Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México
|
|
|
- Jane Cain
- 5 years ago
- Views:
Transcription



1 Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México
2 The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients from several studies recalled experiencing moderate to extreme pain, anxiety, fear and inability to sleep during ICU stay. Managing sedation is an important unmet challenge in ICUs worldwide. Pain management is often left aside despite major interventions There is no gold standard regarding pharmacological options for managing pain and sedation Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine
3 The target Identification of the critically ill patient s need for pain relief and correct level of sedation decreases the risk of complications and reduces the LOS. Personalized pain treatment and sedation in the ICU also improve the patient s comfort and raise the tolerance threshold for ICU treatment
4
5 Sedation Analgesia Model Patients are given constant sedatives to relieve anxiety or distress, with extra analgesia given to relieve pain. There is a tendency of oversedation between 40-60% of the patients There are several adverse effects of the drugs use in the sedation model
6 Sedation-Analgesia Model Recent publications have found that there are advantages of sedation protocols, assessment scales and daily interruptions of sedatives. However there is a great heterogeneity in sedation practices across countries Ideally, patients need to be awake or only lightly sedated unless there is a clinical need for deep sedation Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine

7 Sedation-Analgesia Model Burry et al: Critical care med 2015
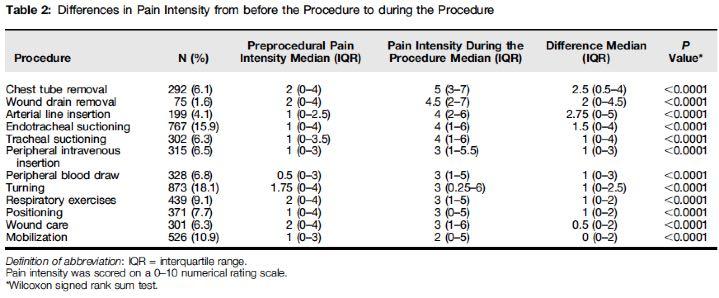
8 Pain in the ICU Two possible origins: Acute pain from the basal illness Acute pain from ICU procedures Reasons for untreated pain: Underestimate pain in the sedated patient Lack of knowledge of specific assessment tools

9 Pain: The unmet player
10
11 Gélinas et al: In pursuit of pain: recent advances and future directions in pain assessment in the ICU: Intensive Care Med (2014) 40, 1009
12 Pain in the ICU Successful analgesia starts with identifying and managing conditions that contribute to pain, well before the use of any medications. Insomnia, anxiety and delirium can amplify the pain experience and also require prompt treatment. Azzam & Abdulkader : Pain in the ICU A Psychiatric Perspective (2013) J of Intensive Care Medicine, 28 (3) 140
13 Clinical recommendations
14 Clinical recommendations

15 Analgo sedation
16 Analgo-Sedation The ICU is an hostile environment Pain is often the root cause of distress Anxiety Dyspnea Delirium Sleep deprivation
17 Analgosedation The primary goal is to address pain and then add a hypnotic agent if necessary Analgesia based sedation Analgesia first sedation It is an approach to ICU sedation that may ameliorate significant patient safety concerns associated commonly with sedative agents. Puts a focus on the unmet need of providing adequate pain relief. Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine
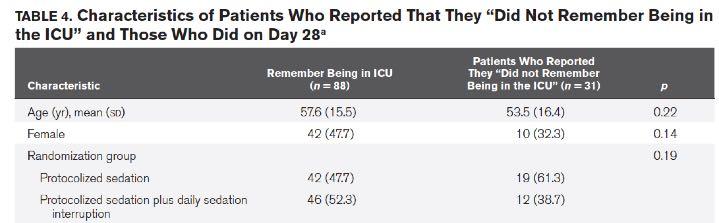
18 Analgosedation The trials reviewed by Devabhakthuni et al (2012) showed that: Comparing the use of remifentanil to propofol or midazolam, the approach of using remifentanil alone in continuous infusion: Led to optimal patient comfort studies None of the remifentanil studies used daily sedation interruption Patients treated with this model were more likely to be weaned from ventilation more quickly, spend less time on ventilator support, and have a shorter ICU length of stay. Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine
19 Analgosedation There has been also drawbacks in the analgosedation model: Delirium has also been found to be associated with morphine administration. Recall for unpleasant events before regaining consciousness, nightmares and hallucinations. Immunosuppressive effects of opioids Strong withdrawal effect following the discontinuation Hyperalgesia and increased analgesic requirements following cessation of remifentanil infusions Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine
20 Analgosedation There are some concerns about the use of analgosedation if the patient: Requires deeper levels of sedation (such as those with elevated intracranial pressure) Ventilator disynchrony Severe agitation Other specific conditions Bartel B: New Sedation Practices in the Adult Intensive Care Unit: Analgosedation; South Dakota Medicine
21 Analgosedation Which opioid is the best? Remifentanil is the ideal based on its pharmacokinetic properties More important role in patients with neurologic conditions that require closer monitoring. Cause hyperalgesia Fentanyl is also a reasonable choice with similar outcomes when compared to remifentanil Morphine accumulates in renal failure and has deleriogenic effects Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530
22
23 Clinical recommendations A shift in current sedations practices to analgosedation should be considered in the care of mechanically ventilated ICU patients. Clinicians must avoid oversedation, which can be accomplished with the use of protocols and daily sedation interruptions. Sedation interruptions should be targeted at achieving the lightest level of sedation possible to prevent excessive drug accumulation Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530 Shahriari et al Effects of pain management program on the LOS of patient with decrease level of consciousness: Iranian Jurnal of Nursing and Midwifery Research (2015) 20 (4)
24 Clinical recommendations When possible, analgesic effectiveness and requirements should be monitored through patient self-report. Those unavailable to communicate, a validated assessment tool for pain should be use (visual analog pain scale or behavioral pain scale) Patient discomfort should be treated with analgesics such as remifentanil or fentanyl; leaving morphine reserved as a second-line agent due to its adverse effects. Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530
25 Clinical recommendations The use of hypnotic agents such as propofol or dexmedetomidine should be considered in all patients requiring rescue therapy after the initiation of analgosedation. Benzodiazepines use should be kept to a minimum. The use of sparing agents such as acetaminophen or NSAIDs is currently under research Devabhakthuni S, et al: Analgosedation: A Pafadigm shift in ICU Sedation Practice: Ann Pharmacother, 2012; 46: 530
26 Clinical recommendations Anxiety, delirium and pain are not mutually exclusive, and treatment of one may exacerbate the other (eg: excessive ansiolytic administration promoting delirium) Physicians must understand the relation of neuropsychiatric conditions of pain (multimodal sedation?) Sedation protocols Azzam & Abdulkader : Pain in the ICU A Psychiatric Perspective (2013) J of Intensive Care Medicine, 28 (3) 140
27 Conclusions Critical care improves and patients benefit when ICU clinicians practice thoughtful and systematic pain management. Guidance through protocols is the best strategy to minimize pain and improve comfort without oversedation. Analgosedation although promising, needs further clinical confirmation
28 Analgosedation Pros and Cons Advantages Reduction in hypnotics Less mechanical ventilation time Shorter ICU length of stay Rapid onset and ofset of action Overall ICU cost savings? Disadvantages Delirium Higher incidence of recall Nightmares Hallucinations Immunosuppression Withdrawal Hyperalgesia
29 Algoritmo para Sedación y Analgesia en TI Sedación Agitación Corta Prolongada Sí No Evaluar con escalas 1B Dexmedetomidina 1B Sedación basada en la analgesia 1B Propofol 1B Evaluar con escalas 1B Interrupción diaria de la sedación 1B Propofol 1B Dexmedetomidina 1C Lorazepam 1C Midazolam 1C Sí Evaluar factores predisponentes 1B Dolor No Evaluar con escalas de sedación y alcanzar objetivos 1B Morfina 1C Fentanilo 1C Evaluar dolor cada min. 1C Remifentanilo 1C Ajustar opioides 1C Evaluar cada 4 horas con escalas y ajustar dosis 1C Evaluar causa de incomodidad: 1C Hipoxia Alteración metabólica Reacción adverse a fármacos Síndrome de abstinencia Cama húmeda Retención urinaria Modo ventilatorio inadecuado Dexmedetomdina 1B Propofol 1B FEPIMCTI


30 Hand Made

31
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Sedation and Analgesia in the Critically Ill
 12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Pain Management in the NICU. Tamorah Lewis MD, PhD
 Pain Management in the NICU & Iatrogenic Opiate Withdrawal Tamorah Lewis MD, PhD Assistant Professor Divisions of Neonatology & Clinical Pharmacology, Toxicology and Therapeutic Innovation The Children's
Pain Management in the NICU & Iatrogenic Opiate Withdrawal Tamorah Lewis MD, PhD Assistant Professor Divisions of Neonatology & Clinical Pharmacology, Toxicology and Therapeutic Innovation The Children's
New approaches of sedation in critically ill patients.
 New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Sedation is a dynamic process.
 19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Prolonged opioid therapy in the Critically Ill Pediatric Patient
 PBLD Table #22 Prolonged opioid therapy in the Critically Ill Pediatric Patient Arlyne K. Thung, M.D. Assistant Professor, Anesthesiology & Shu-Ming Wang, M.D. Associate Professor, Anesthesiology Yale
PBLD Table #22 Prolonged opioid therapy in the Critically Ill Pediatric Patient Arlyne K. Thung, M.D. Assistant Professor, Anesthesiology & Shu-Ming Wang, M.D. Associate Professor, Anesthesiology Yale
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
From the Department of Pharmacy (JM, CAF) and Department of Pulmonary and Critical
 and Department of Pulmonary and Critical") PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: POLICY LAST UPDATED:
 EFFECTIVE DATE: POLICY LAST UPDATED:") Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 01 08 2013 OVERVIEW Monitored anesthesia care is a specific anesthesia service for a diagnostic or
Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 01 08 2013 OVERVIEW Monitored anesthesia care is a specific anesthesia service for a diagnostic or
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
SEDATION / ANALGESIA for Brain Failure Patient INASNACC
 SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative Care Service
 954 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative
954 Journal of Pain and Symptom Management Vol. 26 No. 4 October 2003 Clinical Note Ventilator Withdrawal: Procedures and Outcomes. Report of a Collaboration Between a Critical Care Division and a Palliative
1
 Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Approach to agitated patient in ICU
 Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES
 WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
Update on the Management and Monitoring of Deep Analgesia and Sedation in the Intensive Care Unit
 AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
PICU Sedation Holidays. Jorge G. Sainz MD FAAP Medical Director PICU Medical Director Transport
 Jorge G. Sainz MD FAAP Medical Director PICU Medical Director Transport jsainz@elpasochildrens.org 1. Define sedation holiday. Objectives 2. Review differences between adult and pediatric sedation in ICU
Jorge G. Sainz MD FAAP Medical Director PICU Medical Director Transport jsainz@elpasochildrens.org 1. Define sedation holiday. Objectives 2. Review differences between adult and pediatric sedation in ICU
The Difficult to Sedate ICU Patient
 The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
Pathway to Pain Control
 Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, 2017
Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, 2017
ADMINISTRATION OF PALLIATIVE SEDATION TO THE DYING PATIENT
 ADMINISTRATION OF PALLIATIVE SEDATION TO THE DYING PATIENT PURPOSE To specify the circumstances under which the administration of Palliative Sedation is clinically and ethically appropriate for a dying
ADMINISTRATION OF PALLIATIVE SEDATION TO THE DYING PATIENT PURPOSE To specify the circumstances under which the administration of Palliative Sedation is clinically and ethically appropriate for a dying
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
SEDATION FOR SMALL PROCEDURES
 SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
Ketofol: risky or revolutionary: CPD article IV
 Ketofol: risky or revolutionary: CPD article IV Abstract Ketofol, a sedative/analgesic combination of ketamine and propofol, which can be administered as a mixture in the same syringe or independently,
Ketofol: risky or revolutionary: CPD article IV Abstract Ketofol, a sedative/analgesic combination of ketamine and propofol, which can be administered as a mixture in the same syringe or independently,
States of Consciousness
 Myers PSYCHOLOGY (7th Ed) Chapter 7 States of Consciousness Waking Consciousness Consciousness our awareness of ourselves and our environments Sleep and Dreams Biological Rhythms periodic physiological
Myers PSYCHOLOGY (7th Ed) Chapter 7 States of Consciousness Waking Consciousness Consciousness our awareness of ourselves and our environments Sleep and Dreams Biological Rhythms periodic physiological
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Sedation in Children
 CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Role of Quetiapine in an Adult Critical Care Practice
 American Journal of Pharmacology and Pharmacotherapeutics Short Communication Role of Quetiapine in an Adult Critical Care Practice Vikram Anumakonda* Dudley Group of Hospitals NHS Foundation Trust Birmingham,
American Journal of Pharmacology and Pharmacotherapeutics Short Communication Role of Quetiapine in an Adult Critical Care Practice Vikram Anumakonda* Dudley Group of Hospitals NHS Foundation Trust Birmingham,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
 Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
The Quebec Palliative Sedation Guidelines. Rose DeAngelis, N, MSc(A), CHPCN (C)
, CHPCN (C)") The Quebec Palliative Sedation Guidelines Rose DeAngelis, N, MSc(A), CHPCN (C) CHPCA Conference September 2017 Conflict of Interest Statements There is no financial or in-kind support for this presentation.
The Quebec Palliative Sedation Guidelines Rose DeAngelis, N, MSc(A), CHPCN (C) CHPCA Conference September 2017 Conflict of Interest Statements There is no financial or in-kind support for this presentation.
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE
 MONITORING SYSTEM FOR CRITICAL CARE") REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE WHAT IS THE BIS MONITORING SYSTEM? The BIS brain monitoring system generates a processed EEG parameter that provides
REFERENCE GUIDE USING THE BISPECTRAL INDEX (BIS ) MONITORING SYSTEM FOR CRITICAL CARE WHAT IS THE BIS MONITORING SYSTEM? The BIS brain monitoring system generates a processed EEG parameter that provides
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
WITHDRAWING FROM BUPRENORPHINE THERAPY
 WITHDRAWING FROM BUPRENORPHINE THERAPY VARIOUS REASONS TO STOP BUPRENORPHINE pregnancy and lactation emergency surgery/elective surgery difficult to manage side effects of buprenorphine patients showing
WITHDRAWING FROM BUPRENORPHINE THERAPY VARIOUS REASONS TO STOP BUPRENORPHINE pregnancy and lactation emergency surgery/elective surgery difficult to manage side effects of buprenorphine patients showing
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally?
 Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally? Dick Tibboel; Erwin Ista; Nienke Vet; Monique van Dijk Erasmus MC Sophia Children s Hospital Rotterdam, The Netherlands
Sedation and analgesia in pediatric mechanical ventilation: are we doing it optimally? Dick Tibboel; Erwin Ista; Nienke Vet; Monique van Dijk Erasmus MC Sophia Children s Hospital Rotterdam, The Netherlands
The Way UP: How Four Cross-Cutting Strategies Can Reduce Harm Across the Board
 The Way UP: How Four Cross-Cutting Strategies Can Reduce Harm Across the Board 1 Today s Agenda 11:30 11:35: Welcome & Introductions Nikki Medalen & Jean Roland, Quality Health Associates of North Dakota
The Way UP: How Four Cross-Cutting Strategies Can Reduce Harm Across the Board 1 Today s Agenda 11:30 11:35: Welcome & Introductions Nikki Medalen & Jean Roland, Quality Health Associates of North Dakota
Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure. Supplement 2 Table of Contents
 Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure Supplement 2 Table of Contents RESTORE Algorithm and Box-by-Box Instructions Page 1 of 2
Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure Supplement 2 Table of Contents RESTORE Algorithm and Box-by-Box Instructions Page 1 of 2
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Series 2 dexmedetomidine, tramadol, fentanyl, intellectually disabled patients:
 Series 2 dexmedetomidine, tramadol, fentanyl, intellectually disabled patients: Read the following published scientific articles and answer the questions at the end: Abstract We get a substantial number
Series 2 dexmedetomidine, tramadol, fentanyl, intellectually disabled patients: Read the following published scientific articles and answer the questions at the end: Abstract We get a substantial number
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Analgesia and Sedation in Intensive Care Unit
 Rev Bras Anestesiol 2010; 60: 6: 648-658 REVIEW ARTICLE REVIEW ARTICLE Analgesia and Sedation in Intensive Care Unit Rioko Kimiko Sakata, TSA 1 Summary: Sakata RK Analgesia and Sedation in Intensive Care
Rev Bras Anestesiol 2010; 60: 6: 648-658 REVIEW ARTICLE REVIEW ARTICLE Analgesia and Sedation in Intensive Care Unit Rioko Kimiko Sakata, TSA 1 Summary: Sakata RK Analgesia and Sedation in Intensive Care
BIS Brain Monitoring for Critical Care
 BIS Brain Monitoring for Critical Care The Bispectral Index (BIS ) is a processed EEG parameter that provides a direct measure of the effects of sedatives on the brain. The BIS monitoring value is represented
BIS Brain Monitoring for Critical Care The Bispectral Index (BIS ) is a processed EEG parameter that provides a direct measure of the effects of sedatives on the brain. The BIS monitoring value is represented
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces
 16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
Barb Supanich, RSM, MD, FAAHPM Medical Director, Palliative Care Team September 9, 2010
 Barb Supanich, RSM, MD, FAAHPM Medical Director, Palliative Care Team September 9, 2010 Learner Goals Define Palliative Sedation Identify at least two pertinent Ethical Issues for the patient, family and
Barb Supanich, RSM, MD, FAAHPM Medical Director, Palliative Care Team September 9, 2010 Learner Goals Define Palliative Sedation Identify at least two pertinent Ethical Issues for the patient, family and
Randomized controlled trial of daily interruption of sedatives in critically ill children
 Pediatric Anesthesia ISSN 1155-5645 ORIGINAL ARTICLE Randomized controlled trial of daily interruption of sedatives in critically ill children Carin W. M. Verlaat 1, Ger P. Heesen 1, Nienke J. Vet 2, Matthijs
Pediatric Anesthesia ISSN 1155-5645 ORIGINAL ARTICLE Randomized controlled trial of daily interruption of sedatives in critically ill children Carin W. M. Verlaat 1, Ger P. Heesen 1, Nienke J. Vet 2, Matthijs
Chapter 25. General Anesthetics
 Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Activation-synthesis hypothesis. compulsive drug craving and use, despite adverse consequences. Addition. Amphetamines. Barbiturates.
 Activation-synthesis hypothesis Suggests that in the brain engages in a lot of neural activity that is random. Dreams make sense of this activity. Addition compulsive drug craving and use, despite adverse
Activation-synthesis hypothesis Suggests that in the brain engages in a lot of neural activity that is random. Dreams make sense of this activity. Addition compulsive drug craving and use, despite adverse
BPG 06: Sedation. Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects.
 Statement of Best Practice BPG 06: Sedation Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects. 1: Introduction Indication for sedation will
Statement of Best Practice BPG 06: Sedation Patients receive appropriate sedation to meet their needs, optimising comfort and with minimal adverse effects. 1: Introduction Indication for sedation will
Index. Note: Page numbers of article titles are in boldface type. Pain Management in Critical Care
 Pain Management in Critical Care Index Note: Page numbers of article titles are in boldface type. Acetaminophen, for pain, 215 dosage of, 216 in children, 287-288 Addiction, to medication, defined, 277
Pain Management in Critical Care Index Note: Page numbers of article titles are in boldface type. Acetaminophen, for pain, 215 dosage of, 216 in children, 287-288 Addiction, to medication, defined, 277
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Chapter 004 Procedural Sedation and Analgesia
 Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Opioid Prescribing for Acute Pain. Care for People 15 Years of Age and Older
 Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can