Effectiveness of Compounded Bioidentical Hormone Replacement Therapy: An Observational. Cohort Study
|
|
|
- Richard Goodwin
- 6 years ago
- Views:
Transcription
1 Effectiveness of Compounded Bioidentical Hormone Replacement Therapy: An Observational Cohort Study Andres D. Ruiz, Pharm.D., M.Sc., College of Pharmacy, The University of Texas, Austin, TX; The University of Texas Health Science Center, San Antonio, TX; Oakdell Pharmacy Inc., San Antonio, TX; Kelly R. Daniels, Pharm.D., College of Pharmacy, The University of Texas, Austin, TX; The University of Texas Health Science Center, San Antonio, TX; Oakdell Pharmacy, Inc., San Antonio, TX; Jamie C. Barner, Ph.D., College of Pharmacy, The University of Texas, Austin, TX; John J. Carson, R.Ph., Oakdell Pharmacy, San Antonio, TX; Christopher R. Frei, Pharm.D., M.Sc., BCPS, College of Pharmacy, The University of Texas, Austin, TX; The University of Texas Health Science Center, San Antonio, TX; Institution Addresses: The University of Texas at Austin: 1 University Station A1900, Austin, TX, The University of Texas Health Science Center at San Antonio: 7703 Floyd Curl Dr., San Antonio, TX, Oakdell Pharmacy, Inc.: 7220 Louis Pasteur, Suite 176, San Antonio, TX,
2 Correspondence: Christopher R. Frei, Pharm.D., M.Sc., BCPS, The University of Texas Health Science Center at San Antonio (UTHSCSA), Pharmacotherapy Education and Research Center (PERC), 7703 Floyd Curl Dr., MSC-6220, San Antonio, TX , (210) (office), (210) (fax), 2
3 Abstract Background Bioidentical Hormone Replacement Therapy (BHRT) is believed it to be a safer and equally effective alternative to Conventional Hormone Therapy for the relief of menopausal symptoms; however, data are needed to support these claims. The objective of this study is to evaluate the effectiveness of compounded BHRT provided in six community pharmacies. Methods This was an observational cohort study of women between the ages of who received a compounded BHRT product from January 1, 2003 to April 30, 2010 in six community pharmacies. Data included patient demographics, comorbidities, therapeutic outcomes, and hormone therapies. Women self-rated menopausal symptoms as absent, mild, moderate, or severe. Descriptive statistics were used to characterize the patient population, BHRT use, and adverse events. Patient symptom severity was compared at baseline and 3 to 6 months followup using the Wilcoxon signed-rank test. Results Women (n=296) receiving BHRT at Oakdell Pharmacy had a mean (standard deviation) age of 52 (9) years. The most common BHRT dosage forms utilized were topical (71%) and oral (43%). Compounded BHRT regimens were generally initiated at low doses regardless of route. Women experienced a 25% decrease in emotional lability (p<0.01), a 25% decrease in irritability (p<0.01), and a 22% reduction in anxiety (p=0.01) within 3 to 6 months. These women also 3
4 experienced a 14% reduction in night sweats (p=0.09) and a 6% reduction in hot flashes (p=0.50). Conclusions This study demonstrates that compounded BHRT improves mood symptoms. Larger studies are needed to examine the impact on vasomotor symptoms and to evaluate the safety of compounded BHRT with regards to MI and breast cancer. 4
5 Background Bioidentical Hormone Replacement Therapy (BHRT) describes supplementation of hormones that are molecularly identical to those hormones produced in the human body. Unlike manufactured Conventional Hormone Therapy (CHT), such as conjugated estrogens (CE) and medroxyprogesterone acetate (MPA), BHRT hormones do not contain extra structural moieties which may alter hormone receptor binding and function in the human body. The Professional Compounding Centers of America (PCCA) estimates that 1 in 4 compounded products in the United States are a form of Hormone Replacement Therapy (HRT) [1]. Compounded BHRT is a form of personalized medicine whereby the dose, regimen, and dosage forms are customized based on the patient s symptoms, hormone levels, and preferences. Hormone levels are obtained by either serum or salivary testing and are measured to assess a woman s hormonal stage of life and to create customized therapies. The idea is that these individualized preparations containing bioidentical hormones may improve the safety and effectiveness of treating menopausal symptoms. Compounded BHRT is perceived to be more effective, better tolerated, with fewer health risks than its CHT counterpart [2-4]. This study first describes the characteristics and prescribing patterns of compounded BHRT in six community pharmacies. Three specific aims are then addressed: (1) determine if compounded BHRT is effective in treating menopausal symptoms, (2) identify which BHRT compounds are most effective, and (3) determine if compounded BHRT is safe. 5
6 Methods This was an observational cohort study of female patients age treated for menopause-related hormone imbalances from January 1, 2003 to April 30, 2010 in six community pharmacies. The University of Texas Health Science Center at San Antonio Institutional Review Board reviewed and approved this study; protocol number HSC H. Oakdell Pharmacy, Inc. is comprised of six independent community pharmacies located throughout San Antonio, Texas and has offered BHRT consultation services since Currently, more than 1,000 women receive their compounded BHRT at Oakdell Pharmacy. Patient charts are maintained locally at the pharmacy. Pharmacists who provide BHRT consultation services at Oakdell Pharmacy are trained through PCCA educational symposiums and other BHRT-focused seminars. At these seminars, credentialed medical professionals (e.g., physicians and pharmacists) provide evidence-based BHRT education. In addition, pharmacists who care for BHRT patients at Oakdell must have BHRT-related continuing education credit. Patients are referred to the Oakdell Wellness Center through physicians, family members, and friends. BHRT consultation services consist of an extensive initial evaluation, hormone replacement education, and follow-up visits. Patients complete a new patient evaluation form and a laboratory hormone panel prior to their initial visit. This hormone panel, determined through serum or salivary testing, aids in identification of sex hormone deficiencies, adrenal function deficiencies, and thyroid dysfunction. Additional hormone panels are recommended 3-6 months after BHRT initiation, annually, and when deemed necessary to assist with BHRT customization. During the initial evaluation, patients are questioned regarding 6
7 medical history, menopausal symptoms, and treatment goals. They are educated on several components of hormone therapy including: hormonal changes of menopause, causative factors associated with menopausal symptoms, risks and benefits of hormone therapy (both conventional and bioidentical therapies), and different BHRT dosage forms. During initial evaluation and follow-up visits, pharmacists use a standardized form to monitor symptom resolution and adverse effects. This form lists several symptoms associated with menopause. Patients are asked to indicate whether their symptoms are absent, mild, moderate, or severe. The pharmacist and patient decide on an individualized treatment plan consisting of either (1) a prescription recommendation to be faxed to their physician for modification, signature, and approval and/or (2) over-the-counter (OTC) products. The pharmacist s letter to the physician describes the patient s hormone imbalance(s), laboratory results, and current menopausal symptoms. It also suggests a customized BHRT regimen and outlines the benefits of compounded BHRT. BHRT compounds vary by active ingredients, dose, and dosage form. Once the physician s approval is received, the individualized BHRT compound is prepared. The most common compounded BHRT hormones include: biest (estriol/estradiol in varying concentrations), triest (estriol/estradiol/estrone) progesterone, testosterone, and dehydroepiandosterone (DHEA). Table 1 depicts common bioidentical hormone dose classifications. Patients are instructed to complete monthly evaluation forms for the first few months and every six months thereafter to monitor menopausal symptoms and side effects. Upon review of a patient s evaluation form, the pharmacist decides if further laboratory work, 7
8 telephone, or face-to-face follow-up is needed. The pharmacist then makes changes to the patient s therapy in consultation with the patient and their physician. Patient Eligibility The first 1,000 adult ( 18 years of age) women receiving compounded BHRT at Oakdell Pharmacy Inc., from January 1, 2003 to April 30, 2010 were eligible for this study. Patients were excluded if they received compounded BHRT from Oakdell Pharmacy, but were managed outside the Oakdell Pharmacy system (i.e., physicians offices). Patients were also excluded if they did not complete a follow-up hormone evaluation form. All data were collected at Oakdell Pharmacy from the existing medical records. Data Collection A customized, data collection instrument was developed using Microsoft Access 2007 software. The instrument was designed to mimic the appearance of the initial patient intake and follow-up forms used during pharmacist consultations at Oakdell Pharmacy. All research personnel were trained on the tool prior to collection of any patient data. Data included patient demographics, comorbidities, laboratory values, medications, and adverse effects of hormone therapy. The last-observation-carried-forward (LOCF) method was used to determine BHRT effectiveness at 3 and 6 months follow-up. If patient data were available at 6 months, those data were used. That is, if patient data were available at 3 months, but not 6 months, then the data from 3 months were used. LOCF is an accepted method used by other HRT studies [5-7]. 8
9 The dependent variables utilized in this study were vasomotor symptoms, mood symptoms, myocardial infarction, and breast cancer. A decrease in symptom intensity was defined as a decrease in symptom ratings from baseline to follow-up (three to six months). Baseline and follow-up symptom ratings were also compared at each time point using the percentage of patients reporting either moderate or severe. Myocardial infarction and breast cancer adverse event rates were reported as events and cases per 10,000 person years. Adverse event (AE) rates were calculated with the following method: 10,000 X number of adverse events (average follow-up time to AE) X (# of patients with AE follow-ups) The independent variables utilized in this study were BHRT regimen and BHRT dosage form. The term estrogen was used to describe the use of any of the estrogen combinations [i.e., triest (estriol 80%/estradiol 10%/estrone 10%), biest (estriol 80%/estradiol 20%), biest (estriol 70%/estradiol 30%), biest (estriol 50%/estradiol 50%)]. Patient s length of therapy (LOT) was obtained from the pharmacy records and patient charts. LOT was calculated using the following method: date of most current BHRT prescription fill minus date of original fill. The patient s treatment timeframe was obtained from pharmacy records and was calculated as the date of follow-up minus the date of baseline assessment. Data and Statistical Analysis All statistical analyses were performed using JMP 8.0 (SAS Corp., Cary, NC). Statistical significance was defined as an alpha less than Descriptive statistics (e.g., means, medians, 9
10 and frequencies) were used to characterize the patient demographics, BHRT use, symptom resolution, and adverse effects. Patient demographics, baseline characteristics, comorbid conditions, baseline menopausal symptoms, dosing regimens, symptom improvement, and adverse effects were compared between groups. Categorical variables were compared using chi-square and Fisher s exact tests. Continuous variables were tested for normality using the Shapiro Wilk-W Test. Normally distributed variables were reported as means (standard deviations), while non-normally distributed variables were reported as medians (25th and 75th percentiles). Paired data were compared using the Wilcoxon signed-rank test. All tests were two-sided. 10
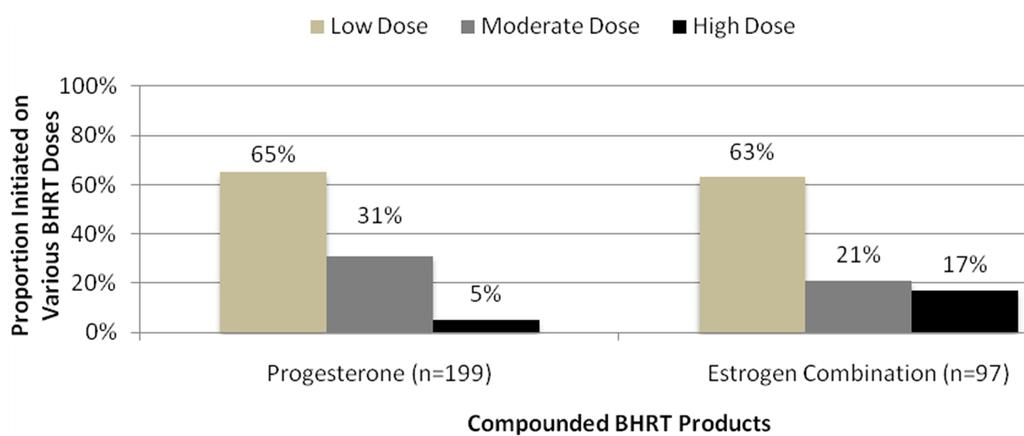
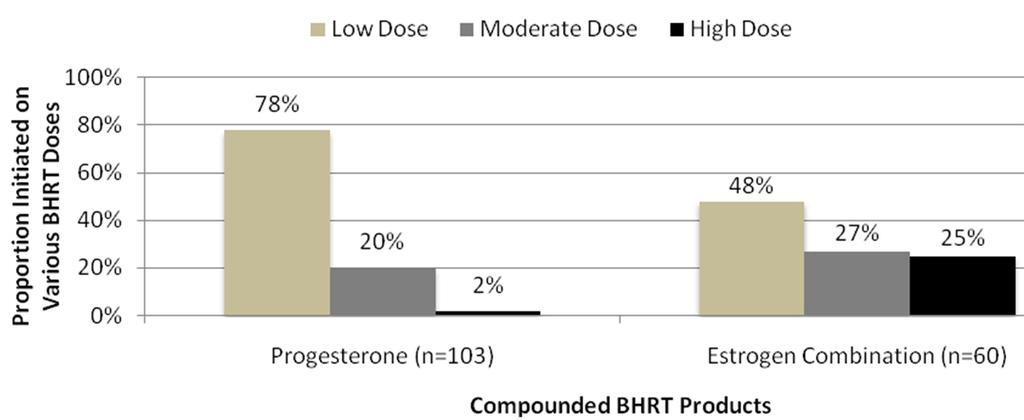
11 Results Population Characteristics Overall, 296 women met study criteria. The mean (standard deviation) age was 52 (9) years and the mean weight was 153 (32) lbs. Only 1% of women reported a history of heart disease; however, nearly one-quarter of women reported at least one of the following CHD risk factors: dyslipidemia (21%), hypertension (12%), or diabetes (4%). Few women reported a history of thyroid disorders (14%), cancer (3%), or coagulopathies (2%). One-third of the women had a hysterectomy and one-quarter had an oophorectomy. Many women reported caffeine (73%) or alcohol (54%) use, but few reported tobacco (8%) use. The majority of women had not received prior hormone therapy; 8% reported prior CHT use and 13% reported prior BHRT use. BHRT use Characteristics at Oakdell Pharmacy All women received progesterone (P4) as monotherapy (43%) or in combination with estrogen (57%). Few baseline characteristics differed between women on P4 monotherapy and estrogen+p4 combination therapy (Table 2). Women initiated on P4 monotherapy were younger (50 vs. 53 years, p<0.01), less likely to be hysterectomized (27% vs. 38%, p=0.02) and oophorectomized (21% vs. 32%, p=0.04), and more likely to have a history of hypertension (17% vs. 9%, p=0.04). Various compounded BHRT dosage forms were utilized (Figure 1). Topical therapy was used most often (72%), followed by oral (43%), vaginal (23%), and sublingual (4%) therapy. Some women received multiple dosage forms simultaneously. Women receiving a single dosage form were initiated on topical therapy most often (40%) followed by oral (20%) and sublingual 11
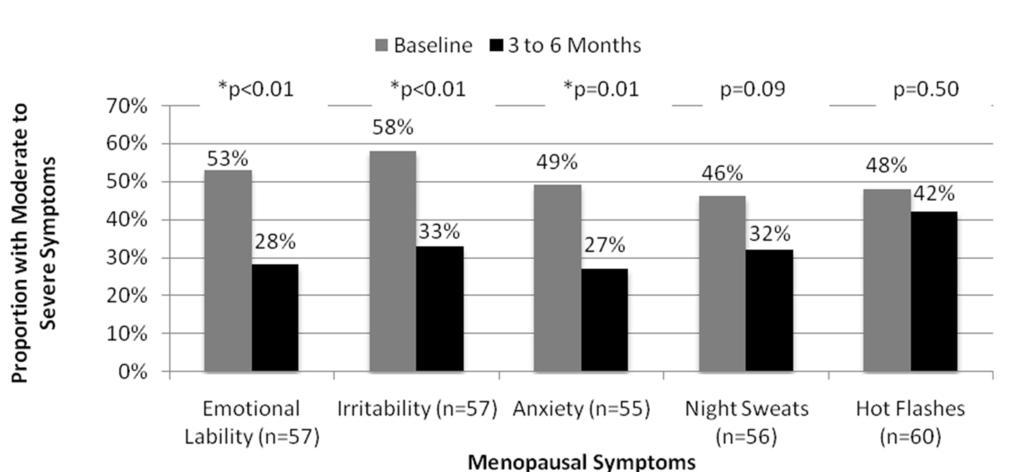
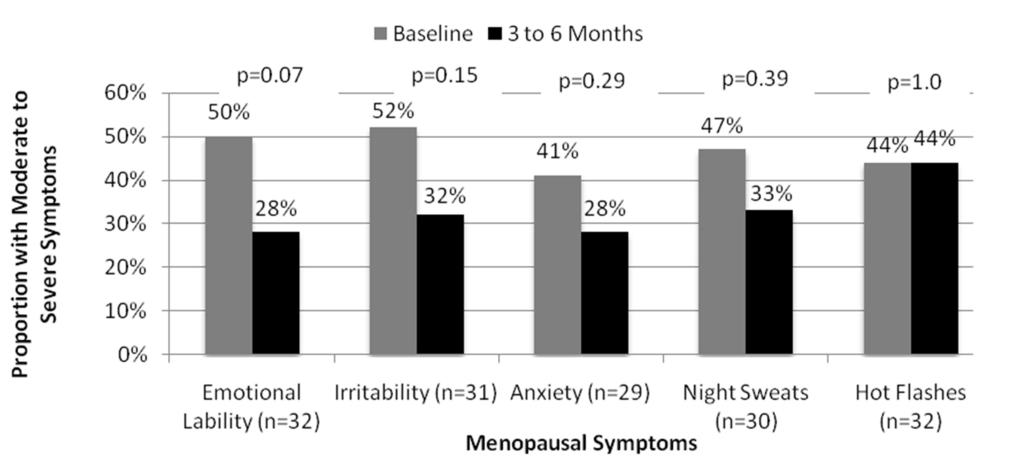
12 (2%). Women receiving combination dosage forms were initiated on topical+oral therapy most often (16%), followed by topical+vaginal therapy (12%), topical+oral+vaginal therapy (4%), oral+vaginal therapy (4%), and sublingual+oral therapy (2%). Women initiated on P4 monotherapy received more topical therapy (83% vs. 63%), and less oral (27% vs. 55%), vaginal (14% vs. 28%), and sublingual therapies (2% vs. 6%) than women initiated on estrogen+p4 combination therapy. Therapy was generally initiated at low doses (Figures 2 and Figure 3). Low-dose progesterone monotherapy was initiated in 65% of patients receiving topical therapy and 78% of patients receiving oral therapy. Low-dose estrogen was initiated in 63% of patients receiving topical therapy and 48% of patients receiving oral therapy. Biest 50/50 (51%) and biest 80/20 (45%) were the most common topical estrogen combination therapies. Biest 50/50 (53%) and triest (35%) were most common oral estrogen combination therapies. These estrogen combination therapies were also frequently initiated at low doses. BHRT Effectiveness Women initiated on compounded BHRT experienced significant reductions in moderate to severe mood symptoms within 3 to 6 months (Figure 4). Overall, women experienced a 25% decrease in emotional lability (53% vs. 28%, p<0.01), a 25% decrease in irritability (58% vs. 33%, p<0.01), and a 22% reduction in anxiety (49% vs. 27%, p=0.01). Women receiving compounded BHRT also experienced non-significant reductions in vasomotor symptoms within 3 to 6 months of therapy. Night sweats were reduced by 14% (46% vs. 32%, p=0.09) and hot flashes were reduced by 6% (48% vs. 42%, p=0.5) (Figure 4). 12
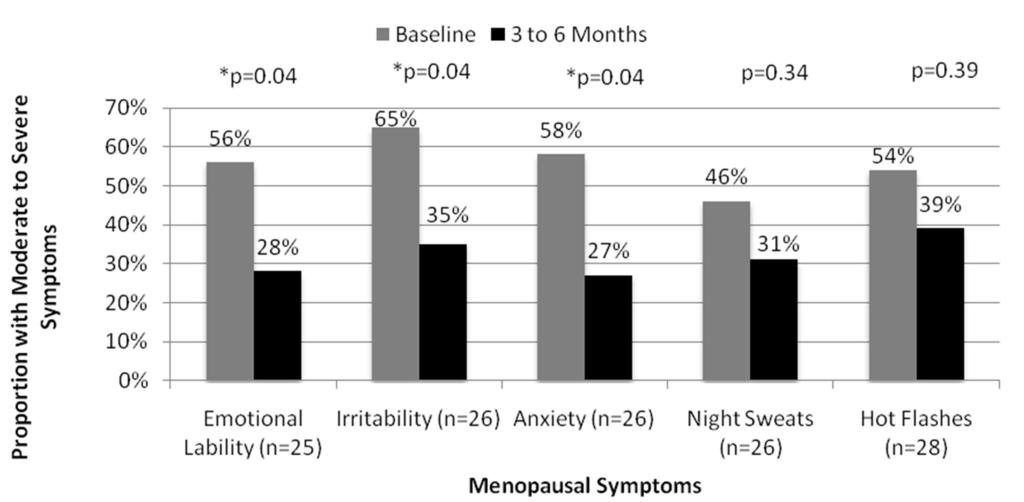
13 Women initiated on P4 monotherapy generally experienced a greater reduction in moderate to severe mood symptoms within 3 to 6 months compared to women initiated on estrogen+p4 combination therapy (Figures 5 and Figure 6). Women receiving P4 monotherapy experienced a 28% reduction in emotional lability (56% vs. 28%, p=0.04), a 30% decrease in irritability (65% vs. 35%, p=0.04), and a 31% reduction in anxiety (58% vs. 27%, p=0.04). Although non-significant, women initiated on estrogen+p4 combination therapy experienced a 22% reduction in emotional lability (50% vs. 28%, p=0.07), a 20% decrease in irritability (52% vs. 32%, p=0.15), and a 13% reduction in anxiety (41% vs. 28%, p=0.29). Moderate to severe night sweats decreased by 15% in women who received P4 monotherapy (46% vs. 31%, p=0.34) and 14% in women who received estrogen+p4 combination therapy (47% vs. 33%, p=0.39). Hot flashes were reduced by 15% with P4 monotherapy (54% vs. 39%, p=0.39) and no improvements were seen with estrogen+p4 combination therapy (44% vs. 44%, p=1.0). BHRT Safety From this cohort of 296 women initiated on compounded BHRT, 62 (21%) had documented follow-up regarding myocardial infarction and breast cancer. These 62 women had an average follow-up of 1.9 years for a total of 117 person years. During this timeframe, no woman initiated on compounded BHRT experienced a myocardial infarction (MI) or breast cancer. 13
14 Discussion This study confirms that compounded BHRT is effective for improving mood symptoms. The sample size was inadequate to draw firm conclusions regarding the utility of compounded BHRT for vasomotor symptoms, but the observed trends are encouraging. This is the first time compounded BHRT therapy has been evaluated, but there are several studies that confirm the effectiveness of manufactured BHRT. Trials have shown estrone (E1) and estradiol (E2) to be effective for reducing menopausal symptoms as monotherapy or combination therapy, but trials have not been conducted to evaluate the effectiveness of estriol (E3). The effectiveness of E1 for reducing the severity of menopausal symptoms has also been observed. Takahashi [7] conducted an open label trial in 53 women receiving 2mg E1 for 12 months. Menopausal relief was evaluated using the Kupperman index (KI) for severity. Women who underwent natural menopause experienced a 50% reduction in their KI score (p<0.01), whereas women who underwent surgical menopause experienced an 80% reduction in their score (p<0.01). The KI is a numerical conversion index of 11 menopausal symptoms (including vasomotor and mood symptoms) designed to measure total menopausal relief. Although individual symptoms were not evaluated, E1 was shown to be effective for relief of composite menopausal symptoms. Large randomized controlled trials (RCTs) have documented E2 s effectiveness for relieving menopausal symptoms [8,9]. Simon and colleagues[8] conducted a RCT in 484 women randomized to receive 0.87 grams/day (0.52mg E2), 1.7 grams/day (1.02mg E2), or 2.6 grams/day of E2 gel (1.56mg E2) for 12 weeks. Within 3 to 5 weeks, these women experienced 14
15 a reduction in hot flash severity (p<0.01) and a reduction in hot flash rate by at least 7 hot flashes/day (p<0.001). Additionally, the 1.7 grams/day E2 (1.02mg E2) improved patient s Utian Quality of Life emotional score (0.9 vs. 0.2, p<0.05). Similar to our method of evaluating severity, women reported hot flashes as severity ratings, yet limited numerical data were available to evaluate the extent of vasomotor symptom reduction. Additionally, E1 and E3 combination therapy has been shown to be effective for reducing menopausal symptoms. Padwick and colleagues[10] conducted a 6 month RCT of 20 women randomized to receive oral E2 (2mg) or oral E1 (1mg) + E2 (2mg). This study evaluated menopausal symptom relief using graphic rating scales. Women randomized to receive oral E2 (2mg) experienced a significant reduction in hot flashes (62%, p<0.01) and night sweats (77%, p<0.01), and non-significant improvements in anxiety (26%), irritability (18%), and emotional lability (5%)(p values not given). Women receiving oral E1 (1mg) + E2 (2mg) experienced significant reductions in hot flashes (41%, p<0.01), night sweats (56%, p<0.05), and anxiety (44%, p<0.01), and non-significant improvements in irritability (32%) and emotional lability (5%). Despite use of a different method to evaluate symptom relief, this study provides additional data that supports the use of combination estrogens for reducing vasomotor and mood symptoms. Although estrogens are generally regarded as the therapeutic hormones in hormone replacement therapy [11], P4 monotherapy has also been shown to be effective in treating menopausal symptoms [12-14]. Leonetti and colleagues [12]conducted a single-center RCT of 102 women within 5 years of menopause who were randomized them to receive P4 monotherapy (20 mg) or placebo. Significant improvements or resolution of vasomotor 15
16 symptoms were seen at 4 months in P4 treated patients compared to placebo (83% vs 19%; p<0.001). Two other RCTs have documented non-significant improvements in menopausal symptoms [13,14]. Wren and colleagues[13] evaluated 80 women randomized to receive topical P4 monotherapy (32 mg) or placebo. A reduction in vasomotor (-1.0 vs. 0; p=0.07) and anxiety (-1.0 vs. 0; p=0.10) symptoms was reported at 12 weeks. Another RCT conducted by Benster and colleagues[14] randomized 223 women to receive P4 monotherapy (5mg, 20mg, 40mg, and 60mg) or placebo. The investigators observed a reduction in vasomotor symptoms for P4 5mg (-0.4; p=0.22), 20mg (-0.4; p=0.23), 40mg (-0.6; p=0.06), and 60mg (-0.4; p=0.23). These trials utilized the Greene Climacteric Scale, in which patients self-rated their symptom severity (i.e. absent, mild, moderate, and severe). This approach is similar to our study. Manufactured E2+P4 combination therapy has also demonstrated effectiveness in reducing menopausal symptoms. Vashisht and colleagues[15] conducted an open label 48- week study in 41 women with the secondary objective of improvements in menopausal symptoms. Treatment with E2 gel (1mg) + P4 cream (40mg) applied daily significantly reduced moderate to severe vasomotor and anxiety symptoms at 24 weeks (p<0.05). Anxiety was further reduced at 48 weeks of therapy when compared to the reduction at 34 weeks of therapy (p<0.05). Similar to P4 monotherapy trials, the Greene Climacteric Scale was utilized to evaluate mood and vasomotor symptoms improvement. Collectively, these findings support the effectiveness of BHRT in reducing menopausal symptoms. Furthermore, this study provides some of the first clinical evidence in support of compounded BHRT. 16
17 BHRT Safety Large RCTs by the Women s Health Initiative (WHI) and Heart and Estrogen/Progestin Replacement Study (HERS) have documented deleterious effects associated with CHT in postmenopausal women. Woman randomized to receive CE + MPA combination therapy experienced a 1.47 and 1.32 fold increase in non-fatal MI in the HERS and WHI studies respectively [16,17]. The WHI also demonstrated a 1.26 fold increase in breast cancer in patients receiving CE + MPA [16]. There are currently no trials that evaluate BHRT risk for MI and breast cancer. This study only had 117 person-years of follow-up and none of these women experienced an MI or breast cancer; however, the study lacks a sufficient sample size to make firm statements about the safety of compounded BHRT. It is noteworthy that the Postmenopausal Estrogen/Progestin Interventions (PEPI) trial, Gerhard trial, and Estrogen in Prevention of Atherosclerosis (EPAT) trials have all three demonstrated that BHRT improves cardiovascular surrogate markers. Women in the PEPI trial who received CE + cyclic P4 experienced a decreased in LDL, increase in HDL, decrease in fibrinogen levels, and decrease in fasting glucose compared to those women on placebo [18]. Gerhard and colleagues[19] demonstrated that women who received transdermal E2 + cyclical vaginal P4 experienced improved vascular reactivity and an 8.4% reduction in LDL compared to placebo. Finally, the EPAT trial demonstrated that women who received oral E2 compared to placebo experienced a decrease in carotid intima thickness progression, increase in HDL, decrease in LDL, and decrease in HbA1c [20]. Based on the favorable effects on cardiovascular surrogate markers, BHRT may eventually prove to be cardio-neutral or even cardioprotective. 17
18 Smaller RCTs provide encouraging results regarding the impact of BHRT on breast cancer. Two RCTs by Chang and colleagues[21] and Foidart and colleagues[22] demonstrated that women receiving topical P4 experienced a reduction in breast epithelial proliferative markers via reductions in mitotic divisions and proliferating cell nuclear antigen (PCNA) labeling index % compared to placebo. These studies support the belief that P4 may prevent breast epithelial hyperplasia. A large observational study demonstrated that women who used E3 or estrogen+p4 combination therapy were not at increased risk of breast cancer as compared to women who had never used HRT [23]. Limitations This study has strengths and limitations. First, these six pharmacies were located in one geographical region; therefore, these findings may not be generalized to all settings. The sample size is insufficient to assess the safety of compounded BHRT or its impact on vasomotor symptoms. Our method of obtaining effectiveness data also lends itself to potential rater bias. Patients might have attempted to please the health care provider by reporting improvement in menopausal symptoms. Additionally, the rating scale utilized in the majority of manufactured BHRT clinical trials differed from this study. The Greene Climacteric Scale and The Kupperman index may be more effective for evaluating menopausal symptom outcomes with HRT. Finally, this study did not evaluate changes in regimens from baseline to follow-up (3 to 6 months); therefore, improvements in menopausal symptoms were attributed to the initial regimen women received. 18
19 Conclusions Our study is one of the first to provide clinical evidence for the effectiveness of compounded BHRT. Given the deleterious effects of CHT observed in the WHI and HERS trials, these data are of great value. Our study provides clear evidence that compounded BHRT is effective for reducing menopausal mood symptoms. Larger studies are needed to examine the impact of compounded BHRT on vasomotor symptoms and to evaluate the safety of compounded BHRT with regards to MI and breast cancer. 19
20 Competing Interests: ADR and JJC are employees of Oakdell Pharmacy, Inc. All other authors have no competing interests. Author s Contributions: Dr. Ruiz had full access to study data and was the primary person involved in the study design, study concepts, data collection, data analysis, data interpretation, and manuscript drafting. Drs. Frei and Daniels assisted in drafting the original article, were involved in study design, and manuscript editing. Dr. Barner and Mr. Carson were involved in the study design and manuscript editing. Acknowledgments: To Oakdell Pharmacy, Inc. and The University of Texas at Austin College of Pharmacy for financial support. Source of Funding: Oakdell Pharmacy Inc. and The University of Texas at Austin College of Pharmacy provided financial support for Dr. Ruiz s and Dr. Daniels training programs. 20
21 References [1] Biundo B. Personal Communication. Professional Compounding Centers of America. In. San Antonio;22 December [2] Holtorf K. The bioidentical hormone debate: are bioidentical hormones (estradiol, estriol, and progesterone) safer or more efficacious than commonly used synthetic versions in hormone replacement therapy? Postgrad Med 2009;121: [3] Lorentzen J. Hormone replacement therapy: The evolution of hormone treatment. Int J Pharmaceut Compounding 2001;5:336. [4] Wepfer S. The science behind bioidentical hormone replacement therapy. Int J Pharmaceut Compounding 2001;5:10 [5] Bachmann GA, Schaefers M, Uddin A, Utian WH. Lowest effective transdermal 17betaestradiol dose for relief of hot flushes in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2007;110: [6] Soares CN, Almeida OP, Joffe H, Cohen LS. Efficacy of estradiol for the treatment of depressive disorders in perimenopausal women: a double-blind, randomized, placebocontrolled trial. Arch Gen Psychiatry 2001;58: [7] Takahashi K, Okada M, Ozaki T, et al. Safety and efficacy of oestriol for symptoms of natural or surgically induced menopause. Hum Reprod 2000;15: [8] Simon JA, Bouchard C, Waldbaum A, Utian W, Zborowski J, Snabes MC. Low dose of transdermal estradiol gel for treatment of symptomatic postmenopausal women: a randomized controlled trial. Obstet Gynecol 2007;109:
22 [9] Notelovitz M, Lenihan JP, McDermott M, Kerber IJ, Nanavati N, Arce J. Initial 17betaestradiol dose for treating vasomotor symptoms. Obstet Gynecol 2000;95: [10] Padwick ML, Siddle NC, Lane G, et al. Oestriol with oestradiol verses oestradiol alone: a comparison of endometrial, symptomatic and psychological effects. Br J Obstet Gynaecol 1986;93: [11] Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17: [12] Leonetti HB, Longo S, Anasti JN. Transdermal progesterone cream for vasomotor symptoms and postmenopausal bone loss. Obstet Gynecol 1999;94: [13] Wren BG, Champion SM, Willetts K, Manga RZ, Eden JA. Transdermal progesterone and its effect on vasomotor symptoms, blood lipid levels, bone metabolic markers, moods, and quality of life for postmenopausal women. Menopause 2003;10:13-8. [14] Benster B, Carey A, Wadsworth F, Vashisht A, Domoney C, Studd J. A double-blind placebo-controlled study to evaluate the effect of progestelle progesterone cream on postmenopausal women. Menopause Int 2009;15:63-9. [15] Vashisht A, Wadsworth F, Carey A, Carey B, Studd J. A study to look at hormonal absorption of progesterone cream used in conjunction with transdermal estrogen. Gynecol Endocrinol 2005;21: [16] Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA 2002;288:
23 [17] Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA 1998;280: [18] Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. The Writing Group for the PEPI Trial. JAMA 1995;273: [19] Gerhard M, Walsh BW, Tawakol A, et al. Estradiol therapy combined with progesterone and endothelium-dependent vasodilation in postmenopausal women. Circulation 1998;98: [20] Hodis HN, Mack WJ, Lobo RA, et al. Estrogen in the prevention of atherosclerosis. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 2001;135: [21] Chang KJ, Lee TT, Linares-Cruz G, Fournier S, de Lignieres B. Influences of percutaneous administration of estradiol and progesterone on human breast epithelial cell cycle in vivo. Fertil Steril 1995;63: [22] Foidart JM, Colin C, Denoo X, et al. Estradiol and progesterone regulate the proliferation of human breast epithelial cells. Fertil Steril 1998;69: [23] Fournier A, Berrino F, Clavel-Chapelon F. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008;107:
24 Figure 1. Baseline BHRT Dosage Forms at Oakdell Pharmacy, n=296 Figure 2. Topical BHRT Doses at Baseline, n=210 Figure 3. Oral BHRT Doses at Baseline, N=128 Figure 4. Effectiveness of Compounded BHRT to Alleviate Moderate to Severe Menopausal Symptoms Figure 5. Effectiveness of P4 Monotherapy to Alleviate Moderate to Severe Menopausal Symptoms Figure 6. Effectiveness of Estrogen+P4 Combination Therapy to Alleviate Moderate to Severe Menopausal Symptoms 24
25 Table 1. Common Compounded Bioidentical Hormones Dose Classifications Dose Classification Dose Range Topical Estrogen Low Dose Moderate Dose High Dose 0.5mg mg >1mg Oral Estrogen Low Dose Moderate Dose High Dose 1mg 1.1-2mg >2mg Topical Progesterone Low Dose Moderate Dose High Dose <20mg 21-50mg >50mg Oral Progesterone Low Dose <100 Moderate Dose High Dose >200 25
26 Table 2. Baseline Characteristics Demographic Estrogen+P4 (N=170) P4 (N=126) P-value (Estrogen+P4 vs. P4) Age (yrs); mean (SD) 53 (7) 50 (10) <0.01 Weight (lbs); mean (SD) Comorbid Conditions; % 152 (32) 155 (32) 0.49 Heart disease Dyslipidemia Hypertension Diabetes Cancer Thyroid Coagulopathies Hysterectomized; % Ovaries Removed; % Tobacco use; % Caffeine use; % Alcohol use; % Baseline CHT; % Baseline BHRT; %
27 Figure 1
28 Figure 2
29 Figure 3
30 Figure 4
31 Figure 5
32 Figure 6
Natural Hormones Replacement An Evidence and Practice Based Approach
 Natural Hormones Replacement An Evidence and Practice Based Approach Andres Ruiz, PharmD, MSc, FACA President/Partner Stonegate Pharmacy PRESENTED BY THE AMERICAN COLLEGE OF APOTHECARIES 2830 SUMMER OAKS
Natural Hormones Replacement An Evidence and Practice Based Approach Andres Ruiz, PharmD, MSc, FACA President/Partner Stonegate Pharmacy PRESENTED BY THE AMERICAN COLLEGE OF APOTHECARIES 2830 SUMMER OAKS
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Presentation to the Clinical Utility of Treating Patients with Compounded Bioidentical Hormone Therapy
 Presentation to the Clinical Utility of Treating Patients with Compounded Bioidentical Hormone Therapy March 5, 2019 Nese Yuksel, BScPharm, PharmD, FCSHP, NCMP Professor Faculty of Pharmacy and Pharmaceutical
Presentation to the Clinical Utility of Treating Patients with Compounded Bioidentical Hormone Therapy March 5, 2019 Nese Yuksel, BScPharm, PharmD, FCSHP, NCMP Professor Faculty of Pharmacy and Pharmaceutical
Bioidentical Hormones: Just the Facts
 Bioidentical Hormones: Just the Facts Melissa McNeil, MD, MPH Professor of Medicine and Obstetrics, Gynecology and Reproductive Sciences Chief, Section of Women s Health University of Pittsburgh Disclosures!
Bioidentical Hormones: Just the Facts Melissa McNeil, MD, MPH Professor of Medicine and Obstetrics, Gynecology and Reproductive Sciences Chief, Section of Women s Health University of Pittsburgh Disclosures!
Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
 presents Converting Patients from Conventional Pioneering Technologies For to Bioidentical Lifestyle Based Medicine Hormone Therapy with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
presents Converting Patients from Conventional Pioneering Technologies For to Bioidentical Lifestyle Based Medicine Hormone Therapy with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
Post-menopausal hormone replacement therapy. Evan Klass, MD May 17, 2018
 Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice
 Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice JoAnn E. Manson, MD, DrPH, FACP Chief, Division of Preventive Medicine Interim Executive Director, Connors Center Brigham and
Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice JoAnn E. Manson, MD, DrPH, FACP Chief, Division of Preventive Medicine Interim Executive Director, Connors Center Brigham and
OBSTETRICS & GYNECOLOGY
 JANUARY 2012 COMPOUNDING PHARMACY SOLUTIONS PRESCRIPTION COMPOUNDING WWW.CPSRXS. COM We customize individual prescriptions for the specific needs of our patients. INSIDE THIS ISSUE: Female Sexual Arousal
JANUARY 2012 COMPOUNDING PHARMACY SOLUTIONS PRESCRIPTION COMPOUNDING WWW.CPSRXS. COM We customize individual prescriptions for the specific needs of our patients. INSIDE THIS ISSUE: Female Sexual Arousal
2016. All Rights Reserved. 1
 Pamela W. Smith, M.D., MPH, MS Copyright 2016 The suggested dosages are for educational purposes only. They are suggestions for patients with normal renal and hepatic function. They are based upon my research
Pamela W. Smith, M.D., MPH, MS Copyright 2016 The suggested dosages are for educational purposes only. They are suggestions for patients with normal renal and hepatic function. They are based upon my research
Answers to Your Questions on Bioidentical Hormone Therapy
 Answers to Your Questions on Bioidentical Hormone Therapy Question #1: What is bioidentical hormone therapy? There is no real scientific definition for bioidentical hormones, because this term originated
Answers to Your Questions on Bioidentical Hormone Therapy Question #1: What is bioidentical hormone therapy? There is no real scientific definition for bioidentical hormones, because this term originated
Appendix: Reference Table of HT Brand Names
 Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Postmenopausal hormones and coronary artery disease: potential benefits and risks
 CLIMACTERIC 2007;10(Suppl 2):21 26 Postmenopausal hormones and coronary artery disease: potential benefits and risks R. A. Department of Obstetrics and Gynecology, Columbia University, New York, New York,
CLIMACTERIC 2007;10(Suppl 2):21 26 Postmenopausal hormones and coronary artery disease: potential benefits and risks R. A. Department of Obstetrics and Gynecology, Columbia University, New York, New York,
Menopausal Symptoms. Hormone Therapy Products Available in Canada for the Treatment of. Physician Desk Reference - 3rd Edition
 Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
WHI Estrogen--Progestin vs. Placebo (Women with intact uterus)
") HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
OBSTETRICS & GYNECOLOGY
 AUGUST 2011 NORLAND AVENUE PHARMACY PRESCRIPTION COMPOUNDING N ORLANDA VENUEP HARMACY. COM We customize individual prescriptions for the specific needs of our patients. INSIDE THIS ISSUE: BHRT for Menopause
AUGUST 2011 NORLAND AVENUE PHARMACY PRESCRIPTION COMPOUNDING N ORLANDA VENUEP HARMACY. COM We customize individual prescriptions for the specific needs of our patients. INSIDE THIS ISSUE: BHRT for Menopause
25 mg oestradiol implants--the dosage of first choice for subcutaneous oestrogen replacement therapy?
 Research Subcutaneous estrogen replacement therapy. Jones SC. Journal of Reproductive Medicine March, 2004; 49(3):139-142. Department of Obstetrics and Gynecology, Keesler Medical Center, Keesler Air Force
Research Subcutaneous estrogen replacement therapy. Jones SC. Journal of Reproductive Medicine March, 2004; 49(3):139-142. Department of Obstetrics and Gynecology, Keesler Medical Center, Keesler Air Force
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc.
 OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
Women s Health: Managing Menopause. Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School
 Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Therapeutic Cohort Results
 Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
Hormone therapy for menopausal vasomotor symptoms
 Hormone therapy for menopausal vasomotor symptoms Given our available (better) options for treating hot flashes, can we reduce our use of medroxyprogesterone acetate? OBG Manag. 2014;26(7):10,13 15. Robert
Hormone therapy for menopausal vasomotor symptoms Given our available (better) options for treating hot flashes, can we reduce our use of medroxyprogesterone acetate? OBG Manag. 2014;26(7):10,13 15. Robert
HT: Where do we stand after WHI?
 HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
Management of Perimenopausal symptoms
 Management of Perimenopausal symptoms Serge Rozenberg CHU St Pierre Université libre de Bruxelles Belgium serge_rozenberg@stpierre-bru.be serge.rozenberg@skynet.be Conflict of interest & Disclosure Conflicts
Management of Perimenopausal symptoms Serge Rozenberg CHU St Pierre Université libre de Bruxelles Belgium serge_rozenberg@stpierre-bru.be serge.rozenberg@skynet.be Conflict of interest & Disclosure Conflicts
MENOPAUSE. I have no disclosures 10/11/18 OBJECTIVES WHAT S NEW? WHAT S SAFE?
 MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
Sex, hormones and the heart
 Sex, hormones and the heart Dr Louise Newson BSc(Hons) MBChB(Hons) MRCP FRCGP www.menopausedoctor.co.uk #IandA2017 Declaration I have had financial relationships (lecturer, writer, member of advisory boards
Sex, hormones and the heart Dr Louise Newson BSc(Hons) MBChB(Hons) MRCP FRCGP www.menopausedoctor.co.uk #IandA2017 Declaration I have had financial relationships (lecturer, writer, member of advisory boards
Arizona Natural Medicine, L.L.C W. Ray Road, Suite 1, Chandler, AZ
 MENOPAUSE: THE ROAD TO HARMONY by Dr. Sarv Varta Khalsa, N.M.D. Have you been feeling like your emotions are out of control lately? Do you feel irritable one minute, snapping impatiently at your family
MENOPAUSE: THE ROAD TO HARMONY by Dr. Sarv Varta Khalsa, N.M.D. Have you been feeling like your emotions are out of control lately? Do you feel irritable one minute, snapping impatiently at your family
Navigating the Change: Leading Patients Through Menopause
 4:30pm - 5:30pm: Breakout 5 - Women s Health Option A: Navigating the Change: Leading Patients Through Menopause ACPE UAN 0107-0000-10-025-L01-P 0.1 CEU/1.0 Hr. Activity Type: Application-Based Program
4:30pm - 5:30pm: Breakout 5 - Women s Health Option A: Navigating the Change: Leading Patients Through Menopause ACPE UAN 0107-0000-10-025-L01-P 0.1 CEU/1.0 Hr. Activity Type: Application-Based Program
KAJARIN Pure Reflections of Nature
 KAJARIN Pure Reflections of Nature FAQS - General Guidelines What is the dosage of the active ingredients in Kajarin products? 4 Balance has approximately 28.9mg of Progesterone per pump 4 Balance Plus
KAJARIN Pure Reflections of Nature FAQS - General Guidelines What is the dosage of the active ingredients in Kajarin products? 4 Balance has approximately 28.9mg of Progesterone per pump 4 Balance Plus
Department of Obstetrics and Gynecology, Osaka Medical College, Takatsuki-city, Osaka , Japan. Pituitary gonadotropin, Clinical managament
 Original Article Adequate Reduction Degree of Pituitary Gonadotropin Level in the Clinical Management of Short-Term Hormone Replacement Therapy of Women with Menopausal Symptoms Department of Obstetrics
Original Article Adequate Reduction Degree of Pituitary Gonadotropin Level in the Clinical Management of Short-Term Hormone Replacement Therapy of Women with Menopausal Symptoms Department of Obstetrics
Financial Conflicts of Interest
 Hormone Treatment of Menopausal Women: What Are the Data Telling Us (and Not Telling Us)? S. Mitchell Harman, M.D., Ph.D. Chief, Endocrine Division Phoenix VA Health Care System Clinical Professor, Medicine
Hormone Treatment of Menopausal Women: What Are the Data Telling Us (and Not Telling Us)? S. Mitchell Harman, M.D., Ph.D. Chief, Endocrine Division Phoenix VA Health Care System Clinical Professor, Medicine
Menopause and HRT. John Smiddy and Alistair Ledsam
 Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
HRT in Perimenopausal Women. Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College
 HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
Effects of TX-001HR on Uterine Bleeding Rates in Menopausal Women with Vasomotor Symptoms
 Effects of TX-001HR on Uterine Bleeding Rates in Menopausal Women with Vasomotor Symptoms Photo (compulsory) Steven R Goldstein, MD 1 ; Ginger D Constantine, MD 2 ; David F Archer, MD 3 ; James H Pickar,
Effects of TX-001HR on Uterine Bleeding Rates in Menopausal Women with Vasomotor Symptoms Photo (compulsory) Steven R Goldstein, MD 1 ; Ginger D Constantine, MD 2 ; David F Archer, MD 3 ; James H Pickar,
5. Summary of Data Reported and Evaluation
 326 5. Summary of Data Reported and Evaluation 5.1 Exposure data Combined estrogen progestogen menopausal therapy involves the co-administration of an estrogen and a progestogen to peri- or postmenopausal
326 5. Summary of Data Reported and Evaluation 5.1 Exposure data Combined estrogen progestogen menopausal therapy involves the co-administration of an estrogen and a progestogen to peri- or postmenopausal
Coronary Heart Disease in Women Go Red for Women
 Coronary Heart Disease in Women Go Red for Women Dr Fiona Stewart Green Lane Cardiovascular Service and National Women s Health Auckland City Hospital Auckland Heart Group Women are Different from Men
Coronary Heart Disease in Women Go Red for Women Dr Fiona Stewart Green Lane Cardiovascular Service and National Women s Health Auckland City Hospital Auckland Heart Group Women are Different from Men
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Low & Ultra Low Dose HRT The Cardiovascular Impact
 Low & Ultra Low Dose HRT The Cardiovascular Impact Wyeth Symposium, Turin 29 th Sept 2007 Nick Panay Consultant Gynaecologist Queen Charlotte s & Chelsea and Chelsea & Westminster Hospitals Honorary Senior
Low & Ultra Low Dose HRT The Cardiovascular Impact Wyeth Symposium, Turin 29 th Sept 2007 Nick Panay Consultant Gynaecologist Queen Charlotte s & Chelsea and Chelsea & Westminster Hospitals Honorary Senior
AusPharm CE Hormone therapy 23/09/10. Hormone therapy
 Hormone therapy Learning objectives: Assess options to address quality of life and health concerns of menopausal women Outline indications for hormone therapy Counsel women on the risks and benefits of
Hormone therapy Learning objectives: Assess options to address quality of life and health concerns of menopausal women Outline indications for hormone therapy Counsel women on the risks and benefits of
SERMS, Hormone Therapy and Calcitonin
 SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
Postmenopausal hormone therapy - cardiac disease risks and benefits
 Postmenopausal hormone therapy - cardiac disease risks and benefits Tomi S. Mikkola, MD Helsinki University Central Hospital Department of Obstetrics and Gynecology Helsinki, Finland Disclosures Speaker/consulting
Postmenopausal hormone therapy - cardiac disease risks and benefits Tomi S. Mikkola, MD Helsinki University Central Hospital Department of Obstetrics and Gynecology Helsinki, Finland Disclosures Speaker/consulting
WEIGHING UP THE RISKS OF HRT. Department of Endocrinology Chris Hani Baragwanath Academic Hospital
 WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
How HRT Hurts the Heart
 How HRT Hurts the Heart Coronary artery disease (CAD) is a killer and recent studies have come up with evidence that HRT might have a role in increasing CAD among women. Why? Zaheer Lakhani, MD, FRCP For
How HRT Hurts the Heart Coronary artery disease (CAD) is a killer and recent studies have come up with evidence that HRT might have a role in increasing CAD among women. Why? Zaheer Lakhani, MD, FRCP For
The 6 th Scientific Meeting of the Asia Pacific Menopause Federation
 Predicting the menopause The menopause marks the end of ovarian follicular activity and is said to have occurred after 12 months amenorrhoea. The average age of the menopause is between 45 and 60 years
Predicting the menopause The menopause marks the end of ovarian follicular activity and is said to have occurred after 12 months amenorrhoea. The average age of the menopause is between 45 and 60 years
UPDATE: Women s Health Issues
 UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
BioIdentical Hormone Replacement Therapy for Women
 BioIdentical Hormone Replacement Therapy for Women Bio-Identical Hormones are manufactured hormone products from soy or yam. They are changed in a laboratory so that the hormones produced are identical
BioIdentical Hormone Replacement Therapy for Women Bio-Identical Hormones are manufactured hormone products from soy or yam. They are changed in a laboratory so that the hormones produced are identical
Menopause 101. Sharzad Green, Pharm.D. Community Clinical Pharmacy
 Menopause 101 Sharzad Green, Pharm.D. Community Clinical Pharmacy 1 She has such different moods. One day she is all smiles and happiness. Other days there is no living with her. Throughout a woman s life,
Menopause 101 Sharzad Green, Pharm.D. Community Clinical Pharmacy 1 She has such different moods. One day she is all smiles and happiness. Other days there is no living with her. Throughout a woman s life,
Supplementary Online Content
 Supplementary Online Content Gartlehner G, Patel SV, Feltner C, et al. Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Women: Evidence Report and Systematic Review for
Supplementary Online Content Gartlehner G, Patel SV, Feltner C, et al. Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Women: Evidence Report and Systematic Review for
Outline. Estrogens and SERMS The forgotten few! How Does Estrogen Work in Bone? Its Complex!!! 6/14/2013
 Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Hormones friend or foe? Undertreatment and quality of life. No conflicts of interest to declare
 Hormones friend or foe? Undertreatment and quality of life Anette Tønnes Pedersen MD, Ph.D. Consultant, Associate professor Dept. Of Gynecology / Fertility Clinic Rigshospitalet No conflicts of interest
Hormones friend or foe? Undertreatment and quality of life Anette Tønnes Pedersen MD, Ph.D. Consultant, Associate professor Dept. Of Gynecology / Fertility Clinic Rigshospitalet No conflicts of interest
Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD
 Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD JoAnn V. Pinkerton, MD Professor of Obstetrics and Gynecology Director,
Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD JoAnn V. Pinkerton, MD Professor of Obstetrics and Gynecology Director,
Estrogen and progestogen therapy in postmenopausal women
 Estrogen and progestogen therapy in postmenopausal women The Practice Committee of the American Society for Reproductive Medicine American Society for Reproductive Medicine, Birmingham, Alabama Hormone
Estrogen and progestogen therapy in postmenopausal women The Practice Committee of the American Society for Reproductive Medicine American Society for Reproductive Medicine, Birmingham, Alabama Hormone
Stella Milsom. Endocrinologist Fertility Associates Auckland
 Stella Milsom Endocrinologist Fertility Associates Auckland 8:30-9:25 WS #71: Bio-Identical Hormone Therapy - Fact or Fiction 9:35-10:30 WS #81: Bio-Identical Hormone Therapy - Fact or Fiction (Repeated)
Stella Milsom Endocrinologist Fertility Associates Auckland 8:30-9:25 WS #71: Bio-Identical Hormone Therapy - Fact or Fiction 9:35-10:30 WS #81: Bio-Identical Hormone Therapy - Fact or Fiction (Repeated)
PERIMENOPAUSE. Objectives. Disclosure. The Perimenopause Perimenopause Menopause. Definitions of Menopausal Transition: STRAW.
 PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
The Practice Committee of the American Society for Reproductive Medicine,
 FERTILITY AND STERILITY VOL. 81, NO. 1, JANUARY 2004 Copyright 2004 American Society for Reproductive Medicine Published by Elsevier Inc. Printed on acid-free paper in U.S.A. PRACTICE COMMITTEE Estrogen
FERTILITY AND STERILITY VOL. 81, NO. 1, JANUARY 2004 Copyright 2004 American Society for Reproductive Medicine Published by Elsevier Inc. Printed on acid-free paper in U.S.A. PRACTICE COMMITTEE Estrogen
Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be
 is a big decision and should be") Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be made with input from your healthcare provider. After the decision has been made to take HT, many women don t realize
Deciding whether or not to use Hormone Therapy (HT) is a big decision and should be made with input from your healthcare provider. After the decision has been made to take HT, many women don t realize
Hormone Restoration and Support
 Hormone Restoration and Support As a doctor with a strong interest in functional medicine, I strive to help my patients to achieve optimal health in the best ways I know how. This encompasses a combined,
Hormone Restoration and Support As a doctor with a strong interest in functional medicine, I strive to help my patients to achieve optimal health in the best ways I know how. This encompasses a combined,
Hormones. Synthetic. Bioidentical. vs. SPECIAL REPORT. for Menopause. by Dr. Mark Stengler
 SPECIAL REPORT Synthetic vs. Bioidentical Hormones for Menopause by Dr. Mark Stengler www.markstengler.com All rights reserved. This program, or parts thereof, may not be reproduced in any form without
SPECIAL REPORT Synthetic vs. Bioidentical Hormones for Menopause by Dr. Mark Stengler www.markstengler.com All rights reserved. This program, or parts thereof, may not be reproduced in any form without
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
HOW TO MAKE SENSE OF MENOPAUSE. by Steven. F. Hotze, M.D.
 HOW TO MAKE SENSE OF MENOPAUSE by Steven. F. Hotze, M.D. INTRODUCTION Dr. Hotze is founder of Hotze Health & Wellness Center and author of the book Hormones, Health, and Happiness. He has enabled thousands
HOW TO MAKE SENSE OF MENOPAUSE by Steven. F. Hotze, M.D. INTRODUCTION Dr. Hotze is founder of Hotze Health & Wellness Center and author of the book Hormones, Health, and Happiness. He has enabled thousands
Postmenopausal hormone therapy and cancer risk
 International Congress Series 1279 (2005) 133 140 www.ics-elsevier.com Postmenopausal hormone therapy and cancer risk P. Kenemans*, R.A. Verstraeten, R.H.M. Verheijen Department of Obstetrics and Gynaecology,
International Congress Series 1279 (2005) 133 140 www.ics-elsevier.com Postmenopausal hormone therapy and cancer risk P. Kenemans*, R.A. Verstraeten, R.H.M. Verheijen Department of Obstetrics and Gynaecology,
Restore Balance. Three simple steps to hormone therapy that works. Feel and look great with bioidentical hormone therapy as individual as you!
 Restore Balance Three simple steps to hormone therapy that works Feel and look great with bioidentical hormone therapy as individual as you! Hormone therapy can alleviate the symptoms of menopause and
Restore Balance Three simple steps to hormone therapy that works Feel and look great with bioidentical hormone therapy as individual as you! Hormone therapy can alleviate the symptoms of menopause and
A Practitioner s Toolkit for the Management of the Menopause
 Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Virtual Mentor Ethics Journal of the American Medical Association November 2005, Volume 7, Number 11
 Virtual Mentor Ethics Journal of the American Medical Association November 2005, Volume 7, Number 11 Clinical Pearl Post Women's Health Initiative Menopausal Women and Hormone Therapy by JoAnn V. Pinkerton,
Virtual Mentor Ethics Journal of the American Medical Association November 2005, Volume 7, Number 11 Clinical Pearl Post Women's Health Initiative Menopausal Women and Hormone Therapy by JoAnn V. Pinkerton,
Menopausal hormone therapy currently has no evidence-based role for
 IN PERSPECTIVE HT and CVD Prevention: From Myth to Reality Nanette K. Wenger, M.D. What the studies show, in a nutshell The impact on coronary prevention Alternative solutions Professor of Medicine (Cardiology),
IN PERSPECTIVE HT and CVD Prevention: From Myth to Reality Nanette K. Wenger, M.D. What the studies show, in a nutshell The impact on coronary prevention Alternative solutions Professor of Medicine (Cardiology),
OVERVIEW OF MENOPAUSE
 OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals
 Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals Literature Review (January 2009) Hormone Therapy for Women Women's Health
Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals Literature Review (January 2009) Hormone Therapy for Women Women's Health
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Difference between vagifem and yuvafem
 Difference between vagifem and yuvafem Generally, when estrogen is prescribed for a postmenopausal woman with a uterus, a progestin should also be considered to reduce the risk of endometrial cancer. Estrogen-alone
Difference between vagifem and yuvafem Generally, when estrogen is prescribed for a postmenopausal woman with a uterus, a progestin should also be considered to reduce the risk of endometrial cancer. Estrogen-alone
Controversies in Primary Care Pros and Cons of HRT on patients with CHD
 Controversies in Primary Care Pros and Cons of HRT on patients with CHD Claire Bellone MSc Clinical Nurse Specialist Menopause Nottingham Declaration Honorariums & Sponsorship from Bayer, Novonortis, Wyeth
Controversies in Primary Care Pros and Cons of HRT on patients with CHD Claire Bellone MSc Clinical Nurse Specialist Menopause Nottingham Declaration Honorariums & Sponsorship from Bayer, Novonortis, Wyeth
Bioidentical Hormones
 2014 Bioidentical Hormones Bioidentical Hormones for Menopause-related Vasomotor Symptoms What are menopause-related vasomotor symptoms? Menopause is defined as not menstruating (having your period) for
2014 Bioidentical Hormones Bioidentical Hormones for Menopause-related Vasomotor Symptoms What are menopause-related vasomotor symptoms? Menopause is defined as not menstruating (having your period) for
HRT & Menopause Where Do We Stand Now?
 HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
22/09/2014. Menopause Management. Menopause. Menopause symptoms
 Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
Current Topics in Hormone Replacement Therapy
 Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Menopause: diagnosis and management NICE guideline NG23. Published November 2015
 Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK
 2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
What s New in Menopause Management. Objectives
 What s New in Menopause Management Leslee L. Subak, MD Professor of Obstetrics, Gynecology & Reproductive Science University of California, San Francisco Objectives Define the menopause transition Review
What s New in Menopause Management Leslee L. Subak, MD Professor of Obstetrics, Gynecology & Reproductive Science University of California, San Francisco Objectives Define the menopause transition Review
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
Menopausal Management: What Has Changed?
 Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
New products and regimens (since 2003)
") CLIMACTERIC 2007;10(Suppl 2):109 114 New products and regimens (since 2003) N. West London Menopause & PMS Centre, London, UK Key words: HORMONE REPLACEMENT THERAPY, ULTRA-LOW-DOSE THERAPY, TRANSDERMAL
CLIMACTERIC 2007;10(Suppl 2):109 114 New products and regimens (since 2003) N. West London Menopause & PMS Centre, London, UK Key words: HORMONE REPLACEMENT THERAPY, ULTRA-LOW-DOSE THERAPY, TRANSDERMAL
James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
 Disclosure Estrogen Therapy After Postmenopausal Hysterectomy: Issues, Challenges, Risks/Benefits James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
Disclosure Estrogen Therapy After Postmenopausal Hysterectomy: Issues, Challenges, Risks/Benefits James H. Liu, M.D. Arthur H. Bill Professor Chair of Reproductive Biology Dept of Obstetrics and Gynecology
Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting Disclosure
 Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting 2015 Disclosure The faculty and planners for this activity, as well as the CME staff, do not have any relevant
Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting 2015 Disclosure The faculty and planners for this activity, as well as the CME staff, do not have any relevant
WARNING LETTER DEPARTMENT OF HEALTH & HUMAN SERVICES TRANSMITTED BY FACSIMILE
 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration Rockville, MD 20857 TRANSMITTED BY FACSIMILE Carole S. Ben-Maimon, M.D. President and Chief Operating Officer One
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration Rockville, MD 20857 TRANSMITTED BY FACSIMILE Carole S. Ben-Maimon, M.D. President and Chief Operating Officer One
HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL
 HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL INTRODUCTION NORMAL WOMEN HAVE MENOPAUSE AT A MEAN AGE OF 51 YEARS, WITH 95 PERCENT
HORMONE REPLACEMENT THERAPY-UPDATE KHALED SAKHEL, MD FACOG FACS FAIUM ASSOCIATE PROFESSOR EASTERN VIRGINIA MEDICAL SCHOOL INTRODUCTION NORMAL WOMEN HAVE MENOPAUSE AT A MEAN AGE OF 51 YEARS, WITH 95 PERCENT
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts
 Benefits & Risks - The Facts") Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Hormone Replacement Therapy (HRT) Benefits & Risks - The Facts HRT is a prescription only treatment that replaces some of the lost oestrogen and progesterone hormones which occur during menopause. It can
Hormone therapy. Dr. med. Frank Luzuy
 Hormone therapy Dr. med. Frank Luzuy Reasons for Initiating/Continuing HT* Menopause-Related Symptoms Osteoporosis, Bone Loss, Fracture Prevention Doctor Prescribed It, Told Me to Take It Cardiovascular
Hormone therapy Dr. med. Frank Luzuy Reasons for Initiating/Continuing HT* Menopause-Related Symptoms Osteoporosis, Bone Loss, Fracture Prevention Doctor Prescribed It, Told Me to Take It Cardiovascular
The preferred treatment for osteoporosis
 Alternate Options to Hormone Replacement Therapy for Osteoporosis James R. Shoemaker, DO Andrea B. Klemes, DO This presentation, developed from a symposium lecture at the 40th Annual Convention of the
Alternate Options to Hormone Replacement Therapy for Osteoporosis James R. Shoemaker, DO Andrea B. Klemes, DO This presentation, developed from a symposium lecture at the 40th Annual Convention of the
One Day Hormone Check
 One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
One Day Hormone Check Patient: EMILY TEST DOB: January 18, 1948 Sex: F MRN: 0000000004 Order Number: J5070009 Completed: March 07, 2014 Received: March 07, 2014 Collected: March 07, 2014 Alec Smart, ND
Long-term safety of unopposed estrogen used by women surviving myocardial infarction: 14-year follow-up of the ESPRIT randomised controlled trial
 DOI: 10.1111/1471-0528.12598 www.bjog.org Epidemiology Long-term safety of unopposed estrogen used by women surviving myocardial infarction: 14-year follow-up of the ESPRIT randomised controlled trial
DOI: 10.1111/1471-0528.12598 www.bjog.org Epidemiology Long-term safety of unopposed estrogen used by women surviving myocardial infarction: 14-year follow-up of the ESPRIT randomised controlled trial
Something has changed? The literature from 2008 to present?
 Something has changed? The literature from 2008 to present? Elina Hemminki National Institute for Health and Welfare, Helsinki, Finland Rome Oct 7, 2011: Post-menopausal hormone therapy and women's information
Something has changed? The literature from 2008 to present? Elina Hemminki National Institute for Health and Welfare, Helsinki, Finland Rome Oct 7, 2011: Post-menopausal hormone therapy and women's information
Potential dangers of hormone replacement therapy in women at high risk
 ESC meeting, Stockholm, August 30, 16.30-18.00, 2010 Potential dangers of hormone replacement therapy in women at high risk Karin Schenck-Gustafsson MD, PhD, FESC Professor, Chief consultant Department
ESC meeting, Stockholm, August 30, 16.30-18.00, 2010 Potential dangers of hormone replacement therapy in women at high risk Karin Schenck-Gustafsson MD, PhD, FESC Professor, Chief consultant Department
Case Presentation. Learning Objectives. Case Presentation. Case Presentation
 Learning Objectives To apply up to date information about the natural history of menopause to improve the care of individual women To counsel women about the risks and benefits of systemic hormone therapy
Learning Objectives To apply up to date information about the natural history of menopause to improve the care of individual women To counsel women about the risks and benefits of systemic hormone therapy
Ms. Y. Outline. Updates of SERMs and Estrogen
 Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Hormone Consultation for Women
 Healthway Compounding Pharmacy 2544 McLeod Dr. N., Ste. 2 Saginaw, MI 48604 989-791-1691 Toll Free: 866-883-8868 Fax: 989-791-4603 Hormone Consultation for Women Today s Date: / / Patient Name: Birth date:
Healthway Compounding Pharmacy 2544 McLeod Dr. N., Ste. 2 Saginaw, MI 48604 989-791-1691 Toll Free: 866-883-8868 Fax: 989-791-4603 Hormone Consultation for Women Today s Date: / / Patient Name: Birth date:
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D
 HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
Balancing Hormone Function in Women By Meghna Thacker, NMD
 Balancing Hormone Function in Women By Meghna Thacker, NMD Hormone function is central to health and well being in both men as well as women. A problem encountered with any one endocrine gland can lead
Balancing Hormone Function in Women By Meghna Thacker, NMD Hormone function is central to health and well being in both men as well as women. A problem encountered with any one endocrine gland can lead
presents with Ken Sekine, MD
 presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice
presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice