GI/Hepatology Test Review 2015GI. Brenda Shinar, MDa
|
|
|
- Edith Briggs
- 5 years ago
- Views:
Transcription

1 15.
2 GI/Hepatology Test Review 2015GI Brenda Shinar, MDa
3 Question 20.QueQuestion 1. B; Empiric treatment with antibiotics
 14 C d xylose breath test Hydrogen breath test Treatment 7 10 days: Augmentin or Flagyl +")
4 Diagnose and treat small intestinal bacterial overgrowth (SIBO) Symptoms of SIBO: Bloating, flatulance Abdominal pain Watery diarrhea Dyspepsia Weight loss Macrocytic anemia due to B12 malabsorption Diagnosis: Jejunal aspirate (gold standard) 14 C d xylose breath test Hydrogen breath test Treatment 7 10 days: Augmentin or Flagyl + Bactrim
5 D. No treatment at this time Question 2.
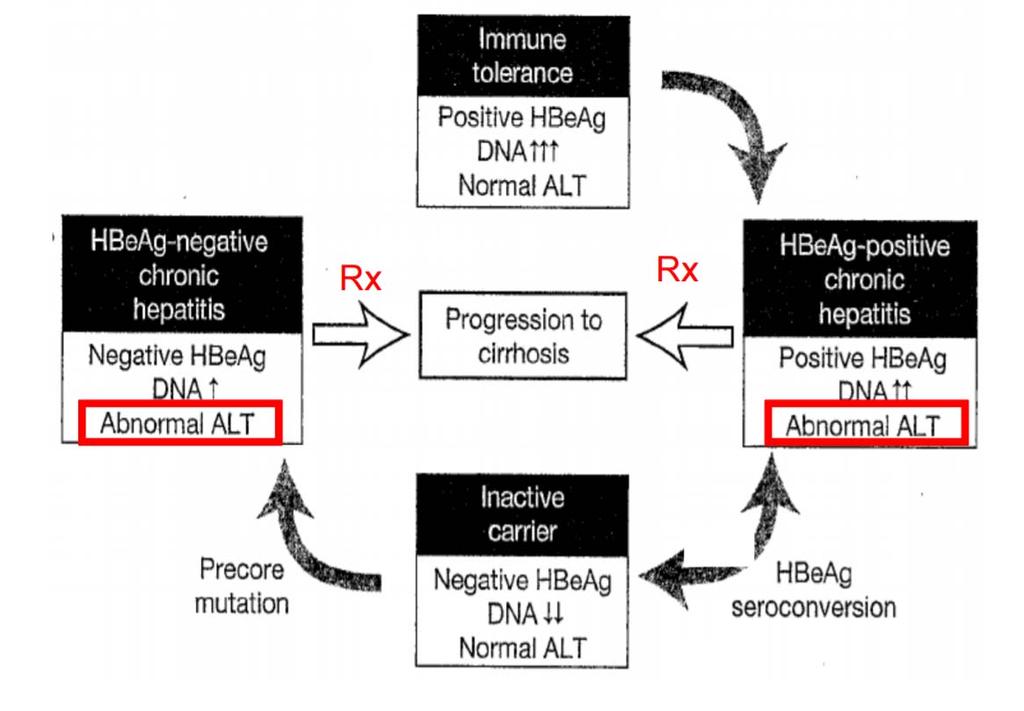
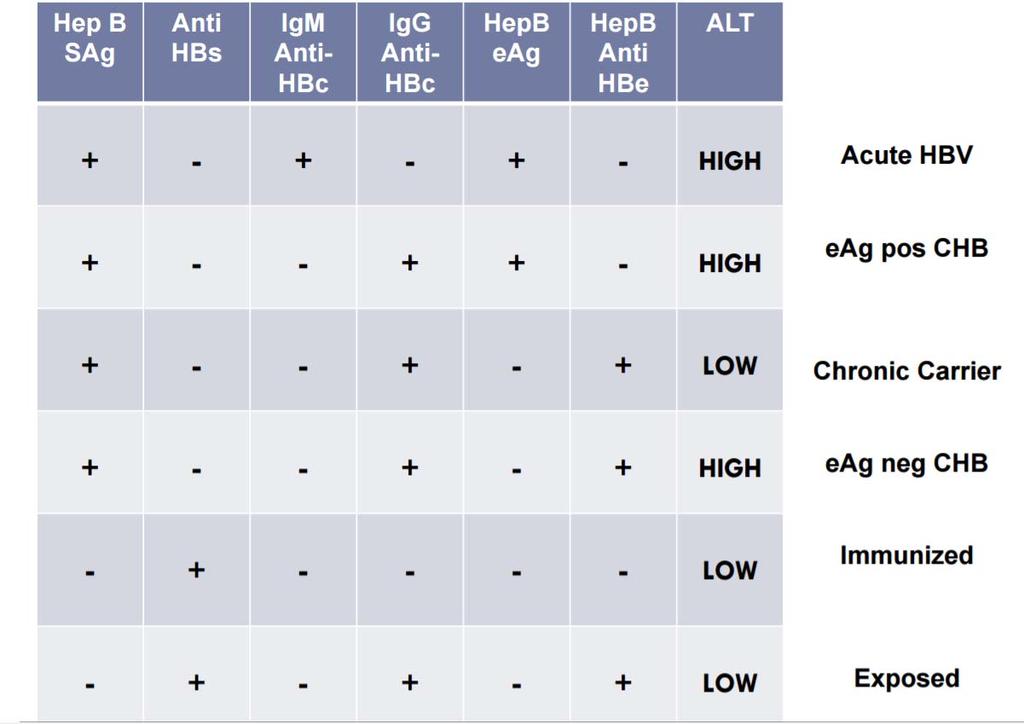
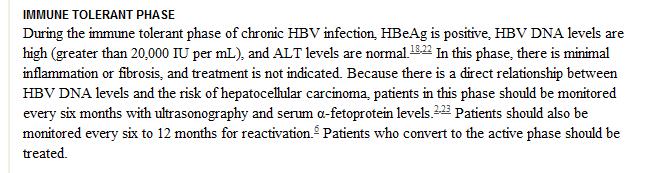
6 Manage Hep B virus infection in a patient in the immune tolerant phase
7
8
9
10 C; Trial of a proton pump inhibitor Question 3.

11 Manage gastroesophageal reflux disease with an empiric trial of a proton pump inhibitor
12 A; Certolizumab Question 4.

13 Treat Crohn disease in a pregnant patient SEVERITY SCORING FOR CROHN DISEASE: Crohn Disease Activity Index (CDAI) UNSAFE DRUGS FOR CROHN DISEASE IN PREGNANCY: Methotrexate Ciprofloxacin SAFE DRUGS FOR CROHN DISEASE IN PREGNANCY: 5 amino salicylates Prednisone Biologic agents (certolizumab, infliximab)
14 Question 5. C; Discontinue sugar free sweeteners
15 Sugar free alcohols: sorbitol xylitol mannitol isomalt maltitol Side effects: gas, bloating cramping Diarrhea (osmotic)
16 Osomotic: (watery) No diarrhea when fasting ( stool Na + K) = gap Stool osm gap > 125 = osmotic Secretory: (watery) Large volume, persists when fasting (stool Na+K) = gap < 50 = secretory Inflammatory: (white cells, blood) Fecal calprotectin (93% sensitive, 96% specific in adults Fecal WBC Sed rate/ CRP Fatty: Greasy, oily stool Quantitative fecal fat
17 B; 3 years Question 6.

18 Provide colonoscopy surveillance following a diagnosis of a serrated polyp
19 B; Celecoxib and omeprazole Question 7.

20 Treat a patient at risk for NSAID induced GI toxicity with a PPI and a COX 2 inhibitor Patients with ONE or MORE of the MODERATE risk factors should be given PPI therapy for PRIMARY prevention of gastrointestinal toxicity to NSAIDS! COMBINED USE OF COX 2 INHIBITORS AND PPIs In patients considered to be at exceptionally high risk for peptic ulcer disease, combining a selective COX 2 inhibitor with a proton pump inhibitor (PPI) may confer added protection against gastrointestinal (GI) toxicity. A randomized controlled trial of Helicobacter pylori negative patients who had been hospitalized for upper GI bleeding associated with nonselective nonsteroidal anti inflammatory drugs (NSAID) use found that after 13 months none of the patients on celecoxib in combination with a PPI had recurrent bleeding compared with 9 percent of patients on celecoxib and placebo [24].
21 D; Initiate omeprazole Question 8.

22 Manage short bowel syndrome with acid suppression therapy Likelihood or resuming an oral diet Amount of bowel remaining Type of bowel remaining Presence of a colon and ileocecal valve Intestinal adaptation Citrulline concentration < 20 micromol/liter predicts permanent intestinal failure 95% PPV, 86% NPV Treatment of short bowel syndrome PPI or H2 blocker for gastric acid suppression (oversecretors) Replacement of stomal/fecal fluid losses Electrolyte replacement Loperamide Thickeners
23 A; Endoscopic ablation Question 9.


24 Manage high grade dysplasia in a patient with Barrett esophagus American Gastrointestinal Association Guidelines 2011 for Management of High Grade Barrett s dysplasia is to undergo Endoscopic Ablation: Radiofrequency ablation Photodynamic Therapy Endoscopic mucosal resection NOT Esophagectomy! HIGH grade Barrett s without definitive treatment requires repeat surveillance in 3 months!
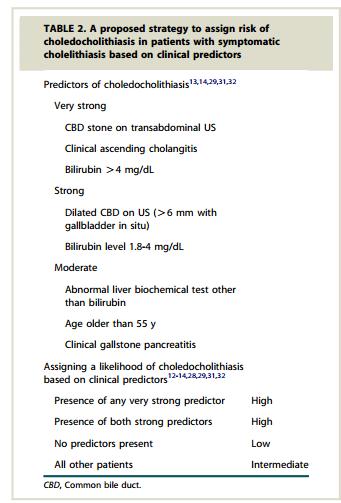
25 Question 10. C; Endoscopic retrograde cholangiopancreatography (ERCP)
26 Manage acute cholangitis Clinical Syndrome: Fever Abdominal Pain Jaundice Hypotension Altered mental status Diagnosis: Suspected: fever/rigors, labs consistent with inflammation, AND jaundice OR abnormal LFTs Definite: Suspected PLUS biliary dilation on imaging, or stone/stent/stricture Treatment: Obtain blood cultures Empiric antibiotics (E. coli, Klebsiella, Enterococcus, Anaerobes) ERCP within 24 hours MRCP if unsure or EUS if cannot perform MRCP
27
28 B; Infliximab Question 11.
29 Treat ulcerative colitis with the appropriate maintenance therapy Induce Remission (Mild to Moderate Dz): 5 ASA topical or systemic or both Topical steroids Prednisone for patients who fail the above therapies to induce remission; Steroid Dependent/ Steroid Refractory Prednisone mg q day until improvement, then taper 5 10 mg q week until 20 mg q day 3x risk of infection on steroids, bone disease, cataracts, hyperglycemia, etc Maintain Remission: TPMT deficiency: CANNOT use azathioprine or 6 MP ; neutropenia
30 B; Liver transplant evaluation Question 12.


31 Manage hepatocellular carcinoma in a patient who meets the Milan criteria Criteria For Liver Transplant for HCC Single Lesion 5 cm Up to 3 lesions, none larger than 3 cm No vascular invasion No regional node or extrahepatic distant metastases 5 year survival with transplant 75% or higher
32 E; Repeat upper endoscopy Question 13.
33 Diagnose the cause of obscure gastrointestinal bleeding with repeat upper endoscopy Causes of obscure GI blood loss:: Upper source 29 56% Lower source 20 30% Synchronous source 1 17% No source found 29 52% Age < 40 Small bowel tumors, celiac dz, Crohn Age > 40 Vascular ectasia, NSAID induced, celiac
34 D; Stop alcohol intake Question 14.
35 Evaluation of a patient for iron overload
36 Primary and Secondary Causes of Iron Overload
37 B; Crohn colitis Question 15.
38 Diagnosis of Crohn disease 80% involve small bowel Transmural inflammation 5 ASA tx ineffective Skip lesions, rectal sparing Mouth to anus Diagnose Crohn Colitis Assess severity clinically and endoscopically Crohn Disease Activity Index (CDAI)) Initiate treatment Step up vs. Top down ANTI TNF THERAPY WITH OR WITHOUT 6 MP OR AZATHIOPRINE RESULTED IN HIGHEST REMISSION RATES (SONIC trial; NEJM September,2010) Alternative is to start simultaneous azathioprine or 6 MP and steroids with goal of stopping steroids in 3 months
39 C; Primary biliary cirrhosis Question 16.
40 Diagnose Primary Biliary Cirrhosis Signs and Symptoms: Fatigue Pruritis Xanthomas/Xanthelasma Other autoimmune diseases Isolated elevated alkaline phosphatase Diagnosis: No extrahepatic biliary dilatation PLUS 2 of the following: Alkaline phosphatase 1.5 ULN Anti mitochondrial antibody 1:40 Liver biopsy consistent with destruction of biliary caniculi Treatment: Ursodeoxycholic acid
41 Question 17. A; Discharge home with close follow up
42 Manage acute diverticulitis Diverticulosis: Intrinsic weakness where vessel penetrates the colon wall Simultaneous or excessive haustral contractions Inadequate dietary fiber COMMON in Western populations 40% by age 60 and 60% by age 80 Diverticulitis: (fever, LLQ pain, WBC) (1 in 5 with diverticulosis): Uncomplicated Recurrent uncomplicated Complicated Smoldering CT is diagnostic test of choice Management decisions: Outpatient or inpatient Antibiotics (gm neg and anaerobes) Bowel rest *Following resolution (2 6 weeks later) the entire colon needs endoscopic evaluation to look for mimickers, ie. cancer/polyps Preventing future episodes: Surgical resection of diseased segment High fiber diet No association between seeds, nuts, or popcorn consumption
43 A; Acute mesenteric ischemia Question 18.
44 Diagnose acute mesenteric ischemia 1) Acute arterial mesenteric ischemia Pain out of proportion Afib, unanticoagulated Thromboembolus to SMA Known vasculopath High mortality: dead bowel 2) Chronic arterial mesenteric ischemia Hungry Afraid to eat due to pain Weight loss Known vasculopath 3) Subacute venous hypertension related mesenteric ischemia Unusual hypercoagulable state Polycythemia Vera, Paroxysmal Nocturnal Hemoglobinuria (PNH) Occlusive portal vein clot propagates to SMV 4) Colonic ischemia Elderly Hypotension /Dehydration event Mucosal ischemia especially watershed areas (splenic flexure and sigmoid) Increase perfusion pressure to treat; avoid hypotension No need for angiogram
45 D; Supportive care Question 19.
46 Manage acute diarrhea Definition: Acute < 14 days Chronic > 4 weeks Osmotic, secretory, inflammatory or malabsorptive Most acute cases of diarrhea are self limited and require no further evaluation FEATURES that require additional evaluation: Fever> 38.5 C (101.3 F) Bloody stool Pregnancy Elderly or immunocompromised Hospitalized Food handler Recent antibiotics Volume depleted Severe abdominal pain
47 Manage acute diarrhea Stool cultures: Immunocompromised, including HIV Bloody diarrhea Underlying IBD Food handlers Pregnant patients: Listeria is not found in stool cultures; only blood cultures!
48 D; Ultrasound of liver and spleen Question 20.
49 Manage nonalcoholic steatohepatitis 30% of adults in US have NAFLD 20% of patients with NAFLD have NASH Platelets are predictive of progression to cirrhosis <150,000/uL, confirm with ultrasound Risk factors for progession to cirrhosis: Age > 50 years Treatment for all: Weight loss Monitor AST/ALT q 3 6 months BMI > 28 Serum triglycerides >150 Statins are okay ALT > 2x ULN 3hLzaslo47TIANaSkvSZLQ8GVunRMpf6b AASLD Guidelines For Biopsy Proven NASH: Diabetics: Pioglitazone 45 mg/day (1B) Non diabetics: Vitamin E 800 U/ day (1B)
Western Health Specialist Clinics Access & Referral Guidelines
 Gastroenterology Specialist Clinics at Western Health: Western Health provides the following Specialist Clinics for patients who require assessment and management of Gastroenterology / Hepatology conditions.
Gastroenterology Specialist Clinics at Western Health: Western Health provides the following Specialist Clinics for patients who require assessment and management of Gastroenterology / Hepatology conditions.
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
DIY Tricks of the Trade
 DIY Tricks of the Trade Simple Solutions to Common GI Consultations Art DeCross MD AGAF Associate Professor of Medicine Division of Gastroenterology &Hepatology University of Rochester No Financial Disclosures
DIY Tricks of the Trade Simple Solutions to Common GI Consultations Art DeCross MD AGAF Associate Professor of Medicine Division of Gastroenterology &Hepatology University of Rochester No Financial Disclosures
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
8/29/2016 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW. LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES
 DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
DIVERTICULAR DISEASE: WHAT EVERY NURSE PRACTITIONER SHOULD KNOW LENORE LAMANNA Ed.D, ANP-C LEARNING OBJECTIVES Define Diverticular Disease Discuss Epidemiology and Pathophysiology of Diverticular disease
Chronic diarrhea. Dr.Nasser E.Daryani Professor of Tehran Medical University
 1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Management of the Hospitalized IBD Patient. Drew DuPont MD
 Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
Management of the Hospitalized IBD Patient Drew DuPont MD Ulcerative Colitis: Indications for Admission Severe ulcerative colitis Frequent loose bloody stools ( 6 per day) Severe cramps Systemic toxicity:
NEURO- GASTRO- ENTEROLOGY & MOTILITY OESO- PHAGUS LOGY. Room A Room B Room C Room E1 Room E2 Room M Room N1 Room N2 Room L8 Room 1.
 ONCO ENTERO RADIO & SATURDAY SUNDAY MONDAY TUESDAY WEDNESDAY Saturday, October 15, 2016 Room A Room B Room C Room E1 09:00-10:30 Peptic ulcer : Still important for gastroenterologists 11:00-13:00 Video
ONCO ENTERO RADIO & SATURDAY SUNDAY MONDAY TUESDAY WEDNESDAY Saturday, October 15, 2016 Room A Room B Room C Room E1 09:00-10:30 Peptic ulcer : Still important for gastroenterologists 11:00-13:00 Video
CHRONIC DIARRHEA DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS
 DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE THAN 4 WEEKS") DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 CHRONIC DIARRHEA DEFINITION: *LOOSE, WATERY STOOLS *MORE THAN 3 TIMES A DAY *FOR MORE
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
University Medical Center at Brackenridge. Gastroenterology Clinic Worksheet
 Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
Crohn's Disease. What causes Crohn s disease? What are the symptoms?
 Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Digestion: Small and Large Intestines Pathology
 Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Digestion: Small and Large Intestines Pathology Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one onone relationship with a qualified health
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Top 10 Things you need to know about IBD. Suresh Pola, MD Kaiser San Diego
 Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
Top 10 Things you need to know about IBD Suresh Pola, MD Kaiser San Diego Top 10 Things to Know: IBD What you can eat How to treat the pain Not all diarrhea is a flare Ways to reduce your risk of getting
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
Patient Name Date of Birth Age. Other phone ( ) . Other
 . Other") GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Gastroenterology Fellowship Program
 Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
The Primary Functional Diagnosis of the G.I. & Biliary System
 Functional Physiology, Dysfunctions, and Assessments of the G.I. and Gallbladder a 3-part Webinar Series The Functional Diagnosis Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software
Functional Physiology, Dysfunctions, and Assessments of the G.I. and Gallbladder a 3-part Webinar Series The Functional Diagnosis Webinars With DR. DICKEN WEATHERBY Creator of the Blood Chemistry Software
Gastroenterology and Feeding Issues in Fanconi Anemia
 Gastroenterology and Feeding Issues in Fanconi Anemia Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition August 12, 2012 GI problems in FA 5% have gastrointestinal tract
Gastroenterology and Feeding Issues in Fanconi Anemia Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition August 12, 2012 GI problems in FA 5% have gastrointestinal tract
LIVER SPECIALTY CONFERENCE USCAP Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA
 LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
LIVER SPECIALTY CONFERENCE USCAP 2016 Maha Guindi, M.D. Clinical Professor of Pathology Cedars-Sinai Medical Center Los Angeles, CA Nothing to disclose Case History 47-year-old male, long standing ileal
GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY
 Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
SIBO
 SIBO What is it? Small Intestinal Bowel Overgrowth A chronic bacterial infection of the small intestine Caused by bad bacteria such as E Coli and Clostridium migrating to the small intestine There is not
SIBO What is it? Small Intestinal Bowel Overgrowth A chronic bacterial infection of the small intestine Caused by bad bacteria such as E Coli and Clostridium migrating to the small intestine There is not
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
Serologic Markers CONVENTIONAL ANTIBODIES ANTIBODIES UNCONVENTIONAL. AIH Type I
 Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Bloating, Flatulence, and
 A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
Gastroenterology. 3. Which of the following clotting factors is dependent on Vitamin K? a) II b) VII c) IX d) X e) All of the above
 II b) VII c) IX d) X e) All of the above") Gastroenterology 1. Which one of the following is not a symptom of Vitamin A deficiency? a) Keratomalacia b) Poor wound healing c) Osteomalacia d) Night blindness 2. Which one of the following is not a
Gastroenterology 1. Which one of the following is not a symptom of Vitamin A deficiency? a) Keratomalacia b) Poor wound healing c) Osteomalacia d) Night blindness 2. Which one of the following is not a
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Irritable Bowel Syndrome vs Inflammatory Bowel Disease
 Irritable Bowel Syndrome vs Inflammatory Bowel Disease Lana Bistritz MD FRCPC Royal Alexandra Hospital Faculty/Presenter Disclosure Faculty: Lana Bistritz Relationships with financial sponsors: Grants/Research
Irritable Bowel Syndrome vs Inflammatory Bowel Disease Lana Bistritz MD FRCPC Royal Alexandra Hospital Faculty/Presenter Disclosure Faculty: Lana Bistritz Relationships with financial sponsors: Grants/Research
Gastrointestinal, Hepatic, and Nutritional Challenges in FA
 Gastrointestinal, Hepatic, and Nutritional Challenges in FA Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition June 29, 2014 GI problems in FA 5% have gastrointestinal tract
Gastrointestinal, Hepatic, and Nutritional Challenges in FA Sarah Jane Schwarzenberg, MD Pediatric Gastroenterology, Hepatology and Nutrition June 29, 2014 GI problems in FA 5% have gastrointestinal tract
2017 Canadian Association of Gastroenterology Educational Needs Assessment Report
 2017 Canadian Association of Gastroenterology Educational Needs Assessment Report Kevin A. Waschke MD., CM., FRCPC, FASGE VP Education Affairs, Canadian Association of Gastroenterology Karen Sparkes BASc
2017 Canadian Association of Gastroenterology Educational Needs Assessment Report Kevin A. Waschke MD., CM., FRCPC, FASGE VP Education Affairs, Canadian Association of Gastroenterology Karen Sparkes BASc
EVALUATION OF ABNORMAL LIVER TESTS
 EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
INFLAMMATORY BOWEL DISEASE
 National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
National University Faculty of Medicine INFLAMMATORY BOWEL DISEASE Gehan M. Osman, MD. MBBS Pediatrician Jaffar Ibn Auf Specialized Hospital EDUCATIONAL OBJECTIVES Definitions and spectrum of (IBD) Epidemiology
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
AAIM: GI Workshop Follow Up to Case Studies. Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease
 AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Pediatric Primary Sclerosing Cholangitis and Potential Therapies
 Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial
Pediatric Primary Sclerosing Cholangitis and Potential Therapies Philip Rosenthal, M.D. Professor of Pediatrics & Surgery University of California, San Francisco DISCLOSURE I have the following financial
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain
 Flexbook by Brian Lindshield is in the public domain") Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Clinical Evaluation of CHRONIC DIARRHEA. By Dr. Mohamed El-Awady
 Clinical Evaluation of CHRONIC DIARRHEA By Dr. Mohamed El-Awady Definition Stool weight of more than 300 gm / 24 h more than 4 weeks (Feldman et al 2002) CLINICAL CLASSIFICATION 1) Large-Volume Versus
Clinical Evaluation of CHRONIC DIARRHEA By Dr. Mohamed El-Awady Definition Stool weight of more than 300 gm / 24 h more than 4 weeks (Feldman et al 2002) CLINICAL CLASSIFICATION 1) Large-Volume Versus
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
2017 NEEDS ASSESSMENT SURVEY
 2017 NEEDS ASSESSMENT SURVEY Quick Overview: Educational Topic Findings The online 2017 Needs Assessment survey was programmed through SurveyMonkey and a personalized request to complete the questionnaire
2017 NEEDS ASSESSMENT SURVEY Quick Overview: Educational Topic Findings The online 2017 Needs Assessment survey was programmed through SurveyMonkey and a personalized request to complete the questionnaire
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease When is diarrhea not just diarrhea?
 Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Inflammatory Bowel Disease When is diarrhea not just diarrhea? Jackie Kazik, MA, PA C CME Resources CAPA Annual Conference, 2011 Inflammatory Bowel Disease Objectives Discuss what is known about the pathophysiology
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
ACG Clinical Guideline: Primary Sclerosing Cholangitis
 ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Patient Interview Form
 Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
ABNORMAL LIVER FUNCTION TESTS. Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust
 ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Internal Medicine Jeopardy Game
 Internal Medicine Jeopardy Game Ziad Mattar, M.D. Chief Medical Resident University of Toledo Single Double Date Final Single Diarrhea GERD Urgent Matters Gallery Action & Reaction 100 100 100 100 100
Internal Medicine Jeopardy Game Ziad Mattar, M.D. Chief Medical Resident University of Toledo Single Double Date Final Single Diarrhea GERD Urgent Matters Gallery Action & Reaction 100 100 100 100 100
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
General and Colonoscopy Data Collection Form
 Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما
 بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
بسم الله الرحمن الرحيم أوتيتم من العلم إال قليال وما 1 2 Goals of the Lecture: What is the portal vein? How common is PVT? What conditions are associated with PVT? How does patient with PVT present? How
INFLAMMATORY BOWEL DISEASE
 1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
The Road to Remission
 The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
The Road to Remission Understanding, Treating and Living with Inflammatory Bowel Disease IBDCenterOrlando.com As many as 1.5 million Americans currently suffer from inflammatory bowel disease (IBD), and
Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews
 Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews DR. NILESH CHANDE COORDINATING EDITOR, IBD REVIEW GROUP; UNIVERSITY OF WESTERN ONTARIO, LONDON, ON CANADA An international organisation
Controversies in IBD: Resolving clinical dilemmas using Cochrane reviews DR. NILESH CHANDE COORDINATING EDITOR, IBD REVIEW GROUP; UNIVERSITY OF WESTERN ONTARIO, LONDON, ON CANADA An international organisation
Improving outcome of Inflammatory Bowel Disease in children
 Improving outcome of Inflammatory Bowel Disease in children Dinesh Pashankar, MD Pediatric Gastroenterologist Director- Pediatric IBD program Yale University School of Medicine Pediatric Gastroenterology
Improving outcome of Inflammatory Bowel Disease in children Dinesh Pashankar, MD Pediatric Gastroenterologist Director- Pediatric IBD program Yale University School of Medicine Pediatric Gastroenterology
PATIENT HISTORY FORM
 PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
CASE STUDY: ULCERATIVE COLITIS. Sammi Montag Dietetic Intern
 CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
CASE STUDY: ULCERATIVE COLITIS Sammi Montag Dietetic Intern 2013-2014 PATIENT (CK) INTRODUCTION 26 year old female Chief complaint: bloody diarrhea and abdominal pain Admitting diagnosis: Ulcerative colitis
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery