Review of Urinary Tract Infection
|
|
|
- Augustine Mason
- 5 years ago
- Views:
Transcription
1 Review of Urinary Tract Infection Anthony P. Buonanno, Jr., MD Lehigh Area Medical Associates, Allentown, Pennsylvania Clinical Assistant Professor of Internal Medicine, Penn State University, Hershey, Pennsylvania Brian J. Damweber, MPAS, PA-C Lehigh Area Medical Associates, Allentown, Pennsylvania US Pharm. 2006;6:HS-26-HS-36. Urinary tract infection (UTI) - a broad term used to describe bacterial infection of the urethra, bladder, and kidneys--is a problem frequently encountered by health care providers today. In addition to bacteria, viruses and fungi are other infectious agents that colonize the urinary tract. Traditionally, UTIs are categorized as uncomplicated or complicated, or by site of infection. Infections may be symptomatic or asymptomatic. Lower UTIs include urethritis and cystitis, and upper tract infections include pyelonephritis and renal abscesses. Acute infections are usually associated with a single pathogen; chronic infections are usually polymicrobial. The economic impact of bacterial UTIs is a major factor affecting health care expenses today. Both outpatient and inpatient treatment contribute to overall costs. The urinary tract is the most common site of hospital infection, accounting for more than 40% of nosocomial infections (estimated to be 600,000 patients per year) reported by acute care hospitals. 1 The vast majority of hospital-acquired infections are due to indwelling catheters. On average, a hospitalacquired UTI increases length of stay by one day, resulting in nearly one million extra hospital days. The economic impact is between $424 million and $451 million annually. 2 UTI accounts for approximately eight million health care provider visits in the United States. More than 100,000 hospitalizations per year are due to infections of the urinary tract. Uncomplicated cystitis is by far the most common outpatient infection, while pyelonephritis accounts for the majority of inpatient visits. 3 Diagnosis of UTIs accounts for an estimated $6 billion in health care expenditures. 4 Epidemiology Nearly half of all women will have a UTI once in their lives. 5 It has been reported that one third of women will have had at least one UTI by age 24 years. 6 Simple, uncomplicated UTIs are quite common in women ages 20 to 50. The geriatric community is frequently affected by these infections. Notably, these infections often do not cause symptoms.7 UTIs are the second most common type of infection in the geriatric population, accounting for nearly 25% of all infections in the elderly. 6 Fifty percent of elderly women are affected by asymptomatic bacteriuria. In many cases, bladder catheriterization is a contributing factor; 38% of chronic care residents require bladder catheterization, a cause for the increasing incidence of UTIs in the elderly. 8 The pediatric population is also affected by UTIs. Bacteriuria is present in 2.7% of boys and 0.7% of girls. 9 Uncircumcised males have a higher incidence of infection. Uncircumcised infants younger than 6 months have a higher incidence of gram-negative uropathogens. 6 The rate of hospital admission is higher in uncircumcised boys, since this population has a 12-fold increased UTI risk. 10 A study by Nuutinen and Uhari found that 35% of boys and 32% of girls who had their first UTI before age 1 contracted a recurrent UTI during the next three years. 11
2 Other risk factors for exposure in infants are hospitalization and catheterization. Children between ages 1 and 5 years have a 4.5% increased incidence of bacteriuria. Pathophysiologic Considerations Transitional epithelium transports urine from the kidneys to an elastic bladder. The bladder stores large volumes of urine at low pressures. 12 The incidence of cystitis is greater in women, primarily due to the proximity of the urethral opening to the vagina and perianal area. Risk factors for UTIs in women include fecal contamination, recent UTI, decreased fluid intake, irregular emptying, sexual intercourse, diaphragm and/or spermicide use, a symptomatic partner, pregnancy, menopause, low vaginal ph or dryness of mucosa, neurogenic bladder, renal disease, urologic anatomic abnormalities, instrumentation, immunosuppression, hospitalization, nephrolithiasis, and diabetes. 5 UTIs are less likely to occur in men under 50 years of age. Unlike female anatomy, the male urethra is separated from the rectum by several centimeters and is keratinized by squamous epithelium. The incidence of UTI becomes similar in men and women at age 65, given the increased proportion of men with benign prostatic hypertrophy. 12 Approximately one fifth of men in their 70s have experienced a UTI. 13 Other risk factors for men include urologic abnormalities, neurogenic bladder, instrumentation, anal intercourse, and immunosuppression 5 Immunosuppressed states in males and females include age, diabetes, multiple sclerosis, HIV, and other chronic illnesses that may impair the immune system. For the diabetic patient, the risk of UTI is greater in females than in males. Diabetic patients generally seem to have a twofold to fourfold increased incidence of bacteriuria, 13 leading to a higher incidence of pyelonephritis. Symptoms of UTI are similar among the sexes: Dysuria (painful urination), urgency, hesitancy, polyuria, and incomplete voiding may all be associated with acute cystitis. Urinary incontinence, hematuria, and suprapubic or low back pain may also be present. Typically, females with acute dysuria have one of three types of infections: acute cystitis; acute urethritis due to Chlamydia trachomatis, Neisseria gonorrheae, or herpes simplex virus; or vaginitis due to Candida or Trichomonas. Symptoms that indicate pyelonephritis include fever, costovertebral angle pain, nausea, and vomiting. Hematuria may occur in any UTI, but it is more suggestive of nephrolithiasis when accompanied by flank pain. In the pediatric population during the first 8 to 12 weeks of life, UTI may be associated with bacteremia. Symptoms in infants up to 2 years old may include difficulty with feeding, nausea and vomiting, or failure to thrive. Children ages 2 to 5 may demonstrate fever and abdominal pain. Children under 5 are at risk for renal scarring.14 Children older than 5 may have the same symptomatology as adults. As many as 25% of young children without pyelonephritis have renal bacteriuria. 15 As in other age groups, urine culture is the goal standard for diagnosis of UTI. However, an adequate sterile urine culture is often difficult to obtain in the pediatric patient. The urinalysis will support the presumptive diagnosis of UTI. Markers for infection in a urinalysis are the presence of nitrites, leukocytes esterase, bacteria, or white blood cells. 16 An infant who is evaluated for fever may require lumbar puncture, in addition to blood cultures, to evaluate UTI with secondary bacteremia.
3 Diagnosis The diagnoses for acute pyelonephritis, cystitis, and asymptomatic bacteriuria are made by the presence of bacteria in the urine, usually based on a clean midstream urine sample. There must be a minimum of 105 colony-forming units per milliliter (cfu/ml) of uropathogens for diagnosis of acute pyelonephritis and asymptomatic bacteriuria but only 103 cfu/ml for the diagnosis of cystitis. Up to one third of cystitis cases would be missed if the criterion for diagnosis were the same as that for upper tract infections. 17 Uncomplicated UTI refers to cystitis and pyelonephritis that occurs in young, healthy, nonpregnant, or ambulatory postmenopausal women--all of whom have an anatomically and functionally normal urinary tract. Patients with complicated UTIs are those who have an associated risk for infection in the urinary tract (e.g., those with neurogenic bladder, nephrolithiasis, hospital-acquired infection, diabetes, indwelling catheters, or who are immunosuppressed). Resistant organisms can be seen in either complicated or uncomplicated UTIs. 17 Because UTIs occur in young healthy men infrequently, there is debate whether to consider these infections complicated or uncomplicated, given the paucity of studies in this patient group. The organisms and sensitivity patterns seem to be the same as in women with uncomplicated cystitis. Empiric treatment for cystitis would utilize the same antibiotic choices used in women, but three-day regimens are not recommended because of the lack of supporting data. A pretreatment urine culture should be obtained in all men with UTI; however, a posttreatment culture is usually not necessary. Recurrent infections require evaluation for prostatitis, and if negative, an evaluation for anatomic abnormalities should ensue. 17 In practicality, using bacteriuria for the diagnosis of cystitis can be cumbersome, since urine culture is not performed in many cases of uncomplicated cystitis. Urine microscopy has a low sensitivity (40% to 70%) but a high specificity (85% to 95%) for the diagnosis of UTI. Pyuria is present in most cases of pyelonephritis--estimated to be about 90%. Presence of pyuria increases the sensitivity (95%) and specifity (71%) for the diagnosis of acute pyelonephritis. White cell casts always point to an upper tract infection.18 Urine culture is positive in 90% of cases of pyelonephritis, and 20% of hospitalized cases have positive blood cultures. The cultures were obtained prior to antibiotic therapy in these cases. There is no evidence that positive blood cultures indicate a more complicated course in immunocompetent individuals. 19 Dipstick urinalysis has become the most frequently used test due to its cost and fast results. Studies have shown that dipstick urinalysis, in combination with clinician judgment, greatly improves diagnostic accuracy in the patient with nonspecific symptoms. Urine dipstick is positive if there is a presence of nitrate and/or if there is a positive reaction greater than or equal to trace leukocyte esterase. 20 Patients should be screened for asymptomatic bacteriuria in cases of pregnancy or prior to a urologic procedure or surgery. Urine culture is the method of choice, since the other types of studies lack the sensitivity and specificity in these cases. During pregnancy, UTIs are common in the sixth week and peak during weeks 22 to 24. Pregnant women have a prevalence of asymptomatic bacteriuria of 2% to 7%. If untreated, 20% to 30% of these women will develop acute pyelonephritis later in pregnancy. When pyelonephritis occurs late in pregnancy, there is an association with preterm labor. Treatment has been shown to decrease this risk by 90%.
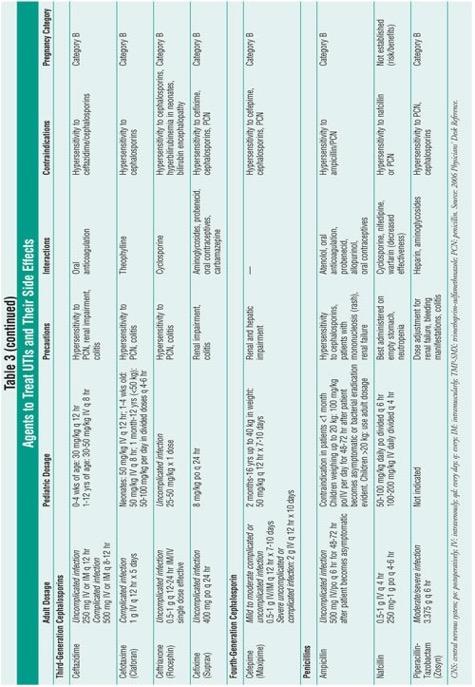
4 The current recommendation by the Infectious Diseases Society of America is to obtain a urine culture at the end of the first trimester, and if positive, to treat the bacteriuria. Intrauterine growth retardation and neonatal death have also been linked to asymptomatic bacteriuria. There are no indications for screening elderly patients in the community or in institutions for asymptomatic bacteriuria, as treatment has not been shown to benefit these individuals. 21 Imaging The diagnosis of pyelonephritis can usually be made by history, physical examination, and laboratory tests. Imaging may be necessary when the diagnosis is in question, when there are recurrent infections, or if the patient responds poorly to appropriate antibiotic therapy after three days. Computed tomography (CT) with intravenous (IV) contrast is the test of choice when evaluating the urinary tract. The most common CT finding in pyelonephritis is wedgeshaped lesions of decreased attenuation with or without swelling. Anatomic abnormalities and perinephric abscesses can also be seen on contrast-enhanced scans. Renal ultrasound is also used to evaluate the collecting system and pyelonephritis and may show ureteral dilation, suggesting obstruction. Although renal ultrasound is helpful, a CT scan is more sensitive. Magnetic resonance imaging may be used in patients who are allergic to iodinated contrast.22 Diagnostic studies for UTI in pediatric patients are important, given the potential long-term sequelae associated with undiagnosed or recurrent UTIs. Recurrence may be a marker for genitourinary abnormalities, and imaging is recommended after the first infection with concomitant fever. Vesicoureteral reflux encompasses a variety of conditions that represent the most common abnormality observed in infants and young children. This condition can lead to recurrent UTIs, resulting in secondary scarring that causes an increased risk of progression to renal disease into adulthood. Children with poor clinical response to appropriate treatment should have immediate renal and bladder ultrasound (RBUS) and voiding cystourethrography (VCUG). 23 Treatment Prevention of UTI is always the goal of clinicians. There are many proven and unproven strategies to accomplish this task (see table 1). Most UTIs will clear spontaneously if untreated, but symptoms may persist for a significantly longer period of time. Tables 2 and 3 review first-line and alternative treatments for UTI, outlining the adverse effects of each agent. In one study, one in 38 women progressed from uncomplicated cystitis to pyelonephritis without treatment. 17 The most common organisms by far are gram-negative bacilli. Escherichia coli causes 80% of all community-acquired UTIs among otherwise healthy individuals, and roughly half of UTIs occur in hospitalized patients and diabetic patients. 2 Other bacteriuria include gram-negative rods such as Proteus, Klebsiella, and Enterobacter. Antibiotic resistance has become an important factor to consider in the treatment of infections. Resistance may occur in ambulatory, institutionalized, and hospitalized infections. E. coli resistance has been progressing for more than a decade. 24
 has been significant, and therefore, it is no longer the first therapeutic choice in complicated UTI or pyelonephritis.")

5 !! E. coli Resistance: The resistance pattern is not uniform in the U.S.; in 2000, it ranged from 10% in the Northeast to 22% in the West. 25 The resistance to trimethoprim-sulfamethoxazole (TMP-SMX) has been significant, and therefore, it is no longer the first therapeutic choice in complicated UTI or pyelonephritis. Given the concern of resistance progressing with the fluoroquinolones, TMP-SMX remains first-line therapy for the most common uncomplicated cystitis.24 Fluoroquinolones are the primary therapy for complicated cystitis and acute pyelonephritis. There is still relatively low resistance to fluoroquinolones for E. coli, but resistance is significantly emerging with enterococci. Tendonitis and, rarely, Achilles heel rupture in the geriatric population have been noted with the quinolones. 26 Nitrofurantoin is associated with low levels of E. coli resistance, which is theorized to be due to its multiple mechanisms of action, but the agent has poor tissue and plasma concentration. Thus, nitrofurantoin has no use beyond the urinary tract.24 Beta-lactams have significant problems with resistance--up to 40% in Fosfomycin is indicated only for uncomplicated cystitis and has low reported resistance. 24
6 Urinary Catheters: Any catheterization of the bladder increases the risk of infection, but indwelling has a higher risk than intermittent catheterization. Treatment of asymptomatic bacteriuria in patients with chronic indwelling catheters has shown no benefit. 21 When a patient becomes symptomatic, blood and urine cultures should be obtained prior to treatment. Antibiotics should be initiated immediately after cultures and should be tailored to the patient, institution, and susceptibility patterns. Cystitis: For uncomplicated cystitis in women, a three-day course of TMP-SMX is recommended; if the patient is older, a longer course of therapy (seven to 10 days) should be considered. This recommendation applies to areas where E. coli resistance is less than 20%. Studies have examined three-day courses of ciprofloxacin versus TMP-SMX, and the results of bacteria eradication were similar in uncomplicated cystitis. If the patient is allergic to sulfa, alternative therapies are nitrofurantoin for seven days or single-dose fosfomycin. Fluoroquinolones are first-line therapy in areas where E. coli resistance is greater than 20%. 27 In pregnant patients with cystitis, a seven-day duration is preferred for nitrofurantoin or cephalexin. However, fosfomycin in a single dose is another alternative. 27 Women with recurrent bouts of cystitis may need to consider an alternative form of contraception. Spermicides and diaphragms may predispose women to infection. Postcoital prophylaxis should be instituted only after the current infection is treated and a negative urine culture is obtained. Single-dose TMP-SMX, nitrofurantoin, or fluoroquinolones can be used after intercourse. 18 Complicated Cystitis: In complicated UTIs, a wide range of bacteria can cause infection. Fluoroquinolones are effective first-line treatment, given their broad spectrum of coverage for mild to moderate infections. For more seriously ill, hospitalized patients, initial empiric therapy includes ampicillin and gentamicin. Alternative choices of antimicrobials are third-generation cephalosporins, pipercillin-tazobactam, meropenem, or ciprofloxacin, based on sensitivities. The expected length of treatment for complicated UTIs is 10 to 14 days. Switching from IV to postoperative coverage largely depends on clinical improvement. Pseudomonas and Enterococcus are difficult to treat and may require a longer course of IV antibiotics. Repeat cultures are recommended one to two weeks after the completion of therapy. If a patient fails to respond to treatment, repeat cultures should be attained along with imaging studies to rule out persistent infection secondary to anatomic abnormalities or stone disease. 28 Most complicated UTIs are nosocomial in origin. The most common pathogens are gramnegative bacteria, which have been shown to colonize the meatus. Hand washing and good aseptic technique are imperative in preventing infection. Practitioners must be cautious when determining the need for indwelling Foley catheters. Intermittent catheterization reduces the risk of bacteriuria. If a chronic indwelling Foley catheter is indicated, then the catheter should be changed at least once every 30 days. Perinephric abscess is considered a complicated UTI. The most common causative organism is Staphylococcus aureus. First-line treatment is IV nafcillin or a third-generation cephalosporin. Vancomycin may be used as an alternative. In most cases, patients will need surgical intervention or aspiration of the infected fluid collection. 29
7 Acute Pyelonephritis: Many patients with pyelonephritis need to be hospitalized. (See Table 4 for indications.) Patients who do not meet absolute indications for hospitalization are treated successfully in about 90% of cases with outpatient oral regimens. After the urine culture is obtained, empiric therapy consists of an oral fluoroquinolone for outpatient treatment. Patients requiring hospitalization should receive an IV fluoroquinolone or an aminoglycoside alone or in combination with an extended-spectrum cephalosporin or ampicillin. Oral treatment may be instituted once the patient is afebrile, clinically improved, and able to tolerate oral medications and hydration. 19 The duration of therapy in pyelonephritis is controversial. In acute, uncomplicated pyelonephritis, therapy duration ranges from seven to 14 days. Beta-lactams generally require 10 to 14 days, while the more common fluoroquinolones or TMP-SMX can require a duration of seven to 10 days. Complicated pyelonephritis may require a longer course of treatment, especially if the patients are immunocompromised. Generally, these patients require 14 to 21 days of therapy or even longer depending on their clinical course. 17 Pediatric Population Group B streptococcus is the most common organism seen in neonates. Overall, E. coli is the most typical organism found in the pediatric population, accounting for 75% to 90% of all cases. Hospitalized children may require frequent catheterizations, making Enterococcus and Pseudomonas a possible consideration. 30 Management of UTI in the neonatal population is largely geared toward preventing bacteremia, given the high risk of meningitis in this age group. Another goal in the treatment of pediatric patients is prompt diagnosis and empiric treatment to prevent progression of renal disease and to identify any urinary tract abnormalities. 15 Infants and children younger than 5 years of age should be hospitalized if the clinical suspicion is high for systemic infection. According to the American Academy of Pediatrics (AAP), hospitalization should also be considered if noncompliance is a concern, if outpatient treatment has failed, or if the patient is immunocompromised. A hospitalized patient who remains afebrile for 48 hours and tolerates oral antibiotics may be discharged with continued therapy on oral antibiotics. Once the infection has cleared, additional tests may be required to rule out abnormalities of the urinary tract (RBUS and VCUG). 23 The choice of antimicrobial depends on a number of different factors, such as the patient's clinical status, age (which may be associated with specific pathogens), and local sensitivity patterns in the area of practice.15 For neonates with a diagnosis of UTI and hydronephrosis, amoxicillin is recommended at one third of the normal dosage. 31 Sulfamethoxazole, TMP- SMX, or cephalosporins are beneficial first-line choices for children who are able to tolerate oral medications. 32 In children who have failed oral therapy, ceftriaxone or gentamicin administered intramuscularly has been shown to be effective in treating UTI. 23 The AAP recommends seven to 10 days of treatment for uncomplicated UTIs. For febrile infants with a UTI and children with presumed pyelonephritis, a 14-day course of therapy is recommended. Prophylactic antimicrobials may be used in children with symptomatic UTIs with anatomic abnormalities. There are few data to support the use of antibiotics in children without anatomic anomalies. 33

8 !
9 !

10 ! References 1. Centers for Disease Control and Prevention. Guideline for the Prevention of catheter-associated Urinary Tract Infections. Available at: 2. Brown P, Foxman B. Epidemiology of urinary tract infections transmission and risk factors, incidence and costs. Infec Dis Clin N Am. 2003;17: IDSA Practice Guidelines for antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in women. Available at: 4. Stamm WE, Norrby SR. Urinary tract infections: Disease panorama and challenges. J Infec Dis. 2001;183:S1. 5. Green MB, Bailey PP. Infectious processes: Urinary tract infections and sexually transmitted diseases. In: Buttaro TM, Trybulski J, Bailey PP, Sandberg-Cook J, eds. Primary Care: A Collaborative Practice. St. Louis, MO: Mosby; Foxman B. Epidemiology of urinary tract infections: incidence, morbidity and economic costs. Am J Med. 2002;113: NCHS: Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, Vital and Health Statistics Series 1999:13(143). 8. Warren, JW, Steinberg, L, Hebel, JR, et al. The prevalence of urinary catheterization in Maryland nursing homes. Arch Intern Med. 1989:149: Wettergren B, Jodal U, Jonasson G. Epidemiology of bacteriuria during the first year of life. Acta Paediatr Scand. 1995;74: To T, Agha M, Dick PT, Feldman W. Cohort sudy on the circumcision of newborn boys and subsequent risk of urinary tract infection. Lancet. 1998;352: Nuutinen M, Uhari M. Recurrence and follow-up after urinary tract infection under the age of 1 year. Pediatric Nephrology. 2001;16: Hooten TM, Scholes D, Hughes JP, et al. A prospective study of risk factors from symptomatic urinary tract infections in young women. N Engl J. Med. 1996;335:
11 13. Ronald A, Ludwig E. Urinary tract infections in adults with diabetes. Int J Antimicrobial Agents. 2001;17: MacNeily AE. Pediatric urinary tract infections: current controversies. Canadian J Urol. 2001;8: Schlager TA. Urinary tract infections in infants and children. Infec Dis Clin N Am. 2003;17: Layton KL. Diagnosis and management of pediatric urinary tract infections. Clin Fam Practice. 2003;5: Hooten T. The current management strategies for community-acquired urinary tract infection. Infect Dis Clin N Am. 2003;17: Fihn S. Acute uncomplicated urinary tract infection in women. N Engl J Med. 2003;349: Ramakrishnan K, Scheid D. Diagnosis and management of acute pyelonephritis in adults. Am Fam Physician. 2005;71: Sultana R, Zalstein S, Cameron P, Campbell D. Dipstick urinalysis and the accuracy of the clinical diagnosis of urinary tract infection. J Emerg Med. 2001;20: Nicolle L. Asymptomatic bacteriuria: When to screen and when to treat. Infec Dis Clin N Am. 2003;17: Kawashima A, Leroy A. Radiologic evaluation of patients with renal infections. Infec Dis Clin N Am. 2003;17: Shortliffe L, McCue J. Urinary tract infection at age extremes: pediatrics and geriatrics. Am J Med. 2002;133: Gupta K. Emerging antibiotic resistance in urinary tract pathogens. Infec Dis Clin N Am. 2003;17: Gupta K, Sahm DF, et al. Antimicrobial resistance among uropathogens that cause community acquired urinary tract infections in women: a nationwide analysis. Clin Infec Dis. 2001;33: Gold L, Igra H. Levofloxacin-induced tendon rupture: A case report and review of the literature. J Am Board Fam Practice 2003;16: Mehnert-Kay S. Diagnosis and management of uncomplicated urinary tract infections. Am Fam Physician. 2005;72: Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med. 1993;329: Sanford Guide for Microbiology; Perinephric Abscess, 2005: Elder JS. Urinary tract infections. In: Behrman RE, Kliegman FM, Jenson HB, eds. Nelson Textbook of Pediatrics. Philadelphia, PA: W.B. Saunders; 2000: Caldemone A. Antibiotic prophylaxis for infants with congenital hydronephrosis [letter]. Pediatric Infec Dis J. 1999;18: American Academy of Pediatrics. Subcommittee on Urinary Tract Infection. Practice parameter: diagnosis, treatment, and evaluation of urinary tract infection in infants and young children. Pediatrics. 1999;103: Dagan R, Phillip M, Watemberg NM, et al. Outpatient treatment of serious community-acquired pediatric infections using once daily intramuscular ceftriaxone. Pediatric Infec Dis J. 1987;6: UrologyHealthChannel. Available: Lynch D. Cranberry for prevention of urinary tract infections. Am Fam Physician. 2004;70:
Urinary tract infection. Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine
 Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
Urinary tract infection Mohamed Ahmed Fouad Lecturer of pediatrics Jazan faculty of medicine Objectives To differentiate between types of urinary tract infections To recognize the epidemiology of UTI in
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys.
 UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
UTI are the most common genitourinary disease of childhood. The prevalence of UTI at all ages is girls and 1% of boys. 1-3% of Below 1 yr. male: female ratio is 4:1 especially among uncircumcised males,
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
Urinary tract infections, renal malformations and scarring
 Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Treatment Regimens for Bacterial Urinary Tract Infections. Characteristic Pathogen. E. coli, S.saprophyticus P.mirabilis, K.
 HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela
 Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Diagnostic approach and microorganism resistance pattern in UTI Yeva Rosana, Anis Karuniawati, Yulia Rosa, Budiman Bela Microbiology Department Medical Faculty, University of Indonesia Urinary Tract Infection
Lecture 1: Genito-urinary system. ISK
 Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
Urinary Tract Infections Lecture 1: Genito-urinary system. ISK 07 08 2009. Getting Clear on the Terminology UTI Cystitis Urosepsis Asymptomatic Bacteriuria Asymptomatic UTI Pyuria Symptomatic UTI Pylonephritis
Pediatric urinary tract infection. Dr. Nariman Fahmi Pediatrics/2013
 Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
Pediatric urinary tract infection Dr. Nariman Fahmi Pediatrics/2013 objectives EPIDEMIOLOGY CAUSATIVE PATHOGENS PATHOGENESIS CATEGORIES OF URINARY TRACT INFECTIONS AND CLINICAL MANIFESTATIONS IN pediatrics
It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra
 UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
UTI Dr jayaprakash.k.p,asst prof,ich,govt.medical college,kottayam What is UTI? It is an infection affecting any of the following parts like kidney,ureter,bladder or urethra What is prevalence of UTI?
SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL
 URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
URINARY TRACT INFECTION SHABNAM TEHRANI M.D., MPH ASSISTANT PROFESSOR OF INFECTIOUS DISEASESE &TROPICAL MEDICINE RESEARCH CENTER, SHAHID BEHESHTI UNIVERSITY OF MEDICAL SCIENCES Definition inflammatory
11/15/2010. Asymptomatic Bacteriuria UTI. Symptomatic UTI. Asymptomatic UTI. Cystitis. Pylonephritis. Pyuria. Urosepsis
 Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
Urinary Tract Infections Renal vein Inferior vena cava Urinary bladder Urethra Renal artery Kidney Aorta Ureter Lecture 1: Genito-urinary system. 06 08 2010. (a) Sherwood Fig. 12-6a, p.530 An introduction
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE)
") KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
TMP/SMZ DS Ciprofloxacin Norfloxacin Ofloxacin Cefadroxil * 30 Amoxicilin 86* 19 25
 Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
Anatomy kidney ureters bladder urethra upper lower
 Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
Urinary tract Anatomy The urinary tract consists of the kidney, ureters, bladder, and urethra. Urinary tract infections can be either: upper or lower based primarily on the anatomic location of the infection.
ASPIRES Urinary Tract Infection Algorithm
 ASPIRES Urinary Tract Infection Algorithm Dr. Jennifer Grant Dr. Tim Lau Donna Leung February 2013 VCH Antimicrobial Stewardship 1 Programme: Innovation, Research, Education & Safety KEY PRINCIPLES 1.
ASPIRES Urinary Tract Infection Algorithm Dr. Jennifer Grant Dr. Tim Lau Donna Leung February 2013 VCH Antimicrobial Stewardship 1 Programme: Innovation, Research, Education & Safety KEY PRINCIPLES 1.
Urinary Tract Infections: From Simple to Complex. Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014
 Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
UTI Update: Have We Been Led Astray? Disclosure. Objectives
 UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
UTI Update: Have We Been Led Astray? KAAP Sept 28, 2012 Robert Wittler, MD 1 Disclosure Neither I nor any member of my immediate family has a financial relationship or interest with any entity related
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
Diagnosis and Management of UTI s in Care Home Settings. To Dip or Not to Dip?
 Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST
 RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST MUST KNOW PROF. MD. ENAMUL KARIM Professor of Medicine Green Life Medical College INTRODUCTION Urinary tract infection (UTI) is one of the commonest
RECURRENT URINARY TRACT INFECTIONS: WHAT AN INTERNIST MUST KNOW PROF. MD. ENAMUL KARIM Professor of Medicine Green Life Medical College INTRODUCTION Urinary tract infection (UTI) is one of the commonest
P. Brandstrom has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 P. Brandstrom has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylaxis or not? Per Brandström Queen Silvia Children s Hospital Gothenburg
P. Brandstrom has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylaxis or not? Per Brandström Queen Silvia Children s Hospital Gothenburg
Bacterial Infections of the Urinary System *
 OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
OpenStax-CNX module: m64804 1 Bacterial Infections of the Urinary System * Douglas Risser This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 1 Learning
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile in urinary bladder.. It contains fluids,
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acinetobacter baumannii, carbapenem-resistant, 497 498 Adolescents, urinary tract infections in, 520 521 Aminoglycosides, for UTIs and
Index Note: Page numbers of article titles are in boldface type. A Acinetobacter baumannii, carbapenem-resistant, 497 498 Adolescents, urinary tract infections in, 520 521 Aminoglycosides, for UTIs and
OCTOBER 2017 DRUG ANTIBIOTICS. Presence of bacteria in the urine with no symptoms or clinical signs.
 OCTOBER 2017 DRUG ANTIBIOTICS This optimal usage guide is mainly intended for primary care health professionnals. It is provided for information purposes only and should not replace the clinician s judgement.
OCTOBER 2017 DRUG ANTIBIOTICS This optimal usage guide is mainly intended for primary care health professionnals. It is provided for information purposes only and should not replace the clinician s judgement.
Paediatrica Indonesiana. Urine dipstick test for diagnosing urinary tract infection
 Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Paediatrica Indonesiana VOLUME 53 November NUMBER 6 Original Article Urine dipstick test for diagnosing urinary tract infection Syarifah Julinawati, Oke Rina, Rosmayanti, Rafita Ramayati, Rusdidjas Abstract
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase
 By Dr. Lindokuhle Mahlase") UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
Asyntomatic bacteriuria, Urinary Tract Infection
 Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Device-associated Events Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of
Medical Management of childhood UTI and VUR. Dr Patrina HY Caldwell Paediatric Continence Education, CFA 15 th November 2013
 Medical Management of childhood UTI and VUR Dr Patrina HY Caldwell Paediatric Continence Education, CFA 15 th November 2013 Terminology According to the current ICCS terminology guidelines Bladder and
Medical Management of childhood UTI and VUR Dr Patrina HY Caldwell Paediatric Continence Education, CFA 15 th November 2013 Terminology According to the current ICCS terminology guidelines Bladder and
An update on the management of urinary tract infection. Citation Hong Kong Practitioner, 1997, v. 19 n. 3, p
 Title An update on the management of urinary tract infection Author(s) Chan, TM Citation Hong Kong Practitioner, 1997, v. 19 n. 3, p. 137-141 Issued Date 1997 URL http://hdl.handle.net/10722/45038 Rights
Title An update on the management of urinary tract infection Author(s) Chan, TM Citation Hong Kong Practitioner, 1997, v. 19 n. 3, p. 137-141 Issued Date 1997 URL http://hdl.handle.net/10722/45038 Rights
Lower Urinary Tract Infection (UTI) in Males
 in Males") Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
Lower Urinary Tract Infection (UTI) in Males Clinical presentation For patients in care homes see UTI in adults where IV Antibiotics in the community may be appropriate (under development) History and
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018
 When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs
 ASCENSION TEXAS No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs Austin Area Society of Health-System Pharmacists April 26, 2018 Amy Carr, PharmD PGY-2 Infectious Diseases Pharmacy
ASCENSION TEXAS No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs Austin Area Society of Health-System Pharmacists April 26, 2018 Amy Carr, PharmD PGY-2 Infectious Diseases Pharmacy
Urinary tract infections Dr. Hala Al Daghistani
 Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
Urinary tract infections Dr. Hala Al Daghistani UTIs are considered to be one of the most common bacterial infections. Diagnosis depends on the symptoms, urinalysis, and urine culture. UTIs occur more
6/4/2018. Conflicts Disclosure. Objectives. Introduction. Classifications of UTI. Host Defenses. Management of Recurrent Urinary Tract Infections
 Conflicts Disclosure Presenter has no conflicts of interest to disclose Management of Recurrent Urinary Tract Infections COLIN M. GOUDELOCKE, M.D. JUNE 14, 2018 Objectives Attendees will review the identification
Conflicts Disclosure Presenter has no conflicts of interest to disclose Management of Recurrent Urinary Tract Infections COLIN M. GOUDELOCKE, M.D. JUNE 14, 2018 Objectives Attendees will review the identification
UTI: A practical approach. Justin Seroy, DO Infectious Disease Attending BUMC-P
 UTI: A practical approach Justin Seroy, DO Infectious Disease Attending BUMC-P UTI Pathophysiology Uropathogens colonize urethra, vagina or perineal area -> Enter lower urinary tract ->bladder ->kidney
UTI: A practical approach Justin Seroy, DO Infectious Disease Attending BUMC-P UTI Pathophysiology Uropathogens colonize urethra, vagina or perineal area -> Enter lower urinary tract ->bladder ->kidney
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS
 CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
Urinary Tract Infections: From Pyelonephritis to Asymptomatic Bacteriuria. Leslee L. Subak, MD
 Urinary Tract Infections: From Pyelonephritis to Asymptomatic Bacteriuria Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology & Urology University of California, San Francisco UTI Prevalence
Urinary Tract Infections: From Pyelonephritis to Asymptomatic Bacteriuria Leslee L. Subak, MD Professor Obstetrics, Gynecology & RS Epidemiology & Urology University of California, San Francisco UTI Prevalence
None. Appropriate collection minimizes contamination Sample should be delivered to the laboratory in a timely fashion to limit bacterial growth
 None Christopher J. Graber, MD MPH Assistant Clinical Professor of Medicine, UCLA Infectious Diseases Section VA Greater Los Angeles Healthcare System November 19, 2011 Clin Infect Dis 2005;40:643-54 Clin
None Christopher J. Graber, MD MPH Assistant Clinical Professor of Medicine, UCLA Infectious Diseases Section VA Greater Los Angeles Healthcare System November 19, 2011 Clin Infect Dis 2005;40:643-54 Clin
UTI. Monica Tegeler, MD
 4 UTI Monica Tegeler, MD 2 Diagnosis Stone criteria >100,000 colonies of bacteria growing in urine with no more than 2 species of microorganisms Dysuria OR Fever AND 1 of following: Frequency Urgency Suprapubic
4 UTI Monica Tegeler, MD 2 Diagnosis Stone criteria >100,000 colonies of bacteria growing in urine with no more than 2 species of microorganisms Dysuria OR Fever AND 1 of following: Frequency Urgency Suprapubic
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Update in diagnosis and management of UTIs
 Update in diagnosis and management of UTIs I have no disclosures Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Challenges in cystitis Complicated UTI/pyelonephritis Asymptomatic
Update in diagnosis and management of UTIs I have no disclosures Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Challenges in cystitis Complicated UTI/pyelonephritis Asymptomatic
Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured
 9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
Prescribing Guidelines for Urinary Tract Infections
 Prescribing Guidelines for Urinary Tract Infections Urinary Tract Infections in Children Urinary tract infections (UTIs) are common infections of childhood that may affect any part of the urinary tract,
Prescribing Guidelines for Urinary Tract Infections Urinary Tract Infections in Children Urinary tract infections (UTIs) are common infections of childhood that may affect any part of the urinary tract,
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
CHALLENGING UTI S: PRIMARY CARE MANAGEMENT
 CHALLENGING UTI S: PRIMARY CARE MANAGEMENT Wendy L. Wright, MS, RN, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare, PLLC @ Amherst and @ Concord, NH Partner
CHALLENGING UTI S: PRIMARY CARE MANAGEMENT Wendy L. Wright, MS, RN, APRN, FNP, FAANP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare, PLLC @ Amherst and @ Concord, NH Partner
Urinary Tract Infections
 Urinary Tract Infections Dr Mere Kende MBBS, MMed (Path), MAACB, MACRRM, MACTM Lecturer, SMHS, Taurama campus, UPNG Urinary Tract Infections Definitions (Terms) Microbiology and epidemiology Pathogenesis
Urinary Tract Infections Dr Mere Kende MBBS, MMed (Path), MAACB, MACRRM, MACTM Lecturer, SMHS, Taurama campus, UPNG Urinary Tract Infections Definitions (Terms) Microbiology and epidemiology Pathogenesis
Urinary Tract Infection in Women Over the Age of 65: Is Age Alone a Marker of Complication?
 Urinary Tract Infection in Women Over the Age of 65: Is Age Alone a Marker of Complication? Michael L. Grover, DO, Jesse D. Bracamonte, DO, Anup K. Kanodia, MD, Frederick D. Edwards, MD, and Amy L. Weaver,
Urinary Tract Infection in Women Over the Age of 65: Is Age Alone a Marker of Complication? Michael L. Grover, DO, Jesse D. Bracamonte, DO, Anup K. Kanodia, MD, Frederick D. Edwards, MD, and Amy L. Weaver,
Urinary Tract Infection
 67 Urinary Tract Infection Dr Kawa Ahmad PhD Pharmaceutics 1 Introduction The term urinary tract infection (UTI) usually refers to the presence of organisms in the urinary tract together with symptoms,
67 Urinary Tract Infection Dr Kawa Ahmad PhD Pharmaceutics 1 Introduction The term urinary tract infection (UTI) usually refers to the presence of organisms in the urinary tract together with symptoms,
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Definition/Epidemiology Approach to premenopausal and postmenopausal women A couple tricky cases DISCLOSURES. No financial relationships to disclose.
 DISCLOSURES RECURRENT URINARY TRACT INFECTIONS No financial relationships to disclose. Anna C. Kirby, MD, MAS Acting Assistant Professor University of Washington Division of Urogynecology Department of
DISCLOSURES RECURRENT URINARY TRACT INFECTIONS No financial relationships to disclose. Anna C. Kirby, MD, MAS Acting Assistant Professor University of Washington Division of Urogynecology Department of
Nicolette Janzen, MD Texas Children's Hospital
 Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Which UTIs Need a VCUG? Applying AAP Guidelines Nicolette Janzen, MD Texas Children's Hospital Goals 1 2 3 4 5 Review the guidelines Present clinical scenarios Discuss VCUG and nuclear cystogram Discuss
Outpatient Management of Pediatric Urinary Tract Infection Clinical Practice Guideline MedStar Health
 Outpatient Management of Pediatric Urinary Tract Infection Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Outpatient Management of Pediatric Urinary Tract Infection Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions regarding
Investigators Meeting
 Outcomes of Urinary Tract Infection Management by Pharmacists (R x OUTMAP) Investigators Meeting June 11, 2017 Overview 1. Introductions and Opening Remarks 2. Epidemiology and Definitions 3. UTI Assessment
Outcomes of Urinary Tract Infection Management by Pharmacists (R x OUTMAP) Investigators Meeting June 11, 2017 Overview 1. Introductions and Opening Remarks 2. Epidemiology and Definitions 3. UTI Assessment
Children s Services Medical Guideline
 See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
See also: NICE Guidelines These local guidelines are in conjunction with NICE UTI Algorithms Renal scarring and subsequent nephropathy are important causes of later hypertension and renal failure. Early
URINARY TRACT INFECTIONS Mark Schuster, M.D., Ph.D.
 - 351-20. URINARY TRACT INFECTIONS Mark Schuster, M.D., Ph.D. This review is based on textbooks of pediatrics (Roth and Gonzales in Oski et al., 1994), pediatric primary care ( ), and pediatric infectious
- 351-20. URINARY TRACT INFECTIONS Mark Schuster, M.D., Ph.D. This review is based on textbooks of pediatrics (Roth and Gonzales in Oski et al., 1994), pediatric primary care ( ), and pediatric infectious
Urinary Tract Infection. Clinical Background. Quality Department
 Quality Department Guidelines for Clinical Care Ambulatory Urinary Tract Infection Guideline Team Team Leader Steven E Gradwohl, MD General Medicine Team Members Catherine M Bettcher, MD Family Medicine
Quality Department Guidelines for Clinical Care Ambulatory Urinary Tract Infection Guideline Team Team Leader Steven E Gradwohl, MD General Medicine Team Members Catherine M Bettcher, MD Family Medicine
THE EFFECT OF DIABETES MELLITUS ON THE CLINICAL AND MICRO-BIOLOGICAL OUTCOMES IN PATIENTS WITH ACUTE PYELONEPHRITIS
 American Journal of Infectious Diseases 10 (2): 71-76, 2014 ISSN: 1553-6203 2014 Science Publication doi:10.3844/ajidsp.2014.71.76 Published Online 10 (2) 2014 (http://www.thescipub.com/ajid.toc) THE EFFECT
American Journal of Infectious Diseases 10 (2): 71-76, 2014 ISSN: 1553-6203 2014 Science Publication doi:10.3844/ajidsp.2014.71.76 Published Online 10 (2) 2014 (http://www.thescipub.com/ajid.toc) THE EFFECT
URINARY TRACT INFECTIONS IN LONG TERM CARE. Tuesday, 8 November, 11
 URINARY TRACT INFECTIONS IN LONG TERM CARE OBJECTIVES UNDERSTAND THE SCALE OF DISEASE IN LTC SETTINGS DEVELOP AN UNDERSTANDING OF THE DIFFERENT PRESENTATIONS OF UTIs IN THIS SETTING AND WORKUP BECOME AWARE
URINARY TRACT INFECTIONS IN LONG TERM CARE OBJECTIVES UNDERSTAND THE SCALE OF DISEASE IN LTC SETTINGS DEVELOP AN UNDERSTANDING OF THE DIFFERENT PRESENTATIONS OF UTIs IN THIS SETTING AND WORKUP BECOME AWARE
GUIDELINES ON UROLOGICAL INFECTIONS
 GUIDELINES ON UROLOGICAL INFECTIONS (Text update April 2010) M. Grabe (chairman), T.E. Bjerklund-Johansen, H. Botto, M. Çek, K.G. Naber, R.S. Pickard, P. Tenke, F. Wagenlehner, B. Wullt Introduction Infections
GUIDELINES ON UROLOGICAL INFECTIONS (Text update April 2010) M. Grabe (chairman), T.E. Bjerklund-Johansen, H. Botto, M. Çek, K.G. Naber, R.S. Pickard, P. Tenke, F. Wagenlehner, B. Wullt Introduction Infections
GUIDELINES ON THE MANAGEMENT OF URINARY AND MALE GENITAL TRACT INFECTIONS
 GUIDELINES ON THE MANAGEMENT OF URINARY AND MALE GENITAL TRACT INFECTIONS M. Grabe (chairman), M.C. Bishop, T.E. Bjerklund-Johansen, H. Botto, M. Çek, B. Lobel, K.G. Naber, J. Palou, P. Tenke Introduction
GUIDELINES ON THE MANAGEMENT OF URINARY AND MALE GENITAL TRACT INFECTIONS M. Grabe (chairman), M.C. Bishop, T.E. Bjerklund-Johansen, H. Botto, M. Çek, B. Lobel, K.G. Naber, J. Palou, P. Tenke Introduction
1/21/2016. Overview. Significance
 Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
(Facility Name and Address) (1D) Surveillance of Urinary Tract Infections in the Long-Term Care Setting
 (1D) Surveillance of Urinary Tract Infections in the Long-Term Care Setting") Policy Number: 1D Date: 4/16/14 Version: 1 (1D) Surveillance of Urinary Tract Infections in the Long-Term Care Setting Introduction: One-quarter of the older adult population in the United States will
Policy Number: 1D Date: 4/16/14 Version: 1 (1D) Surveillance of Urinary Tract Infections in the Long-Term Care Setting Introduction: One-quarter of the older adult population in the United States will
Managing Urinary Tract Infections in the Nursing Home: Myths, Mysteries and Realities
 ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 1 Number 2 Managing Urinary Tract Infections in the Nursing Home: Myths, Mysteries and Realities H Kamel Citation H Kamel. Managing Urinary
ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 1 Number 2 Managing Urinary Tract Infections in the Nursing Home: Myths, Mysteries and Realities H Kamel Citation H Kamel. Managing Urinary
Antibiotic Guidelines for URINARY TRACT/ UROLOGY infections
 Antibiotic Guidelines f URINARY TRACT/ UROLOGY infections CLINICAL CONDITION USEFUL INFORMATION RECOMMENDATIONS ALTERNATIVE (suitable in serious penicillin allergy) Asymptomatic Bacteriuria (in the absence
Antibiotic Guidelines f URINARY TRACT/ UROLOGY infections CLINICAL CONDITION USEFUL INFORMATION RECOMMENDATIONS ALTERNATIVE (suitable in serious penicillin allergy) Asymptomatic Bacteriuria (in the absence
Pediatric Urinary Tract Infections
 Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Pediatric Urinary Tract Infections Sarmistha B. Hauger M.D. Pediatric Infectious Diseases Specially For Children Dell Children s Medical Center of Central Texas CME Conference 5/08 Pediatric UTI Epidemiology
Key Definitions. Downloaded from
 Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Key Definitions In order to make sure that every member of the team is clear about the definitions that will be used, we have provided a list of key terms in the next few pages along with commonly used
Urinary Tract Infections KIDNEY INFECTIONS. Dr. AMMAR FADIL
 Urinary Tract Infections KIDNEY INFECTIONS Dr. AMMAR FADIL General principles Urinary tract infections (UTIs) is inflammatory response of the urothelium to bacterial invasion. are common affect men and
Urinary Tract Infections KIDNEY INFECTIONS Dr. AMMAR FADIL General principles Urinary tract infections (UTIs) is inflammatory response of the urothelium to bacterial invasion. are common affect men and
PYELONEPHRITIS. Wendy Glaberson 11/8/13
 PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
PYELONEPHRITIS Wendy Glaberson 11/8/13 A 19mo infant girl was seen in the ED 3 days ago and diagnosed with a UTI. She was afebrile at the time and discharged on broad spectrum antibiotics. The child returns
Evidence Based Management of Urinary Tract Infections
 Evidence Based Management of Urinary Tract Infections Urinary tract infection (UTI) is the most common bacterial infection in humans. They account for more than 8.6 million physician visits (84% by women)
Evidence Based Management of Urinary Tract Infections Urinary tract infection (UTI) is the most common bacterial infection in humans. They account for more than 8.6 million physician visits (84% by women)
Which is urinary tract infection (UTI) How is urinary tract infection. Clinical features of UTI in the elderly. Preventive measures in the elderly
 How is urinary tract infection. Clinical features of UTI in the elderly. Preventive measures in the elderly") O Which is urinary tract infection (UTI) How is urinary tract infection How is the diagnosis of UTI in the elderly Clinical features of UTI in the elderly Therapeutic considerations in the elderly Preventive
O Which is urinary tract infection (UTI) How is urinary tract infection How is the diagnosis of UTI in the elderly Clinical features of UTI in the elderly Therapeutic considerations in the elderly Preventive
State of Kuwait Ministry of Health Infection Control Directorate. Guidelines for prevention of catheter associated urinary tract infection
 State of Kuwait Ministry of Health Infection Control Directorate Guidelines for prevention of catheter associated urinary tract infection Updated 2010 1 Introduction: The urinary tract is one of the most
State of Kuwait Ministry of Health Infection Control Directorate Guidelines for prevention of catheter associated urinary tract infection Updated 2010 1 Introduction: The urinary tract is one of the most
Urinary Tract Infections. Keri A. Mattes, Pharm.D., BCPS September 15, 2003
 Urinary Tract Infections Keri A. Mattes, Pharm.D., BCPS September 15, 2003 Urinary Tract Infections 7 million episodes of acute cystitis and 250,000 episodes of pyelonephritis annually in the U.S. Epidemiology
Urinary Tract Infections Keri A. Mattes, Pharm.D., BCPS September 15, 2003 Urinary Tract Infections 7 million episodes of acute cystitis and 250,000 episodes of pyelonephritis annually in the U.S. Epidemiology
Urinary Tract Infections in Children
 Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
Urinary Tract Infections in Children Eric Balighian, MD,* Michael Burke, MD* *St Agnes Hospital, Baltimore, MD Educational Gaps Consideration of risk factors for urinary tract infections (UTIs) in young
Asymptomatic bacteriuria When to screen and when to treat
 Infect Dis Clin N Am 17 (2003) 367 394 Asymptomatic bacteriuria When to screen and when to treat Lindsay E. Nicolle, MD Departments of Internal Medicine and Medical Microbiology, University of Manitoba,
Infect Dis Clin N Am 17 (2003) 367 394 Asymptomatic bacteriuria When to screen and when to treat Lindsay E. Nicolle, MD Departments of Internal Medicine and Medical Microbiology, University of Manitoba,
Recurrent Pediatric UTI Revisited 2013
 Recurrent Pediatric UTI Revisited 2013 PIDSP 21.2.2013 Shai Ashkenazi, MD, MSc Medicine changes constantly Some aspects of the standard practice of ~40 years are probably not valid and need to be changed
Recurrent Pediatric UTI Revisited 2013 PIDSP 21.2.2013 Shai Ashkenazi, MD, MSc Medicine changes constantly Some aspects of the standard practice of ~40 years are probably not valid and need to be changed
Evidence to support discontinuing the use of dipsticks to diagnose a urinary tract infection (UTI) in residents of long-term care homes (LTCHs)
 in residents of long-term care homes (LTCHs)") August 2016 UTI Program Evidence to support discontinuing the use of dipsticks to diagnose a urinary tract infection (UTI) in residents of long-term care homes (LTCHs) A core component of the UTI Program
August 2016 UTI Program Evidence to support discontinuing the use of dipsticks to diagnose a urinary tract infection (UTI) in residents of long-term care homes (LTCHs) A core component of the UTI Program
CLINICAL CHARACTERISTICS AND ANTIBIOTIC RESISTANCE PATTERN OF PATHOGENS IN PEDIATRIC URINARY TRACT INFECTION
 CLINICAL CHARACTERISTICS AND ANTIBIOTIC RESISTANCE PATTERN OF PATHOGENS IN PEDIATRIC URINARY TRACT INFECTION Yupaporn Amornchaicharoensuk Faculty of Medicine, Navamindradhiraj University, Bangkok, Thailand
CLINICAL CHARACTERISTICS AND ANTIBIOTIC RESISTANCE PATTERN OF PATHOGENS IN PEDIATRIC URINARY TRACT INFECTION Yupaporn Amornchaicharoensuk Faculty of Medicine, Navamindradhiraj University, Bangkok, Thailand
Urinary tract infection ประส ทธ อ พาพรรณ สาขาว ชาโรคต ดเช อ ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยศ รนคร นทรว โรฒ
 Urinary tract infection ประส ทธ อ พาพรรณ สาขาว ชาโรคต ดเช อ ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยศ รนคร นทรว โรฒ Introduction Urinary tract infections (UTIs) are extremely common. Most frequent in
Urinary tract infection ประส ทธ อ พาพรรณ สาขาว ชาโรคต ดเช อ ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล ยศ รนคร นทรว โรฒ Introduction Urinary tract infections (UTIs) are extremely common. Most frequent in
Outline. Urinary Tract Infection. Classification - UTI. Adult Genito-Urinary Infections Epidemiology, Etiology, and Diagnosis
 Adult Genito-Urinary Infections Epidemiology, Etiology, and Diagnosis Geoffrey N. Box, M.D. Assistant Professor Director, Laparoscopic Urologic Surgery The Ohio State University Definitions: Urinary Tract
Adult Genito-Urinary Infections Epidemiology, Etiology, and Diagnosis Geoffrey N. Box, M.D. Assistant Professor Director, Laparoscopic Urologic Surgery The Ohio State University Definitions: Urinary Tract
MODULE 2: ADULT URINARY TRACT INFECTIONS
 MODULE 2: ADULT URINARY TRACT INFECTIONS KEYWORDS: Urinary tract infection (UTI); cystitis; pyelonephritis; uropathogens; antibiotics LEARNING OBJECTIVES At the end of this clerkship, the learner will
MODULE 2: ADULT URINARY TRACT INFECTIONS KEYWORDS: Urinary tract infection (UTI); cystitis; pyelonephritis; uropathogens; antibiotics LEARNING OBJECTIVES At the end of this clerkship, the learner will
Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age
 Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Proceeding S.Z.P.G.M.I. Vol: 25(2): pp. 61-65, 2011. Yield of Suprapubic Aspirate versus Bag Collection in Diagnosis of UTI in Children 0 to 6 Months of Age Lubna Riaz, Muhammad Aslam, Waqar Hussain, Anita
Still Feelin the Burn? You Might Have a Urinary Tract Infection
 Still Feelin the Burn? You Might Have a Urinary Tract Infection Jason Alegro, Pharm.D. BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
Still Feelin the Burn? You Might Have a Urinary Tract Infection Jason Alegro, Pharm.D. BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist
 Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Still Feelin the Burn? You Might Have a Urinary Tract Infection
 Still Feelin the Burn? You Might Have a Urinary Tract Infection Jason Alegro, Pharm.D. BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
Still Feelin the Burn? You Might Have a Urinary Tract Infection Jason Alegro, Pharm.D. BCPS Assistant Professor of Clinical Sciences, Roosevelt University Infectious Diseases Clinical Pharmacy Specialist,
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist
 UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
Microbiology. Hani Masaadeh. Hadeel Al-Momani
 Microbiology UTI 1 Hani Masaadeh Hadeel Al-Momani 1 Page #1 Date :27/4/2016 Lecture#1 Micro Lecture#21 UGS Subject : UTI *Urinary tract is normally sterile due to the fact that bacteria moving upwards
Microbiology UTI 1 Hani Masaadeh Hadeel Al-Momani 1 Page #1 Date :27/4/2016 Lecture#1 Micro Lecture#21 UGS Subject : UTI *Urinary tract is normally sterile due to the fact that bacteria moving upwards
MODULE 5: HEMATURIA LEARNING OBJECTIVES DEFINITION. KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer
 MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
Urinary tract infections
 بسم رلاهللا Urinary tract infections This sheet will only contain extra notes said by the dr. UTIs: - is the second most common type of infections in community(second only to RTIs) - Incidence=20-30% of
بسم رلاهللا Urinary tract infections This sheet will only contain extra notes said by the dr. UTIs: - is the second most common type of infections in community(second only to RTIs) - Incidence=20-30% of
CLINICAL PRACTICE GUIDELINE FROM THE AMERICAN ACADEMY OF PEDIATRICS
 FROM THE AMERICAN ACADEMY OF PEDIATRICS CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children
FROM THE AMERICAN ACADEMY OF PEDIATRICS CLINICAL PRACTICE GUIDELINE Urinary Tract Infection: Clinical Practice Guideline for the Diagnosis and Management of the Initial UTI in Febrile Infants and Children