Review Article Understanding Thoracic Outlet Syndrome
|
|
|
- Stanley Atkins
- 5 years ago
- Views:
Transcription
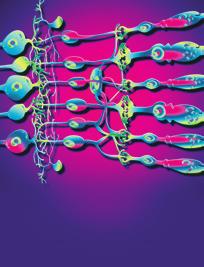
1 Scientifica, Article ID , 6 pages Review Article Understanding Thoracic Outlet Syndrome Julie Freischlag 1 and Kristine Orion 2 1 Division of Vascular Surgery, Department of Surgery, The Johns Hopkins Hospital, 720 Rutland Avenue, Ross 759, Baltimore, MD 21205, USA 2 Division of Vascular Surgery, Department of Surgery, The Johns Hopkins Hospital, 600 N. Wolfe Street, Halsted 668, Baltimore, MD 21287, USA Correspondence should be addressed to Kristine Orion; korion1@jhmi.edu Received 9 March 2014; Accepted 28 June 2014; Published 20 July 2014 AcademicEditor:SamyS.Nitecki Copyright 2014 J. Freischlag and K. Orion. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The diagnosis of thoracic outlet syndrome was once debated in the world of vascular surgery. Today, it is more understood and surprisingly less infrequent than once thought. Thoracic outlet syndrome (TOS) is composed of three types: neurogenic, venous, and arterial. Each type is in distinction to the others when considering patient presentation and diagnosis. Remarkable advances have been made in surgical approach, physical therapy, and rehabilitation of these patients. Dedicated centers of excellence with multidisciplinary teams have been developed and continue to lead the way in future research. 1. Introduction Thoracic outlet syndrome (TOS) is a disease which involves compression of the neurovascular bundle as it exits the thoracic girdle. Twenty years ago, the existence of such a syndrome was poorly understood and therefore its acceptance as a medical diagnosis was controversial [1]. Today, however, the syndrome is better recognized; its symptoms and pathophysiology are more clearly defined. And, as the number of patients undergoing successful treatment increases, TOS is becoming a common diagnosis in vascular surgery clinics around the world. 2. Embryology The thoracic outlet is anatomically defined by the space between the first thoracic vertebra, first rib, and manubrium of the sternum. Anteriorly, the subclavius tendon lies next to the subclavian vein. Next, the scalene separates the subclavian vein from the subclavian artery. The brachial plexus travels posterior and laterally to the artery and is accompanied by the middle scalene muscle (Figure 1). It is a very small space, already occupied by the anterior scalene, the subclavius, and prevertebral muscles. The thoracic outlet is also dynamic; the volume changes with respiration and any activity of the neck, thorax, or arm [2]. Additionally, cervical ribs or anomalous first ribs, which tend to be more cephalad or fused with thesecondrib,canfurtheraffectthedimensionsofthe thoracic outlet [3]. As the space continuously contracts and expands, there may be impingement of the brachial plexus or subclavian vessels by the osseous structures. Simultaneously, fibrosis and scarring may occur, which can then cause encroachment or inflammation. 3. Pathogenesis and Clinical Presentation There are three types of TOS: neurogenic, venous, and arterial. As these structures travel together while exiting the thorax and entering the axilla, it can be understood why any of the three can be affected. What is not so understood is why neurogenic is much more common than either the venous or arterial thoracic outlet syndrome. Neurogenic thoracic outlet syndrome (ntos) makes up approximately 95% of all patients suffering from this syndrome. Patients can present with vague symptomatology butmostoftencomplainofpainandnumbnessintheir fingers, hands, or arms on the affected side. Many of these patients have experienced some type of trauma, typically
. Figure 2: Radiographs show both a fully formed and a partially developed cervical rib (reprinted with permission of Elsevier; see [8]). motor vehicle accidents or falls.")
2 2 Scientifica Brachial plexus Subclavian artery Anterior scalene muscle Subclavian vein Fully formed Partially developed 1st rib Figure 1: Anatomy of the thoracic outlet (reprinted with permission of Elsevier; see [8]). Figure 2: Radiographs show both a fully formed and a partially developed cervical rib (reprinted with permission of Elsevier; see [8]). motor vehicle accidents or falls. Patients seem to additionally describe a history vigorous repetitive activity, likely related to their profession or lifestyle. In our practice, 50% of patients presentwithahistoryofeithertraumaorchronicrepetitive motion. It is suspected that the formation of scar tissue and adhesions may play a likely role in this relationship. Tissue contraction from scar or adhesions can certainly affect the dynamics of the already small thoracic outlet. Furthermore, they may directly impinge on the nerves or vessels. Venous thoracic outlet syndrome (vtos) makes up an additional 3 5% of patients. This group of patients suffers from compression of the axillosubclavian vein which ultimately results in thrombosis. It has been described as effort thrombosis or Paget-Schroetter syndrome [4]. Thrombosis may be acute or chronic, occlusive or partially obstructive. Patients will report acute onset purple-red discoloration of a swollen extremity. It is felt that the vein may most often be inflamed causing scarring and narrowing over time until acute thrombosis. There is usually concurrent dull aching pain especially in the recumbent position as well as a sense of heaviness. As time progresses, patients will notice visibly dilated superficial veins across the shoulder, chest, back, and neck as explained by venous collateral development [5]. vtos is also associated with trauma or repetitive motion. Patients mayhaveahypercoagulablehistory;however,itisrare(5 15%). Occasionally, a medical implant such as central venous catheters, pacemakers, or defibrillator wires may be present and, therefore, those patients do not have compression as their etiology for venous thrombosis, but a foreign body. Finally, arterial thoracic outlet syndrome (atos) is the rarest form accounting for only 1-2%. Continuous friction of the subclavian artery and the underlying first rib from pulsation and activity can cause fibrosis and stenosis of the artery. Poststenotic aneurysms can then form. Both the narrowed artery and aneurysms can cause arterial thrombosis. In the chronic phase, patients experience claudication or pain with activity of the arm/hand which generally subsides with the cessation of movement. In the subacute stage, as emboli form and travel distally, patients present with focal symptoms of ischemia in the form of a severely painful blue or white finger [6]. Acutely, the subclavian artery can completely thrombose, leavingthepatientwithathreatenedlimb.manyofthese patients will have a cervical rib or other rib anomaly such as a rudimentary rib or fused cervical, 1st and/or second ribs (Figure 2). A recent study from Michigan found an astonishing incidence of 29% for bony abnormalities in their TOS patients and the strongest association occurred with arterial TOS [7]. 4. Diagnosis TOS is often a diagnosis of exclusion. Other causes such asherniatedcervicaldisks,rotatorcuffinjuries,peripheral nerve entrapment, chronic pain syndromes, psychological conditions, multiple sclerosis, hypercoagulable disorders, atrial fibrillation with distal emboli, and upper extremity deep venous thrombosis all need to be considered because they can mimic the symptoms of TOS [9]. Venous and arterial TOS are more easily diagnosed with a combination of clinical presentation and imaging. In vtos, a duplex ultrasound is the most dominant noninvasive study. A complete evaluation of both the subclavian and axillary veins is important using both grey-scale imaging and Doppler spectral waveform analysis. Velocities and waveforms are obtained in resting and the abducted position of the arm. Dampening of the waveform or marked decrease in velocities while the arm is abducted can assure the diagnosis of vtos. Patients will frequently have already been diagnosed with some type of venous thrombosis which can also be seen on ultrasound. Using ultrasound for diagnosis of arterial TOS is similar. Arterial pulse waveforms are again reduced; however, velocities will be increased with stenosis or absent in complete occlusion. Most patients should have a plain chest X-ray to evaluateforcervicalribsorotherbonyabnormalities.finally, CTA or traditional angiography can be utilized to identify more clearly the occlusion, aneurysm, or distal embolization. Diagnosing neurogenic TOS is the least clear. It is not uncommonforpatientstohavebeendiagnosedwithseveral other conditions and have failed their treatment plans such as cervical fusion, carpel tunnel release, surgical repair of the rotator cuff, or simply prolonged physical therapy. Intuitively, if the brachial plexus is impinged upon and plexopathy occurs, an MRI should show some type of inflammation of
3 Scientifica 3 the nerve or surrounding soft tissue, but this has not been consistently true. Several maneuvers have been developed which together with a good clinical history may diagnose ntos. The elevated arm stress test (EAST) is a quick assessment in which the patient is asked to abduct the shoulder 90 degrees, flex the elbows at 90 degrees, and face the hands forward while alternately opening and closing their hands at a rate of one per second for 3 minutes. One can actually see decreased ability to open and close their hands or lowering of the arm during the EAST in patients with neurogenic TOS. Patients rate the amount and location of discomfort, pain, fatigue, and numbness. Unfortunately, those with carpal tunnel syndrome, ulnar neuropathy, or fibromyalgia will demonstrate symptoms as well. The Adson maneuver may be performed seated or standing. The patient is requested to take a deep breath and rotate and extend their head as far as possible towards the unaffected side. The affected side arm is abducted with the elbow flexed, and the examiner s fingers should be placed on the radial pulse. The test will reproduce symptoms or obliterate the ipsilateral radial pulse. One can also listen for a bruit underneath the clavicle during the Adson s test to document compression. Another positive finding suggestive of ntos is tenderness to palpation at the scalene triangle or the insertion of the pectoralis minor. A more objective examination is the lidocaine scalene block test. Under image guidance, either computed tomography, ultrasound, or fluoroscopy, the anterior scalene muscle is injected with lidocaine. Patients with ntos should have some decrease or complete relief of symptoms for four hours. In our practice, an initial lidocaine block is utilized and, if positive, predicts 90% success for subsequent treatments including physical therapy and surgical intervention. Interestingly, our review of 159 patients showed that younger patients (<40 years) are more likely to achieve symptom relief overall after transaxillary decompression; however, successful lidocaine blocks better predicted increased surgical success in patients >40 years old [10]. Additionally, botulinum toxin A (Botox) can be used for temporary symptom respite. We frequently perform this injection at a second setting. Botox takes two weeks to work but can last three months and can help patients progress with physical therapy. This technique has been examined nationally, including a study from Boston which concluded that botulinum toxin injection with ultrasound guidance is safe and well tolerated in subjects with suspected ntos for interim relief [11]. In our institution, we begin our diagnosis algorithm with a good history and physical as well as vascular lab studies if arterial or venous outlet syndrome is suspected. If our vascularlabduplexisconsistentwithvtosoratos,we will schedule the patient for surgery (see next paragraph). We do not routinely utilize venous lysis preoperatively, nor do we employ CT venogram until the postoperative time period. It is useful to perform CTA in atos, especially when arterial reconstruction is considered. In neurogenic TOS, most patients will already come with chest X-rays and cervical spine MRIs. We usually do not require any more imaging. We perform several clinical maneuvers as previously mentioned, and if we suspect ntos, we refer the patient to rehab. Many of our patients will resolve with physical therapy. Of those still symptomatic and compliant to the physical therapy regimen, may then be scheduled for a lidocaine scalene block test. If the block provides a decrease or relief of symptoms, we will evaluate the patient s overall fitness for surgery. 5. Treatment Surgical intervention, specifically first rib resection and anterior scalenectomy (FRRS), is indicated for both venous andarterialtos.sequelaeofbothtypesareboundtorecur without a definitive operation. Traditionally, anticoagulation and arm elevation was the treatment for vtos. In more recent years, lysis with or without venoplasty has been offered for patients with vtos. They were then referred to vascular or thoracic surgeons for a first rib resection three months later. However, we know now that preoperative thrombolysis and venoplasty impart no benefit over routine anticoagulation in regard to vein patency or symptom resolution for these patients. In fact, many will rethrombose in the 3-month interval, awaiting surgery [12]. We recommend FRRS (described in the following section) once the patient has been diagnosed with vtos. Patients will be at various stages in treatment, some having undergone lysis or plasty and some not having. Anticoagulation is then resumed three days after surgery. If the patient has undergone thrombolytic therapy, we try to schedule them as soon as possible. Invasive venography is performed two weeks postoperatively to identify subclavian vein pathology that may require further venoplasty. Those patients who have lesion-free patent subclavian veins are told to stop anticoagulation. Those undergoing additional endovascular treatment are continued on anticoagulation for 1-2 months until followup. If duplex ultrasound demonstrates vein patency at that time, anticoagulation is stopped. If thrombosis persists, anticoagulation is generally continued foramaximumof6months.theneedforlong-termanticoagulation may vary if the affected patient has an additional underlying hypercoagulable condition. Uniformly,allpatientswitharterialthoracicoutletsyndrome will need full anticoagulation and varying degrees of surgical intervention. atos is the rarest form of this disease and can be quite unique to each patient in regard to symptoms, acuity of presentation, and aneurysmal degeneration. If an aneurysm is present, the patient may require an arterial reconstruction in addition to FRRS. This may alter one from a transaxillary approach to a supraclavicular technique. Arterial reconstruction with an interposition bypass may be achieved using saphenous vein or synthetic grafts. Treatment for neurogenic TOS, although less clear in the past, is more certain today. Clinicians agree that the initial management is nonoperative. Approximately 60 70% of patients with ntos can be successfully treated with avoidance of activities that precipitate symptoms, ergonomic modifications to the workplace, and selective use of pharmacologic agents such as nonsteroidal anti-inflammatories, antidepressants, and muscle relaxants. Physical therapy is also a very important component for these patients. Conservative
![4 Scientifica Figure 4: Use of the periosteal elevator to remove tissue from the first rib (reprinted with permission of Elsevier; see [8]).](/docs-images/82/85064900/images/4-0.jpg "Figure 3: Machleder retractor with incision marked just below axillary hair line. management should be attempted for 8 12 weeks before considering surgery.")
 FRRS has been performed via a supraclavicular incision; however, we favor the exposure of a transaxillary approach")

4 4 Scientifica Figure 4: Use of the periosteal elevator to remove tissue from the first rib (reprinted with permission of Elsevier; see [8]). Figure 3: Machleder retractor with incision marked just below axillary hair line. management should be attempted for 8 12 weeks before considering surgery. Those that fail should undergo a lidocaine scalenemuscleinjection.iftheyrespondtothisblock,they maybeevaluatedtoseeiftheyarephysicallyfitforfrrs. 6. First Rib Resection and Scalenectomy (FRRS) FRRS has been performed via a supraclavicular incision; however, we favor the exposure of a transaxillary approach andusethistechniqueforallourpatientsregardlessofsize. FRRS is performed under general anesthesia with avoidance of any long-acting paralytics for intraoperative nerve identification and monitoring. Positioning and retraction are the most important aspects of obtaining an adequate surgical field of view [13].Thepatientisplacedonabeanbaginthe lateral position with the operative side up. Ample padding withfoamorpillowsshouldbeusedinordertoprotect pressure points as the bean bag is inflated. The axilla and arm are prepped circumferentially to the wrist and a Machleder retractor is utilized. This retractor allows excellent exposure of the thoracic outlet without the laborious need for an assistant to extend the arm throughout the surgery. The borders of the latissimus dorsi muscle and pectoralis major muscle are marked, and the incision is made between the two just below the axillary hair line (Figure 3). Dissection is taken down directly to the chest wall in order to avoid disturbing the axillary lymphatic bed. Gentle blunt dissection is then performed towards the apex of the axilla and first rib. Lighted hand-held retractors are used to provide illumination deep into the operative field. The anatomy is identified; the vein will be fluttering with respiration; the artery will be pulsatile (in vtos, the vein can be fibrotic and more difficult to detect). The first rib is identified as the scalene muscle will insert on its most cephalad edge. Sharp periosteal elevators are used to Figure 5: Transection of the anterior scalene muscle with a right angle clamp and scissors (reprinted with permission of Elsevier; see [8]). clear intercostals and mobilize the first rib (Figure 4). Inferiorly, the pleura is gently peeled off the rib, but pneumothorax can be encountered in patients with significant scarring. Next, the subclavius muscle is divided sharply, which is followed by high division of the anterior scalene muscle (Figure 5). Great care must be taken to avoid injury to the artery during this step. Once the rib is completely mobilized, a rib cutter is used anteriorly first, next to the subclavian vein. Finally, the rib is then transected posteriorly at the level of or just anterior to the brachial plexus. Frequently a second transection is performed just behind the brachial plexus to assure that no scarring will occur between the nerves and the rib in the postoperative period causing recurrent symptoms 20% of the time. The rib is removed (Figure 6)andthespaceisinspected for hemostasis. If a pneumothorax has occurred, a small 12- French chest tube is placed prior to closing the incision in two or three layers. Postoperatively, the patient is kept overnight for observation after a plain chest radiograph is performed in the recovery area. Pain is controlled with a PCA and muscle relaxers. The patient is provided with a sling for comfort and is allowed immediate ambulation. Chest tubes are removed

5 Scientifica 5 Figure 6: First rib removed. in the morning, and 95% of patients are discharged home the following day. All patients receive physical therapy starting 2 weeks after the surgery. Physical therapy is a specific 8-week regimen that focuses on postural training as well as strength training in the shoulder, chest, and neck. During weeks 1 3, therapists work on mobilizing the thoracic and cervical spine using thoracic extension and cervical flexion. This also begins to tease the patient s stretch and pain sensations. Patients concentrate on diaphragmatic breathing and perform gentle scapular posterior depression exercises. Finally, they start posture training. In Weeks 4 6, patients add mild resistance training to improve scapular stability and mobility of the glenohumeral joint and rotator cuff. The most common complication for FRRS is pneumothorax and occurs up to 10% of the time. Bleeding and need for reoperation are rare but we still avoid using strong nonsteroidals such as Toradol in the immediate postoperative setting. Infection is also uncommon despite the proximity of the incision to the axillary hair line and apocrine sweat glands. We utilize skin glue on the incision which aids in preventing contamination with sweat. Injuries to the brachial plexus or long thoracic nerves occur in <1% of cases. 7. Outcomes after FRRS Neurogenic TOS is the most investigated form of TOS. Because surgical treatment focuses on alleviation of pain and numbness, outcomes must be analyzed using subjective means. Several forms can be utilized: Short-Form 12 (SF- 12), Brief Pain Inventory (BPI), and Cervical Brachial Symptom Questionnaire (CBSQ). Previous studies have shown improvement in quality of life with short-term followup (2 years after FRRS) but then a decline at three years. A more recent report including 87 ntos patients demonstrated no difference in quality of life between short-term followup and a prolonged followup of 44 months. Overall, 90% of patients will have relief of their symptoms after FRRS [14]. Therefore, symptom recurrence or surgical failure happens 10% of the time. As already mentioned, a positive lidocaine scalene block is a clinical indicator that a patient will have a successful response to surgical intervention but this is not a guarantee. In our analysis of 182 patients at the Johns Hopkins Hospital [15] having undergone FRRS, older age (>40) was significantly predictive of a poor outcome. Longer duration of symptoms and active smoking were more associated with unresolved symptoms. Finally, those patients with comorbid chronic pain syndromes are more likely to have persistent pain postoperatively. What is interesting is that, in contrast to unresolved symptoms, patients with recurrent symptoms are well managed with physical therapy. Additionally, Botox injections can be helpful with recurrent symptoms to relax the painful muscles in the shoulder and back areas. All surgical failures or recurrences for ntos should also be reevaluated in clinic for contralateral symptoms. Bilateral ntos can occur frequently in patients with cervical ribs. A second FRRS after 1 year may improve their results. We wait a year to ensure adequate recuperation from the first operation. In2008,welookedattherateofreturntoworkforour TOS patients. Although 34% of neurogenic and 8% of venous patients were disabled or unemployed upon presentation, astounding 50% of neurogenic and 77% of venous patients eventually returned to activity or full-time work over a 12- month followup [16]. 8. Recent Developments in TOS As more and more patients are treated for TOS, the referral pattern has begun to change. Typically, patients were evaluated and treated by several other disciplines before being considered for TOS. Now, patients are being referred earlier with a shorter duration of symptoms, which improves theirchanceofasuccessfulsurgicaltreatment.ariseof presentation in adolescents has also been observed. Case reports have emphasized that these younger patients have more prevalent unusual anatomy such as cervical ribs or abnormal tendon insertions. Many adolescents will describe repetitive and vigorous activity such as competitive sports or instrumental performance. Noteworthy, adolescents also seem to present more frequently with venous or arterial TOS than adults [17]. FRRS has been safely and successfully performed in this population with a rapid return to their busy lives. Modern experience indicates that a multidisciplinary comprehensive approach to TOS improves outcomes. Centers of TOS excellence have been established throughout the country which provide a well-organized and uniformed process for these patients [18]. Dedicated nurses, physician assistants, physical therapists, medical physicians, surgeons, neurologists, and pain management anesthesiologists who understand TOS can efficiently diagnose patients, create focused management algorithms, and deliver specialized postoperative attention. 9. Future Research Although TOS has come a long way in the last half century, there are many avenues left to explore. Diagnosis still remains the most debated aspect of neurogenic TOS. Despite multiple maneuvers and even the lidocaine scalene block, the test results rely on patient symptomatology alone. Continued
6 6 Scientifica research would be beneficial to find a more objective analysis. Some have suggested using MRI or CTAs preoperatively to compare TOS patients with control patients to further assist in diagnosis. Secondly, in the case of atos, it is unclear if prosthetic or autologous tissue is better for reconstruction. Patency rates and need for reoperations are important aspects as in any vascular reconstruction. As arterial TOS is the rarest form, a study to resolve this issue would require multiple centers. Finally, we have adopted the protocol of performing venography two weeks after first rib resection and scalenectomy. There may still be some amount of postoperative inflammation at this interval, so the timing of these venograms should be investigated. 10. Conclusion Today, we can begin to understand thoracic outlet syndrome. The embryology and pathophysiology make sense. We appreciatethattherearethreetypesofthoracicoutletsyndrome. Each type has a different patient presentation; yet all three can be successfully treated with FRRS. The controversy of whether thoracic outlet syndrome exists is slowly being put to rest. Conflict of Interests The authors declare that there is no conflict of interests regarding the publication of this paper. References [1] H. Machleder, A brief history of the thoracic outlet compression syndromes, in Thoracic Outlet Syndrome, K. A. Illig, R. W. Thompson,J.A.Freischlag,D.M.Donahue,S.E.Jordan,andP. I. Edgelow, Eds., pp. 3 9, Springer, New York, NY, USA, [2] R.S.TubbsandM.M.Shoja, Embryologyofthethoracicoutlet, in Thoracic Outlet Syndrome, K. A. Illig, R. W. Thompson, J.A.Freischlag,D.M.Donahue,S.E.Jordan,andP.I.Edgelow, Eds., Springer, New York, NY, USA, [3]R.J.Sanders, AnatomyandpathophysiologyofATOS, in Thoracic Outlet Syndrome, K.A.Illig,R.W.Thomson,J.A. Freischlag,D.M.Donahue,S.E.Jordan,andP.I.Edgelow,Eds., Springer, [4] R. L. Feinberg, Clinical presentation and patient evaluation in VTOS, in Thoracic Outlet Syndrome, K. A. Illig, R. W. Thompson, J. A. Freischlag, D. M. Donahue, S. E. Jordan, and P. I. Edgelow, Eds., pp , Springer, London, UK, [5] A.J.DoyleandD.L.Gillespie, VTOSfortheprimarycareteam: when to consider the diagnosis, in Thoracic Outlet Syndrome,K. A. Illig, R. W. Thompson, J. A. Freischlag, D. M. Donahue, S. E. Jordan, and P. I. Edgelow, Eds., Springer, [6] A. Azizzadeh and R. W. Thompson, Clinical presentation and patient evaluation in ATOS, in Thoracic Outlet Syndrome, pp , Springer, London, UK, [7] A. E. Weber and E. Criado, Relevance of bone anomalies in patients with thoracic outlet syndrome, Annals of Vascular Surgery,vol.28,no.4,pp ,2014. [8] W.BrandonandJ.A.Freischlag, Thoracicoutletsyndromes, in Current Surgical Therapy,J.L.CameronandA.M.Cameron, Eds., Elsevier, New York, NY, USA, 11th edition, [9] B.S.BrookeandJ.A.Freischlag, Contemporarymanagement of thoracic outlet syndrome, Current Opinion in Cardiology, vol.25,no.6,pp ,2010. [10] Y. W. Lum, B. S. Brooke, K. Likes et al., Impact of anterior scalene lidocaine blocks on predicting surgical success in older patients with neurogenic thoracic outlet syndrome, Vascular Surgery,vol.55,no.5,pp ,2012. [11] M. Torriani, R. Gupta, and D. M. Donahue, Botulinum toxin injection in neurogenic thoracic outlet syndrome: results and experience using a ultrasound-guided approach, Skeletal Radiology,vol.39,no.10,pp ,2010. [12] J. L. Guzzo, K. Chang, J. Demos, J. H. Black, and J. A. Freischlag, Preoperative thrombolysis and venoplasty affords no benefit in patency following first rib resection and scalenectomy for subacute and chronic subclavian vein thrombosis, Vascular Surgery,vol.52,no.3,pp ,2010. [13] N.O.GlebovaandJ.A.Freischlag, Thoracicoutletsyndrome: transaxillary approach, in Master Techniques in Surgery: Thoracic Surgery, D. Mathisen and C. Morse, Eds., Lippincott Williams & Wilkins, Philadelphia, Pa, USA, [14] D. H. Rochlin, M. M. Gilson, K. C. Likes et al., Qualityof-life scores in neurogenic thoracic outlet syndrome patients undergoing first rib resection and scalenectomy, Vascular Surgery,vol.57,no.2,pp ,2013. [15] D. H. Rochlin, K. C. Likes, M. M. Gilson, P. J. Christo, and J. A. Freischlag, Management of unresolved, recurrent, and/or contralateral neurogenic symptoms in patients following first ribresectionandscalenectomy, Vascular Surgery,vol. 56, no. 4, pp , [16] D. C. Chang, L. A. Rotellini-Coltvet, D. Mukherjee, R. de Leon, and J. A. Freischlag, Surgical intervention for thoracic outlet syndrome improves patient s quality of life, JournalofVascular Surgery,vol.49,no.3,pp ,Mar2009. [17]K.Chang,E.Graf,K.Davis,J.Demos,T.Roethle,andJ.A. Freischlag, Spectrum of thoracic outlet syndrome presentation in adolescents, Archives of Surgery, vol. 146, no. 12, pp , [18] V. B. Emery and R. W. Thompson, Pathways of care and treatment options for patients with NTOS, in Thoracic Outlet Syndrome, K.A.Illig,R.W.Thompson,J.A.Freischlag,D.M. Donahue, S. E. Jordan, and P. I. Edgelow, Eds., pp , Springer, London, UK, 2013.
















7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Compression of neural or vascular structures within the
 Thoracic Outlet Syndrome: Transaxillary Approach Margaret Clarke Tracci, MD, JD Compression of neural or vascular structures within the constrained space of the thoracic outlet may give rise to 3 separate
Thoracic Outlet Syndrome: Transaxillary Approach Margaret Clarke Tracci, MD, JD Compression of neural or vascular structures within the constrained space of the thoracic outlet may give rise to 3 separate
4/3/2014. Disclosures. Venous Thoracic Outlet Syndrome: Our Approach and Results. Paget Schroetter Syndrome. Paget Schroetter Syndrome.
 Disclosures No relevant financial relationships with commercial interests Venous Thoracic Outlet Syndrome: Our Approach and Julie A. Freischlag, M.D. Vice Chancellor for Human Health Sciences Dean of the
Disclosures No relevant financial relationships with commercial interests Venous Thoracic Outlet Syndrome: Our Approach and Julie A. Freischlag, M.D. Vice Chancellor for Human Health Sciences Dean of the
Thoracic Outlet Syndrome
 Thoracic Outlet Syndrome Cristina Sola, BSN, RN-BC Nurse Manager Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science Center at Houston Memorial Hermann
Thoracic Outlet Syndrome Cristina Sola, BSN, RN-BC Nurse Manager Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science Center at Houston Memorial Hermann
THORACIC OUTLET SYNDROME (T.O.S.) Prof J van Marle
 Prof J van Marle") THORACIC OUTLET SYNDROME (T.O.S.) Prof J van Marle 1. Definition Clinical syndrome caused by compression of the neurovascular bundle as it passes through the thoracic outlet, a narrow space bordered by
THORACIC OUTLET SYNDROME (T.O.S.) Prof J van Marle 1. Definition Clinical syndrome caused by compression of the neurovascular bundle as it passes through the thoracic outlet, a narrow space bordered by
Thoracic Outlet Syndrome
 Disclosures None relevant to this discussion The Management of Thoracic Outlet Syndrome: Acute Charles Eichler MD Professor, Department of Surgery Division of Vascular and Endovascular Surgery University
Disclosures None relevant to this discussion The Management of Thoracic Outlet Syndrome: Acute Charles Eichler MD Professor, Department of Surgery Division of Vascular and Endovascular Surgery University
Richard Dobrusin DO FACOFP
 Richard Dobrusin DO FACOFP Define Thoracic Outlet Syndrome (TOS) Describe the Mechanisms of Dysfunction List Diagnostic tests for (TOS) Understand (TOS) referral patterns Discuss Treatment Options Definition:
Richard Dobrusin DO FACOFP Define Thoracic Outlet Syndrome (TOS) Describe the Mechanisms of Dysfunction List Diagnostic tests for (TOS) Understand (TOS) referral patterns Discuss Treatment Options Definition:
Pseudothrombosis of the Subclavian Vein
 416507JDMXXX10.1177/8756479311416507Wash ko et al.journal of Diagnostic Medical Sonography Pseudothrombosis of the Subclavian Vein Journal of Diagnostic Medical Sonography 27(5) 231 235 The Author(s) 2011
416507JDMXXX10.1177/8756479311416507Wash ko et al.journal of Diagnostic Medical Sonography Pseudothrombosis of the Subclavian Vein Journal of Diagnostic Medical Sonography 27(5) 231 235 The Author(s) 2011
Vascular Injuries in the Throwing Shoulder MLB Winter Meeting 2015
 Neurovascular Problems in the Throwing Athlete s Shoulder Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Team Physician, Chicago White Sox and Bulls Chief Medical Editor,
Neurovascular Problems in the Throwing Athlete s Shoulder Professor, Department of Orthopedics Head, Section of Shoulder and Elbow Surgery Team Physician, Chicago White Sox and Bulls Chief Medical Editor,
Thoracic Outlet Syndrome
 Thoracic Outlet Syndrome Part 1: The Scalene Triangle TOS: Vascular Symptom Presentation Venous persistent/intermittent edema heaviness and fatigue deep pain in neck/shoulder increased pain at night warm
Thoracic Outlet Syndrome Part 1: The Scalene Triangle TOS: Vascular Symptom Presentation Venous persistent/intermittent edema heaviness and fatigue deep pain in neck/shoulder increased pain at night warm
THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA
 THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates THE THORACIC OUTLET
THORACIC OUTLET SYNDROME: A FREQUENT CAUSE OF NON-DISCOGENIC BRACHIALGIA Debora Garozzo Brachial Plexus and Peripheral Nerve Surgery Unit Neurospinal Hospital Dubai, United Arab Emirates THE THORACIC OUTLET
ORIGINAL ARTICLE. Spectrum of Thoracic Outlet Syndrome Presentation in Adolescents
 ORIGINAL ARTICLE Spectrum of Thoracic Outlet Syndrome Presentation in Adolescents Kevin Chang, BA; Emma Graf; Kylie Davis; Jasmine Demos, CRNP; Taylor Roethle; Julie Ann Freischlag, MD Objective: To study
ORIGINAL ARTICLE Spectrum of Thoracic Outlet Syndrome Presentation in Adolescents Kevin Chang, BA; Emma Graf; Kylie Davis; Jasmine Demos, CRNP; Taylor Roethle; Julie Ann Freischlag, MD Objective: To study
The Brachial Plexus and Thoracic Outlet Syndrome
 The Brachial Plexus and Thoracic Outlet Syndrome Understanding Signs and Symptoms By Joseph E. Muscolino, DC The brachial plexus of nerves and the subclavian/axillary artery and vein comprise a neurovascular
The Brachial Plexus and Thoracic Outlet Syndrome Understanding Signs and Symptoms By Joseph E. Muscolino, DC The brachial plexus of nerves and the subclavian/axillary artery and vein comprise a neurovascular
Upper Extremity Venous Duplex. Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016
 Upper Extremity Venous Duplex Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016 Patricia A. (Tish) Poe, BA RVT FSVU Director of Quality Assurance Navix Diagnostix Patricia A. Poe
Upper Extremity Venous Duplex Michigan Sonographers Society Fall Ultrasound Symposium October 15, 2016 Patricia A. (Tish) Poe, BA RVT FSVU Director of Quality Assurance Navix Diagnostix Patricia A. Poe
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome)
") A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
A Patient s Guide to Ulnar Nerve Entrapment at the Wrist (Guyon s Canal Syndrome) Introduction The ulnar nerve is often called the funny bone at the elbow. However, there is little funny about injury to
ADHESIVE CAPSULITIS (FROZEN SHOULDER)
") ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
ADHESIVE CAPSULITIS (FROZEN SHOULDER) Frozen shoulder, or adhesive capsulitis is a condition that generally begins with the gradual onset of pain followed by a limitation of shoulder motion. The discomfort
Paget-Schrötter Syndrome and the Thoracic Outlet. Carl Aschkenasi September 6, 2001
 Paget-Schrötter Syndrome and the Thoracic Outlet Carl Aschkenasi September 6, 2001 1 Our Patient: Acute onset left arm pain J.B. is a 44 yo male lawyer Has had a hx of occasional mild L arm pain on exertion
Paget-Schrötter Syndrome and the Thoracic Outlet Carl Aschkenasi September 6, 2001 1 Our Patient: Acute onset left arm pain J.B. is a 44 yo male lawyer Has had a hx of occasional mild L arm pain on exertion
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME
 ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
ROTATOR CUFF INJURIES / IMPINGEMENT SYNDROME Shoulder injuries are common in patients across all ages, from young, athletic people to the aging population. Two of the most common problems occur in the
Treatment of acute thrombosis of axillo-subclavian vein
 Treatment of acute thrombosis of axillo-subclavian vein Yang Jin Park Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine CASE A 32-year-old male patient 3-day history of
Treatment of acute thrombosis of axillo-subclavian vein Yang Jin Park Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine CASE A 32-year-old male patient 3-day history of
Case 1. Your diagnosis
 Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
Case 1 44-year-old midwife presented with intermittent pins and needles in the little and ring fingers with blanching. Symptoms were exacerbated by cold exposure. Your diagnosis Diagnosis Hypothenar syndrome
Clinical examination of the shoulder girdle
 Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
University Journal of Medicine and Medical Specialities
 ISSN 2455-2852 2018, Vol. 4(5) Imaging Assessment of Vascular Thoracic Outlet Syndrome BALAJI A AYYAMPERUMAL Department of Radio Diagnosis,MADRAS MEDICAL COLLEGE AND GOVERNMENT GENERAL HOSPITAL Abstract
ISSN 2455-2852 2018, Vol. 4(5) Imaging Assessment of Vascular Thoracic Outlet Syndrome BALAJI A AYYAMPERUMAL Department of Radio Diagnosis,MADRAS MEDICAL COLLEGE AND GOVERNMENT GENERAL HOSPITAL Abstract
THORACIC OUTLET SYNDROME AND THE OVERHEAD ATHLETE LISA PIROPATO, PT, DPT, ATC NORTHEAST INDIANA SPORTS MEDICINE SYMPOSIUM MARCH 25, 2017
 THORACIC OUTLET SYNDROME AND THE OVERHEAD ATHLETE LISA PIROPATO, PT, DPT, ATC NORTHEAST INDIANA SPORTS MEDICINE SYMPOSIUM MARCH 25, 2017 LEARNING OBJECTIVES Explain the etiologies of thoracic outlet syndrome.
THORACIC OUTLET SYNDROME AND THE OVERHEAD ATHLETE LISA PIROPATO, PT, DPT, ATC NORTHEAST INDIANA SPORTS MEDICINE SYMPOSIUM MARCH 25, 2017 LEARNING OBJECTIVES Explain the etiologies of thoracic outlet syndrome.
Case Report Successful Closed Reduction of a Lateral Elbow Dislocation
 Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
Case Reports in Orthopedics Volume 2016, Article ID 5934281, 5 pages http://dx.doi.org/10.1155/2016/5934281 Case Report Successful Closed Reduction of a Lateral Elbow Dislocation Kenya Watanabe, Takuma
A Patient s Guide to Quadrilateral Space Syndrome
 A Patient s Guide to Quadrilateral Space Syndrome Orthopedic and Sports Medicine 825 South 8th Street, #550 Minneapolis, MN 55404 Phone: 612-333-5000 Fax: 612-333-6922 DISCLAIMER: The information in this
A Patient s Guide to Quadrilateral Space Syndrome Orthopedic and Sports Medicine 825 South 8th Street, #550 Minneapolis, MN 55404 Phone: 612-333-5000 Fax: 612-333-6922 DISCLAIMER: The information in this
82a Orthopedic Massage! Introduction - Thoracic Outlet"
 82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
D E L L O N I N S T I T U T E S F O R P E R I P H E R A L N E R V E S U R G E R Y
 Thoracic Outlet (TOS), Winged Scapula, Brachial Plexus Compression 12 D E L L O N I N S T I T U T E S F O R P E R I P H E R A L N E R V E S U R G E R Y 1122 KENILWORTH DRIVE, SUITE 18, TOWSON, MARYLAND
Thoracic Outlet (TOS), Winged Scapula, Brachial Plexus Compression 12 D E L L O N I N S T I T U T E S F O R P E R I P H E R A L N E R V E S U R G E R Y 1122 KENILWORTH DRIVE, SUITE 18, TOWSON, MARYLAND
Thoracic outlet syndrome: first rib resection
 Review rticle Page 1 of 7 Thoracic outlet syndrome: first rib resection ornelis G. Vos 1, Çag das Ünlü 1, Michiel T. Voûte 2, Rob H. W. van de Mortel 3, Jean-Paul P. M. de Vries 3 1 Department of Surgery,
Review rticle Page 1 of 7 Thoracic outlet syndrome: first rib resection ornelis G. Vos 1, Çag das Ünlü 1, Michiel T. Voûte 2, Rob H. W. van de Mortel 3, Jean-Paul P. M. de Vries 3 1 Department of Surgery,
The treatment of Paget-Schroetter syndrome or effort
 Reoperations After Failed Transaxillary First Rib Resection to Treat Paget-Schroetter Syndrome Patients J. Ernesto Molina, MD Division of Cardiothoracic Surgery, University of Minnesota, Medical School,
Reoperations After Failed Transaxillary First Rib Resection to Treat Paget-Schroetter Syndrome Patients J. Ernesto Molina, MD Division of Cardiothoracic Surgery, University of Minnesota, Medical School,
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Tom Eisele, Benedikt M. Muenz, and Grigorios Korosoglou. Department of Cardiology & Vascular Medicine, GRN Hospital Weinheim, Weinheim, Germany
 Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
SAMPLE CHAPTERS UNESCO-EOLSS MANAGEMENT OF SUBCLAVIAN VEIN THROMBOSIS KNOWN AS PAGET-SCHROETTER SYNDROME
 MANAGEMENT OF SUBCLAVIAN VEIN THROMBOSIS KNOWN AS PAGETSCHROETTER SYNDROME J. Ernesto Molina University of Minnesota, Minneapolis, Minnesota, U.S.A. Keywords: Thoracic outlet, Venous disease Contents 1.
MANAGEMENT OF SUBCLAVIAN VEIN THROMBOSIS KNOWN AS PAGETSCHROETTER SYNDROME J. Ernesto Molina University of Minnesota, Minneapolis, Minnesota, U.S.A. Keywords: Thoracic outlet, Venous disease Contents 1.
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
A simple MRI technique for the assessment of thoracic outlet compression syndrome (TOCS)
") A simple MRI technique for the assessment of thoracic outlet compression syndrome (TOCS) Poster No.: C-3128 Congress: ECR 2010 Type: Scientific Exhibit Topic: Vascular Authors: E. Fanou, M. Cowling; Stoke-on-Trent/UK
A simple MRI technique for the assessment of thoracic outlet compression syndrome (TOCS) Poster No.: C-3128 Congress: ECR 2010 Type: Scientific Exhibit Topic: Vascular Authors: E. Fanou, M. Cowling; Stoke-on-Trent/UK
5 minutes: Attendance and Breath of Arrival. 50 minutes: Problem Solving Torso
 5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Torso Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here on time
5 minutes: Attendance and Breath of Arrival 50 minutes: Problem Solving Torso Punctuality- everybody's time is precious: o o Be ready to learn by the start of class, we'll have you out of here on time
Thoracic Outlet Syndrome
 James J. Lehman, DC, MBA, FACO Associate Professor of Clinical Sciences Director Health Sciences Postgraduate EducaCon University of Bridgeport Diagnosis is the key to successful treatment James J. Lehman,
James J. Lehman, DC, MBA, FACO Associate Professor of Clinical Sciences Director Health Sciences Postgraduate EducaCon University of Bridgeport Diagnosis is the key to successful treatment James J. Lehman,
thoracic outlet syndrome
 29 thoracic outlet syndrome N. Garcia-Henriquez, K.A. Illig Thoracic outlet syndrome (TOS) is a term describing one or more patterns of symptoms as a result of compression of the neurovascular bundle at
29 thoracic outlet syndrome N. Garcia-Henriquez, K.A. Illig Thoracic outlet syndrome (TOS) is a term describing one or more patterns of symptoms as a result of compression of the neurovascular bundle at
Brachial plexus blockade within the interscalene groove involves local anesthetic
 Interscalene Brachial Plexus Block- How I do it. Part 1 of a 2 part discussion on technique. Stuart Grant Professor of Anesthesiology Duke University Medical Center Durham NC Brachial plexus blockade within
Interscalene Brachial Plexus Block- How I do it. Part 1 of a 2 part discussion on technique. Stuart Grant Professor of Anesthesiology Duke University Medical Center Durham NC Brachial plexus blockade within
Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric Patient
 Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
Hindawi Case Reports in Orthopedics Volume 2017, Article ID 6354284, 4 pages https://doi.org/10.1155/2017/6354284 Case Report Elastic Intramedullary Nailing of a Medial Clavicle Fracture in a Pediatric
The posterolateral thoracotomy is still probably the
 Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
THORACIC OUTLET DECOMPRESSION
 THORACIC OUTLET DECOMPRESSION Thesis Submitted in partial fulfillment of the degree of M.D. in general surgery By Abd El Aty Mohammed Sakr Supervised by Prof. Dr. Amr Ahmed Gad Prof. of vascular surgery
THORACIC OUTLET DECOMPRESSION Thesis Submitted in partial fulfillment of the degree of M.D. in general surgery By Abd El Aty Mohammed Sakr Supervised by Prof. Dr. Amr Ahmed Gad Prof. of vascular surgery
Outcome of Surgical Treatment for Arterial Thoracic Outlet Syndrome
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 6 Ver. IV (June. 2017), PP 09-13 www.iosrjournals.org Outcome of Surgical Treatment for Arterial
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 6 Ver. IV (June. 2017), PP 09-13 www.iosrjournals.org Outcome of Surgical Treatment for Arterial
Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm
 Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Case Reports in Vascular Medicine, Article ID 716752, 4 pages http://dx.doi.org/10.1155/2014/716752 Case Report Endovascular Repair of a Large Profunda Femoris Artery Pseudoaneurysm Ahsan Syed Khalid,
Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior
 Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior picture Symptoms and signs Aching or throbbing in the lateral forearm extending to thumb and
Symptoms and Referred Pain from Myofascial Trigger Points in the Anterior Scalene Muscle or Scalenus Anterior picture Symptoms and signs Aching or throbbing in the lateral forearm extending to thumb and
Thoracic outlet syndrome (TOS) results from compression
 results from compression") Safety and Efficacy of the Supraclavicular Approach to Thoracic Outlet Decompression Thomas S. Maxey, MD, T. Brett Reece, MD, Peter I. Ellman, MD, Curtis G. Tribble, MD, Nancy Harthun, MD, Irving L. Kron,
Safety and Efficacy of the Supraclavicular Approach to Thoracic Outlet Decompression Thomas S. Maxey, MD, T. Brett Reece, MD, Peter I. Ellman, MD, Curtis G. Tribble, MD, Nancy Harthun, MD, Irving L. Kron,
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS. Please check with the LCC bookstore for the required texts for this class.
 LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
LABETTE COMMUNITY COLLEGE BRIEF SYLLABUS SPECIAL NOTE: This brief syllabus is not intended to be a legal contract. A full syllabus will be distributed to students at the first class session. TEXT AND SUPPLEMENTARY
Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture Dislocation of the Elbow in an Adult
 Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Hindawi Case Reports in Orthopedics Volume 2018, Article ID 5401634, 6 pages https://doi.org/10.1155/2018/5401634 Case Report Intra-Articular Entrapment of the Medial Epicondyle following a Traumatic Fracture
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson
 Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V?
 Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Case Reports in Surgery, Article ID 723756, 4 pages http://dx.doi.org/10.1155/2014/723756 Case Report Medial Radial Head Dislocation Associated with a Proximal Olecranon Fracture: A Bado Type V? Neil Segaren,
Karl A. Illig, MD, and Mathew Wooster, MD
 Neurogenic Thoracic Outlet Syndrome Karl A. Illig, MD, and Mathew Wooster, MD Perhaps no condition treated by vascular surgeons has been associated with more confusion, subjectivity, and nihilism than
Neurogenic Thoracic Outlet Syndrome Karl A. Illig, MD, and Mathew Wooster, MD Perhaps no condition treated by vascular surgeons has been associated with more confusion, subjectivity, and nihilism than
 Nerve Compression Syndromes Median Nerve Carpal Tunnel Syndrome Pronator Syndrome Ulnar Nerve Cubital Tunnel Syndrome Ulnar Tunnel Syndrome TOS www.fisiokinesiterapia.biz Carpal Tunnel Syndrome (CTS) Definition
Nerve Compression Syndromes Median Nerve Carpal Tunnel Syndrome Pronator Syndrome Ulnar Nerve Cubital Tunnel Syndrome Ulnar Tunnel Syndrome TOS www.fisiokinesiterapia.biz Carpal Tunnel Syndrome (CTS) Definition
CERVICAL SPINE TIPS A
 CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
CERVICAL SPINE TIPS A Musculoskeletal Approach to managing Neck Pain An ALGORITHM, as a management guide Rick Bernau & Ian Wallbridge June 2010 THE PROCESS An interactive approach to the management of
Subclavian vein obstruction without thrombosis
 Subclavian vein obstruction without thrombosis Richard J. Sanders, MD, a and Sharon L. Hammond, MD, a,b Denver, Colo Background: Unilateral arm swelling caused by subclavian vein obstruction without thrombosis
Subclavian vein obstruction without thrombosis Richard J. Sanders, MD, a and Sharon L. Hammond, MD, a,b Denver, Colo Background: Unilateral arm swelling caused by subclavian vein obstruction without thrombosis
Official Definition. Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist.
 Mod 2 MMT Course Official Definition Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist. epidemiology Affects an estimated 3
Mod 2 MMT Course Official Definition Carpal tunnel syndrome, the most common focal peripheral neuropathy, results from compression of the median nerve at the wrist. epidemiology Affects an estimated 3
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS
 SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
SHOULDER IMPINGEMENT / ROTATOR CUFF TENDONITIS / SUBACROMIAL BURSITIS The terms impingement, rotator cuff tendonitis, and subacromial bursitis, all refer to a spectrum of the same condition. Anatomy The
What you need to know about Carpal Tunnel Syndrome
 What you need to know about Carpal Tunnel Syndrome and Other Disorders of the Neck, Shoulder, Elbow, Wrist and Hands It is my mission to empower patients with knowledge and care so that they can enjoy
What you need to know about Carpal Tunnel Syndrome and Other Disorders of the Neck, Shoulder, Elbow, Wrist and Hands It is my mission to empower patients with knowledge and care so that they can enjoy
James Lawrence Guzzo, MD, Kevin Chang, BA, Jasmine Demos, CRNP, CPNP, James H. Black, MD, and Julie A. Freischlag, MD, Baltimore, Md
 From the Southern Association for Vascular Surgery Preoperative thrombolysis and venoplasty affords no benefit in patency following first rib resection and scalenectomy for subacute and chronic subclavian
From the Southern Association for Vascular Surgery Preoperative thrombolysis and venoplasty affords no benefit in patency following first rib resection and scalenectomy for subacute and chronic subclavian
Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
 Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
Case Reports in Otolaryngology Volume 2016, Article ID 2028402, 4 pages http://dx.doi.org/10.1155/2016/2028402 Case Report Tortuous Common Carotid Artery: A Report of Four Cases Observed in Cadaveric Dissections
Gateway to the upper limb. An area of transition between the neck and the arm.
 Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Suprascapular Nerve Entrapment
 Suprascapular Nerve Entrapment Suprascapular nerve entrapment is an uncommon nerve condition in the shoulder, causing pain and weakness. It involves compression of the suprascapular nerve at the top or
Suprascapular Nerve Entrapment Suprascapular nerve entrapment is an uncommon nerve condition in the shoulder, causing pain and weakness. It involves compression of the suprascapular nerve at the top or
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy
 Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Volume 2016, Article ID 5184196, 4 pages http://dx.doi.org/10.1155/2016/5184196 Case Report Internal Jugular Vein Thrombosis in Isolated Tuberculous Cervical Lymphadenopathy Sanjay Khaladkar, Avadhesh
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Michael Meuse, M.D. Vascular and Interventional Radiology Iliac Vein Compression Syndrome Left CIV compressed by right CIA Virchow 1851: DVT L>R May and Thurner 1954: venous spurs Cockett and Thomas 1965:
Appendix. Suggested Forms to Gather Information from Patients with TOS
 Appendix Suggested Forms to Gather Information from Patients with TOS Three forms seem to be most useful for patients with thoracic outlet syndrome, and we urge all who treat this disorder to use them
Appendix Suggested Forms to Gather Information from Patients with TOS Three forms seem to be most useful for patients with thoracic outlet syndrome, and we urge all who treat this disorder to use them
CARPAL TUNNEL SYNDROME
 CARPAL TUNNEL SYNDROME Carpal tunnel syndrome results from the pinching or entrapping of the median nerve in the underside of the wrist. The actual pathology in most cases is due to either a decrease in
CARPAL TUNNEL SYNDROME Carpal tunnel syndrome results from the pinching or entrapping of the median nerve in the underside of the wrist. The actual pathology in most cases is due to either a decrease in
Clinical examination of the wrist, thumb and hand
 Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Work Related Musculoskeletal Disorders
 Work Related Musculoskeletal Disorders Upper Extremity Disorders Carpel tunnel syndrome Cubital tunnel syndrome Thoracic outlet syndrome Raynaud s syndrome (white finger) Rotator cuff syndrome DeQuervain
Work Related Musculoskeletal Disorders Upper Extremity Disorders Carpel tunnel syndrome Cubital tunnel syndrome Thoracic outlet syndrome Raynaud s syndrome (white finger) Rotator cuff syndrome DeQuervain
Unit 3 -- Relieve the Burden of Shoulder Dysfunction. Upper Torso & Shoulder Unit Study Guide
 Unit 3 -- Relieve the Burden of Shoulder Dysfunction Upper Torso & Shoulder Unit Study Guide This unit identifies problems of the shoulder joint and thoracic regions. Module 1 Module 2 Module 3 Module
Unit 3 -- Relieve the Burden of Shoulder Dysfunction Upper Torso & Shoulder Unit Study Guide This unit identifies problems of the shoulder joint and thoracic regions. Module 1 Module 2 Module 3 Module
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial Head with Both-Bone Forearm Fracture
 Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
Case Reports in Orthopedics Volume 2016, Article ID 8598139, 5 pages http://dx.doi.org/10.1155/2016/8598139 Case Report An Undescribed Monteggia Type 3 Equivalent Lesion: Lateral Dislocation of Radial
Subclavian and Axillary Artery Aneurysms
 Subclavian and Axillary Artery Aneurysms April 2008 Francesco A Aiello, M.D. Assistant Professor of Surgery Division of Vascular Endovascular Surgery University of Massachusetts Medical School None DISCLOSURES
Subclavian and Axillary Artery Aneurysms April 2008 Francesco A Aiello, M.D. Assistant Professor of Surgery Division of Vascular Endovascular Surgery University of Massachusetts Medical School None DISCLOSURES
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Emergency Approach to the Subclavian and Innominate Vessels
 Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM
 TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM OBJECTIVES Understand how we interact with technology new and old Understand how injury occurs Texting
TECHNOLOGY AND HOW WE USE IT TO DAMAGE OURSELVES WILLIAM A. DELP, DO ASSISTANT PROFESSOR OF OMM GA PCOM OBJECTIVES Understand how we interact with technology new and old Understand how injury occurs Texting
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
 Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Case Reports in Cardiology Volume 2016, Article ID 4979182, 4 pages http://dx.doi.org/10.1155/2016/4979182 Case Report Asymptomatic Pulmonary Vein Stenosis: Hemodynamic Adaptation and Successful Ablation
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Charlotte Shoulder Institute
 Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
Charlotte Shoulder Institute Patient Centered. Research Driven. Outcome Maximized. James R. Romanowski, M.D. Novant Health Perry & Cook Orthopedics and Sports Medicine 2826 Randolph Rd. Charlotte, NC 28211
RIB INJURIES. Contents What are rib injuries?...3
 Contents What are rib injuries?.............................................3 What are the symptoms and how is it diagnosed?.....................4 YOUR GUIDE TO RIB INJURIES Are there any complications
Contents What are rib injuries?.............................................3 What are the symptoms and how is it diagnosed?.....................4 YOUR GUIDE TO RIB INJURIES Are there any complications
The supraclavicular approach to scalenectomy and first rib resection: Description of technique
 The supraclavicular approach to scalenectomy and first rib resection: Description of technique Richard J. Sanders, M.D., and Susan Raymer, Denver, Colo. Supraclavicular first rib resection has been performed
The supraclavicular approach to scalenectomy and first rib resection: Description of technique Richard J. Sanders, M.D., and Susan Raymer, Denver, Colo. Supraclavicular first rib resection has been performed
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Upper extremity paraesthesia: Clinical assessment and reasoning
 Journal of Bodywork and Movement Therapies (2008) 12, 268 273 Journal of Bodywork and Movement Therapies www.intl.elsevierhealth.com/journals/jbmt CASE REVIEW Upper extremity paraesthesia: Clinical assessment
Journal of Bodywork and Movement Therapies (2008) 12, 268 273 Journal of Bodywork and Movement Therapies www.intl.elsevierhealth.com/journals/jbmt CASE REVIEW Upper extremity paraesthesia: Clinical assessment
Research Article A Novel Surgical Approach to Lipomatous Tumours of the Deltoid Region
 Sarcoma Volume 2010, Article ID 495834, 4 pages doi:10.1155/2010/495834 Research Article A Novel Surgical Approach to Lipomatous Tumours of the Deltoid Region Emad Al Absi, Tamanna Karim, Nigel Colterjohn,
Sarcoma Volume 2010, Article ID 495834, 4 pages doi:10.1155/2010/495834 Research Article A Novel Surgical Approach to Lipomatous Tumours of the Deltoid Region Emad Al Absi, Tamanna Karim, Nigel Colterjohn,
Department of Internal Medicine, Saitama Citizens Medical Center, Saitama , Japan
 Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
Case Reports in Cardiology Volume 2016, Article ID 8790347, 5 pages http://dx.doi.org/10.1155/2016/8790347 Case Report GuideLiner Catheter Use for Percutaneous Intervention Involving Anomalous Origin of
Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions.
 Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel
 Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Case Reports in Vascular Medicine Volume 2015, Article ID 725168, 4 pages http://dx.doi.org/10.1155/2015/725168 Case Report Successful Implantation of a Coronary Stent Graft in a Peripheral Vessel Alexander
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Most patients with neurologic thoracic outlet syndrome
 ORIGINAL ARTICLES: GENERAL THORACIC Upper Plexus Thoracic Outlet Syndrome: Optimal Therapy Harold C. Urschel, Jr, MD, and Maruf A. Razzuk, MD Division of Thoracic and Cardiovascular Surgery, The University
ORIGINAL ARTICLES: GENERAL THORACIC Upper Plexus Thoracic Outlet Syndrome: Optimal Therapy Harold C. Urschel, Jr, MD, and Maruf A. Razzuk, MD Division of Thoracic and Cardiovascular Surgery, The University
PREMIER SPINE CARE. Adrian P. Jackson, MD (Cervical Spine Specialist) Anterior Cervical Discectomy and Fusion (ACDF)
 Anterior Cervical Discectomy and Fusion (ACDF)") PREMIER SPINE CARE Adrian P. Jackson, MD (Cervical Spine Specialist) Anterior Cervical Discectomy and Fusion (ACDF) After your physical examination and a review of your films, you have been recommended
PREMIER SPINE CARE Adrian P. Jackson, MD (Cervical Spine Specialist) Anterior Cervical Discectomy and Fusion (ACDF) After your physical examination and a review of your films, you have been recommended
Kettering Breast Service. Advice and Arm Exercises Following Breast Surgery. Information
 Kettering Breast Service Advice and Arm Exercises Following Breast Surgery Information Exercises following breast surgery are an important part of post-operative care. The gentle exercises contained in
Kettering Breast Service Advice and Arm Exercises Following Breast Surgery Information Exercises following breast surgery are an important part of post-operative care. The gentle exercises contained in
CERVICAL STRAIN AND SPRAIN
 CERVICAL STRAIN AND SPRAIN Description Cervical strain/sprain is an injury to the neck caused when it is forcefully whipped or forced backward or forward. The structures involved are the muscles, ligaments,
CERVICAL STRAIN AND SPRAIN Description Cervical strain/sprain is an injury to the neck caused when it is forcefully whipped or forced backward or forward. The structures involved are the muscles, ligaments,