016
AHRQ Safety Program for Long-term Care: HAIs/CAUTI. Catheter Associated Urinary Tract Infection (CAUTI) Definitions and Reporting
 Definitions and Reporting") AHRQ Safety Program for Long-term Care: HAIs/CAUTI Catheter Associated Urinary Tract Infection (CAUTI) Definitions and Reporting Onboarding Webinar #2 for LTC Facility Team Leads and Core Team August 13,
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Catheter Associated Urinary Tract Infection (CAUTI) Definitions and Reporting Onboarding Webinar #2 for LTC Facility Team Leads and Core Team August 13,
Medical Coding Exam System - Week 1 Day 2 Practice Exam Questions 1-25
 1 Medical Coding Exam System - Week 1 Day 2 Practice Exam Questions 1-25 1. A man suffered a severe crushing injury to his left upper leg. Two days after surgery, the doctor completed a dressing change
1 Medical Coding Exam System - Week 1 Day 2 Practice Exam Questions 1-25 1. A man suffered a severe crushing injury to his left upper leg. Two days after surgery, the doctor completed a dressing change
Preventing Surgical Site Infections: The SSI Bundle
 Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies
 Surveillance Definitions Case Studies") LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies PRIMARY BSI Primary bloodstream infections (BSI) Organism cultured from the blood that is not related to an infection
LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies PRIMARY BSI Primary bloodstream infections (BSI) Organism cultured from the blood that is not related to an infection
Supplementary Online Content
 Supplementary Online Content Bhangu A, Singh P, Lundy J, Bowley DM. Systemic review and meta-analysis of randomized clinical trials comparing primary vs delayed primary skin closure in contaminated and
Supplementary Online Content Bhangu A, Singh P, Lundy J, Bowley DM. Systemic review and meta-analysis of randomized clinical trials comparing primary vs delayed primary skin closure in contaminated and
January 2015 Updates. Dec.4, 2014 SCR Education Call
 January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
Sample page. Anesthesia. Cross Coder. Essential links from CPT codes to ICD-10-CM and HCPCS
 Cross Coder 2018 Anesthesia Essential links from CPT codes to ICD-10-CM and HCPCS POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents Introduction...i
Cross Coder 2018 Anesthesia Essential links from CPT codes to ICD-10-CM and HCPCS POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years. Visit optum360coding.com. Contents Introduction...i
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January December 2010
 Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2010 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Table of
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2010 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Table of
LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies
 Surveillance Definitions Case Studies") LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies PRIMARY BSI Primary bloodstream infections (BSI) Organism cultured from the blood that is not related to an infection
LABORATORY CONFIRMED BLOODSTREAM INFECTIONS (LCBI) Surveillance Definitions Case Studies PRIMARY BSI Primary bloodstream infections (BSI) Organism cultured from the blood that is not related to an infection
Variable Updates January 2014
 Variable Updates January 2014 Surgeon National Provider Identifier (NPI) Variable Name: Surgeon NPI Intent of Variable: For sites to have the ability to track each surgeon s surgical cases. Definition:
Variable Updates January 2014 Surgeon National Provider Identifier (NPI) Variable Name: Surgeon NPI Intent of Variable: For sites to have the ability to track each surgeon s surgical cases. Definition:
Key Definitions. Downloaded from
 Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Surgical site infections
 SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Surgical site infections Key facts Surgical site infections (SSIs) are among the most common healthcare-associated infections (HAIs). They are
SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Surgical site infections Key facts Surgical site infections (SSIs) are among the most common healthcare-associated infections (HAIs). They are
Performance Measure. Inpatient Clinical Process of Care Measures
 Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
Acute Myocardial Infarction (AMI) 's Maryland Hospital Performance Evaluation System: Inpatient s Quality Based Reimbursement () Measures Highlighted in Green (02/27/2014) Inpatient Clinical Process of
HAIs in the USA. March 23, 2017 Department of Public Health Sciences. Infectious Disease Epidemiology BMTRY 713 (Healthcare Associated Infection )
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 17 Healthcare-Associated Infections (HAIs) Learning Objectives 1. Describe magnitude and implication of HAIs 2. Identify the main risk
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 17 Healthcare-Associated Infections (HAIs) Learning Objectives 1. Describe magnitude and implication of HAIs 2. Identify the main risk
FOOT AND ANKLE ARTHROSCOPY
 FOOT AND ANKLE ARTHROSCOPY Information for Patients WHAT IS FOOT AND ANKLE ARTHROSCOPY? The foot and the ankle are crucial for human movement. The balanced action of many bones, joints, muscles and tendons
FOOT AND ANKLE ARTHROSCOPY Information for Patients WHAT IS FOOT AND ANKLE ARTHROSCOPY? The foot and the ankle are crucial for human movement. The balanced action of many bones, joints, muscles and tendons
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
DEPARTMENT NAME GASTROSTOMY CARE AND MANAGEMENT
 GASTROSTOMY CARE AND MANAGEMENT Texas Children s Hospital Advanced Practice Provider Conference Pediatric Surgery April 4 th, 2019 Madison Fitzgerald PA-C, Celia Flores PA-C OBJECTIVES 1. Identify the
GASTROSTOMY CARE AND MANAGEMENT Texas Children s Hospital Advanced Practice Provider Conference Pediatric Surgery April 4 th, 2019 Madison Fitzgerald PA-C, Celia Flores PA-C OBJECTIVES 1. Identify the
South West Regional Wound Care Toolkit F. PRINCIPLES OF TREATMENT BASED ON ETIOLOGY (TREAT THE CAUSE)
") F. PRINCIPLES OF TREATMENT BASED ON ETIOLOGY (TREAT THE CAUSE) F.5 SURGICAL WOUND (CLOSED AND OPEN) 5.1 Background to Etiology Closed surgical wounds are well-approximated with a palpable healing ridge
F. PRINCIPLES OF TREATMENT BASED ON ETIOLOGY (TREAT THE CAUSE) F.5 SURGICAL WOUND (CLOSED AND OPEN) 5.1 Background to Etiology Closed surgical wounds are well-approximated with a palpable healing ridge