When Back Pain is More than Just a Pain in the Back
|
|
|
- Gwendolyn Williamson
- 5 years ago
- Views:
Transcription

1 When Back Pain is More than Just a Pain in the Back Spinal Infections Shakeel A. Chowdhry MD FAANS FAHA Clinical Assistant Professor Division of Neurosurgery University of Chicago Pritzker School of Medicine NorthShore University HealthSystem Department of Neurosurgery
2 None Disclosures
3 Overview Anatomy and pathophysiology Common Organisms Presentation Diagnostic Workup Differential Diagnoses Management Outcomes (not necessarily in this order)

, multifidus,")
4 Bone Joints Posterior Elements» Spinous Process, Lamina, Facet Pedicle Vertebral Body Intervertebral Disk Facet Ligaments» Nucleus Pulposus» Annulus ALL, PLL, Ligamentum Flavum, Interspinous Ligament Muscle Quadratus lumborum, erector spinae (illiocostalis, spinalis, logissimus), multifidus, iliopsoas


5 Anatomy of Disease Discitis Osteomyelitis / Spondylitis Epidural Abscess Subdural Empyema Spinal Cord Abscess Reihsaus, E., H. Waldbaur and Walter Seeling. Spinal epidural abscess: a meta-analysis of 915 patients. Neurosurgical Review 23 (2000):
6 Routes of Entry Hematogenous Spread Direct Innoculation 6
7 Brief History Epidural Abscess 1761: Morgangi alludes to pyogenic infection of spinal epidural space 1820: first description, Bergasmaschi 1901: first successful drainage, Barth Walter Dandy reported mortality rate of 83% with spinal epidural abscess

8 Diagnosis can be difficult
9 Why does it Matter? Time will allow clear determination Risks of Waiting Pain Progression of Infection Spinal Instability Neurologic Deficit


10
11 According to court records, the patient was admitted to the emergency room after suffering from back pain in Dr. Sarah Barbour, a specialist in infectious diseases, was tapped to manage the patient s care, but, according to the medical malpractice lawsuit, Barbour failed to notice that the woman s back pain was being caused by an infection that had reached her central nervous system. The infection, court documents say, ate into the woman s thoracic spine, leaving her permanently disabled. The plaintiff was released from the hospital, with a discharge diagnosis of paralysis, 12 days after being admitted. She is confined to a wheelchair, her attorneys say, and still has no functional use of her legs. $18 million in compensation (Georgia). The jury verdict, rendered in Chatham County State Court, assessed millions in dollars of damages against a Savannah hospital, a physician specializing in infectious diseases and Southcoast Medical Group, the doctor s former employer. Dr. Sarah Barbour, along with her former employer, Southcoast Medical Group, have been ordered to pay $16.2 million in damages for their share in the liability. An additional $1.8 million has been assessed against St. Joseph s / Candler, a medical consortium that owns the hospital. 2016, New York: $2,000,000 Verdict. A 39-year old male with cerebral palsy goes to Hudson Valley Hospital with back pain. He is diagnosed with a back strain and is then discharged. Four days later, he returns with rib pain, back pain, and shortness of breath, just to be diagnosed again with a back strain. He returns the next day again, with tingling and numbness in his legs. He is admitted for pneumonia. It takes three days for him to be diagnosed with an epidural abscess with marked compression of his spinal cord. He alleges that the staff was negligent in failing to heed the signs of an epidural abscess and failing to timely diagnose the abscess. The defendants deny liability, and argue he was not experiencing symptoms of a spinal cord abscess during his first two emergency room visits, and that once his condition worsened the proper tests were done and the abscess was diagnosed. Plaintiff argues he suffers urinary incontinence and further damage to his spinal cord requiring future surgeries as a result. A jury awards the plaintiff $2,000, , Pennsylvania: $12,500,000 Verdict. A 53-year old man goes to the ER with neck pain and tingling in his left arm. He is admitted to the hospital. His condition worsens as he develops a fever, urinary issues, and has trouble walking. The day after his admission, he is examined by the infectious disease specialists, who suspects an epidural abscess on his spine and orders an MRI. This is interpreted by the defendant radiologist as normal, without showing an abscess or fluid collection in the plaintiff's spine. The infectious disease specialist continues to have concerns about a cervical abscess and transfers him to a different hospital where surgery is done the next day. Plaintiff argues the delay of over 24 hours in surgical intervention allowed his abscess to put pressure on his spinal cord, leaving him permanently paralyzed in his arms and legs. The defendants argue that his condition was evaluated properly and that the radiologist stated the abscess was not visible on the MRI. A jury finds the radiologist and neurologist negligent, and awards the man $12,500,000, which includes $500,000 to his wife for loss of consortium. 2014, Florida: $19,250,000 Verdict. A 36-year old woman goes to the ER complaining of an infected cyst on the back of her right shoulder. It is drained and treated, and the plaintiff is discharged with antibiotics. She returns two days later, with the same complaints. The wound is repacked by another physician. A day after this she goes to a medical clinic, and is told to go back to the ER for repacking of her wound and a surgical consult. She does this, and the wound is repacked, and a surgeon instructs her to come back for another appointment in two weeks. However, before the two weeks is over, she goes back to the ER with severe radiating chest pain. She is discharged. Two days later, she returns again with the same complaints of severe radiating chest pain, and she is discharged with medicine after a pulmonary embolism is ruled out, but no CT or MRI is done. She returns the same evening again and is admitted. Paralysis begins to set in. It is then discovered that she has a spinal epidural abscess originating from the infected cyst on her shoulder three weeks earlier. Surgery is done in an attempt to relieve the pressure on her spinal cord caused by the abscess, but she ultimately suffers permanent paralysis below the waist. She argues that the delay in treatment and admission to the hospital led to a delay in diagnosing and treating her spinal abscess, causing her paralysis. The plaintiff is awarded gross damages of $19,250,000, and her net award was $8,000,000. The parties settled while post-trial motions were pending.
12 According to court records, the patient was admitted to the emergency room after suffering from back pain in Dr. Sarah Barbour, a specialist in infectious diseases, was tapped to manage the patient s care, but, according to the medical malpractice lawsuit, Barbour failed to notice that the woman s back pain was being caused by an infection that had reached her central nervous system. The infection, court documents say, ate into the woman s thoracic spine, leaving her permanently disabled. The plaintiff was released from the hospital, with a discharge diagnosis of paralysis, 12 days after being admitted. She is confined to a wheelchair, her attorneys say, and still has no functional use of her legs. $18 Million In Compensation, Georgia The jury verdict, rendered in Chatham County State Court, assessed millions in dollars of damages against a Savannah hospital, a physician specializing in infectious diseases and Southcoast Medical Group, the doctor s former employer. Dr. Sarah Barbour, along with her former employer, Southcoast Medical Group, have been ordered to pay $16.2 million in damages for their share in the liability. An additional $1.8 million has been assessed against St. Joseph s / Candler, a medical consortium that owns the hospital. 2016, New York: $2,000,000 Verdict. A 39-year old male with cerebral palsy goes to Hudson Valley Hospital with back pain. He is diagnosed with a back strain and is then discharged. Four days later, he returns with rib pain, back pain, and shortness of breath, just to be diagnosed again with a back strain. He returns the next day again, with tingling and numbness in his legs. He is admitted for pneumonia. It takes three days for him to be diagnosed with an epidural abscess with marked compression of his spinal cord. He alleges that the staff was negligent in failing to heed the signs of an epidural abscess and failing to timely diagnose the abscess. The defendants deny liability, and argue he was not experiencing symptoms of a spinal cord abscess during his first two emergency room visits, and that once his condition worsened the proper tests were done and the abscess was diagnosed. Plaintiff argues he suffers urinary incontinence and further damage to his spinal cord requiring future surgeries as a result. A jury awards the plaintiff $2,000, , Pennsylvania: $12,500,000 Verdict. A 53-year old man goes to the ER with neck pain and tingling in his left arm. He is admitted to the hospital. His condition worsens as he develops a fever, urinary issues, and has trouble walking. The day after his admission, he is examined by the infectious disease specialists, who suspects an epidural abscess on his spine and orders an MRI. This is interpreted by the defendant radiologist as normal, without showing an abscess or fluid collection in the plaintiff's spine. The infectious disease specialist continues to have concerns about a cervical abscess and transfers him to a different hospital where surgery is done the next day. Plaintiff argues the delay of over 24 hours in surgical intervention allowed his abscess to put pressure on his spinal cord, leaving him permanently paralyzed in his arms and legs. The defendants argue that his condition was evaluated properly and that the radiologist stated the abscess was not visible on the MRI. A jury finds the radiologist and neurologist negligent, and awards the man $12,500,000, which includes $500,000 to his wife for loss of consortium. 2014, Florida: $19,250,000 Verdict. A 36-year old woman goes to the ER complaining of an infected cyst on the back of her right shoulder. It is drained and treated, and the plaintiff is discharged with antibiotics. She returns two days later, with the same complaints. The wound is repacked by another physician. A day after this she goes to a medical clinic, and is told to go back to the ER for repacking of her wound and a surgical consult. She does this, and the wound is repacked, and a surgeon instructs her to come back for another appointment in two weeks. However, before the two weeks is over, she goes back to the ER with severe radiating chest pain. She is discharged. Two days later, she returns again with the same complaints of severe radiating chest pain, and she is discharged with medicine after a pulmonary embolism is ruled out, but no CT or MRI is done. She returns the same evening again and is admitted. Paralysis begins to set in. It is then discovered that she has a spinal epidural abscess originating from the infected cyst on her shoulder three weeks earlier. Surgery is done in an attempt to relieve the pressure on her spinal cord caused by the abscess, but she ultimately suffers permanent paralysis below the waist. She argues that the delay in treatment and admission to the hospital led to a delay in diagnosing and treating her spinal abscess, causing her paralysis. The plaintiff is awarded gross damages of $19,250,000, and her net award was $8,000,000. The parties settled while post-trial motions were pending.
13 Assessment of malpractice claims due to spinal epidural abscess J. Mason DePasse, MD, Roy Ruttiman, BS, Adam E. M. Eltorai, MS, Mark A. Palumbo, MD, and Alan H. Daniels, MD Division of Spine Surgery, Department of Orthopaedics, Warren Alpert Medical School of Brown University, Providence, Rhode Island OBJECTIVE Spinal epidural abscesses (SEAs) can be difficult to diagnose and may result in neurological compromise or even death. Delays in diagnosis or treatment may worsen the prognosis. While SEA presents a high risk for litigation, little is known about the medicolegal rami cations of this condition. An enhanced understanding of potential legal impli- cations is important for practicing spine surgeons, emergency medicine physicians, and internists. METHODS The VerdictSearch database, a large legal-claims database, was queried for epidural abscess related legal cases. Demographic and clinical data were examined for all claims; any irrelevant cases or cases with incomplete information were excluded. The effects of age of the plaintiff, sex of the plaintiff, presence of a known infection, resulting paraplegia or quadriplegia, delay in diagnosis, and delay in treatment on the proportion of plaintiff rulings and size of payments were assessed. RESULTS In total, 56 cases met the inclusion criteria. Of the 56 cases, 17 (30.4%) were settled, 22 (39.3%) resulted in a defendant ruling, and 17 (30.4%) resulted in a plaintiff ruling. The mean award for plaintiff rulings was $5,277,468 ± $6,348,462 (range $185,000 $19,792,000), which was significantly larger than the mean award for cases that were settled out of court, $1,914,265 ± $1,313,322 (range $100,000 $4,500,000) (p < 0.05). The mean age of the plaintiffs was 47.0 ± 14.4 years; 23 (41.1%) of the plaintiffs were female and 33 (58.9%) were male. The proportion of plaintiff verdicts and size of monetary awards were not affected by age or sex (p > 0.49). The presence of a previously known infection was also not associated with the proportion of plaintiff verdicts or indemnity payments (p > 0.29). In contrast, juries were more likely to rule in favor of plaintiffs who became paraplegic or quadriplegic (p = 0.03) compared with plaintiffs who suffered pain or isolated weakness. Monetary awards for paraplegic or quadriplegic patients were also signficantly higher (p = 0.003). Plaintiffs were more likely to win if there was a delay in diagnosis (p = 0.04) or delay in treatment (p = 0.006), although there was no difference in monetary awards (p > 0.57). Internists were the most commonly sued physician (named in 13 suits [23.2%]), followed by emergency medicine physicians (named in 8 [14.3%]), and orthopedic surgeons (named in 3 [5.4%]). CONCLUSIONS This investigation is the largest examination of legal claims due to spinal epidural abscess to date. The proportion of plaintiff verdicts was signi cantly higher in cases in which the patient became paraplegic or quadriplegic and in cases in which there was delay in diagnosis or treatment. Additionally, paralysis is linked to large sums awarded to the plaintiff. Nonsurgeon physicians, who are often responsible for initial diagnosis, were more likely to be sued than were surgeons.
14 Assessment of malpractice claims due to spinal epidural abscess J. Mason DePasse, MD, Roy Ruttiman, BS, Adam E. M. Eltorai, MS, Mark A. Palumbo, MD, and Alan H. Daniels, MD Division of Spine Surgery, Department of Orthopaedics, Warren Alpert Medical School of Brown University, Providence, Rhode Island OBJECTIVE Spinal epidural abscesses (SEAs) can be difficult to diagnose and may result in neurological compromise or even death. Delays in diagnosis or treatment may worsen the prognosis. While SEA presents a high risk for litigation, little is known about the medicolegal rami cations of this condition. An enhanced understanding of potential legal impli- cations is important for practicing spine surgeons, emergency medicine physicians, and internists. METHODS The VerdictSearch database, a large legal-claims database, was queried for epidural abscess related legal cases. Demographic and clinical data were examined for all claims; any irrelevant cases or cases with incomplete information were excluded. The effects of age of the plaintiff, sex of the plaintiff, presence of a known infection, resulting paraplegia or quadriplegia, delay in diagnosis, and delay in treatment on the proportion of plaintiff rulings and size of payments were assessed. RESULTS In total, 56 cases met the inclusion criteria. Of the 56 cases, 17 (30.4%) were settled, 22 (39.3%) resulted in a defendant ruling, and 17 (30.4%) resulted in a plaintiff ruling. The mean award for plaintiff rulings was $5,277,468 ± $6,348,462 (range $185,000 $19,792,000), which was significantly larger than the mean award for cases that were settled out of court, $1,914,265 ± $1,313,322 (range $100,000 $4,500,000) (p < 0.05). The mean age of the plaintiffs was 47.0 ± 14.4 years; 23 (41.1%) of the plaintiffs were female and 33 (58.9%) were male. The proportion of plaintiff verdicts and size of monetary awards were not affected by age or sex (p > 0.49). The presence of a previously known infection was also not associated with the proportion of plaintiff verdicts or indemnity payments (p > 0.29). In contrast, juries were more likely to rule in favor of plaintiffs who became paraplegic or quadriplegic (p = 0.03) compared with plaintiffs who suffered pain or isolated weakness. Monetary awards for paraplegic or quadriplegic patients were also signficantly higher (p = 0.003). Plaintiffs were more likely to win if there was a delay in diagnosis (p = 0.04) or delay in treatment (p = 0.006), although there was no difference in monetary awards (p > 0.57). Internists were the most commonly sued physician (named in 13 suits [23.2%]), followed by emergency medicine physicians (named in 8 [14.3%]), and orthopedic surgeons (named in 3 [5.4%]). CONCLUSIONS This investigation is the largest examination of legal claims due to spinal epidural abscess to date. The proportion of plaintiff verdicts was signi cantly higher in cases in which the patient became paraplegic or quadriplegic and in cases in which there was delay in diagnosis or treatment. Additionally, paralysis is linked to large sums awarded to the plaintiff. Nonsurgeon physicians, who are often responsible for initial diagnosis, were more likely to be sued than were surgeons.
15 Source of Infection In 14 cases (25%), the plaintiff had a known source of infection prior to diagnosis of SEA, such as remote Staphylococcus skin infection, pneumonia, or known bacteremia. When compared with the 25 cases (44.6%) with no known infection or other risk factors, there was no difference in proportion of settlements, proportion of plaintiff verdicts, or indemnity payments (p > 0.29).
16 Risk factors Briefly IV drug use Immunosuppressed AIDS, chronic steroids, EtOH abuse Open wounds / Trauma Systemic/hematologic infections Chronic Infections Hardware- Joints/Valve Prior Spinal Surgery Poorly controlled DM
17 Exam Findings Back pain Meningismus occasionally Fever Neurologic signs Radicular pain Bowel/bladder symptoms Weakness
18 Evaluation Vitals Labs WBC ESR/CRP/ Procalcitonin Imaging Plain films Nuclear Medicine studies Computed Tomography Magnetic Resonance Imaging» CT myelo not recommended Fever generally present with hematogenous spread as underlying cause May be rare in chronic cases Leukocytosis also may not be present High clinical suspicion MRI with gadolinium

19 Imaging Regis W. Haid, Howard H. Kaufman, Sydney S. Schochet, Gary D. Marano; Epidural Lipomatosis Simulating an Epidural Abscess: Case Report and Literature Review, Neurosurgery, Volume 21, Issue 5, 1 November 1987, Pages ,
20 Categories of Spinal Infections (Iliopsoas muscle abscess) Discitis Osteomyelitis / Spondylitis Spinal epidural abscess Subdural Empyema Spinal Cord Infection
21 Psoas abscess Iliopsoas muscle (Psoas and iliacus) 30% have a psoas minor as well anterior to psoas T12-L5 ventral to spine Primary hip flexor Assess iliopsoas inflammation» Active: flex hip against resistance» Passive: lay unaffected side down and hyperextend affected side Mortality rate 2.4% (primary infection), 19% (secondary infection sepsis usual cause of death
22 Discitis Inflammation of the disk space Enters from the cartilaginous endplate Spontaneous Post-Op Juvenile discitis H. Flu most often Primordial feeding arteries are implicated (involute in 20s) Back pain Often focal Exacerbated by movement May radiate Paravertebral muscle spasms Up to 70% are afebrile Unlikely to cause radicular sx s or meningismus
23 CBC, Inflamm markers Blood cx Percutaneous Biopsy Aerobic, Anerobic, fungal, mycobacterium Open surgery for biopsy when dx unclear infection persists
 CT Endplate fragmentation Paravertebral soft tissue swelling w/ obliteration of fat planes Paravertebral abscess All 3 then discitis very")
24 Imaging PF of low use Sclerosis usually takes 4-12 weeks Late finding: widening of disk space and erosion into VB Nuc medicine May miss TB (Pott s disease) CT Endplate fragmentation Paravertebral soft tissue swelling w/ obliteration of fat planes Paravertebral abscess All 3 then discitis very likely
25 Pathogens Staph aureus most common Strep albus, Strep epidermidis Gram (-)» E Coli» Proteus spp Abx Treat for 6 wks IV then PO OR Treat IV until inflammatory markers normalize (~4-6 weeks) then PO
26 Vertebral Osteomyelitis (VO) 2-4% of all cases of osteomyelitis 1:250,000 incidence Recently rising Increases with age 2:1 (male:female) Lumbar > thoracic > cervical > sacrum
27 Diagnosis Needle biopsy Surgical Indication Instability, kyphosis, cord compression Neurologic deficit Vast majority (>90%) do not require surgical intervention when detected early
28 Risk factors for VO IVDU Diabetes Mellitus Unusual bacterial infections, fungal (candida) Chronic Hemodialysis Osteo changes can occur without infection Immunosuppression AIDS Chronic Steroid Use EtOH Infective endocarditis Prior spinal surgery ESI/Myelogram Elderly
29 Clinical Localized pain (90%) Fever (52%) <spikes and chills rare> Weight loss Paraspinal muscle spasms WBC May be normal ESR/CRP elevated Only 17% will have neurologic symptoms
30 Spontaneous Sources UTI (most common), respiratory tract, soft tissue (skin boils, IVDU), dental flora 37% without identifiable source Route of spread Hemotagenous spondylodiscitis» Arterial» Spinal venous epidural plexus (Batson s plexus) Direct extension» Surgery, LP, trauma, local infection
31 Organisms for VO Staph aureus (>50%) E. Coli (distant 2 nd ) IVDU: Pseudomonas and S. aureus UTI: E. Coli and Proteus spp Respiratory Tract: Strep pneumoniae EtOH: Klebsiella pneumoniae Endocarditis Acute: S. Aureus Subacute: Streptococcus spp. Tuberculosis: Mycobacterium tuberculosis Rare Nocardia Polymicrobial (<2.5% of pyogenic infection) Mycobacterium avium complex in AIDS Abx minimum 6 weeks
32 Imaging Modality Sensitivity Specificity Accuracy Plain films 82% 57% 73% Bone Scan 90% 78% 86% Gallium Scan (radioactive tracer) 92% 100% 93% Bone Scan + Gallium Scan 90% 100% 94% MRI 96% 92% 94% Greenberg
33 Epidural Spinal Abscess (ESA) Incidence: per 10,000 hospital admissions / years old (average age) Most common location Thoracic (50%), Lumbar (35%), cervical (15%) 82% posterior to cord Often associated with vertebral osteomyelitis (VO) and discitis
34 Chronic dz with immune compromise in 60% (study of only 40 patients) DM 32% IVDU 18% CRF 12% EtOH abuse 10%
35 WBC Commonly elevated in acute period (16K) but normal in chronic (9K) ESR, CRP, Procalcitonin Cultures
36 Severe pain over spine Radicular symptoms, bowel/bladder dysfunction, weakness - rapidly progressive Mechanism Mechanical Compression Venous congestion/thrombophlebitis 3 days 4.5 days 24 hrs Back pain Root sx s Weakness Paraplegia/Tetraplegia
37 Surgical Indications Liquid abscess (vs phlegmon) Target sign Cord compression Lumbar spine does not carry risk of thrombophlebitis Greater tolerance to nonoperative management Nonoperative management of ESA requires very close vigilance

38 Radiographic Findings CT Destructive bony changes MRI Target sign

: e621.")
39 Radiographic Findings CT requires fair amount of bony involvement to reliably indicate infection Bodman A, Riordan M, Chin L S. (May 23, 2016) Delayed Presentation of a Cervical Spinal Epidural Abscess of Dental Origin after a Fall in an Elderly Patient. Cureus 8(5): e621. doi: /cureus.621

40 Source of Infection Hematogenous Skin infection» Furuncle(boil) found in only 15% Parenteral injections» IVDU Bacterial endocarditis UTI Resp infection Pharyngeal/Dental abscess Post Procedure Laminectomy (0.67%) ESI, LP, epidural catheter etc Direct Extension Decubitus Ulcer Psoas Abscess Trauma / Open wound Phayngeal Infection Mediastinitis Pyelonephritis w/ abscess Dermus sinus tract
41 Organisms Staph aureus (>50%) Aerobic and anaerobic streptococcus spp (2 nd most common Escherichia Coli Pseudomonas aeruginosa Diplococcus peumoniae Serratia maercescens Chronic Infections TB Fungal: cytptococcus, aspergillosis, brucellosis Parasitic: Echinococcus Multiple organisms ~10% Anaerobes ~8%
» Switch to PCN (nafcillin, rocephin) if MRSA ruled out Follow-up eval Abx success <radiographic, lab,")
42 Obtain specimen IR guided biopsy/drainage Surgical drainage» Abscess vs Phlegmon» Level» Extent of Compression» Instability Treatment Broad spectrum antibiotics Vancomycin + Flagyl + third generation Cephalosporin (cefepime when suspect pseudomonas)» Switch to PCN (nafcillin, rocephin) if MRSA ruled out Follow-up eval Abx success <radiographic, lab, exam>

43 DOI: /ojmn
44 Outcome Fatal in 4-31% Worse outcome for older and those paralyzed prior to surgery Severe neurologic deficits rarely improve Exception: Pott s disease Mortality due to original focus of infection or complication of residual paralysis (e.g. PE)
45 Differential Diagnosis Epidural hematoma Spinal Tumor Meningitis Transverse Myelitis Bone tumors can resemble VO Infection centers on disk space often Tumors often spare disk space

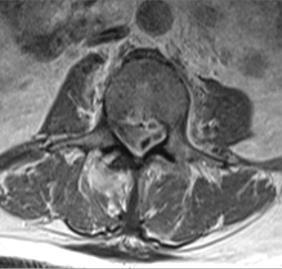
46 Cases Workup for PE Remote lumbar laminectomy with foot drop Obesity, DM, chronic focal back pain Afebrile



47 Source: ABSCESS Site: EPIDURAL Pseudomonas aeruginosa Cases


48
 osteomyelitis and diskitis")
 months later with continuing back pain")

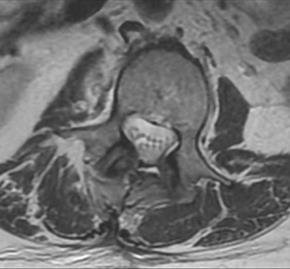
49 Case #2 49-year-old recurrent infections (bacteremia and sepsis) osteomyelitis and diskitis several months ago (left) and underwent right BKA. (right) months later with continuing back pain despite antibiotics. weakness involving his left leg recently had a drain placed in his psoas abscess. MRSA, pseudomonas

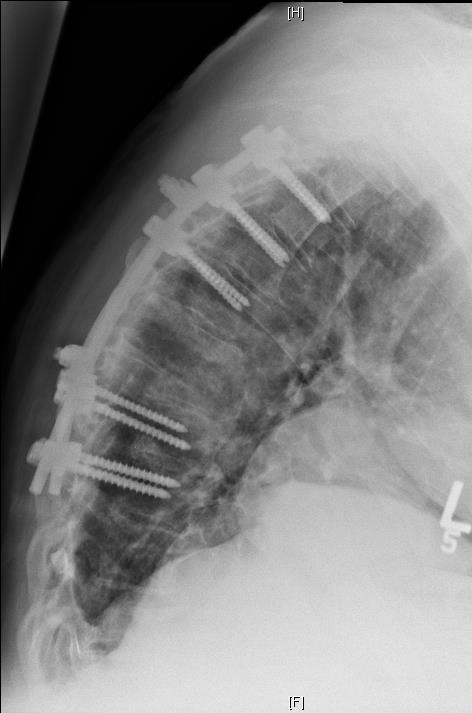
50 Case #3 Hx neurocystercosis s/p VPS 10 yrs ago Neck pain Gram + bacteremia Couldn t tolerate MRI d/t neck pain


51



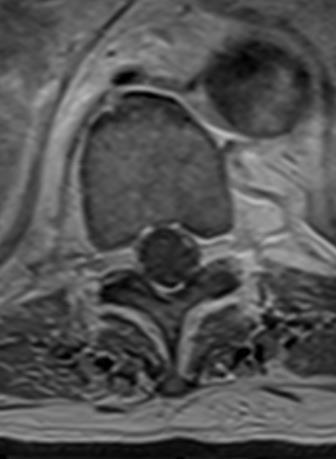
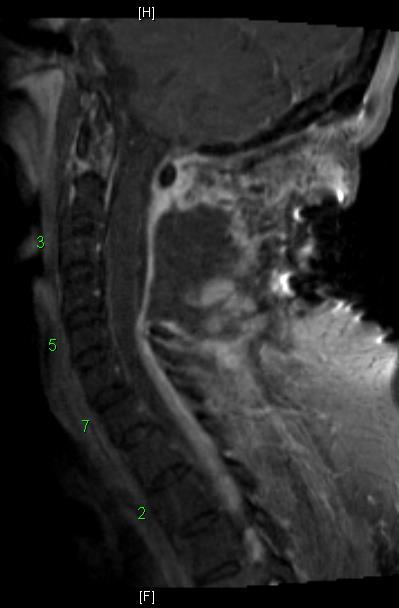
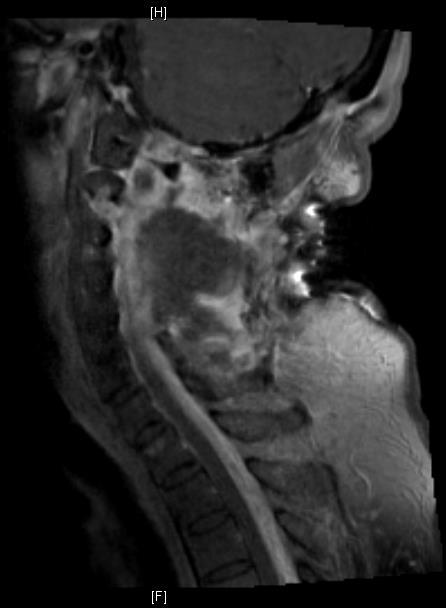
52 Case #4 80-year-old gentleman fevers and back pain no lower extremity weakness. Imaging: marked degenerative changes at L4-5 with stenosis and incompetence facets, appears to be chronic and longstanding. significant ventral epidural fluid extending from this area of stenosis up to the level of T12. CRP was elevated into the 200 range white count was also elevated febrile to 102 degrees.
53 Questions? Shakeel A. Chowdhry MD
Spinal epidural abscess (SEA) is an infection within. Assessment of malpractice claims due to spinal epidural abscess
 is an infection within. Assessment of malpractice claims due to spinal epidural abscess") CLINICAL ARTICLE J Neurosurg Spine 27:476 480, 2017 Assessment of malpractice claims due to spinal epidural abscess J. Mason DePasse, MD, Roy Ruttiman, BS, Adam E. M. Eltorai, MS, Mark A. Palumbo, MD,
CLINICAL ARTICLE J Neurosurg Spine 27:476 480, 2017 Assessment of malpractice claims due to spinal epidural abscess J. Mason DePasse, MD, Roy Ruttiman, BS, Adam E. M. Eltorai, MS, Mark A. Palumbo, MD,
Spinal infection. Outline ANATOMY 6/2/2017. Anatomy Pathogen
 Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
 www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
Ross JS, Brant-Zawadzki M, et al. Diagnostic Imaging: Spine 2004; V-1-5. Greenspan A. Orthopedic Radiology: A Practical Approach 1997; V-19-3
 MR Imaging of Spinal Infections 台大醫院 台大醫學院 影像醫學部 放射線科 許昭禹醫師 / 施庭芳主任 2009/02/14 Risk factors of spinal infections Advanced age > 50 Intravenous drug abuse Immunosuppression or immune deficiency Long-term
MR Imaging of Spinal Infections 台大醫院 台大醫學院 影像醫學部 放射線科 許昭禹醫師 / 施庭芳主任 2009/02/14 Risk factors of spinal infections Advanced age > 50 Intravenous drug abuse Immunosuppression or immune deficiency Long-term
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Emergency Neurological Life Support Spinal Cord Compression
 Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Emergency Neurological Life Support Spinal Cord Compression Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Spinal Cord Compression Table of Contents Emergency Neurological Life Support...
Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of the Knee
 Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
Medical malpractice litigation increasingly affects. Malpractice litigation following spine surgery
 CLINICAL ARTICLE J Neurosurg Spine 27:470 475, 2017 Malpractice litigation following spine surgery Alan H. Daniels, MD, 1 4 Roy Ruttiman, MS, 1,2 Adam E. M. Eltorai, MS, 1,2 J. Mason DePasse, MD, 1 3 Bielinsky
CLINICAL ARTICLE J Neurosurg Spine 27:470 475, 2017 Malpractice litigation following spine surgery Alan H. Daniels, MD, 1 4 Roy Ruttiman, MS, 1,2 Adam E. M. Eltorai, MS, 1,2 J. Mason DePasse, MD, 1 3 Bielinsky
Introduction to Neuroimaging spine. John J. McCormick MD
 Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
PSOAS ABSCESS. Dr Noman Ullah Wazir
 PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
Diagnostics of Spondylodiscitis and its most frequent complications
 Diagnostics of Spondylodiscitis and its most frequent complications Poster No.: C-1536 Congress: ECR 2017 Type: Educational Exhibit Authors: M. Veselova, V. Mazaev, M. Molodtsov; Moscow/RU Keywords: Musculoskeletal
Diagnostics of Spondylodiscitis and its most frequent complications Poster No.: C-1536 Congress: ECR 2017 Type: Educational Exhibit Authors: M. Veselova, V. Mazaev, M. Molodtsov; Moscow/RU Keywords: Musculoskeletal
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
Outline. Introduction / Epidemiology. Anatomy / Pain generators. Diagnosis. Treatment. Most Important lecture!!
 Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Vertebral and Paravertebral Diseases
 Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Department of Radiology University of California San Diego Vertebral and Paravertebral Diseases John R. Hesselink, M.D. Vertebral / Paravertebral Disease (Extradural) Metastatic disease Primary bone tumors
Moath Darweesh. Zaid Emad. Anas Abu -Humaidan
 3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
INFECTION & INFLAMMATION IMAGING
 INFECTION & INFLAMMATION IMAGING Radiopharmaceutical Drug Interactions & Other Interesting Case Studies MICHELLE RUNDIO, CNMT NCT MBA PCI NUCLEAR IN-111 WHITE BLOOD CELL IMAGING Interactions, Imaging Parameters
INFECTION & INFLAMMATION IMAGING Radiopharmaceutical Drug Interactions & Other Interesting Case Studies MICHELLE RUNDIO, CNMT NCT MBA PCI NUCLEAR IN-111 WHITE BLOOD CELL IMAGING Interactions, Imaging Parameters
SpineFAQs. Lumbar Spondylolisthesis
 SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
Thoracic and Lumbar Spine Anatomy.
 Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION
 CLINICAL VIGNETTE 2017; 3:2 SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION Editor-in-Chief: Idowu, Olufemi E. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria.
CLINICAL VIGNETTE 2017; 3:2 SPINAL MAGNETIC RESONANCE IMAGING INTERPRETATION Editor-in-Chief: Idowu, Olufemi E. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria.
IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF MULTNOMAH ) ) ) ) ) ) ) ) ) ) ) ) ) GENERAL JURISDICTION AND COMMON FACTUAL ALLEGATIONS
 ) ) ) ) ) ) ) ) ) ) ) ) GENERAL JURISDICTION AND COMMON FACTUAL ALLEGATIONS") Phillip C. Gilbert, OSB No. rd S.E. Avenue Suite A Gresham, Oregon 00-1 Phone: (0-00 Fax: (0-01 pgilbert@teleport.com IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF MULTNOMAH DAWN D. JOHNSON
Phillip C. Gilbert, OSB No. rd S.E. Avenue Suite A Gresham, Oregon 00-1 Phone: (0-00 Fax: (0-01 pgilbert@teleport.com IN THE CIRCUIT COURT OF THE STATE OF OREGON FOR THE COUNTY OF MULTNOMAH DAWN D. JOHNSON
ISPUB.COM. Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay. P Chudgar INTRODUCTION SPINE
 ISPUB.COM The Internet Journal of Radiology Volume 8 Number 2 Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay P Chudgar Citation P Chudgar.. The Internet Journal of Radiology.
ISPUB.COM The Internet Journal of Radiology Volume 8 Number 2 Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay P Chudgar Citation P Chudgar.. The Internet Journal of Radiology.
Pott disease (spinal tuberculosis): MR and CT imaging
: MR and CT imaging") Pott disease (spinal tuberculosis): MR and CT imaging Poster No.: C-1422 Congress: ECR 2016 Type: Educational Exhibit Authors: G. Beretis, K. Giannaki, M. Fasoula, D. Kypriotis, T. Dagla, T.-P. Mantzouranis;
Pott disease (spinal tuberculosis): MR and CT imaging Poster No.: C-1422 Congress: ECR 2016 Type: Educational Exhibit Authors: G. Beretis, K. Giannaki, M. Fasoula, D. Kypriotis, T. Dagla, T.-P. Mantzouranis;
Mohammad Ashraf. - Bahaa Najjar. - Mousa Al-Abbadi. 1 P a g e
 - 4 - Mohammad Ashraf - Bahaa Najjar - Mousa Al-Abbadi 1 P a g e Fractures (cont d). Healing of fractures: There are a lot of factors determine the proper healing of the fracture. For example: Displaced
- 4 - Mohammad Ashraf - Bahaa Najjar - Mousa Al-Abbadi 1 P a g e Fractures (cont d). Healing of fractures: There are a lot of factors determine the proper healing of the fracture. For example: Displaced
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji
 Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Anterior Cervical Discectomy and Fusion Surgery
 Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Disclaimer This movie is an educational resource only and should not be used to manage orthopaedic health. All decisions about the management of orthopaedic conditions must be made in conjunction with
Functional Anatomy and Exam of the Lumbar Spine. Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation
 Functional Anatomy and Exam of the Lumbar Spine Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation Disclosure Anatomical Review Quick Review of Bony and Ligamentous structures Discal anatomy
Functional Anatomy and Exam of the Lumbar Spine Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation Disclosure Anatomical Review Quick Review of Bony and Ligamentous structures Discal anatomy
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL
 SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
SPINAL CHAPTER, NESON DEGENERATIVE SPINAL DISEASE PRABIN SHRESTHA ANISH M SINGH B&B HOSPITAL INTRODUCTION DEGENERATIVE SPINAL DISEASE Gradual loss of normal structure and function of spine with time Also
Alan H Daniels, MD. Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University
 Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
GET BACK TO YOUR FUTURE WITH SPECIALIZED SPINE CARE. A Guide for Patients
 GET BACK TO YOUR FUTURE WITH SPECIALIZED SPINE CARE A Guide for Patients Your Spine Deserves Special Care Your spine is at the center of a delicately balanced system that controls all of your body s movements.
GET BACK TO YOUR FUTURE WITH SPECIALIZED SPINE CARE A Guide for Patients Your Spine Deserves Special Care Your spine is at the center of a delicately balanced system that controls all of your body s movements.
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY
 Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Case Presentation: Diagnosing Spinal Epidural Abscess
 Case Presentation: Diagnosing Spinal Epidural Abscess Introduction Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural
Case Presentation: Diagnosing Spinal Epidural Abscess Introduction Failure to diagnose is the most common medical error in the practice of emergency, urgent care and primary care medicine. Spinal epidural
MUSCULOSKELETAL INFECTIONS IN CHILDREN. Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool
 MUSCULOSKELETAL INFECTIONS IN CHILDREN Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool MUSCULOSKELETAL INFECTIONS Common and uncommon infections Common and uncommon presentations Imaging
MUSCULOSKELETAL INFECTIONS IN CHILDREN Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool MUSCULOSKELETAL INFECTIONS Common and uncommon infections Common and uncommon presentations Imaging
Case Discussion: Post-implant infections & explant decision making
 Author Information Full Names: Sailesh Arulkumar, MD David Provenzano, MD Affiliation: Sailesh Arulkumar MD: Attending Pain Physician, The Orthopaedic Center, Tulsa OK David Provenzano, MD: Attending Pain
Author Information Full Names: Sailesh Arulkumar, MD David Provenzano, MD Affiliation: Sailesh Arulkumar MD: Attending Pain Physician, The Orthopaedic Center, Tulsa OK David Provenzano, MD: Attending Pain
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Osteomyelitis Samir S. Shah, MD, MSCE
 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases
Bioactive glass S53P4 in spine surgery -results from a prospective 11-year-follow-up
 Bioactive glass S53P4 in spine surgery -results from a prospective 11-year-follow-up Janek Frantzén M.D., Neurosurgeon Turku University Hospital, Finland ROME SPINE 2011 7.12.2011 1 Clinical Development
Bioactive glass S53P4 in spine surgery -results from a prospective 11-year-follow-up Janek Frantzén M.D., Neurosurgeon Turku University Hospital, Finland ROME SPINE 2011 7.12.2011 1 Clinical Development
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology University of Washington, Seattle, WA
 ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
ASA Closed Claims Project: Regional Anesthesia Claims 1990 or later Lorri A. Lee MD Department of Anesthesiology, Seattle, WA OVERVIEW 1. Closed Claims Project 2. Peripheral Nerve Blocks 3. Neuraxial Claims
ACDF. Anterior Cervical Discectomy and Fusion. An introduction to
 An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
The Biomechanics of the Human Spine. Basic Biomechanics, 6 th edition By Susan J. Hall, Ph.D.
 Chapter 9 The Biomechanics of the Human Spine Structure of the Spine The spine is a curved stack of 33 vertebrae structurally divided into five regions: cervical region - 7 vertebrae thoracic region -
Chapter 9 The Biomechanics of the Human Spine Structure of the Spine The spine is a curved stack of 33 vertebrae structurally divided into five regions: cervical region - 7 vertebrae thoracic region -
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Primary care referral criteria for musculoskeletal MRI scans
 Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
Types of bone/joint infections. Bone and Joint Infections. Septic Arthritis. Pathogenesis. Pathogenesis. Bacterial arthritis: predisposing factors
 Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Disclosure. Thoracolumbar Tumors. Intraspinal Tumor Removal Options 6/4/2011. Minimally Invasive Approaches for Spinal Tumors
 Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
Minimally Invasive Approaches for Spinal Tumors Praveen V. Mummaneni, M.D. Disclosure Medtronic (Consultant, Grants) DePuy (Consultant, Other Financial Support) Associate Professor Dept. of Neurosurgery
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Thank you for choosing Saint Joseph s Hospital Health Center for your spine surgery. Updated Jan 2017
 Thank you for choosing Saint Joseph s Hospital Health Center for your spine surgery Updated Jan 2017 This class is designed to give you some basic, important information about spine surgery We will cover
Thank you for choosing Saint Joseph s Hospital Health Center for your spine surgery Updated Jan 2017 This class is designed to give you some basic, important information about spine surgery We will cover
PATIENT: DOB: TODAY S DATE:
 1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
NECK AND BACK PAIN AN INTRODUCTION TO
 AN INTRODUCTION TO NECK AND BACK PAIN This booklet provides general information on neck and back pain. It is not meant to replace any personal conversations that you might wish to have with your physician
AN INTRODUCTION TO NECK AND BACK PAIN This booklet provides general information on neck and back pain. It is not meant to replace any personal conversations that you might wish to have with your physician
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES
 REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
HIDDEN IN PLAIN SITE:
 HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
Spinal epidural abscess is uncommon but has the potential
 J Neurosurg Spine 14:765 770, 2011 Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain Clinical
J Neurosurg Spine 14:765 770, 2011 Prospective evaluation of a clinical decision guideline to diagnose spinal epidural abscess in patients who present to the emergency department with spine pain Clinical
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Spine. Neuroradiology. Spine. Spine Pathology. Distribution of fractures. Radiological algorithm. Role of radiology 18/11/2015
 Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Spine Neuroradiology Spine Prof.Dr.Nail Bulakbaşı X Ray: AP/L/Oblique Vertebra & disc spaces CT & CTA Vertebra, discs, vessels MRI & MRA Vertebra, disc, vessels, meninges Spinal cord & nerves Myelography
Musculoskeletal Infection and Inflammation
 F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
Analysis of Neurosurgery Risks
 % of claim volume Analysis of Neurosurgery Risks Surgical and diagnostic-related allegations are the two most frequent case types involving neurosurgeons. Of lesser frequency and severity were medication-related
% of claim volume Analysis of Neurosurgery Risks Surgical and diagnostic-related allegations are the two most frequent case types involving neurosurgeons. Of lesser frequency and severity were medication-related
CHERYL McGAULEY, as Personal Representative of the Estate of WALTER L. McGAULEY, SR.,
 COUNTY AND COURT: Alachua County Circuit Court NAME OF CASE: CHERYL McGAULEY, as Personal Representative of the Estate of WALTER L. McGAULEY, SR., v. Plaintiff, DOCTORS RADIOLOGY GROUP OF GAINESVILLE,
COUNTY AND COURT: Alachua County Circuit Court NAME OF CASE: CHERYL McGAULEY, as Personal Representative of the Estate of WALTER L. McGAULEY, SR., v. Plaintiff, DOCTORS RADIOLOGY GROUP OF GAINESVILLE,
The vault bones Frontal Parietals Occiput Temporals Sphenoid Ethmoid
 The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
Premier Orthopedic Spine Center
 Premier Orthopedic Spine Center Atrium Medical Center Professional Buliding 200 Medical Center Dr., Ste. 375 Middletown, Ohio 45005 Neck Questionnaire Patient Date Family Physician The onset of my neck
Premier Orthopedic Spine Center Atrium Medical Center Professional Buliding 200 Medical Center Dr., Ste. 375 Middletown, Ohio 45005 Neck Questionnaire Patient Date Family Physician The onset of my neck
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
All About? What is Sciatica. Disclaimer. Integrated web marketing. Multimedia Health Education
 What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
INJECTION FOR YOUR BACK & NECK
 INJECTION FOR YOUR BACK & NECK CERVICAL EPIDURAL CERVICAL FACET BLOCKS LUMBAR EPIDURAL FACET BLOCKS ROOT BLOCKS INJECTIONS FOR YOUR BACK A lumbar caudal epidural steroid injection is an outpatient procedure
INJECTION FOR YOUR BACK & NECK CERVICAL EPIDURAL CERVICAL FACET BLOCKS LUMBAR EPIDURAL FACET BLOCKS ROOT BLOCKS INJECTIONS FOR YOUR BACK A lumbar caudal epidural steroid injection is an outpatient procedure
Normal Recovery or Complication: The Risks of Post-Operative Care
 Normal Recovery or Complication: The Risks of Post-Operative Care Darrell Ranum, JD, CPHRM Vice President Patient Safety and Risk Management Department Ohio Hospital Association Convention June 14, 2016
Normal Recovery or Complication: The Risks of Post-Operative Care Darrell Ranum, JD, CPHRM Vice President Patient Safety and Risk Management Department Ohio Hospital Association Convention June 14, 2016
SpineFAQs. Neck Pain Diagnosis and Treatment
 SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
J Korean Soc Spine Surg 2016 Sep;23(3): Originally published online September 30, 2016;
: Originally published online September 30, 2016;") Journal of Korean Society of Spine Surgery Multifocal Extensive Spinal Tuberculosis Accompanying Isolated Involvement of Posterior Elements - A Case Report - Dong-Eun Shin, M.D., Sang-June Lee, M.D., Young
Journal of Korean Society of Spine Surgery Multifocal Extensive Spinal Tuberculosis Accompanying Isolated Involvement of Posterior Elements - A Case Report - Dong-Eun Shin, M.D., Sang-June Lee, M.D., Young
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
OMT for the ACOFP Boards: A Review of Clinical and Basic Information
 OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute
 A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
Quiles v Rojas 2015 NY Slip Op 31664(U) January 5, 2015 Supreme Court, Bronx County Docket Number: /11 Judge: Howard H. Sherman Cases posted
 January 5, 2015 Supreme Court, Bronx County Docket Number: /11 Judge: Howard H. Sherman Cases posted") Quiles v Rojas 2015 NY Slip Op 31664(U) January 5, 2015 Supreme Court, Bronx County Docket Number: 306567/11 Judge: Howard H. Sherman Cases posted with a "30000" identifier, i.e., 2013 NY Slip Op 30001(U),
Quiles v Rojas 2015 NY Slip Op 31664(U) January 5, 2015 Supreme Court, Bronx County Docket Number: 306567/11 Judge: Howard H. Sherman Cases posted with a "30000" identifier, i.e., 2013 NY Slip Op 30001(U),
Critical Review Form Diagnostic Test
 Critical Review Form Diagnostic Test The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess, J Emerg Med 2004; 26:285-291 Objectives: To
Critical Review Form Diagnostic Test The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess, J Emerg Med 2004; 26:285-291 Objectives: To
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Two Level Vertebral Osteomyelitis Without Spinal Epidural Abscess Secondary to Spinal and Epidural Anesthesia: Two Case
 Article ID: WMC003938 ISSN 2046-1690 Two Level Vertebral Osteomyelitis Without Spinal Epidural Abscess Secondary to Spinal and Epidural Anesthesia: Two Case Corresponding Author: Dr. Ergun Karavelioglu,
Article ID: WMC003938 ISSN 2046-1690 Two Level Vertebral Osteomyelitis Without Spinal Epidural Abscess Secondary to Spinal and Epidural Anesthesia: Two Case Corresponding Author: Dr. Ergun Karavelioglu,
DIAGNOSTIC USE OF MAGNETIC RESONANCE IMAGING (MRI) OF A CERVICAL EPIDURAL ABSCESS AND SPONDYLODISCITIS IN AN INFANT CASE REPORT
 OF A CERVICAL EPIDURAL ABSCESS AND SPONDYLODISCITIS IN AN INFANT CASE REPORT") DOI: 10.15386/cjmed-460 Case Reports DIAGNOSTIC USE OF MAGNETIC RESONANCE IMAGING (MRI) OF A CERVICAL EPIDURAL ABSCESS AND SPONDYLODISCITIS IN AN INFANT CASE REPORT IULIAN RAUS 1, SIMONA TATAR 2, ROXANA
DOI: 10.15386/cjmed-460 Case Reports DIAGNOSTIC USE OF MAGNETIC RESONANCE IMAGING (MRI) OF A CERVICAL EPIDURAL ABSCESS AND SPONDYLODISCITIS IN AN INFANT CASE REPORT IULIAN RAUS 1, SIMONA TATAR 2, ROXANA
Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment
 Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment 1 Seminars in Ultrasound, CT, and MRI June 2009; Volume 30; Number 3; pp. 168-173 Vincenzo Giuliano, MD, Antonio Pinto,
Kinematic Cervical Spine Magnetic Resonance Imaging in Low-Impact Trauma Assessment 1 Seminars in Ultrasound, CT, and MRI June 2009; Volume 30; Number 3; pp. 168-173 Vincenzo Giuliano, MD, Antonio Pinto,
Chapter 35 Back Pain. Episode overview: Wisecracks: Crack Cast Show Notes Back Pain July 2016
 Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health
 UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Bilateral Psoas Abscess in the Emergency Department Permalink https://escholarship.org/uc/item/8296x9cx
UC Irvine Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health Title Bilateral Psoas Abscess in the Emergency Department Permalink https://escholarship.org/uc/item/8296x9cx
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F ST. PAUL FIRE & MARINE INSURANCE, INSURANCE CARRIER
 BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F407478 CHRIS TURPIN WEST FOODS, INC. ST. PAUL FIRE & MARINE INSURANCE, INSURANCE CARRIER CLAIMANT RESPONDENT RESPONDENT OPINION FILED DECEMBER
BEFORE THE ARKANSAS WORKERS' COMPENSATION COMMISSION CLAIM NO. F407478 CHRIS TURPIN WEST FOODS, INC. ST. PAUL FIRE & MARINE INSURANCE, INSURANCE CARRIER CLAIMANT RESPONDENT RESPONDENT OPINION FILED DECEMBER
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Infectious Spondylodiscitis
 Beth Israel Deaconess Medical Center Harvard Medical School Advanced Radiology Clerkship September 2009 Infectious Spondylodiscitis Sebastián Bravo Grau (University los Andes - Faculty of Medicine 7th
Beth Israel Deaconess Medical Center Harvard Medical School Advanced Radiology Clerkship September 2009 Infectious Spondylodiscitis Sebastián Bravo Grau (University los Andes - Faculty of Medicine 7th
BACK PAIN. Disclaimer. Integrated web marketing. Multimedia Health Education
 BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
Low Back Pain Optimal Management in General Practice
 Low Back Pain Optimal Management in General Practice Dr Neil Hearnden Musculoskeletal Physician M.B. B.S. FRACGP. Grad Dip Musculoskeletal.Med. (Otago) MAFMM Arana Hills Medical Centre Brisbane Outcome
Low Back Pain Optimal Management in General Practice Dr Neil Hearnden Musculoskeletal Physician M.B. B.S. FRACGP. Grad Dip Musculoskeletal.Med. (Otago) MAFMM Arana Hills Medical Centre Brisbane Outcome
Main Menu. Trunk and Spinal Column click here. The Power is in Your Hands
 1 The Trunk and Spinal Column click here Main Menu K.9 http://www.handsonlineeducation.com/classes/k9/k9entry.htm[3/27/18, 2:00:55 PM] The Trunk and Spinal Column Vertebral column complex 24 intricate
1 The Trunk and Spinal Column click here Main Menu K.9 http://www.handsonlineeducation.com/classes/k9/k9entry.htm[3/27/18, 2:00:55 PM] The Trunk and Spinal Column Vertebral column complex 24 intricate
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected