In this second part of this two-part article
|
|
|
- Ann Thomas
- 5 years ago
- Views:
Transcription


1 Reconstruction of complex wounds in the trunk and pelvis: part two BY ANDREW BURD, SAMIM GHORBANIAN In this second part of this two-part article we begin by looking at component separation which is a technique of reconfiguring anatomical layers to allow intrinsic reconstruction of the integrity of the anterior abdominal wall. We then move into the domain of flaps but these are not typical flaps. By definition a flap comprises reconstructive tissue that retains its vascularity during positional transfer. Flaps can be categorised and defined in a number of ways including composition, vascular supply and movement. Component separation Component separation was brought to the forefront in 1990 by Ramirez et al. as another option for midline abdominal wall reconstruction [1]. This is an increasing problem in the era of obesity, burst abdomens and ventral hernias. Component separation restores the integrity of the abdominal wall and variations of the technique are present in the literature as early as 1916 (Gibson et al.). The technique involves a bipedicled advancement flap involving the rectus abdominis muscles, internal oblique and transversus abdominis muscles with or without a supplemental mesh. It remains a neurotised flap and can allow functionality that can provide stable soft tissue coverage with a good cosmetic appearance. It is most commonly indicated in repair of large, midline abdominal wall incisional hernias that have failed suture closure or mesh repair or secondary to abdominal wall resection due to malignancy or trauma. The type of defect that can be repaired is in the midline and up to about 20cm in diameter. It is also important to identify previous incisions and whether they may have compromised the innervation or blood supply of the abdominal components. In particular the superior and deep inferior epigastric arteries, which supply the rectus flap in conjunction with segmental intercostal vessels, if disrupted the rectus is supplied by collaterals from the internal oblique and the transversus abdominis muscles. The component separation method disconnects the muscle layers from their fascial sheaths to allow separate expansion of each muscle and a larger surface area. In the anterior approach, the abdominal pannus is carefully elevated from the underlying rectus and external oblique fascia, an incision is made in the external oblique aponeurosis 2cm lateral to the border of the rectus and external oblique muscles (i.e. semilunar line) and extending from the costal margin to the inguinal ligament. Separation of the external oblique muscle from the underlying internal oblique muscle results in approximately 5cm of advancement in the upper third of the abdomen, 10cm in the mid abdomen, and 3cm in the lower third of the abdomen. If this is not sufficient, the rectus muscle can be dissected free of its posterior sheath. This can lead to an additional 2 to 4cm of flap advancement. Some modification includes the use of mesh to reinforce the repair or an endoscopic method which can minimise ischaemia to the skin flaps. Recurrence rates for component separation repair without mesh are not significantly different from standard mesh hernia repairs but rates using mesh appear to be slightly lower, ranging from 4-10%. Flaps The local fillet flap: Figure 1 demonstrates the case of Susan, an incredibly brave woman, dying from advanced breast cancer, has been shared before in an open access editorial written in JPRAS [2]. This was a desperate measure to improve the quality of life of a dying patient and perhaps it was luck that it had such a dramatic and positive effect. But it led to an understanding that in highly selected cases significant improvement can be achieved in providing dignity and an improved quality of life in the dying patient. It is beyond the scope of this present article to discuss the philosophy and ethics of surgical palliation but it must be a consideration. Some years later when submitting a series of cases for publication in internationally recognised palliative care journals the response of the reviewers was uniformly prejudiced and biased. The Figure 1


![Finally, we found a journal with pragmatic editors who recognized the unique nature of our work and a case series was published [3].](/docs-images/84/90803470/images/2-2.jpg "A local transposition flap: The principle of transposing local tissue to reconstruct a defect created following tumour excision is")




.")


2 FEATURE palliative care physicians could manage pain, they could manage smell, they could manage the psychological distress of patients and there was no place for surgery. After repeated rejections in palliative care journals we submitted our paper to surgical journals. The response was initially bizarre; this was not evidence-based, we did not have randomised controls, etc. Finally, we found a journal with pragmatic editors who recognized the unique nature of our work and a case series was published [3]. A local transposition flap: The principle of transposing local tissue to reconstruct a defect created following tumour excision is well established. It is simple geometry and the principles can be scaled up. In Figure 2, a 56-year-old female patient presented with a two-year history of a fungating chest wall tumour. MRI depicted a left anterior chest mass invading dermal and subcutaneous tissues and PET-CT confirmed multiple right lung nodules with increased uptake in the right axillary nodes. An incisional biopsy revealed a malignant spindle cell neoplasm although the origin, skin or breast, was in doubt. The tumour needed excision with a wide margin for quality of life reasons. Prior to excision the tumour was isolated in a betadine soaked gauze and a defect created. The educated scalpel indicated involvement of the lower part of the sternum which was also excised. How then to reconstruct the defect? A simple transposition flap. At the same time a right axillary block dissection was performed. Ten months later the patient represented with a large left supraclavicular mass (Figure 3). A forequarter amputation was performed with in continuity excision of the local recurrent tumour. The defect was closed with a simple local flap. Followup two years later reported the patient had returned to work, as a caretaker in an apartment block and there was no evidence of recurrent disease. It led to an understanding that in highly selected cases significant improvement can be achieved in providing dignity and an improved quality of life in the dying patient. Pedicled flaps: When discussing the definition of a pedicled flap there is often some confusion regarding the composition of the pedicle and the anatomical relationship between the donor and recipient site. The first case (Figure 4) shows a simple V-Y advancement flap in the axilla based on a thoracodorsal artery perforator flap. This is not a complex wound but the case is included to illustrate a point although this may be contentious! The second case (Figure 5) shows a challenging fungating leiomyosarcoma on the right anterior chest wall. After excision, the Figure 4 Figure 2 Figure 3 Figure 5
.")


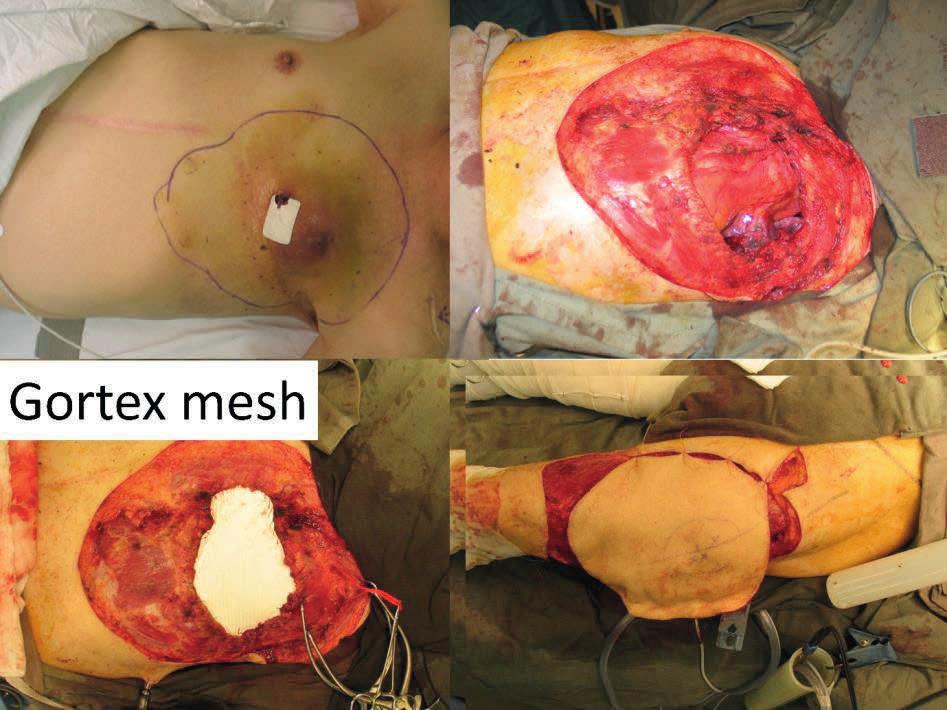
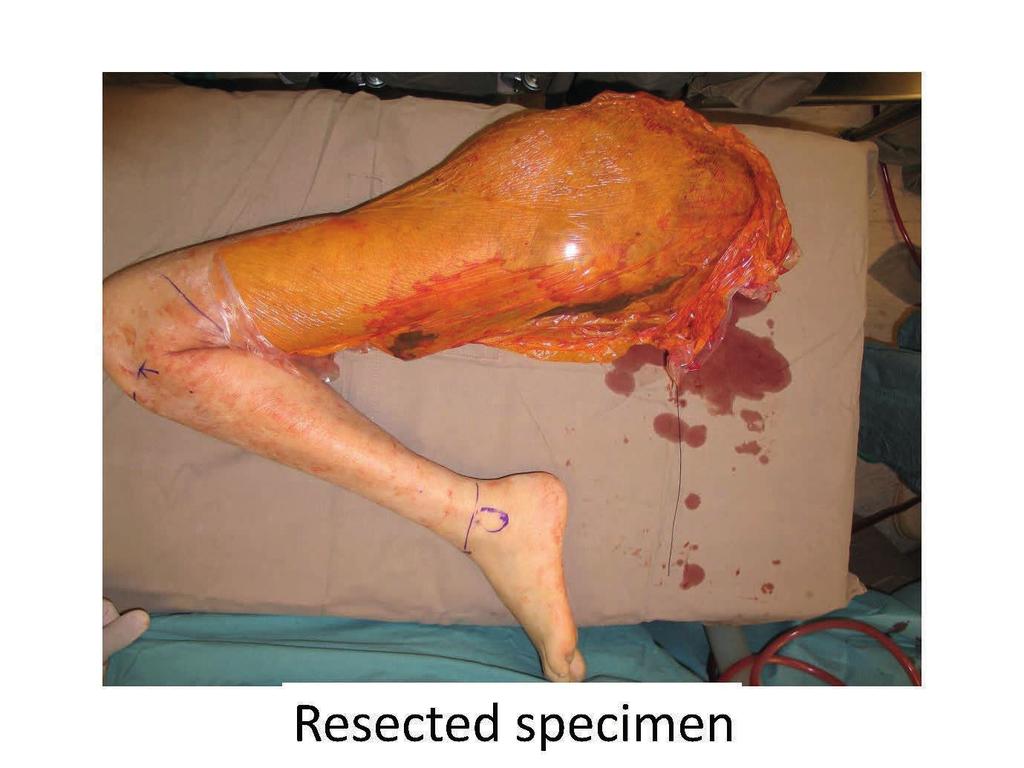
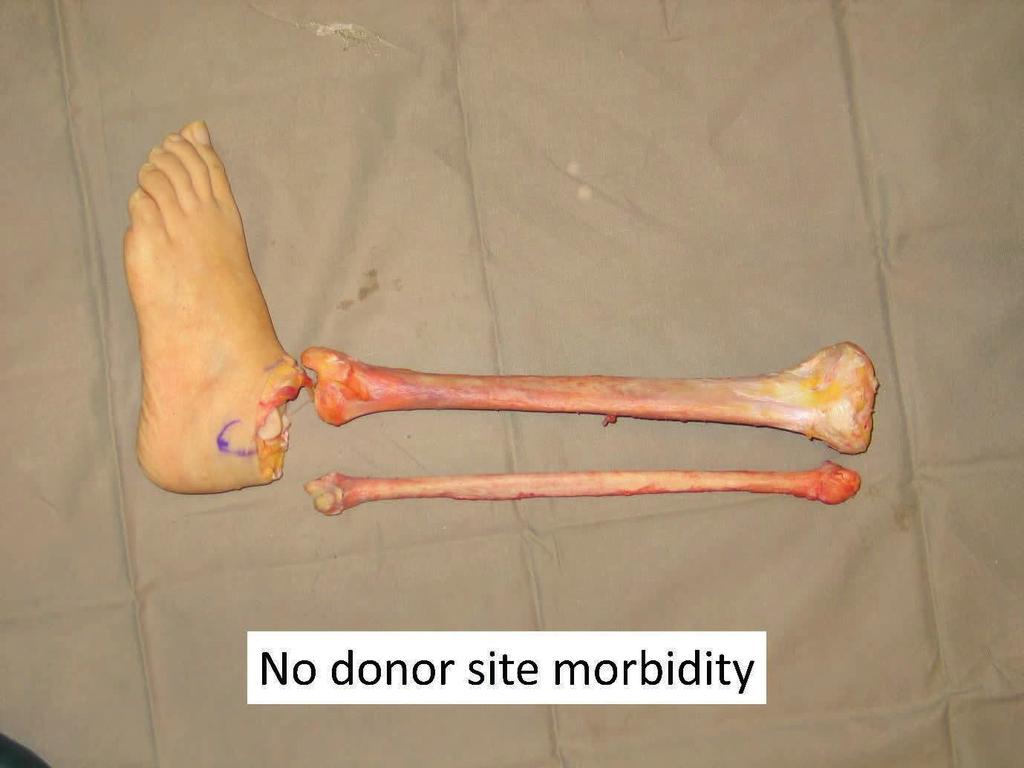
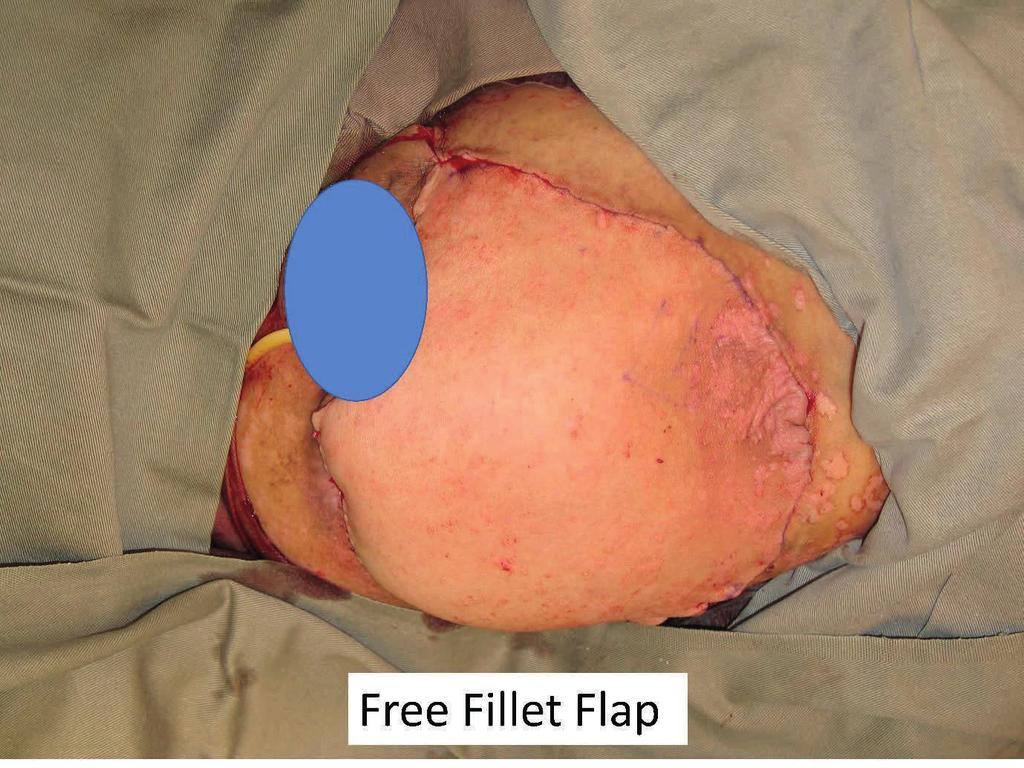
3 defect could be closed with a pedicled latissimus dorsi flap, or a pedicled vertical rectus abdominis myocutaneous (VRAM) or transverse rectus abdominis myocutaneous (TRAM). Large abdominal wall defects can be closed with a pedicled anterolateral thigh flap as illustrated in the next case (Figure 6). The patient had a local recurrence after a previous hindquarter amputation. Faecal diversion had already been performed and now urinary diversion was needed before closure of the abdominal wall defect with a pedicled anterolateral thigh flap. The donor site was reduced in size by inverting the skin margins and the muscle was grafted. This is an example of quality of life surgery where not only the patient but also the relatives have to be considered. This patient, as was also the case with Susan (mentioned previously), had a devoted partner who struggled to support her whilst being overcome with nausea at the smell of the fungating tumour. Smell is a very powerful force with a strong subjective overlay and must never be discounted by professional health workers. Replacement of the entire abdominal wall can be achieved by a pedicled anterior thigh flap based on perforators from the combined vascular pedicles of the superficial femoral artery and the descending branch of the lateral femoral circumflex artery. In Figure 7 the abdominal wall had been previously excised and a mesh applied following tumour excision. A large flap can be used to cover from the pubis to the xiphisternum and the donor defect closed with t-split thickness skin graft. Figure 6 Free tissue transfer: Breast reconstruction using free tissue transfer is one of the more common operations performed in plastic surgery units in the UK. In Figure 8 (overleaf) the pathology was rather different being an angiosarcoma of the male breast. This case illustrates an interesting reflection of the difference between the healthcare systems in the UK and in Hong Kong. In the UK such a patient would typically go to their family doctor who would make a referral to an NHS centre where there would be a multidisciplinary team (MDT) who would discuss the most appropriate treatment. In Hong Kong there is not a well-established primary care service and if a patient does not go through the public service they would seek advice from a specialist de novo. Of course, the whole point of the MDT is to allow the respective specialists to discuss the merits and drawbacks of the various therapeutic strategies. Angiosarcoma is a challenging pathology which is usually radio-resistant. The patient realised that they most probably had a tumour and so decided to see an oncologist. The oncologist ordered imaging that revealed multiple pulmonary nodules and so used this to justify chemotherapy. After three cycles of chemotherapy there was a reduction in pulmonary deposits but the primary tumour remained unchanged and so at this stage referred the patient for a surgical opinion. The thought was that if the tumour mass could be debulked the residual malignancy might respond to the chemotherapy. The tumour was excised widely and in depth to leave a defect with exposed mediastinum and lung. The compartmentalisation of the thoracic cavity was reconstituted with a Gortex mesh. The skin defect was reconstructed with a large anterolateral thigh free flap and the patient was discharged home 10 days post-surgery. Figure 7 Free fillet flap: Fungating girdle tumour present both challenges in control but also opportunities in reconstruction. It is essential to be able to achieve proximal vascular control before attempting to ablate local disease. There is a fine line between surgical futility and surgical palliation. The situation is rather different from medical futility where the concept is to protect doctors from patients or relatives who will not accept that further treatment will result in no benefit. Laws were needed to protect doctors from being sued by patients or relatives when they refused to continue what was regarded as a futile treatment. The situation is different for surgery where patients have to be protected from surgeons whose belief in their surgical skills exceeds their practical abilities. Nevertheless, there will be cases where appropriate imaging can indicate the possibility of achieving vascular control enabling the resection of extremely large tumours. The point with girdle tumours is the distal limb may not be involved with any pathology and thus can be a source for reconstructive tissue which will not be associated with any donor site morbidity. The next patient (Figure 9 overleaf) was a dramatic case of a massive fungating and bleeding tumour. After extensive discussion the patient consented to surgery. The resected specimen is shown which shows the lack of involvement of the distal lower leg. The soft




4 FEATURE Figure 8 Figure 9


 a young patient is shown who has had a hind quarter amputation and now progressive local disease has resulted in multiple faecal fistulas.")


5 tissues were stripped at periosteal level to allow a large flap to be raised to close the pelvic defect. The patient survived for 36 months and became a patient counsellor for other patients with advanced malignant disease. She gave full permission for her photograph to be used so that she could be an inspiration to others both in life and in death. Negative pressure therapy: No discussion of the management of complex wounds of the trunk would be complete without including the mention of negative pressure therapy. This has multiple roles including the active preparation of wounds for definitive surgical closure, closure without surgery and also in the comfort care of the dying patient. In this illustrated case (Figure 10) a young patient is shown who has had a hind quarter amputation and now progressive local disease has resulted in multiple faecal fistulas. Management of the wound was requiring painful dressing changes three times a day that was distressing for both the patient and the mother who insisted on caring for her dying son. The patient was taken to theatre for one final debridement and closure of the fistulas and the application of an irrigating negative pressure wound therapy device. No further dressing changes were necessary in the subsequent few days and the patient was allowed to die both in comfort and with dignity. Summary This two-part article has covered a broad scope of reconstructive options which reflect a variety of technical challenges in the surgical procedures. It must be remembered though that it is the outcome as experienced by the patient and their relatives that is most important. The temporal element is very important when considering the implications of growth in children and value of days and weeks in the dying. In all cases we must be humble and honest in approach, yet brave and fearless, although not foolhardy, in execution. References 1. Ramirez OM, Ruas E, Dellon AL. Components separation method for closure of abdominalwall defects: an anatomic and clinical study. Plastic and Reconstructive Surgery 1990;86(3): Burd A. Obituaries, death and dying. Journal of Plastic, Reconstructive & Aesthetic Surgery 2008;61(9): Burd A, Wong KC, Kumta SM. Aggressive surgical palliation for advanced girdle tumours. Indian Journal of Plastic Surgery 2012;45(1):16. AUTHORS Andrew Burd, Locum Consultant Burns and Plastic Surgeon, Nottingham University Hospitals NHS Trust, UK. E: darburd@gmail.com Samim Ghorbanian, Plastic Surgery Trainee, Nottingham University Hospitals NHS Trust, UK. Declaration of competing interests: None declared. Figure 10
4/30/2010. Options for abdominal wall reconstruction. Scott L. Hansen, MD
 Components Separation Scott L. Hansen, MD University of California, San Francisco Chief, Plastic and Reconstructive Surgery San Francisco General Hospital Overview Options for abdominal wall reconstruction
Components Separation Scott L. Hansen, MD University of California, San Francisco Chief, Plastic and Reconstructive Surgery San Francisco General Hospital Overview Options for abdominal wall reconstruction
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty
 CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
CASE REPORT An Innovative Solution to Complex Inguinal Defect: Deepithelialized SIEA Flap With Mini Abdominoplasty Augustine Reid Wilson, MS, Justin Daggett, MD, Michael Harrington, MD, MPH, and Deniz
-primarily by apposition of the anterior rectus
 2 Component separation Cop HARVEY CHIM, KAREN KIM EVANS, AND SAMIR MARDINI Mater al Introduction 7 Preoperative markings 7 Intraoperative details 9 Technique modification: Component separation with preservation
2 Component separation Cop HARVEY CHIM, KAREN KIM EVANS, AND SAMIR MARDINI Mater al Introduction 7 Preoperative markings 7 Intraoperative details 9 Technique modification: Component separation with preservation
Abdomen: Introduction. Prof. Oluwadiya KS
 Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
Abdomen: Introduction Prof. Oluwadiya KS www.oluwadiya.com Abdominopelvic Cavity Abdominal Cavity Pelvic Cavity Extends from the inferior margin of the thorax to the superior margin of the pelvis and the
Extended double pedicle free tensor
 e141 Case Report Extended double pedicle free tensor fascia latae myocutaneous flap for abdominal wall reconstruction Dorai A A, Halim A S ABSTRACT Extensive full thickness anterior abdominal wall defects
e141 Case Report Extended double pedicle free tensor fascia latae myocutaneous flap for abdominal wall reconstruction Dorai A A, Halim A S ABSTRACT Extensive full thickness anterior abdominal wall defects
Endoscopic assisted harvest of the pedicled pectoralis major muscle flap
 British Journal of Plastic Surgery (2005) 58, 170 174 Endoscopic assisted harvest of the pedicled pectoralis major muscle flap Arif Turkmen*, A. Graeme B. Perks Plastic Surgery Department, Nottingham City
British Journal of Plastic Surgery (2005) 58, 170 174 Endoscopic assisted harvest of the pedicled pectoralis major muscle flap Arif Turkmen*, A. Graeme B. Perks Plastic Surgery Department, Nottingham City
Chest Wall Tumors and Reconstruction: Lateral Chest Wall. Dr. Robert Kelly
 Chest Wall Tumors and Reconstruction: Lateral Chest Wall Dr. Robert Kelly THORACIC PROGRAMME: ADVANCES IN CHEST WALL SURGERY AND OSTEOSYNTHESIS Dr. José Ribas Milanez de Campos Assistant, Professor, Department
Chest Wall Tumors and Reconstruction: Lateral Chest Wall Dr. Robert Kelly THORACIC PROGRAMME: ADVANCES IN CHEST WALL SURGERY AND OSTEOSYNTHESIS Dr. José Ribas Milanez de Campos Assistant, Professor, Department
Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate surgical options
 across Ontario: Patient indications and appropriate surgical options") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
Breast Reconstruction Options
 Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC
 Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Case Study. TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis.
 Case Study TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis. TRAM Flap Reconstruction with an Associated Complication Challenge Insulin-dependent diabetes
Case Study TRAM Flap Reconstruction with an Associated Complication. Repair using DermaMatrix Acellular Dermis. TRAM Flap Reconstruction with an Associated Complication Challenge Insulin-dependent diabetes
Chest wall reconstruction using a combined musculocutaneous anterolateral anteromedial thigh flap
 Free full text on www.ijps.org Case Report DOI: 10.4103/0970-0358.63966 Chest wall reconstruction using a combined musculocutaneous anterolateral anteromedial thigh flap Pearlie W. W. Tan, Chin-Ho Wong,
Free full text on www.ijps.org Case Report DOI: 10.4103/0970-0358.63966 Chest wall reconstruction using a combined musculocutaneous anterolateral anteromedial thigh flap Pearlie W. W. Tan, Chin-Ho Wong,
Tor Chiu. Deep Inferior Epigastric Artery Perforator Flap 161
 18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study
 Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study Saeed Chowdhry, MD, Ron Hazani, MD, Philip Collis, BS, and Bradon J. Wilhelmi, MD University of
Anatomical Landmarks for Safe Elevation of the Deep Inferior Epigastric Perforator Flap: A Cadaveric Study Saeed Chowdhry, MD, Ron Hazani, MD, Philip Collis, BS, and Bradon J. Wilhelmi, MD University of
JPRAS Open 3 (2015) 1e5. Contents lists available at ScienceDirect. JPRAS Open. journal homepage:
 1e5. Contents lists available at ScienceDirect. JPRAS Open. journal homepage:") JPRAS Open 3 (2015) 1e5 Contents lists available at ScienceDirect JPRAS Open journal homepage: http://www.journals.elsevier.com/ jpras-open Case report The pedicled transverse partial latissimus dorsi
JPRAS Open 3 (2015) 1e5 Contents lists available at ScienceDirect JPRAS Open journal homepage: http://www.journals.elsevier.com/ jpras-open Case report The pedicled transverse partial latissimus dorsi
BOAST 4 Algorithm. 6th September 2013
 BOAST 4 Algorithm 6th September 2013 Background The British Orthopaedic Association and the British Association of Plastic, Reconstructive and Aesthetic Surgeons reviewed their 1997 guidance and published
BOAST 4 Algorithm 6th September 2013 Background The British Orthopaedic Association and the British Association of Plastic, Reconstructive and Aesthetic Surgeons reviewed their 1997 guidance and published
Abdominal Wall Reconstruction With the Free Tensor Fascia Lata Musculofasciocutaneous Flap Using Intraperitoneal Gastroepiploic Recipient Vessels
 Abdominal Wall Reconstruction With the Free Tensor Fascia Lata Musculofasciocutaneous Flap Using Intraperitoneal Gastroepiploic Recipient Vessels Pierre M. Chevray, MD, PhD* Navin K. Singh, MD The authors
Abdominal Wall Reconstruction With the Free Tensor Fascia Lata Musculofasciocutaneous Flap Using Intraperitoneal Gastroepiploic Recipient Vessels Pierre M. Chevray, MD, PhD* Navin K. Singh, MD The authors
Policy No: FCHN.MP Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14
 Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14 SUBJECT: Abdominoplasty, Panniculectomy and Ventral/Incisional Hernia RELATED POLICIES/RELATED DESKTOP PROCEDURES:
Page 1 of 6 Date Originated: Last Review Date Current Revision Date 7/10/07 06/2014 7/2/14 SUBJECT: Abdominoplasty, Panniculectomy and Ventral/Incisional Hernia RELATED POLICIES/RELATED DESKTOP PROCEDURES:
Interesting Case Series. Scalp Reconstruction With Free Latissimus Dorsi Muscle
 Interesting Case Series Scalp Reconstruction With Free Latissimus Dorsi Muscle Danielle H. Rochlin, BA, Justin M. Broyles, MD, and Justin M. Sacks, MD Department of Plastic and Reconstructive Surgery,
Interesting Case Series Scalp Reconstruction With Free Latissimus Dorsi Muscle Danielle H. Rochlin, BA, Justin M. Broyles, MD, and Justin M. Sacks, MD Department of Plastic and Reconstructive Surgery,
Radial Artery Pedicle Flap To Cover Exposed Mesh After Abdominal Wound Dehiscence-An Easy Solution To A Difficult Problem
 ISPUB.COM The Internet Journal of Plastic Surgery Volume 6 Number 1 Radial Artery Pedicle Flap To Cover Exposed Mesh After Abdominal Wound Dehiscence-An Easy Solution To A Difficult Problem S Tripathy,
ISPUB.COM The Internet Journal of Plastic Surgery Volume 6 Number 1 Radial Artery Pedicle Flap To Cover Exposed Mesh After Abdominal Wound Dehiscence-An Easy Solution To A Difficult Problem S Tripathy,
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery.
 This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
Principles of plastic and reconstructive surgery
 Plastic surgery - in general Principles of plastic and reconstructive surgery Dr. T. Németh, DVM, Ph.D, Diplomate ECVS Assoc. Professor and Head Definition: Surgical correction of morphological and/or
Plastic surgery - in general Principles of plastic and reconstructive surgery Dr. T. Németh, DVM, Ph.D, Diplomate ECVS Assoc. Professor and Head Definition: Surgical correction of morphological and/or
Breast Reconstruction with Superficial Inferior Epigastric Artery Flaps: A Prospective Comparison with TRAM and DIEP Flaps
 Breast Reconstruction with Superficial Inferior Epigastric Artery Flaps: A Prospective Comparison with TRAM and DIEP Flaps Pierre M. Chevray, M.D., Ph.D. Houston, Texas Breast reconstruction using the
Breast Reconstruction with Superficial Inferior Epigastric Artery Flaps: A Prospective Comparison with TRAM and DIEP Flaps Pierre M. Chevray, M.D., Ph.D. Houston, Texas Breast reconstruction using the
The Modified External Oblique Musculocutaneous Flap for Reconstruction of Extensive Post-Mastectomy Radio Necrosis: Clinical and Anatomical Study
 Egypt, J. Plast. Reconstr. Surg., Vol. 28, No. 1, January: 1-5, 2004 The Modified External Oblique Musculocutaneous Flap for Reconstruction of Extensive Post-Mastectomy Radio Necrosis: Clinical and Anatomical
Egypt, J. Plast. Reconstr. Surg., Vol. 28, No. 1, January: 1-5, 2004 The Modified External Oblique Musculocutaneous Flap for Reconstruction of Extensive Post-Mastectomy Radio Necrosis: Clinical and Anatomical
Flaps vs Grafts. Ronen Avram, MD MSc FRCSC
 Flaps vs Grafts Ronen Avram, MD MSc FRCSC POS Keratoacanthoma is not a malignant tumor! Methods of Reconstruction Reconstructive Ladder Primary closure Primary Delayed Secondary Intention Skin Graft Pedicled
Flaps vs Grafts Ronen Avram, MD MSc FRCSC POS Keratoacanthoma is not a malignant tumor! Methods of Reconstruction Reconstructive Ladder Primary closure Primary Delayed Secondary Intention Skin Graft Pedicled
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY RECTUS ABDOMINIS FLAP FOR HEAD & NECK RECONSTRUCTION Patrik Pipkorn, Brian Nussenbaum The rectus abdominis flap is based on the deep inferior
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY RECTUS ABDOMINIS FLAP FOR HEAD & NECK RECONSTRUCTION Patrik Pipkorn, Brian Nussenbaum The rectus abdominis flap is based on the deep inferior
Endoscopic Component Separation November Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine
 Endoscopic Component Separation November 2014 Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine Abdominal Wall Anatomy External Oblique Rectus Abdominus Internal Oblique
Endoscopic Component Separation November 2014 Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine Abdominal Wall Anatomy External Oblique Rectus Abdominus Internal Oblique
Farah S, Kiyingi A, Leinkram C. The Melbourne Hernia Clinic Masada Hospital 26 Balaclava Road St Kilda East Victoria, Australia 3168.
 Medium to Long term results following open intra-abdominal repair of large incisional hernias with a new composite polypropylene and silicone mesh, without components separation. Farah S, Kiyingi A, Leinkram
Medium to Long term results following open intra-abdominal repair of large incisional hernias with a new composite polypropylene and silicone mesh, without components separation. Farah S, Kiyingi A, Leinkram
Septic Bone and Joint Surgery
 Septic Bone and Joint Surgery Bearbeitet von Reinhard Schnettler 1. Auflage 2010. Buch. 328 S. Hardcover ISBN 978 3 13 149031 5 Format (B x L): 19,5 x 27 cm Weitere Fachgebiete > Medizin > Chirurgie >
Septic Bone and Joint Surgery Bearbeitet von Reinhard Schnettler 1. Auflage 2010. Buch. 328 S. Hardcover ISBN 978 3 13 149031 5 Format (B x L): 19,5 x 27 cm Weitere Fachgebiete > Medizin > Chirurgie >
CODING AND PRACTICE MANAGEMENT CORNER
 Hernia repair and complex abdominal wall reconstruction by Christopher Senkowski, MD, FACS; Mark Savarise, MD, FACS; John S. Roth, MD, FACS; and Jan Nagle, MS, RPh 52 The American College of Surgeons (ACS)
Hernia repair and complex abdominal wall reconstruction by Christopher Senkowski, MD, FACS; Mark Savarise, MD, FACS; John S. Roth, MD, FACS; and Jan Nagle, MS, RPh 52 The American College of Surgeons (ACS)
Case Report. XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect.
 Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA
 FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
Kenneth C. Shestak, M.D., Howard J. D. Edington, M.D., and Ronald R. Johnson, M.D.
 CME The Separation of Anatomic Components Technique for the Reconstruction of Massive Midline Abdominal Wall Defects: Anatomy, Surgical Technique, Applications, and Limitations Revisited Kenneth C. Shestak,
CME The Separation of Anatomic Components Technique for the Reconstruction of Massive Midline Abdominal Wall Defects: Anatomy, Surgical Technique, Applications, and Limitations Revisited Kenneth C. Shestak,
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST
 (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST") CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST I have constructed this lecture based on publications by leading cardiothoracic American surgeons: Timothy
CORONARY ARTERY BYPASS GRAFTING (CABG) (Part 1) Mark Shikhman, MD, Ph.D., CSA Andrea Scott, CST I have constructed this lecture based on publications by leading cardiothoracic American surgeons: Timothy
Lecture 01 Internal surface of anterolateral abdominal wall. BY Dr Farooq Khan Aurakzai
 Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Borders of the Abdomen
 Abdominal wall Borders of the Abdomen Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below Borders Superior: Costal cartilages 7-12. Xiphoid process:
Abdominal wall Borders of the Abdomen Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below Borders Superior: Costal cartilages 7-12. Xiphoid process:
New 2010 CPT Codes (italic font represents a new or revised code/description)
") New 2010 CPT Codes (italic font represents a new or revised code/description) 14301 Adjacent tissue transfer or rearrangement, any area; defect 30.1 sq cm to 60.0 sq cm 14302 each additional 30.0 sq cm,
New 2010 CPT Codes (italic font represents a new or revised code/description) 14301 Adjacent tissue transfer or rearrangement, any area; defect 30.1 sq cm to 60.0 sq cm 14302 each additional 30.0 sq cm,
Breast Reconstruction. Westmead Breast Cancer Institute
 Breast Reconstruction Westmead Breast Cancer Institute What is breast reconstruction? Breast reconstruction is a surgical procedure that creates a shape on the chest wall following a mastectomy. Occasionally,
Breast Reconstruction Westmead Breast Cancer Institute What is breast reconstruction? Breast reconstruction is a surgical procedure that creates a shape on the chest wall following a mastectomy. Occasionally,
Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes
 DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
COMBINED ABDOMINAL FLAP FOR MAJOR HAND RECONSTRUCTION
 Int. J. Pharm. Med. & Bio. Sc. 2013 2014 Srinivas Somashekar et al., 2014 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 3, No. 1, January 2014 2014 IJPMBS. All Rights Reserved COMBINED ABDOMINAL FLAP
Int. J. Pharm. Med. & Bio. Sc. 2013 2014 Srinivas Somashekar et al., 2014 Research Paper ISSN 2278 5221 www.ijpmbs.com Vol. 3, No. 1, January 2014 2014 IJPMBS. All Rights Reserved COMBINED ABDOMINAL FLAP
The progress in microsurgical procedures has led
 Original Article Breast reconstruction with free anterolateral thigh flap Ranjit Raje, Ramesh Chepauk, Kanti Shetty, Rajendra Prasad J. S. Plastic & Reconstructive Services, Department of Surgical Oncology,
Original Article Breast reconstruction with free anterolateral thigh flap Ranjit Raje, Ramesh Chepauk, Kanti Shetty, Rajendra Prasad J. S. Plastic & Reconstructive Services, Department of Surgical Oncology,
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Reconstruction of axillary scar contractures retrospective study of 124 cases over 25 years
 British Journal of Plastic Surgery (2003), 56, 100 105 q 2003 The British Association of Plastic Surgeons. Published by Elsevier Science Ltd. All rights reserved. doi:10.1016/s0007-1226(03)00035-3 Reconstruction
British Journal of Plastic Surgery (2003), 56, 100 105 q 2003 The British Association of Plastic Surgeons. Published by Elsevier Science Ltd. All rights reserved. doi:10.1016/s0007-1226(03)00035-3 Reconstruction
Breast Restoration Surgery After a mastectomy
 UW MEDICINE PATIENT EDUCATION Breast Restoration Surgery After a mastectomy This handout explains the most common procedures that are used at University of Washington Medical Center (UWMC) to restore a
UW MEDICINE PATIENT EDUCATION Breast Restoration Surgery After a mastectomy This handout explains the most common procedures that are used at University of Washington Medical Center (UWMC) to restore a
JMSCR Vol 07 Issue 01 Page January 2019
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v7i1.36 Original Article A Study on the
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v7i1.36 Original Article A Study on the
Aesthetic and Functional Abdominal Wall Reconstruction After Multiple Bowel Perforations Secondary to Liposuction
 Aesthetic and Functional Abdominal Wall Reconstruction After Multiple Bowel Perforations Secondary to Liposuction Aesthetic Plastic Surgery ISSN 0364-216X Volume 35 Number 2 Aesth Plast Surg (2011) 35:274-277
Aesthetic and Functional Abdominal Wall Reconstruction After Multiple Bowel Perforations Secondary to Liposuction Aesthetic Plastic Surgery ISSN 0364-216X Volume 35 Number 2 Aesth Plast Surg (2011) 35:274-277
CT of the Abdominal Wall
 1207 CT of the Abdominal Wall PhilipGoodma& 2 and Bharat Raval1 CT is an excellent method for evaluating the abdominal wall. Various abnormalities including hernia, hematoma, abscess, tumor, and neuromuscular
1207 CT of the Abdominal Wall PhilipGoodma& 2 and Bharat Raval1 CT is an excellent method for evaluating the abdominal wall. Various abnormalities including hernia, hematoma, abscess, tumor, and neuromuscular
The lateral incisional hernia: anatomical considerations for a standardized retromuscular sublay repair
 Hernia (2009) 13:293 297 DOI 10.1007/s10029-009-0479-0 ORIGINAL ARTICLE The lateral incisional hernia: anatomical considerations for a standardized retromuscular sublay repair M. Stumpf J. Conze A. Prescher
Hernia (2009) 13:293 297 DOI 10.1007/s10029-009-0479-0 ORIGINAL ARTICLE The lateral incisional hernia: anatomical considerations for a standardized retromuscular sublay repair M. Stumpf J. Conze A. Prescher
Role of free tissue transfer in management of chronic venous ulcer
 Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
BREAST RECONSTRUCTION POST MASTECTOMY
 UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...
Gross Anatomy ABDOMEN/SESSION 1 Dr. Firas M. Ghazi
 Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Scapular & Parascapular flap FLAP TERRITORY ANATOMY. is normally accompanied by two venae comitantes.
 Scapular & Parascapular flap FLAP TERRITORY This is a composite flap that is situated over the scapula with various incisional arrangements. It can be harvested as a skin and subcutaneous tissue flap,
Scapular & Parascapular flap FLAP TERRITORY This is a composite flap that is situated over the scapula with various incisional arrangements. It can be harvested as a skin and subcutaneous tissue flap,
Interesting Case Series. Fournier s Gangrene and the Reconstructive Challenges for the Plastic Surgeon
 Interesting Case Series Fournier s Gangrene and the Reconstructive Challenges for the Plastic Surgeon David Izadi, MB, BChir, MA(Oxon), MA(Cantab), MRCS, James Coelho, BMBS, MSc, MRCS, Sameer Gurjal, MBBCh,
Interesting Case Series Fournier s Gangrene and the Reconstructive Challenges for the Plastic Surgeon David Izadi, MB, BChir, MA(Oxon), MA(Cantab), MRCS, James Coelho, BMBS, MSc, MRCS, Sameer Gurjal, MBBCh,
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Thoracoplasty for the Management of Postpneumonectomy Empyema
 ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 9 Number 2 Thoracoplasty for the Management of Postpneumonectomy Empyema S Mullangi, G Diaz-Fuentes, S Khaneja Citation S Mullangi,
ISPUB.COM The Internet Journal of Thoracic and Cardiovascular Surgery Volume 9 Number 2 Thoracoplasty for the Management of Postpneumonectomy Empyema S Mullangi, G Diaz-Fuentes, S Khaneja Citation S Mullangi,
Breast Reconstruction Surgery
 Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
Aesthetic surgery techniques after excision of dermatofibrosarcoma protuberans: a case report
 British Journal of Plastic Surgery (2005) 58, 556 560 CASE REPORT Aesthetic surgery techniques after excision of dermatofibrosarcoma protuberans: a case report G. Dagregorio a, *, V. Darsonval b a Department
British Journal of Plastic Surgery (2005) 58, 556 560 CASE REPORT Aesthetic surgery techniques after excision of dermatofibrosarcoma protuberans: a case report G. Dagregorio a, *, V. Darsonval b a Department
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
musculoskeletal system anatomy nerves of the lower limb 1 done by: dina sawadha & mohammad abukabeer What is the importance of plexuses? plexuses provides us the advantage of a phenomenon called convergence
2013 MCT CPC-H Quiz #8 Chapters 13 and 14
 2013 MCT CPC-H Quiz #8 Chapters 13 and 14 Name: Date: Instructor: Score: 1. A female patient presents to the outpatient clinic for excision of a 4.8 cm malignant melanoma of the left inner thigh. A 6 cm
2013 MCT CPC-H Quiz #8 Chapters 13 and 14 Name: Date: Instructor: Score: 1. A female patient presents to the outpatient clinic for excision of a 4.8 cm malignant melanoma of the left inner thigh. A 6 cm
Medical Journal of the Volume 20 Islamic Republic of Iran Number 3 Fall 1385 November Original Articles
 Medical Journal of the Volume 0 Islamic Republic of Iran Number 3 Fall 38 November 00 Original Articles ANATOMY OF THE SUPERFICIAL INFERIOR EPIGASTRIC ARTERY FLAP MAHDI FATHI, M.D., EBRAHIM HATAMIPOUR,
Medical Journal of the Volume 0 Islamic Republic of Iran Number 3 Fall 38 November 00 Original Articles ANATOMY OF THE SUPERFICIAL INFERIOR EPIGASTRIC ARTERY FLAP MAHDI FATHI, M.D., EBRAHIM HATAMIPOUR,
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT. Dr Farooq Khan Aurakzai. Dated:
 Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD
 STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP
 INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify
INFORMED CONSENT-BREAST RECONSTRUCTION WITH TRAM ABDOMINAL MUSCLE FLAP 2000 American Society of Plastic Surgeons. Purchasers of the Patient Consultation Resource Book are given a limited license to modify
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Anatomical Study of Pectoral Nerves and its Implications in Surgery
 DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction
 Version History Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction Version Summary of change Date Issued 2.0 Endorsed by the Governance Committee 20.02.08 2.1 Circulated
Version History Guideline for the Management of Patients Suitable for Immediate Breast Reconstruction Version Summary of change Date Issued 2.0 Endorsed by the Governance Committee 20.02.08 2.1 Circulated
Medical Policy Original Effective Date: Revised Date: Page 1 of 8
 Page 1 of 8 Disclaimer Description Coverage Determination Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans, or the plan
Page 1 of 8 Disclaimer Description Coverage Determination Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans, or the plan
Reconstruction of the Chest Wall
 HOW TO DO IT Reconstruction of the Chest Wall Reed 0. Dingman, M.D., and Louis C. Argenta, M.D. ABSTRACT Reconstruction of the chest wall can now be accomplished reliably and expeditiously. Past experience
HOW TO DO IT Reconstruction of the Chest Wall Reed 0. Dingman, M.D., and Louis C. Argenta, M.D. ABSTRACT Reconstruction of the chest wall can now be accomplished reliably and expeditiously. Past experience
The use of peritoneal flaps in the repair of large incisional hernia
 The use of peritoneal flaps in the repair of large incisional hernia Marc Huyghe MD GZA St Augustinus Hospital (Antwerp) Mesh 2017 - Paris Peritoneal flap in the repair of incisional hernia - definition
The use of peritoneal flaps in the repair of large incisional hernia Marc Huyghe MD GZA St Augustinus Hospital (Antwerp) Mesh 2017 - Paris Peritoneal flap in the repair of incisional hernia - definition
Achieving ideal donor site aesthetics with autologous breast reconstruction
 Review Article Achieving ideal donor site aesthetics with autologous breast reconstruction Maurice Y. Nahabedian Department of Plastic Surgery, Georgetown University, Washington, DC 20007, USA Correspondence
Review Article Achieving ideal donor site aesthetics with autologous breast reconstruction Maurice Y. Nahabedian Department of Plastic Surgery, Georgetown University, Washington, DC 20007, USA Correspondence
GI anatomy Lecture: 2 د. عصام طارق
 GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
BREAST RECONSTRUCTION POST MASTECTOMY
 UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
Research Article Immediate versus Delayed Sarcoma Reconstruction: Impact on Outcomes
 Sarcoma Volume 2016, Article ID 7972318, 5 pages http://dx.doi.org/10.1155/2016/7972318 Research Article Immediate versus Delayed Sarcoma Reconstruction: Impact on Outcomes Kyle J. Sanniec, 1 Cristine
Sarcoma Volume 2016, Article ID 7972318, 5 pages http://dx.doi.org/10.1155/2016/7972318 Research Article Immediate versus Delayed Sarcoma Reconstruction: Impact on Outcomes Kyle J. Sanniec, 1 Cristine
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Intercostal Muscles LO4
 Intercostal Muscles LO4 4 List the structures, from superficial to deep, in an intercostal space. Describe their relationships to each other, to the associated neurovascular bundle and to the pleural cavity.
Intercostal Muscles LO4 4 List the structures, from superficial to deep, in an intercostal space. Describe their relationships to each other, to the associated neurovascular bundle and to the pleural cavity.
THE THORACIC WALL. Boundaries Posteriorly by the thoracic part of the vertebral column. Anteriorly by the sternum and costal cartilages
 THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces Superiorly by the suprapleural
THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces Superiorly by the suprapleural
Chapter 1: Introduction to the Human Body Test Bank
 Chapter 1: Introduction to the Human Body Test Bank MULTIPLE CHOICE 1. What is the branch of science that studies how the body functions? a. Anatomy b. Histology c. Pathology d. Physiology 2. Which word
Chapter 1: Introduction to the Human Body Test Bank MULTIPLE CHOICE 1. What is the branch of science that studies how the body functions? a. Anatomy b. Histology c. Pathology d. Physiology 2. Which word
Current Strategies in Breast Reconstruction
 Current Strategies in Breast Reconstruction Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery 12 th Annual School of
Current Strategies in Breast Reconstruction Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery 12 th Annual School of
Case Report The Reverse Latissimus Dorsi Flap for Large Lower Lumbar Defect
 Case Reports in Surgery Volume 2012, Article ID 964625, 5 pages doi:10.1155/2012/964625 Case Report The Reverse Latissimus Dorsi Flap for Large Lower Lumbar Defect Bouraoui Kotti, Olfa Jaidane, Jamel Ben
Case Reports in Surgery Volume 2012, Article ID 964625, 5 pages doi:10.1155/2012/964625 Case Report The Reverse Latissimus Dorsi Flap for Large Lower Lumbar Defect Bouraoui Kotti, Olfa Jaidane, Jamel Ben
Breast Reconstruction: Current Strategies and Future Opportunities
 Breast Reconstruction: Current Strategies and Future Opportunities Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery
Breast Reconstruction: Current Strategies and Future Opportunities Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery
The free thoracodorsal artery perforator flap in head and neck reconstruction
 European Annals of Otorhinolaryngology, Head and Neck diseases (2012) 129, 167 171 Available online at www.sciencedirect.com TECHNICAL NOTE The free thoracodorsal artery perforator flap in head and neck
European Annals of Otorhinolaryngology, Head and Neck diseases (2012) 129, 167 171 Available online at www.sciencedirect.com TECHNICAL NOTE The free thoracodorsal artery perforator flap in head and neck
Procedure Information Guide
 Procedure Information Guide Breast reconstruction with abdominal tissue flap Brought to you in association with EIDO and endorsed by the The Royal College of Surgeons of England Discovery has made every
Procedure Information Guide Breast reconstruction with abdominal tissue flap Brought to you in association with EIDO and endorsed by the The Royal College of Surgeons of England Discovery has made every
Chapter 3 - Anatomical considerations for surgery of the anterolateral abdominal wall
 Chapter 3 - Anatomical considerations for surgery of the anterolateral abdominal wall H.J.A.A. van Geffen R.K.J. Simmermacher K. Bosscha Chr. van der Werken B. Hillen Published in: Hernia (2004) 8:93-97
Chapter 3 - Anatomical considerations for surgery of the anterolateral abdominal wall H.J.A.A. van Geffen R.K.J. Simmermacher K. Bosscha Chr. van der Werken B. Hillen Published in: Hernia (2004) 8:93-97
Cost-utility analysis comparing free and pedicled TRAM flap for breast reconstruction Thoma A, Khuthaila D, Rockwell G, Veltri K
 Cost-utility analysis comparing free and pedicled TRAM flap for breast reconstruction Thoma A, Khuthaila D, Rockwell G, Veltri K Record Status This is a critical abstract of an economic evaluation that
Cost-utility analysis comparing free and pedicled TRAM flap for breast reconstruction Thoma A, Khuthaila D, Rockwell G, Veltri K Record Status This is a critical abstract of an economic evaluation that
REINFORCED BIOSCAFFOLDS
 REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
REINFORCED BIOSCAFFOLDS Midline Incisional Open OviTex 1S Resorbable Clinical Case Study: Open Abdomen Incisional Herniorrhaphy in Contaminated (CDC Class IV) Operative Field Performed by Dr. Michael Sawyer,
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Selected Operative Procedure Categories for KNHSS SSI Surveillance
 Selected Operative Procedure Categories for KNHSS SSI Surveillance Breast Surgery Excision of lesion or tissue of breast including radical, modified, or quadrant resection, lumpectomy, incisional biopsy,
Selected Operative Procedure Categories for KNHSS SSI Surveillance Breast Surgery Excision of lesion or tissue of breast including radical, modified, or quadrant resection, lumpectomy, incisional biopsy,
Breast debridement and closure cpt
 Breast debridement and closure cpt Close Breast debridement cpt code Medicare Billing Guidelines, Medicare payment and reimbursment, Medicare codes. Here is a list of CPT codes and Diagnoses that are.
Breast debridement and closure cpt Close Breast debridement cpt code Medicare Billing Guidelines, Medicare payment and reimbursment, Medicare codes. Here is a list of CPT codes and Diagnoses that are.
Pedicled Fillet of Leg Flap for Extensive Pressure Sore Coverage
 Pedicled Fillet of Leg Flap for Extensive Pressure Sore Coverage Shareef Jandali, MD, and David W. Low, MD Division of Plastic Surgery, University of Pennsylvania Health System, Philadelphia Correspondence:
Pedicled Fillet of Leg Flap for Extensive Pressure Sore Coverage Shareef Jandali, MD, and David W. Low, MD Division of Plastic Surgery, University of Pennsylvania Health System, Philadelphia Correspondence:
NBME Anatomy Review. Sylvia Nelsen, Ph.D. March 19, 2015
 NBME Anatomy Review Sylvia Nelsen, Ph.D. March 19, 2015 UPPER & LOWER LIMBS 1. What is the most likely diagnosis in this case? A. Rotator cuff tendinitis: pain w/o weakness B. Adhesive capsulitis: absolute
NBME Anatomy Review Sylvia Nelsen, Ph.D. March 19, 2015 UPPER & LOWER LIMBS 1. What is the most likely diagnosis in this case? A. Rotator cuff tendinitis: pain w/o weakness B. Adhesive capsulitis: absolute
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
The bi-pedicle post-auricular tube flap for reconstruction of partial ear defects
 The British Association of Plastic Surgeons (2003) 56, 593 598 The bi-pedicle post-auricular tube flap for reconstruction of partial ear defects Mohammed G. Ellabban*, Maamoun I. Maamoun, Moustafa Elsharkawi
The British Association of Plastic Surgeons (2003) 56, 593 598 The bi-pedicle post-auricular tube flap for reconstruction of partial ear defects Mohammed G. Ellabban*, Maamoun I. Maamoun, Moustafa Elsharkawi
Knee Disarticulation Amputation
 Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle
Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle