Osteomyelitis Samir S. Shah, MD, MSCE
|
|
|
- Wilfred Carroll
- 5 years ago
- Views:
Transcription
1 Osteomyelitis Samir S. Shah, MD, MSCE Professor, Department of Pediatrics University of Cincinnati College of Medicine Director, Division of Hospital Medicine Attending Physician in Infectious Diseases & Hospital Medicine James M. Ewell Endowed Chair Cincinnati Children's Hospital Medical Center
2 Disclosures Current sources of research funding National Institute of Allergy & Infectious Diseases Patient-Centered Outcomes Research Institute National Heart, Lung, & Blood Institute Cincinnati Children s Research Foundation No financial conflicts of interest
3 Objectives Review data supporting the role of early conversion to oral therapy for children with acute hematogenous osteomyelitis Discuss a comprehensive for the evidence-based management of acute hematogenous osteomyelitis AHO = acute hematogenous osteomyelitis
4 CCHMC Guideline- Population Age 3 months- 21 years Clinical suspicion for acute bone infection
5 CCHMC Guideline- Excludes Non-acute osteomyelitis (symptoms >2 weeks) Non-hematogenous osteomyelitis Prior fracture or surgery at site Infections from penetrating trauma Pressure ulcers leading to osteomyelitis Atypical patients Immunocompromised Multifocal disease Medically complex patients
6 CCHMC Guideline Local expert consensus Admit to Hospital Medicine Orthopedic consultation Infectious Diseases consultation
7 CCHMC Guideline- Initial Evaluation C-reactive protein Elevated CRP consistent with AHO Normal or minimal elevation suggests other cause ESR not recommended- limited value Correlates with CRP but rises & declines more slowly Procalcitonin not recommended Insufficient data Complete blood count Normal in 65% of cases May suggest alternate cause Blood culture X-ray of affected site
8 CCHMC Guideline- AHO Diagnosis CRP >2 mg/dl High sensitivity (98%) Insufficiently specific to differentiate from other infections One or more Characteristic pain Localized signs or symptoms Reduced ROM Reduced weight bearing Lack of alternate explanation
9 CCHMC Guideline Cultures Obtain blood culture prior to antibiotics Insufficient data to recommend routine bone aspiration prior to antibiotics If vancomycin initiated, strongly consider source culture Defer antibiotics for up to 24h in patients who do not meet formal sepsis criteria if bone or tissue culture will be performed Start empiric antibiotics immediately once intended cultures obtained or with positive culture from sterile site (e.g., blood, bone)
10 CCHMC Guideline- Treatment Cefazolin for most patients
11 CCHMC Guideline- Why Cefazolin? Most effective antibiotic vs. MSSA CCHMC osteomyelitis >70% MSSA Modest prevalence of clindamycin-resistant MSSA Modest prevalence of clindamycin-resistant MRSA Effective vs. K. kingae Screen for MRSA risk factors
12 CCHMC Guideline- Treatment Cefazolin for most patients Clindamycin if MRSA risk factors Any prior hospitalization with MRSA infection History of other MRSA infection in past 2 years History of skin abscesses in past 2 years Abscess associated with current infection Immediate family members with MRSA skin abscesses or other infection recently
13 CCHMC Guideline- Age <4 years Review risk factors for Kingella kingae Concomitant mucositis, stomatitis, or oral ulcers Mild clinical disease, especially if not responsive to initial clindamycin treatment Clindamycin does not cover K. kingae If clindamycin initiated, consider adding cefazolin or ceftriaxone based on history & risk factors
14 CCHMC Guideline- Critically Ill Vancomycin & cefazolin for critical illness Definition of critical illness ICU admission Meets formal pediatric sepsis criteria Overall ill appearance Requires large volume fluid resuscitation Seriously consider source (i.e. bone) culture when feasible
15 CCHMC Guideline- Imaging MRI Recommended to confirm diagnosis Highly sensitive May guide decisions regarding need for surgery Tc99 bone scan is not generally recommended
16 CCHMC Guideline Indications for surgical intervention Abscess >1cm identified on clinical exam or imaging Failure to improve after 48h of reasonable medical therapy
17 CCHMC Guideline- Ongoing Labs CRP To follow response to therapy Frequency Not more often than every 48 h Less often if patient is improving or received surgery or bone debridement Blood culture 1 per day for at least 2 days Daily if bacteremia persists Not recommended Repeat CBC Any ESR
18 CCHMC Guideline- Oral Therapy Patients should transition to oral therapy as standard practice Contraindications to oral therapy Unable to take oral medication Underlying condition affecting drug absorption Isolate resistant to oral antibiotic options Concerns about patient adherence are not a contraindication to oral therapy Focus on interventions to promote adherence to oral regimen
19 CCHMC Guideline- Oral Therapy Criteria for transition to oral therapy IV therapy for at least 72h (some exceptions) Significant clinical improvement Improvement in initial symptoms Resolution of fever Resolution of bacteremia Caution if total duration of bacteremia >3 days CRP decreased by 33% from initial value or values downtrending Causative bacteria identified & susceptibilities confirmed OR no organism identified & relevant cultures no growth for >48 h
20 CCHMC Guideline- Discharge Criteria If oral transition criteria met Oral test dose given Consider additional observation on oral antibiotics if patient is young or if administration of first dose is challenging Patient has medication in hand Consider blister pack for those receiving pills or capsules If requires IV therapy, ensure that homecare arranged Education completed Follow-up scheduled (ID, Ortho, PMD)
21 CCHMC Guideline- Follow-up Visits Oral therapy ID 7-10 days after discharge 4 weeks after discharge +/- 1 week Additional follow-up as indicated More frequent follow-up if issues arise or suspected Orthopedics 2-4 weeks after discharge if immobilization or surgical intervention 4 weeks after discharge with growth plate involvement IV therapy ID clinic weekly Orthopedics as above
22 CCHMC Guideline- Follow-up Labs CRP At 1st follow-up visit At 2 nd follow-up visit if not normal at initial visit Provide guidance for blood draw prior to appointment No other follow-up labs required unless specific indication exists
23 CCHMC Guideline- Antibiotic Duration 28 days of therapy if CRP normal Clinical symptoms resolved Elevated ESR (if checked) is not an indication for prolonging antibiotic therapy
24 Harms of Prolonged IV Therapy Complications Hospital-acquired Catheter placement-associated Catheter-associated Medication error Financial costs Healthcare system Family Emotional toll Schroeder A. JHM 2014
25 Considerations for Early Switch to Oral Therapy Clinical improvement observed Oral route not compromised Vomiting, malabsorption, severe diarrhea, or patient refusal of oral medications Laboratory or other markers improving (not always necessary if other criteria are met) Indication for oral therapy i.e., not meningitis, not endocarditis Comparable oral antibiotic option available
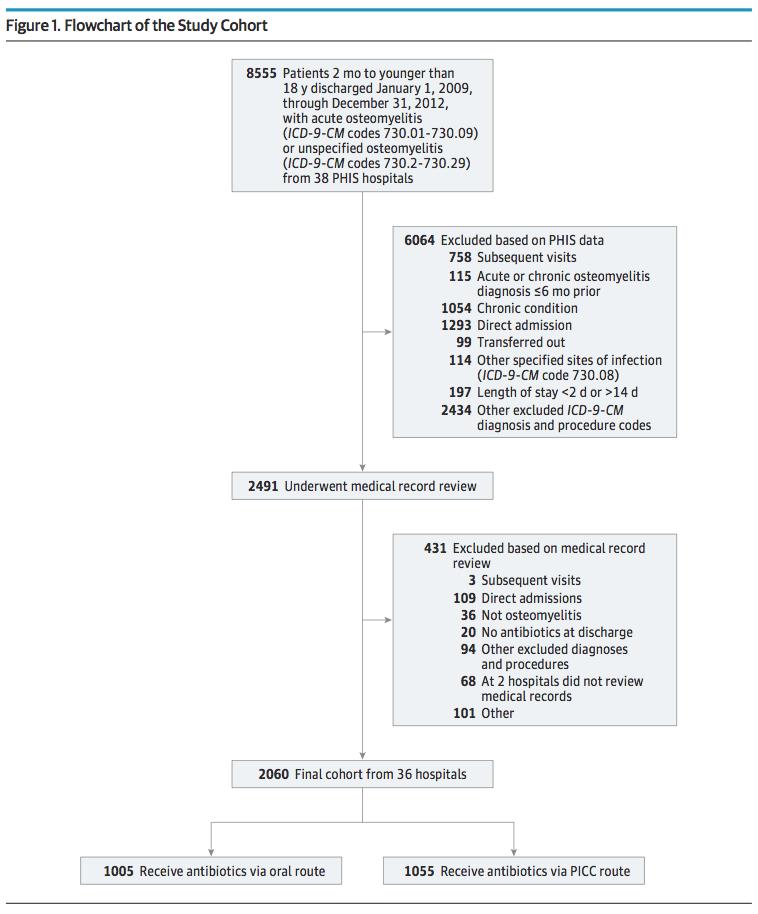
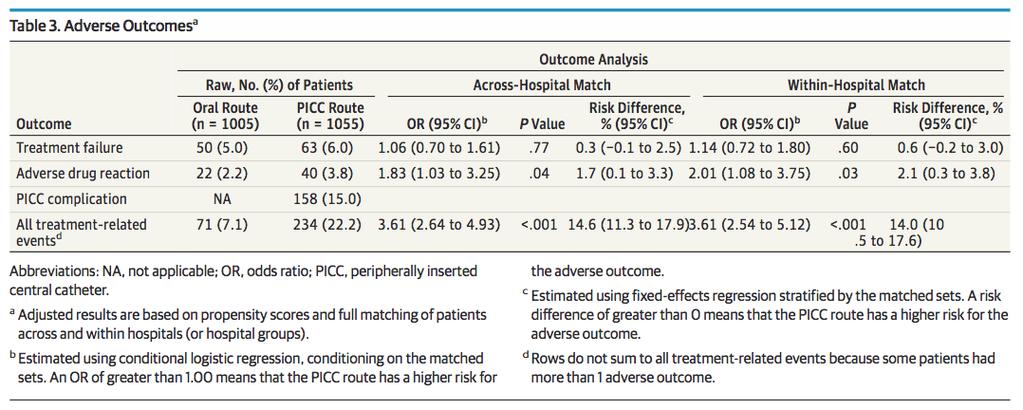
26 Osteomyelitis: Primary Outcome Main Exposure Post-discharge antibiotics via PICC or oral route Main Outcome Treatment failure ED or hospital revisit resulting in escalation of therapy (e.g., change in antibiotics, switch from PO to IV, abscess drainage, bone debridement) Secondary Outcomes Adverse drug reaction (e.g., neutropenia, acute kidney injury, Stevens-Johnson) PICC complication (including fever evaluation) Composite of primary & secondary outcomes
27
28 Large and evenly distributed variation in use of PICCs No correlation between hospital osteo volume and use of PICCs

29 Osteomyelitis Matching reduces differences
30 Osteomyelitis: Results
31 Osteomyelitis: Results Isolation of MRSA as the causative organism did not modify the effect of the treatment route on the outcome of treatment failure.
32 Osteomyelitis Children discharged to complete antibiotic course via oral route did NOT have a higher rate of treatment failure MRSA+ infections did not have more treatment failures High rate of serious PICC complications 15% required ED revisit or rehospitalization Bloodstream infections Thromboembolism PICC displacement/breakage
33 Osteomyelitis Likely to be strongest evidence available to answer question RCT not feasible Results consistent, even with rise in MRSA prevalence (study period ) Stop using PICC lines to treat acute osteomyelitis in otherwise healthy children who can tolerate oral route Oral route equally effective, fewer complications, less expensive and more convenient
34 Thank
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infectious Diseases Society of America Emerging Infections Network. Comments for Query: Osteomyelitis in Children
 Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
Infectious Diseases Society of America Emerging Infections Network Comments for Query: Osteomyelitis in Children Choice of antimicrobial At our institution, we typically start with clindamycin (unless
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Mortality Rate was unsightly!!! 4/24/2013. Sepsis Quality Improvement Project
 Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Management of Acute Haematogenous Osteomyelitis. SAPOS ICL 2017 Anthony Robertson
 Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Physician's Core Measure Pocket Guide AMI
 Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Community Acquired Pneumonia
 April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
April 2014 References: 1. Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, Kaplan SL Mace SE, McCracken Jr. GH, Moor MR, St. Peter SD, Stockwell JA, and Swanson JT. The Management of
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Antibiotic Management of Pediatric Osteomyelitis
 Reprinted from www.antimicrobe.org Sandra Arnold, M.D. Antibiotic Management of Pediatric Osteomyelitis Several points uncertainty exist regarding the antimicrobial management of acute hematogenous osteomyelitis,
Reprinted from www.antimicrobe.org Sandra Arnold, M.D. Antibiotic Management of Pediatric Osteomyelitis Several points uncertainty exist regarding the antimicrobial management of acute hematogenous osteomyelitis,
Treatment of infection
 Clinica Ortopedica e Traumatologica Università degli Studi di Pavia Fondazione IRCCS Policlinico San Matteo Chairman: Prof. F. Benazzo Goals: - Healing of infection - Healing of fracture - Try to keep
Clinica Ortopedica e Traumatologica Università degli Studi di Pavia Fondazione IRCCS Policlinico San Matteo Chairman: Prof. F. Benazzo Goals: - Healing of infection - Healing of fracture - Try to keep
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia
 Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia Amanda Guth 1 Amy Slenker MD 1,2 1 Department of Infectious Diseases, Lehigh Valley Health Network
Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia Amanda Guth 1 Amy Slenker MD 1,2 1 Department of Infectious Diseases, Lehigh Valley Health Network
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Acute Osteomyelitis: similar to septic arthritis but up to 40% may be afebrile swelling overlying the bone & tenderness
 Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital
 Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
Andrea Marmor, MD Associate Clinical Professor, Pediatrics UCSF San Francisco General Hospital Carambola is a 16 mo old girl brought to the ED for crying nonstop She has been not herself for about a week,
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines
 Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?
 Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?") Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
Update in Hospital Medicine. Disclosures 10/30/2017. none Oregon Chapter ACP Scientific Meeting
 Update in Hospital Medicine 2017 Oregon Chapter ACP Scientific Meeting DATE: November 4, 2017 PRESENTED BY: Joel Papak, MD FACP Disclosures none 1 How well do you think you keep up with the medical literature?
Update in Hospital Medicine 2017 Oregon Chapter ACP Scientific Meeting DATE: November 4, 2017 PRESENTED BY: Joel Papak, MD FACP Disclosures none 1 How well do you think you keep up with the medical literature?
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW
 OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW Dr. Roshan Sah* and Prof. Lui Ke bin Department of Orthopaedics, The First Affiliated Peoples Hospital of Yangtze University, Jingzhou, Hubei, PR.
OSTEOMYELITIS AND SEPTIC ARTHRITIS IN CHILDREN: REVIEW Dr. Roshan Sah* and Prof. Lui Ke bin Department of Orthopaedics, The First Affiliated Peoples Hospital of Yangtze University, Jingzhou, Hubei, PR.
Osteomyelitis Revisited
 Osteomyelitis Revisited Alan Jay Block, DPM, MS, FASPS, FACFAS Co-Chairman My Leg My Choice Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in
Osteomyelitis Revisited Alan Jay Block, DPM, MS, FASPS, FACFAS Co-Chairman My Leg My Choice Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in
Antimicrobial Guidelines for the Empirical Management of Diabetic Foot Infections
 Antimicrobial Guidelines for the Empirical Management of Diabetic Foot Infections Version 7.2 PAGL Inclusion Approved at January 2017 PGC APPROVED BY: TRUST REFERENCE: B3/2017 AWP REF: UHL Policies and
Antimicrobial Guidelines for the Empirical Management of Diabetic Foot Infections Version 7.2 PAGL Inclusion Approved at January 2017 PGC APPROVED BY: TRUST REFERENCE: B3/2017 AWP REF: UHL Policies and
Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of the Knee
 Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
HIDDEN IN PLAIN SITE:
 HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
Evidence-based Management of Fever in Infants and Young Children
 Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Evidence-based Management of Fever in Infants and Young Children Shabnam Jain, MD, MPH Associate Professor of Pediatrics Emory University Medical Director for Clinical Effectiveness Objectives Understand
Osteomyelitis Revisited
 Osteomyelitis Revisited Alan Jay Block, DPM, MS, FASPS, FACFAS Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in -Chief The Journal of the
Osteomyelitis Revisited Alan Jay Block, DPM, MS, FASPS, FACFAS Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in -Chief The Journal of the
CASE STUDY: ULCERATIVE COLITIS. Sammi Montag Dietetic Intern
 CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]
![Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]](/thumbs/83/87318178.jpg "Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]") Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Renal Unit. Catheter Related Bacteraemia Guidelines
 Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Evelina London Children s Hospital (ELCH)
") Evelina London Children s Hospital (ELCH) Lead Consultant Jenny Handforth PID Pharmacist Faye Chappell Paediatric OPAT CNS Vacant Overview Paediatric OPAT in London Paediatric OPAT ELCH Children s Hospital
Evelina London Children s Hospital (ELCH) Lead Consultant Jenny Handforth PID Pharmacist Faye Chappell Paediatric OPAT CNS Vacant Overview Paediatric OPAT in London Paediatric OPAT ELCH Children s Hospital
Curricular Components for Infectious Diseases EPA
 Curricular Components for Infectious Diseases EPA 1. EPA Title Management of previously healthy patients with a pediatric infectious disease. 2. Description of the A key role for subspecialists is to provide
Curricular Components for Infectious Diseases EPA 1. EPA Title Management of previously healthy patients with a pediatric infectious disease. 2. Description of the A key role for subspecialists is to provide
Infection. Arthrocentesis: Cell count Differential Culture. Infection and associated microorganism(s) confirmed
 confirmed") Painful joint History and examination Radiograph of affected joint Erythrocyte sedimentation rate C-reactive protein Infection No infection suspected Arthrocentesis: Cell count Differential Culture Stop
Painful joint History and examination Radiograph of affected joint Erythrocyte sedimentation rate C-reactive protein Infection No infection suspected Arthrocentesis: Cell count Differential Culture Stop
MANAGEMENT OF HAEMODIALYSIS CATHETER RELATED BLOOD STREAM INFECTION
 MANAGEMENT OF HAEMODIALYSIS CATHETER RELATED BLOOD STREAM INFECTION RRCV CMG Renal and Transplant Service 1. Introduction Catheter related blood stream infection (CR-BSI) is a common complication in patients
MANAGEMENT OF HAEMODIALYSIS CATHETER RELATED BLOOD STREAM INFECTION RRCV CMG Renal and Transplant Service 1. Introduction Catheter related blood stream infection (CR-BSI) is a common complication in patients
Pediatric Potpourri: What do we now?
 Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
Pediatric Potpourri: What do we now? April 19, 2013 Robert Wittler, MD 1 Disclosure I have no relevant financial relationships with the manufacturer(s) of any commercial products(s) and/or provider of
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Daniel C. DeSimone, MD Assistant Professor of Medicine
 Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases
 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases") Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
Pediatric Mysteries (including FWS / FUO) 13 June 2017 Tony Moody MD Duke Pediatric Infectious Diseases Disclosures Advisory board member for GSK (for belimumab pregnancy registry). Co-founder of Grid
CLINICAL USE OF GLYCOPEPTIDES. Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel
 CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
ED-SCANS: OVERALL DECISION SUPPORT ALGORITHM. Is This Strictly a Pain Episode? Decision 7: Referrals
 ED-SCANS: OVERALL DECISION SUPPORT ALGORITHM Decision 1: Triage Decision 2: Analgesic Management Is This Strictly a Pain Episode? Decision 3: Diagnostic Evaluation Decision 4: High Risk / High User Decision
ED-SCANS: OVERALL DECISION SUPPORT ALGORITHM Decision 1: Triage Decision 2: Analgesic Management Is This Strictly a Pain Episode? Decision 3: Diagnostic Evaluation Decision 4: High Risk / High User Decision
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Forty-Eighth Annual Teaching Conference Pediatrics for the Practitioner -UT Health Science Center San Antonio School of Medicine June 10-12, 2011
 The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
The 48 th Annual Pediatrics for the Practitioner Symposium June 11, 2011 James H. Brien, DO James H. Brien, DO has no relevant financial relationships with commercial interests to disclose. Case #1 4½-month-old
Utility of magnetic resonance imaging in the follow-up of children affected by acute osteomyelitis.
 Curr Pediatr Res 017; 1 (): 354-358 ISSN 0971-903 www.currentpediatrics.com Utility of magnetic resonance imaging in the follow-up of children affected by acute osteomyelitis. Valentina Fabiano 1, Giulia
Curr Pediatr Res 017; 1 (): 354-358 ISSN 0971-903 www.currentpediatrics.com Utility of magnetic resonance imaging in the follow-up of children affected by acute osteomyelitis. Valentina Fabiano 1, Giulia
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery
 Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery") Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl
 Case Reports in Orthopedics Volume 2015, Article ID 853974, 4 pages http://dx.doi.org/10.1155/2015/853974 Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl Masashi
Case Reports in Orthopedics Volume 2015, Article ID 853974, 4 pages http://dx.doi.org/10.1155/2015/853974 Case Report Arthroscopic Treatment of Septic Arthritis of the Elbow in a 4-Year-Old Girl Masashi
Pathophysiology and Etiology
 Sinusitis Pathophysiology and Etiology Sinusitis is inflammation of the mucosa of one or more sinuses. It can be either acute chronic. Chronic sinusitis is diagnosed if symptoms are present for more than
Sinusitis Pathophysiology and Etiology Sinusitis is inflammation of the mucosa of one or more sinuses. It can be either acute chronic. Chronic sinusitis is diagnosed if symptoms are present for more than
Objectives. Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection
 that drive empiric antimicrobial selection") Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
Objectives Define classes of uncomplicated skin and soft tissue infection (SSTI) that drive empiric antimicrobial selection Purulent SSTI Non-purulent SSTI Recognize conditions that suggest complications
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017
 Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017 Procalcitonin (PCT) PCT isbeing studied as a biomarker for infection PCT consists of 116 amino
Procalcitonin YUKON KUSKOKWIM HEALTH CORPORATION PRESENTED BY: CURT BUCHHOLZ, MD AUGUST 2017 Procalcitonin (PCT) PCT isbeing studied as a biomarker for infection PCT consists of 116 amino
Of 142 cases where sex was known, 56 percent were male; of 127cases where race was known, 90 percent were white, 4 percent were
 Group B Streptococcus Surveillance Report 2014 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: November 2015 Background The Active Bacterial Core surveillance
Group B Streptococcus Surveillance Report 2014 Oregon Active Bacterial Core Surveillance (ABCs) Center for Public Health Practice Updated: November 2015 Background The Active Bacterial Core surveillance
Percutaneous (Keyhole) Removal of Kidney Stone(s)
 Removal of Kidney Stone(s)") Who can I contact if I have a problem when I get home? If you experience any problems related to your surgery or admission once you have been discharged home. Please feel free to contact 4A, 4B or 4C ward
Who can I contact if I have a problem when I get home? If you experience any problems related to your surgery or admission once you have been discharged home. Please feel free to contact 4A, 4B or 4C ward
Sepsis and Infective Endocarditis
 Sepsis and Infective Endocarditis Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University in Prague and University Military Hospital Bacteremia and Sepsis bacteremia
Sepsis and Infective Endocarditis Michal Holub Department of Infectious Diseases First Faculty of Medicine Charles University in Prague and University Military Hospital Bacteremia and Sepsis bacteremia
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates
 Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Clinical and Molecular Characteristics of Community- Acquired Methicillin-Resistant Staphylococcus Aureus Infections In Chinese Neonates Xuzhuang Shen Beijing Children's Hospital, Capital Medical University,
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
If these vaccines haven t been given, please follow guidelines below for emergency procedures.
 MANAGEMENT OF PATIIENTS POST SPLENECTOMY & HYPOSPLENIIC PATIIENTS Splenectomised and hyposplenic patients are at increased risk of life-threatening infections due to encapsulated micro-organisms such as
MANAGEMENT OF PATIIENTS POST SPLENECTOMY & HYPOSPLENIIC PATIIENTS Splenectomised and hyposplenic patients are at increased risk of life-threatening infections due to encapsulated micro-organisms such as
Haemophilus influenzae, Invasive Disease rev Jan 2018
 Haemophilus influenzae, Invasive Disease rev Jan 2018 BASIC EPIDEMIOLOGY Infectious Agent Haemophilus influenzae (H. influenzae) is a small, Gram-negative bacillus, a bacterium capable of causing a range
Haemophilus influenzae, Invasive Disease rev Jan 2018 BASIC EPIDEMIOLOGY Infectious Agent Haemophilus influenzae (H. influenzae) is a small, Gram-negative bacillus, a bacterium capable of causing a range
Faculty Disclosure. Stephen I. Pelton, MD. Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
Faculty Disclosure Stephen I. Pelton, MD Dr. Pelton has listed no financial interest/arrangement that would be considered a conflict of interest. Advances in the management of fever in infants 0 to 3 and
CASE STUDY ON INPATIENT MALNUTRITION DISCUSSION
 CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
CASE STUDY ON INPATIENT MALNUTRITION Elena Kret-Sudjian MD, PhD, UC Davis Medical Center A 59 year-old white man with a history of diabetes, severe PVD, CKD IV, chronic hepatitis C admitted for non-healing
Infections Amenable to OPAT. (Nabin Shrestha + Ajay Mathur)
") 3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
Lemuel Shattuck Hospital Consultation Service
 Lemuel Shattuck Hospital Consultation Service a) Goals, Objectives, and ACGME Competencies Goals Learn how to manage complicated infectious disease problems in a public health setting. Learn how to provide
Lemuel Shattuck Hospital Consultation Service a) Goals, Objectives, and ACGME Competencies Goals Learn how to manage complicated infectious disease problems in a public health setting. Learn how to provide
Usefulness of Procalcitonin in the management of Infections in ICU. P Damas CHU Sart Tilman Liège
 Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
EDUCATIONAL COMMENTARY VANCOMYCIN MONITORING
 EDUCATIONAL COMMENTARY VANCOMYCIN MONITORING Commentary provided by: Julie Hall, MHS, MT (ASCP) Assistant Dean, College of Health Professions Assistant Professor, Medical Laboratory Science Grand Valley
EDUCATIONAL COMMENTARY VANCOMYCIN MONITORING Commentary provided by: Julie Hall, MHS, MT (ASCP) Assistant Dean, College of Health Professions Assistant Professor, Medical Laboratory Science Grand Valley
Enhanced EARS-Net Surveillance REPORT FOR 2012 DATA
 Enhanced EARS-Net Surveillance REPORT FOR DATA 1 In this report Main results for Proposed changes to the enhanced programme Abbreviations Used Here BSI Bloodstream Infections CVC Central Venous Catheter
Enhanced EARS-Net Surveillance REPORT FOR DATA 1 In this report Main results for Proposed changes to the enhanced programme Abbreviations Used Here BSI Bloodstream Infections CVC Central Venous Catheter
Bone and prosthetic joint infections: what the ID specialist needs?
 Bone and prosthetic joint infections: what the ID specialist needs? Andrej Trampuz Charité University Medicine Berlin Center for Septic Surgery Hip and knee replacements in Europe Germany Austria Belgium
Bone and prosthetic joint infections: what the ID specialist needs? Andrej Trampuz Charité University Medicine Berlin Center for Septic Surgery Hip and knee replacements in Europe Germany Austria Belgium
IR Central Venous Access [ ] Pre Procedure
![IR Central Venous Access [ ] Pre Procedure](/thumbs/90/104119758.jpg "IR Central Venous Access [ ] Pre Procedure") IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
Advanced Pediatric Emergency Medicine Assembly
 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
(+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Updates in Osteomyelitis Management
 Updates in Osteomyelitis Management Russell McCulloh, MD Assistant Professor, Pediatrics and Internal Medicine Divisions of Hospital Medicine and Infectious Diseases Children s Mercy Hospital Disclosure
Updates in Osteomyelitis Management Russell McCulloh, MD Assistant Professor, Pediatrics and Internal Medicine Divisions of Hospital Medicine and Infectious Diseases Children s Mercy Hospital Disclosure
Lapatinib and Capecitabine Therapy
 Lapatinib and Capecitabine Therapy This protocol should be read in conjunction with NCCP protocol 00216 Capecitabine Monotherapy. INDICATIONS FOR USE: INDICATION Treatment of adult patients with breast
Lapatinib and Capecitabine Therapy This protocol should be read in conjunction with NCCP protocol 00216 Capecitabine Monotherapy. INDICATIONS FOR USE: INDICATION Treatment of adult patients with breast
Tocilizumab Guided Questionnaire Gastrointestinal Perforation and Related Events
 Tocilizumab Guided Questionnaire Gastrointestinal Perforation and Related Events AER: Site : Local Case ID: Patient Date of Birth (dd-mmm-yyyy): Patient ID/Initials: Patient Gender: M F Patient Weight
Tocilizumab Guided Questionnaire Gastrointestinal Perforation and Related Events AER: Site : Local Case ID: Patient Date of Birth (dd-mmm-yyyy): Patient ID/Initials: Patient Gender: M F Patient Weight
Percutaneous removal of kidney stone(s): procedurespecific information
: procedurespecific information") PATIENT INFORMATION Percutaneous removal of kidney stone(s): procedurespecific information What is the evidence base for this information? This leaflet includes advice from consensus panels, the British
PATIENT INFORMATION Percutaneous removal of kidney stone(s): procedurespecific information What is the evidence base for this information? This leaflet includes advice from consensus panels, the British
Prevention of CAUTI is discussed in the CDC/HICPAC document, Guideline for Prevention of Catheter-associated Urinary Tract Infection 4.
 Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
Urinary Tract Infection (Catheter-Associated Urinary Tract Infection [CA] and Non-Catheter-Associated Urinary Tract Infection []) and Other Urinary System Infection [USI]) Events Introduction: Urinary
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS
 CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
CARE PATHWAY FOR CHILDREN AND YOUNG PERSONS WITH FEBRILE NEUTROPENIA, NEUTROPENIC SEPSIS OR SUSPECTED CENTRAL VENOUS LINE INFECTIONS This Care Pathway has been developed by a multidisciplinary team. It
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Tibial Nonunions: Should I Tackle and How
 Tibial Nonunions: Should I Tackle and How Frank R. Avilucea, MD Assistant Professor Department of Orthopaedic Surgery University of Cincinnati Medical Center Disclosures Journal Reviewer Journal of Bone
Tibial Nonunions: Should I Tackle and How Frank R. Avilucea, MD Assistant Professor Department of Orthopaedic Surgery University of Cincinnati Medical Center Disclosures Journal Reviewer Journal of Bone
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies
 The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
The Role of Observation Care in the Evaluation and Management of Cancer Emergencies Adam Klotz, MD Associate Attending Physician Memorial Sloan Kettering Cancer Center FACULTY DISCLOSURE Nothing to disclose
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Reviewing the recent literature to answer clinical questions: Should I change my practice?
 Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer
Reviewing the recent literature to answer clinical questions: Should I change my practice? JILL MILLER, MD PEM ATTENDING CHKD ASSISTANT PROFESSOR PEDIATRICS, EVMS Objectives Review the literature to answer