Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
|
|
|
- Ashley Pierce
- 5 years ago
- Views:
Transcription
1 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18
2 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize current evidence for appropriate utilization of red blood cells, platelets, and cryoprecipitate

3 PBM definition: the timely application of evidence-based medical and surgical concepts designed to maintain hemoglobin concentration, optimize hemostasis and minimize blood loss in an effort to improve patient outcomes -Society for the Advancement of Blood Management 3
4 The IHI Triple Aim IHI Triple Aim is a framework developed by the Institute for Healthcare Improvement Improving the patient experience of care (including quality and satisfaction); Improving the health of populations; and Reducing the per capita cost of health care.
5 Why Patient Blood Management? Agency for Healthcare Research and Quality reported in 2013 that the most frequent procedure performed during hospitalization in 2010 was blood transfusion 11% of hospital stays with a procedure received transfusion 126% increased incidence compared to 1997 The Joint Commission and American Medical Association identified over-transfusion of red blood cells, as one of five target areas to reduce instances of overuse Anemia is common 9% females age % of nursing home residents 12.8% at hospital discharge May exceed 50% in patients hospitalized with CHF or pneumonia


6 Risks of allogeneic blood exposure Direct causal risks: Viral exposure Bacterial contamination Citrate exposure: - acidosis, hypocalcemia Hyperkalemia Mistransfusion Volume overload Transfusion reactions Indirect plausible risks: Immunomodulation Infection Pneumonia Slowed wound healing Prolonged ventilator use Increased length of stay Increased cost Increased morbidity and mortality Decreased exposure = increased safety and decreased cost
7 Risks of anemia Independent association with mortality in multiple patient populations Especially in patients with cardiovascular disease 30day mortality in adult Jehovah s witness patients undergoing noncardiac surgery
8 From Product Focus to Patient Focus = the transformational next step Whether and when to transfuse Optimal Care of the bleeding, coagulopathic, or anemic patient
9 MYTH 1 Patients should be transfused to a hemoglobin of 10 g/dl or hematocrit of 30% (the 10/30 rule )
10 Evidence for Red Blood Cell Transfusion Restrictive vs Liberal Transfusion Randomized Controlled Trials (RCT) Over 7000 patients enrolled in various trials Many are small but three have >900 patients Results consistently suggest that restrictive transfusion approach is safe No adequately powered RCT in acute coronary syndrome A restrictive approach appears safe and is often associated with decreased morbidity and mortality.
11 Restrictive vs Liberal RBC Transfusion RCT n PATIENTS RESTRICTIVE LIBERAL OUTCOME RESULT TRICC 838 ICU day mort Not Signif TRACS 512 CABG/Valve day mort or organ failure FOCUS 2016 Hip fracture & CV disease day mort or inability to walk 10 CRIT 45 ACS day mort, MI, revasc MINT 110 ACS or CAD with PCI day mort, MI, revasc Not Signif Not Signif Favor Restrictive Not Signif Villanueva 921 UGI bleed day mort Favor Restrictive Robertson 200 TBI month GCS Not signif TRISS 998 Septic shock day mort, ischemia, life support Not signif
12 MYTH 1 Patients should be transfused to a hemoglobin of 10 g/dl or hematocrit of 30% (the 10/30 rule )
13 MYTH 2 But, really, cardiac patients should have a hemoglobin of 10 g/dl or hematocrit of 30% (the 10/30 rule )
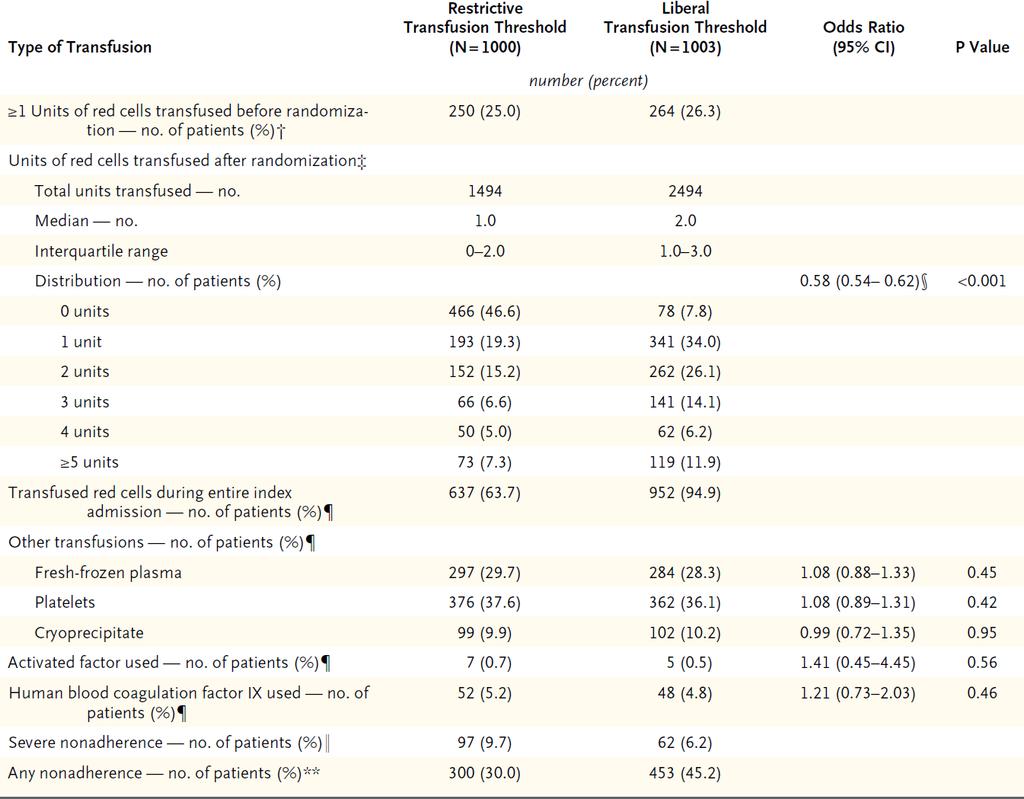
14 n=1000 restrictive (Hgb 7.5 g/dl), n=1003 liberal (Hgb 9 g/dl)) 53.4% in restrictive group and 92.2% in liberal group received transfusion Primary outcome composite of serious infection (sepsis or wound infection) or an ischemic event (permanent stroke, MI, gut infarct, AKI) within 3 mos. after randomization Primary-outcome reached in 35.1% in restrictive group and 33.0% in liberal group Serious postop complications outside the primary-outcome occurred in 35.7% in restrictive group and 34.2% in liberal group BUT more deaths in restrictive group (4.2%) than liberal (2.6%) p=0.045
15
16 After randomization, the difference in hemoglobin between groups was only 1 g/dl An assessment of causes of death or of serious adverse events that preceded death did not suggest any specific cause-and-effect relationship (analysis limited by small number of deaths n= 68 and also by reality that cardiac surgical deaths typically occur after a sequence of adverse events)
17 MYTH 2 But, really, cardiac patients should have a hemoglobin of 10 g/dl or hematocrit of 30% (the 10/30 rule )
18 MYTH 3 Old blood is bad (the storage lesion )
19 n=1211 fresh-blood (6.1 ± 4.9 days), n=1219 standard blood (22.0 ± 8.4 days)) 96.4% in fresh group and 97.1% in standard group received transfusion Primary outcome 90-day all-cause mortality Secondary outcomes major illnesses; duration of respiratory, hemodynamic, or renal support; LOS; transfusion reactions
20
21 MYTH 3 Old blood is bad (the storage lesion )
22 Physiology Overview The primary way that oxygen is delivered in the body is via hemoglobin-binding within our erythrocytes. Anemia is associated with a compensatory increase in cardiac index and, when severe, may decrease tissue oxygenation. Packed red blood cells (RBC) consist of erythrocytes concentrated from whole blood donations by centrifugation OR collected by apheresis. Transfusing PRBC in an anemic patient may improve tissue oxygenation in some situations, but, in many situations, the risk of transfusing PRBC may be greater than the probability of benefit.
23 Red Blood Cell Transfusion Overview In non-hemorrhaging patients: RBC transfusion should not be considered until the hemoglobin is less than 7-8 g/dl. Caveats: lack of adequately powered RCT in ACS and higher end of spectrum for post-cpb The decision to transfuse should be based on clinical assessment after correction of hypovolemia (i.e. not solely on hemoglobin). Transfusions should be ordered one unit at a time, followed by repeat clinical evaluation.
24 Clinical Assessment Common signs and symptoms of anemia may include: Shortness of breath Fatigue Tachycardia Hypovolemia can mimic symptomatic anemia, and it is important to correct, which can often be accomplished with crystalloids.
25 Transfusion Mechanics In a stable, non-bleeding or hemolyzing adult transfused with compatible PRBC: Hemoglobin equilibrates in 15 mins after transfusion One PRBC unit will increase Hgb by 1 g/dl and Hct by 3% Infusion rate: as patient can tolerate, generally over 75 mins-4 hrs (maximum) All PRBC in all GHS hospitals are leukoreduced.
26 Adverse effects of transfusion contrasted with other life risks. Estimates of the current risk per unit of red blood cell transfused (or per platelet transfused, as designated), in blue, are contrasted against risk for fatality per year for various life events, in green. Risk is depicted on a logarithmic scale. HIV, human immunodeficiency virus; HCV, hepatitis C virus; HBV, hepatitis B virus; TRALI, transfusion-related acute lung injury; TACO, transfusion-associated circulatory overload. (Adapted from Carson JL, Grossman BJ, Kleinman S, et al. Red Blood Cell Transfusion: A Clinical Practice Guideline From the AABB. Ann Intern Med, 2012;157:49-58.)
27 Risks of Transfusion The greatest risks of transfusion are not always causally linked to known transfusion reactions. Villanueva et al showed a 4% absolute increase in mortality in patients with upper GI hemorrhage when they were transfused to a target hemoglobin of 9 g/dl (rather than 7 g/dl) Recent meta-analysis (Rhode JM, et al) showed a 5% increase in the pooled risk of serious infection in patients who were liberally transfused.
28 Considerations for Future Transfusion Avoidance Anemia diagnosis and management Anemia labs Parenteral iron, B12, folate, ESAs Patient education Treat anemia prior to elective surgery Opportunity to manage anemia while patient in the hospital Avoid excessive phlebotomy (e.g. daily labs) Arrest bleeding promptly don t wait Optimize coagulation
29 MYTH 4 My hem/onc patient has special circumstances XYZ over everyone else, so give prophylactic platelet transfusions to keep platelets >20,000
30 To give or not to give, that is the question Summary of moderate quality evidence: Three RCTs compared bleeding outcomes in inpatients with radiation and/or chemotherapyassociated hypoproliferative thrombocytopenia assigned to receive or not receive prophylactic platelet transfusions Outcomes: prophylactic transfusions significantly reduced risk for spontaneous grade 2 or greater bleeding
31 Evidence for Platelet Transfusion Summary of moderate quality evidence: Four RCTs examined the threshold platelet count at which platelets should be transfused prophylactically in inpatients with therapyinduced hypoproliferative thrombocytopenia Outcomes: the 10,000/μL threshold was associated with fewer number days bleeding, lower platelet usage, and fewer transfusion reactions and a 20,000/μL or 30,000/μL threshold was not associated with statistically lower incidence of grade 2 or greater bleeding
32 MYTH 4 My hem/onc patient has special circumstances XYZ over everyone else, so transfuse platelets to 20,000
33 MYTH 5 When my patient s platelet count is low, I should give two units of platelets
34 Evidence for Platelet Transfusion Summary of moderate quality evidence: Two RCTs compared high-dose platelets (defined as two apheresis units) to standard dose of one unit Outcomes: prophylactic transfusion of high-dose platelets did not reduce the risk for bleeding compared with standard-dose
35 Evidence for Platelet Transfusion Summary of moderate quality evidence: Four RCTs examined whether prophylactic transfusion of low-dose platelets (defined as onehalf apheresis unit) would provide hemostasis equal to standard dose of one unit in patients with therapy-induced hypoproliferative thrombocytopenia Outcomes: no difference in grade 2 or greater bleeding between standard and low-dose
36 MYTH 5 When my patient s platelet count is low, I should give two units of platelets
37 Platelet Overview Platelets are obtained by two different methods: platelet concentrates from whole blood or apheresis platelets GHS uses only apheresis platelets at all sites Unlike other blood components, platelets must be stored at room temperature, limiting the shelf life to 5 days because of the risk for bacterial growth during storage Platelet transfusion risks include allergic/anaphylactoid, febrile non-hemolytic, sepsis, and transfusion-related acute lung injury Sepsis from a bacterially contaminated platelet represents the most frequent infectious complication from any blood product
38 Platelet Overview Most platelet transfusions are given prophylactically to reduce the risk for spontaneous bleeding in thrombocytopenic patients Transfusions should be ordered one unit at a time, followed by repeat platelet count and clinical evaluation. Greater doses are not effective and lower doses, equal to one-half of a standard apheresis unit, are equally effective
39 Platelet Transfusion Mechanics Measure platelet count from minutes after transfusion One apheresis platelet will increase platelet count by 30,000-60,000/μL in average-sized adults In neonates and infants, a dose of 5-10 ml/kg will increase platelet count by 50, ,000/μL Response to platelet transfusion is adversely affected by fever, sepsis, splenomegaly, severe bleeding, consumptive coagulopathy, HLA alloimmunization, and certain medications (e.g. amphotericin B) All apheresis platelets are inherently leukoreduced
40 Evidence for Platelet Transfusion Evidence supporting prophylactic transfusion for invasive procedures is based on: 8 observational studies of CVC placement 7 observational studies of LP in children 1 series on 167 invasive procedures including 29 major surgeries and 24 moderately invasive procedures Meta-analysis of 6 RCTs and a single pilot study on cardiac surgical patients Evidence supporting platelet transfusion and platelet inhibitor drugs can be found in 6 observational studies
41 Platelet transfusion considerations Consider consult with Laboratory Medicine if bleeding persists Consider whether additional clinical factors are contributing to the risk of bleeding (renal failure, medications, end-organ dysfunction, coagulopathy). If renal failure, consider DDAVP. Platelets are contraindicated in patients with thrombotic thrombocytopenic purpura (TTP) and heparin-induced thrombocytopenia (HIT) unless life-threatening hemorrhage
42 MYTH 6 Cryoprecipitate is off the market in many European countries in lieu of fibrinogen concentrate
43 Cryoprecipitate Overview Cryoprecipitate was originally developed as therapy for hemophilia A, due to the factor VIII content With the advance in recombinant factor development, cryoprecipitate is no longer used for its original purpose but is instead used for acquired coagulopathy, such as in clinical settings associated with hemorrhage
44 Cryoprecipitate Overview The usual recommendation of cryoprecipitate transfusion to supplement fibrinogen when fibrinogen level is <100 mg/dl is empiric and not based on solid clinical evidence Randomized controlled trials are needed to determine the clinical efficacy of cryoprecipitate, compared with the efficacy of alternative preparations The development of fibrinogen concentrate, along with safety concerns related to TRALI and transfusion-transmitted infection, has led to the withdraw of cryoprecipitate from the market in many European countries
45 MYTH 6 Cryoprecipitate is off the market in many European countries in lieu of fibrinogen concentrate
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion triggers in acute coronary syndromes: The MINT trial
 Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
Transfusion triggers in acute coronary syndromes: The MINT trial Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Objectives Review evidence on transfusion triggers
Patient Blood Management: Enough is Enough
 Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Patient Blood Management: Enough is Enough Richard Benjamin, MBChB, PhD, FRCPath Professor of Pathology Georgetown University Medical Center Washington, D.C. Chief Medical Officer Cerus Corporation Concord,
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Transfusion Indications: Update in 2019
 Transfusion Indications: Update in 2019 Yulia Lin, MD, FRCPC, CTBS Division Head, Transfusion Medicine, Sunnybrook HSC Associate Professor, Dept of Laboratory Medicine and Pathobiology, University of Toronto
Transfusion Indications: Update in 2019 Yulia Lin, MD, FRCPC, CTBS Division Head, Transfusion Medicine, Sunnybrook HSC Associate Professor, Dept of Laboratory Medicine and Pathobiology, University of Toronto
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Blood transfusions in ICU: double-edged sword. Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal
 Physician-in-Chief, CHUM Professor, University of Montreal") Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
Blood transfusions in ICU: double-edged sword Paul Hébert, MD MHSc(Epid) Physician-in-Chief, CHUM Professor, University of Montreal Canadian Critical Care Trials Group Collaborating for Impact Leading
ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE
 ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE WEIQIANG GAO HEM/ONC FELLOW FACULTY DISCUSSANT SIOBAN KEEL, MD OCT. 24, 2014 CASE PRESENTATION 25 F, a Jehovah s witness, w/ h/o synovial sarcoma
ERYTHROPOIETIC STIMULATING AGENTS IN THE ICU: A MOVING PUZZLE WEIQIANG GAO HEM/ONC FELLOW FACULTY DISCUSSANT SIOBAN KEEL, MD OCT. 24, 2014 CASE PRESENTATION 25 F, a Jehovah s witness, w/ h/o synovial sarcoma
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Goal Directed Therapy : Liberal vs Restrictive Transfusion.. Syafri Kamsul Arif
 Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Advances in Transfusion and Blood Conservation
 Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Risk of ID transmission. Patient Blood Management - Blood Safety and Component Utilization. Transfusion and Cancer 4/9/2014
 Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Patient Blood Management: At the Forefront of Quality and Value in Healthcare
 Patient Blood Management: At the Forefront of Quality and Value in Healthcare Ryan A. Metcalf, MD, CQA(ASQ) Associate Medical Director, University Hospital Transfusion Services and ARUP Blood Services
Patient Blood Management: At the Forefront of Quality and Value in Healthcare Ryan A. Metcalf, MD, CQA(ASQ) Associate Medical Director, University Hospital Transfusion Services and ARUP Blood Services
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Transfusion: indications (RBC, platelets, granulocytes, plasma)
") Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion Medicine Update KEMC Nov 5, 2014
 Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Transfusion Medicine Update KEMC Nov 5, 2014 Allison Collins MD FRCPC Ontario Regional Blood Coordinating Network Physician Clinical Project Coordinator Disclosure I have no conflict of interest with this
Patient Blood Management. Marisa B. Marques, MD UAB Department of Pathology November 17, 2016
 Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Patient Blood Management Marisa B. Marques, MD UAB Department of Pathology November 17, 2016 Learning Objectives Upon completion of the session, the participant will: 1) Differentiate between the various
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto
 Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
Patient Blood Management Are you providing this? Jeannie Callum, BA, MD, FRCPC Associate Professor, University of Toronto Disclosures Relevant relationships with commercial entities: Octapharma, CSL Behring
JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION. Maggie Woods PGY-3
 JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION Maggie Woods PGY-3 BACKGROUND Objective: To describe evidence for current guidelines, review trends, examine the risks of transfusion
JOURNAL CLUB INDICATIONS FOR AND ADVERSE EFFECTS OF RED CELL TRANSFUSION Maggie Woods PGY-3 BACKGROUND Objective: To describe evidence for current guidelines, review trends, examine the risks of transfusion
The ABC s of Blood Components. Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service
SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service") The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
Controversies in Transfusion Medicine
 Controversies in Transfusion Medicine Jeffrey L. Carson, M.D. Richard C. Reynolds Professor of Medicine Chief, Division of General Internal Medicine Robert Wood Johnson Medical School New Brunswick, New
Controversies in Transfusion Medicine Jeffrey L. Carson, M.D. Richard C. Reynolds Professor of Medicine Chief, Division of General Internal Medicine Robert Wood Johnson Medical School New Brunswick, New
Dr Tushar Mahambrey. Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool
 Dr Tushar Mahambrey Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool History Why do we give blood Why does anaemia occur in critical care patients
Dr Tushar Mahambrey Consu ltant Critical Care Med icine & Anaesthetics St Helens and Knowsley N H S teaching hospitals Liverpool History Why do we give blood Why does anaemia occur in critical care patients
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy. Megan Boysen Osborn, MD, MHPE
 Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
Thinking Twice About Transfusions: When TACOS and TRALIs Turn Treatment Into Tragedy Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion Reactions Megan Boysen Osborn, MD, MHPE Let s TACO bout Transfusion
POLICY NO. Printed copies are for reference only. Please refer to the electronic copy for the latest version.
 Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Pretransfusion Testing
 Pretransfusion Testing Blood transfusion services The immunohematologic testing needed for By proper patient blood typing, component Dr. selection Reham and Talaat compatibility testing. Which Blood ensure
Pretransfusion Testing Blood transfusion services The immunohematologic testing needed for By proper patient blood typing, component Dr. selection Reham and Talaat compatibility testing. Which Blood ensure
Haematology and Transfusion
 Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Science Evidence Cost
 Anemia, Evidence, and Anemic Evidence: Is there a rational approach to perioperative transfusion? Elizabeth L Whitlock, MD, MSc Resident physician, Anesthesia & Perioperative Care University of California,
Anemia, Evidence, and Anemic Evidence: Is there a rational approach to perioperative transfusion? Elizabeth L Whitlock, MD, MSc Resident physician, Anesthesia & Perioperative Care University of California,
TRANSFUSION REACTIONS
 14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
14 TRANSFUSION REACTIONS 14.1 INTRODUCTION Transfusion of blood and blood products are reported to cause reactions during or after procedure specially in patients who receive multiple transfusions. These
Transfusion Medicine Best Practices: Indications for Blood Components
 Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Blood is serious business
 Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion at RCH BLOOD TRANSFUSION Anthea Greenway Dept of Clinical Haematology >10000 fresh blood products per year Supports craniofacial and cardiac surgery Support bone marrow, liver transplant and
Transfusion Triggers. Richard Soutar January 2012
 Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
Transfusion Triggers Richard Soutar January 2012 1 Educational objectives: To understand the risks of transfusion - the known, the uncertain and unknown To understand the fear of the unknown in Transfusion
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
WRHA Blood Conservation Service WRHA Transfusion Practice Committee. TEAM TRANSFUSION Differential Diagnosis of Adverse Events
 WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
WRHA Blood Conservation Service WRHA Transfusion Practice Committee TEAM TRANSFUSION Differential Diagnosis of Adverse Events MANITOBA ADVERSE EVENT REPORTING SYSTEM DATA FLOW REACTION Physician orders
In the United States, transfusion reactions are reported to occur. Global Prevalence. Evolution of Transfusion Practices
 Evolution of Transfusion Practices TRALI, TACO, and other Transfusion Complications Michael Rieker, DNP, CRNA Wake Forest Baptist Medical Center 1665 - The first Blood transfusions of record take place.
Evolution of Transfusion Practices TRALI, TACO, and other Transfusion Complications Michael Rieker, DNP, CRNA Wake Forest Baptist Medical Center 1665 - The first Blood transfusions of record take place.
Transfusion Medicine III
 Transfusion Medicine III Blood Products from Collection to Use D. Joe Chaffin, MD Loma Linda University 3/5/2019 FFP WB RBC Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep
Transfusion Medicine III Blood Products from Collection to Use D. Joe Chaffin, MD Loma Linda University 3/5/2019 FFP WB RBC Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep
Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital
 Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Transfusions in Acute Care Too Little?
 Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
TRANSFUSIONS FIRST, DO NO HARM
 TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
TRANSFUSIONS FIRST, DO NO HARM BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women BECAUSE In OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT RISKS versus BENEFITS versus
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created
 Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
CMC Medical Staff Transfusion Guidelines. Table of Contents edition INTRODUCTION:
 CMC Medical Staff Transfusion Guidelines 2014 edition INTRODUCTION: The CMC Blood Component and Transfusion Guidelines have been approved by the multidisciplinary Transfusion Committee. These are based
CMC Medical Staff Transfusion Guidelines 2014 edition INTRODUCTION: The CMC Blood Component and Transfusion Guidelines have been approved by the multidisciplinary Transfusion Committee. These are based
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC
 RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
RENAL & HEMATOLOGY EMERGENCIES JEFF SIMONS B.S. F-PC GOALS Overview of renal system anatomy / physiology Discuss common medical / trauma renal issues Identify associated assessment keys GOALS Introduction
How we View & Approach TACO
 How we View & Approach TACO Annual Blood Transfusion & Hemovigilance Symposium Ede, Netherlands May 22, 3014 Mark A. Popovsky, M.D. Chief Medical Officer, Haemonetics Corporation Associate Clinical Professor,
How we View & Approach TACO Annual Blood Transfusion & Hemovigilance Symposium Ede, Netherlands May 22, 3014 Mark A. Popovsky, M.D. Chief Medical Officer, Haemonetics Corporation Associate Clinical Professor,
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Transfusion Limbo How Low Will You Go? Safely. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Boot Camp Transfusion Reactions
 Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
Boot Camp Transfusion Reactions Dr. Kristine Roland Regional Medical Lead for Transfusion Medicine, VCH Objectives By the end of this session, you should be able to: Describe in common language the potential
TRANSFUSION OVERUSE. Exposing an International Problem and Patient Safety Issue
 TRANSFUSION OVERUSE Exposing an International Problem and Patient Safety Issue Blood transfusion is far riskier than what people believe, and is responsible for billions in wasted healthcare dollars every
TRANSFUSION OVERUSE Exposing an International Problem and Patient Safety Issue Blood transfusion is far riskier than what people believe, and is responsible for billions in wasted healthcare dollars every
Blood Transfusion Project. Reducing Transfusion in the MARCQI Population
 Blood Transfusion Project Reducing Transfusion in the MARCQI Population Anemia in Healthy Awake Volunteers Critical hemoglobin threshold unknown in humans At 6 g/dl Decline in cognitive function At 5 g/dl
Blood Transfusion Project Reducing Transfusion in the MARCQI Population Anemia in Healthy Awake Volunteers Critical hemoglobin threshold unknown in humans At 6 g/dl Decline in cognitive function At 5 g/dl
ORBcoN Spring Symposium April 2015
 ORBcoN Spring Symposium April 2015 CFPC CoI Templates: Slide 1 Faculty: Gail Murray Relationships with commercial interests: Former Member of the Advisory Board 2012 with Takeda Canada for Feraheme CFPC
ORBcoN Spring Symposium April 2015 CFPC CoI Templates: Slide 1 Faculty: Gail Murray Relationships with commercial interests: Former Member of the Advisory Board 2012 with Takeda Canada for Feraheme CFPC
Three decades of transfusion Toronto, Critical Care Canada Forum, October 30, 2014.
 Three decades of transfusion Toronto, Critical Care Canada Forum, October 30, 2014. Jacques Lacroix For the Canadian Critical Care Trials Group and the PALISI Network Pediatric Intensive Care Unit Sainte-Justine
Three decades of transfusion Toronto, Critical Care Canada Forum, October 30, 2014. Jacques Lacroix For the Canadian Critical Care Trials Group and the PALISI Network Pediatric Intensive Care Unit Sainte-Justine
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Approach to a patient with suspected blood transfusion reaction. Raju Vaddepally, MD
 Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
Approach to a patient with suspected blood transfusion reaction Raju Vaddepally, MD Goals Detection of Acute Transfusion Reactions (ATR) Clinical and Laboratory Evaluation of ATR Management of individual
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Blood Management 2016
 Blood Management 2016 2016 AAHKS Annual Meeting Orthopaedic Team Member Course Harpal S. Khanuja, MD Associate Professor Chief of Adult Reconstruction Johns Hopkins University Chair, Johns Hopkins Bayview
Blood Management 2016 2016 AAHKS Annual Meeting Orthopaedic Team Member Course Harpal S. Khanuja, MD Associate Professor Chief of Adult Reconstruction Johns Hopkins University Chair, Johns Hopkins Bayview
Updates in the Management of Anemia in Cancer. Taylor M. Ortiz, MD May 19, 2017
 Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Transfusion Therapy: When to Use It and How to Minimize It
 Chapter 144 Transfusion Therapy: When to Use It and How to Minimize It Amanda Wehler and Samir M. Fakhry Introduction Physicians encounter a large spectrum of medical and surgical conditions that may require
Chapter 144 Transfusion Therapy: When to Use It and How to Minimize It Amanda Wehler and Samir M. Fakhry Introduction Physicians encounter a large spectrum of medical and surgical conditions that may require
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD
 Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
Preoperative anemia Common, consequential and correctable in non-emergent surgery By Kathrine Frey, MD Preoperative anemia is common, especially in patients undergoing nonemergent high-blood-loss surgical
HB TRIGGER & SINGLE UNITS
 HB TRIGGER & SINGLE UNITS Conflict of Interest Disclosure I hereby declare the following potential conflicts of interest concerning my presentation: Consultancy: none Research Funding: 2 RCTs funded by
HB TRIGGER & SINGLE UNITS Conflict of Interest Disclosure I hereby declare the following potential conflicts of interest concerning my presentation: Consultancy: none Research Funding: 2 RCTs funded by
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
An Approach to the Patient Refractory to Platelets Transfusion. Harold Alvarez, MD
 Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Harold Alvarez, MD Objectives Explain the etiology of platelet refractoriness Discuss the different types of platelet refractoriness Describe how platelet refractoriness is diagnosed Discuss different
Blood and blood component therapy in the critically ill patient
 Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
Blood and blood component therapy in the critically ill patient Dr Liesel Bösenberg Specialist Physician and Fellow in Critical Care Kalafong Hospital Points that we shall ponder Transfusion triggers EGDT
Epogen / Procrit. Epogen / Procrit (epoetin alfa) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.10.06 Section: Prescription Drugs Effective Date: April1, 2014 Subject: Epogen / Procrit Page: 1 of 7
PEDIATRIC TRANSFUSION MEDICINE AS A SUB-SPECIALITY TO TRANSFUSION MEDICINE
 PEDIATRIC TRANSFUSION MEDICINE AS A SUB-SPECIALITY TO TRANSFUSION MEDICINE Prof. Neelam Marwaha MD; FAMS; FISHTM. Head, Dept. of Transfusion Medicine PGIMER Chandigarh Dr. Hari Krishan Dhawan MD. Assistant
PEDIATRIC TRANSFUSION MEDICINE AS A SUB-SPECIALITY TO TRANSFUSION MEDICINE Prof. Neelam Marwaha MD; FAMS; FISHTM. Head, Dept. of Transfusion Medicine PGIMER Chandigarh Dr. Hari Krishan Dhawan MD. Assistant
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Vijay M. Patel, 1 Anna W. Rains, 2 and Christopher T. Clark Introduction
 Blood Transfusion Volume 2016, Article ID 2859720, 6 pages http://dx.doi.org/10.1155/2016/2859720 Research Article Effectiveness of Provider Education Followed by Computerized Provider Order Entry Alerts
Blood Transfusion Volume 2016, Article ID 2859720, 6 pages http://dx.doi.org/10.1155/2016/2859720 Research Article Effectiveness of Provider Education Followed by Computerized Provider Order Entry Alerts
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Blood Products & Transfusion. Karim Rafaat, M.D.
 Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
The Bleeding Jehovah s Witness: A Nightmare Scenario?
 The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses
The Bleeding Jehovah s Witness: A Nightmare Scenario? David Smith, Bristol Hospital Liaison Committee for Jehovah s Witnesses SW RTC: Bleeding in the Medical Patient - 21 February 2018 Jehovah s Witnesses