Pre-Operative Anemia: Common, Consequential and Correctable
|
|
|
- Kristopher Summers
- 6 years ago
- Views:
Transcription
1 Pre-Operative Anemia: Common, Consequential and Correctable Anemia Blood loss and bleeding Triad of independent risk factors for Adverse Outcomes Transfusion
 and Director of Patient Blood Management and Pre-OP Anemia Services, Fairview Southdale Hospital AABB Standards Committee: Patient Blood Management Society for the Advancement of Blood")
2 Credentials and Conflicts of Interest Pathologist (AP/CP/Tx. Med) and Director of Patient Blood Management and Pre-OP Anemia Services, Fairview Southdale Hospital AABB Standards Committee: Patient Blood Management Society for the Advancement of Blood Management (SABM) Iron Corner Expert Panel. AABB/SABM PBM liaison committee Medtronic Speakers Bureau for Rethinking Blood Conservation Chief Medical Officer, Patient Readiness Institute.

3 Fairview Southdale Hospital 350 Beds 1700 total joint procedures/year 350 CV surgery procedures/year Patient Blood Management: 2008 Sustained > 35% reduction all blood components, 2750 fewer red cells/year Pre-Operative Anemia Management:2011



4 Patients deserve all the care they need none they don t, efficiently, effectively and at least cost. Don Berwick, MD

5 Objectives Recognize prevalence of pre-operative anemia Learn impact of pre-operative anemia on postoperative outcomes Review causes and diagnosis of anemia Become familiar with the medical treatments for anemia and their safety/risks Suggest components and some details of a pre-operative anemia management program
6 Anemia WHO definition- Hgb < 12g/dL (f, premenopausal), < 13 g/dl (m) 20% of world population, iron deficiency most common cause Present in 5-75% of Pre-Surgical Patients, varies by surgery type
7 Patients (%) Incidence of Anemia Increases With Age N = 65, WHO anemia definition Men Women > 90 Age (years) Kulier A et al. Anaesthesist. 2001;50:73-86.
8 Herzog CA, Muster HA, Li S, Collins AJ. Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the Medicare population. J Card Fail. 2004;10(6):

9 Pre-Operative Anemia Scope 5-75% of surgical patients 25-30% Elective Joint replacement % CABG > 50 % Valve replacement Greatest Predictor of transfusion Overall a real, but modifiable, problem Significant results-ex. Patient Blood Management Program with pre-operative anemia avoidance component has 5% transfusion rate for elective joint replacements rather 40% in unmanaged programs
10 Anemia in High Blood Loss Surgery Patients: overall 40 +%, 20-30%, Valve replacement 50-65% Numbers are even higher if using > 12 g/dl for females ( STS < 13 for M and F) Women disadvantaged by lower Hgb cutoff in addition to lower body mass, red cell mass and blood volume
11 Meet Your Patient, Mitzi 75 year old spry female Lives independently alone Primary Hip surgery in 3 weeks 135 Lbs Hgb 11.6 gm/dl What is her likelihood of transfusion?
12 Orthopedic Surgery Transfusion Hemoglobin European Overview (OETHEO Study) Transfusion 2003, (43)


13 TRANSFUSION RISK: Score 3: 50% Score 4: 80%
14 Your Patient, Mitzi 75 year old female, P-THA in 3 weeks Hgb 11.6 gm/dl Transfusion likelihood > 40% Does Mitzi have other peri-operative risks than transfusion?
15 Effect of Preoperative Anemia Pre-Surgical anemia alone is associated with increased morbidity and mortality Pre-Surgical anemia is the strongest predictor of need for blood transfusion Blood Transfusion is also associated with increased morbidity and mortality in a dose dependent manner

16 Risk Associated with Preoperative Anemia in Cardiac Surgery: A Multicenter Cohort Study Keyvan Karkouti, et al; Circulation, Jan 2, 2008 Pre-Operative anemia independently associated with adverse outcomes (n= 3500, Hgb < 12.5, 7 hosp, 500 pts each, retrospective) Association independent of transfusions Propensity matched: Death = 51% increase Stroke = 60% increase Acute kidney injury 1 = 80% increase Second most predictive variable after CPB time patients 1 > 100% increase in Creatinine above normal or dialysis Kathrine Frey, MD Fairview Southdale
 Circulation. 2007;116: 471-479.")
17 4804 patients Hgb < 12 with non-cardiac adverse events (renal, cerebral) Hgb < 11 with cardiac component Patients with comorbidities did worse (Euroscore > 4) Circulation. 2007;116:
 Khaled M Musallam et al.")
18 Pre-op Anemia Outcomes in Non CV Surgery Even mild preoperative anemia is independently associated with an increased risk of 30- day morbidity and mortality in patients undergoing major non-cardiac surgery. NSQUIP data base ,425 non emergent Patients 30% Anemic (69,229) Khaled M Musallam et al., Preoperative anaemia and postoperative outcomes in non-cardiac surgery: a retrospective cohort study, Lancet 2011; 378: , Oct 2011
19 Your Patient, Mitzi 75 year old female Primary Hip surgery in 3 weeks 135 Lbs Hgb 11.6 gm/dl Transfusion likelihood > 40% Is blood safe?

20


21 Effect of blood transfusion on long term survival after CV surgery Retrospective study; primary CABG (N=1915) Patients transfused and not transfused in hospital matched by propensity score 5-year mortality: 2x higher in transfused group 5-year mortality (comorbidity correction): remained 70% higher in transfused group (p<.001) This figure was published in Annals of Thoracic Surgery, vol. 74, Engoren MC, et al, Effect of Blood Transfusion on Long Term Survival After Cardiac Operation pages Hospital, , Sept 2014 Elsevier 2002.
 and mortality Serious Hazards of Transfusion,")
22 Blood Transfusion: Avoid when Possible Evidence if compelling that blood transfusion is associated with increased morbidity (surgical site infection, increase ventilator time, renal complications, other lung injury, increased LOS) and mortality Serious Hazards of Transfusion, SHOT
23 Your Patient, Mitzi 75 year old female, P-THA in 3 weeks Hgb 11.6 gm/dl Transfusion likelihood > 40% Anemia and transfusion are undesirable Why could her Hgb be low?
24 Causes of Anemia Decreased Production of RBCs or Hgb Heme: Iron deficiency (absolute, inflammatory, functional) Globin chains: Vitamin B 12, folate, Thal/Hgb-opathy Medications: H2 Blockers, PPI s, some CV meds, anticoagulants Inflammation: Affects Iron and Erythropoietin negatively Marrow Failure: MDS, tumor Increased Red Cell Destruction or Loss Blood loss (GI,GU, GYN) Hemolysis (intra and extravascular)
25 Anemia in Elective Pre-Surgical Population Iron deficiency (30%)- poor diet, blood loss, impaired absorption Anemia of Chronic Disease ( inflammatory iron deficiency) (25%) Chronic Kidney Disease (15-20%) B 12 deficiency (3%) Folate deficiency (5%) Medication related ( inhibited erythropoiesis and/or anticoagulant-associated bleeding) Blood loss- Recent Invasive Procedure ( ex. Angiogram can have 1-2 gm Hgb loss into soft tissues ) Unexplained Anemia of the elderly (UAE) MULTIFACTORIAL (ex. CKD + IDA + Medication components)
26 Iron Restricted Erythropoiesis
27 Absolute Iron deficiency-lack of stored iron Chronic blood loss-can t absorb enough Fe to keep up with losses Diminished intestinal absorption- Celiac Disease, post surgical (bariatric) Diminished intake- Vegetarian Medications- Antacids (H2 blockers, Proton Pump Inhibitors, Tums (Ca2+)
, autoimmune disease, infections Happens")
28 Anemia of Inflammation: Iron Sequestration (decreased iron absorption and bioavailability, Fe present but not accessible) Interleukin 6, increases hepcidin production Impaired enteric absorption Impaired release of storage iron Decreased transferrin, increased ferritin Patients-Chronic inflammatory disease (DM, CHF), autoimmune disease, infections Happens postoperatively too
29 Functional Iron deficiency Patient receiving erythropoietin therapy or with increased endogenous erythropoietin may have iron on board but the speed of red cell production drive outpaces body s ability to release stored iron. Transferrin saturation decreases within one week of initiation of ESA therapy

30 Iron Restricted Erythropoiesis
31 Your Patient, Mitzi 75 year old female, P-THA in 3 weeks, Hgb 11.6 gm/dl Transfusion likelihood > 40% Anemia and transfusion are undesirable What additional lab tests are needed?


32 Lab Testing Initial Panel CBC (need more than just Hgb) Reticulocyte count Creatinine with GFR Serum Iron, % saturation TIBC Ferritin Add on tests as needed CRP (i) Red cell folate Serum B12 Soluble transferrin receptor Reticulocyte Hgb LDH Haptoglobin DAT Differential blood morphology Type and Screen Hepcidin (future)
 increased, medical history chronic disease/inflammation Renal failure associated, normocytic, Cr > 1.")
33 Anemias Absolute Iron deficiency- normocytic or microcytic, % saturation < 20% Ferritin < 100, increased RDW, increased plts ( sometimes) Inflammatory Iron Sequestration- normocytic, % sat < 20 %, Ferritin > 100, CRP (i) increased, medical history chronic disease/inflammation Renal failure associated, normocytic, Cr > 1.2, GFR 59 or < Thalassemia-microcytic, erythrocytosis, nl iron studies or increased iron
, treat with oral iron with Vitamin C Iron deficiency anemia- initially normocytic, as severity increased,")
34 Iron Deficiency- Anemia is Late Stage, Microcytosis is Even Later Iron depletion: near absent storage iron, no anemia, asymptomatic, treat with oral iron with Vitamin C Iron deficiency without anemia-stored and blood borne iron below normal, can be asymptomatic or symptomatic (fatigue), treat with oral iron with Vitamin C Iron deficiency anemia- initially normocytic, as severity increased, microcytic
35 Your Patient, Mitzi 75 y/o female, P-THA 3 weeks Transfusion likelihood > 40% Anemia and transfusion are undesirable Hgb 11.6, retic 1.1%, Cr 1.2, GFR 46, % saturation 32, Ferritin 90


36 Mitzi- Hgb 11.6, retic 1.1% % sat 23, Ferritin 90 Cr 1.2, GFR 46
37 Your Patient, Mitzi 75 y/o female, 135 lbs, P-THA 3 weeks Hgb 11.6, retic 1.1%, Cr 1.2, GFR 46, % saturation 23, Ferritin 90 Diagnosis: Mild anemia w/o regeneration, CKD Stage 3, with low iron stores What does treatment include and what is timeframe for improvement? Is treatment safe?
38 Anemia Treatment Safely increase Hgb gm/week Treatment Options: IV iron, enteric iron, Erythropoietin stimulating agents (ESA s), Vitamin B-12, folate, treat co-morbidities, delay and defer IV iron, effect at 1 week, max effect at 2 weeks, several doses needed (1 gram divided dose common) ESA action onset 4-6 days, max at 10 days, must give with iron to avoid functional iron deficiency
39 Conditions treated and agents: IDA (absolute iron deficiency)- IV iron effect at 1 week, Iron effect, max at 2 weeks, several doses needed ( 1 gram divided dose common) Anemia of chronic disease/inflammation- IV iron (despite high ) and sub Q erythropoietin, EPO action onset 4-6 days, max at 10 days Renal failure associated- Sub Q Epo and IV iron, correct iron stores prior to starting ESA
, short timeframe to surgery. Give with Vitamin C. Parenteral - few adverse drug events. Overall 3/1M doses, life threatening 0.")
40 IRON- the heavy lifter of anemia management Enteric - lower cost, slow response, 30-40% of patients have GI intolerance, poor absorption in tolerant patients (antacids, gastritis, other malabsorption, inflammatory conditions), short timeframe to surgery. Give with Vitamin C. Parenteral - few adverse drug events. Overall 3/1M doses, life threatening 0.6/1M doses, common reactions are urticarial, flushing and hypotension
41 IV iron dosing mg Iron for each gm/dl hgb deficit Plus mg to replace true iron stores if tsat < 10 (regardless of ferritin) OR tsat < 20 AND ferritin < 100 ng/dl Normal hgb + decreased Ferritin [100 ferritin] x 10 Acute blood loss mg per cc

42
43 Erythropoietin 165 amino acid glycoprotein hormone synthesized primarily in the kidneys ( adult 9:1 kidney:liver). Recombinant forms for patient care. Primary role involves the programmed cell death of red cell precursors. It induces red cell production by promoting production and differentiation of red cells from their progenitor cells. EPO also exerts a protective role against tissue ischemia by activating biochemical mechanisms that provide anti-apoptotic anti-oxidative and antiinflammatory response to hypoxia
44 Effective for Pre-Operative anemia Check CMS guidelines - Elective Hip and Knee surgery HCTS < 39 Not on label for CV or vascular surgery CKD Stage 3 and > and HCTS < 30 or symptomatic with ending Hcts 36 Patient can t be Iron deficient at start of treatment - Give iron with ESA Goodenough Transfusion 34:66-71, 1994 J Thorac Cardiovasc Surg 2001;122: Sowade Blood :
45 European Epoetin Alfa Surgery Trial Orthopedics: Multicenter trial EPO v routine (6 countries- 700 pts) Anemic pts hgb g/dl EPO 40 Iu/ kg/wk x 3 + DOS + iron both groups (oral treatment/iv or oral control) Results: higher hgb levels throughout 12% v. 46% transfusion No effect post op recovery (time ambulation, d/c, infection rate Time to ambulation, d/c longer in transfused v. non-transfused Side Effects comparable Hospital, Sept 2014 Weber, Eur J Anaesthesiol April 2005;22(4):
46 EPO and Thrombosis RCT 680 spine pts 600 u/kg x 4 doses (1 per week x 4 weeks) vs. standard of care Rate all DVT by doppler on POD 4 only Greater in EPO than control (4.7 v 2.1) Rate of symptomatic DVT same for both groups Post hoc analysis of combined PE + DVT same for both groups Only mechanical DVT prophylaxis post op (joint replacement patients use anticoagulants as well) Basis for thromboprophylaxis Spine 2009; 34: Spine 2009; 34SSSpine 2009; 34: :
47 D Ambra. Ann Thorac Surg 1997; 64: Basis for the FDA exclusion of ESA for use in CV surgery 182 patients randomized to 150 or 300 IU/Kg of EPO or placebo Pre-Op day 5, DOS and POD 2 after CABG (8 doses) Trend toward increased mortality in treatment groups (p=.06) 4/5 deaths possibly drug related due to thrombotic or vascular events 2/4 deaths were > 3 months post op No deaths in the placebo group No difference in non-fatal complications in the treated and placebo groups
48 D Ambra. Ann Thorac Surg 1997; 64: Study not applicable for pre-operative anemia, transfusion reduction was measurement (not beneficial) Mean baseline Hgb /- 1 gm/dl in 3 groups 89% male, 94% CABG Attempt to exclude iron deficiency but parameters were Ferritin < 20, % Sat 16 91% hematologically normal Basis for the FDA exclusion of ESA for use in CV surgery
49 Preoperative very short-term, high-dose erythropoietin administration diminishes blood transfusion rate in off-pump coronary artery bypass: A randomized blind controlled study Prospective European Study, 320 consecutive CAB only pts, 158 got ESA, 162 controls EPO 14,000 IU Pre OP Days 2 and 1; 8,000 IU DOS and 8,000 IU POD 1 and 2 (5 doses) Given to patients unless Hgb >14.5 or Cr > 2 Endpoint transfusion POD 4 Hgb 15.5% higher in treatment group, less blood needed/tx No adverse events related to ESA use but short follow up, no differences in 45 day mortality Patients with most benefit noted to be those with anemia Weltert,L. J Thorac Cardiovasc Surg 2010;139:621-7
50 Effects of Preoperative Intravenous Erythropoietin Plus Iron on Outcome in Anemic Patients After Cardiac Valve Replacement (Spain) 75 consecutive patients- EPO + IV iron x 5 doses 59 observational cohort Post op morbidity OR 0.13 p = In hospital mortality OR 0.16 p = 0.04 Decreased postop renal failure OR 0.23 p = 0.03 Transfusion rate 67 v 93% p=0.01 LOS (median) 10 v 15 p Adjusted for Operative Risk Score, type of intervention, time of CPB, year of surgery Hospital, Sept 2014 Cladellas M, Am J Cardiol 2012;110:
51 Role of ESA Therapy in Cardiac Surgery Goodenough L. et al. Update on erythropoiesis-stimulating agents. Best Practice & Research Clinical Anesthesiology 27 (2013) Unresolved Question Valuable tool for patients with special requirements such as Jehovah s Witness. In selected populations such as off pump CABG. short-term, high dose ESA has been shown to diminish blood transfusion rates. Until additional safety data are forthcoming, the off label use of ESA in patients undergoing cardiac or vascular surgery in the US cannot be recommended.
52 On warnings, Patient signs Informed ESA- black box o Increased mortality, o Serious cardiovascular and thrombo-embolic events Consent for ESA Rx. o Increased mortality and/or o Increased risk of tumor progression or recurrence If there were a black box for red cell transfusion o Increased mortality, o Lung injury o Circulatory overload o Tumor progression recurrence o Infection o Thrombo-embolic events o Hemolysis o Renal failure and o Allergic reactions.
53 ESA Dosing Only one ESA approved for pre-surgical use, joint replacement and Jehovah s Witness u/kg/week for 4 weeks
54 Presurgical EPO - summary Use with caution CKD, malignancy, h/o VTE Use Lowest dose (with IV iron!) Consider Thromboprophylaxis high risk pts
55 Your Patient, Mitzi 75 y/o female, P-THA 3 weeks Hgb 11.6, retic 1.1%, Cr 1.2, GFR 46, % saturation 23, Ferritin 90 Diagnosis: Mild anemia w/o regeneration, CKD Stage 3, borderline low iron stores, having joint replacement (ESA on label) Treatment: ESA x 2 with IV iron 600 mg in divided 300 mg doses, gave iron before starting ESA How did she do?
56 75 y/o female, P-THA 3 weeks, Mild anemia w/o regeneration, CKD Stage 3, borderline low iron stores Treatment: ESA x 2 with IV iron 600 mg in divided 300 mg doses, gave iron before starting ESA Initial Labs: Hgb 11.6, retic 1.1%, Cr 1.2, GFR 46, % saturation 23, Ferritin 90 Day of Surgery Labs: Hgb 13.5, retic 3.4% Not transfused, lowest Hgb in hospital 10.2, LOS 3 days
57 Pre-Operative Anemia Evaluation Current process- None Patient to PCD* when convenient or directed PCD likely doesn t see anemia as problem Transfusion might be needed (blood is safe) Surgery already scheduled *PCD=Primary Care Doctor Better process- Anemia evaluation start when surgery need identified Patient to PCD for early pre op including anemia eval with Hgb target Patient to Anemia program that does this and hands patient into PCD/Hospital with best red cell mass
58 Role and Responsibilities of a Pre-Surgical Anemia Management Program To provide best surgical outcome for patients Reliably identify and distinguish treatable and triage-worthy anemic patients (PCD, Heme, GI) Provide effective and reimbursable treatment recommendations and treatment Reliably communicate findings (to Surgeon, PCD, Patient)
59 Pre-Operative Anemia Programs- DON T serve as chronic anemia management services. DON T eliminate need for hematologist services at times. DON T provide for care other than for anemia.
60 Patient Enrollment Options Directed by Primary Care Providers Directed by Surgeons Sub component of Pre-Operative Clinic program, for certain procedures Directed from surgery schedule, cases 3+ weeks out, certain DRGs Enrollment options - ad hoc consult or pre-surgical requirement
61 Personnel Needed Medical Director, generally part time in conjunction with primary specialty (Pathologist, Anesthesiologist, Hospitalist, Hematologist, Other) Nurse(s) Administrative Assistant IT support



62 Anemia Screening and Diagnosis Medical history and current medications Surgical procedure and timeframe

63 Lab Testing: Use an Algorithm Draw enough blood initially for follow on tests PCD made aware of any abnormalities. Patient sent to PCD for anemia not in keeping with medical history, Hgb < 10, multiple hematologic abnormalities, etc.
64 Anemia Treatment Use standardized order sets, including coding for pharmacy approval and reimbursement IV iron is the most commonly used agent ESA use: Non CV or vascular surgery, anemia's with inflammatory or renal components, no autologous blood donation, check state CMS rules Patients getting ESA need concomitant iron and DVT prophylaxis in hospital

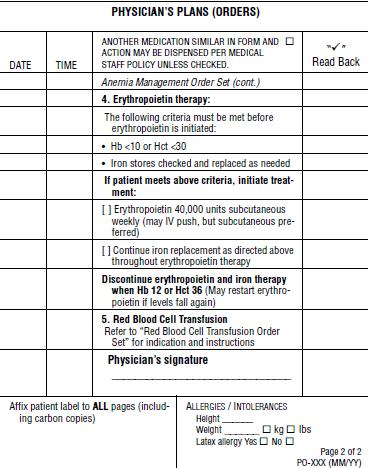
65 Sample Order Set for Pre-Operative Anemia Management
66 Rules, Regulations, and Logistics Labs- CMS doesn't reimburse for labs >30 days from surgery, evaluate patient with known anemia ASAP as anemic patient rather than pre-surgical. Medications-strict rules for use of iron with lab test evidence and proper coding. Same for Erythropoietin and also black box warnings and patient informed consent needed. ESA- Black Box, increased mortality, serious cardiovascular and thromboembolic events, and/or increased risk of tumor progression or recurrence Black Box for red cell transfusion - increased mortality, lung injury, circulatory overload, tumor progression or recurrence, infection, thrombo-embolic events, hemolysis, renal failure and allergic reactions.
67 Costs Every red cell unit NOT TRANSFUSED saves the hospital $ ( component not transfused and no procedure costs) Iron therapy safe and reimbursed ESA therapy on label safe and reimbursed
68 Patient Blood Management Performance Measures (2011) PBM 6: Pre-Operative Anemia Formal protocols for preoperative testing of Hgb for potential high-blood loss elective surgeries would be used to identify and intervene for optimal management of blood resources. Early recognition of anemia offers patients an opportunity to receive the most appropriate transfusion-sparing strategy and avoid the risk of a potential transfusion. Use in elective surgical patients for whom blood transfusion is a probability (defined as any procedure for which a preoperative blood type and crossmatch is requested). Test a minimum of 30 days before the scheduled procedure
69 Pre-Operative Anemia: Summary Prevalence: 25% Ortho, 25% CABG, 50% valve surgery Consequences: Increased M&M even if mild anemia (hgb 10-12) and if no transfusion Transfusion Consequences: Increased M&M, dose dependent Anemia Causes: Iron restricted hematopoiesis (absolute, inflammatory, functional), renal disease, medications, multifactorial Anemia Diagnosis: Standard lab panel with add on tests and an algorithm Anemia Treatment: On label IV iron (most common tx.) and ESA safe and effective, use order sets, consider thrombo-prophylaxis for ESA, when using ESA iron replacement is also needed Who evaluate: All elective patients needing T & C on SBOS, Expected blood loss > 300 ml with 3 or > weeks to surgery Communication imperative, especially with PCD with any anemic patient
70 References Goodenough LT et al. Detection, evaluation, and management of pre-operative anemia in the elective orthopaedic surgical patient: NATA guidelines. Br J Anaesth 106 (1):13-22 (2011) Goodenough, LT and Shander, A. Current Status of Pharmacologic Therapies in Patient Blood Management. Anesth Analg 2013; 116 : Goodenough, LT. Iron deficiency syndromes and iron restricted erythropoiesis. Transfusion 2012;52:
Peri-Surgical Anemia and the TAVR Patient
 Peri-Surgical Anemia and the TAVR Patient Kathrine P Frey, MD Fairview Southdale Hospital Director of Blood and Pre-Operative Anemia Management April, 2015 MIDWEST VALVE SYMPOSIUM, April 2015 Credentials
Peri-Surgical Anemia and the TAVR Patient Kathrine P Frey, MD Fairview Southdale Hospital Director of Blood and Pre-Operative Anemia Management April, 2015 MIDWEST VALVE SYMPOSIUM, April 2015 Credentials
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD
 Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
HMO: Medical (provider setting); Rx (out patient) PPO/CDHP: Rx
; Rx (out patient) PPO/CDHP: Rx") BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Epogen, Procrit (epoetin alfa, injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Epogen, Procrit (epoetin alfa, injection) Commercial HMO/PPO/CDHP
Anemia Management: Using Epo and Iron
 Anemia Management: Using Epo and Iron Ky Stoltzfus, MD University of Kansas Medical Center Assistant Professor Department of Internal Medicine January 23, 2013 Regulation of red cell production Treatment
Anemia Management: Using Epo and Iron Ky Stoltzfus, MD University of Kansas Medical Center Assistant Professor Department of Internal Medicine January 23, 2013 Regulation of red cell production Treatment
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON
 IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
Epogen / Procrit. Epogen / Procrit (epoetin alfa) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University
 Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
10/15/2015. Clinical Utility of Immature Cell Indices DISCUSSION POINTS HEALTHCARE REFORM PAYMENT MODEL EXPERIMENTS
 Clinical Utility of Immature Cell Indices Leveraging Technology to Help Manage Anemia and Blood Utilization donnellyj@sysmex.com 2015 Sysmex America, Inc. All rights reserved. For Clinical Support Team
Clinical Utility of Immature Cell Indices Leveraging Technology to Help Manage Anemia and Blood Utilization donnellyj@sysmex.com 2015 Sysmex America, Inc. All rights reserved. For Clinical Support Team
Emerging Evidence On Anemia
 Emerging Evidence On Anemia Evidence, Education, and Better Patient Outcomes www.sabm.org Provided by the Society for the Advancement of Blood Management, Inc., a nonprofit corporation. 35 Engle Street,
Emerging Evidence On Anemia Evidence, Education, and Better Patient Outcomes www.sabm.org Provided by the Society for the Advancement of Blood Management, Inc., a nonprofit corporation. 35 Engle Street,
Aranesp. Aranesp (darbepoetin alfa) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.01 Subject: Aranesp Page: 1 of 6 Last Review Date: September 15, 2017 Aranesp Description Aranesp
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.01 Subject: Aranesp Page: 1 of 6 Last Review Date: September 15, 2017 Aranesp Description Aranesp
Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN
 Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN Professor of Medicine Director, Division of Nephrology and Hypertension University of Oklahoma College of Medicine Definition
Anemia Management in Peritoneal Dialysis Patients Pranay Kathuria, FACP, FASN Professor of Medicine Director, Division of Nephrology and Hypertension University of Oklahoma College of Medicine Definition
ANEMIA IN THE PRE-SURGICAL PATIENT
 ANEMIA IN THE PRE-SURGICAL PATIENT Recognition, Diagnosis, and Management New Insights and Concepts for the Primary Care Provider Anemia is a significant and modifiable risk factor for increased perioperative
ANEMIA IN THE PRE-SURGICAL PATIENT Recognition, Diagnosis, and Management New Insights and Concepts for the Primary Care Provider Anemia is a significant and modifiable risk factor for increased perioperative
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients
 Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients Ellinor I. Peerschke, Ph.D., F.A.H.A. Vice Chair, Laboratory Medicine Chief, Hematology & Coagulation Laboratory Services Memorial Sloan Kettering
Utilizing Sysmex RET He to Evaluate Anemia in Cancer Patients Ellinor I. Peerschke, Ph.D., F.A.H.A. Vice Chair, Laboratory Medicine Chief, Hematology & Coagulation Laboratory Services Memorial Sloan Kettering
Anemia in the elderly. Nattiya Teawtrakul MD., PhD
 Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Medication Prior Authorization Form
 Procrit, Aranesp and (Epoetin Alfa) Policy Number: 1043 Policy History Approve Date: 12/11/2015 Effective Date: 12/11/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not
Procrit, Aranesp and (Epoetin Alfa) Policy Number: 1043 Policy History Approve Date: 12/11/2015 Effective Date: 12/11/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not
ANEMIA IN THE PRE-SURGICAL PATIENT
 ANEMIA IN THE PRE-SURGICAL PATIENT RECOGNITION, DIAGNOSIS AND MANAGEMENT New Insights and Concepts for the Primary Care Provider Anemia is a significant and modifiable risk factor for increased perioperative
ANEMIA IN THE PRE-SURGICAL PATIENT RECOGNITION, DIAGNOSIS AND MANAGEMENT New Insights and Concepts for the Primary Care Provider Anemia is a significant and modifiable risk factor for increased perioperative
27/01/2019. Anaemia, Transfusion and TACO Lise Estcourt. Anaemia. What is anaemia?
 Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
Advances in Transfusion and Blood Conservation
 Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Anaemia & Cancer. John de Vos Consultant Haematologist RSCH
 Anaemia & Cancer John de Vos Consultant Haematologist RSCH overview Definitions & setting the scene Causes Consequences Biology Treatment Personal approach Patient Clinical team Anaemia - Definition :
Anaemia & Cancer John de Vos Consultant Haematologist RSCH overview Definitions & setting the scene Causes Consequences Biology Treatment Personal approach Patient Clinical team Anaemia - Definition :
Anaemia in the ICU: Is there an alternative to using blood transfusion?
 Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Anaemia in the ICU: Is there an alternative to using blood transfusion? Tim Walsh Professor of Critical Care, Edinburgh University World Health Organisation grading of the severity of anaemia Grade of
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Conversion Dosing Guide:
 Conversion Dosing Guide: From epoetin alfa to Aranesp in patients with anemia due to CKD on dialysis Indication Aranesp (darbepoetin alfa) is indicated for the treatment of anemia due to chronic kidney
Conversion Dosing Guide: From epoetin alfa to Aranesp in patients with anemia due to CKD on dialysis Indication Aranesp (darbepoetin alfa) is indicated for the treatment of anemia due to chronic kidney
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA)
") AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA) Drugs Covered Procrit Epogen Aranesp Authorization guidelines For patients who meet all of the following: Does
AETNA BETTER HEALTH Prior Authorization guideline for Erythropoiesis Stimulating Agents (ESA) Drugs Covered Procrit Epogen Aranesp Authorization guidelines For patients who meet all of the following: Does
Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017
 Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017 John Strouse, MD, PhD Instructor (temp) Medicine and Pediatrics Director, Adult Sickle Cell Program April 20, 2017 1 Disclosures I have no
Oral Iron Safe, Effective, and Misunderstood Duke Debates 2017 John Strouse, MD, PhD Instructor (temp) Medicine and Pediatrics Director, Adult Sickle Cell Program April 20, 2017 1 Disclosures I have no
Drugs Used in Anemia
 Drugs Used in Anemia Drugs of Anemia Anemia is defined as a below-normal plasma hemoglobin concentration resulting from: a decreased number of circulating red blood cells or an abnormally low total hemoglobin
Drugs Used in Anemia Drugs of Anemia Anemia is defined as a below-normal plasma hemoglobin concentration resulting from: a decreased number of circulating red blood cells or an abnormally low total hemoglobin
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
Iron Deficiency Anaemia but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service
 Iron Deficiency but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service 1 3 Questions 1. Is anaemia incurable in my patient? 2. Is anaemia unavoidable in my bleeding patient? 3. Is
Iron Deficiency but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service 1 3 Questions 1. Is anaemia incurable in my patient? 2. Is anaemia unavoidable in my bleeding patient? 3. Is
Erythropoiesis Stimulating Agents (ESAs): Epoetin Alfa * DIALYSIS *
: Epoetin Alfa * DIALYSIS *") Erythropoiesis Stimulating Agents (ESAs): Epoetin Alfa * DIALYSIS * DESCRIPTION Erythropoietin is a glycoprotein produced in the kidneys responsible for the stimulation of red blood cell production. Epoetin
Erythropoiesis Stimulating Agents (ESAs): Epoetin Alfa * DIALYSIS * DESCRIPTION Erythropoietin is a glycoprotein produced in the kidneys responsible for the stimulation of red blood cell production. Epoetin
Objectives. Current WHO Definition of Anemia. Implication for Clinical Practice 10/8/18. Prevalence of Iron Deficiency in Women Undergoing Surgery
 Pre-operative Anemia Clinic Dr Mike Scott MB ChB FRCP FRCA FFICM Professor in Anesthesiology and Critical Care Medicine Divisional Lead for Critical Care Medicine VCU Health System, Richmond, VA Professor
Pre-operative Anemia Clinic Dr Mike Scott MB ChB FRCP FRCA FFICM Professor in Anesthesiology and Critical Care Medicine Divisional Lead for Critical Care Medicine VCU Health System, Richmond, VA Professor
Stages of chronic kidney disease
 For mass reproduction, content licensing and permissions contact Dowden Health Media. Jonathan J. Taliercio, DO Department of Nephrology and Hypertension, Cleveland Clinic, Cleveland, Ohio talierj@ccf.org
For mass reproduction, content licensing and permissions contact Dowden Health Media. Jonathan J. Taliercio, DO Department of Nephrology and Hypertension, Cleveland Clinic, Cleveland, Ohio talierj@ccf.org
No Disclosures 03/20/2019. Learning Objectives. Renal Anemia: The Basics
 Renal Anemia: The Basics Meredith Atkinson, M.D., M.H.S. Associate Professor of Pediatrics Johns Hopkins School of Medicine 16 March 2019 No Disclosures Learning Objectives At the end of this session the
Renal Anemia: The Basics Meredith Atkinson, M.D., M.H.S. Associate Professor of Pediatrics Johns Hopkins School of Medicine 16 March 2019 No Disclosures Learning Objectives At the end of this session the
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
To report SUSPECTED ADVERSE REACTIONS, contact Hospira, Inc., a Pfizer company, at , or FDA at FDA-1088 or
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RETACRIT safely and effectively. See full prescribing information for RETACRIT. RETACRIT (epoetin
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use RETACRIT safely and effectively. See full prescribing information for RETACRIT. RETACRIT (epoetin
ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE
 ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE WEIQIANG GAO HEM/ONC FELLOW FACULTY DISCUSSANT SIOBAN KEEL, MD OCT. 24, 2014 CASE PRESENTATION 25 F, a Jehovah s witness, w/ h/o synovial sarcoma
ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE WEIQIANG GAO HEM/ONC FELLOW FACULTY DISCUSSANT SIOBAN KEEL, MD OCT. 24, 2014 CASE PRESENTATION 25 F, a Jehovah s witness, w/ h/o synovial sarcoma
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED
 INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
SYNOPSIS. Issue Date: 04 February 2009 Document No.: EDMS -USRA
 SYNOPSIS Issue Date: 04 February 2009 Document No.: EDMS -USRA-10751204 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Johnson & Johnson Pharmaceutical Research & Development,
SYNOPSIS Issue Date: 04 February 2009 Document No.: EDMS -USRA-10751204 Name of Sponsor/Company Name of Finished Product Name of Active Ingredient(s) Johnson & Johnson Pharmaceutical Research & Development,
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only.
 The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
The clinical trial information provided in this public disclosure synopsis is supplied for informational purposes only. Please note that the results reported in any single trial may not reflect the overall
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia 1: Fourth year Medical Students/ Feb/22/ Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor
 Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
The Changing Clinical Landscape of Anemia Management in Patients With CKD: An Update From San Diego Presentation 1
 Presentation 1 The following is a transcript from a web-based CME-certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational grants
Presentation 1 The following is a transcript from a web-based CME-certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational grants
Updates in the Management of Anemia in Cancer. Taylor M. Ortiz, MD May 19, 2017
 Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Management of anemia in CKD
 Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
ORBcoN Spring Symposium April 2015
 ORBcoN Spring Symposium April 2015 CFPC CoI Templates: Slide 1 Faculty: Gail Murray Relationships with commercial interests: Former Member of the Advisory Board 2012 with Takeda Canada for Feraheme CFPC
ORBcoN Spring Symposium April 2015 CFPC CoI Templates: Slide 1 Faculty: Gail Murray Relationships with commercial interests: Former Member of the Advisory Board 2012 with Takeda Canada for Feraheme CFPC
Topic owner: Mollie Grow MD MPH, updated June 2018
 Iron deficiency Anemia UW Pediatrics Outpatient Clinical Guidelines Sources: AAP Clinical Report Diagnosis and Prevention of Iron Deficiency and Iron- Deficiency Anemia in Infants and Young Children (0
Iron deficiency Anemia UW Pediatrics Outpatient Clinical Guidelines Sources: AAP Clinical Report Diagnosis and Prevention of Iron Deficiency and Iron- Deficiency Anemia in Infants and Young Children (0
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
PROCRIT (epoetin alfa) for Injection
 for Injection") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PROCRIT safely and effectively. See full prescribing information for PROCRIT. PROCRIT (epoetin alfa)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PROCRIT safely and effectively. See full prescribing information for PROCRIT. PROCRIT (epoetin alfa)
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Patient Blood Management. Marisa B. Marques, MD UAB Department of Pathology November 17, 2016
 Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Preparing for Patients at High Risk of Transfusion
 18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
Perioperative VTE Prophylaxis
 Perioperative VTE Prophylaxis Gregory J. Misky, M.D. Assistant Professor of Medicine University Of Colorado Denver You recommend the following 72 y.o. man admitted for an elective R hip repair. Patient
Perioperative VTE Prophylaxis Gregory J. Misky, M.D. Assistant Professor of Medicine University Of Colorado Denver You recommend the following 72 y.o. man admitted for an elective R hip repair. Patient
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
ARANESP (darbepoetin alfa) injection, for intravenous or subcutaneous use Initial U.S. Approval: 2001
 injection, for intravenous or subcutaneous use Initial U.S. Approval: 2001") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use ARANESP safely and effectively. See full prescribing information for ARANESP. ARANESP (darbepoetin
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use ARANESP safely and effectively. See full prescribing information for ARANESP. ARANESP (darbepoetin
5/1/2017 DISCUSSION POINTS. Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN
 DISCUSSION POINTS Importance of hematological immature cell indices Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN Investigate the evidence for clinical utility:
DISCUSSION POINTS Importance of hematological immature cell indices Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN Investigate the evidence for clinical utility:
Summary of Recommendation Statements Kidney International Supplements (2012) 2, ; doi: /kisup
 2, ; doi: /kisup") http://www.kidney-international.org & 2012 KDIGO Summary of Recommendation Statements Kidney International Supplements (2012) 2, 283 287; doi:10.1038/kisup.2012.41 Chapter 1: Diagnosis and evaluation of
http://www.kidney-international.org & 2012 KDIGO Summary of Recommendation Statements Kidney International Supplements (2012) 2, 283 287; doi:10.1038/kisup.2012.41 Chapter 1: Diagnosis and evaluation of
RAPID REFERRAL ANEMIA CLINICS
 RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
Patient Blood Management. vs. Dr. Petro-Lize Wessels PBM Consultant SANBS August 2018
 Patient Blood Management vs. Dr. Petro-Lize Wessels PBM Consultant SANBS August 2018 Overview Definition 3 Predictors of negative clinical outcomes 3 Pillars of patient blood management What is my role?
Patient Blood Management vs. Dr. Petro-Lize Wessels PBM Consultant SANBS August 2018 Overview Definition 3 Predictors of negative clinical outcomes 3 Pillars of patient blood management What is my role?
Martin Besser Consultant Haematologist Papworth Hospital
 Martin Besser Consultant Haematologist Papworth Hospital Important modifiable risk factor for morbidity and mortality in all forms of surgery (Australian PBM guidelines) 140g/l 100g/l 80g/l Patients should
Martin Besser Consultant Haematologist Papworth Hospital Important modifiable risk factor for morbidity and mortality in all forms of surgery (Australian PBM guidelines) 140g/l 100g/l 80g/l Patients should
Evolving Evidence on Anemia, Transfusion, Intravenous Iron and Pa8ent Outcomes
 Evolving Evidence on Anemia, Transfusion, Intravenous Iron and Pa8ent Outcomes A Need for Updated Intravenous Iron Coverage Irwin Gross M.D. Aryeh Shander M.D. Michael Auerbach M.D. Overview Requested
Evolving Evidence on Anemia, Transfusion, Intravenous Iron and Pa8ent Outcomes A Need for Updated Intravenous Iron Coverage Irwin Gross M.D. Aryeh Shander M.D. Michael Auerbach M.D. Overview Requested
Evidence-Based Hematological Solutions
 Evidence-Based Hematological Solutions Beyond the Routine CBC Objectives Describe novel hematology parameters and their derivation. Investigate the evidence for their clinical utility. Discuss how new
Evidence-Based Hematological Solutions Beyond the Routine CBC Objectives Describe novel hematology parameters and their derivation. Investigate the evidence for their clinical utility. Discuss how new
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
ANEMIA OF CHRONIC KIDNEY DISEASE
 Understanding Your Hemodialysis Access Options UNDERSTANDING ANEMIA OF CHRONIC KIDNEY DISEASE UNDERSTANDING ANEMIA OF CHRONIC KIDNEY DISEASE WHAT IS CHRONIC KIDNEY DISEASE (CKD)? When someone has CKD,
Understanding Your Hemodialysis Access Options UNDERSTANDING ANEMIA OF CHRONIC KIDNEY DISEASE UNDERSTANDING ANEMIA OF CHRONIC KIDNEY DISEASE WHAT IS CHRONIC KIDNEY DISEASE (CKD)? When someone has CKD,
Moderators: Heather A. Nyman, Pharm.D., BCPS Clinical Pharmacist, Dialysis, University of Utah Dialysis Program, Salt Lake City, Utah
 Immunology/Transplantation and Nephrology PRNs Focus Session Long-term Management of the Renal Transplant Recipient Activity No. 0217-0000-11-076-L01-P (Knowledge-Based Activity) Monday, October 17 1:30
Immunology/Transplantation and Nephrology PRNs Focus Session Long-term Management of the Renal Transplant Recipient Activity No. 0217-0000-11-076-L01-P (Knowledge-Based Activity) Monday, October 17 1:30
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
Effective Health Care Program
 Comparative Effectiveness Review Number 83 Effective Health Care Program Biomarkers for Assessing and Managing Iron Deficiency Anemia in Late-Stage Chronic Kidney Disease Executive Summary Background Chronic
Comparative Effectiveness Review Number 83 Effective Health Care Program Biomarkers for Assessing and Managing Iron Deficiency Anemia in Late-Stage Chronic Kidney Disease Executive Summary Background Chronic
Future Direction of Anemia Management in ESRD. Jay B. Wish, MD 2008 Nephrology Update March 20, 2008
 Future Direction of Anemia Management in ESRD Jay B. Wish, MD 2008 Nephrology Update March 20, 2008 The Evidence Normal Hct Study and CHOIR demonstrate adverse outcomes in ESA patients with target Hgb
Future Direction of Anemia Management in ESRD Jay B. Wish, MD 2008 Nephrology Update March 20, 2008 The Evidence Normal Hct Study and CHOIR demonstrate adverse outcomes in ESA patients with target Hgb
PROCRIT DOSAGE AND ADMINISTRATION PROCRIT
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PROCRIT safely and effectively. See full prescribing information for PROCRIT. injection, for intravenous
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PROCRIT safely and effectively. See full prescribing information for PROCRIT. injection, for intravenous
An Oncologist s Approach to Anemia in Adults Christie J. Hilton, DO
 An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
NURSE OR PHARMACIST-LED ANEMIA MANAGEMENT PROTOCOL EDUCATIONAL PACKAGE TABLE OF CONTENTS:
 CANN-NET ANEMIA MANAGEMENT FOR HEMODIALYSIS CENTRES NURSE OR PHARMACIST-LED ANEMIA MANAGEMENT TABLE OF CONTENTS: PROTOCOL EDUCATIONAL PACKAGE Page 2: CANN-NET Anemia Management Protocol: Educational Document
CANN-NET ANEMIA MANAGEMENT FOR HEMODIALYSIS CENTRES NURSE OR PHARMACIST-LED ANEMIA MANAGEMENT TABLE OF CONTENTS: PROTOCOL EDUCATIONAL PACKAGE Page 2: CANN-NET Anemia Management Protocol: Educational Document
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL. Revised May 30, 2012
 CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Managing peri-operative anaemiathe Papworth way. Dr Andrew A Klein Royal Papworth Hospital Cambridge UK
 Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Anemia and Iron Deficiency: What Every Cardiologist Needs to Know
 6th Saudi HF Group Symposium Riyadh - December 8-9, 2017 Anemia and Iron Deficiency: What Every Cardiologist Needs to Know Ammar Chaudhary MBChB, FRCPC Consultant Cardiologist Advanced Heart Failure Department
6th Saudi HF Group Symposium Riyadh - December 8-9, 2017 Anemia and Iron Deficiency: What Every Cardiologist Needs to Know Ammar Chaudhary MBChB, FRCPC Consultant Cardiologist Advanced Heart Failure Department
Literature Scan: Erythropoiesis Stimulating Agents
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Pre-operative Anaemia Colorectal and Orthopaedic Surgery
 Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Multiple case reports of successful use, with only one case report of intra device thrombotic event
 rfviia in VAD Patients Limited data exist regarding safety Multiple factors increase pro thrombotic potential Multiple case reports of successful use, with only one case report of intra device thrombotic
rfviia in VAD Patients Limited data exist regarding safety Multiple factors increase pro thrombotic potential Multiple case reports of successful use, with only one case report of intra device thrombotic
Drug Class Prior Authorization Criteria Erythropoiesis Stimulating Agents (ESAs)
") Drug Class Prior Authorization Criteria Erythropoiesis Stimulating Agents (ESAs) Line of Business: Medicaid P & T Approval Date: May 16, 2018 Effective Date: July 1, 2018 This policy has been developed
Drug Class Prior Authorization Criteria Erythropoiesis Stimulating Agents (ESAs) Line of Business: Medicaid P & T Approval Date: May 16, 2018 Effective Date: July 1, 2018 This policy has been developed
Blood Management of the Cardiac Patient in the Postoperative Period
 Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
RED CELL DISTRIBUTION WIDTH
 RED CELL DISTRIBUTION WIDTH A NEW MARKER OF EXERCISE INTOLERANCE IN PATIENTS WITH CHRONIC HEART FAILURE Emeline Van Craenenbroeck, Paul Beckers, Nadine Possemiers, Christiaan Vrints, Viviane Conraads Cardiology
RED CELL DISTRIBUTION WIDTH A NEW MARKER OF EXERCISE INTOLERANCE IN PATIENTS WITH CHRONIC HEART FAILURE Emeline Van Craenenbroeck, Paul Beckers, Nadine Possemiers, Christiaan Vrints, Viviane Conraads Cardiology
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth
 Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
Hematopoiesis, The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid.
 Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia. Ioannis Griveas, MD, PhD
 Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease.
 Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease. Goldsmith D, Blackman A, Gabbay F, June 2013 Kidney Disease: Improving Global Outcomes (KDIGO)
Comment on European Renal Best Practice Position Statement on Anaemia Management in Chronic Kidney Disease. Goldsmith D, Blackman A, Gabbay F, June 2013 Kidney Disease: Improving Global Outcomes (KDIGO)
Anemia Update. Target Hb TREAT study Functional iron deficiency - Hepcidin Biosimilar epoetins
 Anemia Update Peter Bárány Department of Renal Medicine/ Karolinska University Hospital and Division of Renal Medicine Department of Clinical Science, Intervention and Technology Karolinska Institutet,
Anemia Update Peter Bárány Department of Renal Medicine/ Karolinska University Hospital and Division of Renal Medicine Department of Clinical Science, Intervention and Technology Karolinska Institutet,
Understanding Your Hemodialysis Access Options UNDERSTANDING IRON AND CHRONIC KIDNEY DISEASE
 Understanding Your Hemodialysis Access Options UNDERSTANDING IRON AND CHRONIC KIDNEY DISEASE UNDERSTANDING IRON AND CHRONIC KIDNEY DISEASE WHAT IS CHRONIC KIDNEY DISEASE (CKD)? When someone has CKD, it
Understanding Your Hemodialysis Access Options UNDERSTANDING IRON AND CHRONIC KIDNEY DISEASE UNDERSTANDING IRON AND CHRONIC KIDNEY DISEASE WHAT IS CHRONIC KIDNEY DISEASE (CKD)? When someone has CKD, it
C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School
 Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Novel Strategies to Prevent Pulmonary Embolism and DVT: APEX Trial and Substudies C. Michael Gibson, M.S., M.D. Professor of Medicine Harvard Medical School Conflict of Interest Statement 2 Present Research/Grant
Blood Management 2016
 Blood Management 2016 2016 AAHKS Annual Meeting Orthopaedic Team Member Course Harpal S. Khanuja, MD Associate Professor Chief of Adult Reconstruction Johns Hopkins University Chair, Johns Hopkins Bayview
Blood Management 2016 2016 AAHKS Annual Meeting Orthopaedic Team Member Course Harpal S. Khanuja, MD Associate Professor Chief of Adult Reconstruction Johns Hopkins University Chair, Johns Hopkins Bayview
Haematology and Transfusion
 Haematology and Transfusion Prof Dr Wolfram Engelhardt Anaesthesiology and Intensive Care Medicine Offenburg Hospital, Germany dr.w.engelhardt@gmail.com James Blundell 1828 Lancet 1828; 11:321 Erythrocytes
Haematology and Transfusion Prof Dr Wolfram Engelhardt Anaesthesiology and Intensive Care Medicine Offenburg Hospital, Germany dr.w.engelhardt@gmail.com James Blundell 1828 Lancet 1828; 11:321 Erythrocytes
Guideline developed by Shelley Crary, MD, MS,* in collaboration with the ANGELS team. Last reviewed by Shelley Crary, MD, MS, January 19, 2017.
 Microcytic Anemia Guideline developed by Shelley Crary, MD, MS,* in collaboration with the ANGELS team. Last reviewed by Shelley Crary, MD, MS, January 19, 2017. Dr. Crary is a member of the hemophilia
Microcytic Anemia Guideline developed by Shelley Crary, MD, MS,* in collaboration with the ANGELS team. Last reviewed by Shelley Crary, MD, MS, January 19, 2017. Dr. Crary is a member of the hemophilia
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas