PRACTICAL INSIGHTS IN ORAL PATHOLOGY. Kirk Y. Hirata, MD January 13, 2017
|
|
|
- Francine Wiggins
- 5 years ago
- Views:
Transcription
1 PRACTICAL INSIGHTS IN ORAL PATHOLOGY Kirk Y. Hirata, MD January 13, 2017
2 ROAD TO THE PODIUM? : LLUSM : Anatomic and Clinical Pathology Residency, UH John A. Burns School of Medicine : Hematopathology Fellowship, Scripps Clinic, San Diego July 1995: HPL - new business, niche?
3 ORAL PATHOLOGY outpatient biopsies, some were from dentists s/o inflammation, benign odontogenic cyst, etc no service to general dentists or oral surgeons wife was a dentist, residency at QMC idea?
4 ORAL PATHOLOGY telephone calls lunches (marketing) textbooks courses, including microscopy began to acquire cases QMC dental resident teaching once a month







5


6
7 AFTER 21 YEARS established myself in the community as an oral pathologist QMC Dental Residency Program has been recognized 7 TH edition of Jordan (1999) UCSF consultation service

8 Dr. Richard Jordan Professor of Oral Pathology, Pathology & Radiation Oncology UCSF Dermatopathology & Oral Pathology Service I feel fortunate to have joined this group of outstanding dermatopathologists. I believe that my training, experience and expertise in oral and maxillofacial pathology expands the scope and breadth of services that we are able to offer the medical and dental community for their diagnostic pathology needs. I initially trained as a dentist at the University of Toronto that was followed by an internship at the Toronto Western Hospital (now the University Health Network). Following training in anatomic pathology I completed a residency in oral and maxillofacial pathology under the direction of Dr. Jim Main. I also completed a fellowship in oral medicine and then a Master of Science degree in oral pathology. I was fortunate to be able to train with Professor Paul Speight at the University of London were I was awarded a PhD degree in Experimental Pathology. My first faculty position was at the University of Toronto where I practiced oral pathology and oral medicine and developed a research program in oral cancer. In 2000 I relocated to the University of California San Francisco and have been director of the oral pathology service since I have published over 130 peer reviewed publications, many invited reviews and I am the author of two leading textbooks, one in oral pathology (Regezi, Sciubba and Jordan. Oral Pathology: Clinical pathologic correlations 6th ed) and the other in oral medicine (Lewis and Jordan. Color Handbook of Oral Medicine 2nd edition). I am also the Medical Director (working with Dr. Nilsa Ramirez and Dr. Soon Paik) of the NRG Oncology Biospecimen Bank that is based in San Francisco, Columbus OH and Pittsburgh PA supporting phase II and phase III practice changing therapeutic trials for head and neck, breast, colorectal, lung, prostate and brain cancers. Enrolling 5099 patients each year, this biospecimen bank collects, stores, reviews and distributes over 150,000 biospecimens each year as part of the primary trials and translational research. I am delighted to contribute to the UCSF Dermatopathology and Oral Pathology Service and enjoy providing a high level of diagnostic pathology and expert opinion for clinicians and pathologists for lesions in the head and neck.
9

10 ACKNOWLEDGEMENTS



11 GOALS/OBJECTIVES community practice, not OM surgeons lesions you are likely to encounter what is the next step? discuss and advise with patient
12 LESION TYPES Mucosal bumps White/red Pigmented Vesiculobullous Jaw cysts and tumors Bone
13 LECTURE SCHEDULE Mucosal bumps White/red lesions - not SCCA Pigmented lesions BREAK Vesiculobullous lesions Jaw cysts (few tumors) Bone lesions - including BRONJ
14 MUCOSAL BUMPS raised lesions, usually with intact mucosa and normal color irritation fibroma mucocele vascular lesions PG/POF/PGCG squamous papilloma neural lesions




15 IRRITATION FIBROMA reactive fibrosis (scar) recurrence with irritation or trauma no malignant potential




16 VARIANTS


17 DENTURE-INDUCED FIBROUS HYPERPLASIA inflammatory fibrous hyperplasia, epulis fissuratum chronic trauma related to ill-fitting denture surgery and new denture




18 MUCOCELE cyst-like collection of mucin that spills from traumatized salivary duct common in 1 st 3 decades excision including salivary gland tissue in vicinity


19 SJÖGREN S SYNDROME Focus = glandular area that contains 50 or more lymphocytes/plasma cells Focus score = # foci in 4 mm2 area Focus score > 1 is consistent with SS





20 VASCULAR LESION bluish bleb, small or large






21 PYOGENIC GRANULOMA reactive proliferation of blood vessels and fibroblasts etiology - plaque, hormone recurrence 5%





22 PERIPHERAL OSSIFYING FIBROMA fibroblast proliferation with mineralized component (woven bone or cementum)



23 PERIPHERAL GIANT CELL GRANULOMA proliferation of mononuclear and multinucleated giant cells excision, remove underlying irritating factor - 15% recurrence


24 SQUAMOUS PAPILLOMA/ VERRUCA VULGARIS exophytic/verrucous growth younger patients HPV subtype 2, 6, 11







25 NEURAL LESION most common benign spindle cell lesion in oral cavity solitary, traumatic etiology granular cell tumor


,")
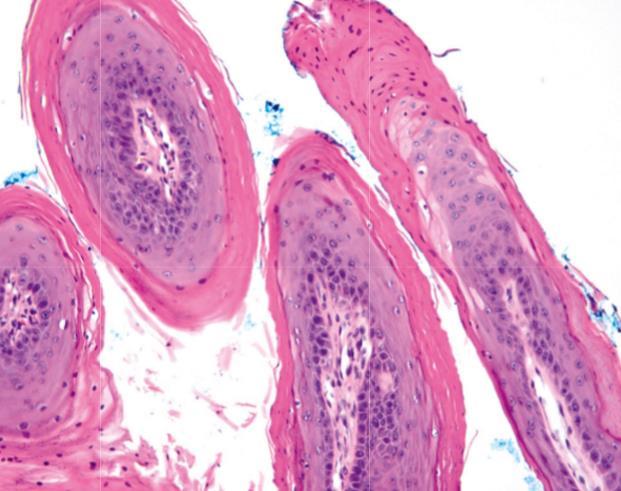
26 FORDYCE S GRANULES 1 to 3 mm yellowish papules, adults (60%), buccal mucosa and lip



27 ECTOPIC LYMPHOID TISSUE small, yellow-white, dome-shaped elevations normal tissue in unusual location lingual tonsil

28 GINGIVAL LESION/NODULE reactive/inflammatory peripheral (extraosseous) cyst or tumor soft tissue tumor extension of intrabony lesion into gingiva metastasis



29
30 WHITE/RED LESIONS (WHO DEFINITIONS) Leukoplakia - persistent white mucosal patch or plaque that cannot be scraped off Erythroplakia - persistent red mucosal patch with or without erosion Erythroleukoplakia - speckled lesion with features of both Verrucous hyperplasia - superficial lesion, white and corrugated
31 ERYTHROLEUKOPLAKIA (SPECKLED)/ERYTHROPLAKIA some leukoplakic lesions develop scattered patches of redness epithelial cells no longer produce keratin and atrophic, allowing underlying microvasculature to show through less common than leukoplakia, but greater potential for dysplasia at the time of biopsy




32

33 LEUKOPLAKIA
34 CLINICAL FEATURES older individuals (60 years), males, young? lower lip, buccal mucosa, gingiva (70%) lip vermilion, oral floor, and tongue - more often associated with dysplasia or carcinoma
35 GENERALIZATIONS 16% (5 to 25%) of benign hyperkeratosis will develop into dysplasia and/or carcinoma 16-36% of dysplasias develop into invasive carcinoma
36

37




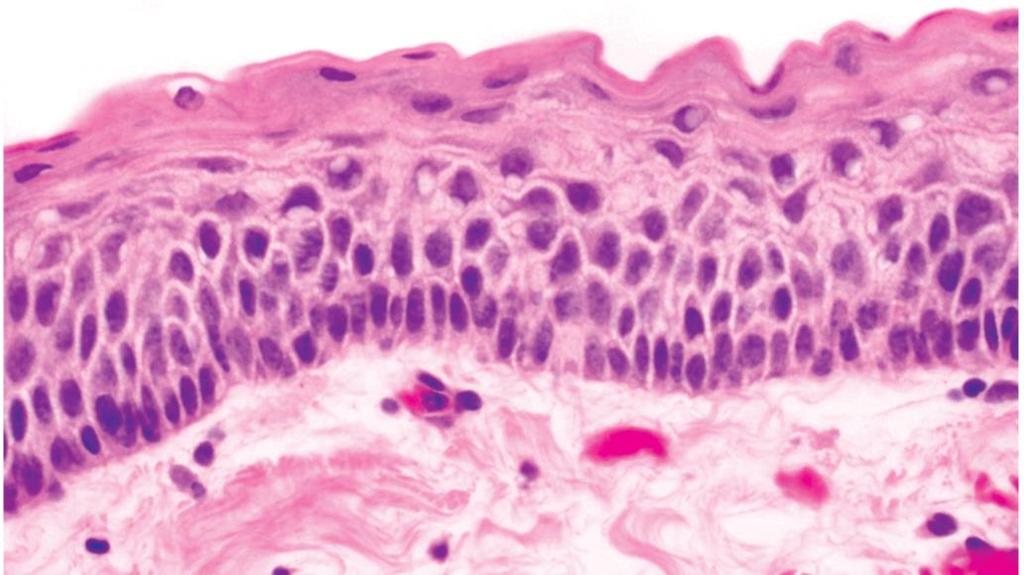
38 GRADES OF EPITHELIAL DYSPLASIA CIS - absence of invasion, metastasis cannot occur MILD MODERATE SEVERE/CIS

39
40





41 SQUAMOUS CELL CARCINOMA
42
43
44

45

46

47

48
49
50
51
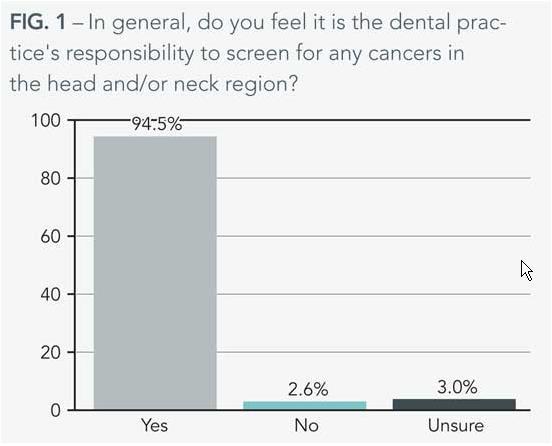
52 DENTAL SCREENING all patient exams should include a comprehensive history systematic visual and tactile examination of not only the oral soft tissues, but also those of the head and neck ancillary techniques to aid in the identification of premalignant and malignant oral lesions
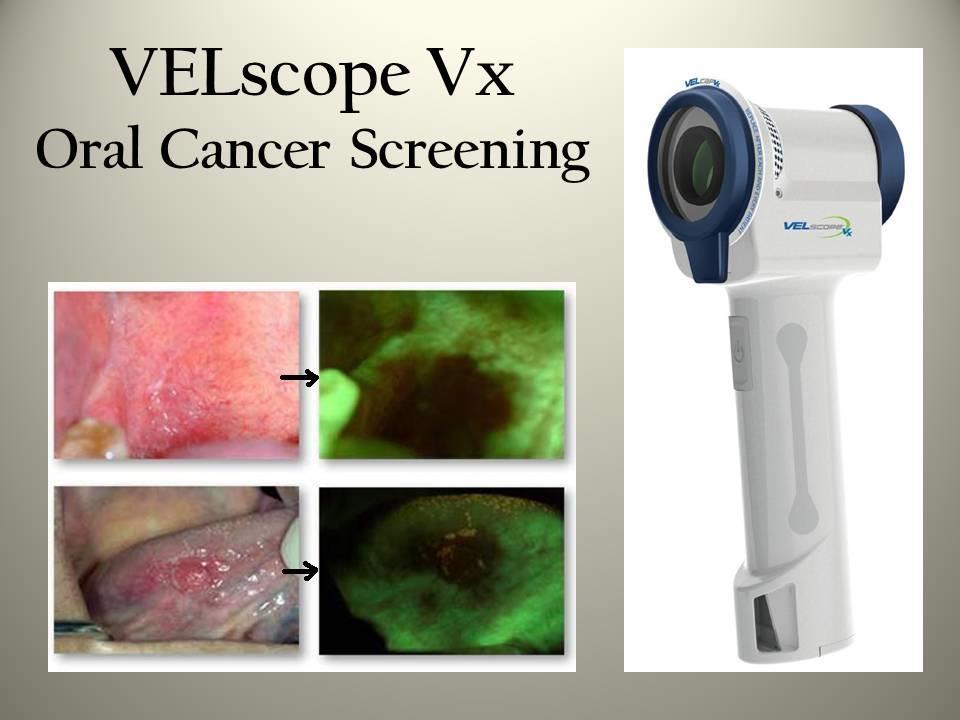
53 ORAL CANCER SCREENING DEVICE commercial devices were designed to further assist the dental practitioner identify early tissue changes assess the biological significance of a mucosal lesion explore morphological and biochemical tissue alterations that cannot be observed by normal incandescent light

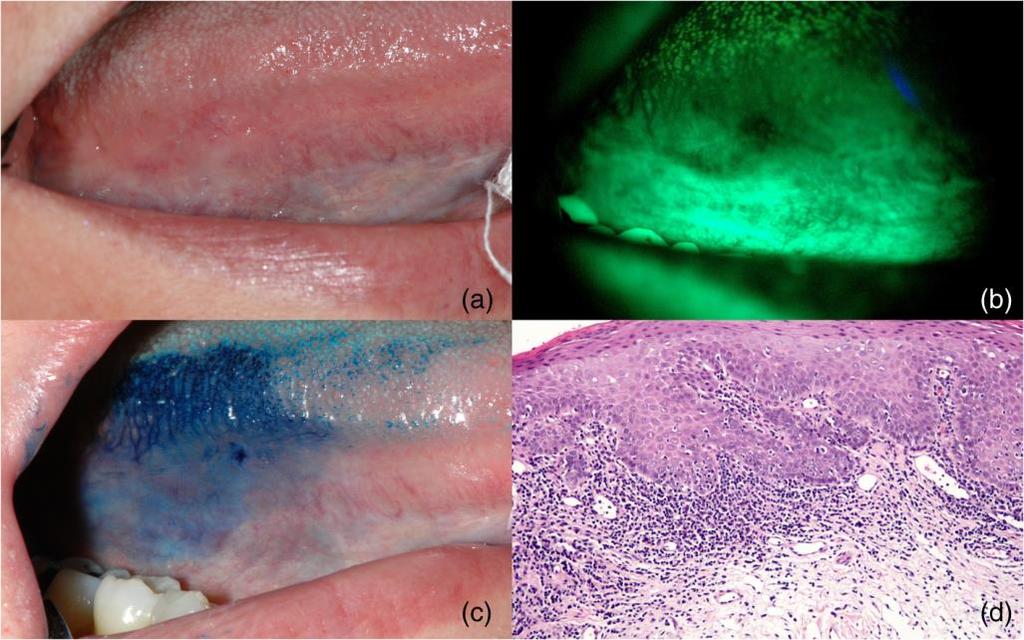
54 Toluidine Blue

55


56
57



58


59
60 ADA COUNCIL ON SCIENTIFIC AFFAIRS AND THE CDC conclude that these adjunctive aids may not significantly improve the detection and diagnosis of potentially malignant lesions current level of scientific evidence was insufficient to support recommending the routine use of any of these devices in routine practice
61 JADA, Vol. 141, May 2010 until then? increased patient education about the risks for oral cancer clinical vigilance suspicious or persistent lesions should be biopsied histologic examination remains the current gold standard for oral cancer and precancer diagnosis

62
63 SALIVA TEST FOR ORAL CANCER SaliMark OSCC (PeriRx, LLC) noninvasive, oral diagnostic technology - salivary exrna biomarker test for oral SCC decade of NIH-funded research and prevalidation work at UCLA and MSU signature mutations (biomarkers) that may be associated with oral cancers screening test for early detection (before symptoms) to reduce morbidity and mortality



64
65 TREATMENT AND PROGNOSIS (LEUKOPLAKIA) clinical term, biopsy required for diagnosis and to guide appropriate management tobacco cessation complete excision for moderate dysplasia and greater 10-35% recurrence rate, new lesions clinical evaluation every 6 months, longterm f/u
66 MANAGEMENT
67 SMOKELESS TOBACCO (TOBACCO POUCH KERATOSIS) chewing tobacco, dry snuff, and moist snuff - latter most popular younger age (12 years), highest prevalence in midwestern and SE states gingival recession and bone resorption, increased caries? dysplasia is uncommon, usually mild, regress





68 TOBACCO POUCH KERATOSIS

69
70 BETEL HABIT 10-20% of the world s population (WHO estimates 600 million people) cultural, early age, habitually chew 16 to 24 hours daily Indian subcontinent and Asian countries (SE Asia, Taiwan, Southern China, Polynesia, Micronesia including Guam) psychoactive substance - nicotine, alcohol, caffeine, betel nut
71 BETEL QUID (PAAN) quid - leaf wrapped around a mixture of areca nut, slaked lime, possibly tobacco, and sometimes sweeteners and spices commercially available, freeze-dried betel quid substitutes (pan masala, gutkha, mawa) slaked lime releases alkaloids from the areca nut - feeling of euphoria



72

73
74 ORAL SUBMUCOUS FIBROSIS alkaloids also stimulate fibroblasts resulting in oral submucous fibrosis - high risk, precancerous condition chronic, progressive scarring of the oral (buccal) mucosa - interincisal distance of 20 mm inability to open the mouth (trismus) and generalized oral burning sensation (stomatopyrosis) with intolerance to spicy foods
75 ORAL SUBMUCOUS FIBROSIS dysplasia in 10 to 15% of cases carcinoma in 6% does not regress with habit cessation limited treatment 8% rate of malignant transformation (19x risk)




76
77 RAISING AWARENESS any evidence of health benefits is limited WHO classifies betel nut as a carcinogen FDA has placed nut on its Poisonous Plants Database CDC warns of addiction, oral fibrosis, and cancer Taiwan - Betel Nut Prevention Day
78 PIGMENTED LESIONS usually brown in color alarming when raised or erosion includes vascular lesions - blanch




79 AMALGAM TATTOO macule, usually localized and evenly pigmented gingiva adjacent to amalgam restorations or crowns, apicoectomy with amalgam retrofill leaches out or traumatically implanted and stains reticulin fibers (argyrophilic)




80 ORAL MELANOTIC MACULE adults, 5 th decade less than 1 cm, evenly pigmented idiopathic, postinflammatory hypermelanosis


81 ORAL MELANOCYTIC NEVUS 3 rd or 4 th decade macule, plaque, or nodule intramucosal, blue nevus excision is curative



82 BLUE NEVUS


83
84 MUCOSAL MELANOMA 1-8% of head and neck melanoma, much more common in sinonasal cavity older patients, males (blacks, asians) > 1 cm, irregularly pigmented, borders irregular, nodularity and ulcer excision, recurrence rate is 50%, survival may not be improved with radiotherapy




85
86 BREAK
87 VESICULOBULLOUS LESIONS 3 P s - lichen planus, mucous membrane pemphigoid, pemphigus vulgaris Wickham striae middle age females skin findings slough (blister) when rub vs Candida Michele s solution - DIF

88 DIF


89
90 LICHEN PLANUS/LICHENOID MUCOSITIS considered autoimmune by some, target lesion not yet identified middle age females skin involvement in 10-15% of patients malignant transformation?


 topical")
91 LICHEN PLANUS reticulated keratosis with variable erythema T-cell destruction of basal cells (lichenoid) topical antiinflammatory therapy

92


93 IMMUNOFLUORESCENCE Shaggy junction Civatte bodies

94
95 MUCOUS MEMBRANE PEMPHIGOID subepithelial blistering with autoantibodies desquamative gingivitis DIF shows linear IgG or C3 at basement membrane zone




96 Mucous membrane pemphigoid




97 PEMPHIGUS VULGARIS Ashkenazi-Jewish descent, Caucasian in US, Asians painful erosions/ulcers - palate antibodies against desmoglein-3 DIF - intercellular deposition of IgG

98

99
100 JAW CYSTS


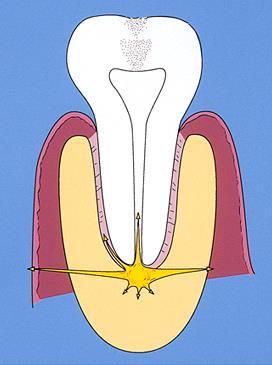
101 TOOTH ANATOMY

102
103

104
, osteoclast activation with bone resorption (periapical radiolucency) abscess spreads along path of least resistance")
105 PERIAPICAL PATHOLOGY pulpal death from cavity/restoration or trauma accumulation of inflammatory cells at the apex of a nonvital tooth (periodontitis), osteoclast activation with bone resorption (periapical radiolucency) abscess spreads along path of least resistance (parulis)
106 disease
107



108 PERIAPICAL CYST
109 ODONTOGENIC CYSTS cysts within jaw bones lined by odontogenic epithelium developmental or inflammatory in origin although rare, most primary intraosseous carcinomas arise from malignant transformation of the lining of an odontogenic cyst
")
 of")



110 DENTIGEROUS CYST (FOLLICULAR/ERUPTION) originates from follicle around crown (CEJ) of unerupted tooth - impacted wisdom most common (20%) accumulation of fluid, 5 mm 10 to 30 years of age, slight male ameloblastoma, SCC, mucoepidermoid carcinoma




111



112
113 KERATOCYSTIC ODONTOGENIC TUMOR (ODONTOGENIC KERATOCYST) cell rests of the dental lamina associated molecular genetic alterations, so now considered a benign cystic neoplasm 10 to 40 years, slight male, mandible high recurrence rate (30%), mural cysts nevoid basal cell carcinoma (Gorlin) syndrome

114




115
116 OKC TREATMENT enucleation and curettage peripheral ostectomy with a bone bur chemical cauterization with Carnoy s solution marsupialization with drainage tube to allow decompression and reduction in size before removal
117 NEVOID BASAL CELL CARCINOMA SYNDROME
118 ORTHOKERATINIZED ODONTOGENIC CYST orthokeratinized variant of OKC orthokeratinized epithelial lining (as compared to parakeratin of OKC) young adults, male, posterior mandible enucleation with curettage, rarely recurs



119 ORTHOKERATINIZED ODONTOGENIC CYST
120 GINGIVAL CYST newborn (up to 3 months) - rupture spontaneously alveolar mucosa - remnants of dental lamina (rests of Serres) adults - soft tissue counterpart of LPC mandibular canine and premolar area simple surgical excision




121 GINGIVAL CYST
122 LATERAL PERIODONTAL (BOTRYOID) CYST occurs along the lateral root surface rests of dental lamina intrabony counterpart of the adult gingival cyst 5 th to 7 th decade, mandibular premolarcanine-lateral incisor area conservative enucleation, recurrence is unusual

123






124 LATERAL PERIODONTAL CYST
125 CALCIFYING ODONTOGENIC CYST (CALCIFYING CYSTIC ODONTOGENIC TUMOR/GORLIN CYST) odontogenic epithelium containing ghost cells which may undergo calcification cystic and/or solid incisor and canine area 2 nd to 4 th decade (30 years) can be extraosseous (peripheral) simple enucleation, few recurrences

126



127



128 GLANDULAR ODONTOGENIC CYST rare, aggressive behavior middle-aged adults, anterior mandible enucleation and curettage, en bloc resection for multilocular lesions recurrence (30%)
129 ODONTOGENIC TUMORS

130

131



132 AMELOBLASTOMA conventional solid or multicystic (intraosseous) unicystic peripheral (extraosseous)





133 SOLID AMELOBLASTOMA CYSTIC AMELOBLASTOMA




134 PERIPHERAL AMELOBLASTOMA
135 ODONTOGENIC TUMORS





136 ODONTOMA mixed tumors composed of both epithelial and mesenchymal tissues compound vs complex


137 MIXED TUMORS ameloblastic fibroma ameloblastic fibro-odontoma
138 ODONTOGENIC TUMORS



139 ODONTOGENIC MYXOMA multilocular with honeycomb pattern recurrence



140 CEMENTOBLASTOMA true cementoma rare neoplasm of cementoblasts fused to root of tooth 2 nd and 3 rd decades mandible > maxilla
141 BONE Tori and exostoses Osteonecrosis and osteomyelitis Fibro-osseous lesions Bone cysts Bone cancer



142 TORI/EXOSTOSES bony outgrowths, bilateral and symmetric developmental, racial predisposition trauma, BRONJ

143 IDIOPATHIC OSTEOSCLEROSIS intraosseous radiopacity not related to teeth dense bone island/scar

144 CONDENSING OSTEITIS children and young adults similar to IO, but at or very close to apices of teeth molar and premolar areas of mandible pulpitis from large carious lesions or deep coronal restorations chronic occlusal trauma or low grade inflammation
145 OSTEONECROSIS/ OSTEOMYELITIS ON, medication-induced is recently recognized and fairly common may result in OM exposed bone OM, usually result of dental infection pain both associated with sequestrum formation and/or sinus tract
146 OSTEOMYELITIS infection of medullary bone with suppuration and sequestra formation bacterial male predominance mandible > maxilla chronic systemic diseases, immunocompromised status are predisposing surgical debridement, antibiotics




147




148





149 FIBRO-OSSEOUS LESIONS proliferation of fibroblast-like cells and deposition of osseous or cementum-like material cemento-osseous dysplasia ossifying fibroma
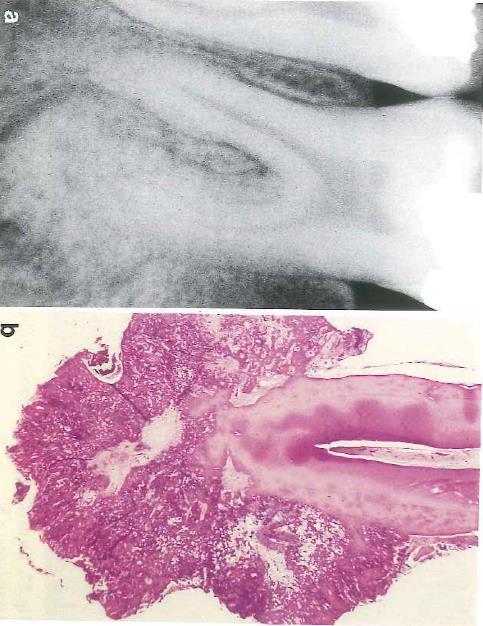
150 BONE CYSTS nasopalatine duct cyst - anterior midline palate, area of incisive canal simple (idiopathic, traumatic) 1st 2 decades, males mandibular molar-premolar area serosanguineous fluid or empty cavity Stafne bone cavity 5 th to 7 th decade, males entrapped salivary gland tissue, pressure resorption







151





152
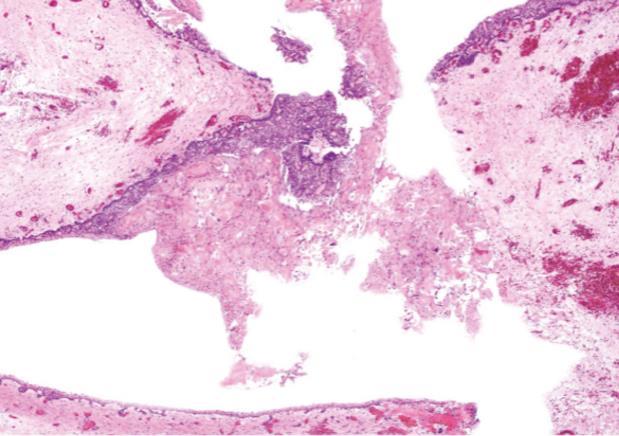
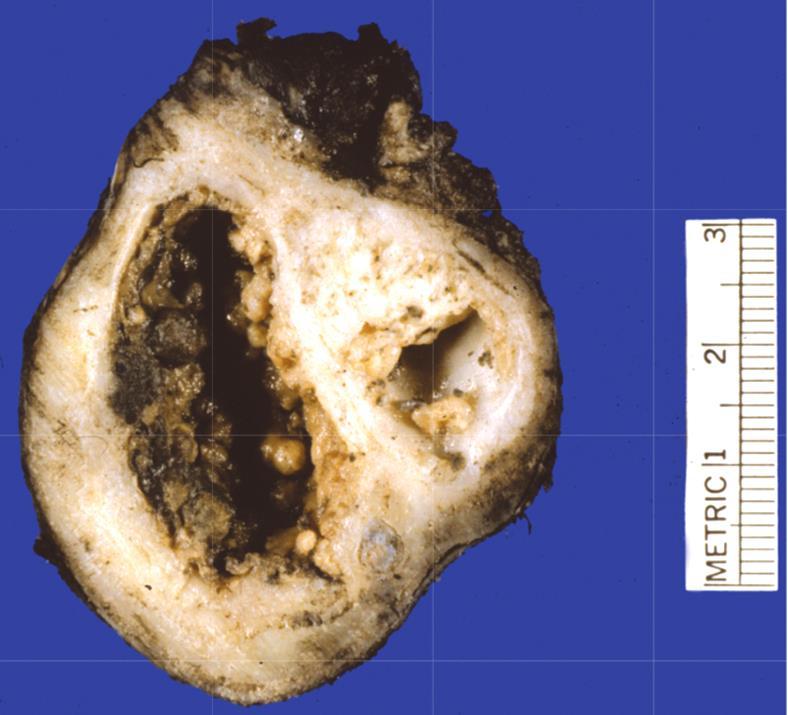
153 BRONJ 2003: a pattern of jaw osteonecrosis began to be recognized difficult to treat and associated with certain medications - bisphosphonates (BRONJ) 2011 (ADA): antiresorptive-related, due to association with a monoclonal antibody (denosumab) designed to prevent osteoclastic maturation (ARONJ)

154 BRONJ

155 MRONJ 2014 (AAOMS): medication-related due to discovery that antiangiogenic therapies may also be implicated risk is increased if agents are combined with bisphosphonates

156 MRONJ
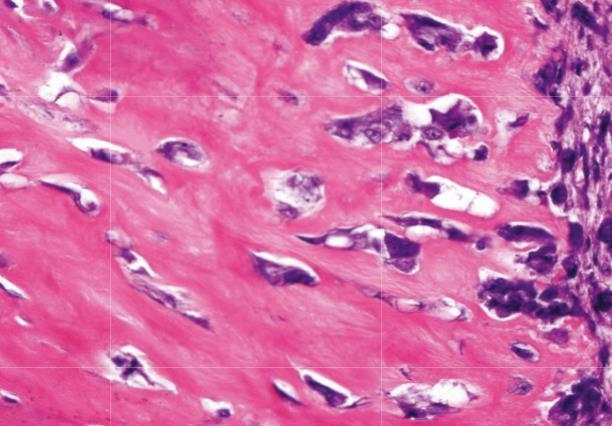
157 MRONJ (Pathogenesis) once in the serum, 50% of bisphosphonates are cleared by the kidneys with the remainder going to bone osteoclasts and osteoblasts have affinity for medication, incorporated into bone matrix - inhibit osteoclastic function resulting in disruption of the basic cellular unit (BMU)

158 MRONJ
159 RISK FACTORS advanced patient age (> 65 years) steroid use or chemotherapy diabetes smoking or alcohol poor oral hygiene duration of drug use > 3 years
160 CLINICAL FEATURES mandible > maxilla necrosis following dental extraction spontaneous, denture pressure, or minor trauma of a torus most are painful serum C-telopeptide (CTX) - not reliable in predicting risk of MRONJ
161 TREATMENT best therapeutic approach is prevention manipulation of bone should be avoided osteonecrosis can be minimized with antibiotic prophylaxis drug holiday (3 months) is controversial annual IV zoledronic acid - surgery in 2 months benefits of antiresorptive therapy greatly outweigh the risk of developing MRONJ

162 PECOS


163

164

165 Christopher Klem, MD, FACS Otolaryngology Head and Neck Cancer and Reconstructive Surgeon MD Anderson Cancer Network Certified Physician Christopher Klem, MD, is a Head and Neck Surgeon at the Queen s Head and Neck Institute. He recently served as the Chief of Otolaryngology Head and Neck Surgery at Tripler Army Medical Center and retired as a Colonel from the Army after serving 26 years on active duty. Dr. Klem graduated from the Uniformed Services University of the Health Sciences in 1998 and performed his residency training in Otolaryngology Head and Neck Surgery at Walter Reed Army Medical Center. He served as Clinical Instructor in Otolaryngology at both Walter Reed and the University of Maryland for a year after residency. After completing a two-year fellowship in Head and Neck Oncologic and Microvascular Reconstructive Surgery at MD Anderson Cancer Center in Houston, Texas, Dr. Klem moved to Hawaii and served as an Army physician at Tripler Army Medical Center for 8 years. In 2010, he deployed to Helmand Province in Afghanistan as a Head and Neck Surgeon where he performed more microvascular reconstructive surgeries in a combat zone than anyone ever has. Although he practices the entire spectrum of benign and malignant Head and Neck tumors, Dr. Klem s special interests include oral cavity cancer, salivary gland tumors, thyroid and parathyroid, and complex microvascular reconstruction. He is recognized as one of the leaders in Head and Neck Clinical Ultrasound and instructs frequently for the American College of Surgeons. Dr. Klem holds appointments as Assistant Professor of Surgery at the University of Hawaii John A. Burns School of Medicine and the Uniformed Services University of the Health Sciences. Education & Training Medical School: Uniformed Services University of the Health Sciences Residency: Walter Reed Army Medical Center Professional Credentials Certifications: Otolaryngology Head and Neck Surgery Fellowships: MD Anderson Cancer Center, Head and Neck Oncologic and Microvascular Reconstructive Surgery


166 Daniel Alam, MD, FACS Otolaryngology Head and Neck Cancer and Reconstructive Surgeon MD Anderson Cancer Network Certified Physician Daniel Alam, MD, is a specialist in head and neck reconstructive surgery, including complex microvascular reconstructions to repair major facial injuries and cancer defects. He was the primary microvascular surgeon of the first face transplant procedure in the U.S. at the Cleveland Clinic. Dr. Alam has developed six new surgical procedures over the last five years, from minimally invasive surgeries for facial paralysis to complex facial reconstruction methods. The success rate of microvascular reconstruction in his section at the Cleveland Clinic was unparalleled nationally. Dr. Alam also serves as a Clinical Professor of Surgery at the University of Hawaii John A. Burns School of Medicine. After graduating from the Johns Hopkins University School of Medicine as valedictorian, Dr. Alam received his surgical training with an internship at Massachusetts General Hospital, followed by residency at the Harvard Medical School s Combined Hospitals Program in Otolaryngology/Head and Neck Surgery. He then completed a fellowship in facial plastic and reconstructive surgery at the UCLA Medical Center and served on its faculty as a clinical instructor in facial plastic surgery. Before joining Queen s, Dr. Alam served as the Section Head of Facial Aesthetic and Reconstructive Surgery in the Head and Neck Institute at the Cleveland Clinic and as Professor of Surgery at the Lerner College of Medicine at Case Western Reserve University. He holds senior-level academic positions in the American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS). He is the director of an AAFPRS-sanctioned Fellowship in Facial Plastic Surgery, and serves on the organization s board of directors. Dr. Alam is a member of the AAFPRS National Academic Curriculum Committee, leading the section on facial paralysis and rehabilitation. He also serves on the editorial boards of four major journals. Education & Training Medical School: Johns Hopkins University School of Medicine Residency: Harvard Medical School, Combined Hospitals Program in Otolaryngology/Head and Neck Surgery Professional Credentials Certifications: Otolaryngology/Head and neck reconstructive surgery Fellowships: UCLA Medical Center, facial plastic and reconstructive surgery

167 KIRK Y. HIRATA, MD ANATOMIC/ORAL PATHOLOGY & HEMATOPATHOLOGY 1301 PUNCHBOWL STREET, IOLANI 4 HONOLULU, HAWAII PHONE: (808) /FAX: (808) khirata@queens.org
Vascular. Extravasated blood. Melanocytic. Tattoo. Epidermolysis bullosa. Lichen planus. Pemphigoid Pemphigus Lupus. Candidosis. Surface Epithelial
 Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Problem diagnoses. Current issues in Anatomic pathology. Problem Diagnoses in Tumors of the Oral Cavity 5/29/2009
 Current issues in Anatomic pathology Problem Diagnoses in Tumors of the Oral Cavity Richard Jordan DDS PhD FRCPath Professor of Oral Pathology & Pathology Director, UCSF Oral Pathology Diagnostic Laboratory
Current issues in Anatomic pathology Problem Diagnoses in Tumors of the Oral Cavity Richard Jordan DDS PhD FRCPath Professor of Oral Pathology & Pathology Director, UCSF Oral Pathology Diagnostic Laboratory
Differential Diagnosis of Oral Masses. Gingival Lesions
 Differential Diagnosis of Oral Masses Gingival Lesions Gingival/Alveolar Ridge Masses Parulis Periodontal Abscess Tori and Exostoses Reactive Proliferations Peripheral Odontogenic Cysts Peripheral Odontogenic
Differential Diagnosis of Oral Masses Gingival Lesions Gingival/Alveolar Ridge Masses Parulis Periodontal Abscess Tori and Exostoses Reactive Proliferations Peripheral Odontogenic Cysts Peripheral Odontogenic
Origin of Odontogenic Cysts & Tumors
 Origin of Odontogenic Cysts & Tumors Odontogenic Apparatus Origin of Odontogenic Cysts & Tumors Odontogenic Apparatus Remnants of dental lamina Reduced enamel epithelium Odontogenic rests Basal cell layer
Origin of Odontogenic Cysts & Tumors Odontogenic Apparatus Origin of Odontogenic Cysts & Tumors Odontogenic Apparatus Remnants of dental lamina Reduced enamel epithelium Odontogenic rests Basal cell layer
TANYA A. WRIGHT, DDS OBJECTIVES
 TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
RADIOGRAPHIC INTERPRETATION Differential Diagnosis
 RADIOGRAPHIC INTERPRETATION Differential Diagnosis MODULE 1: The Introduction. Chief complaint Demographics Age Sex Race Historical findings Physical findings Clinical Radiographic Location Maxilla/mandible
RADIOGRAPHIC INTERPRETATION Differential Diagnosis MODULE 1: The Introduction. Chief complaint Demographics Age Sex Race Historical findings Physical findings Clinical Radiographic Location Maxilla/mandible
Index. oralmaxsurgery.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adenomatoid odontogenic tumor, pediatric, 50 51 Ameloblastic carcinoma, pediatric, 17, 49 Ameloblastic fibro-odontoma, pediatric, 54 Ameloblastic
Index Note: Page numbers of article titles are in boldface type. A Adenomatoid odontogenic tumor, pediatric, 50 51 Ameloblastic carcinoma, pediatric, 17, 49 Ameloblastic fibro-odontoma, pediatric, 54 Ameloblastic
Differential Diagnosis of Oral Lesions. An Interactive Lecture Using Audience Response Polling. John L. Alonge, MS, DDS
 Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
That. Name QUIZ. 60 SEPTEMBER 2017 // dentaltown.com
 QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
MANSOURA UNIVERSITY FACULTY OF DENTISTRY ORAL PATHOLOGY DEPT
 MANSOURA UNIVERSITY FACULTY OF DENTISTRY ORAL PATHOLOGY DEPT THIRD YEAR Course Director: Dr. Nadia M. Lotfy Professor of Oral Pathology Dr. Manal Mohamed Zyada Associate Professor of Oral Pathology Oral
MANSOURA UNIVERSITY FACULTY OF DENTISTRY ORAL PATHOLOGY DEPT THIRD YEAR Course Director: Dr. Nadia M. Lotfy Professor of Oral Pathology Dr. Manal Mohamed Zyada Associate Professor of Oral Pathology Oral
IN THE NAME OF GOD. Dr.kheirandish DDS,MSC Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology ODONTOGENIC CYSTS AND TUMORS Chapter 15 I. DENTIGEROUS CYST II. III. IV. ERUPTION CYST ODONTOGENIC KERATOCYST Orthokeratinized
IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology ODONTOGENIC CYSTS AND TUMORS Chapter 15 I. DENTIGEROUS CYST II. III. IV. ERUPTION CYST ODONTOGENIC KERATOCYST Orthokeratinized
Premalignant lesions may expose to a promoting. factor & may be induced to undergo malignant. Carcinoma in situ displays the cytologic features of
 بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
Disclosure. Educational Objectives. Terminology. Odontogenic Cysts. Terminology
 Disclosure Lisa J. Koenig BChD, DDS, MS Professor & Program Director, Oral Medicine and Oral Radiology Marquette University School of Dentistry Consultant to Soredex for the Scanora 3D and 3Dx Author/Editor
Disclosure Lisa J. Koenig BChD, DDS, MS Professor & Program Director, Oral Medicine and Oral Radiology Marquette University School of Dentistry Consultant to Soredex for the Scanora 3D and 3Dx Author/Editor
4Ps LUMPS AND BUMPS B.L.&T. BUMPS, LUMPS, AND TATTOOS. Most Common BUMP in the oral cavity Fibroma INTERDENTAL PAPILLAE LESIONS
 B.L.&T. BUMPS, LUMPS, AND TATTOOS LUMPS AND BUMPS DIFFERENTIAL DIAGNOSIS FOR LUMPS AND BUMPS Traumatic Fibroma Papilloma Epulis Fissuratum Inflammatory Papillary Hyperplasia Lesions of Attached Gingiva
B.L.&T. BUMPS, LUMPS, AND TATTOOS LUMPS AND BUMPS DIFFERENTIAL DIAGNOSIS FOR LUMPS AND BUMPS Traumatic Fibroma Papilloma Epulis Fissuratum Inflammatory Papillary Hyperplasia Lesions of Attached Gingiva
Common/Important Radiolucencies. B. Most Common Location Apex of permanent first molar, rare in primary teeth.
 Cincinnati Dental Association Breakfast at Tiffany s: The Jewels and Gems of Oral Pathology November 17, 2010 John A. Svirsky, DDS, MEd Virginia Commonwealth University 804-828-0547 FAX: 804-828-6234 EMAIL:
Cincinnati Dental Association Breakfast at Tiffany s: The Jewels and Gems of Oral Pathology November 17, 2010 John A. Svirsky, DDS, MEd Virginia Commonwealth University 804-828-0547 FAX: 804-828-6234 EMAIL:
Inter-radicular Radiolucencies
 Inter-radicular Radiolucencies Differential Diagnosis Laterally Displaced Radicular Cyst Accessory canals Root fracture Lateral Periodontal Cyst Botryoid variant Odontogenic Keratocyst Incisive Canal Cyst
Inter-radicular Radiolucencies Differential Diagnosis Laterally Displaced Radicular Cyst Accessory canals Root fracture Lateral Periodontal Cyst Botryoid variant Odontogenic Keratocyst Incisive Canal Cyst
Contents. 3 Diagnostic Tests and Studies Introduction Examination... 27
 Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES)
") NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
Pigmented lesions of the Oral cavity
 Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Epithelial Sources. Rests of Serres Rests of Malassez Reduced Enamel Epithelium Surface Mucosa
 ODONTOGENIC CYSTS Epithelial Sources Rests of Serres Rests of Malassez Reduced Enamel Epithelium Surface Mucosa Epithelial Sources Surface Epithelium Rests of Serres Reduced Enamel Epithelium Rests of
ODONTOGENIC CYSTS Epithelial Sources Rests of Serres Rests of Malassez Reduced Enamel Epithelium Surface Mucosa Epithelial Sources Surface Epithelium Rests of Serres Reduced Enamel Epithelium Rests of
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
DISEASES OF THE JAWS I
 DISEASES OF THE JAWS I ODONTOGENIC AND PERIODONTAL INFECTIONS ODONTOGENIC INFECTIONS PERIAPICAL GRANULOMA PERIAPICAL ABSCESS APICAL PERIODONTAL CYST PHOENIX ABSCESS FISTULA, DRAINING SINUS SPACE INFECTIONS
DISEASES OF THE JAWS I ODONTOGENIC AND PERIODONTAL INFECTIONS ODONTOGENIC INFECTIONS PERIAPICAL GRANULOMA PERIAPICAL ABSCESS APICAL PERIODONTAL CYST PHOENIX ABSCESS FISTULA, DRAINING SINUS SPACE INFECTIONS
Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II ( )
") King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
Contents. 1 Normal Anatomy Introduction... 17
 Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Differential Diagnosis of Radiolucent Lesions of the Jaws
 Differential Diagnosis of Radiolucent Lesions of the Jaws Multilocular Multilocular Radiolucencies Odontogenic Keratocyst Botryoid Odontogenic Cyst Glandular odontogenic Cyst Invasive Ameloblastoma Central
Differential Diagnosis of Radiolucent Lesions of the Jaws Multilocular Multilocular Radiolucencies Odontogenic Keratocyst Botryoid Odontogenic Cyst Glandular odontogenic Cyst Invasive Ameloblastoma Central
Diagnostic Detectives: Catching common culprits and spotting a mimic in Oral Medicine, Oral Radiology and Oral Pathology. Outline
 Diagnostic Detectives: Catching common culprits and spotting a mimic in Oral Medicine, Oral Radiology and Oral Pathology Who is your detective alter ego? Dr. Kristina Perschbacher Oral Pathology and Oral
Diagnostic Detectives: Catching common culprits and spotting a mimic in Oral Medicine, Oral Radiology and Oral Pathology Who is your detective alter ego? Dr. Kristina Perschbacher Oral Pathology and Oral
Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II ( )
") King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
The clinical appearance and diagnosis of odontogenic cysts. SE Arc-Állcsont-Szájsebészeti és Fogászati Klinika BUDAPEST
 The clinical appearance and diagnosis of odontogenic cysts SE Arc-Állcsont-Szájsebészeti és Fogászati Klinika BUDAPEST DEFINITION A cyst is a sac with walls of connective tissue, lined by epithelium, containing
The clinical appearance and diagnosis of odontogenic cysts SE Arc-Állcsont-Szájsebészeti és Fogászati Klinika BUDAPEST DEFINITION A cyst is a sac with walls of connective tissue, lined by epithelium, containing
A survey of biopsied oral lesions in pediatric dental patients
 PEDIATRIC DENTISTRY/Copyright 1986 by The American Academy of Pediatric Dentistry Volume 8 Number 2 A survey of biopsied oral lesions in pediatric dental patients Robert L. Skinner, MS W.D. Davenport,
PEDIATRIC DENTISTRY/Copyright 1986 by The American Academy of Pediatric Dentistry Volume 8 Number 2 A survey of biopsied oral lesions in pediatric dental patients Robert L. Skinner, MS W.D. Davenport,
CHAPTER 8 SECTION 1.4 ORAL SURGERY TRICARE/CHAMPUS POLICY MANUAL M DEC 1998 SPECIAL BENEFIT INFORMATION
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
LEUKOPLAKIA Definition Epidemiology Clinical presentation
 LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Pre-reading - radiolucencies
 Pre-reading - radiolucencies Multiple radiolucencies o Suggests a systemic cause o Most likely: cherubism or KCOT s of nevoid basal cell carcinoma syndrome o Sometimes: florid osseous dysplasia (if limited
Pre-reading - radiolucencies Multiple radiolucencies o Suggests a systemic cause o Most likely: cherubism or KCOT s of nevoid basal cell carcinoma syndrome o Sometimes: florid osseous dysplasia (if limited
The Oral Cavity. Image source:
 The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School
 Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Tumors in Dogs Gingival Enlargement
 Oral Tumors in Dogs Is that lump you re seeing in your dog s mouth normal? Or is it something to be concerned about? The easiest way to know for sure is to have it evaluated by a veterinarian. When you
Oral Tumors in Dogs Is that lump you re seeing in your dog s mouth normal? Or is it something to be concerned about? The easiest way to know for sure is to have it evaluated by a veterinarian. When you
Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II ( )
") King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
King Saud University College of Dentistry Dept. of Oral Medicine & Diagnostic Sciences Division of Oral & Maxillofacial Radiology Course Description 343 DDS- Clinical Oral and Maxillofacial Radiology II
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
A Case Report of Odontogenic Keratocyst in Anterior Mandibule Position
 A Case Report of Odontogenic Keratocyst in Anterior Mandibule Position Malihe Moeini 1, Seyed Ehsan Anvar 2, Rasool Barzegari Bafghi 3* 1.Resident of Oral and Maxillofacial Radiology, Faculty of Dentistry,
A Case Report of Odontogenic Keratocyst in Anterior Mandibule Position Malihe Moeini 1, Seyed Ehsan Anvar 2, Rasool Barzegari Bafghi 3* 1.Resident of Oral and Maxillofacial Radiology, Faculty of Dentistry,
Large Dentigerous Cyst
 Volume 16.2.1 Feb 2016 This Lecture Series qualifies for 0.5 Informal CPD Learning Hours Large Dentigerous Cyst By Dr Hassem Geha A 55 year-old male presented with a painless swelling in the right mandible.
Volume 16.2.1 Feb 2016 This Lecture Series qualifies for 0.5 Informal CPD Learning Hours Large Dentigerous Cyst By Dr Hassem Geha A 55 year-old male presented with a painless swelling in the right mandible.
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Jaws: Cysts and Odontogenic Neoplasms
 Topic 10: Jaw Cysts General Features of Jaw Cysts Sources of Epithelium in Cysts Radiographic Features of Jaw Cysts Microscopic Features of Jaw Cysts Treatment and Prognosis of Jaw Cysts Classification
Topic 10: Jaw Cysts General Features of Jaw Cysts Sources of Epithelium in Cysts Radiographic Features of Jaw Cysts Microscopic Features of Jaw Cysts Treatment and Prognosis of Jaw Cysts Classification
Head and Neck Cancer How to recognize it in your office
 Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
高雄醫學大學 口腔醫學院 口腔病理影像科 牙科 X 光影像判讀 教學範例
 高雄醫學大學 口腔醫學院 口腔病理影像科 牙科 X 光影像判讀 教學範例 Content Image No. 001 Dentigerous cyst over left upper embedded canine--------------------- 頁 1 Image No. 002---------------------------------------------------------------
高雄醫學大學 口腔醫學院 口腔病理影像科 牙科 X 光影像判讀 教學範例 Content Image No. 001 Dentigerous cyst over left upper embedded canine--------------------- 頁 1 Image No. 002---------------------------------------------------------------
Oral Cancer. Online Course:
 Continuing Education Brought to you by Oral Cancer Course Author(s): Richard C. Jordan, DDS, PhD, FRCD(C) FRCPath CE Credits: 1 hour Intended Audience: Dentists, Dental Hygienists, Dental Assistants, Dental
Continuing Education Brought to you by Oral Cancer Course Author(s): Richard C. Jordan, DDS, PhD, FRCD(C) FRCPath CE Credits: 1 hour Intended Audience: Dentists, Dental Hygienists, Dental Assistants, Dental
Periodontal Disease. Radiology of Periodontal Disease. Periodontal Disease. The Role of Radiology in Assessment of Periodontal Disease
 Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Case Report A Giant Cell Fibroma and Focal Fibrous Hyperplasia in a Young Child: A Case Report
 Hindawi Publishing Corporation Case Reports in Dentistry Volume 2012, Article ID 370242, 5 pages doi:10.1155/2012/370242 Case Report A Giant Cell Fibroma and Focal Fibrous Hyperplasia in a Young Child:
Hindawi Publishing Corporation Case Reports in Dentistry Volume 2012, Article ID 370242, 5 pages doi:10.1155/2012/370242 Case Report A Giant Cell Fibroma and Focal Fibrous Hyperplasia in a Young Child:
IMAGING OF CYSTS OF THE JAWS July 2002 N. Serman
 IMAGING OF CYSTS OF THE JAWS July 2002 N. Serman This is an area where radiology plays an important role in assisting with the diagnosis, determining the size of the lesion and the relationship to adjacent
IMAGING OF CYSTS OF THE JAWS July 2002 N. Serman This is an area where radiology plays an important role in assisting with the diagnosis, determining the size of the lesion and the relationship to adjacent
MALIGNANT TUMOURS OF THE JAWS
 MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
MALIGNANT TUMOURS OF THE JAWS MALIGNANT TUMOURS OF THE JAWS Squamous cell carcinoma Osteogenic sarcoma Chondrosarcoma Fibrosarcoma Malignant lymphomas (incl. Burkitt s) Multiple myeloma Ameloblastoma Secondary
Diagnosis. overt Examination. Definitive Examination. History. atient interview. Personal History. Clinical Examination.
 Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
Fundamental & Preventive Curvatures of Teeth and Tooth Development. Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L.
 Dr. Margaret L.") Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Radiographic features of cysts and benign tumors of the jaws. Cyst. Effects on adjacent structures. Types. Odontogenic Cysts. Non-Odontogenic cysts
 Radiographic features of cysts and benign tumors of the jaws Cyst A Cyst is a benign pathologic cavity filled with fluid, lined by epithelium, and surrounded by a connective tissue wall Steven R. Singer,
Radiographic features of cysts and benign tumors of the jaws Cyst A Cyst is a benign pathologic cavity filled with fluid, lined by epithelium, and surrounded by a connective tissue wall Steven R. Singer,
Lesions & Lifestyles
 Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Development of teeth. 5.DM - Pedo
 Development of teeth 5.DM - Pedo Tooth development process of continuous changes in predetermined order starts from dental lamina A band of ectodermal cells growing from the epithelium of the embryonic
Development of teeth 5.DM - Pedo Tooth development process of continuous changes in predetermined order starts from dental lamina A band of ectodermal cells growing from the epithelium of the embryonic
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
High yield oral pathology
 High yield oral pathology Molly S. Rosebush DDS, MS Benign radiopaque lesions Touro Infirmary Dental Seminar March 9, 2018 Odontoma Most common odontogenic tumor More likely a developmental anomaly (hamartoma)
High yield oral pathology Molly S. Rosebush DDS, MS Benign radiopaque lesions Touro Infirmary Dental Seminar March 9, 2018 Odontoma Most common odontogenic tumor More likely a developmental anomaly (hamartoma)
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Role of the Dental Hygienist in Oral Pathology. Role of the Dental Hygienist in Oral Pathology. Cancers of the Oral Cavity.
 Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Odontomes and Odontogenic tumours
 Odontomes and Odontogenic tumours Odontomes Developmental hamartoma Hamartoma: normal tissue in abnormal location Any cells to be neoplastic it must be able to replicate, which is not seen in hamartoma
Odontomes and Odontogenic tumours Odontomes Developmental hamartoma Hamartoma: normal tissue in abnormal location Any cells to be neoplastic it must be able to replicate, which is not seen in hamartoma
Pathology of the Alimentary System. Lecture 3 Teeth, tonsils, salivary glands & tongue
 Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 3 Teeth, tonsils, salivary glands & tongue Enrique Aburto Fall 2014 II. Diseases of teeth & dental tissues Structure & function
Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 3 Teeth, tonsils, salivary glands & tongue Enrique Aburto Fall 2014 II. Diseases of teeth & dental tissues Structure & function
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients. Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology
 Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Case Report A Review and Report of Peripheral Giant Cell Granuloma in a 4-Year-Old Child
 Volume 2016, Article ID 7536304, 4 pages http://dx.doi.org/10.1155/2016/7536304 Case Report A Review and Report of Peripheral Giant Cell Granuloma in a 4-Year-Old Child Afsaneh Nekouei, Alireza Eshghi,
Volume 2016, Article ID 7536304, 4 pages http://dx.doi.org/10.1155/2016/7536304 Case Report A Review and Report of Peripheral Giant Cell Granuloma in a 4-Year-Old Child Afsaneh Nekouei, Alireza Eshghi,
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Dental Morphology and Vocabulary
 Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
The resident will be assigned to be on call with the Oral and Maxillofacial service. Call will be set according to PARO guidelines.
 Goals and Objectives for the Otolaryngology-Head & Neck Resident on the Oral and Maxillofacial Surgery (OMFS) Rotation St. Catharines General Hospital (1 four-week rotational block) During the second year
Goals and Objectives for the Otolaryngology-Head & Neck Resident on the Oral and Maxillofacial Surgery (OMFS) Rotation St. Catharines General Hospital (1 four-week rotational block) During the second year
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Case Report Basal Cell Ameloblastoma of Mandible: A Rare Case Report with Review
 Case Reports in Dentistry Volume 2013, Article ID 187820, 4 pages http://dx.doi.org/10.1155/2013/187820 Case Report Basal Cell Ameloblastoma of Mandible: A Rare Case Report with Review Hemant Shakya, 1
Case Reports in Dentistry Volume 2013, Article ID 187820, 4 pages http://dx.doi.org/10.1155/2013/187820 Case Report Basal Cell Ameloblastoma of Mandible: A Rare Case Report with Review Hemant Shakya, 1
For the Patient: Bisphosphonates and Oral Health in Multiple Myeloma
 For the Patient: Bisphosphonates and Oral Health in Multiple Myeloma Regular dental care is very important for all cancer patients. As soon as possible after your cancer diagnosis, your dentist should
For the Patient: Bisphosphonates and Oral Health in Multiple Myeloma Regular dental care is very important for all cancer patients. As soon as possible after your cancer diagnosis, your dentist should
PREVENTION OF ORAL CANCER
 PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
CYSTS OF THE JAW AND SOFT TISSUES
 CYSTS OF THE JAW AND SOFT TISSUES Definition: it is a pathological cavity lined by epithelium containing fluid or semifluid (true cyst). If the cyst not lined by epithelium it is pseudo- cyst. Classification
CYSTS OF THE JAW AND SOFT TISSUES Definition: it is a pathological cavity lined by epithelium containing fluid or semifluid (true cyst). If the cyst not lined by epithelium it is pseudo- cyst. Classification
Dysplasia, Mimics and Other Controversies
 Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
Dysplasia, Mimics and Other Controversies Mary S. Richardson, MD Dept. of Pathology Medical University of South Carolina Charleston, SC Notice of Faculty Disclosure In accordance with ACGME guidelines,
SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY
 MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
Educational Cases EQA November T.J. Palmer Raigmore Hospital Inverness
 Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Educational Cases EQA November 2013 T.J. Palmer Raigmore Hospital Inverness Case 2 Clinical Details Dob 11 February 1951 PMH: 1964 Extraction of 45 aet 13 yr 1966 Cyst between 44 and 46 enucleated 1973
Glandular Odontogenic Cyst Coexisting with a Dentigerous Cyst: Case Report
 SmyrnaMed Case 2018;2(1): 1-5 ISSN (Online): 2564-6869 www.smyrnamed.com Glandular Odontogenic Cyst Coexisting with a Dentigerous Cyst: Case Report Assist.Prof.Dr. Serap Keskin Tunç 1, Dt. Erkan Feslihan
SmyrnaMed Case 2018;2(1): 1-5 ISSN (Online): 2564-6869 www.smyrnamed.com Glandular Odontogenic Cyst Coexisting with a Dentigerous Cyst: Case Report Assist.Prof.Dr. Serap Keskin Tunç 1, Dt. Erkan Feslihan
Radiology. & supporting structures. Lec. 14 Common diseases of teeth Dr. Areej
 Radiology Lec. 14 Common diseases of teeth Dr. Areej & supporting structures A radiograph is only one part of the diagnostic process. Usually one does NOT make a diagnosis solely from a radiograph. A diagnosis
Radiology Lec. 14 Common diseases of teeth Dr. Areej & supporting structures A radiograph is only one part of the diagnostic process. Usually one does NOT make a diagnosis solely from a radiograph. A diagnosis
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: http://www.ivis.org October 14(Fri) ~ 17(Mon) 2011 ICC Jeju, Korea 2011 WSAVA
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: http://www.ivis.org October 14(Fri) ~ 17(Mon) 2011 ICC Jeju, Korea 2011 WSAVA
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
[ 06-10] Dr. B. Siva Reddy, Dr. B. Ajay Reginald, Dr. D. Sireesha, Dr. Meda Samatha India Abstract: Keywords ARTICLE 20/07/ /09/2018
![[ 06-10] Dr. B. Siva Reddy, Dr. B. Ajay Reginald, Dr. D. Sireesha, Dr. Meda Samatha India Abstract: Keywords ARTICLE 20/07/ /09/2018](/thumbs/87/95905171.jpg "[ 06-10] Dr. B. Siva Reddy, Dr. B. Ajay Reginald, Dr. D. Sireesha, Dr. Meda Samatha India Abstract: Keywords ARTICLE 20/07/ /09/2018") Dentigerous Cyst Associated with an Impacted Mesiodens: A Rare Case Report with Review of Literature [PP: 06-10] Dr. B. Siva Reddy, Dr. B. Ajay Reginald, Dr. D. Sireesha, Dr. Meda Samatha, Department of
Dentigerous Cyst Associated with an Impacted Mesiodens: A Rare Case Report with Review of Literature [PP: 06-10] Dr. B. Siva Reddy, Dr. B. Ajay Reginald, Dr. D. Sireesha, Dr. Meda Samatha, Department of
OROPHYRENGEAL CANCERS
 OROPHYRENGEAL CANCERS INTRODUCTION 2 % 4 % of all malignant Tumors in west Asia India 40% Men ^ Age :Over 60 yrs 90% of all oral cancers results from Tobacco and Alcohol Pan (Betel Leaf,Nut, Lime), Reverse
OROPHYRENGEAL CANCERS INTRODUCTION 2 % 4 % of all malignant Tumors in west Asia India 40% Men ^ Age :Over 60 yrs 90% of all oral cancers results from Tobacco and Alcohol Pan (Betel Leaf,Nut, Lime), Reverse
Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I)
") Introduction: Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I) Oral Epithelial Tumors may be: Benign tumors Sequamous cell Papilloma Malignant tumors Sequamous cell carcinoma, Basal cell carcinoma
Introduction: Oral Epithelial Tumors, Melanocytic Nevi, and Melanoma (I) Oral Epithelial Tumors may be: Benign tumors Sequamous cell Papilloma Malignant tumors Sequamous cell carcinoma, Basal cell carcinoma
2018 Dental Code Set For dates of service from 1/1/ /31/2018
 D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT D0140 LIMITED ORAL EVALUATION - PROBLEM FOCUSED D0150 COMPREHENSIVE ORAL EVALUATION - NEW OR ESTABLISHED PATIENT D0160 DETAILED AND EXTENSIVE ORAL EVALUATION
D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT D0140 LIMITED ORAL EVALUATION - PROBLEM FOCUSED D0150 COMPREHENSIVE ORAL EVALUATION - NEW OR ESTABLISHED PATIENT D0160 DETAILED AND EXTENSIVE ORAL EVALUATION
2018 Dental Code Set
 D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0251 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0393 D0470 D0502 PERIODIC ORAL EVALUATION ESTABLISHED PATIENT LIMITED ORAL
D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0251 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0393 D0470 D0502 PERIODIC ORAL EVALUATION ESTABLISHED PATIENT LIMITED ORAL
Oral pathology. General structure of teeth
 Oral pathology Contents: 1. General structure of teeth 2. Common structural inflammatory lesions 3. Tumor like lesions 4. Infections 5. Oral manifestations of systemic disease 6. Tumors of oral cavity
Oral pathology Contents: 1. General structure of teeth 2. Common structural inflammatory lesions 3. Tumor like lesions 4. Infections 5. Oral manifestations of systemic disease 6. Tumors of oral cavity
2014 Update Revisions for: AAOMS Strategies for patient management with or at risk for medication-related osteonecrosis of the jaw:
 AAOMS Strategies for patient management with or at risk for medication-related osteonecrosis of the jaw: 2007 2009 2014 2014 Update Revisions for: Diagnosis, Staging, Management strategies, (our main interest)
AAOMS Strategies for patient management with or at risk for medication-related osteonecrosis of the jaw: 2007 2009 2014 2014 Update Revisions for: Diagnosis, Staging, Management strategies, (our main interest)
Diagnostic sieve. Looking Beyond the Vermillion Border. Time bombs for medical GPs! Normal oral mucosa
 Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Treatment Modalities of Odontogenic Keratocyst of Maxilla and Mandible: Our Experience
 wjd Parveen Akhter Lone et al Original Research 10.5005/jp-journals-10015-1344 Treatment Modalities of Odontogenic Keratocyst of Maxilla and Mandible: Our Experience 1 Parveen Akhter Lone, 2 Mohan Singh,
wjd Parveen Akhter Lone et al Original Research 10.5005/jp-journals-10015-1344 Treatment Modalities of Odontogenic Keratocyst of Maxilla and Mandible: Our Experience 1 Parveen Akhter Lone, 2 Mohan Singh,
MDG Dental Plan Comparison
 D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem.
 Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Chapter 5. Developmental Disorders. Copyright 2014, 2009, 2004, 2000, 1996, 1992 by Saunders, an imprint of Elsevier Inc 1
 Chapter 5 Developmental Disorders Copyright 2014, 2009, 2004, 2000, 1996, 1992 by Saunders, an imprint of Elsevier Inc 1 Outline Ø Embryonic Development of the Face, Oral Cavity, and Teeth Ø Developmental
Chapter 5 Developmental Disorders Copyright 2014, 2009, 2004, 2000, 1996, 1992 by Saunders, an imprint of Elsevier Inc 1 Outline Ø Embryonic Development of the Face, Oral Cavity, and Teeth Ø Developmental
An unusual site of Adenomatoid Odontogenic Tumor: A rare case report
 J. Int Oral Health 2010 Case Report All right reserved An unusual site of Adenomatoid Odontogenic Tumor: A rare case report Sapna Panjwani*, Anjana Bagewadi**, Vaishali Keluskar*** *Post Graduate Student
J. Int Oral Health 2010 Case Report All right reserved An unusual site of Adenomatoid Odontogenic Tumor: A rare case report Sapna Panjwani*, Anjana Bagewadi**, Vaishali Keluskar*** *Post Graduate Student
SUTTER MEDICAL CENTER, SACRAMENTO
 Department of Surgery & Dental Section - Delineation of Privileges INITIAL: [ ] RENEWED: [ ] DATE: ADDITIONAL: [ ] Privileges are granted for Sutter General Hospital, Sutter Memorial Hospital, Sutter Center
Department of Surgery & Dental Section - Delineation of Privileges INITIAL: [ ] RENEWED: [ ] DATE: ADDITIONAL: [ ] Privileges are granted for Sutter General Hospital, Sutter Memorial Hospital, Sutter Center
Oral Cancer FAQs. What is oral cancer? How many people are diagnosed with oral cancer each year?
 Oral Cancer FAQs What is oral cancer? Oral cancer or oral cavity cancer, is cancer that starts in the mouth. Areas affected by this type of cancer are the lips, the inside lining of the lips and cheeks
Oral Cancer FAQs What is oral cancer? Oral cancer or oral cavity cancer, is cancer that starts in the mouth. Areas affected by this type of cancer are the lips, the inside lining of the lips and cheeks
There are three referral categories used in the dental referral system:
 Restorative Dentistry Referral Criteria Restorative Dentistry referral criteria are outlined to provide General Dental Practitioners (GDPs), Community Dental Service (CDS) Dentists, Primary Care Specialists,
Restorative Dentistry Referral Criteria Restorative Dentistry referral criteria are outlined to provide General Dental Practitioners (GDPs), Community Dental Service (CDS) Dentists, Primary Care Specialists,
Papule in the Right Floor of the Mouth
 Continuing Education Brought to you by Papule in the Right Floor of the Mouth Course Author(s): H. Stan McGuff, DDS; Anne Cale Jones, DDS; Michaell A. Huber, DDS; Online Case: www.dentalcare.com/en-us/professional-education/case-challenges/case-challenge-070
Continuing Education Brought to you by Papule in the Right Floor of the Mouth Course Author(s): H. Stan McGuff, DDS; Anne Cale Jones, DDS; Michaell A. Huber, DDS; Online Case: www.dentalcare.com/en-us/professional-education/case-challenges/case-challenge-070
Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S.
 Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S. Residency Site Director Weill Cornell Medical Center Associate Professor Division of Head
Evaluation and Management of Head and Neck Cancer in Patients with Fanconi anemia David I. Kutler, M.D., F.A.C.S. Residency Site Director Weill Cornell Medical Center Associate Professor Division of Head
Tumors or Masses in the Mouth (Oral Masses) Basics
 Basics") Tumors or Masses in the Mouth (Oral Masses) Basics OVERVIEW Oral refers to the mouth; oral masses are tumors or growths located in the mouth Oral masses may be benign or malignant (that is, cancer); 4
Tumors or Masses in the Mouth (Oral Masses) Basics OVERVIEW Oral refers to the mouth; oral masses are tumors or growths located in the mouth Oral masses may be benign or malignant (that is, cancer); 4
Oral Medicine FULL Referral Guide (FRG)
") Oral Medicine FULL Referral Guide (FRG) Yorkshire & the Humber February 2017 Version 1 Contents Introduction... 1 Oral Medicine Referral Decision Process 1 Step 1. Oral Medicine Condition?... 2 A. Soft
Oral Medicine FULL Referral Guide (FRG) Yorkshire & the Humber February 2017 Version 1 Contents Introduction... 1 Oral Medicine Referral Decision Process 1 Step 1. Oral Medicine Condition?... 2 A. Soft