Focus on Upper Gastrointestinal Problems
|
|
|
- Gillian Bryant
- 5 years ago
- Views:
Transcription
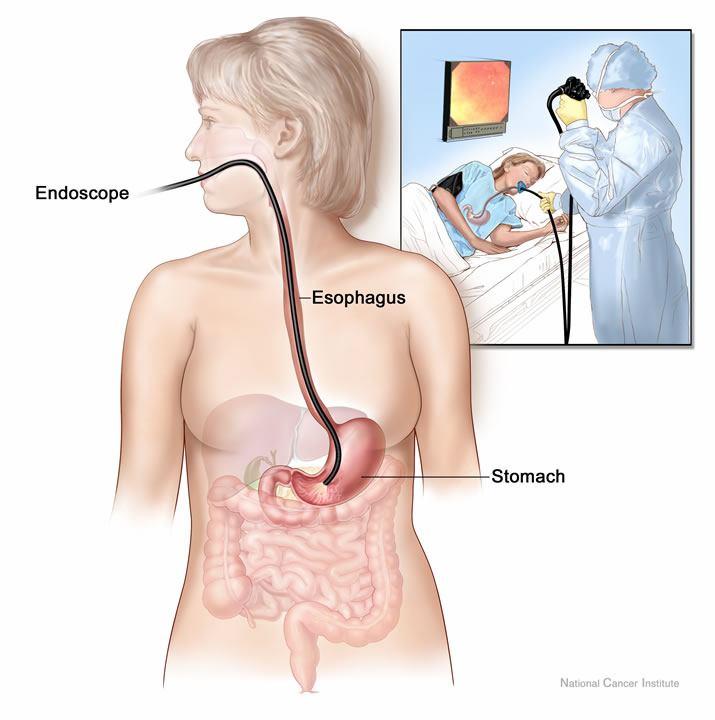
1 Focus on Upper Gastrointestinal Problems Chapter 42, Nursing Management: Upper Gastrointestinal Problems Revised for Voice Thread Nursing 246 Gastroesophageal Reflux Disease GERD (a syndrome if with tissue damage) Reflux of gastric secretions into esophagus. Predisposing conditions: Results in: - irritation pyrosis (heartburn) - inflammation - esophogitis, - difficulty swallowing dysphagia GERD Etiology and Pathophysiology Fig
2 GERD-Diagnosis Barium swallow Upper GI Esophageal endoscopy X-Ray Contrast and Nuclear Medicine Studies Barium Swallow UGI Series Barium Swallow Outlines the esophagus Contrast is INGESTED Barium Gastrografin (water soluble contrast) 2


3 Upper GI Series Esophagus, stomach, duodenum Also uses barium sulfate milkshake If air contrast is desired patient will also ingest some carbonated powder Exam usually 30 Longer if waits to see small bowel 3

4 4
, proton pump inhibitors (Protonix, Nexium), prokinetic meds (metaclopromide) Hiatal Hernia bulging upwards of a portion of stomach through diaphragmatic opening Acid from stomach spills into")
5 Patient Education (GERD) Lifestyle changes time of meals, clothing, smoking Dietary changes fat, alcohol, spices, chocolate, caffeine Medications- antacids (maalox, tums), H2 blockers (Tagamet, Pepcid), proton pump inhibitors (Protonix, Nexium), prokinetic meds (metaclopromide) Hiatal Hernia bulging upwards of a portion of stomach through diaphragmatic opening Acid from stomach spills into esophagus 5


6 Surgical Therapy (Hiatal Hernia) Objective is to reduce reflux by enhancing integrity of LES LES = Procedure: fundoplication Can be preformed via laparoscope Prevents reflux in 90% of patients. Relapse common 6

7 Peptic Ulcer Disease Ulceration occurs mostly in: Antrum (lesser curvature) Duodenum Mucosal Defensive System is impaired MUCUS BICARBONATE SUFFICIENT BLOOD FLOW PROSTAGLANDINS More Physiology of PUD Ulcer will not form in absence of acid Rarely gastric acid alone causes There must be something else disrupting the mucosa H. pylori Inadequate blood flow Smoking NSAIDs H. pylori is a gram-negative, microoerophilic, spiral bacillus originally cultured in 1982 from gastric biopsy specimens in patients with documented gastritis. 7



8 Dr. Marshall's stomach biopsy taken 8 days after he drank a culture of H. pylori Even shallow ulcers can erode near a blood vessel and cause an acute upper GI hemorrhage 8

9 Duodenal ulcer of the posterior wall penetrating into the head of the pancreas resulting in walled-off perforation. H. Pylori Helicobacter pylori bacterium Promotes peptic ulcer formation Treatment: triple therapy More Physiology of PUD Ulcer will not form in absence of acid BUT rarely gastric acid alone causes There must be something else disrupting the mucosa H. pylori Inadequate blood flow Smoking NSAIDs 9
 Replaces endogenous prostaglandins PPI 10")
10 Stress Ulcers Erosive gastritis caused by transient GI ischemia (low blood supply) - shock, burns, surgery imbalance of acid and mucus barrier Prevention: prophylactic meds: Antacids, H2 blockers, PPIs How to Treat For Specific Causes of PUD H. pylori Antibiotics and acid suppression NSAIDS Avoid If must use Cytotec (Misoprostel) Replaces endogenous prostaglandins PPI 10
 Usually once a day Prilosec, Prevacid, Protonix, Aciphex Nexium + Protonix= PO, IV form Prilosec not indicated for")
11 Systemic Acid Blockers Histamine 2 Take any time of day with no food restrictions Usually twice daily Zantac, Tagamet, Pepcid = IV and PO Tagamet = oldest one and lots of drug interactions not for elderly Axid = PO only Proton Pump Inhibitors Take in AM before breakfast (30 ) Usually once a day Prilosec, Prevacid, Protonix, Aciphex Nexium + Protonix= PO, IV form Prilosec not indicated for those on Coumadin Complications of Chronic Ulcer Disease Hemorrhage more common with duodenal ulcers Perforation most lethal complication (PERITONITIS) Gastric outlet obstruction-scaring scaring and atrophy of pylorus. 11
 What is it the vagus nerves does to the stomach?")
12 Surgical Interventions (Cancer or Ulcer Disease) Procedures: gastrectomy: billroth I or II Partial or total resection of stomach vagotomy: cutting vagus nerve to decrease gastric acid secretion pyloroplasty: pyloric dilatation For ulcer disease, all are rarely performed now Question(s) What is it the vagus nerves does to the stomach? Hint: Vagal stimulation occurs with the sight and smell of food 12

13 Total gastrectomy for stomach cancer (total gastrectomy with esophagojejunostomy) Nursing interventions Post-Op Care If NG tube present, maintain patency *do not reinsert if it comes out!! LOCATION LOCATION LOCATION! Patient may have abdominal incision(s) AND chest tube(s) Teaching about dietary needs is ongoing throughout post-op op time Continues to discharge Peptic Ulcer Disease Surgical Therapy for PUD Postoperative care NG Tube Aspirate observed for Color Bright red at first with darkening within first 24 hours Color changes yellow-green within 36 to 48 hours Amount Odor 13
14 Peptic Ulcer Disease Surgical Therapy for PUD Postoperative care (cont d) NG suction must be in working order and patency maintained Observe for signs of peristalsis and lower abdominal discomfort Intestinal obstruction Peptic Ulcer Disease Surgical Therapy for PUD Postop care (cont d) Accurate I/O essential Vital signs every 4 hours Frequent position changes IV therapy Observe for signs of infection Long-term complication pernicious pernicious anemia Dumping Syndrome Cause is reduced gastric capacity Symptoms occur min. after a meal, feelings of weakness, sweating, palpitations, dizziness Due to large bolus of hypertonic fluid entering intestine and fluid is drawn into the bowel, causes distention of bowel. Advise patient to lie down, it will pass. 14
15 Dietary Measures 6 small feedings per day Avoid fluids with meals minutes before or after Avoid concentrated sweets High protein diet and include some fat with each meal Nutritional Interventions Eliminate drinking fluids with meals Dry foods with low carbohydrate content (avoid high sugar diet) Rest after meals Focus on Nausea and Vomiting Chapter 42, Nursing Management: Upper Gastrointestinal Problems revised 15
16 Nausea and Vomiting Most common manifestations of GI diseases Nausea and Vomiting Etiology and Pathophysiology Occurs from GI disorders Pregnancy Infectious diseases CNS disorders Cardiovascular problems Metabolic disorders Side effects of drugs Psychologic factors Nausea and Vomiting Etiology and Pathophysiology Vomiting also can occur when the GI tract becomes irritated, excited, or distended Vomiting can be a protective mechanism 16
17 Nausea and Vomiting Clinical Manifestations Nausea Subjective complaint Usually accompanied by anorexia Vomiting Dehydration can rapidly occur when prolonged Water and essential electrolytes are lost Nausea and Vomiting Clinical Manifestations Metabolic alkalosis from loss of gastric HCl Metabolic acidosis from loss of bicarbonate if the contents from the small intestine are vomited Nausea and Vomiting Collaborative Care Fecal odor and bile indicates a lower obstruction Color of emesis aids in determining presence and source, if bleeding Time of day occurring 17
18 Nausea and Vomiting Collaborative Care Nondrug therapy Acupuncture Acupressure Botanicals Ginger Peppermint oil Breathing exercises Nausea and Vomiting Collaborative Care Nutritional therapy IV fluids to replace fluid and electrolytes, glucose NG tube suction to decompress stomach Nausea and Vomiting Collaborative Care Nutritional therapy (cont d) Clear liquids started first 5 to 15 ml fluid every 15 to 20 minutes No extremely hot/cold liquids Room-temp carbonated beverages without carbonation okay Warm tea May advance to dry toast, crackers 18
19 Nausea and Vomiting Collaborative Care Use Gatorade, broth with caution because of Advance to high carbohydrates, low fat next since easier to digest Baked potato, plain gelatin, cereal with milk Eat slowly and in small amounts Nausea and Vomiting Collaborative Care Nutritional therapy (cont d) Fluids between meals instead of with meals to avoid overdistention Dietitian may be helpful with appropriate food with adequate nutritional value Nursing Management Nursing Diagnoses Nausea Deficient fluid volume Imbalanced nutrition: Less than body requirements 19
20 Nursing Management Gerontologic Considerations More likely to have cardiac or renal insufficiency Increased risk for life-threatening fluid/electrolyte imbalances Increased susceptibility to CNS side effects of antiemetic drugs Nursing Management Gerontologic Considerations Caution with fluid replacement in patients with HF Alteration in LOC greater risk for aspiration Anti-Emetics Prokinetic Serotonin Receptor Agonists Dopamine Antagonists Glucocorticoids Cannabinoids Benzodiazepines Motion Sickness Drugs 20

21 Key Points AntiEmetics It s s easier to prevent nausea than treat it! Give prophylactically! Most cause sedation Special precaution during pregnancy Thalidomide tragedy 1957 to 1962 in UK, Canada, Germany, Japan - not FDA approved prevented morning sickness 12,000 babies who survived, with phocomelia (flipper-like arms or legs) Prokinetic Drug - Reglan AKA Metoclopramide Dopamine and serotonin receptor blocker BUT also increases UPPER GI motility Used for post-op op Nausea/Vomiting Limitation = sedation Good for diabetic gastroparesis Since has serotonin effects see next slides regarding extrapyramidal side effects 21
22 Serotonin Receptor Agonists Basically these three EXPENSIVE Drugs Zofran Kytril Anzemet Used for: CINV Chemotherapy Induced N/V Helps with induction of anesthesia Dopamine Antagonists also famous for Extrapyramidal Phenothiazines Phenergan (prochlorperazine) Compazine Thorazine Butyrophenones Haldol (haloperidol) Inapsine (droperidol) Extrapyramidal Reactions Repetitive Movements Oral-buccal buccal-lingual lingual (Tardive Dyskinesia) Limb, neck, and trunk (Parkinsonian-like) Can occur within the 1 st few days or not for weeks Or appear months and years after use Also associated with the antipsychotics 22



23 ANOTHER OF MODERN MEDICINE S HORROR STORIES: TARDIVE DYSKINESIA IV Phenergan Induced Promethazine IV, IM Can be highly caustic to the lining of blood vessels and surrounding tissue IV use has the highest risk of severe tissue damage Use at lower doses (6.25 to 12.5 mg) Are really just as effective Dilute with 10 ml Normal Saline 23

24 Glucocorticoids SoluMedrol Decadron Useful to prevent post-op op nausea and vomiting Given prior to induction of anesthesia Cannabinoids Marinol Can cause subjective effects similar to those caused by smoking marijuana However Slow onset Did not generate much street interest 24

25 Benzodiazepines Ativan Is really the only one useful for N/V More Specific for Motion Sickness Scopolamine patch Apply evening before surgery or 4 hours before the end of surgery Antihistamines Dramamine Antivert All can cause the triad of: blurred, dry, urinary /constipation the patch should be kept in place for 24 hours following surgery at which time it should be removed and discarded. 25


26 Emesis Basins Most Important Not To Be Without 150,000 to 200,000 hospital admissions each year for UGI bleeding Mortality rate 6% to 10% for past 40 years Increased incidence of UGI bleeding in older adults, especially women, and use of NSAIDs 26
27 Etiology and Pathophysiology Types of UGI bleeding Obvious bleeding Hematemesis Bloody vomitus» Appears fresh, bright red blood or coffee grounds Melena Black, tarry stools» Caused by digestion of blood in GI tract» Black appearance iron Etiology and Pathophysiology Types of UGI bleeding (cont d) Occult bleeding Small amounts of blood in gastric secretions, vomitus, or stools Undetectable by appearance Detectable by guaiac test Etiology and Pathophysiology Bleeding from arterial source profuse bright red The bright red color = blood has not been in contact with the stomach s s acid secretions 27
28 Etiology and Pathophysiology Coffee ground vomitus reveals that the blood has been in the stomach for some time and has been changed by gastric secretions Melena: Slow bleeding from an upper GI source Etiology and Pathophysiology Longer the passage of blood through intestines, the darker the stool color due to breakdown of Hb release of iron Cause of bleeding is not always easy Variety of areas in GI tract may be involved Common Causes of UGI Bleeding Esophageal origin Stomach and duodenal origin Drug-induced origin Systemic disease origin 28

29 Common Causes of Bleeding Esophageal Origin Chronic esophagitis GERD Mucosa-irritating drugs Alcohol Cigarettes Common Causes of Bleeding Esophageal Origin Mallory-Weiss tear Tear in mucosa near esophagogastric junction Related to severe retching/vomiting Linear and longitudinal tears in the esophagus at the EG junction Are believed to be the consequence of severe retching... Mallory Weiss tear at the Gastroesophageal Junction GEJ Are encountered most commonly in alcoholics, attributed to episodes of excessive vomiting and reflux of gastric contents in the setting of an alcoholic stupor... 29



 may cause")
30 Common Causes of Bleeding Esophageal Origin Esophageal varices Usually occurs secondary to cirrhosis of liver due to high pressure secondary to portal hypertension Anything that increases pressure (, ) or causes irritation ( ) may cause massive bleeding 30
31 Common Causes of Bleeding Stomach and Duodenal Origin Gastric cancer Steady blood loss as it grows and ulcerates Hemorrhagic gastritis Peptic ulcer disease Bleeding ulcers account for 50% of UGI bleeding cases Related to H. pylori or drug use (NSAIDs) Common Causes of Bleeding Stomach and Duodenal Origin Polyps Stress-related related mucosal disease 31

32 Peptic Ulcers Fig Common Causes of Bleeding Drug-Induced Origin OTC or prescribed drugs: Major cause of UGI bleeding Irritate and disrupt gastric mucosal barrier Aspirin Excedrin Alka-Seltzer NSAIDs Ibuprofen Corticosteroids Careful history of all commonly used drugs required Emergency Assessment & Management 80% to 85% of patients who have massive hemorrhage spontaneously stop bleeding Cause still must be identified and treatment initiated 32
33 Emergency Assessment & Management Immediate physical examination with emphasis on BP Rate and character of pulse Peripheral perfusion with capillary refill Observation of neck vein distention Emergency Assessment & Management VS every 15 to 30 minutes Signs and symptoms of shock evaluated Abdominal exam Tense, rigid abdomen may indicate perforation and peritonitis Emergency Assessment & Management Once immediate interventions have started Complete history of events leading to bleeding episode Previous bleeding episodes Weight loss Received blood transfusion Other illnesses (liver disease, cirrhosis) Medication use Religious preferences regarding blood or blood product usage 33
34 Emergency Assessment & Management Laboratory studies Emergency Assessment & Management Laboratory tests (cont d) Liver enzymes ABGs Type/cross-match for possible blood transfusions Emergency Assessment & Management Other laboratory studies Vomitus/stools Tested for the presence of gross and occult blood Urinalysis Specific gravity: Indication of the patient s hydration status 34
35 Emergency Assessment & Management Fluid replacement IV lines Should be established for fluid and blood replacement Preferably two IVs 16 or 18 gauge Generally best to begin with an isotonic crystalloid solution (lactated Ringer s solution) Emergency Assessment & Management Blood replacement Whole blood, packed RBCs and fresh frozen plasma Used for replacement of lost volume in massive hemorrhage Packed RBC are preferred over whole blood because of fluid overload and immune reactions Emergency Assessment & Management Blood replacement (cont d) Hb and Hct provide baseline for further treatment Initial Hct may be normal and not reflect loss until 4 to 6 hours after fluid replacement Initially loss of plasma and RBC is equal 35
36 Emergency Assessment & Management Use of supplemental oxygen may help increase blood oxygen saturation Indwelling urinary catheter Accurate urine volume assessment Central venous pressure line to monitor patient s s fluid volume status Diagnostic Studies Endoscopy Primary tool for diagnosing source of bleeding Before performing May need to lavage for clearer view NG or orogastric tube placed and room- temperature water or saline used Never advance orogastric tube against resistance!! Aspiration of stomach contents through a large-bore tube (Ewald tube) to remove clots Diagnostic Studies Angiography Used to diagnose only when endoscopy cannot be done Invasive procedure May not be appropriate for high-risk or unstable patient 36
 probe Electrocoagulation probe Argon plasma coagulation (APC) Neodymium yttrium-aluminum aluminum-garnet (Nd-YAG) laser")
37 Collaborative Care Endoscopic hemostasis therapy Goal: To coagulate or thrombose bleeding artery Useful for gastritis, Mallory-Weiss tear, esophageal and gastric varices, bleeding peptic ulcers, and polyps Collaborative Care Several techniques are used including Thermal (heat) probe Electrocoagulation probe Argon plasma coagulation (APC) Neodymium yttrium-aluminum aluminum-garnet (Nd-YAG) laser common and very effective treatment but its effect is transient 37


38 Clip intact, without bleeding Collaborative Care Surgical therapy Indicated when bleeding continues Regardless of therapy provided Site of bleeding identified 38
39 Collaborative Care Surgical therapy (cont d) Site of hemorrhage determines choice of operation Surgeon must consider age of patient Collaborative Care Drug therapy During acute phase used to Bleeding HCl acid secretion Neutralize HCl acid that is present Collaborative Care Drug therapy (cont d) Injection therapy during endoscopy for acute hemostasis Bleeding due to ulceration Epinephrine 39
40 Collaborative Care Drug therapy (cont d) IV or intraarterial vasopressin (Pitressin) For variceal bleeding Somatostatin analog octreotide (Sandostatin) Used with upper GI bleeding Collaborative Care Drug therapy (cont d) Acid reducers Acidic environment can alter platelet function and clot stabilization Histamine-2 2 receptor blockers (H 2 R) PPIs Antacids Neutralize HCl acid Maintains gastric ph above 5.5 Nursing Management Signs/symptoms of shock Low BP Rapid, weak pulse Increased thirst Cold, clammy skin Restlessness 40
41 Peptic Ulcer Disease Surgical Therapy for PUD Preoperative care Laparoscopic or open surgery techniques Surgeon should educate family/patient on surgical procedure Nurse can clarify questions Peptic Ulcer Disease Surgical Therapy for PUD Preoperative care (cont d) Instructions should be given on Comfort measures Pain relief Coughing and deep breathing NG tube IV fluids Peptic Ulcer Disease Surgical Therapy for PUD Postoperative care Similar to postop care after abdominal laparotomy NG tube used to decompress and decrease pressure on suture line 41
42 Peptic Ulcer Disease Surgical Therapy for PUD Postoperative care (cont d) Aspirate observed for Color Bright red at first with darkening within first 24 hours Color changes yellow-green within 36 to 48 hours Amount Odor NG suction must be in working order and patency maintained Peptic Ulcer Disease Surgical Therapy for PUD Postoperative care (cont d) Observe for signs of peristalsis and lower abdominal discomfort Intestinal obstruction Peptic Ulcer Disease Surgical Therapy for PUD Postop care (cont d) Accurate I/O essential Vital signs every 4 hours Frequent position changes IV therapy Observe for signs of infection Long-term complication pernicious pernicious anemia 42

43 QUESTION(s) Your patient has been admitted with acute UGI bleeding She weighs 320 pounds A foley has been placed in the ER What would be the minimum hourly urine output you would expect to indicate adequate renal perfusion? 43
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
UPPER GI DISEASES 11/15/2014. Lesson Objectives. GI Tract Review. NUTR 2050 Nutrition for Nursing Professionals. Mrs. Deborah A. Hutcheon, MS, RD, LD
 UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Heartburn, also referred to acid reflux, happens when stomach acid flows back (refluxes) into your esophagus.
 into your esophagus.") WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Pharmacology. Drugs that Affect the Gastrointestinal System
 Pharmacology Drugs that Affect the Gastrointestinal System Topics Peptic Ulcer Disease Constipation Diarrhea Emesis Digestion Peptic Ulcer Disease Factors that Increase Acidity Factors that Protect Against
Pharmacology Drugs that Affect the Gastrointestinal System Topics Peptic Ulcer Disease Constipation Diarrhea Emesis Digestion Peptic Ulcer Disease Factors that Increase Acidity Factors that Protect Against
GERD. Gastroesophageal reflux disease, or GERD, occurs when acid from the. stomach backs up into the esophagus. Normally, food travels from the
 GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
Heartburn Overview. Causes & Risk Factors
 Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
DYSPEPSIA Dyspepsia indigestion during or after eating Full Heat, burning or pain Note: one of every four people
 What Is Dyspepsia? Dyspepsia, also known as indigestion, can have multiple symptoms. Feelings of indigestion happen during or after eating. If you have indigestion you might feel: Full during a meal. Painful
What Is Dyspepsia? Dyspepsia, also known as indigestion, can have multiple symptoms. Feelings of indigestion happen during or after eating. If you have indigestion you might feel: Full during a meal. Painful
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
GI -A & P Review PUD. Peptic Ulcer Disease (PUD) Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer
 Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer") GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
GI -A & P Review Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas 8/11/2011
 Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
Lemone and Burke Chapters 21,23-25 ATI M/S Unit 7 Objectives Review A&P Identify diagnostic exams Discuss etiology, pathophysiology, clinical manifestation, and collaborative management of: PUD Hernias
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
 Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
Page 1 of 5 Official reprint from UpToDate www.uptodate.com 2017 UpToDate Patient education: Acid reflux (gastroesophageal reflux disease) in adults (The Basics) Written by the doctors and editors at UpToDate
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Epidemiology of Peptic Ulcer Disease
 Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Symptom Management. Thomas McKain, MD, ABFM, ABHPM Medical Director
 Symptom Management Nausea & Vomiting Thomas McKain, MD, ABFM, ABHPM Medical Director Mr. Jones has nausea and vomiting. May I initiate Compazine from the Comfort Pak? Objectives 1. Delineate the Differential
Symptom Management Nausea & Vomiting Thomas McKain, MD, ABFM, ABHPM Medical Director Mr. Jones has nausea and vomiting. May I initiate Compazine from the Comfort Pak? Objectives 1. Delineate the Differential
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
The usual dose is 40 mg daily with amoxycillin 1.5 g (750 mg b.d.) for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.
 for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.") Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
ANATOMY AND PHYSIOLOGY
 ANATOMY AND PHYSIOLOGY Functions of the gastrointestinal (GI) system: * Process food substances * Absorb the products of digestion into the blood * Excrete unabsorbed materials * Provide an environment
ANATOMY AND PHYSIOLOGY Functions of the gastrointestinal (GI) system: * Process food substances * Absorb the products of digestion into the blood * Excrete unabsorbed materials * Provide an environment
The Aging Digestive System
 The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)?
?") WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
Gastro Esophageal Reflux Disease
 CHAPTER 1 Gastro Esophageal Reflux Disease M.ASHOKKUMAR DEPT OF PHARMACY PRACTICE SRM COLLEGE OF PHARMACY SRM UNIVERSITY ** Click on the arrow at the bottom right to move forward ** ** The arrow at the
CHAPTER 1 Gastro Esophageal Reflux Disease M.ASHOKKUMAR DEPT OF PHARMACY PRACTICE SRM COLLEGE OF PHARMACY SRM UNIVERSITY ** Click on the arrow at the bottom right to move forward ** ** The arrow at the
Upper Gastrointestinal (GI) Tract X-ray (Radiography)
 Tract X-ray (Radiography)") Upper Gastrointestinal (GI) Tract X-ray (Radiography) What is Upper Gastrointestinal (GI) Tract Radiography? What are some common uses of the procedure? How should I prepare? What does the equipment look
Upper Gastrointestinal (GI) Tract X-ray (Radiography) What is Upper Gastrointestinal (GI) Tract Radiography? What are some common uses of the procedure? How should I prepare? What does the equipment look
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Copy right protected Page 1
 DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
DRUGS USED IN ULCERS AND GIT DISORDERS A peptic ulcer, also known as PUD or peptic ulcer disease is an ulcer of an area of the gastrointestinal tract that is usually acidic and thus extremely painful.
Perforated peptic ulcers. Dr V. Roudnitsky KCH
 Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
Gastroesophageal Reflux Disease (GERD) Information for patients UHN Read this handout to learn about: What gastroesohageal reflux (GERD) is Signs and symptoms How your doctor will know if you have it Tests
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Vomiting Approach to diagnosis
 Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
Vomiting Approach to diagnosis By Dr. Sahar El-Gharabawy Associate professor of internal medicine Hepato-gastroenterology Unit )SMH ) Mansoura University Definitions: Nausea: Feeling "sick to the stomach",
Gastro-Esophageal Reflux Disease (GERD)
") Gastro-Esophageal Reflux Disease (GERD) Definition: GERD, or Gastro-Esophageal Reflux Disease, is a digestive disorder, in which partially digested food from the stomach, along with Hydrochloric acid (HCl)
Gastro-Esophageal Reflux Disease (GERD) Definition: GERD, or Gastro-Esophageal Reflux Disease, is a digestive disorder, in which partially digested food from the stomach, along with Hydrochloric acid (HCl)
Heartburn. Understanding and Treating. Heal n Cure For appointments call
 A C P S P E C I A L R E P O R T Understanding and Treating Heartburn What is Heartburn? It begins as a burning pain in the middle of your chest, behind the breastbone, often after a big meal. The burning
A C P S P E C I A L R E P O R T Understanding and Treating Heartburn What is Heartburn? It begins as a burning pain in the middle of your chest, behind the breastbone, often after a big meal. The burning
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
Bariatric Surgery Risk Education Packet Walter J. Chlysta MD, FACS
 Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
OPERATIVE TREATMENT OF ULCER DISEASE
 Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
235 60th Street, West New York, NJ T: (201) F: (201) Main Street, Hackensack, NJ T: (201)
 F: (201) Main Street, Hackensack, NJ T: (201)") 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Barrett's Esophagus WHAT IS BARRETTT'S ESOPHAGUS? Barrett's esophagus
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY PEPTIC ULCER DISEASE PC Bornman RS Du Toit EPIDEMIOLOGY AND PATHOGENESIS The prevalence of duodenal ulcer disease has a variable geographical distribution and differs
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY PEPTIC ULCER DISEASE PC Bornman RS Du Toit EPIDEMIOLOGY AND PATHOGENESIS The prevalence of duodenal ulcer disease has a variable geographical distribution and differs
Methotrexate. About This Drug. Possible Side Effects. Warnings and Precautions
 Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
University of Buea. Faculty of Health Sciences. Programme in Medicine
 Faculty of Health Sciences University of Buea Wednesday, 28 th January 2009 Time: 8 00-10 00 Programme in Medicine MED 303 (Gastrointestinal Physiology) EXAMS (2008-2009) Identify the letter of the choice
Faculty of Health Sciences University of Buea Wednesday, 28 th January 2009 Time: 8 00-10 00 Programme in Medicine MED 303 (Gastrointestinal Physiology) EXAMS (2008-2009) Identify the letter of the choice
https://www.uptodate.com/contents/acid-reflux-gastroesophageal-reflux-disease-in-adults-...
 Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Gastroduodenal Stress Ulceration. Bryan Woolridge POS Rounds 29 October 2003
 Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Chapter 29 Gastrointestinal Intubation
 Chapter 29 Gastrointestinal Intubation Intubation Intubation: placement of a tube into a body structure Types of intubation Orogastric: mouth to stomach Nasogastric: nose to stomach Nasointestinal: nose
Chapter 29 Gastrointestinal Intubation Intubation Intubation: placement of a tube into a body structure Types of intubation Orogastric: mouth to stomach Nasogastric: nose to stomach Nasointestinal: nose
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
Nausea and Vomiting During Pregnancy. Reassuring, with rare exception, that your pregnancy is healthy
 1 Nausea and Vomiting During Pregnancy Keith Merritt, MD Overview Common problem affecting 50-90% of pregnancies between 5 and 18 weeks o Peaks, in most, around 9 weeks o Resolves, in most, by 16 to 18
1 Nausea and Vomiting During Pregnancy Keith Merritt, MD Overview Common problem affecting 50-90% of pregnancies between 5 and 18 weeks o Peaks, in most, around 9 weeks o Resolves, in most, by 16 to 18
Management of Patients With Gastric and Duodenal Disorders
 Chapter 37 Management of Patients With Gastric and Duodenal Disorders LEARNING OBJECTIVES On completion of this chapter, the learner will be able to: 1. Compare the etiology, clinical manifestations, and
Chapter 37 Management of Patients With Gastric and Duodenal Disorders LEARNING OBJECTIVES On completion of this chapter, the learner will be able to: 1. Compare the etiology, clinical manifestations, and
Inguinal Hernia. Hernia Awareness Month. What is a Hernia? Common Hernia Types
 Hernia Awareness Month What is a Hernia? A hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. For example, the intestines may break through a weakened
Hernia Awareness Month What is a Hernia? A hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. For example, the intestines may break through a weakened
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
What Is Peptic Ulcer Disease?
 What Is Peptic Ulcer Disease? Peptic ulcer disease is when painful sores form in the lining of the stomach, duodenum (start of the small intestine) or bowels. An ulcer can cause belly pain and, in some
What Is Peptic Ulcer Disease? Peptic ulcer disease is when painful sores form in the lining of the stomach, duodenum (start of the small intestine) or bowels. An ulcer can cause belly pain and, in some
Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults
 Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults hur till återvinna från prostataoperation Is This Information Right for Me? Yes, if: A doctor said that you have gastroesophageal
Treatment Options for GERD or Acid Reflux Disease A Review of the Research for Adults hur till återvinna från prostataoperation Is This Information Right for Me? Yes, if: A doctor said that you have gastroesophageal
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery.
 Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Chapter 29 - Nausea and Vomiting
 Chapter 29 - Nausea and Vomiting Episode Overview: 1) Describe the mechanism of development of a Hypochloremic Metabolic Alkalosis in vomiting 2) List commonly used anti-emetics including their dose and
Chapter 29 - Nausea and Vomiting Episode Overview: 1) Describe the mechanism of development of a Hypochloremic Metabolic Alkalosis in vomiting 2) List commonly used anti-emetics including their dose and
The STRETTA Procedure
 THE HEARTBURN AND REFLUX STUDY CENTER The STRETTA Procedure Introduction The STRETTA procedure is an advanced state-of-the-art endoscopic technique for the correction of all forms of reflux disease including:
THE HEARTBURN AND REFLUX STUDY CENTER The STRETTA Procedure Introduction The STRETTA procedure is an advanced state-of-the-art endoscopic technique for the correction of all forms of reflux disease including:
Chapter 44 10/17/2015. Care of the Patient with a Gastrointestinal Disorder. The Digestive System. Organs of the Digestive System
 Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
National Digestive Diseases Information Clearinghouse
 Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
Barrett s Esophagus National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Barrett s esophagus? Barrett s esophagus is
North York Endoscopy Instructions
 North York Endoscopy Instructions IMPORTANT INFORMATION: Prior to taking the preparation, please read the details of the procedure, including the risks and benefits. If you agree to the procedure after
North York Endoscopy Instructions IMPORTANT INFORMATION: Prior to taking the preparation, please read the details of the procedure, including the risks and benefits. If you agree to the procedure after
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
Table of Contents: What is a laparoscopic nissen fundoplication?...3. Where will surgery be performed?...3
 Table of Contents: What is a laparoscopic nissen fundoplication?...3 Planning and preparing for the surgery...3-4 Where will surgery be performed?...3 What to expect during surgery and your hospital stay.
Table of Contents: What is a laparoscopic nissen fundoplication?...3 Planning and preparing for the surgery...3-4 Where will surgery be performed?...3 What to expect during surgery and your hospital stay.
STOMACH and DUODENUM DISEASE
 STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Monitor patient s ability to self-administer insulin. (To evaluate safe administration of drug.)
") Nursing Process Focus: Patients Receiving Regular Insulin (Humulin, Novolin) Assessment Prior to administration: Assess any patient allergies. Older forms of insulin are made from beef and pork and may
Nursing Process Focus: Patients Receiving Regular Insulin (Humulin, Novolin) Assessment Prior to administration: Assess any patient allergies. Older forms of insulin are made from beef and pork and may
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS. 1. Which of the following is not a common cause of peptic ulcer disease (PUD)?
?") CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
Gastroesophageal Reflux (GER) and Gastroesophageal Reflux Disease (GERD) in Adults
 and Gastroesophageal Reflux Disease (GERD) in Adults") Gastroesophageal Reflux (GER) and Gastroesophageal Reflux Disease (GERD) in Adults National Digestive Diseases Information Clearinghouse What is GER? Gastroesophageal reflux (GER) occurs when stomach contents
Gastroesophageal Reflux (GER) and Gastroesophageal Reflux Disease (GERD) in Adults National Digestive Diseases Information Clearinghouse What is GER? Gastroesophageal reflux (GER) occurs when stomach contents
Peptic Ulcer Disease and NSAIDs
 Peptic Ulcer Disease and NSAIDs National Digestive Diseases Information Clearinghouse What is a peptic ulcer? A peptic ulcer is a sore on the inner lining of the stomach or duodenum the first part of the
Peptic Ulcer Disease and NSAIDs National Digestive Diseases Information Clearinghouse What is a peptic ulcer? A peptic ulcer is a sore on the inner lining of the stomach or duodenum the first part of the
Diet and Gastrointestinal Problems
 Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20 Diet and Gastrointestinal Problems Objectives Explain uses of diet therapy in gastrointestinal disturbances Identify foods allowed and disallowed in therapeutic diets discussed Adapt normal
Chapter 20. Assisting With Nutrition and Fluids
 Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
Chapter 20 Assisting With Nutrition and Fluids Food and water: Are physical needs Basics of Nutrition Are necessary for life A poor diet and poor eating habits: Increase the risk for diseases and infection
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Laparoscopic Gastric Bypass Information
 1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
GASTRECTOMY. Date of Surgery. Please bring this booklet the day of your surgery. QHC#34
 GASTRECTOMY Date of Surgery Please bring this booklet the day of your surgery. QHC#34 What is a Gastrectomy? A Gastrectomy is the surgical removal of all or part of the stomach. The stomach is the digestion
GASTRECTOMY Date of Surgery Please bring this booklet the day of your surgery. QHC#34 What is a Gastrectomy? A Gastrectomy is the surgical removal of all or part of the stomach. The stomach is the digestion
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Preparing for your Laparoscopic Myotomy
 Preparing for your Laparoscopic Myotomy Pre and post-operative information Department of Table of Contents: What is a Laparoscopic Myotomy...3 Planning for surgery...3 Preparing for surgery/bowel prep.4
Preparing for your Laparoscopic Myotomy Pre and post-operative information Department of Table of Contents: What is a Laparoscopic Myotomy...3 Planning for surgery...3 Preparing for surgery/bowel prep.4
Gastrointestinal. Issues in ElderCare. TCHP Education. Consortium. Part of the ElderCare: Healthcare for the Aging Series
 TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,
TCHP Education Consortium Gastrointestinal Issues in ElderCare Part of the ElderCare: Healthcare for the Aging Series TCHP Education Consortium, 2004, 2007 This educational activity expires December 31,