MUTLIMODALAITY NEUROPHYSIOLOGICAL MONITORING IN SPINE SURGERIES
|
|
|
- Clinton Johns
- 5 years ago
- Views:
Transcription

1 50 th Annual ASET Meeting 2009 August 8 th, 2009 MUTLIMODALAITY NEUROPHYSIOLOGICAL MONITORING IN SPINE SURGERIES FAISAL R. JAHANGIRI, MD, CNIM, D.ABNM Senior Neurophysiologist & Research Coordinator Impulse Monitoring Inc University of Virginia Medical Center Charlottesville, VA
2 What is Neurophysiological Monitoring? IONM (Intraoperative Neurophysiological monitoring) offers protection of neural tissues and organs (brain, spinal cord and peripheral nerves) during surgery. Early irritation or impending injury can often be detected by measuring spontaneous or elicited (evoked) electrical signals produced by the nervous system or attached muscle groups during surgery. IONM has been shown to be effective in reducing operative neurological complications in several types of surgery.
3 The Benefits of Monitoring Increased safety of the surgical procedure. IONM has been shown to play a significant role in reducing patient morbidity and mortality. Increased ability to accommodate more complex cases. IONM helps to identify new neurological impairment early enough to allow prompt correction of the cause. This "early warning" system provides surgeons with the comfort necessary to perform complex cases. Decreased risk of adverse surgical outcomes. IONM guides the degree of surgical intervention and provides a means for assessing the likelihood of postoperative complications.



4 Surgery and IONM BRAIN SPINAL CORD PERIPHERAL NERVES
5 Types of Surgeries Neurosurgery Spinal Fusion Spinal Tumor (Intra-medullary/ Extra-medullary) Tethered Cord Cauda equina lesion Dorsal Root Rhizotomy Brachial plexus tumors Spinal Stimulator Implant Orthopedic Surgery Spinal corrections Scoliosis Hip replacement Sacro Iliac Joint Fusion DLIF / XLIF Interventional Neuro Radiological Procedures Spinal AVM embolization
6 Multi-modality Monitoring in Spinal Surgeries Multi-modality intraoperative neurophysiologic monitoring (IONM), in general, can prevent or lower the risk of devastating neurologic deficit in a wide variety of cases which place neural structures at risk. And although they all have advantages and disadvantages, they are, in combination, an effective means for providing patient protection.
7 Modalities in Spinal Surgeries What are Modalities: Modalities are specific types of electrophysiological tests that can used for testing specific neurological / functional pathways during different types of surgeries. What is protected: Ascending somatosensory pathways functions like proprioception, stereognosis, weight discrimination, touch, vibration Descending motor pathways function like primary voluntary body movements
8 Modalities for Spine Somatosensory Evoked Potential (SSEP) Spontaneous Electromyography Triggered Electromyography Trans Cranial Electrical Motor Evoked Potentials Direct waves Bulbocavernous Reflex Train of Four H-Reflex F-Response (S-EMG) (T-EMG) (TCeMEP) (D-waves) (BCR) (TOF)
9 Modalities Somatosensory Evoked Potentials (SSEP)
10 SSEP Somatosensory Evoked Potentials: This test stimulates the patient distally and records along the pathway as the nerve pulse travels to the brain Optimal for protection of the patients ascending sensory spinal pathways Useful in detection of mechanical and ischemic changes in the peripheral nerves, spinal cord and cortex. Particularly in posterior spinal cord. 95 to 98% specificity to sensory neurological events
11 SSEP Used when Peripheral Nerve, Spinal Cord (Dorsal Column), Brainstem or Cortex is at risk Stimulate Distal Nerves Posterior Tibial/Peroneal/Femoral Nerves Median/Ulnar Nerves Record Distal and Proximal Responses Measure Significant Changes in Responses Latency Amplitude

12 SSEP Primary Somatosensory Cortex Thalamocortical Dorsal Column and Medial Lemniscus Root Entry Zone Peripheral Potential Brachial Plexus Upper Popliteal Fossa Lower (Sensory Nerve Action Potential)
13 SSEP Recordings These are responses recorded after hands and feet stimulation. By recording at multiple locations we can determine the anatomic and functional integrity at different locations along the somatosensory pathway as the pulse travel from periphery to the cortex.
14 SSEP Setup Stimulus Parameters: AEEG Guidelines Pulse: Electric Monopolar rectangular Duration: µsec Intensity: ma Stim Rate: Median (2-8/sec) Tibial (2-10/sec) Sweep: Median (40 ms) / Tibial (60 ms) Averages: Band-pass: Cortical: 1-30 to Hz Recording Parameters: AEEG Guidelines Median Posterior Tibial CPc CPi CPi FPz CPi Ref CPz FPz C5s Ref FPz C5s EPi Ref T12S Ref PFd PFp Spinal: to Hz

15 SSEP SSEP SSEP assesses the sensory pathways from distal nerves through to the cortex. Electrodes are placed on the distal limbs and scalp. A small electrical current is given distally and recording along the pathway and at the scalp Criteria AMPLITUDE 50% decrease from baseline LATENCY 10% increase from baseline

16 Amplitude Reduction ISCHEMIC CHANGES IN SSEP


17 CHANGES IN SSEP Cortical Cortical Cortical Cortical Cervical Cervical Cortical Cervical Cortical Cervical Anesthesia Event Surgical Event

18 Effect of Hypotension on SSEP Case: Drop in MAP from 103 to 76

19 Effect of Positioning on SSEP

20 Effect of Positioning on SSEP

21 Effect of Positioning on SSEP Case Changes in Left Ulnar 64 years old Female Patient Back pain with bilateral foot drop Procedure: Posterior Lumbar Laminectomy and Fusion, L3-L5

22 Effect of Positioning on SSEP Case # 3: Changes on Left side





23 Effect of Positioning on SSEP Case # 4: Changes on Left side
24 Advantages of SSEP SSEPs allows us to evaluate the functional integrity of dorsal column during high risk portions of the procedure. Help prevent brachial plexus injuries during surgery which can sometime occur due to patient positioning. Help assess peripheral blood flow Help differentiate between Evoked Potential loss caused by spinal cord injury, versus peripheral ischemia, versus stroke. SSEPs are still a valuable adjunct to monitoring when used alongside MEP and EEG monitoring.
25 Disadvantages of SSEP SSEPs do not assess motor pathways. SSEPs are highly susceptible to anesthetic agents and changes in hemodynamic variables. The blood supply to pathways monitored by SSEP is different than the blood supply to pathways involving motor function. Therefore SSEP changes do no correlate well with post-operative motor function. Because of these factors, SSEPs are best utilized in conjunction with other modalities of monitoring.
26 SSEP: Anesthesia Preferred N2O 0% Minimal volatile anesthetic 1 MAC% Narcotic medication - Yes Muscle relaxants - Yes Alternative N2O 60% Minimal volatile anesthetic 0.5 MAC Narcotic medication - Yes Muscle relaxants - Yes
27 Effect of Hypotension on SSEP Hypotension can effect SSEP and TCeMEP signals globally. Ischemia will result in delayed time course. Within the spinal cord the grey matter is most sensitive to ischemia with loss of synaptic activity at 1-2 minutes while conduction in sensory and motor white matter shows alteration in different time.
28 Effect of Hypotension on EPs
29 Modalities Trans Cranial Electrical Motor Evoked Potentials (TCeMEP)
30 SPINAL TCeMEP Used when Spinal Cord (Ventral Column), Brainstem or Cortex is at risk Stimulate Motor Cortex ~ V Record Distal Responses Measure Significant Changes in Responses Presence/Absence


31 SPINAL TCeMEP
 Direct Cortical Stimulation (DCS) Spinal MEP s")
32 SPINAL TCeMEP Cortical Stimulation Transcranial Electrical Stimulation (TES) Direct Cortical Stimulation (DCS) Spinal MEP s Muscle MEP s


33 SPINAL TCeMEP Stimulating electrodes are typically placed at C3 and C4 Allows for activation of both upper and lower extremity muscle groups Alternative stimulation sites used are C1 and C2

34 CORTICAL MOTOR PRESENTATION
35 Spinal TCeMEP Surgical Application Special consideration Bite block Anesthesia cortical suppression of motor, EEG monitoring anesthesia load Intermittent runs Contra indication History of seizures Pace makers Cochlear Implants
36 Set Up Criteria Spinal TCeMEP Specific set up and coverage Upper and lower motor pathways Myelopathy suppression of motor function Additional coverage of C5 Additional coverage of bowel/bladder Additional coverage L4, L5 and S1 TceMEP Criteria Increases protection from SSEP only SSEP only 85 to 90% and sensory specific TceMEP is 90 to 100% and motor specific All or nothing CMAP MEP, presents/absents of muscle contraction 50% decrease in amplitude MMEP
37 TCeMEP Setup Stimulus Parameters: FDA Guidelines Pulse: Electric Monopolar rectangular Duration: 50 µsec Intensity: V Inter Stimulus Interval (ISI): Trains: 1-9 Averages: 1 Recording Parameters: Low Cut: 10 Hz High Cut: Hz Sweep: 10 ms/div Gain: 100 µv/div Reject: Off Upper Ext: Delt, FCU, BR, APB & ADM, Lower Ext: Quads, TA, MG, AH & EHB

38 Spinal TCeMEP
39 Spinal TCeMEP Outcome Studies MOTOR EVOKED POTENTIAL MONITORING DURING SPINAL CORD SURGERY; Karl Kothbauer, MD, Pediatric Neurosurgery, Hyman-Newman Institute for Neurology and Neurosurgery Beth Israel Medical Center, New York City Intraoperative loss of muscle MEPs indicates some postoperative impairment of voluntary motor control with a specific of about 90% and sensitivity of 100% For instance muscle MEPs lost in one leg during the resection means that the patient will postoperatively be unable to move this particular extremity
40 Spinal TCeMEP Outcome Studies THRESHOLD-LEVEL REPETITIVE TRANSCRANIAL ELECTRICAL STIMULATION FOR INTRAOPERATIVE MONITORING OF CENTRAL MOTOR CONDUCTION; Blair Calancie, Ph.D., William Harris, M.Sc., G. Fred Brindle, MD., Barth A. Green, MD and Howard J. Landy, MD Study of postoperative clinical outcome in 83 spinal surgery patient using SSEP and TES (TceMEP) Based on this data, the results of sensitivity and specificity calculations were 0.87 and 0.90, respectively, for SSEP monitoring relative to postoperative deficit and 1 and 1 respectively for TES monitoring relative to postoperative motor deficit.
41 Spinal TCeMEP: Case Study C6 tumor 44 year old male, history of cervical meningioma Posterior resection, to be followed by an anterior resection
42 Spinal TCeMEP: Case Study 09:45 13:50 SSEPs TcMEPs
43 Spinal TCeMEP: Case Study 15:20 SSEPs no change TcMEPs Left/Right TA gone Right APB gone Drop in left APB
44 Spinal TCeMEP: Case Study 16:50 SSEPs no change TcMEPs increase in threshold for all muscles
45 Spinal TCeMEP: Case Study Post-Operative: Based on TcMEPs, anterior resection was cancelled Patient awoke with profound right-side weakness, moderate left-side weakness Profound proprioceptive loss in right lower limb Stayed in hospital for 3 weeks and was discharged to rehab and was ambulating at 3 months, with a cane

46 Effect of Hypotension on MEP Case: Drop in MAP from 94 to 62

47 Effect of Neck Positioning on MEP 23 years old Female Patient. Presents with severe muscular dystrophy Procedure: ACDF Changes is SSEP and MEP during Halo placement. Responses returned after repositioning.
48 TCeMEP: Anesthesia TIVA Total Intra Venous Anesthesia (Preferred) N2O 0% Minimal volatile anesthetic 0% Narcotic medication - Yes Fentanyl bolus, and a Propofol infusion ( ug/kg/min) No muscle relaxants Alternative N2O 60% Minimal volatile anesthetic 0.5 MAC Narcotic medication - Yes Fentanyl bolus, and a Propofol infusion ( ug/kg/min) No muscle relaxants
49 Advantages of TCeMEP MEPs record corticospinal tract information allowing us to evaluate the functional integrity of motor tracts during high risk portions of the procedure. MEPs are stable waveforms recorded easily with strict TIVA technique. MEP assess the real-time function of voluntary motor pathways in the spinal cord, and reduce the risk of paraplegia. MEPs help detect ischemic changes in the motor cortex, spinal cord, and peripheral motor nerves.
50 Disadvantages of TCeMEP TCeMEPs have identified risk factors such as tongue lacerations, and in some populations, risk for seizures. TCeMEPs requires no muscle relaxant during the surgical procedures.
51 Modalities Epidural Recordings (D-Waves)
52 D-Wave Setup Stimulus Parameters: FDA Guidelines Pulse: Electric Monopolar rectangular Duration: 50 µsec Intensity: V Inter Stimulus Interval (ISI): Trains: 1 Averages: 1 Recording Parameters: Low Cut: 10 Hz High Cut: Hz Sweep: 1-3 ms/div Gain: 100 µv/div Reject: Off Epidural Electodes
53 Epidural (D-Waves)
")
54 Epidural (D-Waves)
55 Epidural (D-Waves) Alarm Criteria: D-wave Muscle Response Motor Status unchanged preserved unchanged unchanged lost on one or both sides temporary motor deficit 30-50% decrease preserved unchanged 30-50% decrease lost on one or both sides temporary motor deficit >50% decrease lost long term motor deficit
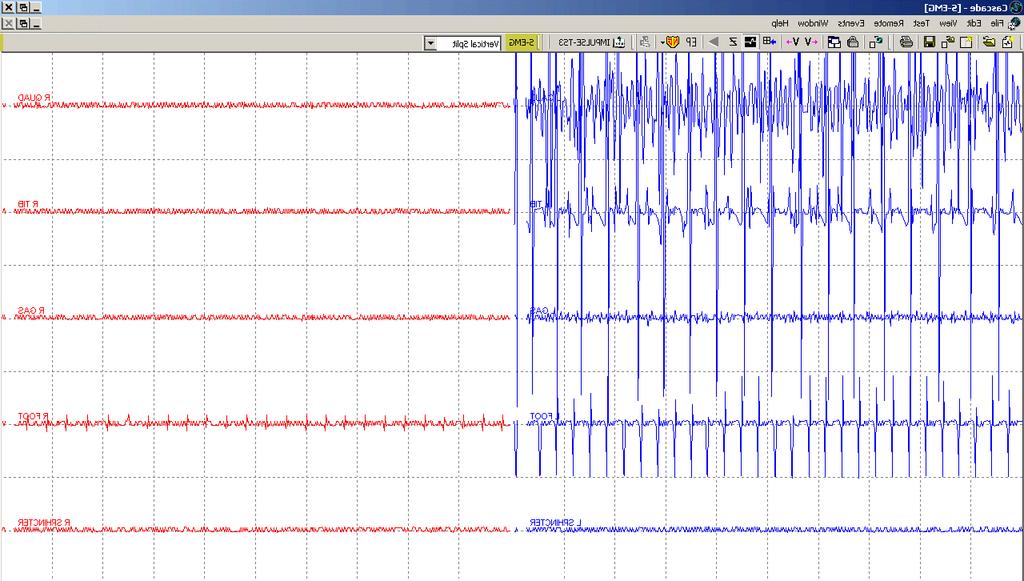
56 Modalities Electromyography (EMG)
 Subdermal electrodes Active triggering of activity (CMAP/T-EMG) Prass")
57 Spinal S-EMG and T-EMG Used when Spinal Roots or Cranial Nerves are at risk Passive recording of activity in muscle (Free-Run EMG / S-EMG) Subdermal electrodes Active triggering of activity (CMAP/T-EMG) Prass probe
58 Spinal S-EMG and T-EMG The lower motor neuron consists of the anterior horn cell, its axon and all the muscle fibers innervated by that axon. Segmental nerve root monitoring involves monitoring the function of the motor unit axon by recording free-run and triggered EMG activity from the muscle fibers of the motor units. The number of nerve fibers innervating a muscle and the number of muscle fibers per motor unit varies from one muscle to another.
59 Spinal EMG Detection of: Stretch Compression Heat Ischemia NOT resection Trauma makes nerves more sensitive Chronic compression leads to demyelination of nerve fibers
60 Spinal S-EMG Abnormal EMG Types: Spikes Bursts Train Neurotonic discharges Irregular Surface Vs Needle Electrodes: Surface pads electrodes are not good for detecting MUP Sub dermal EMG needles are better EMG needles are too selective (Skinner et al. 2008)


61 Spinal S-EMG


62 Spinal T-EMG T-EMG Triggered electromyography are recorded from the distal muscles. Activity recorded is associated with nerve, nerve root and pedicle screw electrical stimulation. T-EMG T-EMG is used for: Direct nerve stimulation Pedicle Screw stimulation 6 ma triggered pedicle stimulation response. Indicating probably pedicle wall breach


63 Spinal T-EMG Reference Current Leak Error fluid, soft tissue, etc Pedicle Screw CURRENT FLOW What is Happening During Pedicle Screw Stimulation?
64 EMG THRESHOLD INTENSITIES FOR PEDICLE SCREW STIMULATION REFERENCE BAD GOOD Calancie et al ma >10 ma Maguire et al ma >6 ma Glassman et al ma >10 ma >15 ma Lenke et al ma >8 ma Clements et al ma >11 ma

65 Spinal T-EMG
66 Spinal S-EMG and T-EMG Outcome Studies SPINE SURGERY; Edward C. Benzel, Volume 2, Techniques, Complication, Avoidance and Management, Chapter 95, Intraoperative Electromyelography Monitoring Monitored and non-monitored outcome studies Separated into 2 groups Group I (n=185) without monitoring Group II (n=205) with monitoring Group I: Incidence of surgically induced radiculopathies was 9.6% Group II: Incidence of surgically induced radiculopathies was <1.0%
67 Modalities Train Of Four (TOF)
68 D-Wave Setup Stimulus Parameters: Setup Mode: TOF Pulse: Electric Monopolar rectangular Duration: 100 µsec Intensity: ma Stim Rate: 2 Hz Recording Parameters: Low Cut: 10 Hz High Cut: Hz Sweep: 20 ms/div Gain: 100 µv/div Muscles: APB/ADM or AH/EHB Train: 1 Nerves: Median or Posterior Tibial


69 Train of Four: TOF 4/4
70 Modalities Bulbo Cavernous Reflex (BCR)
71 Bulbocavernous Reflex (BCR) For patients at risk for low sacral neural injury. Patients are maintained with propofol, opiate infusion, and low inhalant anesthesia without muscle relaxant. Cutaneous sensory nerves of the penis (or clitoris) are stimulated For BCR recording, needle electrodes were placed into the external anal sphincter (EAS) bilaterally.


72 Bulbocavernous Reflex (BCR) Bulbacavernosa Reflex useful in determine functional status of the Pudendal sensory motor reflex and conus medullaris during surgical intervention.
73 Modalities Selective Dorsal Root Rhizotomy (SDR)
74 Selective Dorsal Root Rhizotomy (SDR) Selective dorsal rhizotomy (SDR) is a procedure for the treatment of spasticity in some children with cerebral palsy. The incidence of cerebral palsy ranges from per thousand school-age children. Of these children about 75% will have a spastic variety. Some of these children may benefit by reducing their spasticity through selective dorsal rhizotomy. Utilizing t-emg has been reported as an effective tool for selection of abnormal rootlets.
75 Selective Dorsal Root Rhizotomy (SDR) Schematic Diagram of Intraoperative EMG Responses Decremental Squared Incremental Clonic Multiphasic Sustained Stimulus: 1s Electrical Train



76 Selective Dorsal Root Rhizotomy (SDR)
")
77 Selective Dorsal Root Rhizotomy (SDR) Incremental
78 Modalities Surgical Procedures
79 Spinal Cord: Cervical/Thoracic Anatomical Structures at Risk: Brainstem somatosensory pathways Spinal cord Spinal cord motor pathways Monitoring Modalities Used During Surgery: Somatosensory Evoked Potentials (SSEP) Transcranial Motor Evoked Potentials (TCeMEP) Epidural Evoked Potentials (D-waves) Spontaneous Electromyography (s-emg) for cervical nerve root monitoring
80 Spinal Cord: Lumbar / Sacral Anatomical Structures at Risk: Lumbar and Sacral nerve roots Spinal cord Monitoring Modalities Used During Surgery: Somatosensory Evoked Potentials (SSEP) Transcranial Motor Evoked Potentials (TCeMEP) Spontaneous Electromyography (s-emg) for nerve root monitoring Triggered Electromyography (t-emg) for Pedicle Screw testing Bulbocavernosus Reflex
81 Tethered Cord/Cauda Equina Tumor Anatomical Structures at Risk: Lumbar and Sacral nerve roots Spinal cord Spinal cord motor pathways Monitoring Modalities Used During Surgery: Somatosensory Evoked Potentials (SSEP) Transcranial Motor Evoked Potentials (TCeMEP) Spontaneous Electromyography (s-emg) for nerve root monitoring Triggered Electromyography (t-emg) for Pedicle Screw testing Bulbocavernosus Reflex
82 Spinal Intramedullary Tumor Anatomical Structures at Risk: Spinal cord Spinal cord sensory pathways Spinal cord sensory pathways Monitoring Modalities Used During Surgery: Somatosensory Evoked Potentials (SSEP) Transcranial Motor Evoked Potentials (TCeMEP) Epidural Evoked Potentials (D-waves) Spontaneous Electromyography (s-emg) for cervical nerve root monitoring
83 Spinal Arteriovenous Malformation (AVM) Anatomical Structures at Risk: Arteries Spinal cord Spinal cord sensory pathways Spinal cord sensory pathways Monitoring Modalities Used During Surgery: Somatosensory Evoked Potentials (SSEP) Transcranial Motor Evoked Potentials (TCeMEP)
84 Selective Dorsal Rhizotomy Anatomical Structures at Risk: Peripheral sensory (dorsal) roots Peripheral motor (ventral) roots Monitoring Modalities Used During Surgery: Spontaneous Electromyography (s-emg) for nerve root monitoring Triggered Electromyography (t-emg) for nerve root monitoring Train of Four (TOF)
85 Spinal Cord Stimulator Implant Anatomical Structures at Risk: Spinal Cord Monitoring Modalities Used During Surgery: Spontaneous Electromyography (s-emg) for localization Triggered Electromyography (t-emg) for localization of stimulator Train of Four (TOF)
86 Multimodality by Surgeries ACDF: SSEP S-EMG TCeMEP PCF: SSEP S-EMG T-EMG TCeMEP Occiput-C2 Fusion: SSEP TCeMEP Anterior Lumbar Fusion: SSEP S-EMG Posterior Lumbar Fusion: SSEP S-EMG T-EMG Tethered Cord SSEP S-EMG T-EMG TCeMEP Extra-medullary Cord Tumor SSEP S-EMG T-EMG TCeMEP Intra-medullary cord tumor SSEP S-EMG T-EMG TCeMEP D-waves SDR SSEP S-EMG T-EMG TCeMEP DLIF/XLIF: SSEP S-EMG Cauda Equina Tumor SSEP S-EMG T-EMG TCeMEP BCR Spinal AVM: SSEP TCeMEP Scoliosis SSEP S-EMG T-EMG TCeMEP
87 Challenges in Neurophysiological monitoring
88 Challenges in Neuromonitoring Unfortunately, we all too often encounter technical and physiological challenges that we must overcome in order to adequately protect our patients. Becoming familiar with potential technical and physiological challenges can facilitate more positive intraoperative experience for the entire surgical team.
89 Technical Changes Stimulation problems Recording problems Physiological Anesthesia Temperature Mean Arterial Pressure Positioning effects Surgical
90 Challenges in Neuromonitoring Physiological / Technical Challenges: Compromised blood flow to the extremities (peripheral ischemia, blood clots, BP cuff occlusion) Positioning of extremities I.V. Infiltration Hypothermia / Hyperthermia Scalp Edema-impeded stimulus delivery Failure of stimulus delivery (multiple etiologies) Failure of recording electrodes /equipment/ systems Extraneous Artifact
91 Multi-Modality Neurophysiological Monitoring Employing a multi-disciplinary surgical approach including: TCeMEP, SSEP, EMG, EEG and maintaining mean arterial pressure of at least 70 mmhg all contribute collectively to the significant reduction of post-operative paraplegia in the cervical, thoracic, lumbar spine and brain surgeries.
92 Benefits Improved patient care. Reduce patient neurological deficits. Reduce surgical morbidity and mortality.
93 Goals Identify significant changes in spinal function. Intervene and prevent permanent neurological damage.

94 THANK YOU
Audit and Compliance Department 1
 Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
Electrophysiologic assessment of neurologic injury
 Electrophysiologic assessment of neurologic injury Gregory A Kinney, PhD Dept of Rehabilitation Medicine University of Washington Seattle, WA Electrophysiologic Monitoring of Spinal Cord Function http://faculty.etsu.edu/currie/images/neuro2.jpg
Electrophysiologic assessment of neurologic injury Gregory A Kinney, PhD Dept of Rehabilitation Medicine University of Washington Seattle, WA Electrophysiologic Monitoring of Spinal Cord Function http://faculty.etsu.edu/currie/images/neuro2.jpg
Track One. Spine Surgery.
 Track One Spine Surgery www.asnm.org 18 Spine Instrumentation: Methodology and Approaches Ricardo B. V. Fontes, MD, PhD www.asnm.org 19 Spine instrumenta-on: methodology and approaches Ricardo Fontes,
Track One Spine Surgery www.asnm.org 18 Spine Instrumentation: Methodology and Approaches Ricardo B. V. Fontes, MD, PhD www.asnm.org 19 Spine instrumenta-on: methodology and approaches Ricardo Fontes,
IOM at University of. Training for physicians. art of IOM. neurologic. injury during surgery. surgery on by IOM. that rate is.
 Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
SEP Monitoring. Outline. Outline 1/22/2015. Development of SEPs Stimulation and recording techniques Predictive value of SEP Uses of SEP monitoring
 SEP Monitoring Andres A Gonzalez, MD Director, Surgical Neurophysiology Keck Medical Center of USC University of Southern California Outline Development of SEPs Stimulation and recording techniques Predictive
SEP Monitoring Andres A Gonzalez, MD Director, Surgical Neurophysiology Keck Medical Center of USC University of Southern California Outline Development of SEPs Stimulation and recording techniques Predictive
SEP Monitoring. Andres A Gonzalez, MD Director, Surgical Neurophysiology Keck Medical Center of USC University of Southern California
 SEP Monitoring Andres A Gonzalez, MD Director, Surgical Neurophysiology Keck Medical Center of USC University of Southern California Outline Development of SEPs Stimulation and recording techniques Predictive
SEP Monitoring Andres A Gonzalez, MD Director, Surgical Neurophysiology Keck Medical Center of USC University of Southern California Outline Development of SEPs Stimulation and recording techniques Predictive
Management of Bone and Spinal Cord in Spinal Surgery.
 Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
Neuroprotection for Scoliosis Surgery
 Neuroprotection for Scoliosis Surgery Mary Ellen McCann, MD, MPH Associate Professor of Anaesthesia Harvard Medical School Children s Hospital Boston mary.mccann@childrens.harvard.edu Disclosure I have
Neuroprotection for Scoliosis Surgery Mary Ellen McCann, MD, MPH Associate Professor of Anaesthesia Harvard Medical School Children s Hospital Boston mary.mccann@childrens.harvard.edu Disclosure I have
Medical Policy Manual
 Medical Policy Manual Policy Number: 0013 Effective Date: Reviewed Date: Next Review: August 2019 CLINICAL BACKGROUND INTRAOPERATIVE NEUROMONITORING BACKGROUND Intraoperative neurophysiologic monitoring
Medical Policy Manual Policy Number: 0013 Effective Date: Reviewed Date: Next Review: August 2019 CLINICAL BACKGROUND INTRAOPERATIVE NEUROMONITORING BACKGROUND Intraoperative neurophysiologic monitoring
A Patient s Guide to Intraoperative Monitoring
 A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Intraoperative Monitoring 228 West Main, Suite C Missoula, MT 59802 Phone: info@spineuniversity.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Neurological Complications in EOS and Neuromonitoring Issues
 Neurological Complications in EOS and Neuromonitoring Issues G. Bollini, M. Gavaret Timone Children s Hospital Marseilles, France ICEOS Meeting San Diego 2013 Disclaimer Consultancy Agreements: Depuy Synthes,
Neurological Complications in EOS and Neuromonitoring Issues G. Bollini, M. Gavaret Timone Children s Hospital Marseilles, France ICEOS Meeting San Diego 2013 Disclaimer Consultancy Agreements: Depuy Synthes,
ION Intraoperative Neurophysiology
 ION Intraoperative Neurophysiology EMG Course in Bucharest, September 18-19, 2012 Roland Flink Prof MD PhD Department of Clinical Neurophysiology What to monitor? Cortical function Tumour surgery Epilepsy
ION Intraoperative Neurophysiology EMG Course in Bucharest, September 18-19, 2012 Roland Flink Prof MD PhD Department of Clinical Neurophysiology What to monitor? Cortical function Tumour surgery Epilepsy
Protocol. Intraoperative Neurophysiologic Monitoring (sensoryevoked potentials, motor-evoked potentials, EEG monitoring)
") Intraoperative Neurophysiologic Monitoring (sensoryevoked potentials, motor-evoked potentials, EEG monitoring) (70158) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/15 Preauthorization
Intraoperative Neurophysiologic Monitoring (sensoryevoked potentials, motor-evoked potentials, EEG monitoring) (70158) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/15 Preauthorization
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING FOR MICROVASCULAR DECOMPRESSION SURGERY IN PATIENTS WITH HEMIFACIAL SPASM
 INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING FOR MICROVASCULAR DECOMPRESSION SURGERY IN PATIENTS WITH HEMIFACIAL SPASM WILLIAM D. MUSTAIN, PH.D., CNIM, BCS-IOM DEPARTMENT OF OTOLARYNGOLOGY AND COMMUNICATIVE
INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING FOR MICROVASCULAR DECOMPRESSION SURGERY IN PATIENTS WITH HEMIFACIAL SPASM WILLIAM D. MUSTAIN, PH.D., CNIM, BCS-IOM DEPARTMENT OF OTOLARYNGOLOGY AND COMMUNICATIVE
6/16/2016 IOM APPROACHES TO THE PUDENDAL NERVE TEAL TAYLOR, REEGT/REPT/CNIM EVOKES, LLC A SENSITIVE SUBJECT: I DON T WANT TO WEAR A DIAPER
 IOM APPROACHES TO THE PUDENDAL NERVE TEAL TAYLOR, REEGT/REPT/CNIM EVOKES, LLC A SENSITIVE SUBJECT: I DON T WANT TO WEAR A DIAPER In IOM we continuously work to protect the Sensory and Motor Function of
IOM APPROACHES TO THE PUDENDAL NERVE TEAL TAYLOR, REEGT/REPT/CNIM EVOKES, LLC A SENSITIVE SUBJECT: I DON T WANT TO WEAR A DIAPER In IOM we continuously work to protect the Sensory and Motor Function of
FAISAL R. JAHANGIRI A BRIEF OVERVIEW OF SCIENCE & BENEFITS INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING (IONM)
") INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING (IONM) A BRIEF OVERVIEW OF SCIENCE & BENEFITS FAISAL R. JAHANGIRI MD, CNIM, D.ABNM, FASNM VICE PRESIDENT OF CLINICAL AFFAIRS AXIS NEUROMONITORING LLC RICHARDSON,
INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING (IONM) A BRIEF OVERVIEW OF SCIENCE & BENEFITS FAISAL R. JAHANGIRI MD, CNIM, D.ABNM, FASNM VICE PRESIDENT OF CLINICAL AFFAIRS AXIS NEUROMONITORING LLC RICHARDSON,
Neuromonitorisation in prevention of motor-deficit during pediatric spine surgeries
 Neuromonitorisation in prevention of motor-deficit during pediatric spine surgeries *M. Biscevic 1, S. Biscevic 2, F. Ljuca 3, B. Smrke 4, C. Ozturk 5, M. Tiric-Campara 6 1 Spine centre, Orthopedics, KCUS,
Neuromonitorisation in prevention of motor-deficit during pediatric spine surgeries *M. Biscevic 1, S. Biscevic 2, F. Ljuca 3, B. Smrke 4, C. Ozturk 5, M. Tiric-Campara 6 1 Spine centre, Orthopedics, KCUS,
NVM5 NERVE MONITORING SYSTEM AN INTRODUCTION TO
 AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
AN INTRODUCTION TO NVM5 NERVE MONITORING SYSTEM This booklet is designed to inform you about the use of NVM5 nerve monitoring in the course of your surgery. It is not meant to replace any personal conversations
Lecturer. Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014
 Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Intraoperative neurophysiological monitoring for the anaesthetist
 Intraoperative neurophysiological monitoring for the anaesthetist Part 1: A review of the theory and practice of intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB, DA(SA), Registrar
Intraoperative neurophysiological monitoring for the anaesthetist Part 1: A review of the theory and practice of intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB, DA(SA), Registrar
What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction?
 London, 2016 What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction? David B. Vodušek Medical Faculty, University of Ljubljana, Slovenia vodusek.david.b@gmail.com
London, 2016 What is the role for neurophysiology in the evaluation of patients with uro-genito-anal dysfunction? David B. Vodušek Medical Faculty, University of Ljubljana, Slovenia vodusek.david.b@gmail.com
Chapter 12b. Overview
 Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Chapter 12b Spinal Cord Overview Spinal cord gross anatomy Spinal meninges Sectional anatomy Sensory pathways Motor pathways Spinal cord pathologies 1 The Adult Spinal Cord About 18 inches (45 cm) long
Why can t we get good baseline motor evoked potentials in this. patient? Laura Hemmer, M.D. Antoun Koht, M.D.
 Why can t we get good baseline motor evoked potentials in this SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. patient? Laura Hemmer,
Why can t we get good baseline motor evoked potentials in this SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. patient? Laura Hemmer,
Corporate Medical Policy
 Corporate Medical Policy Intraoperative Neurophysiologic Monitoring File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intraoperative_neurophysiologic_monitoring 11/2012 5/2017 5/2018
Corporate Medical Policy Intraoperative Neurophysiologic Monitoring File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intraoperative_neurophysiologic_monitoring 11/2012 5/2017 5/2018
Human Anatomy. Spinal Cord and Spinal Nerves
 Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Human Anatomy Spinal Cord and Spinal Nerves 1 The Spinal Cord Link between the brain and the body. Exhibits some functional independence from the brain. The spinal cord and spinal nerves serve two functions:
Intraoperative Monitoring: Role in Epilepsy Based Tumor Surgery December 2, 2012
 Intraoperative Monitoring: Role in Epilepsy Based Tumor Surgery December 2, 2012 Aatif M. Husain, M.D. Duke University and Veterans Affairs Medical Centers, Durham, NC American Epilepsy Society Annual
Intraoperative Monitoring: Role in Epilepsy Based Tumor Surgery December 2, 2012 Aatif M. Husain, M.D. Duke University and Veterans Affairs Medical Centers, Durham, NC American Epilepsy Society Annual
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Lecture 14: The Spinal Cord
 Lecture 14: The Spinal Cord M/O Chapters 16 69. Describe the relationship(s) between the following structures: root, nerve, ramus, plexus, tract, nucleus, and ganglion. 70. Trace the path of information
Lecture 14: The Spinal Cord M/O Chapters 16 69. Describe the relationship(s) between the following structures: root, nerve, ramus, plexus, tract, nucleus, and ganglion. 70. Trace the path of information
ACCOMPANYING EDITORIAL
 NEUROSURGICAL FOCUS Neurosurg Focus 43 (4):E8, 2017 Intraoperative neuromonitoring alerts in a pediatric deformity center Maria Zuccaro, PhD, CNIM, 1 James Zuccaro, DC, DABNM, 1 Amer F. Samdani, MD, 2
NEUROSURGICAL FOCUS Neurosurg Focus 43 (4):E8, 2017 Intraoperative neuromonitoring alerts in a pediatric deformity center Maria Zuccaro, PhD, CNIM, 1 James Zuccaro, DC, DABNM, 1 Amer F. Samdani, MD, 2
Intraoperative monitoring for tethered cord surgery: an update
 Neurosurg Focus 16 (2):Article 8, 2004, Click here to return to Table of Contents Intraoperative monitoring for tethered cord surgery: an update KARL F. KOTHBAUER, M.D., AND KLAUS NOVAK, M.D. Divisions
Neurosurg Focus 16 (2):Article 8, 2004, Click here to return to Table of Contents Intraoperative monitoring for tethered cord surgery: an update KARL F. KOTHBAUER, M.D., AND KLAUS NOVAK, M.D. Divisions
Intra-operative neurologic injuries: Avoidance and prompt response
 Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
Intra-operative neurologic injuries: Avoidance and prompt response James S. Harrop MD, FACS Professor Neurological and Orthopedic Surgery Director, Division of Spine and Peripheral Nerve Surgery Nsurg
The Spinal Cord. The Nervous System. The Spinal Cord. The Spinal Cord 1/2/2016. Continuation of CNS inferior to foramen magnum.
 The Nervous System Spinal Cord Continuation of CNS inferior to foramen magnum Simpler than the brain Conducts impulses to and from brain Two way conduction pathway Reflex actions Passes through vertebral
The Nervous System Spinal Cord Continuation of CNS inferior to foramen magnum Simpler than the brain Conducts impulses to and from brain Two way conduction pathway Reflex actions Passes through vertebral
Somatosenory Evoked Potentials. Ronald Emerson, MD Cornell University Hospital for Special Surgery New York
 Somatosenory Evoked Potentials Ronald Emerson, MD Cornell University Hospital for Special Surgery New York Median SSEPs CPc - Ci CPi - Epc SC5 Epc Medial Lemniscus Epi - Epc Spinal Cord Dorsal Gray Tibial
Somatosenory Evoked Potentials Ronald Emerson, MD Cornell University Hospital for Special Surgery New York Median SSEPs CPc - Ci CPi - Epc SC5 Epc Medial Lemniscus Epi - Epc Spinal Cord Dorsal Gray Tibial
Somatosenory Evoked Potentials
 Somatosenory Evoked Potentials Ronald Emerson, MD Cornell University Hospital for Special Surgery New York Median SSEPs CPc - Ci CPi - Epc SC5 Epc Medial Lemniscus Epi - Epc Spinal Cord Dorsal Gray Tibial
Somatosenory Evoked Potentials Ronald Emerson, MD Cornell University Hospital for Special Surgery New York Median SSEPs CPc - Ci CPi - Epc SC5 Epc Medial Lemniscus Epi - Epc Spinal Cord Dorsal Gray Tibial
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
This document presents the American Society of Neurophysiological
 Journal of Clinical Monitoring and Computing (2005) 19: 437 461 DOI: 10.1007/s10877-005-0086-2 C Springer 2006 Specialty Section on Surgical Neuromonitoring INTRAOPERATIVE MONITORING OF SEGMENTAL SPINAL
Journal of Clinical Monitoring and Computing (2005) 19: 437 461 DOI: 10.1007/s10877-005-0086-2 C Springer 2006 Specialty Section on Surgical Neuromonitoring INTRAOPERATIVE MONITORING OF SEGMENTAL SPINAL
Gross Morphology of Spinal Cord
 Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
SPECTRUM NEUROLOGY GROUP
 SPECTRUM NEUROLOGY GROUP On-Site Diagnostic Testing Patient Care with Quality About Spectrum Neurology Group... Patient Care With Quality Spectrum Neurology Group (SNG), leaders in diagnostic testing,
SPECTRUM NEUROLOGY GROUP On-Site Diagnostic Testing Patient Care with Quality About Spectrum Neurology Group... Patient Care With Quality Spectrum Neurology Group (SNG), leaders in diagnostic testing,
What cranial nerves can we monitor?
 What cranial nerves can we monitor? Laura Hemmer, M.D. SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. What cranial nerve (CN)
What cranial nerves can we monitor? Laura Hemmer, M.D. SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. What cranial nerve (CN)
A/Professor Arun Aggarwal Balmain Hospital
 A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
Chapter 13. The Spinal Cord & Spinal Nerves. Spinal Cord. Spinal Cord Protection. Meninges. Together with brain forms the CNS Functions
 Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Spinal Cord Chapter 13 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Intraoperative Neurophsyiologic Monitoring (sensory-evoked potentials, motor-evoked potentials, EEG monitoring) Original Policy Date
 Original Policy Date") MP 7.01.43 Intraoperative Neurophsyiologic Monitoring (sensory-evoked potentials, motor-evoked potentials, EEG monitoring) Medical Policy Section Surgery Issue 12:2013 Original Policy Date 12:2013 Last
MP 7.01.43 Intraoperative Neurophsyiologic Monitoring (sensory-evoked potentials, motor-evoked potentials, EEG monitoring) Medical Policy Section Surgery Issue 12:2013 Original Policy Date 12:2013 Last
Intraoperative spinal cord monitoring is performed
 J Neurosurg Spine 14:748 753, 2011 Factors predicting the feasibility of monitoring lower-limb muscle motor evoked potentials in patients undergoing excision of spinal cord tumors Clinical article Vedantam
J Neurosurg Spine 14:748 753, 2011 Factors predicting the feasibility of monitoring lower-limb muscle motor evoked potentials in patients undergoing excision of spinal cord tumors Clinical article Vedantam
Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves
 Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper as needed,
Human Anatomy - Problem Drill 11: The Spinal Cord and Spinal Nerves Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully, (2) Work the problems on paper as needed,
Spinal Cord Protection. Chapter 13 The Spinal Cord & Spinal Nerves. External Anatomy of Spinal Cord. Structures Covering the Spinal Cord
 Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
Spinal Cord Protection Chapter 13 The Spinal Cord & Spinal Nerves We are only going to cover Pages 420-434 and 447 Together with brain forms the CNS Functions spinal cord reflexes integration (summation
Chapter 13: The Spinal Cord and Spinal Nerves
 Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Chapter 13: The Spinal Cord and Spinal Nerves Spinal Cord Anatomy Protective structures: Vertebral column and the meninges protect the spinal cord and provide physical stability. a. Dura mater, b. Arachnoid,
Role of IONM in reducing the incidence and severity in pediatric patients with AIS
 Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
THE CONTRIBUTION OF INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING IN NEUROSURGERY
 LUCIAN BLAGA UNIVERSITY SIBIU FACULTY OF MEDICINE DOCTORAL SCHOOL THE CONTRIBUTION OF INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING IN NEUROSURGERY PhD THESIS SUMMARY Academic supervisor: Prof. Univ. Dr.
LUCIAN BLAGA UNIVERSITY SIBIU FACULTY OF MEDICINE DOCTORAL SCHOOL THE CONTRIBUTION OF INTRAOPERATIVE NEUROPHYSIOLOGICAL MONITORING IN NEUROSURGERY PhD THESIS SUMMARY Academic supervisor: Prof. Univ. Dr.
Fig Cervical spinal nerves. Cervical enlargement C7. Dural sheath. Subarachnoid space. Thoracic. Spinal cord Vertebra (cut) spinal nerves
 spinal nerves") Fig. 13.1 C1 Cervical enlargement C7 Cervical spinal nerves Dural sheath Subarachnoid space Thoracic spinal nerves Spinal cord Vertebra (cut) Lumbar enlargement Medullary cone T12 Spinal nerve Spinal nerve
Fig. 13.1 C1 Cervical enlargement C7 Cervical spinal nerves Dural sheath Subarachnoid space Thoracic spinal nerves Spinal cord Vertebra (cut) Lumbar enlargement Medullary cone T12 Spinal nerve Spinal nerve
William R Taylor MD UCSD Neurosurgery June 13, 2017
 William R Taylor MD UCSD Neurosurgery June 13, 2017 The mini-open lateral transpsoas approach was introduced in the literature in 2006 and uses evoked electromyography integrated into the approach and
William R Taylor MD UCSD Neurosurgery June 13, 2017 The mini-open lateral transpsoas approach was introduced in the literature in 2006 and uses evoked electromyography integrated into the approach and
Intraoperative neurophysiological monitoring for the anaesthetist
 Intraoperative neurophysiological monitoring for the anaesthetist Part 2: A review of anaesthesia and its implications for intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB,
Intraoperative neurophysiological monitoring for the anaesthetist Part 2: A review of anaesthesia and its implications for intraoperative neurophysiological monitoring Abstract Van Der Walt JJN, MBChB,
Current Practice of Motor Evoked Potential Monitoring: Results of a Survey
 Journal of Clinical Neurophysiology 19(5):454 460, Lippincott Williams & Wilkins, Inc., Philadelphia 2002 American Clinical Neurophysiology Society Current Practice of Motor Evoked Potential Monitoring:
Journal of Clinical Neurophysiology 19(5):454 460, Lippincott Williams & Wilkins, Inc., Philadelphia 2002 American Clinical Neurophysiology Society Current Practice of Motor Evoked Potential Monitoring:
Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for
 Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Chapter 13 Outline Note: Please refer to handout Spinal Plexuses and Representative Spinal Nerves for what you need to know from Exhibits 13.1 13.4 I. INTRODUCTION A. The spinal cord and spinal nerves
Vestibular Schwannoma Surgery with the use of Intraoperative Monitoring
 Vestibular Schwannoma Surgery with the use of Intraoperative Monitoring Division of Neurosurgery, University of Cape Town August 2018 SNSA Sonia Nunes, Alan Taylor, David Le Feveure Vestibular Schwannoma
Vestibular Schwannoma Surgery with the use of Intraoperative Monitoring Division of Neurosurgery, University of Cape Town August 2018 SNSA Sonia Nunes, Alan Taylor, David Le Feveure Vestibular Schwannoma
Lecture VIII. The Spinal Cord, Reflexes and Brain Pathways!
 Reflexes and Brain Bio 3411! Monday!! 1! Readings! NEUROSCIENCE 5 th ed: Review Chapter 1 pp. 11-21;!!Read Chapter 9 pp. 189-194, 198! THE BRAIN ATLAS 3 rd ed:! Read pp. 4-17 on class web site! Look at
Reflexes and Brain Bio 3411! Monday!! 1! Readings! NEUROSCIENCE 5 th ed: Review Chapter 1 pp. 11-21;!!Read Chapter 9 pp. 189-194, 198! THE BRAIN ATLAS 3 rd ed:! Read pp. 4-17 on class web site! Look at
CHAPTER 10 THE SOMATOSENSORY SYSTEM
 CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
CHAPTER 10 THE SOMATOSENSORY SYSTEM 10.1. SOMATOSENSORY MODALITIES "Somatosensory" is really a catch-all term to designate senses other than vision, hearing, balance, taste and smell. Receptors that could
Urodynamic and electrophysiological investigations in neuro-urology
 Urodynamic and electrophysiological investigations in neuro-urology Pr. Gerard Amarenco Neuro-Urology and Pelvic-Floor Investigations Department Tenon Hospital, Assistance Publique Hôpitaux de Paris, Er6,
Urodynamic and electrophysiological investigations in neuro-urology Pr. Gerard Amarenco Neuro-Urology and Pelvic-Floor Investigations Department Tenon Hospital, Assistance Publique Hôpitaux de Paris, Er6,
ANS/BSCN Guidelines for Neurophysiological Recordings of the Spinal Cord during Corrective Spinal Deformity Surgery
 ANS/BSCN Guidelines for Neurophysiological Recordings of the Spinal Cord during Corrective Spinal Deformity Surgery Contributors: Peter Walsh MSc Clinical Physiologist 1, Dr Joseph Cowan Consultant in
ANS/BSCN Guidelines for Neurophysiological Recordings of the Spinal Cord during Corrective Spinal Deformity Surgery Contributors: Peter Walsh MSc Clinical Physiologist 1, Dr Joseph Cowan Consultant in
An Electrode Configuration for Recording Muscle Motor Evoked Potentials in the Upper Extremities during Intraoperative Neurophysiological Monitoring
 Technical Note J Korean Neurosurg Soc 60 (4) : 475-480, 2017 https://doi.org/10.3340/jkns.2016.0506.006 pissn 2005-3711 eissn 1598-7876 An Electrode Configuration for Recording Muscle Motor Evoked Potentials
Technical Note J Korean Neurosurg Soc 60 (4) : 475-480, 2017 https://doi.org/10.3340/jkns.2016.0506.006 pissn 2005-3711 eissn 1598-7876 An Electrode Configuration for Recording Muscle Motor Evoked Potentials
Index. Note: Page numbers of article titles are in boldface type.
 Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Neurol Clin N Am 20 (2002) 605 617 Index Note: Page numbers of article titles are in boldface type. A ALS. See Amyotrophic lateral sclerosis (ALS) Amyotrophic lateral sclerosis (ALS) active denervation
Spinal Cord Organization. January 12, 2011
 Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
Spinal Cord Organization January 12, 2011 Spinal Cord 31 segments terminates at L1-L2 special components - conus medullaris - cauda equina no input from the face Spinal Cord, Roots & Nerves Dorsal root
Multimodal Intraoperative Neurophysiological Monitoring in Spinal Cord Surgery
 DOI: 10.5137/1019-5149.JTN.16414-15.1 Received: 23.10.2015 / Accepted: 28.12.2015 Published Online: 28.07.2016 Original Investigation Multimodal Intraoperative Neurophysiological Monitoring in Spinal Cord
DOI: 10.5137/1019-5149.JTN.16414-15.1 Received: 23.10.2015 / Accepted: 28.12.2015 Published Online: 28.07.2016 Original Investigation Multimodal Intraoperative Neurophysiological Monitoring in Spinal Cord
Cortical Control of Movement
 Strick Lecture 2 March 24, 2006 Page 1 Cortical Control of Movement Four parts of this lecture: I) Anatomical Framework, II) Physiological Framework, III) Primary Motor Cortex Function and IV) Premotor
Strick Lecture 2 March 24, 2006 Page 1 Cortical Control of Movement Four parts of this lecture: I) Anatomical Framework, II) Physiological Framework, III) Primary Motor Cortex Function and IV) Premotor
Femoral nerve palsy is a feared neurological complication
 SPINE Volume 39, Number 15, pp 1254-1260 2014, Lippincott Williams & Wilkins SURGERY Saphenous Nerve Somatosensory Evoked Potentials A Novel Technique to Monitor the Femoral Nerve During Transpoas Lumbar
SPINE Volume 39, Number 15, pp 1254-1260 2014, Lippincott Williams & Wilkins SURGERY Saphenous Nerve Somatosensory Evoked Potentials A Novel Technique to Monitor the Femoral Nerve During Transpoas Lumbar
Overview. Spinal Anatomy Spaces & Meninges Spinal Cord. Anatomy of the dura. Anatomy of the arachnoid. Anatomy of the spinal meninges
 European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
European Course in Neuroradiology Module 1 - Anatomy and Embryology Dubrovnik, October 2018 Spinal Anatomy Spaces & Meninges Spinal Cord Johan Van Goethem Overview spinal meninges & spaces spinal cord
BIOH111. o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system
 BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 Textbook and required/recommended
BIOH111 o Cell Module o Tissue Module o Integumentary system o Skeletal system o Muscle system o Nervous system o Endocrine system Endeavour College of Natural Health endeavour.edu.au 1 Textbook and required/recommended
Spinal cord. We have extension of the pia mater below L1-L2 called filum terminale
 Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Spinal cord Part of the CNS extend from foramen magnum to the level of L1-L2 (it is shorter than the vertebral column) it is covered by spinal meninges. It is cylindrical in shape. It s lower end become
Department of Neurology/Division of Anatomical Sciences
 Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
Spinal Cord I Lecture Outline and Objectives CNS/Head and Neck Sequence TOPIC: FACULTY: THE SPINAL CORD AND SPINAL NERVES, Part I Department of Neurology/Division of Anatomical Sciences LECTURE: Monday,
SOMATIC SENSATION PART I: ALS ANTEROLATERAL SYSTEM (or SPINOTHALAMIC SYSTEM) FOR PAIN AND TEMPERATURE
 FOR PAIN AND TEMPERATURE") Dental Neuroanatomy Thursday, February 3, 2011 Suzanne S. Stensaas, PhD SOMATIC SENSATION PART I: ALS ANTEROLATERAL SYSTEM (or SPINOTHALAMIC SYSTEM) FOR PAIN AND TEMPERATURE Reading: Waxman 26 th ed, :
Dental Neuroanatomy Thursday, February 3, 2011 Suzanne S. Stensaas, PhD SOMATIC SENSATION PART I: ALS ANTEROLATERAL SYSTEM (or SPINOTHALAMIC SYSTEM) FOR PAIN AND TEMPERATURE Reading: Waxman 26 th ed, :
Anatomy of the Spinal Cord
 Spinal Cord Anatomy of the Spinal Cord Anatomy of the Spinal Cord Posterior spinal arteries Lateral corticospinal tract Dorsal column Spinothalamic tract Anterior spinal artery Anterior white commissure
Spinal Cord Anatomy of the Spinal Cord Anatomy of the Spinal Cord Posterior spinal arteries Lateral corticospinal tract Dorsal column Spinothalamic tract Anterior spinal artery Anterior white commissure
Intraoperative Neurophysiologic Monitoring
 Intraoperative Neurophysiologic Monitoring Policy Number: 7.01.58 Last Review: 7/2017 Origination: 10/1988 Next Review: 5/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Intraoperative Neurophysiologic Monitoring Policy Number: 7.01.58 Last Review: 7/2017 Origination: 10/1988 Next Review: 5/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Perineal Electrophysiologic Tests
 Perineal disorders and emg! Perineal Electrophysiologic Tests Voiding dysfunction Stress Urinary Incontinence urgency OAB Urge Incontinence nocturia Pr. Gerard Amarenco Mixed Incontinence frequency Service
Perineal disorders and emg! Perineal Electrophysiologic Tests Voiding dysfunction Stress Urinary Incontinence urgency OAB Urge Incontinence nocturia Pr. Gerard Amarenco Mixed Incontinence frequency Service
Neurophysiological Monitoring
 2 Basis of Intraoperative Neurophysiological Monitoring Introduction Reducing the Risk of Neurological Deficits Techniques for Reducing Postoperative Neurological Deficits Interpretation of Neuroelectric
2 Basis of Intraoperative Neurophysiological Monitoring Introduction Reducing the Risk of Neurological Deficits Techniques for Reducing Postoperative Neurological Deficits Interpretation of Neuroelectric
Gross Morphology of Spinal Cord
 Gross Morphology of Spinal Cord Done By : Rahmeh Alsukkar ** I did my best and sorry for any mistake ** the sheet does not contain pictures, tables and some slides so please be careful and go back to slides
Gross Morphology of Spinal Cord Done By : Rahmeh Alsukkar ** I did my best and sorry for any mistake ** the sheet does not contain pictures, tables and some slides so please be careful and go back to slides
INTRAOPERATIVE MONITORING USING SOMATOSENSORY EVOKED POTENTIALS A POSITION STATEMENT BY THE AMERICAN SOCIETY OF NEUROPHYSIOLOGICAL MONITORING
 INTRAOPERATIVE MONITORING USING SOMATOSENSORY EVOKED POTENTIALS A POSITION STATEMENT BY THE AMERICAN SOCIETY OF NEUROPHYSIOLOGICAL MONITORING Committee Chairman: J. Richard Toleikis, Ph.D. (Updated December,
INTRAOPERATIVE MONITORING USING SOMATOSENSORY EVOKED POTENTIALS A POSITION STATEMENT BY THE AMERICAN SOCIETY OF NEUROPHYSIOLOGICAL MONITORING Committee Chairman: J. Richard Toleikis, Ph.D. (Updated December,
Nervous System. The Peripheral Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Reflexes Pathways
 Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Sensory Motor Review of CNS v. PNS Central nervous system (CNS) Brain Spinal cord Peripheral nervous system (PNS) All
Nervous System Agenda Review of CNS v. PNS PNS Basics Cranial Nerves Spinal Nerves Sensory Motor Review of CNS v. PNS Central nervous system (CNS) Brain Spinal cord Peripheral nervous system (PNS) All
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Presented by. Andrew Kopka B.S. CNIM R. EEG T
 Presented by Andrew Kopka B.S. CNIM R. EEG T 1 2 ! Common EP s / recordings used in the O.R. SSEP - Somatosensory evoked potentials TcMEP - Transcranial motor evoked potentials BAER - Brainstem auditory
Presented by Andrew Kopka B.S. CNIM R. EEG T 1 2 ! Common EP s / recordings used in the O.R. SSEP - Somatosensory evoked potentials TcMEP - Transcranial motor evoked potentials BAER - Brainstem auditory
ESCOME Pre-Course Outline (v1.09)
") ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
*Anteriolateral spinothalamic tract (STT) : a sensory pathway that is positioned anteriorly and laterally in the spinal cord.
 : a sensory pathway that is positioned anteriorly and laterally in the spinal cord.") *somatic sensations : PAIN *Anteriolateral spinothalamic tract (STT) : a sensory pathway that is positioned anteriorly and laterally in the spinal cord. *This pathway carries a variety of sensory modalities:
*somatic sensations : PAIN *Anteriolateral spinothalamic tract (STT) : a sensory pathway that is positioned anteriorly and laterally in the spinal cord. *This pathway carries a variety of sensory modalities:
SOMATOSENSORY SYSTEMS: Pain and Temperature Kimberle Jacobs, Ph.D.
 SOMATOSENSORY SYSTEMS: Pain and Temperature Kimberle Jacobs, Ph.D. Sensory systems are afferent, meaning that they are carrying information from the periphery TOWARD the central nervous system. The somatosensory
SOMATOSENSORY SYSTEMS: Pain and Temperature Kimberle Jacobs, Ph.D. Sensory systems are afferent, meaning that they are carrying information from the periphery TOWARD the central nervous system. The somatosensory
Decreased Amplitude and Increased Latency in OR Communication During Anterior/Posterior Spinal Fusion
 Title: Moderators: Decreased Amplitude and Increased Latency in OR Communication During Anterior/Posterior Spinal Fusion Wendy Binstock, M.D. Associate Professor, Department of Anesthesia and Critical
Title: Moderators: Decreased Amplitude and Increased Latency in OR Communication During Anterior/Posterior Spinal Fusion Wendy Binstock, M.D. Associate Professor, Department of Anesthesia and Critical
Technologies and architectures" Stimulator, electrodes, system flexibility, reliability, security, etc."
 March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
March 2011 Introduction" Basic principle (Depolarization, hyper polarization, etc.." Stimulation types (Magnetic and electrical)" Main stimulation parameters (Current, voltage, etc )" Characteristics (Muscular
See the corresponding article in this issue, pp J Neurosurg Spine 20: , 2014 AANS, 2014
 See the corresponding article in this issue, pp 692 704. J Neurosurg Spine 20:675 691, 2014 AANS, 2014 Neuromonitoring with pulse-train stimulation for implantation of thoracic pedicle screws: a blinded
See the corresponding article in this issue, pp 692 704. J Neurosurg Spine 20:675 691, 2014 AANS, 2014 Neuromonitoring with pulse-train stimulation for implantation of thoracic pedicle screws: a blinded
Cranial Nerves and Spinal Cord Flashcards
 1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
1. Name the cranial nerves and their Roman numeral. 2. What is Cranial Nerve I called, and what does it 3. Scientists who are trying to find a way to make neurons divide to heal nerve injuries often study
Pathways of proprioception
 The Autonomic Nervous Assess Prof. Fawzia Al-Rouq Department of Physiology College of Medicine King Saud University Pathways of proprioception System posterior column& Spinocerebellar Pathways https://www.youtube.com/watch?v=pmeropok6v8
The Autonomic Nervous Assess Prof. Fawzia Al-Rouq Department of Physiology College of Medicine King Saud University Pathways of proprioception System posterior column& Spinocerebellar Pathways https://www.youtube.com/watch?v=pmeropok6v8
ANATOMY OF SPINAL CORD. Khaleel Alyahya, PhD, MEd King Saud University School of
 ANATOMY OF SPINAL CORD Khaleel Alyahya, PhD, MEd King Saud University School of Medicine @khaleelya OBJECTIVES At the end of the lecture, students should be able to: Describe the external anatomy of the
ANATOMY OF SPINAL CORD Khaleel Alyahya, PhD, MEd King Saud University School of Medicine @khaleelya OBJECTIVES At the end of the lecture, students should be able to: Describe the external anatomy of the
Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses. A & P II Spring, 2014
 Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses A & P II Spring, 2014 Objectives Be able to identify specified spinal cord structures and spinal nerves on models Be familiar with spinal nerve
Lab # 2: Spinal Cord & Nerves, Reflexes and General Senses A & P II Spring, 2014 Objectives Be able to identify specified spinal cord structures and spinal nerves on models Be familiar with spinal nerve
Nerve Conduction Studies NCS
 Nerve Conduction Studies NCS Nerve conduction studies are an essential part of an EMG examination. The clinical usefulness of NCS in the diagnosis of diffuse and local neuropathies has been thoroughly
Nerve Conduction Studies NCS Nerve conduction studies are an essential part of an EMG examination. The clinical usefulness of NCS in the diagnosis of diffuse and local neuropathies has been thoroughly
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13)
") Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
Nervous System: Spinal Cord and Spinal Nerves (Chapter 13) Lecture Materials for Amy Warenda Czura, Ph.D. Suffolk County Community College Eastern Campus Primary Sources for figures and content: Marieb,
The Spinal Cord & Spinal Nerves
 The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
The Spinal Cord & Spinal Nerves Together with brain forms the CNS Functions spinal cord reflexes integration (summation of inhibitory and excitatory) nerve impulses highway for upward and downward travel
Nerve Conduction Studies NCS
 Nerve Conduction Studies NCS Nerve conduction studies are an essential part of an EMG examination. The clinical usefulness of NCS in the diagnosis of diffuse and local neuropathies has been thoroughly
Nerve Conduction Studies NCS Nerve conduction studies are an essential part of an EMG examination. The clinical usefulness of NCS in the diagnosis of diffuse and local neuropathies has been thoroughly
STRUCTURAL ORGANIZATION OF THE NERVOUS SYSTEM
 STRUCTURAL ORGANIZATION OF THE NERVOUS SYSTEM STRUCTURAL ORGANIZATION OF THE BRAIN The central nervous system (CNS), consisting of the brain and spinal cord, receives input from sensory neurons and directs
STRUCTURAL ORGANIZATION OF THE NERVOUS SYSTEM STRUCTURAL ORGANIZATION OF THE BRAIN The central nervous system (CNS), consisting of the brain and spinal cord, receives input from sensory neurons and directs
Lab Activity 13. Spinal Cord. Portland Community College BI 232
 Lab Activity 13 Spinal Cord Portland Community College BI 232 Definitions Tracts: collections of axons in CNS Nerves:collections of axons in PNS Ganglia: collections of neuron cell bodies in PNS Nucleus
Lab Activity 13 Spinal Cord Portland Community College BI 232 Definitions Tracts: collections of axons in CNS Nerves:collections of axons in PNS Ganglia: collections of neuron cell bodies in PNS Nucleus
Neural Integration I: Sensory Pathways and the Somatic Nervous System
 15 Neural Integration I: Sensory Pathways and the Somatic Nervous System PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to Sensory Pathways and
15 Neural Integration I: Sensory Pathways and the Somatic Nervous System PowerPoint Lecture Presentations prepared by Jason LaPres Lone Star College North Harris An Introduction to Sensory Pathways and
MOTOR EVOKED POTENTIALS AND TRANSCUTANEOUS MAGNETO-ELECTRICAL NERVE STIMULATION
 MOTOR EVOKED POTENTIAS AND TRANSCUTANEOUS MAGNETO-EECTRICA NERVE STIMUATION Hongguang iu, in Zhou 1 and Dazong Jiang Xian Jiaotong University, Xian, People s Republic of China 1 Shanxi Normal University,
MOTOR EVOKED POTENTIAS AND TRANSCUTANEOUS MAGNETO-EECTRICA NERVE STIMUATION Hongguang iu, in Zhou 1 and Dazong Jiang Xian Jiaotong University, Xian, People s Republic of China 1 Shanxi Normal University,
Clinical Policy Title: Somatosensory evoked potentials (SEPs or SSEPs) test
 test") Clinical Policy Title: Somatosensory evoked potentials (SEPs or SSEPs) test Clinical Policy Number: 09.01.10 Effective Date: January 1, 2016 Initial Review Date: June 16, 2013 Most Recent Review Date:
Clinical Policy Title: Somatosensory evoked potentials (SEPs or SSEPs) test Clinical Policy Number: 09.01.10 Effective Date: January 1, 2016 Initial Review Date: June 16, 2013 Most Recent Review Date:
CLINICAL GOVERNANCE UPDATED ANS/BSCN GUIDELINES FOR NEUROPHYSIOLOGICAL RECORDINGS OF THE SPINAL CORD DURING CORRECTIVE SPINAL DEFORMITY SURGERY
 CLINICAL GOVERNANCE UPDATED ANS/BSCN GUIDELINES FOR NEUROPHYSIOLOGICAL RECORDINGS OF THE SPINAL CORD DURING CORRECTIVE SPINAL DEFORMITY SURGERY Version 2 Contributors: Grover, H. 1 ; Walsh, P. 2, Sanders,
CLINICAL GOVERNANCE UPDATED ANS/BSCN GUIDELINES FOR NEUROPHYSIOLOGICAL RECORDINGS OF THE SPINAL CORD DURING CORRECTIVE SPINAL DEFORMITY SURGERY Version 2 Contributors: Grover, H. 1 ; Walsh, P. 2, Sanders,