Pathway to Pain Control
|
|
|
- Adela Bradley
- 5 years ago
- Views:
Transcription
1 Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, MFMER slide-1
2 Disclosures The presenters have nothing to disclose 2015 MFMER slide-2
3 Objectives Discuss valid and reliable pain assessment tools in the ICU Recognize common ICU procedures that cause pain, necessitating interventions to prevent pain Describe important strategies to integrate into everyday clinical practice to prevent and manage pain ICU intensive care unit 2015 MFMER slide-3
4 Unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain. 1979;6: MFMER slide-4
5 Background Incidence of significant pain is 50% in ICU patients Approximately 50% of patients have pain at rest Untreated pain is associated with increased morbidities and cost In surgical patients, post-operative pain has been associated with chronic pain ICU intensive care unit Macrae WA. Br J Anaesth. 2008:101: Sinatra R. Pain Med. 2010;11: Barr J. Crit Care Med. 2013;41: MFMER slide-5
6 Caring for ICU Patients Survival Comfort & Preventing Long Term Complications 2015 MFMER slide-6
7 Stressors in the ICU: Patients Evaluation Rank Description Mean Standard Deviation 1 Have pain Not being able to sleep Have tubes in your nose and mouth Not being in control of yourself ICU intensive care unit Novaes MA. Intensive Care Med. 1997;23: MFMER slide-7
8 Sources of Pain Invasive Procedures Daily Care Disease Process Pain Exacerbating Factors Sigakis M. Crit Care Med MFMER slide-8
9 What Do We Care About Untreated Pain? Consequences of Pain Physiological Psychological Social/Economic Sigakis M. Crit Care Med MFMER slide-9
10 Physiological Increased catecholamines Vasoconstriction Impaired tissue perfusion Catabolic hypermetabolism Hyperglycemia Lipolysis Breakdown of muscle Suppression of natural killer cells Sigakis M. Crit Care Med Barr J. Crit Care Med. 2013;41: MFMER slide-10
11 Psychological Insufficient sleep Most traumatic ICU memory Posttraumatic stress disorder Chronic pain ICU intensive care unit Sigakis M. Crit Care Med Barr J. Crit Care Med. 2013;41: MFMER slide-11
12 Socioeconomic Increased duration of mechanical ventilation Increased length of stay Increased mortality Increased cost Decreased quality of life Sigakis M. Crit Care Med Barr J. Crit Care Med. 2013;41: MFMER slide-12
13 Barriers to Treatment of Pain Provider Healthcare System Patient Sigakis M. Crit Care Med MFMER slide-13
14 Objectives Discuss valid and reliable pain assessment tools in the ICU Recognize common ICU procedures that cause pain, necessitating interventions to prevent pain Describe important strategies to integrate into everyday clinical practice to prevent and manage pain ICU intensive care unit 2015 MFMER slide-14

15 Assessing Pain in the ICU Patient s self-report Patient proxy report Clinician s assessment Barr. Crit Care Med. 2013; 41: MFMER slide-15
16 Assessing Pain in the ICU Patient s self-report 1 Search for potential causes of pain 2 Observe patient behavior 3 Patient s proxy report 4 Attempt an analgesic trial 5 ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Chanques. Pain. 2010; 151: Herr. Pain Manag Nurs. 2011; 12: MFMER slide-16
17 Assessing Pain in the ICU Patient s Self-Report Pain assessment tools Numeric Rating Scale Visual Analog Scale Verbal Descriptor Scale ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: MFMER slide-17

18 Assessing Pain in the ICU Patient s Self-Report Not all pain is avoidable Individualized and goal-oriented analgesia is essential ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Chanques. Pain. 2010; 151: MFMER slide-18
19 Assessing Pain in the ICU Patient s Self-Report Pain assessment tools Numeric Rating Scale Visual Analog Scale Verbal Descriptor Scale Limitations Unable to self-report ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: MFMER slide-19
20 Assessing Pain in the ICU Clinician s Assessment Pain assessment tools Facial expressions Body movements Ventilator interaction Consensus Guideline recommended scales Behavioral Pain Scale Critical Care Pain Observation Tool ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Puntillo. Chest. 2009; 135: Li. J Pain. 2008; 9: Arbour. J Trauma Nurs. 2011; 2015 MFMER 18: slide-20
21 Assessing Pain in the ICU Behavioral Pain Scale Item Description Score Facial expression Upper limbs Compliance with mechanical ventilation Relaxed Partially tightened Fully tightened Grimacing No movement Partially bent Fully bent with finger flexion Permanently retracted BPS > 5 = Pain Tolerating movement Coughing but mostly tolerating ventilation Fighting ventilator Unable to control ventilation Total Score ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Puntillo. Chest. 2009; 135: Li. J Pain. 2008; 9: Arbour. J Trauma Nurs. 2011; 18: MFMER slide-21
22 Assessing Pain in the ICU Critical Care Pain Observation Tool Item Description Score Facial expression Body movements Relaxed, neutral: no muscular tension observed Tense: presence of frowning, brow lowering, orbit tightening, and levator contraction Grimacing: all of the above facial movements plus eyelids tightly closed Absent: doesn t move at all Protection: slow, cautious movements, toughing or rubbing the pain site, seeking attention Restlessness: pulling tube, attempting to sit up, moving limbs/thrashing, not following commands, striking at staff, trying to climb out of bed Muscle tension CPOT Relaxed: no resistance to passive > movements 2 = Pain Passive flexion/extension of Tense or rigid: esistance to passive movements upper extremities Very tense or rigid: trong resistance to passive movements, inability to complete them Ventilator compliance Tolerating ventilator or movement: alarms not activated, easy ventilation Coughing but tolerating: alarms spontaneously Fighting ventilator: asynchrony, blocking ventilation, alarms frequently activated OR Talking in normal tone or no sound Vocalization Sighing, moaning Crying out, sobbing Total Score ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Puntillo. Chest. 2009; 135: Li. J Pain. 2008; 9: Arbour. J Trauma Nurs. 2011; 18: MFMER slide-22
23 Assessing Pain in the ICU Clinician s Assessment Pain assessment tools Facial expressions Body movements Ventilator interaction Consensus Guideline recommended scales Behavioral Pain Scale Critical Care Pain Observation Tool Limitations Validation in diverse patient populations Unable to assess behaviors ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Puntillo. Chest. 2009; 135: Li. J Pain. 2008; 9: Arbour. J Trauma Nurs. 2011; 18: MFMER slide-23

24 Assessing Pain in the ICU 70% 60% 50% 40% 30% Incidence of Pain Pain Unassessed Pain Assessed 63% P<0.01 P< % 36% Medication Usage and Patient Outcomes Opioid Duration, hours Sedative Duration, hours Mechanical ventilation, hours Pre Post p 47% 96 54% 84 46% 60 55% 48 NS 0.02 NS % 10% 0% 16% Nosocomial infection 17% 8% 0.05 ICU LOS, days NS Mortality 12% 15% NS Pain Severe Pain More escalation and de-escalation of analgesics and sedatives post-implementation Barr. Crit Care Med. 2013; 41: Chanques. Crit Care Med. 2006; 34: MFMER slide-24
25 Assessing Pain in the ICU Medication Usage Pre Post p Opioids 95% 92% NS Nonopioids 29% 42% 0.01 Multimodal analgesia 24% 35% 0.01 Sedatives 86% 75% 0.01 Neuromuscular blockade 13% 7% 0.01 Days Patient Outcomes Pain Unassessed 11 8 Mechanical Ventilation Pain Assessed P=0.05 P=0.04 ICU Duration Barr. Crit Care Med. 2013; 41: Payen. Anesthes. 2009; 111: MFMER slide-25
26 Assessing Pain in the ICU Impact of Assessing Pain Pain assessment with a validated tool improves patient care Improved pain scores Improved utilization of multimodal analgesics No difference in opioid-related adverse events Decreased utilization of sedatives Decreased utilization of neuromuscular blockade Decreased duration of mechanical ventilation Decreased ICU length of stay Decreased mortality Improved utilization of chronic opioids Payen. Anesthesiology. 2007; 106: Payen. Anesthesiology. 2009; 111: van Gulik. Eur J Anaesthesiol. 2010; 27: ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: Gelinas. Int J Nurs Stud. 2011; 48: Erdek. Int J Qual Health Care. 2004; 16: MFMER slide-26
27 Assessing Pain in the ICU Key Concepts from Consensus Guidelines SCCM/ACCM Pain, Agitation, Delirium Guidelines Pain should be routinely monitored in all adult ICU patients Use of validated pain assessment tools Patient s self-report vs. behavioral pain scales Vital signs should never be used alone for pain assessment in adult ICU patients, but may trigger further assessment of pain ASA Perioperative Pain Guidelines Use standardized, validated instruments to facilitate the regular evaluation and documentation of pain intensity, effects of pain therapy, and side effects caused by therapy ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med 2013; 41: MFMER slide-27
28 Assessing Pain in the ICU Key Concepts from Consensus Guidelines Pain should be routinely assessed and documented with validated pain assessment tools Self-reporting and behavioral pain scales are essential Therapeutic goals of analgesia should be individualized and patient-specific Pain assessment tools have limitations Analgesic trials may be an effective form of assessment ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med. 2013; 41: MFMER slide-28
29 Assessing Pain in the ICU Assessment Question JT is a 70M admitted to the MICU for respiratory failure secondary to pneumonia. He arrives to your unit from the ED intubated with RASS +3. His past medical history and home medication list reveals diagnoses and medications for COPD and chronic pain. Which of the following do you recommend to obtain to improve JT s agitation? A. Vital signs B. Behavioral Pain Scale C. Urine toxicology screen D. Confusion Assessment Method for the ICU 2015 MFMER slide-29
30 Assessing Pain in the ICU Assessment Question JT is a 70M admitted to the MICU for respiratory failure secondary to pneumonia. He arrives to your unit from the ED intubated with RASS +3. His past medical history and home medication list reveals diagnoses and medications for COPD and chronic pain. Which of the following do you recommend to obtain to improve JT s agitation? A. Vital signs B. Behavioral Pain Scale C. Urine toxicology screen D. Confusion Assessment Method for the ICU 2015 MFMER slide-30
31 Objectives Discuss valid and reliable pain assessment tools in the ICU Recognize common ICU procedures that cause pain, necessitating interventions to prevent pain Describe important strategies to integrate into everyday clinical practice to prevent and manage pain ICU intensive care unit 2015 MFMER slide-31
32 Preventing Pain in the ICU Procedural Pain Procedural pain is common in adult ICU patients Pain Score Thunder II: Procedural Pain Intensity Turning Wound Drain Removal Wound Care Tracheal Suctioning Central Line Placement Femoral Sheath Removal ICU intensive care unit Barr. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; 10: MFMER slide-32
33 Preventing Pain in the ICU Procedural Pain Procedural pain is common in adult ICU patients 70% 60% 50% 40% 30% 20% 10% 0% 58% Turning Thunder II: Patients Reporting Increased Procedural Pain Intensity 65% Wound Drain Removal 53% 55% Wound Care Tracheal Suctioning 52% Central Line Placement 47% Femoral Sheath Removal ICU intensive care unit Barr J. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; 10: Puntillo. Am J Crit Care. 2002; 11: MFMER slide-33
34 Preventing Pain in the ICU Procedural Pain Procedural pain is common in adult ICU patients Pain Score Increased Procedural Pain Intensity Pre-Procedure Turning Drain Removal Tracheal Suctioning Post-Procedure P< Line Removal 5.5 Deep Breathing & Coughing ICU intensive care unit Barr. Crit Care Med. 2013; 41: Siffleet. J Clin Nurs. 2007; 16: MFMER slide-34

35 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! Sharp Tiring Shooting Exhausting Stabbing Awful Less than 20% of all patients received opioids before undergoing routine procedures Barr. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; : MFMER slide-35
36 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! 100% Thunder II Untreated Treated Opiates Local Anesthetics 80% 60% 40% 20% 0% Turning Wound Drain Removal Wound Care Tracheal Suctioning Central Line Placement Femoral Sheath Removal Barr. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; 10: Puntillo. Am J Crit Care. 2002; 11: MFMER slide-36
37 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! 100% 80% 63.6% of patients receive NO analgesics before undergoing or during procedure Thunder II Untreated Treated Opiates Local Anesthetics 94% 83% 82% 77% 60% 40% 42% 20% 7% 0% Turning Wound Drain Removal Wound Care Tracheal Suctioning Central Line Placement Femoral Sheath Removal Barr. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; 10: Puntillo. Am J Crit Care. 2002; 11: MFMER slide-37
38 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! 100% 80% 63.6% of patients receive NO analgesics before undergoing or during procedure Thunder II Untreated Treated Opiates Local Anesthetics 90% 60% 40% 20% 0% 14% 15% 20% 0% 0% 2% 4% 0% Turning Wound Drain Removal Wound Care Tracheal Suctioning 16% Central Line Placement 34% 29% Femoral Sheath Removal Barr. Crit Care Med. 2013; 41: Puntillo. Am J Crit Care. 2001; 10: Puntillo. Am J Crit Care. 2002; 11: MFMER slide-38
39 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! 80% 70% 60% 50% 40% 30% 20% 10% 0% 39% 33% Procedural Pain Management Opioid Non-opioid Post-Procedure Opioid 50% 50% 13% 38% 16% 53% 39% 39% Turning Drain Removal Tracheal Suctioning Line Removal Deep Breathing & Coughing Barr. Crit Care Med. 2013; 41: Siffleet. J Clin Nurs. 2007; 16: MFMER slide-39
40 Preventing Pain in the ICU Procedural Pain but procedural pain is not commonly prevented! 80% 70% 60% 50% 40% 30% 20% 10% 0% 15% Procedural Pain Management Opioid Non-opioid Post-Procedure Opioid 67% 6% 13% 31% Turning Drain Removal Tracheal Suctioning Line Removal Deep Breathing & Coughing Barr. Crit Care Med. 2013; 41: Siffleet. J Clin Nurs. 2007; 16: MFMER slide-40

41 Preventing Pain in the ICU Procedural Pain 100% Administration of Pre-emptive Fentanyl for Procedural Pain Associated with Turning Mechanically Ventilated Patients No Pretreatment 94% Procedural Pretreatment 80% 60% 74% 64% 49% 40% 20% 0% P=0.03 Pain P=0.25 Severe Pain Barr. Crit Care Med. 2013; 41: Robleda. Intensive Care Med. 2016; 42: MFMER slide-41
42 Preventing Pain in the ICU Procedural Pain 80% 70% Hospital Day 2 68% 80% 70% Hospital Day 6 68% 60% 50% 40% 30% 20% 60% P<0.01 P< % P<0.01 P< % 26% 30% 30% 17% 20% 18% 10% 0% 4% Procedural Pain Assessment Procedural Pain Treatment 10% 0% 3% Procedural Pain Assessment Procedural Pain Treatment Barr. Crit Care Med. 2013; 41: Payen. Anesthes. 2009; 111: MFMER slide-42
43 Preventing Pain in the ICU Key Concepts from Consensus Guidelines Procedural pain management technique is as important as agent selection Initiate pre-emptive analgesia before procedures, ensuring it is operational during procedures, in order to reduce procedural pain Pre-emptive analgesia is more effective than the same treatment administered during or after the procedure to reduce pain and subsequent analgesics Consider both non-pharmacologic and pharmacologic options ASA. Anesthesiology. 2012; 116: Barr. Crit Care Med 2013; 41: Pogatzki-Zahn. Curr Opin Anaesthesiol. 2006; 19: MFMER slide-43
44 Preventing Pain in the ICU Assessment Question MK is a 65F who remains intubated in the cardiac surgery ICU overnight following CABG. As MK s assigned nurse, you note she is due for tracheal suctioning and wound cares, and her daughter tells you she believes MK would be more comfortable if she were repositioned. Which of the following procedures do you choose to provide pre-emptive procedural pain treatment with a fentanyl bolus to improve MK s pain intensity? A. Tracheal suctioning B. Wound cares C. Turning D. All of the above 2015 MFMER slide-44
45 Preventing Pain in the ICU Assessment Question MK is a 65F who remains intubated in the cardiac surgery ICU overnight following CABG. As MK s assigned nurse, you note she is due for tracheal suctioning and wound cares, and her daughter tells you she believes MK would be more comfortable if she were repositioned. Which of the following procedures do you choose to provide pre-emptive procedural pain treatment with a fentanyl bolus to improve MK s pain intensity? A. Tracheal suctioning B. Wound cares C. Turning D. All of the above 2015 MFMER slide-45
46 Objectives Discuss valid and reliable pain assessment tools in the ICU Recognize common ICU procedures that cause pain, necessitating interventions to prevent pain Describe important strategies to integrate into everyday clinical practice to prevent and manage pain ICU intensive care unit 2015 MFMER slide-46
47 Patient-Centered Multidisciplinary Approach Patient assessments improve outcomes Treat pain as a preventable adverse event Assess pain daily on rounds Analgesia-first sedation is recommend by the PAD guidelines PAD pain, agitation, delirium Barr J. Crit Care Med. 2013; 41: Sessler C. Chest. 2009;135: MFMER slide-47
48 Sedation Analgesia 2015 MFMER slide-48
49 Analgosedation Analgesia-based sedation Agitation is commonly secondary to pain Optimize pain management add sedation as needed Not recommended in certain patient populations Devabhakthuni S. Ann Pharmacotherapy. 2012;46: MFMER slide-49
50 Analgosedation Disadvantages Advantages Devabhakthuni S. Ann Pharmacotherapy. 2012;46: MFMER slide-50
51 A Protocol of No Sedation Study Design Population Intervention Primary Endpoint Secondary Endpoints Randomized, unblinded prospective study in Denmark Critically ill patients expected to need mechanical ventilation for > 24 hours admitted to medical and surgical ICU No sedation: Morphine and haloperidol as needed Sedation: Propofol (Ramsay 3-4) and morphine as needed x 48 hours then midazolam and morphine as needed with daily sedation interruption Number of days without mechanical ventilation in a 28-day period -Length of ICU stay -Length of hospital stay Strom S. Lancet. 2010;375: MFMER slide-51
52 Outcomes Days Without Mechanical Ventilation (From Intubation to Day 28) Days (mean) No Sedation p= Study Group 10 Sedation Length of ICU and hospital stay were shorter in the no sedation group Morphine doses were similar between groups ICU intensive care unit Strom S. Lancet. 2010;375: MFMER slide-52
53 Impact of an Analgesia-Based Sedation Protocol Study Design Retrospective before and after cohort study Population Patients admitted to the medical ICU Intervention New & old sedation/analgesia protocols Primary Endpoint Secondary Endpoints Duration of mechanical ventilation -Medical ICU LOS -RASS scores during mechanical ventilation -CPOT scores -Sedative and analgesic medication use ICU intensive care unit LOS length of stay RASS Richmond Agitation Sedation Scale CPOT Critical Care Pain Observation Tool Faust A. Anesth Analg. 2016; 123: MFMER slide-53
54 Protocol Old Protocol New Protocol Propofol titrated to RASS 0 to -2 Fentanyl titrated to RASS 0 to -2 PRN pain medications for CPOT score RASS +1 to +4 IV morphine initiated Acute agitation treated with fentanyl and midazolam IV push RASS +1 to +4 propofol or dexmedetomidine initiated Daily sedation awakening Faust A. Anesth Analg. 2016; : MFMER slide-54


55 Hours Outcomes Duration of Mechanical Ventilation p= Sedation Protocol Analgosedation Protocol Sedation Protocol Deeper RASS scores during the sedation protocol Improved CPOT scores during analgosedation protocol ICU length of stay was shorter in the analgosedation group Only 38% of patients in the analgosedation group required continuous infusions of sedatives Faust A. Anesth Analg. 2016; 123: MFMER slide-55
56 Opioid Review Fentanyl Hydromorphone Remifentanil Onset 1 2 minutes 5 15 minutes 1 3 minutes Elimination Half Life 2 4 hours* 2 3 hours 3 10 minutes Metabolism CYP3A4 Glucuronidation Active Metabolites *Context sensitive half life Hydrolysis by plasma esterases None None None Barr J. Crit Care Med. 2013;41: MFMER slide-56
57 Administration Techniques Supratherapeutic Steady state Therapeutic Range Subtherapeutic Bolus + Infusion Infusion Infusion (blind titration) Half Lives 2015 MFMER slide-57
58 Population Pharmacokinetics of Fentanyl in the Critically Ill Study Design Population Primary Endpoint Prospective cohort study Patients admitted to the medical and surgical ICU receiving 48 hours of continuous infusion or 2 intermittent doses in 24 hours Duration of infusion: 58 hours Dose: 130 mcg/hr Fentanyl clearance Fentanyl pharmacokinetics in critically ill were affected by severe liver disease, congestive heart failure, and weight Chronic kidney disease did not affect fentanyl clearance Choi L. Crit Care Med. 2016; 44: MFMER slide-58
59 Transitioning to Oral Agents Methadone NMDA receptor antagonist QTc prolongation Long half life titrate cautiously Enteral methadone decreased weaning time from mechanical ventilation Oxycodone Schedule doses to wean from sedation and analgesia for weaning from mechanical ventilation Wanzuita R. Crit Care. 2012;16:R MFMER slide-59
60 Multimodal Pain Agents Acetaminophen Enteral absorption in critically illness? Cost of IV acetaminophen Gabapentin Pregabalin Neuropathic pain Limited literature in critically ill patients Guillain-Barré and post-cabg patients Ketamine NMDA receptor antagonist Option for analgosedation NSAIDS Bleeding risk Kidney injury Dexmedetomidine Clonidine α2 adrenergic receptor agonist Provides sedation and analgesia Patanwala AE. J Intensiv Care Medicine. 2017;31:124. Borde DP. J Cardiothorac Vasc Anesth. 2017;31:124. Pandey CK. Anesh Analg. 2002;95: Barr J. Crit Care Med. 2013; 41: MFMER slide-60
61 What About the Opioid Epidemic? 2015 MFMER slide-61
62 Strategies to Treat and Prevent Pain Assess pain BPS and/or RASS at goal No Yes Fentanyl mcg IV push OR Hydromorphone 0.5-2mg IV push Continue to reassess Yes At RASS and BPS goal with 2-3 boluses No Fentanyl mcg/hr OR Hydromorphone mg/hr with PRN bolus doses for BPS not at goal Yes Undersedated Propofol, dexmedetomidine, midazolam RASS at goal No Oversedated Reduce dose of analgesic
63 Roles in Treating & Preventing Pain Optimal drug selection Ensure BPS and RASS monitoring Pain Treatment & Prevention Education Multidisciplinary collaboration on hospital protocols Assess pain on rounds daily 2015 MFMER slide-63
64 EO is a 83 year old male admitted to the medical ICU with septic shock and respiratory failure. He is on day 2 of mechanical ventilation. He is currently on propofol 50 mcg/kg/min and fentanyl 25 mcg/hr. His BPS score is a 6 and his RASS score is a +1. He is being treated with antibiotics for a pneumonia and he is currently on a norepinephrine infusion at 0.4 mcg/kg/min and a vasopressin infusion at 0.04 units/min. Which of the following options would be best to improve EO s pain management? A. Add acetaminophen 1000mg Q6H via Gtube B. Increase propofol to 70 mcg/kg/min C. Switch propofol to midazolam D. Increase fentanyl to 100 mcg/hr ICU intensive care unit BPS Behavioral Pain Scale RASS Richmond Agitation Sedation Scale 2015 MFMER slide-64
65 Unanswered Questions Difficult patient populations Opioid addiction after ICU admission Patient recollection and reconstructed memories 2015 MFMER slide-65
66 Summary There are deleterious effects of untreated pain Pain should be routinely assessed and documented with reliable and validated tools Routine ICU procedures and cares cause patients pain, and pre-emptive treatment should be considered and provided Analgosedation should be the foundation of pain and agitation management in the ICU Multidisciplinary approach for individualized pain management 2015 MFMER slide-66
67 Questions & Discussion 2015 MFMER slide-67
68 Pathway to Pain Control Assessing, Preventing, and Managing Pain in the Intensive Care Unit Caitlin S. Brown, PharmD Brianne M. Ritchie, PharmD, MBA, BCCCP, BCPS Pharmacy Grand Rounds November 21, MFMER slide-68
69 Assessing Pain in the ICU Etiology of Agitation Gas exchange Hypoxemia Hypercarbia Metabolic Hypoglycemia Acidosis Ventilator-related Endotracheal tube malposition Tension pneumothorax Patient-ventilator dysynchrony Inadequate flow rates High or low tidal volumes Ventilator I/E times Pain Surgical/trauma/procedural Baseline pain Routine care/mobilization Infection Central nervous system Sepsis Ischemia Myocardial Intestinal Cerebral Drug and alcohol-related Intoxication Withdrawal Patient positioning in bed Fear and Anxiety Inability to communicate Sleep deprivation Full bladder or colon Drug side effects Anticholinergic Paradoxical response to benzos 2015 MFMER slide-69
70 Managing Pain in the ICU Difficult patient populations Patient population Chronic opioid users ECMO Severe burns Severe brain injury Obesity Obstructive sleep apnea Dementia or cognitive impairment Pediatrics Barriers to management Intrathecal pumps Buprenorphine requires switch to full agonist Tolerance, sensitization, and hyperalgesia Altered pharmacokinetics Mobilization requirements for lung transplant Altered pharmacokinetics Complex pain physiology Assessment of pain symptoms Altered pharmacokinetics Respiratory depression susceptibility Assessment of pain symptoms Altered pharmacokinetics Assessment of pain symptoms 2015 MFMER slide-70

71 Causes of Pain, Agitation, and Delirium 2015 MFMER slide-71
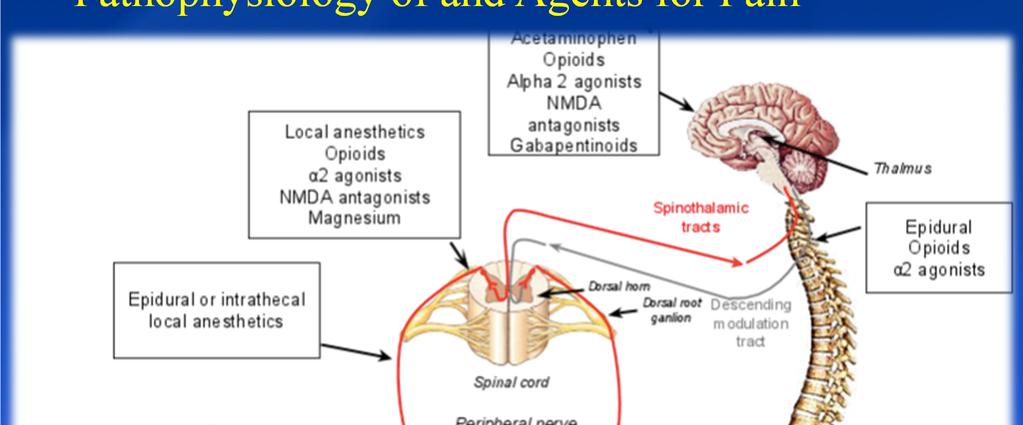
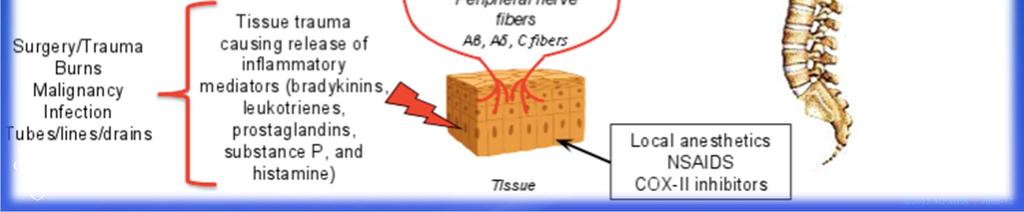
72 Pathophysiology of and Agents for Pain 2015 MFMER slide-72

73 Context-Sensitive Half Life Kim YS. J Neurocrit Care 2015;8: MFMER slide-73
74 Opioid Rotation A change in opioid drug or route of administration with the goal of improving outcomes Literature in cancer and chronic pain patients Mechanism not fully understood Synthetic vs. semi-synthetic Genetic polymorphisms Affinity for different opioid receptors Smith HS. J Pain Research. 2014;7: Fine PG. J Pain Symptom Manag. 2009; 38: MFMER slide-74
75 Opioid Rotation Fentanyl mcg/hr Bolus hydromorphone 2mg Initiate hydromorphone infusion with ~25% reduction 2015 MFMER slide-75
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
KEY REFERENCES laying the foundation for A of ABCDEF bundle
 KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
KEY REFERENCES laying the foundation for A of ABCDEF bundle Puntillo K. Am J Crit Care (Response Procedural Pain) 2001;10:238-251 Payen J. Crit Care Med (Behavioral Pain Scale) 2001;29:2258-2263 Gelinas
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Foundations of Safe and Effective Pain Management
 Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Foundations of Safe and Effective Pain Management Evidence-based Education for Nurses, 2018 Module 1: The Multi-dimensional Nature of Pain Module 2: Pain Assessment and Documentation Module 3: Management
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
SEDATION / ANALGESIA for Brain Failure Patient INASNACC
 SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
SEDATION / ANALGESIA for Brain Failure Patient INASNACC Neuroendocrinological metabolic responses to surgical or traumatic injury Endocrine : increase in ACTH, cortisol, ADH, GH, glucagon, renin, aldosteron,
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México
 Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients
Analgosedation: What Strategy is Best? Guillermo Castorena MD Fundación Clínica Médica Sur México The facts Despite the efforts to optimize sedation and comfort of ICU s patients: More than 50% of patients
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
Sedation and Analgesia in the Critically Ill
 12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
12th Congress of the World Federation of Societies of Intensive and Critical Care Medicine August 29 (Sat.) September 1 (Tue.), 2015 COEX, Seoul, Korea ONE STEP FURTHER: THE PURSUIT OF EXCELLENCE IN CRITICAL
7/6/ ANNUAL MEETING BRINGING THE ABC(DEF) S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES
 S TO THE ICU ICU TRIAD DISCLOSURE ICU TRIAD SEDATION AND ANALGESIA OBJECTIVES") ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
ICU TRIAD BRINGING THE ABC(DEF) S TO THE ICU GINA RIGGI, PHARMD, BCPS, BCCCP CLINICAL HOSPITAL PHARMACIST- TRAUMA INTENSIVE CARE UNIT JACKSON MEMORIAL HOSPITAL MIAMI, FLORIDA Figure 1. Reade M and Finfer
Update on the Management and Monitoring of Deep Analgesia and Sedation in the Intensive Care Unit
 AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
AACN Advanced Critical Care Volume 24, Number 2, pp.101 107 2013, AACN ECG Challenges Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Update on the Management and Monitoring
PAGE 1 OF 8 REFERENCE ORIGINAL ISSUE DATE 06/02 CURRENT EFFECT DATE 04/14. SUBJECT: Patient Care
 [X] & PROCEDURE [ ] PL PAGE 1 OF 8 REFERENCE [ ] All Sharp HealthCare AFFECTED DEPARTMENTS: 327.99 ACCREDITATION: [ ] System Services Outpatient Surgery: [ ] SRS [X] CV-OPS [ ] SCMG [X] GPSC [ ] SHP [X]
[X] & PROCEDURE [ ] PL PAGE 1 OF 8 REFERENCE [ ] All Sharp HealthCare AFFECTED DEPARTMENTS: 327.99 ACCREDITATION: [ ] System Services Outpatient Surgery: [ ] SRS [X] CV-OPS [ ] SCMG [X] GPSC [ ] SHP [X]
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium
 Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
Geriatric Pain Assessment and Management. Robin Arends, DNP, CNP, FNP-BC
 + Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
+ Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
UCSF PAIN SUMMIT /8/15
 UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
UCSF PAIN SUMMIT 2015 5/8/15 Case 3 Geriatric Pain Disclosure Statements UCSF PAIN SUMMIT 2015 Wendy Anderson Patrice Villars 5/8/15 Case 3 Geriatric Pain Pain Management in the Geriatric & End-of-Life
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
 Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
Agitated patient in ICUapproach & management Arjun Srinivasan Agitation Extreme arousal, irritability, excess motor activity driven by internal sense of discomfort such as disease, pain, anxiety and delirium
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces
 16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia
 LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia Carol Long, PhD, RN, FPCN Principal, Capstone Healthcare & Co-Director, Palliative Care for Advanced Dementia, Beatitudes
LUNCH WITH THE EXPERTS: Palliative Care for Advanced Dementia with Pain and Dementia Carol Long, PhD, RN, FPCN Principal, Capstone Healthcare & Co-Director, Palliative Care for Advanced Dementia, Beatitudes
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
1
 Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Pain Module. Opioid-RelatedRespiratory Depression (ORRD)
") Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION
 ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
ANALGESIA AND SEDATION IN MECHANICAL VENTILATION Erik Stoltenberg, MD Abbott Northwestern Hospital February 27, 2018 DISCLOSURE Nothing to disclose AllinaHealthSystem 1 OBJECTIVE To apply knowledge of
Effective Date: August 31, 2006
 SUBJECT: PAIN MANAGEMENT 1. PURPOSE: COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Nursing Care POLICY NUMBER: 317 Effective Date: August 31, 2006 This nursing policy will provide
SUBJECT: PAIN MANAGEMENT 1. PURPOSE: COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION - Nursing Care POLICY NUMBER: 317 Effective Date: August 31, 2006 This nursing policy will provide
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Acute Pain Management in the Opioid Tolerant Patient. Objectives. Opioids. The participant will be able to define opioid tolerance
 Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Improving Pain Management: The UCSF Journey
 Improving Pain Management: The UCSF Journey April 2014 Adam Cooper, RN, MSN Clinical Nurse Educator Institute for Nursing Excellence UCSF Medical Center After this discussion, learners will be able to:
Improving Pain Management: The UCSF Journey April 2014 Adam Cooper, RN, MSN Clinical Nurse Educator Institute for Nursing Excellence UCSF Medical Center After this discussion, learners will be able to:
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
Therapeutic Hypothermia for Post Cardiac Arrest Plan Initial Orders
 Arrest Plan Initial Orders Weight Allergies Therapeutic Hypothermia Guidelines ***Required to continue with ordering Plan.*** Strict Intake and Output q1h, throughout cooling and re warming. Set Up for
Arrest Plan Initial Orders Weight Allergies Therapeutic Hypothermia Guidelines ***Required to continue with ordering Plan.*** Strict Intake and Output q1h, throughout cooling and re warming. Set Up for
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
SEDATION FOR SMALL PROCEDURES
 SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
Validation of the Thai Version Critical Care Pain Observation Tool and Behavioral Pain Scale in Postoperative Mechanically Ventilated ICU Patients
 Validation of the Thai Version Critical Care Pain Observation Tool and Behavioral Pain Scale in Postoperative Mechanically Ventilated ICU Patients J Med Assoc Thai 2017; 100 (Suppl. 7): S9-S19 Full text.
Validation of the Thai Version Critical Care Pain Observation Tool and Behavioral Pain Scale in Postoperative Mechanically Ventilated ICU Patients J Med Assoc Thai 2017; 100 (Suppl. 7): S9-S19 Full text.
DEEP SEDATION TEST QUESTIONS
 Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Labor Epidural: Local Anesthetics and Beyond
 Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure. Supplement 2 Table of Contents
 Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure Supplement 2 Table of Contents RESTORE Algorithm and Box-by-Box Instructions Page 1 of 2
Protocolized Sedation vs Usual Care in Pediatric Patients Mechanically Ventilated for Acute Respiratory Failure Supplement 2 Table of Contents RESTORE Algorithm and Box-by-Box Instructions Page 1 of 2
Chapter 004 Procedural Sedation and Analgesia
 Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
(ADULT) Refer to policy MC.E.48 for neonatal to pediatric pain assessment and management.
 Refer to policy MC.E.48 for neonatal to pediatric pain assessment and management.") Department: Policy/Procedure: PATIENT CARE PAIN ASSESSMENT AND DOCUMENTATION (ADULT) Refer to policy MC.E.48 for neonatal to pediatric pain assessment and management. Definition: Pain can be described
Department: Policy/Procedure: PATIENT CARE PAIN ASSESSMENT AND DOCUMENTATION (ADULT) Refer to policy MC.E.48 for neonatal to pediatric pain assessment and management. Definition: Pain can be described
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Use of PCA devices in Difficult Populations
 Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES
 WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
Part A of this guideline covers the structured assessment and management of pain and sedation.
 Adult Critical Care Pain, Agitation and Delirium (PAD) Guideline ITAPS CMG: Adult Critical Care May 2018 Trust Ref: C24/2018 1. Introduction & Scope The management of analgesia and sedation is pivotal
Adult Critical Care Pain, Agitation and Delirium (PAD) Guideline ITAPS CMG: Adult Critical Care May 2018 Trust Ref: C24/2018 1. Introduction & Scope The management of analgesia and sedation is pivotal
Assessment Algorithm for Sedated Adult ICU Patients
 Assessment Algorithm for Sedated Adult ICU Patients ICU Sedation Guidelines of Care No Rule out/correct reversible causes Use nonpharmacologic treatment Optimize the environment Is patient comfortable
Assessment Algorithm for Sedated Adult ICU Patients ICU Sedation Guidelines of Care No Rule out/correct reversible causes Use nonpharmacologic treatment Optimize the environment Is patient comfortable
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR
 CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
Peri operative pain control. Disclosure. Objectives 9/1/2011. No current conflicts of interest
 Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Sedation is a dynamic process.
 19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory