Pain, Opioids and the EMR. Dr. Gordon Schacter April 12, 2018
|
|
|
- Christal Douglas
- 6 years ago
- Views:
Transcription
1 Pain, Opioids and the EMR Dr. Gordon Schacter April 12, 2018
2 Faculty/Presenter Disclosure Faculty: Gordon Schacter Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: Merck Frost Consulting Fees: KGK Science, Trial Management Group Other: London Middlesex Clinical Lead South West LHIN
3 Disclosure of Commercial Support No Commercial Support Potential for conflict(s) of interest: None
4 Mitigating Potential Bias No drug names are used. No specific EMR vendors names are used. Resources are provided.
5 Background Focus on Chronic Non-Cancer Pain not Acute Pain Resources: Guideline for opioid therapy and chronic noncancer pain. CMAJ May 08, (18) E659- E666; Centre for Effective Practice: Management of Chronic Non Cancer Pain Tool Health Quality Ontario Quality Standards: Opioid Prescribing for Chronic Pain 4
6 Management of Chronic Non-Cancer Pain Step 1: Comprehensive Assessment May need to be completed over more than one visit. Step 2: Management Options Select non-pharmacological and/or pharmacological therapies. (Non-opioids and opioids) Step 3: Initiate, Adapt and Evaluate Step 4: Refer as Appropriate 5
7 Step 1: Comprehensive Assessment People with chronic pain receive a comprehensive assessment, including consideration of their functional status and social determinants of health. A comprehensive assessment includes an assessment of the following The pain condition Any other medical conditions Psychosocial history, including history of trauma Mental health status Medication and substance use history Functional status Sleep patterns Past and current substance use disorder Past pain management and coping strategies 6
8 Comprehensive Assessment People with chronic pain receive a comprehensive assessment, including consideration of their functional status and social determinants of health. A comprehensive assessment includes an assessment of the following The pain condition Any other medical conditions Psychosocial history, including history of trauma Mental health status Medication and substance use history Functional status Sleep patterns Past and current substance use disorder Past pain management and coping strategies 7
9 Comprehensive Assessment The Pain Condition Identify pain diagnoses, e.g., OA, FM or NP If suspected Complex Regional Pain Syndrome (CRPS), consider urgent referral Pain Intensity Exacerbating and alleviating factors Character Systemic symptoms Duration 8

10 OPQRSTUV 9
11 Comprehensive Assessment The Pain Condition Past investigations/consultations Response to current/past treatments (consider whether trial was long enough to evaluate efficacy/side effects) Past medical history Current medications (including prescription, nonprescription, and natural products) 10
12 Comprehensive Assessment People with chronic pain receive a comprehensive assessment, including consideration of their functional status and social determinants of health. A comprehensive assessment includes an assessment of the following The pain condition Any other medical conditions Psychosocial history, including history of trauma Mental health status Medication and substance use history Functional status Sleep patterns Past and current substance use disorder Past pain management and coping strategies 11
13 Comprehensive Assessment Mental Health Status Current and past psychiatric history (e.g., depression PHQ-9[iii],anxiety GAD-7[iv], PTSD) Family psychiatric history Assess psychological yellow flags 12
14 PHQ-9 & GAD-7 13
15 Psychological Yellow Flags 14
16 Comprehensive Assessment People with chronic pain receive a comprehensive assessment, including consideration of their functional status and social determinants of health. A comprehensive assessment includes an assessment of the following The pain condition Any other medical conditions Psychosocial history, including history of trauma Mental health status Medication and substance use history Functional status Sleep patterns Past and current substance use disorder Past pain management and coping strategies 15
17 Comprehensive Assessment Substance use/abuse history Review history of substance use, abuse, and addiction (start with family history then personal history): Alcohol, cannabis, prescription medications, illicit drugs Attendance at an addiction treatment program May use Opioid Risk Tool, however, it has insufficient accuracy for risk stratification Use urine drug testing before starting opioid therapy. Consider annual urine drug testing (or more often, as appropriate) for the use of opioid medication and/or illicit drugs 16
18 Opioid Risk Tool 17
19 Comprehensive Assessment People with chronic pain receive a comprehensive assessment, including consideration of their functional status and social determinants of health. A comprehensive assessment includes an assessment of the following The pain condition Any other medical conditions Psychosocial history, including history of trauma Mental health status Medication and substance use history Functional status Sleep patterns Past and current substance use disorder Past pain management and coping strategies 18
20 Functional Status is a person s ability to perform activities of daily living, work, play, and socialization. Use a validated measure. e.g. Brief Pain Inventory 19

21 Brief Pain Inventory 20
22 Social Determinants of Health The social determinants of health include, but are not limited to, the following: Education Employment Family and social support Geographic location Housing Income Transportation and access to care 21
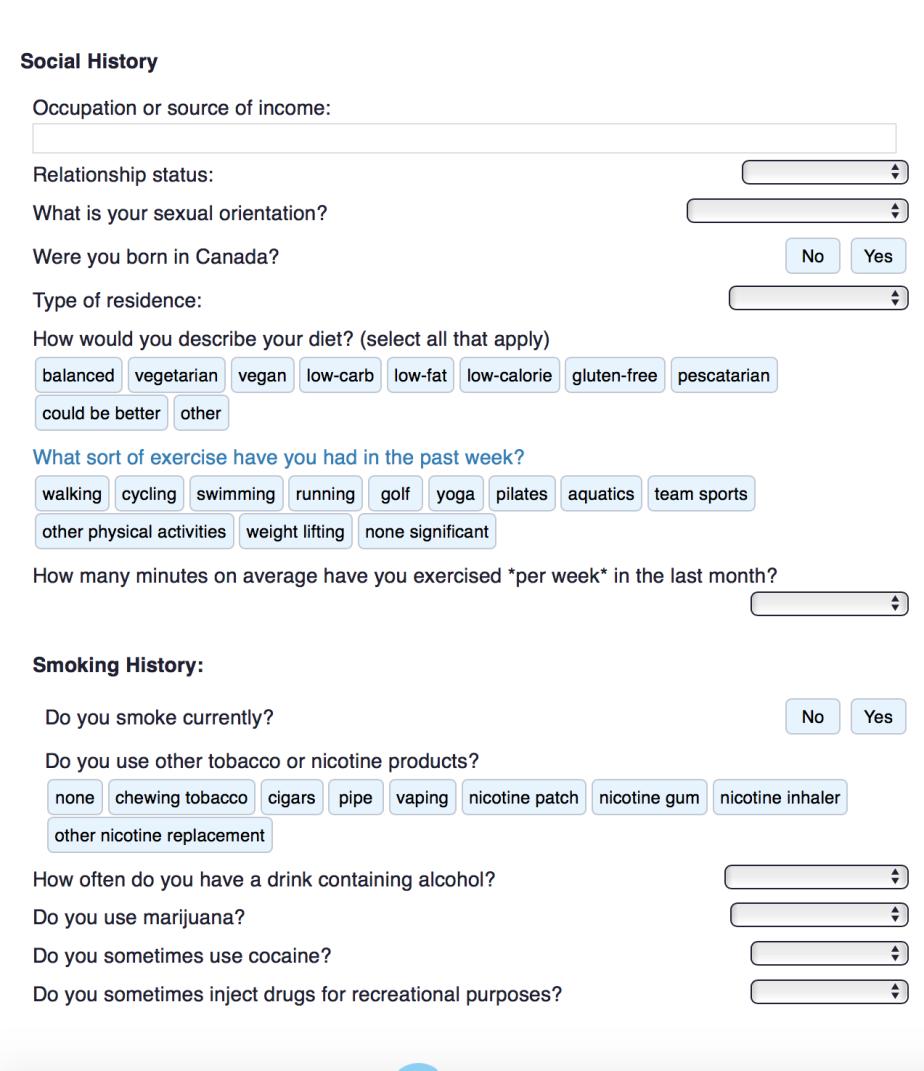
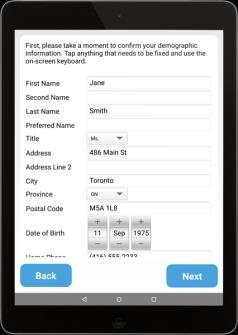
23 SDH Tablet-Based Tools 22
24 Setting Goals for Pain Relief and Function People with chronic pain set goals for pain relief and functional improvement in partnership with their health care professionals. These goals are evaluated regularly. Regular evaluation of goals Management goals should be documented and monitored over time. After initiating an opioid prescription, health care professionals should see the person with chronic pain for follow-up within 28 days. Progress toward management goals should then be reassessed within 2 to 3 months. 23
25 Patient Goals 24
26 Step 2: Management Options First-Line Treatment With Non-opioid Therapies People with chronic pain receive a multimodal combination of non-opioid pharmacotherapy and nonpharmacological therapies as first-line treatment. These therapies are ideally delivered through a multidisciplinary approach. 25
27 Non Pharmacological Therapies Physical Activity Psychological Therapy CBT Physical Therapy Self Management 26


28 Self Management LHIN 1 health-condition LHIN 2 management.ca LHIN 3 management.ca 27
29 Information on Harms of Opioid Use and Shared Decision-Making People with chronic pain, and their families and caregivers as appropriate, receive information about the potential benefits and harms of opioid therapy at the time of both prescribing and dispensing so that they can participate in shared decision-making. 28
30 Opioid Information - Handout Michael G. DeGroote National Pain Centre! Searc h... McMaster FHS NPC Home About Guidelines News Events Links Feedback Contact Canadian Guideline for Safe and E ffective Use of Opioids for Chronic Non-Cancer Pain Appendix B-4: Opioid Information for Patients [BACK] [TOC] [SITE MAP] NOTE: These messages could be used to create patient education materials. Messages for Patients Taking Opioids Note: Opioids are a group of similar medications that are used to help with pain there is more than one type of opioid and they have different names for example, Percocet, OxyContin, Tylenol No. 2, Tramacet. 1. Opioids are used to improve your ability to be active and reduce pain. You and your doctor will set goals and ensure the medication is effective in achieving the goals, e.g. improving your ability to do the things you did before pain prevented you. If you seem to benefit from the pain medication, your doctor will see you for follow-up visits to assess pain relief, any adverse effects, and your ability to meet your set activity goals. 2. There are side effects from opioids, but they can be mostly controlled with increasing your dose slowly. Common side effects include: nausea (28% of patients report it), constipation (26%), drowsiness (24%), dizziness (18%), dry-skin/itching (15%), and vomiting (15%). Side effects can be minimized by slowly increasing the dose of the drug and by using anti-nausea drugs and bowel stimulants. 3. Your doctor will ask you questions and discuss any concerns with you about your possibility of developing addiction. Addiction means that a person uses the drug to get high, and cannot control the urge to take the drug. Most patients do not get high from taking opioids, and addiction is unlikely if your risk for addiction is low: those at greatest risk have a history of addiction with alcohol or other drugs. 4. Opioids can help but they do have risks these can be managed by working cooperatively with your doctor. Take the medication as your doctor prescribed it. Don t drive while your dose is being gradually increased or if the medication is making you sleepy or feel confused. Only one doctor should be prescribing opioid medication for you don t obtain this medication from 29
31 Opioid Treatment Agreement 30
32 Step 3: Initiating Opioids for Chronic Pain After other multimodal therapies have been tried without adequate improvement in pain and function. No contraindications. Trial starts at the lowest effective dose Preferably not to exceed 50 mg morphine equivalents per day. In selected cases in which a higher dose is required for effective pain management and the person with chronic pain has discussed the increased risk of overdose and death with their health care professional, the dose may be titrated up to 90 mg morphine equivalents per day. 31
33 Calculating Morphine MEQ 32
34 Step 3: Evaluate 33
35 Other Important Standards Co-prescribing Opioids and Benzodiazepines People with chronic pain are not prescribed opioids and benzodiazepines at the same time. Opioid Use Disorder People prescribed opioids for chronic pain who are subsequently diagnosed with opioid use disorder have access to opioid agonist therapy. 34

36 Prescription Monitoring Systems Health care professionals who prescribe or dispense opioids have access to a real-time prescription monitoring system at the point of care. Clinical Connect DHDR, Narcotic Monitoring System Contact cswo@sw.ccac-ont.ca for more information 35
37 Tapering and Discontinuation People with chronic pain on long-term opioid therapy, especially those taking 90 mg morphine equivalents or more per day, are periodically offered a trial of tapering to a lower dose or tapering to discontinuation. 36
38 Opioid Tapering Guides 37

39 Opioid Tapering - EMR 38
40 Health Care Professional Education Health care professionals have the knowledge and skills to appropriately assess and treat chronic pain using a multidisciplinary, multimodal approach; appropriately prescribe, monitor, taper, and discontinue opioids; and recognize and treat opioid use disorder. 39
41 Health Care Professional Education Medical Mentoring for Addiction and Pain (OCFP) Safer Opioid Prescribing (U of T) OntarioMD Peer Leaders Partnering for Quality (P4Q) 40
42 Health Care Professional Education Centre for Effective Practice Academic Detailing mic-detailing-service/ LHIN 1: (Erie -St. Clair) Laura Dunn LHIN 2: (South West) Nicole Seymore LHIN 3: pending 41
43 Questions 42
44 Thank you!
Increase in Opioid Related Deaths What the Data Can Tell us. Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes
 Increase in Opioid Related Deaths What the Data Can Tell us Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes Objectives Prescription Opioid Misuse and Abuse: How did we get here? Opioid
Increase in Opioid Related Deaths What the Data Can Tell us Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes Objectives Prescription Opioid Misuse and Abuse: How did we get here? Opioid
Partnered Efforts in Safe Opioid Prescribing
 Partnered Efforts in Safe Opioid Prescribing On the Road with OntarioMD March 7, 2018 Dr. Kevin Samson 2 Partnered Efforts in Safe Opioid Prescribing On the Road with OntarioMD March 7, 2018 Dr. Kevin
Partnered Efforts in Safe Opioid Prescribing On the Road with OntarioMD March 7, 2018 Dr. Kevin Samson 2 Partnered Efforts in Safe Opioid Prescribing On the Road with OntarioMD March 7, 2018 Dr. Kevin
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Opioid Prescribing for Acute Pain. Care for People 15 Years of Age and Older
 Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Opioids and Chronic Pain: Case studies and Personal Experience
 Opioids and Chronic Pain: Case studies and Personal Experience Dr Rupa Patel, MD, CCFP, FCFP Assistant Professor, Department of Family Medicine, Queen s University Kingston Community Health Center Faculty/Presenter
Opioids and Chronic Pain: Case studies and Personal Experience Dr Rupa Patel, MD, CCFP, FCFP Assistant Professor, Department of Family Medicine, Queen s University Kingston Community Health Center Faculty/Presenter
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
2017 Opioid Guideline Update
 2017 Opioid Guideline Update The 2017 Canadian Guideline for Opioid Therapy and Chronic Non-Cancer Pain (CNCP) Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine,
2017 Opioid Guideline Update The 2017 Canadian Guideline for Opioid Therapy and Chronic Non-Cancer Pain (CNCP) Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine,
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Management of Chronic Non Cancer Pain Tool Instruction Manual for Practice Solutions Electronic Medical Record Intended Tool Use
 Management of Chronic Non Cancer Pain Tool Instruction Manual for Practice Solutions Electronic Medical Record Intended Tool Use Clinical best practices and recommendations that follow the Centre for Effective
Management of Chronic Non Cancer Pain Tool Instruction Manual for Practice Solutions Electronic Medical Record Intended Tool Use Clinical best practices and recommendations that follow the Centre for Effective
Narcotics Monitoring System (NMS) Update
 Update") Narcotics Monitoring System (NMS) Update DISCLOSURE OF COMMERCIAL SUPPORT This program has received no financial or in-kind support. Potential for conflict(s) of interest: None Faculty/Presenter Disclosure
Narcotics Monitoring System (NMS) Update DISCLOSURE OF COMMERCIAL SUPPORT This program has received no financial or in-kind support. Potential for conflict(s) of interest: None Faculty/Presenter Disclosure
Learn how MORPHABOND ER can help manage your pain
 Your healthcare provider has prescribed Learn how can help manage your pain What is? MORPHABOND ER (morphine sulfate) extended-release tablets, CII is a strong prescription pain medicine that contains
Your healthcare provider has prescribed Learn how can help manage your pain What is? MORPHABOND ER (morphine sulfate) extended-release tablets, CII is a strong prescription pain medicine that contains
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Community Opioid Load: Concept to Action in Kingston-KFLA
 Community Opioid Load: Concept to Action in Kingston-KFLA Dr Kieran Moore CCFP (EM ) FCFP FRCPC MPH MSc (DM ) Professor of Emergency and Family Medicine Associate Medical Officer of Health, KFLA, Program
Community Opioid Load: Concept to Action in Kingston-KFLA Dr Kieran Moore CCFP (EM ) FCFP FRCPC MPH MSc (DM ) Professor of Emergency and Family Medicine Associate Medical Officer of Health, KFLA, Program
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of Toronto
 Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Team Based Approaches to Chronic Pain Management: Opioid Stewardship Jennifer Wyman, MD, Academic Lead, Opioids Clinical Primer Assistant Professor, Dept. of Family & Community Medicine, University of
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
MOA: Practice Managers Program. Presented by: Kimber Debelak, CMC, CMOM, CMIS. May 17, zpain Management. & New Opioid Laws
 MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Improving emergency department management of acute opioid withdrawal
 Improving emergency department management of acute opioid withdrawal Michelle Klaiman, MD, FRCPPC, DABAM St. Michael s Hospital, University of Toronto Faculty/Presenter Disclosure Faculty: Michelle Klaiman
Improving emergency department management of acute opioid withdrawal Michelle Klaiman, MD, FRCPPC, DABAM St. Michael s Hospital, University of Toronto Faculty/Presenter Disclosure Faculty: Michelle Klaiman
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
NHS Greater Glasgow And Clyde Pain Management Service. Information for Adult Patients who are Prescribed. Pregabalin. For the Treatment of Pain
 NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Pregabalin For the Treatment of Pain This information is not intended to replace your doctor s advice.
NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Pregabalin For the Treatment of Pain This information is not intended to replace your doctor s advice.
Treating pain without pills
 Treating pain without pills Treating pain without pills HealthPartners pain management program Nearly one-third of Americans experience pain. Pain medication is the most commonly prescribed class of drugs
Treating pain without pills Treating pain without pills HealthPartners pain management program Nearly one-third of Americans experience pain. Pain medication is the most commonly prescribed class of drugs
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
The STOP Measure. Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018
 The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Changing the Tide. An EMR facilitated process supporting safe and effective prescribing and de-prescribing of controlled drugs
 Changing the Tide An EMR facilitated process supporting safe and effective prescribing and de-prescribing of controlled drugs Ken Hahlweg MD, CCFP, FCFP Assistant Professor Department of Family Medicine
Changing the Tide An EMR facilitated process supporting safe and effective prescribing and de-prescribing of controlled drugs Ken Hahlweg MD, CCFP, FCFP Assistant Professor Department of Family Medicine
6/6/2017. Faculty/Presenter Disclosure. Disclosure of Commercial Support
 Opioids in Ontario, Canada: The need to reduce the prescribed opioid load; and need for mass casualty preparation Kieran Moore, Professor of Emergency Medicine, Queen s University, Associate Medical Officer
Opioids in Ontario, Canada: The need to reduce the prescribed opioid load; and need for mass casualty preparation Kieran Moore, Professor of Emergency Medicine, Queen s University, Associate Medical Officer
Drug Overdoses A Public Health Problem. Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013. Objectives
 Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID Punta Cana 2018
 MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID USE @joelbordman Punta Cana 2018 Copyright 2017 by Sea Courses Inc All rights reserved. No part of this document may be reproduced, copied, stored, or
MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID USE @joelbordman Punta Cana 2018 Copyright 2017 by Sea Courses Inc All rights reserved. No part of this document may be reproduced, copied, stored, or
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Opioid Prescribing for Acute Pain
 Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Readopt with amendment Med 502, effective (Document #11090), to read as follows:
, to read as follows:") Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT MARK DUNCAN MD UNIVERSITY OF WASHINGTON SPEAKER DISCLOSURES Any conflicts
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences THE UNSTABLE BUPRENORPHINE- NALOXONE PATIENT MARK DUNCAN MD UNIVERSITY OF WASHINGTON SPEAKER DISCLOSURES Any conflicts
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Controlled Substances: A survey of tools and resources required by hospital pharmacists
 Controlled Substances: A survey of tools and resources required by hospital pharmacists TABLE OF CONTENTS 2018. Canadian Society of Hospital Pharmacists About the survey 1 The Short and Snappy 1 What CSHP
Controlled Substances: A survey of tools and resources required by hospital pharmacists TABLE OF CONTENTS 2018. Canadian Society of Hospital Pharmacists About the survey 1 The Short and Snappy 1 What CSHP
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Models of good practice in drug treatment in Europe. Project group
 Models of good practice in drug treatment in Europe ( moretreat 2006329 ) Project group Hamburg, London, Rome, Stockholm, Vienna, Warsaw, Zurich Project duration: 17 months from April 2006 August 2008
Models of good practice in drug treatment in Europe ( moretreat 2006329 ) Project group Hamburg, London, Rome, Stockholm, Vienna, Warsaw, Zurich Project duration: 17 months from April 2006 August 2008
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
Prescription Review Program and College Expectations
 Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial
Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
Post-Stroke Mood & Anxiety Disorder Clinic
 Post-Stroke Mood & Anxiety Disorder Clinic A Collaboration Between The Stroke Program Edmonton Zone, RAH Stroke Prevention Clinic & Psychiatry Shy Amlani, Program Manager, Stroke Program Edmonton Zone
Post-Stroke Mood & Anxiety Disorder Clinic A Collaboration Between The Stroke Program Edmonton Zone, RAH Stroke Prevention Clinic & Psychiatry Shy Amlani, Program Manager, Stroke Program Edmonton Zone
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Slow Release Opioids. Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain
 Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain") NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
The Challenging Patient with Chronic Opioid Usage MD ACP Meeting
 The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
Clinical and Contextual Evidence Reviews
 Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Mindful Prescribing for Acute Pain
 Mindful Prescribing for Acute Pain London Hospitals as a Leader in Changing Opioid Prescribing Dr. Brian Rotenberg, MD MPH FRCSC MAC Vice Chair, St. Joseph s What about new starts? Source: Health Quality
Mindful Prescribing for Acute Pain London Hospitals as a Leader in Changing Opioid Prescribing Dr. Brian Rotenberg, MD MPH FRCSC MAC Vice Chair, St. Joseph s What about new starts? Source: Health Quality
Teaming Up for Safer Pain Management: Strategies for Effective Collaboration
 Teaming Up for Safer Pain Management: Strategies for Effective Collaboration Noah Nesin, MD, FAAFP, Vice President of Medical Affairs, Penobscot Community Health Care Felicity Homsted, PharmD, DPLA, Chief
Teaming Up for Safer Pain Management: Strategies for Effective Collaboration Noah Nesin, MD, FAAFP, Vice President of Medical Affairs, Penobscot Community Health Care Felicity Homsted, PharmD, DPLA, Chief
OLDER ADULTS & DEPRESCRIBING: TREATMENT
 OLDER ADULTS & DEPRESCRIBING: CONTEMPLATION, ASSESSMENT & TREATMENT Jonathan Bertram Faculty/Presenter Disclosure Faculty: Jonathan Bertram Relationships with commercial interests: Grants/Research Support:
OLDER ADULTS & DEPRESCRIBING: CONTEMPLATION, ASSESSMENT & TREATMENT Jonathan Bertram Faculty/Presenter Disclosure Faculty: Jonathan Bertram Relationships with commercial interests: Grants/Research Support:
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Management in the Primary Care Setting
 Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Opioids in the Management of Chronic Pain: An Overview
 Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT
 Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
SUBSTANCE ABUSE IN THE ELDERLY. The Invisible Epidemic
 SUBSTANCE ABUSE IN THE ELDERLY The Invisible Epidemic IS IT POSSIBLE TO TEACH AN OLD DOG NEW TRICKS? GUIDELINES All forms of addiction know no age limit. Don t blame all problems on aging. Few realize
SUBSTANCE ABUSE IN THE ELDERLY The Invisible Epidemic IS IT POSSIBLE TO TEACH AN OLD DOG NEW TRICKS? GUIDELINES All forms of addiction know no age limit. Don t blame all problems on aging. Few realize
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Trigger. Myths About the Use of Medication in Recovery BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
Dr Alistair Dunn. General Practitioner Northland District Health Board Whangarei
 Dr Alistair Dunn General Practitioner Northland District Health Board Whangarei Oxycodone Dr Alistair Dunn Addiction Medicine Specialist General Practitioner Whangarei, Northland. Oxycodone Dr Alistair
Dr Alistair Dunn General Practitioner Northland District Health Board Whangarei Oxycodone Dr Alistair Dunn Addiction Medicine Specialist General Practitioner Whangarei, Northland. Oxycodone Dr Alistair
OPIOID PAIN MEDICATION Agreement and Informed Consent
 OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
Less pain in my life helps me get back to living.
 Eligible patients pay as little as $0 for BELBUCA Less pain in my life helps me get back to living. BELBUCA is: RETHINK RELIEF A strong prescription pain medicine that contains an opioid (narcotic) that
Eligible patients pay as little as $0 for BELBUCA Less pain in my life helps me get back to living. BELBUCA is: RETHINK RELIEF A strong prescription pain medicine that contains an opioid (narcotic) that
Doctor Discussion Guide
 Doctor Discussion Guide Getting the pain relief you need to stay active is important. Keeping track of your symptoms can help you and your healthcare provider determine if there is a need to adjust your
Doctor Discussion Guide Getting the pain relief you need to stay active is important. Keeping track of your symptoms can help you and your healthcare provider determine if there is a need to adjust your
Pharmaceutical Misuse and its Challenges: Opioid Use in Ontario. Ontario Harm Reduction Conference Tara Gomes Tuesday January 31, 2012
 Pharmaceutical Misuse and its Challenges: Opioid Use in Ontario Ontario Harm Reduction Conference Tara Gomes Tuesday January 31, 2012 Objectives To review the prescription opioid crisis To understand the
Pharmaceutical Misuse and its Challenges: Opioid Use in Ontario Ontario Harm Reduction Conference Tara Gomes Tuesday January 31, 2012 Objectives To review the prescription opioid crisis To understand the
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
PROVIDER BULLETIN. Published by Wyoming Workers Compensation Medical Case Management Unit October 21, 2015
 Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Matthew H. Mead Governor State of Wyoming Department of Workforce Services DIVISION OF WORKERS COMPENSATION 1510 East Pershing Boulevard, South Wing Cheyenne, Wyoming 82002 http://www.wyomingworkforce.org
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Medication Guide. Medication Guide. Lazanda (La-ZAN-da) CII. (fentanyl) nasal spray 100 mcg, 400 mcg
 CII. (fentanyl) nasal spray 100 mcg, 400 mcg") Medication Guide Medication Guide Lazanda (La-ZAN-da) CII (fentanyl) nasal spray 100 mcg, 400 mcg IMPORTANT: Do not use Lazanda unless you are regularly using another opioid pain medicine around-the-clock
Medication Guide Medication Guide Lazanda (La-ZAN-da) CII (fentanyl) nasal spray 100 mcg, 400 mcg IMPORTANT: Do not use Lazanda unless you are regularly using another opioid pain medicine around-the-clock
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioids for persistent pain: Information for patients. The British Pain Society's
 The British Pain Society's Opioids for persistent pain: Information for patients A statement prepared on behalf of the British Pain Society, the Faculty of Pain Medicine of the Royal College of Anaesthetists,the
The British Pain Society's Opioids for persistent pain: Information for patients A statement prepared on behalf of the British Pain Society, the Faculty of Pain Medicine of the Royal College of Anaesthetists,the
Implementing Pain and Opioid Management Guidelines in Primary Care Practice
 Implementing Pain and Opioid Management Guidelines in Primary Care Practice Objectives 1. What is the issue? 2. Why use a dedicated dissemination & implementation process? a. Historical perspective Cooperative
Implementing Pain and Opioid Management Guidelines in Primary Care Practice Objectives 1. What is the issue? 2. Why use a dedicated dissemination & implementation process? a. Historical perspective Cooperative
MEDICATION MANAGEMENT AGREEMENT Pain Management Program Participation Agreement and Consent
 MEDICATION MANAGEMENT AGREEMENT Pain Management Program Participation Agreement and Consent Pain may be effectively managed through the use of controlled substance medications (referred to below as opioids
MEDICATION MANAGEMENT AGREEMENT Pain Management Program Participation Agreement and Consent Pain may be effectively managed through the use of controlled substance medications (referred to below as opioids
Guide for Patients and Caregivers
 N FENTORA Fentanyl Buccal/Sublingual Effervescent Tablets 100 mcg, 200 mcg, 400 mcg, 600 mcg, and 800 mcg fentanyl as fentanyl citrate Opioid Analgesic Guide for Patients and Caregivers Manufactured for:
N FENTORA Fentanyl Buccal/Sublingual Effervescent Tablets 100 mcg, 200 mcg, 400 mcg, 600 mcg, and 800 mcg fentanyl as fentanyl citrate Opioid Analgesic Guide for Patients and Caregivers Manufactured for: