Inflammatory bowel disease. Kawa Obeid, PhD
|
|
|
- Shawn Byrd
- 5 years ago
- Views:
Transcription
1 Inflammatory bowel disease Kawa Obeid, PhD 63
2 Introduction Inflammatory bowel disease (IBD) can be divided into two chronic inflammatory disorders of the gastro- intestinal tract, namely Crohn's disease (CD) and ulcerative colitis (UC). Crohn's disease affects any part of the gastro- intestinal tract whereas ulcerative colitis affects the colon and rectum only.
3 Aetiology The causes of both CD and UC are unknown. Infective, immunological, dietary and psychosomatic causes have been suggested, but until recently there has been no evidence for any of these.
4 Environmental Diet: fat intake, fast food ingestion, milk and fibre consumption. Smoking: Crohn's disease: 40% of patients are smokers. Stopping smoking can provoke the emergence of ulcerative colitis. Infection: Exposure to Mycobacterium paratuberculosis has been considered a causative agent of Crohn's disease. Ulcerative colitis may present after an episode of infective diarrhoea. Enteric microflora: Patients with IBD show a loss of immunological tolerance to intestinal microflora and consequently antibiotics often play a role in the treatment of IBD.
5 Environmental Drug: Non- steroidal anti- inflammatory drugs (NSAIDs) such as diclofenac have been reported to exacerbate IBD. Stress: Some patients find that stress triggers a relapse in their IBD and this has been reproduced in animal models. It is thought that stress activates inflammatory mediators.
6 Genetic 15% of first degree relatives have IBD. There is mounting evidence that Crohn's disease and ulcerative colitis result from an inappropriate response of the immune system in the mucosa of the gastro- intestinal tract to normal enteric flora.
7 Pathophysiology of IBD Trigger factors typically cause a severe, prolonged and inappropriate inflammatory response in the gastro- intestinal tract and the ongoing inflammatory reaction leads to an alteration in GIT architecture. Genetically susceptible individuals seem unable to downregulate immune or antigen non- specific inflammatory responses.

8 CD v UC

9 Location and distribution of ulcerative colitis and Crohn's disease

10 Clinical manifestation
11 Extra-intestinal complications of IBD Around 20 30% of patients with IBD will present with extra- intestinal manifestations. They are more commonly seen in patients where IBD affects the colon. Complications affect the joints, skin, bone, eyes, liver and biliary tree and are more common in active disease.
12 Investigations Differential diagnoses of IBD include carcinoma, infection, drug- induced colitis, ischaemia, radiation damage, irritable bowel syndrome and diverticulitis.
13 Endoscopy The key diagnostic investigation in IBD is lower gastro- intestinal tract endoscopy (sigmoidoscopy and colonoscopy), which allows direct visualisation of the large bowel and histopathological assessment from biopsies.. In patients with severe symptoms, it is sometimes necessary to delay a full colonoscopy because of the increased risk of perforation. Radiology Radiological imaging (Computed tomography (CT scan) and magnetic resonance imagery (MRI) is complementary to clinical and endoscopic assessment.
14 Laboratory findings Although not diagnostic, active disease is suggested in patients with raised inflammatory markers that include erythrocyte sedimentation rate (ESR) and C- reactive protein (CRP) in addition to a low haemoglobin and raised platelet count. Vitamin B12 may be low in patients with chronic terminal ileal disease. Low red cell folate and serum albumin, magnesium, calcium, zinc and essential fatty acids also indicate chronic inflammation and malabsorption. Anti- Saccharomyces cer- evisiae antibodies (ASCA) are more likely to be present in Crohn's disease. Stool tests Red and white blood cells can be seen on microscopic examination of fresh stools. Microscopic identification of infective cells such as amoeba may also be visualised.
15 Management Nutritional therapy Nutritional therapy can be considered as an adjunctive or primary treatment. Patients with Crohn's disease are at particular risk of becoming malnourished and developing a variety of nutritional deficiencies Functional and structural damage to the small bowel can cause malabsorption problems and occasionally patients may require a low- lactose diet. Patients who have extensive small bowel resection may experience many nutritional deficiencies because of malabsorption. Iron depletion, hypoproteinemia, deficiencies in water- and fat- soluble vitamins. Where appropriate, and when enteral nutrition is not indicated or adequate, a total parenteral nutrition (TPN) regimen may be prescribed.
16 Drug treatment The main goals of drug treatment are to treat acute attacks, limit drug toxicity, modify the pattern of disease, avoid and/ or manage complications. The choice of drug and route of administration depends on the site, extent and severity of the disease together with the individual's treatment history. Drug therapy is often required for many years and patient preference, acceptability and possible side effects not only affect choice but will impact on medication adherence.
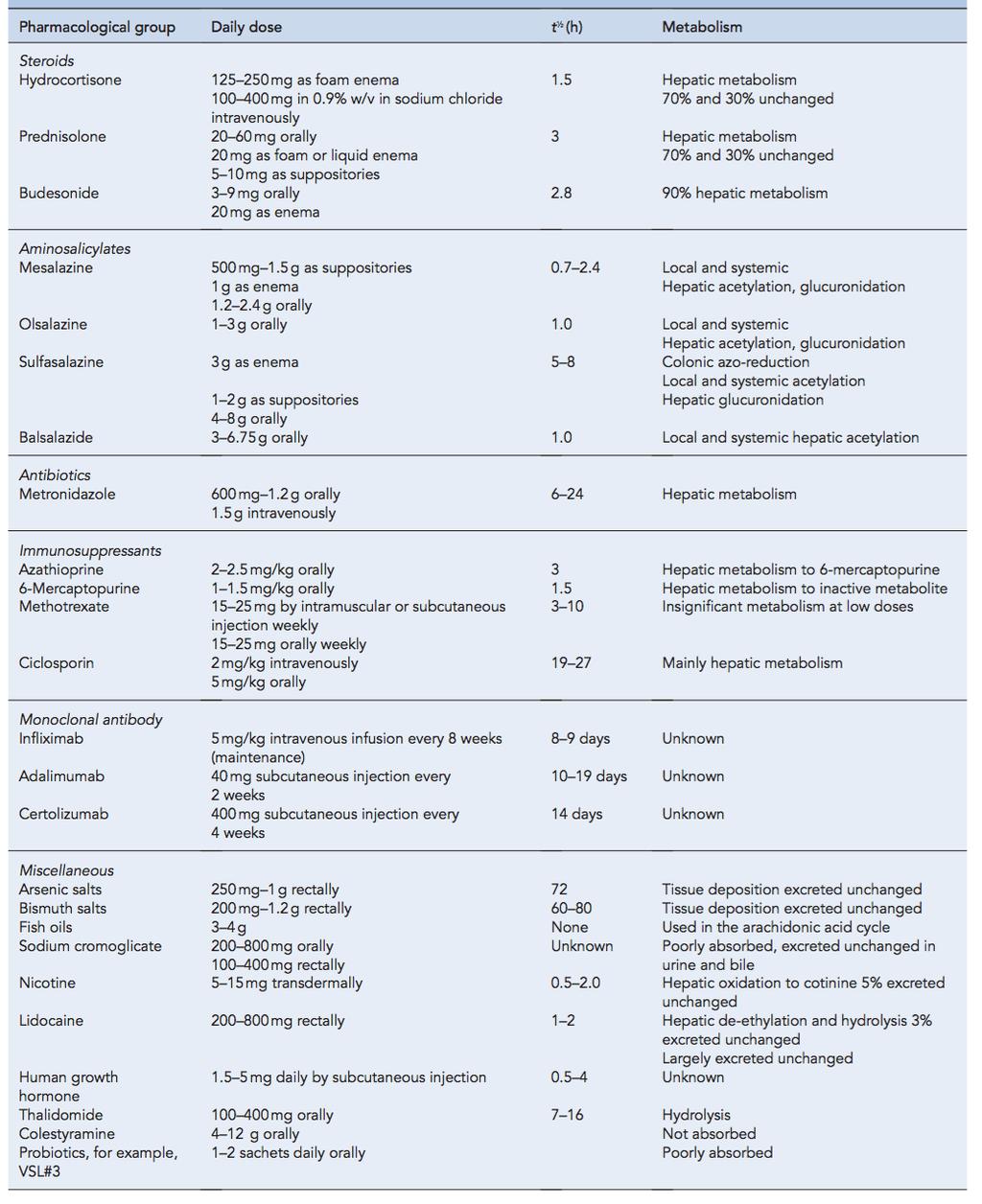
17 Corticosteroids, aminosalicylates and immunosuppressive agents (immunomodulators) such as azathioprine are the mainstays of treatment. Modern advances in treatment, such as the use of Human monoclonal antibody which modify the affected biochemical inflammatory pathways, now have a significant role in treatment of the disease. These are likely to be the main area of future development. Other drugs such as antibiotics, for example, metronidazole, are helpful in some cases, while colestyramine, thalidomide, sodium cromoglicate, bismuth and arsenical salts, nicotine, lidocaine, sucralfate, new steroid entities, cytoprotective agents, aloe vera, probiotics and fish oils are rarely used.
18 The route of administration is a particularly important factor in IBD. In contrast to most other conditions, minimal systemic absorption and maximal intestinal wall drug levels are required with oral therapy. Several delivery strategies have been used to achieve this including the chemical modification of drug molecules, delayed and controlled- release formulations and the use of bioadhesive particles. Proctitis is best treated with suppositories. Where inflammation affects the rectum and sigmoid colon (up to 15 20cm), foam enemas are preferred. In more extensive disease extending to the splenic flexure (30 60cm), liquid enemas are the agents of choice. Enemas or suppositories should be administered just before bedtime in a supine position as this allows a much longer retention time. Liquid enemas can be warmed and should be inserted while lying in the left lateral position.
19 Pharmacotherapy 1. Antidiarrhoeal agents, e.g. loperamide or codeine, may be needed to control florid symptoms, but should be used with caution because the resultant slower clearance of faecal residues may encourage the accumulation of pro- inflammatory agents and infectious agents.
20 2. Corticosteroids are the most effective agents and should be used to bring symptoms under control promptly in CD. Steroids, used intravenously in severe attacks (IV hydrocortisone or methylprednisolone therapy is used, e.g. up to 100 mg hydrocortisone 6- hourly) may be combined with aminosalicylates or, if the patient has been admitted in the previous 2 3 years with moderate to severe attacks, azathioprine. Oral prednisolone mg daily, reducing over 6 8 weeks, is widely used, with or without azathioprine or its metabolite, 6- mercaptopurine. Corticosteroid retention enemas are useful in CD only for rectal or distal colonic disease. In UC, corticosteroids are used to obtain remission in moderate to severe attacks or as an adjunct to aminosalicylates. Corticosteroid retention enemas is used routinely for UC and spare the systemic corticosteroid dose.
21 3. Immunosuppressants Azathioprine, or its metabolite 6- mercaptopurine, is used, especially in CD and moderate to severe UC for its steroid- sparing effect. It is ineffective as sole therapy in active disease as it takes several weeks to exert its effect. They are suitable for long- term maintenance therapy, but there is a high relapse rate on discontinuation. Methotrexate and IV ciclosporin have been used to manage disease resistant to steroids and other immunosuppressants. They are effective in producing remission but not for maintenance therapy.
22 4. Aminosalicylates These include sulfasalazine (SSZ), the original member of this group, which is a salt formed between sulfapyridine (SP) and 5- aminosalicylic acid (5- ASA); olsalazine (a dimer of 5- ASA); mesalazine (modified- release 5- ASA); and balsalazide (5- ASA linked by a diazo bond to 4- aminobenzoyl- beta- alanine, a carrier that has no pharmacological effect, unlike SP). SSZ is not absorbed in the small intestine, and the SP acts as a carrier to deliver 5- ASA to the colon, where the SSZ is split by bacterial action. The SP and some 5- ASA are subsequently absorbed, but about 50% of the 5- ASA remains in the colon to exert a local anti- inflammatory effect.
23 Oral mesalazine is specially formulated for large bowel release, in an attempt to avoid absorption of 5- ASA from the small intestine. It is licensed for the oral treatment of mild to moderate UC and to maintain remission. Olsalazine is similarly split by colonic bacteria to yield only 5- ASA and is licensed to treat mild UC and maintain remission. Balsalazide is a pro- drug of 5- ASA and resembles SSZ in drug delivery. The aminosalicylates are used primarily to induce and maintain remission in UC and for maintenance in CD.. SSZ is the only member of this group licensed for all severities of UC and for active CD, and also has a steroid- sparing effect. However, it has a limited place in the treatment of severe attacks, possibly because its hydrolysis to release 5- ASA is unpredictable in the diseased colon.
24 Few notes Side- effects. If the SP moiety in SSZ causes unacceptable side- effects, and this is more likely in slow acetylators, olsalazine, balsalazide or mesalazine may prove more suitable. However, 5- ASA also causes side- effects, e.g. nausea, headache, rash, and even diarrhoea and occa- sional exacerbation of colitis. SSZ causes a reversible oligospermia and so is unsuitable in men wishing to raise a family. There have also been occasional reports of nephrotoxicity with all aminosalicylates, which should be used cautiously in renal impairment and during pregnancy and breastfeeding. This is due to the absorption of 5- ASA, and mesalazine produces higher serum concentrations of 5- ASA than, olsalazine and balsalazie.
25 Few notes All aminosalicylates may cause blood dyscrasias, e.g. agranulocytosis, aplastic anaemia, leucopenia, neutropenia and thrombocytopenia. Patients should be advised to report any unexplained bruising, bleeding, sore throat, fever or malaise. If any of these occur the drug should be stopped and a full blood count done.
26 5. Biological agents Only one of these, infliximab, is currently used in IBD. human monoclonal antibody against the potent pro- inflammatory TNFalpha. It is used in severe active CD, especially if there is fistulation, and spares the corticosteroid dose. It is also licensed for moderate to severe UC. Recent trials have confirmed that infliximab is effective in UC. It produces about a 60% response rate at 8 weeks and about a 45% remission rate at 30 weeks. There is also significant mucosal healing and a steroid- sparing effect. Consequently, infliximab is likely to be especially beneficial in patients who are unresponsive to corticosteroids or are steroid- dependent, and in those who do not tolerate conventional immunosuppressive treatment. Adalimumab is a fully human anti- TNF anti- body that is currently licensed only for use in rheumatoid disease, but the licence is likely to be extended shortly for use in CD. a loading dose of 160 mg followed by 80 mg 2 weeks later, gives a remission rate of about 36% at 4 weeks. These doses are much larger than those used for RA. It appears to be effective in those who are not responding adequately to infliximab, but it is still antigenic. It has the advantage over infliximab that it is given by SC injection rather than by IV infusion. Certolizumab and natalizumab are under investigation
27 6. Antibiotics Metronidazole or tinidazole may be useful if there is bacterial overgrowth in the bowel or if septic complications occur, because anaerobes are often involved. Bowel perforation may lead to peritonitis and septicaemia, with an urgent need for surgery and parenteral antibiotics, after the identification of microbial sensitivities. Co- trimoxazole (trimethoprim plus sulfamethoxazole) has been used but is now appropriate only for infections of known sensitivity that are unresponsive to other agents. Continuing diarrhoea in well- treated patients is not necessarily due to infection, but may be due to failure of the diseased small bowel to reab- sorb bile salts. Treatment with the anion exchange resin colestyramine is then indicated.
28
29 Diet In contrast to the management of acute episodes, a high- residue diet is preferred unless there is a possibility of bowel obstruction, e.g. as the result of stricture formation. A high carbohydrate, high- protein diet minimizes the possibility of nutritional deficiency due to chronic diarrhoea. Vitamin and mineral supplementation, especially iron, is often given. Avoiding milk or milk products may occasionally be useful in some patients, especially those with small- bowel CD.
30 Surgery Surgery is indicated if medical management fails, for the treatment of complications, e.g. toxic megacolon, perforation, obstruction, malignancy. In UC, colectomy is curative. Colectomy is also carried out as an elective procedure in patients who have had extensive UC for more than 10 years, or if they have ever had a pancolitis, to pre- empt possible malignancy. Surgery is avoided as far as possible in CD, because relapse is common (30% in 5 years, 50% in 10 years) and repeated surgery is debilitating and carries a relatively high cumulative mortality.
31 Prognosis Nearly all CD patients have chronic or recurrent disease, with at least one serious relapse. The probability of recurrence is greater if there was extensive initial disease. In UC, some patients have only a single attack, but many have mild disease, with proctitis only.
32 Thank you Kawa A. Obeid PhD Therapeutics
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
ULCERATIVE COLITIS. Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC
 ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
ULCERATIVE COLITIS Sean Lynch, MD and Richard Bloomfeld, MD Wake Forest University School of Medicine Winston-Salem, NC What is Ulcerative Colitis? Ulcerative colitis (UC) is a disease marked by inflammation
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's Disease. What causes Crohn s disease? What are the symptoms?
 Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
INFLAMMATORY BOWEL DISEASE
 1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice SCOPE Clinical guideline title: Ulcerative colitis: the management of ulcerative colitis Quality standard title: Ulcerative
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
What is ulcerative colitis?
 What is ulcerative colitis? Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon. Ulcers form where inflammation has killed the cells
What is ulcerative colitis? Ulcerative colitis is a disease that causes inflammation and sores, called ulcers, in the lining of the rectum and colon. Ulcers form where inflammation has killed the cells
Medical therapies and IBD
 Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
Speaker Introduction
 Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital
 IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
IBD :- a new era of diagnostics and therapy Dr Martyn Dibb Consultant Luminal Gastroenterologist Royal Liverpool University Hospital Aims To understand the aetiology of IBD To understand the impact that
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online Support Group.
 Online Support Group.") Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
Welcome to Week 2 of the Crohn s & Colitis Foundation of America (CCFA) Online. Last week s material consisted of an overview of inflammatory bowel diseases (IBD), specifically Crohn s disease and ulcerative
Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152
 Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
WHAT IS ULCERATIVE COLITIS?
 235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Ulcerative Colitis WHAT IS ULCERATIVE COLITIS? Ulcerative colitis is
235 60th Street, West New York, NJ 07093 T: (201) 854-4646 F: (201) 854-4647 810 Main Street, Hackensack, NJ 07601 T: (201) 488-0095 Ulcerative Colitis WHAT IS ULCERATIVE COLITIS? Ulcerative colitis is
Guideline Ulcerative colitis: management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Ulcerative colitis: management Draft for consultation, December 0 This guideline covers the care and treatment of adults, children and young
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Ulcerative colitis: management Draft for consultation, December 0 This guideline covers the care and treatment of adults, children and young
Dr. Elmer Schabel, MD. Bundesinstitut für Arzneimittel und Medizinprodukte, Bonn, Germany (No conflicts of interest)
") EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
Guideline scope Diverticular disease: diagnosis and management
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Diverticular disease: diagnosis and management The Department of Health in England has asked NICE to develop a clinical guideline on diverticular
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 20 October 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 October 2010 MEZAVANT LP 1200 mg, prolonged-release gastro-resistant tablets B/60 (CIP code: 378 689-2) Applicant
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 October 2010 MEZAVANT LP 1200 mg, prolonged-release gastro-resistant tablets B/60 (CIP code: 378 689-2) Applicant
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018
 South East London Area Prescribing Committee: Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018 Developed by: South East London IBD Pathway Development Group Approved: February
South East London Area Prescribing Committee: Primary & Secondary Care Inflammatory Bowel Disease Pathway February 2018 Developed by: South East London IBD Pathway Development Group Approved: February
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Aminosalicylates in Inflammatory Bowel Disease in Adults (Review date: July 2020) Page 1
 Page 1") Full Title of Guideline: Author (include email and role): Aminosalicylates in Inflammatory Bowel Disease in Adults Natalie Tse- Senior Clinical Pharmacist (natalie.tse@nuh.nhs.uk) Dr. Nina Lewis- Consultant
Full Title of Guideline: Author (include email and role): Aminosalicylates in Inflammatory Bowel Disease in Adults Natalie Tse- Senior Clinical Pharmacist (natalie.tse@nuh.nhs.uk) Dr. Nina Lewis- Consultant
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Certain genes passed on from parent to child increase the risk of developing Crohn's disease, if the right trigger occurs.
 Topic Page: Crohn's disease Definition: Crohn's disease from Benders' Dictionary of Nutrition and Food Technology Chronic inflammatory disease of the bowel, commonly the terminal ileum, of unknown aetiology,
Topic Page: Crohn's disease Definition: Crohn's disease from Benders' Dictionary of Nutrition and Food Technology Chronic inflammatory disease of the bowel, commonly the terminal ileum, of unknown aetiology,
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Algorithm for managing severe ulcerative colitis
 Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
Tropical Gastroenterology 2014;Suppl:S40 44 Algorithm for managing severe ulcerative colitis Vineet Ahuja 1, Ajay Kumar 2, Rakesh Kochhar 3 ABSTRACT Dept of Gastroenterology, 1 All India Institute of Medical
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Garrick Brown, MD. Digestive Health Specialists Tacoma Gig Harbor
 Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
P a g e 1. Inflammatory Bowel Disease Guidelines
 P a g e 1 Inflammatory Bowel Disease Guidelines Introduction Inflammatory bowel disease (IBD) is a chronic inflammatory disease affecting the gastrointestinal (GI) system. It is comprised of two major
P a g e 1 Inflammatory Bowel Disease Guidelines Introduction Inflammatory bowel disease (IBD) is a chronic inflammatory disease affecting the gastrointestinal (GI) system. It is comprised of two major
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence 4-year surveillance (2017) Ulcerative colitis: management (2013) NICE guideline CG166 Appendix A.2: Summary of new evidence from surveillance Patient information
National Institute for Health and Care Excellence 4-year surveillance (2017) Ulcerative colitis: management (2013) NICE guideline CG166 Appendix A.2: Summary of new evidence from surveillance Patient information
Crohn s Disease. Questions & Answers
 Crohn s Disease Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard - 0141 810 3151 Ph.
Crohn s Disease Questions & Answers GLASGOW COLORECTAL CENTRE Ross Hall Hospital 221 Crookston Road Glasgow G52 3NQ e-mail: info@colorectalcentre.co.uk Ph: Main hospital switchboard - 0141 810 3151 Ph.
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Clinical Study Clinical Study of the Relation between Mucosal Healing and Long-Term Outcomes in Ulcerative Colitis
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2013, Article ID 192794, 6 pages http://dx.doi.org/10.1155/2013/192794 Clinical Study Clinical Study of the Relation between
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
1. Background: Infliximab is administered parenterally; therefore, it is not covered under retail pharmacy benefits.
 Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
10/23/2014. Program Goals
 Program Goals Help you understand ulcerative colitis and its effects Review current treatments, including medications, and surgery Provide tips for managing your disease through diet and complementary
Program Goals Help you understand ulcerative colitis and its effects Review current treatments, including medications, and surgery Provide tips for managing your disease through diet and complementary
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
A Case of Inflammatory Bowel Disease
 A Case of Inflammatory Bowel Disease Dr Barrie Rathbone www.le.ac.uk 26 year old Polish woman Admitted as emergency under surgeons RUQ and RIF pain Abdominal pain had occurred intermittently for a few
A Case of Inflammatory Bowel Disease Dr Barrie Rathbone www.le.ac.uk 26 year old Polish woman Admitted as emergency under surgeons RUQ and RIF pain Abdominal pain had occurred intermittently for a few
My Child Has Inflammatory Bowel Disease : Why? What now? What s next?
 My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
This information explains the advice about Crohn's disease that is set out in NICE guideline CG152.
 Information for the public Published: 1 October 2012 nice.org.uk About this information NICE guidelines provide advice on the care and support that should be offered to people who use health and care services.
Information for the public Published: 1 October 2012 nice.org.uk About this information NICE guidelines provide advice on the care and support that should be offered to people who use health and care services.
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Name of Shared Care Agreement: AZATHIOPRINE/6-MERCAPTOPURINE: Oral immunomodulating drugs for inflammatory bowel disease. Reference number: 01/2008
 Name of Shared Care Agreement: AZATHIOPRINE/6-MERCAPTOPURINE: Oral immunomodulating drugs for inflammatory bowel disease. Reference number: 01/2008 Shared care agreement has been developed appropriately
Name of Shared Care Agreement: AZATHIOPRINE/6-MERCAPTOPURINE: Oral immunomodulating drugs for inflammatory bowel disease. Reference number: 01/2008 Shared care agreement has been developed appropriately
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Understanding Learning is the first step to getting help.
 Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
Understanding Inflammatory Bowel Disease (IBD) Learning is the first step to getting help. This booklet has been created through an educational grant provided by Fulford India Ltd., A subsidiary of Schering-Plough
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
I B D. etter than this. isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES
 I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
The London Gastroenterology Partnership CROHN S DISEASE
 CROHN S DISEASE What is Crohn s disease? Crohn s disease is a condition, in which inflammation develops in parts of the gut leading to symptoms such as diarrhoea, abdominal pain and tiredness. The inflammation
CROHN S DISEASE What is Crohn s disease? Crohn s disease is a condition, in which inflammation develops in parts of the gut leading to symptoms such as diarrhoea, abdominal pain and tiredness. The inflammation
CASE STUDY: ULCERATIVE COLITIS. Sammi Montag Dietetic Intern
 CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
Infliximab (Remicade) for paediatric ulcerative colitis - second line
 for paediatric ulcerative colitis - second line") Infliximab (Remicade) for paediatric ulcerative colitis - second line September 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Infliximab (Remicade) for paediatric ulcerative colitis - second line September 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Top 10 Things you need to know about IBD. Suresh Pola, MD Kaiser San Diego
 Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
Ulcerative Colitis Therapy. Faculty Disclosure. Acknowledgements 28/11/2013. Amy Morse November 30/13
 Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT. Simon Radley Consultant Surgeon March 2013
 DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
DIVERTICULOSIS MEDICAL AND SURGICAL MANAGEMENT Simon Radley Consultant Surgeon March 2013 Definitions Diverticulosis: presence of diverticulae Diverticular disease: diverticulae associated with symptoms
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE
: CROHN S DISEASE") INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE Symptoms The symptoms of Crohn s disease can vary from person to person, based on where the disease is in the body and how bad the inflammation is. The
INFLAMMATORY BOWEL DISEASE (IBD): CROHN S DISEASE Symptoms The symptoms of Crohn s disease can vary from person to person, based on where the disease is in the body and how bad the inflammation is. The
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
What is Inflammatory Bowel Disease (IBD)?
?") INFLAMMATORY BOWEL DISEASE (IBD) What is Inflammatory Bowel Disease (IBD)? Inflammatory bowel disease, or IBD, is when there is inflammation, or swelling, in the gastrointestinal (GI) tract and a lifelong
INFLAMMATORY BOWEL DISEASE (IBD) What is Inflammatory Bowel Disease (IBD)? Inflammatory bowel disease, or IBD, is when there is inflammation, or swelling, in the gastrointestinal (GI) tract and a lifelong
Dr David Rowbotham. The Leeds Teaching Hospitals NHS Trust NHS
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Useful Titbits from the World of Gastroenterology David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura
 Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Soura") Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
Inflammatory Bowel Diseases (IBD) Clinical aspects Nitsan Maharshak M.D., IBD Center, Department of Gastroenterology and Liver Diseases Tel Aviv Sourasky Medical Center Tel Aviv, Israel IBD- clinical features
Title: Author: Journal:
 IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
INFLAMMATORY BOWEL DISEASE. Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic
 INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
INFLAMMATORY BOWEL DISEASE Jean-Paul Achkar, MD Center for Inflammatory Bowel Disease Cleveland Clinic WHAT IS INFLAMMATORY BOWEL DISEASE (IBD)? Chronic inflammation of the intestinal tract Two related
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Clinical Trials in IBD. Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases
 Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Clinical Trials in IBD Bruce Yacyshyn MD Professor of Medicine Division of Digestive Diseases Objectives Today s discussion will address the following topics: Similarities and differences between Crohn
Treatment Options. Suresh Pola, MD Kaiser San Diego
 Treatment Options Suresh Pola, MD Kaiser San Diego Overview of Treatments! Medications! Diet! Complementary and Alternative Medicines! How to treat Pain Treatment Goals and Target! Goals of Treatment should
Treatment Options Suresh Pola, MD Kaiser San Diego Overview of Treatments! Medications! Diet! Complementary and Alternative Medicines! How to treat Pain Treatment Goals and Target! Goals of Treatment should
Guide to Inflammatory Bowel Disease (IBD)
") Guide to Inflammatory Bowel Disease (IBD) Know your gut. Live your life. Scan this QR code to visit our mobile site. To scan download Scanlife from your app store, visit www.getscanlife.com on your mobile
Guide to Inflammatory Bowel Disease (IBD) Know your gut. Live your life. Scan this QR code to visit our mobile site. To scan download Scanlife from your app store, visit www.getscanlife.com on your mobile
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Current management options and recent advances in IBD
 n DRUG REVIEW Current management options and recent advances in IBD Ben Warner BSc, MRCP and Peter Irving MA, MD, FRCP SPL The advent of biological therapies has revolutionised the management of inflammatory
n DRUG REVIEW Current management options and recent advances in IBD Ben Warner BSc, MRCP and Peter Irving MA, MD, FRCP SPL The advent of biological therapies has revolutionised the management of inflammatory
Crohn s Disease. How does Crohn s disease affect the intestinal tract?
 Crohn s Disease Crohn s disease is one of the two main forms of inflammatory bowel disease (IBD). The second main form of inflammatory bowel disease is ulcerative colitis. Crohn s disease causes inflammation
Crohn s Disease Crohn s disease is one of the two main forms of inflammatory bowel disease (IBD). The second main form of inflammatory bowel disease is ulcerative colitis. Crohn s disease causes inflammation
Diarrhoea for the Acute Physician
 Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
Diarrhoea for the Acute Physician STEPHEN INNS GASTROENTEROLOGIST AND PHYSICIAN HUTT VALLEY DHB August 2013 Outline Case History 1 Initial assessment of acute diarrhoea Management of fulminant UC Management
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Inflammatory Bowel Disease (IBD)
") Inflammatory Bowel Disease (IBD) Pharmacotherapy 3 for PharmD Prof. Nailya Bulatova, MD, PhD Fall 2015 1 References DiPiro. Inflammatory Bowel Disease Koda-Kimble. Lower Gastrointestinal Disorders Ulcerative
Inflammatory Bowel Disease (IBD) Pharmacotherapy 3 for PharmD Prof. Nailya Bulatova, MD, PhD Fall 2015 1 References DiPiro. Inflammatory Bowel Disease Koda-Kimble. Lower Gastrointestinal Disorders Ulcerative
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
UNDERSTANDING CROHN S DISEASE
 UNDERSTANDING CROHN S DISEASE START YOUR JOURNEY TOWARD UNDERSTANDING INFLAMMATORY BOWEL DISEASE CONTENTS INTRODUCTION 4 WHAT IS CROHN S DISEASE? 6 Symptoms of Crohn s disease 6 WHAT CAUSES CROHN S DISEASE?
UNDERSTANDING CROHN S DISEASE START YOUR JOURNEY TOWARD UNDERSTANDING INFLAMMATORY BOWEL DISEASE CONTENTS INTRODUCTION 4 WHAT IS CROHN S DISEASE? 6 Symptoms of Crohn s disease 6 WHAT CAUSES CROHN S DISEASE?
Inflammatory Bowel Disease
 Inflammatory Bowel Disease Inflammatory bowel disease (IBD) is a group of inflammatory conditions of the colon and small intestine. Crohn's disease andulcerative colitis are the principal types of inflammatory
Inflammatory Bowel Disease Inflammatory bowel disease (IBD) is a group of inflammatory conditions of the colon and small intestine. Crohn's disease andulcerative colitis are the principal types of inflammatory
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Ulcerative Colitis. ulcerative colitis usually only affects the colon.
 Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
Ulcerative Colitis Introduction Ulcerative colitis is an inflammatory bowel disease. It is one of the 2 most common inflammatory bowel diseases. The other one is Crohn s disease. Ulcerative colitis and
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Trust Guideline. for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis. (*ie aged 16 years and over)
") Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
CHRONIC DIARRHEA DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS
 DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS") DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
What is Crohn's disease?
 What is Crohn's disease? Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area
What is Crohn's disease? Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area
International IBD Genetics Consortium
 International IBD Genetics Consortium PRED4 Thiopurine Induced Pancreatitis Case Report Form Please stick study label here On completion, please return to: Claire Bewshea IBD Pharmacogenetics Research
International IBD Genetics Consortium PRED4 Thiopurine Induced Pancreatitis Case Report Form Please stick study label here On completion, please return to: Claire Bewshea IBD Pharmacogenetics Research
SWL Drug Pathway Ulcerative Colitis Version 3 (Oct 2018) (based on NICE ulcerative colitis commissioning algorithm - with local adaptation)
 (based on NICE ulcerative colitis commissioning algorithm - with local adaptation)") Adult with active ulcerative colitis Does the adult have moderately to severely active ulcerative colitis managed in outpatients with no need for hospitalisation/surgery? Moderately to severely active
Adult with active ulcerative colitis Does the adult have moderately to severely active ulcerative colitis managed in outpatients with no need for hospitalisation/surgery? Moderately to severely active