IMPACT: Evidence-based depression treatment in primary care. Rita Haverkamp, MSN, CNS-BC Virna Little, PsyD, LCSW-R, SAP
|
|
|
- Alan McDonald
- 6 years ago
- Views:
Transcription


1 IMPACT: Evidence-based depression treatment in primary care Rita Haverkamp, MSN, CNS-BC Virna Little, PsyD, LCSW-R, SAP
2 IMPACT: A Practical Approach to Team Based Depression Care
3 What is Depression? Common: 20 million people / year suffer from a depressive illness Disabling: a leading cause of disability (WHO) Curable or treatable: appropriate treatment helps most people
, thoughts of guilt, irritability and thoughts of suicide")
4 Major Depression Common: 5-10 % in primary care Pervasive depressed mood / sadness Loss of interest/ pleasure. plus lack of energy, fatigue, poor sleep and appetite, physical slowing or agitation, poor concentration, physical symptoms (aches and pains), thoughts of guilt, irritability and thoughts of suicide If untreated, depression can last for years Often complicated by chronic medical disorders, chronic pain, anxiety, cognitive impairment, grief/ bereavement, substance abuse
5 Depression takes a large toll on quality of life Hypertension Cancer Diabetes Foot problems Stroke Emhysema Depression Heart disease Arthritis QALYs Quality Adjusted Life Years (QALYs) lost in 2,558 older adults over 4 years. Adjusted for age, gender, and comorbid medical conditions. Unützer et al, Intl Psychogeriatrics, 2000
6 Depression is expensive: Annual Health Costs in 1995 $ No depression $ Mild depression Moderate to severe depression 0 (n=859) 1-2 (n=616) 3-5 (n=659) 6-16 (n=423) Chronic disease score Unützer et al, JAMA, 1997

7 Depression is deadly Older adults have the highest rate of suicide.
8 Risk Factors for Suicide - Male gender - Depression - Alcohol or drug misuse -Pain - Social isolation - Physical illness
9 Few Depressed Adults get Effective Treatment -Only ~ half are treated. -Older adults, men, African Americans and Latinos have particularly low rates of depression treatment. -Many (if not most) prefer treatment by their primary care physician and PCPs prescribe majority of antidepressants.
10 Depression Treatment in Primary Care - Only about half of depressed adults are treated - Only % show substantial improvement over 12 months - Increasing use of antidepressants but treatment is often not effective - Early treatment dropout - Staying on ineffective meds too long - Little access to evidence-based psychosocial treatments
11 Barriers to Effective Depression Care Knowledge and attitudes I didn t know what hit me Stigma of mental illness: I am not crazy Fallacy of good reasons: Isn t depression just a part of being sick or normal aging
12 Barriers to Effective Depression Care Challenges in primary care - Limited time and competing priorities: medical illness, pain, life stressors - Limited follow-up -> early treatment dropout - Staying on ineffective treatments for too long - I thought this was as good as I was going to get - Poor access to mental health expertise
13 Brief history of QI for Depression in Primary Care 1970s 1980s: screening for depression: - Screening may be necessary but is not sufficient 1990s: improved referral to mental health care: - Only 50 % follow-up on referrals and few receive a full course of treatment 1993: AHCPR (now AHRQ) practice guidelines: - Provider training based on guidelines: guidelines and provider education may be necessary but are not sufficient Since 1990: - Over 30 studies in the US and abroad document that systematic collaborative care is more effective than usual care for depression (Gilbody et al, Arch Int Med; 2006). Recent research also supports cost-effectiveness of this approach.
14 Evidence for Collaborative Care for Depression Metaanalysis by Gilbody et al, Archives of Internal Medicine; trials of collaborative care for depression in primary care (US and Europe) - cc consistently more effective than usual care - successful programs include: - active care management (not case management) - support of medication management in primary care - psychiatric consultation Unutzer et al, Report to President s Commisson on Mental Health; Psychiatric Services 2006.
15 Evidence-based team care for depression TWO PROCESSES 1. Systematic diagnosis and outcomes tracking e.g., PHQ-9 to facilitate diagnosis and track depression outcomes 2. Stepped Care a) Change treatment according to evidence-based algorithm if patient is not improving b) Relapse prevention once patient is improved TWO NEW TEAM MEMBERS Care Manager - Patient education / self management support - Close follow-up to make sure pts don t fall through the cracks - Support anti-depressant Rx by PCP - Brief counseling (behavioral activation, PST-PC, CBT, IPT) - Facilitate treatment change / referral to mental health Consulting Psychiatrist - Caseload consultation for care manager and PCP (population-based) - Diagnostic consultation on difficult cases - Consultation focused on patients not improving as expected - Recommendations for additional treatment / referral according to evidence-based guidelines - Relapse prevention

16 The IMPACT Study Funded by John A. Hartford Foundation California Healthcare Foundation
, Elizabeth Lin (Co-PI), Paul Ciechanowski Duke University Linda Harpole")
17 IMPACT Team None of us is as smart as all of us Study coordinating center Jürgen Unützer (PI), Sabine Oishi, Diane Powers, Michael Schoenbaum, Tom Belin, Linqui Tang, Ian Cook. PST-PC experts: Patricia Arean, Mark Hegel Study sites University of Washington / Group Health Cooperative Wayne Katon (PI), Elizabeth Lin (Co-PI), Paul Ciechanowski Duke University Linda Harpole (PI), Eugene Oddone (Co-PI), David Steffens Kaiser Permanente, Southern CA (La Mesa, CA) Richard Della Penna (Co-PI), Lydia Grypma (Co-PI), Mark Zweifach, MD, Rita Haverkamp, RN, MSN, CNS Indiana University Christopher Callahan (PI), Kurt. Kroenke, Hugh. Hendrie (Co-PI) UT Health Sciences Center at San Antonio John Williams (PI), Polly Hitchcock-Noel (Co-PI), Jason Worchel Kaiser Permanente, Northern CA Enid Hunkeler (PI), Patricia Arean (Co-PI) Desert Medical Group Marc Hoffing (PI); Stuart Levine (Co-PI) Study advisory board Lisa Goodale (NDMDA), Rick Birkel (NAMI), Thomas Oxman, Kenneth Wells, Cathy Sherbourne, Lisa Rubenstein, Howard Goldman
18 IMPACT Study ,801 depressed older adults in primary care 18 primary care clinics 8 health care organizations in 5 states - Diverse health care systems (FFS, HMO, VA) primary care providers - Urban and semi-rural settings - Capitated and fee-for-service Funded by John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation, Hogg Foundation
19 IMPACT Study Methods Design: 1,801 depressed older adults with major depression and / or dysthymia (chronic depression) randomly assigned to IMPACT or to Care as Usual Usual Care: Primary care or referral to specialty mental health IMPACT Care: Collaborative / stepped care disease management program for depression in primary care offered for up to 12 months Analyses: Independent assessments of health outcomes and costs for 24 months. Intent to treat analyses Unützer et al, Med Care 2001; 39(8):785-99


20 IMPACT Team Care Model Effective Collaboration Prepared, Pro-active Practice Team Practice Support Informed, Activated Patient
21 Collaborative Care Patient Chooses treatment in consultation with provider(s): antidepressants and / or brief psychotherapy Primary care provider (PCP) Refers; prescribes antidepressant medications + Depression Care Manager + Consulting Psychiatrist Unützer et al, Med Care 2001; 39(8):785-99
22 Treatment Protocol (1) Education, (2) Behavioral Activation / Pleasant Events Scheduling AND (3) a) Antidepressant medication usually an SSRI or other newer antidepressant OR b) Problem Solving Treatment in Primary Care (PST-PC) 6-8 individual sessions followed by monthly group maintenance sessions (4) Maintenance and Relapse Prevention Plan for patients in remission
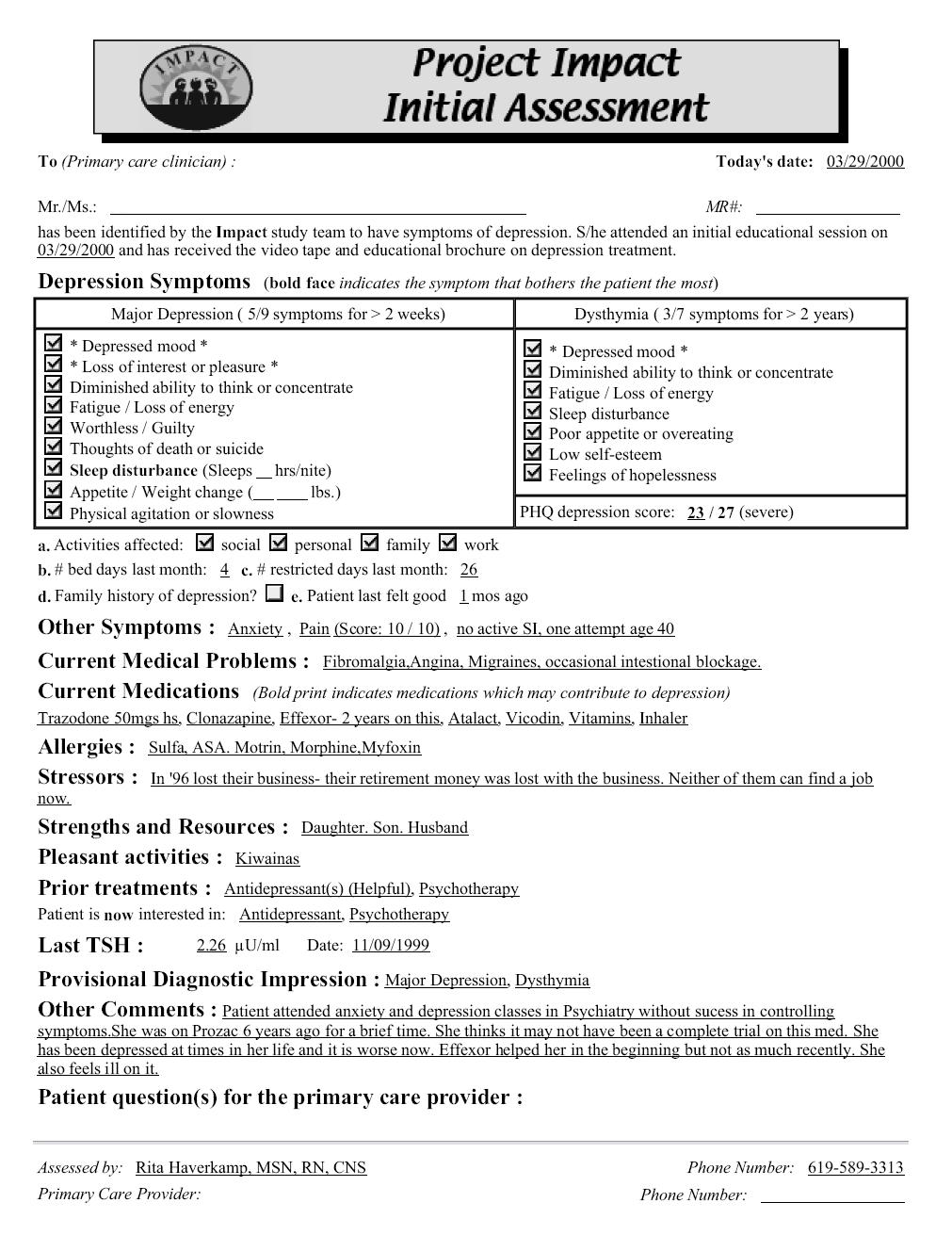
23 Stepped Care Systematic outcomes tracking Patient Health Questionnaire (PHQ-9) Treatment adjustment as needed - based on clinical outcomes - according to evidence-based algorithm - in consultation with team psychiatrist Relapse prevention
24
25 IMPACT Participant Characteristics N = 1,801* Female 65 % Mean age (SD) 71.2 (7.5) Non-white 23 % African American 12 % Latino 8 % All others 3 % Major depression + dysthymia 53 % Cognitive impairment at screening 35 % Mean chronic medical diseases (out of 10) 3.2 Antidepressant use in 3 months prior to study 42 % * No significant baseline differences between intervention and usual care.
26 Improved Satisfaction with Depression Care (% Excellent, Very Good) 100 Usual Care IMPACT percent P=.2375 P<.0001 P< month Unützer et al, JAMA 2002; 288:
27 IMPACT: Doubles the Effectiveness of Usual Care for Depression IMPACT INTERVENTION AFTER IMPACT Mean HSCL-20 Depression Severity Score P=0.55 P<0.01 P<0.01 P<0.01 P<0.01 P<0.01 P<0.01 P<0.01 P<0.01 Baseline * 24 * months IMPACT Usual Care Hunkeler et al, BMJ, 2006.
28 Better Physical Function SF-12 Physical Function Component Summary Score (PCS-12) P<0.01 P=0.35 P<0.01 P< Usual Care IMPACT Baseline 3 mos 6 mos 12 mos Callahan et al, JAGS 2005; 53:
29 Fewer thoughts of suicide % patients with suicidal thoughts Baseline 6 months 12 months IMPACT Usual Care Unutzer et al, JAGS 2006
30 IMPACT Findings Robust Across Diverse Organizations 50 % or greater improvement in depression at 12 months Usual Care IMPACT % Participating Organizations
31 IMPACT Care Benefits Ethnic Minority Populations 50 % or greater improvement in depression at 12 months 60% 54% 50% 40% 30% 20% 43% 19% 23% 42% 14% IMPACT Care Care as Usual 10% 0% White Black Latino Areán et al. Medical Care, 2005
32 IMPACT Summary - Less depression (IMPACT doubles effectiveness of usual care) - Less physical pain - Better functioning - Higher quality of life - Greater patient and provider satisfaction - More cost-effective Photo credit: J. Lott, Seattle Times I got my life back
33 A patient s experience Channel 10 video clip
34 IMPACT in the real world Example: Kaiser Permanente Pilot Study - Compare 284 clients in adapted program with 140 usual care patients and 140 intervention patients in the IMPACT study (Grypma et al, 2006) Dissemination - Implementing program at ~ 10 regional medical centers at KPSC and several clinics at KP Northwest
35 KPSC San Diego After IMPACT Fewer care manager contacts 18.9 IMPACT Study Post-Study Total contacts Clinic visits Phone calls Grypma et al, General Hospital Psychiatry, 2006.
36 IMPACT Remains Effective >= 50 % drop in PHQ-9 depression scores 66% 68% 64% 68% At 3 months IMPACT Post-Study At 6 months Grypma et al, General Hospital Psychiatry, 2006.
37 Lower total health care costs $8,800 $ / year $8,400 $8,000 $7,600 $8,588 $7,949 Study Usual Care Study IMPACT $7,200 $7,471 Post $6,800 Grypma, et al; General Hospital Psychiatry, 2006

38 Long (4 year) Cost effectiveness
39 Long (4 year) Cost effectiveness IMPACT 4-year cost analysis $2,000 $1,000 Total cost $0 -$1,000 -$2,000 -$3,000 Year 1-2 Year 3-4 -$4,000 -$5,000 Cost difference (IV - UC) Source: Unützer, et al. (under review).
40 IMPACT in the real world Example: Institute for Urban Family Health
41 Institute for Urban Family Health Number Percent Age at enrollment: Mean Range 71.6 years years Gender: Female Male Ethnicity: Hispanic African American Caucasian Other Marital Status: Married Single, Widowed, Divorced/separated % 31.0% 37.7% 29.3% 23.4% 9.6% 47.8% 52.2%
42 IMPACT Effective for Depression Mean PHQ-9 Depression Scores Mean Depression Scores Initial 3 Months 6 months Time
43 Change in Depression Initial to 6 months Number of Patients Initial PHQ-9 Depression Scores Under 10: Mild 63% 10-14: Moderate 28% 15-19: Mod. Severe PHQ-9 Score 9% 20+: Severe Number of Patients Month PHQ-9 Depression Scores (Mean Score of 7.91) 65% Under 10: Mild 24% 10-14: Moderate 15-19: Mod. Severe PHQ-9 Sore 5% 6% 20+: Severe


44 A word from providers It is good to see that mental health is once again becoming part of the medical Interview, as so much of our patient's health depends on their mental well being. - Dr. Eric Gayle Project IMPACT has allowed me to incorporate a new tool (PHQ-9)into my primary care practice, which has improved the accuracy of my diagnosis while increasing my efficiency and productivity as well. It helped me identify patients I initially overlooked. -Dr. Joseph Lurio (68 th Street)
45 Key Components of Depression Care Management
46 Bridging the divide between mental health & medical care Mental health is part of overall health Treat mental health disorders where the patient is / feels most comfortable receiving care -Established doctor-patient relationship an important foundation of trust -Less stigma -Better coordination with medical care
47 Collaborative Care benefits patients & providers Patients and providers report high rates of satisfaction with collaborative care for depression - Unutzer et al, JAMA Levine et al, Gen Hosp Psychiatry Saur et al, submitted
48 Depression Care Manager: Core Skills Actively engages the patient in a therapeutic alliance Conducts initial assessment and follow-up visits Educates about depression and goals/expectations of treatment Elicits preferences and encourages treatment adherence Provides Education Close monitoring / follow-up (PHQ-9) Antidepressant management (including side effect management) Brief, structured psychotherapy (PST-PC) Pleasant Events Scheduling / Behavioral Activation
49 Depression Care Manager: Core Skills (con t) Tracks depressive symptoms and treatment response (PHQ-9) Consults with team psychiatrist Collaborates closely with patient s primary care provider (PCP) Provides follow-up and recommendations to PCP who prescribes antidepressants Facilitates referrals to specialty care and community resources Prepares for relapse prevention
50 Depression Care Manager: The Facilitating Presence Actively engages the patient in a therapeutic alliance by: Eliciting concerns Providing information Clarifying preferences Encouraging informed decision-making Conveying hopefulness Teaching skills Monitoring progress Reinforcing self-management
51 Initial Visit Assessment Education Discuss treatment options / plans Coordinate care with PCP Start initial treatment plan Arrange follow-up contact in person or by phone in one week or earlier Document initial visit
52 Care manager video clip: Initial assessment
53
54 Patient Health Questionnaire PHQ-9 Assists with depression diagnosis Helps tracks 9 core symptoms of depression over time Easy to use Patients become familiar with it Can be done over the phone A good teaching tool
55
56 Understanding the PHQ-9 Score PHQ 9 Score = 0-4: No Depression PHQ-9 Score = 5-9: Mild Depression PHQ-9 Score = 10-14: Moderate Depression PHQ-9 Score > 15: Severe Depression
57 PHQ-9: Discussing score with patient Use score to educate patient about depression and to to reduce resistance and stigma Depression is a medical condition We have good treatments for this Don t argue about whether or not patient has depression => focus on symptoms and symptom resolution. Give hope! You don t have to feel this way. This can be treated.
58 Attitudes & Beliefs About Depression Among Older Adults Many older adults know little or nothing about depression Few older adults think of depression is a medical / health problem Older adults may feel like they should handle it themselves About 60 % of people aged 65 and older believe it is normal for people to get depressed as they age
59 Patient Education Depression affects the body, behavior, and thinking. Physical symptoms may be the most apparent. The cycle of depression model Depression can almost always be treated with antidepressant medications or psychotherapy. Recovery from depression is the rule, not the exception but relapse is common if treatment discontinued Minor tranquilizers, drugs, and alcohol can make depression worse, not better.
60 The Cycle of Depression STRESSORS Medical Illness Family Problems Work Problems THOUGHTS & FEELINGS Negative thoughts Low self esteem Sadness Hopelessness DEPRESSION PHYSICAL PROBLEMS Poor sleep Pain Low Energy Poor concentration BEHAVIOR Social Withdrawal Decreased activities Decreased productivity
61 Treatment Planning Patient, PCP & Care Manager all involved in making the treatment plan Treatment plans are individualized because patients differ in medical comorbidity psychiatric comorbidity prior history of depression and treatment current treatments treatment preferences treatment response
62 Patient Education About Antidepressants Key messages - How do these medications work? By restoring a chemical imbalance in the brain - There are several options (over 20 available medications) Anticipate - Patient concerns about medications - Side effects (these can be managed) - Problems with adherence Reinforce - Need for continuation or maintenance treatment to prevent relapse even after the patient feels better
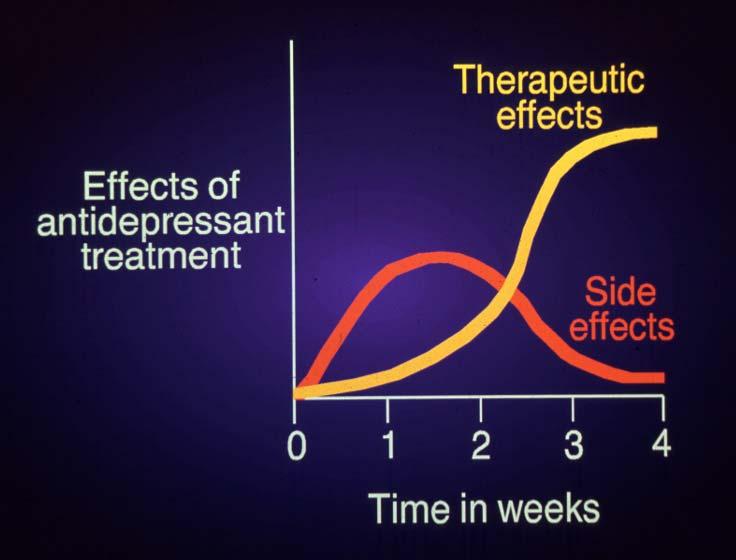
63 Antidepressant Adherence 100% 80% 60% 40% 20% 0% Weeks Lin EH. Med Care 1995;33:67 Key messages: Take medication daily Wait 2-4 weeks for effect Side effects can occur, but often resolve in 1-2 weeks Keep taking medication even if better Check with MD before stopping Not addicting
64
65 Common Side Effects Short term: GI upset / nausea Jitteriness / restlessness / insomnia Sedation / fatigue Long term: Sexual dysfunction (up to 33%) Weight gain (5 to 10%)
66 Managing Side Effects Consult with prescribing provider / team psychiatrist - Are side effects physical or psychological? Short term strategies - Wait and support (e.g., GI side effects) - Adjust medication timing (e.g., take sedating meds at bedtime) - Consider temporary dose reduction - Treat side effects (see intervention manual) Change to a different antidepressant Change to or add PST-PC
67 When and How to Stop Antidepressants? Risk of relapse - 50% if 1 prior episode - 75% if 2 prior episodes - 90% if 3 prior episodes - Also increased with dysthymia and residual depressive symptoms Treat all adults for 4-9 months after initial response. Treat those at high risk for relapse for 2 years or longer. Some may need lifetime treatment. Maintenance treatment should be at full dose. Make a relapse prevention plan. Taper antidepressants slowly to avoid discontinuation syndrome.
68 Remember There are over 20 FDA approved antidepressants. - All are effective in ~ 50 % of patients - it may take several trials until an effective medication is identified for a particular patient - Patients need support during this time If medications are not effective after 8-10 weeks at a therapeutic dose - make sure patient is taking medication as prescribed - consult with prescribing provider - consult with team psychiatrist - a change in treatment plan is likely indicated (e.g., change in medication, augmentation of medication, switch to PST-PC or other depression treatment)
69 Behavioral Activation Depression inactivity and withdrawal = downward cycle of doing less and feeling worse Awareness of this pattern can help some patients understand the purpose and benefit of behavioral activation
70 Behavioral Activation Objective: Reduce depression by gradually increasing engagement in pleasant and enjoyable activities that are client identified Decrease negative emotional response Decrease avoidance patterns
71 Behavioral Activation Purpose: - Help patients re-engage pleasant activities and learn new ways of dealing with distress Goals: - Re-establish routines - Distract from problems or unpleasant events - Increase positively reinforcing experiences - Reduce avoidant patterns - Increase critical thinking
72 Evidence Activity scheduling is relatively uncomplicated, time-efficient and does not require complex skills from patients or therapist. This meta-analysis found clear indications that it is effective. - Cuijpers P, et al. Behavioral activation treatments of depression: A metaanalysis. April 2007 Clinical Psychology Review 27(3): Among more severely depressed patients, behavioral activation was comparable to antidepressant medication, and both significantly outperformed cognitive therapy. - Dimidjian S, et al. Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression. August J Consult Clin Psychol 74(4):
73 Strategies Review pleasant activities for ideas - things that used to be pleasant in the past - consider new activities Make a detailed plan with patient List activities and rate them for mastery and pleasure Choose and schedule a daily pleasant activity Mentally rehearse the selected activity Identify potential barriers (feasibility, realistic activities)
74 Follow-up Celebrate successes Review failures Maybe we picked the wrong activity? What might work better next time?
75 Care manager video clip: Behavioral Activation
76 Problem Solving Treatment Evidence-based Common Sense Brief Practical to Apply Easily Learned by Therapist and Patient High Patient Acceptance and Satisfaction Designed for primary care
77 Psychotherapy Pros: No medication side effects Learned skills retained after treatment Addresses interpersonal / real life problems Accommodates patient who doesn t want medications Alternative for poor response to medications Cons: May take longer to work (6-12 sessions) More time consuming May not be as effective for severe major depression Requires staff training and may vary by provider
78 PST-PC vs. Usual Psychotherapy Treatment Issue Therapist: Session duration: Tx Duration: Total Tx Time: PST-PC Multi-Specialty 30-Minutes 4-8 Sessions 2-5 Hours Psychotherapy Mental Health > One Hour >10 Sessions > 10 Hours
79 Depression, Problems, and Problem Solving Skills Relationship of Problems and Depression - Weak problem solving skills make a person vulnerable to depression. - Life problems can be precipitants of depression. - Once depressed, problems become more difficult to solve. Rationale for Treatment Effectiveness - Problem solving helps patients exert control over problems. - Fewer problems, increased self-efficacy, & hope improve mood. Once learned, skills can help prevent depression in the future. Thomas D Zurilla, Arthur Nezu and colleagues.
80 Three Broad Goals of PST-PC A. Understand the link between current problems in living and current symptoms. B. Use a systematic problem-solving strategy. C. Engage in pleasant, social and physical activities.
81 Seven Steps of PST - PC 1. Clarify and Define the Problem 2. Set Realistic/Achievable Goal 3. Generate Multiple Solutions: i.e., Brainstorming 4. Evaluate and Compare Solutions: i.e., Pros and Cons 5. Select a Feasible Solution 6. Implement the Solution: i.e., Action Plan 7. Evaluate the Outcome
82 Problem Solving Process UNIVERSE OF PROBLEMS Problem Definition Goal Brainstorming Pros and Cons Choosing a Solution Action Plan Outcome Evaluation
83 Follow-Up Contacts Weekly or every other week during acute treatment phase - In person or by telephone to evaluate depression severity (PHQ-9) treatment response Initial focus on - adherence to medications - discuss side effects - follow-up on activation and PST plans Later focus on - complete resolution of symptoms and restoration of functioning - long term treatment adherence
84 Care manager video clip: Follow-up
85 Treatment Response Full response: At least 50% reduction in PHQ-9 score (or less than 5) Partial response: Reduction in PHQ-9 of less than 50% No response: No reduction or increase in PHQ-9 score
86 Most patients will need treatment adjustments Only 30 50% of patients will have a complete response to initial treatment Remaining 50 70% will require at least one change in treatment to get better
87 Seek consultation with psychiatrist when patient... Is severely depressed (PHQ-9 score >20) Fails to respond to treatment Has complicating mental health diagnosis, such as personality disorder or substance abuse Is bipolar or psychotic Has current substance dependence Is suicidal or homicidal
88 What about plan B Treatment recommendations for partial or nonresponses (50-70 % of patients) augment initial treatment choice with psychotherapy (e.g., PST-PC) or medication switch to psychotherapy or an(other) antidepressant (especially if NO response in step one) Also consider: Combination therapy (if not tried earlier) Augmentation with more than one medication Referral to specialty mental health care for additional psychotherapy Electroconvulsive therapy (ECT)
89 If Patients Don t Improve Consider Wrong diagnosis? Problems with treatment adherence? Insufficient dose / duration of treatment? Side effects? Other complicating factors? - psychosocial stressors / barriers - medical problems / medications - psychological barriers - substance abuse - other psychiatric problems Initial treatment not effective (e.g. wrong drug)? Psychiatric consultation
90 Key Elements of Effective Consultation Systematic review & presentation of - entire caseload - focus on patients who are not improving Recommendations to patients and treating providers based on evidence-based guidelines In person consultation or effective referral for complex patients
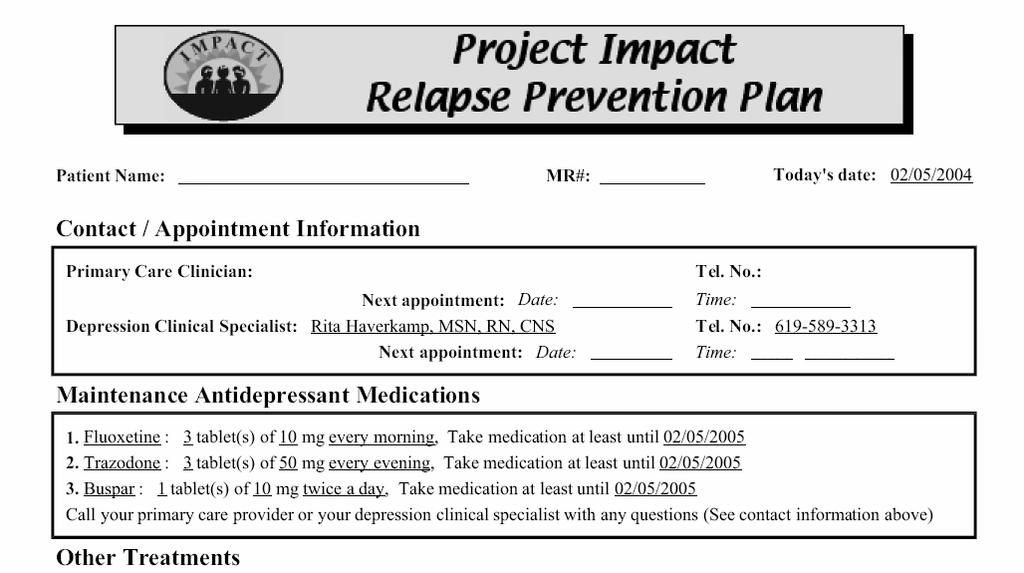
91 Maintenance Treatment for Depression After patient is in remission from acute episode fewer than 2 depressive symptoms Usually a PHQ-9 score less than 5 Make a relapse prevention plan Follow the patient with monthly contacts - usually by telephone calls - individual OR in a maintenance group Bring patient back in for further evaluation if symptoms recur
92
93 Care manager video clip: Relapse Prevention
94 Tracking Systems Tracking is an essential function in the IMPACT program - can be accomplished in many different ways - should be based on needs, resources - each has pros/cons

95 Paper Tracking


96 Excel Tracking
97 EMR Tracking Experience at Institute for Family Health adapting EPIC to facilitate care management
98 Implementing IMPACT

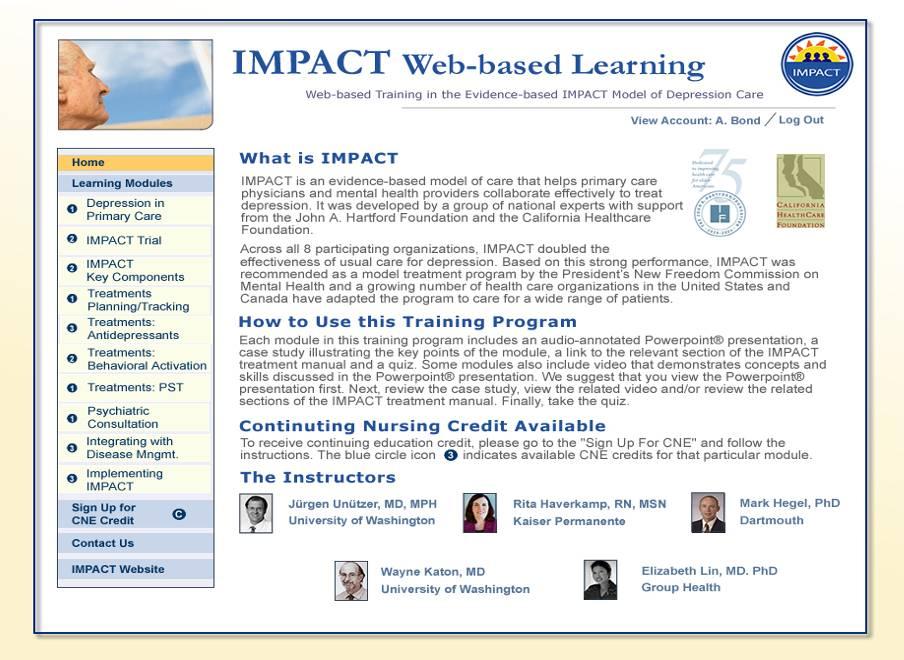
99 FREE materials: - Treatment manuals - Planning guides - Forms - Job descriptions - Much more Training: - Schedule of inperson training - 10 module online training program (free) Evidence: - More information about the evidence base for IMPACT
100



101 Thank You James D. Ralston The IMPACT Implementation Center is located in the Department of Psychiatry at the University of Washington in Seattle Funding for the IMPACT Implementation Center is generously provided by the John A. Hartford Foundation
IMPACT Improving Mood Promoting Access to Collaborative Treatment
 IMPACT Improving Mood Promoting Access to Collaborative Treatment for Late-Life Depression Funded by John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation, Hogg
IMPACT Improving Mood Promoting Access to Collaborative Treatment for Late-Life Depression Funded by John A. Hartford Foundation, California HealthCare Foundation, Robert Wood Johnson Foundation, Hogg
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Care Team Training. Key Components of Collaborative Care. Collaborative Team Approach 4/21/2014 PCP. Core Program. New Roles. Psychiatric Consultant
 Team Training Key Components of Collaborative Collaborative Team Approach Patient PCP Manager New Roles Core Program Psychiatric Consultant Behavioral Health Clinicians Additional Clinic Resources Substance,
Team Training Key Components of Collaborative Collaborative Team Approach Patient PCP Manager New Roles Core Program Psychiatric Consultant Behavioral Health Clinicians Additional Clinic Resources Substance,
Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect of treatment
 University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Fall September, 2006 Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect
University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Fall September, 2006 Making an IMPACT on late-life depression. Partnering with primary care providers can double the effect
The IMPACT Model. Delivering Effective Depression Treatment in the Primary Care Setting
 The IMPACT Model Delivering Effective Depression Treatment in the Primary Care Setting Presenters Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences, UW Rita Haverkamp,
The IMPACT Model Delivering Effective Depression Treatment in the Primary Care Setting Presenters Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences, UW Rita Haverkamp,
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Treating Depression in Disadvantaged Women: What is the evidence?
 Treating Depression in Disadvantaged Women: What is the evidence? Megan Dwight Johnson, MD MPH Associate Professor Medical Director, UWMC Inpatient Psychiatry Department of Psychiatry and Behavioral Sciences
Treating Depression in Disadvantaged Women: What is the evidence? Megan Dwight Johnson, MD MPH Associate Professor Medical Director, UWMC Inpatient Psychiatry Department of Psychiatry and Behavioral Sciences
Patient and Family Engagement and Retention. Care Manager Role. Who is on the recruitment/engagement team? General Recruitment Challenges
 Patient and Family Engagement and Retention Announcement from Archstone Foundation Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Center Trainer Collaborative Care Team Approach Care
Patient and Family Engagement and Retention Announcement from Archstone Foundation Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Center Trainer Collaborative Care Team Approach Care
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Collaborative Care Management of Late-Life Depression in the Primary Care Setting JAMA. 2002;288:
 ORIGINAL CONTRIBUTION Collaborative Care Management of Late-Life Depression in the Primary Care Setting A Randomized Controlled Trial Jürgen Unützer, MD, MPH Wayne Katon, MD Christopher M. Callahan, MD
ORIGINAL CONTRIBUTION Collaborative Care Management of Late-Life Depression in the Primary Care Setting A Randomized Controlled Trial Jürgen Unützer, MD, MPH Wayne Katon, MD Christopher M. Callahan, MD
University of Washington
 Integrated Mental Health Care: closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences University of Washington unutzer@uw.edu
Integrated Mental Health Care: closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Professor & Vice-Chair Psychiatry and Behavioral Sciences University of Washington unutzer@uw.edu
Depression & Diabetes: Pathways and TeamCare Studies
 Depression & Diabetes: Pathways and TeamCare Studies Wayne Katon, MD 1 Mike VonKorff, ScD 2 Elizabeth Lin, MD, MPH 2 Paul Ciechanowski, MD, MPH 1 Evette Ludman, PhD 2 Joan Russo, PhD 1 Carolyn Rutter,
Depression & Diabetes: Pathways and TeamCare Studies Wayne Katon, MD 1 Mike VonKorff, ScD 2 Elizabeth Lin, MD, MPH 2 Paul Ciechanowski, MD, MPH 1 Evette Ludman, PhD 2 Joan Russo, PhD 1 Carolyn Rutter,
New York State Collaborative Care Initiative Thursday, January 24, 2013
 New York State Collaborative Care Initiative Thursday, January 24, 2013 Lloyd Sederer, MD Medical Director New York State Office of Mental Health Key Components of Collaborative Care Jürgen Unützer, MD,
New York State Collaborative Care Initiative Thursday, January 24, 2013 Lloyd Sederer, MD Medical Director New York State Office of Mental Health Key Components of Collaborative Care Jürgen Unützer, MD,
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Primary Care Provider & Psychiatric Consultant Roles. PC/PCP Role Session Objectives. Working as a Team. Joseph Cerimele Anna Ratzliff
 Primary Care Provider & Psychiatric Consultant Roles Joseph Cerimele Anna Ratzliff PC/PCP Role Session Objectives By the end of the session, participants will: 1. Understand the role of the psychiatric
Primary Care Provider & Psychiatric Consultant Roles Joseph Cerimele Anna Ratzliff PC/PCP Role Session Objectives By the end of the session, participants will: 1. Understand the role of the psychiatric
5/12/11. Educational Objectives. Goals
 Educational Objectives Learn: steps for initial depression screening and management in primary care when to refer to mental health providers tools for providers and patients principles of collaborative
Educational Objectives Learn: steps for initial depression screening and management in primary care when to refer to mental health providers tools for providers and patients principles of collaborative
Depression Update. Are you Breathing? 5/16/2017. Agenda for Today and Everyday
 Depression Update Shabana Haxton RN,MSN Depression Care/ Emotional care specialist Kaiser Permanente Riverside 05/23/2017 Are you Breathing? Agenda for Today and Everyday 1 Some Statistics What Depression
Depression Update Shabana Haxton RN,MSN Depression Care/ Emotional care specialist Kaiser Permanente Riverside 05/23/2017 Are you Breathing? Agenda for Today and Everyday 1 Some Statistics What Depression
Integrating Behavioral Health and Primary Care. Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013
 Integrating Behavioral Health and Primary Care Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013 Jürgen Unützer, MD, MPH, MA Disclosures Employment: University of Washington Professor
Integrating Behavioral Health and Primary Care Jürgen Unützer, MD, MPH, MA University of Washington November 13, 2013 Jürgen Unützer, MD, MPH, MA Disclosures Employment: University of Washington Professor
2) Percentage of adult patients (aged 18 years or older) with a diagnosis of major depression or dysthymia and an
 Percentage of adult patients (aged 18 years or older) with a diagnosis of major depression or dysthymia and an") Quality ID #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Prevention, Treatment, and Management of Mental Health
Quality ID #370 (NQF 0710): Depression Remission at Twelve Months National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Prevention, Treatment, and Management of Mental Health
Psychiatric Consultant Role in Collaborative Care Sept 12, 2013
 New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Psychiatric Consultant Role in Collaborative Care Sept 12, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Disorder. Objectives. Under Recognition/ Undertreatment. Making a Diagnosis
 Care Partners Primary Care Provider Lunch & Learn: Why PCPs Love Collaborative Care Presenter: Wayne Bentham, MD The advantage of the collaborative care model of depression management in primary care is
Care Partners Primary Care Provider Lunch & Learn: Why PCPs Love Collaborative Care Presenter: Wayne Bentham, MD The advantage of the collaborative care model of depression management in primary care is
Integrating Behavioral Health into Primary Care: Collaborative-Care Models
 Integrating Behavioral Health into Primary Care: Collaborative-Care Models Presented at the National Health Policy Forum September 17 th, 2013 Marc Avery, MD Clinical Associate Professor Associate Director
Integrating Behavioral Health into Primary Care: Collaborative-Care Models Presented at the National Health Policy Forum September 17 th, 2013 Marc Avery, MD Clinical Associate Professor Associate Director
Depression in Older Adults. Key Issues
 Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression in Older Adults Key Issues Depression and Older Adults: Key Issues is an overview of important information that you should know about depression in older adults. Depression is one of the most
Depression. Content. Depression is common. Depression Facts. Depression kills. Depression attacks young people
 Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Help and Healing: Section 2: Treatment Planning. Treatment and Timelines. Depression Treatment Reference. Care Team Communication
 Help and Healing: Resources for Depression Care and Recovery Section 2: Treatment Planning Treatment and Timelines Depression Treatment Reference Care Team Communication Provider Education Tool - Questions
Help and Healing: Resources for Depression Care and Recovery Section 2: Treatment Planning Treatment and Timelines Depression Treatment Reference Care Team Communication Provider Education Tool - Questions
Understanding Depression
 Understanding Depression What causes Depression? Family History Having family members who have depression may increase a person s risk Deficiencies of certain chemicals in the brain may lead to depression
Understanding Depression What causes Depression? Family History Having family members who have depression may increase a person s risk Deficiencies of certain chemicals in the brain may lead to depression
Depression in Late Life Initiative
 Depression in Late Life Initiative made possible by the Archstone Foundation Depression in Late Life Request for Proposals (RFP) Care Partners: Bridging Families, Clinics, and Communities to Advance Late
Depression in Late Life Initiative made possible by the Archstone Foundation Depression in Late Life Request for Proposals (RFP) Care Partners: Bridging Families, Clinics, and Communities to Advance Late
Relapse Prevention Webinar Agenda Relapse Prevention Planning
 Relapse Prevention Webinar Agenda Relapse Prevention Planning Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Trainer By the end of the webinar you will be able to Describe what a RPP
Relapse Prevention Webinar Agenda Relapse Prevention Planning Rita Haverkamp, MSN, PMHCNS BC, CNS Expert Care Manager and AIMS Trainer By the end of the webinar you will be able to Describe what a RPP
Elderly persons with low incomes
 Service Use and Outcomes Among Elderly Persons With Low Incomes Being Treated for Depression Patricia A. Areán, Ph.D. Amber M. Gum, Ph.D. Lingqi Tang, Ph.D. Jürgen Unützer, M.D., M.P.H. Objective: Older
Service Use and Outcomes Among Elderly Persons With Low Incomes Being Treated for Depression Patricia A. Areán, Ph.D. Amber M. Gum, Ph.D. Lingqi Tang, Ph.D. Jürgen Unützer, M.D., M.P.H. Objective: Older
Comparison of Depression Interventions after Acute Coronary Syndrome. Treatment Manual
 Comparison of Depression Interventions after Acute Coronary Syndrome Treatment Manual v. 05/11/2010 Table of Contents Treatment Manual... 0 Table of Contents... 1 1. CODIACS TREATMENT MANUAL BACKGROUND
Comparison of Depression Interventions after Acute Coronary Syndrome Treatment Manual v. 05/11/2010 Table of Contents Treatment Manual... 0 Table of Contents... 1 1. CODIACS TREATMENT MANUAL BACKGROUND
An Evidence Based Treatment Approach for Older Adults. Helen Stewart, MSW, LCSW Michelle Bonadies, LCSW
 Introduction ti to PEARLS: An Evidence Based Treatment Approach for Older Adults Pillars Helen Stewart, MSW, LCSW Michelle Bonadies, LCSW Overview Depression in Older Adults What is PEARLS? Experience
Introduction ti to PEARLS: An Evidence Based Treatment Approach for Older Adults Pillars Helen Stewart, MSW, LCSW Michelle Bonadies, LCSW Overview Depression in Older Adults What is PEARLS? Experience
PATIENT HEALTH QUESTIONNAIRE PHQ-9 FOR DEPRESSION
 PATIENT HEALTH QUESTIONNAIRE PHQ-9 FOR DEPRESSION USING PHQ-9 DIAGNOSIS AND SCORE FOR INITIAL TREATMENT SELECTION A depression diagnosis that warrants treatment or treatment change, needs at least one
PATIENT HEALTH QUESTIONNAIRE PHQ-9 FOR DEPRESSION USING PHQ-9 DIAGNOSIS AND SCORE FOR INITIAL TREATMENT SELECTION A depression diagnosis that warrants treatment or treatment change, needs at least one
Behavioral Interventions The TEAMcare Approach. Bernadette G. Overstreet BSH Tatiana E. Ramirez DDS., MBA Health Educators Project Turning Point
 Behavioral Interventions The TEAMcare Approach Bernadette G. Overstreet BSH Tatiana E. Ramirez DDS., MBA Health Educators Project Turning Point TEAMcare Background TEAMcare is a comprehensive, cost-effective
Behavioral Interventions The TEAMcare Approach Bernadette G. Overstreet BSH Tatiana E. Ramirez DDS., MBA Health Educators Project Turning Point TEAMcare Background TEAMcare is a comprehensive, cost-effective
Behavioral Activation in the Treatment of Depression: An Effective and Efficient Model in the Primary Care Setting
 Behavioral Activation in the Treatment of Depression: An Effective and Efficient Model in the Primary Care Setting Presenter Bob Davis, LMSW Claystone Clinical Associates Assistant Adjunct Professor Graduate
Behavioral Activation in the Treatment of Depression: An Effective and Efficient Model in the Primary Care Setting Presenter Bob Davis, LMSW Claystone Clinical Associates Assistant Adjunct Professor Graduate
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Resident Rotation: Collaborative Care Consultation Psychiatry
 Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD Ramanpreet Toor, MD James Basinski, MD With contributions from: Jürgen Unützer, MD, MPH, MA Jennifer Sexton, MD, Catherine
Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD Ramanpreet Toor, MD James Basinski, MD With contributions from: Jürgen Unützer, MD, MPH, MA Jennifer Sexton, MD, Catherine
Treating Depressed Patients with Comorbid Trauma. Lori Higa BSN, RN-BC AIMS Consultant/Trainer
 Treating Depressed Patients with Comorbid Trauma Lori Higa BSN, RN-BC AIMS Consultant/Trainer Learning Objectives By the end of this training, participants should be able to: Discuss recent trends in trauma
Treating Depressed Patients with Comorbid Trauma Lori Higa BSN, RN-BC AIMS Consultant/Trainer Learning Objectives By the end of this training, participants should be able to: Discuss recent trends in trauma
CBT / PST Treatment Brief Therapy. Objectives. Lesson learned. Many new tools to help meet the current needs. Current working environment
 CBT / PST Treatment Brief Therapy Rita Haverkamp The speaker has no conflicts of interest to disclose All images used are clipart MSN, PMHCNS-BC, CNS Objectives By the end of this session, you will be
CBT / PST Treatment Brief Therapy Rita Haverkamp The speaker has no conflicts of interest to disclose All images used are clipart MSN, PMHCNS-BC, CNS Objectives By the end of this session, you will be
Behavioral Activation
 Behavioral Activation Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services, Centers
Behavioral Activation Care of Mental, Physical, and Substance use Syndromes! The project described was supported by Grant Number 1C1CMS331048-01-00 from the Department of Health and Human Services, Centers
Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management. Capstone Meeting Tucson, Arizona October 18 20, 2006
 Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management Capstone Meeting Tucson, Arizona October 18 20, 2006 Anonymous, Northwest PCP: You know, when I have a patient who has been
Promoting Healthy Coping & Addressing Negative Emotion in Diabetes Management Capstone Meeting Tucson, Arizona October 18 20, 2006 Anonymous, Northwest PCP: You know, when I have a patient who has been
CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH)
") CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH) The infant and young child should experience a warm, intimate, and continuous relationship with his mother in which both find satisfaction and
CENTER OF EXCELLENCE MATERNAL AND CHILD MENTAL HEALTH (MCMH) The infant and young child should experience a warm, intimate, and continuous relationship with his mother in which both find satisfaction and
AN OVERVIEW OF ANXIETY
 AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
AN OVERVIEW OF ANXIETY Fear and anxiety are a normal part of life. Normal anxiety keeps us alert. Intervention is required when fear and anxiety becomes overwhelming intruding on a persons quality of life.
Achieve Remission in Adult Patients With Non-Psychotic Major Depressive Disorder: Algorithm
 Achieve Remission in Adult Patients With Non-Psychotic Major Depressive Disorder: Algorithm Initiate antidepressant at minimally-effective dose to optimize tolerability. Refer for cognitive-behavioral
Achieve Remission in Adult Patients With Non-Psychotic Major Depressive Disorder: Algorithm Initiate antidepressant at minimally-effective dose to optimize tolerability. Refer for cognitive-behavioral
Summary of guideline for the. treatment of depression RANZCP CLINICAL PRACTICE GUIDELINES ASSESSMENT
 RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
Implementing and Improving Depression Screenings in the Primary Care Setting. Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager
 Implementing and Improving Depression Screenings in the Primary Care Setting Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager Today s Objectives Participants will: Increase understanding
Implementing and Improving Depression Screenings in the Primary Care Setting Janet Tennison, PhD, MSW, LCSW Behavioral Health Project Manager Today s Objectives Participants will: Increase understanding
Depression Assessment and Management. John Kern MD Clinical Professor University of Washington
 Depression Assessment and Management John Kern MD Clinical Professor University of Washington Handouts Antidepressant Treatment Flowchart Managing antidepressant nonresponse handouts 2 Diagnosis PHQ-9
Depression Assessment and Management John Kern MD Clinical Professor University of Washington Handouts Antidepressant Treatment Flowchart Managing antidepressant nonresponse handouts 2 Diagnosis PHQ-9
Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care
: Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care") Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #411 (NQF 0711): Depression Remission at Six Months National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Optimistic News and Practical Tools. The Role of Primary Care in Screening and Managing Teen Depression
 Optimistic News and Practical Tools The Role of Primary Care in Screening and Managing Teen Depression Meg Durbin, MD Palo Alto Medical Foundation DurbinM@pamf.org Educational Objectives Learn: steps for
Optimistic News and Practical Tools The Role of Primary Care in Screening and Managing Teen Depression Meg Durbin, MD Palo Alto Medical Foundation DurbinM@pamf.org Educational Objectives Learn: steps for
MATCP When the Severity of Symptoms Interferes with Progress
 MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
Depression Care. Patient Education Script
 Everybody has the blues from time to time, or reacts to stressful life events with feelings of anxiety, sadness, or anger. Normally these feelings go away with time but when they persist, and are present
Everybody has the blues from time to time, or reacts to stressful life events with feelings of anxiety, sadness, or anger. Normally these feelings go away with time but when they persist, and are present
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
PST-PC Appendix. Introducing PST-PC to the Patient in Session 1. Checklist
 PST-PC Appendix Introducing PST-PC to the Patient in Session 1 Checklist 1. Structure of PST-PC Treatment 6 Visits Today Visit: 1-hour; Visits 2-8: 30-minutes Weekly and Bi-weekly Visits Teach problem
PST-PC Appendix Introducing PST-PC to the Patient in Session 1 Checklist 1. Structure of PST-PC Treatment 6 Visits Today Visit: 1-hour; Visits 2-8: 30-minutes Weekly and Bi-weekly Visits Teach problem
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
What kinds of patients would be appropriate for collaborative care? Goals and Objectives. Overview and Introduction
 What kinds of patients would be appropriate for collaborative care? A) Patients that need brief behavioral interventions/therapy only B) Patients that need medications only C) Patients that need both brief
What kinds of patients would be appropriate for collaborative care? A) Patients that need brief behavioral interventions/therapy only B) Patients that need medications only C) Patients that need both brief
Treatment Algorithm Treatment Algorithm
 Treatment Algorithm Treatment Algorithm Primary Care Toolkit September 2015 Page 2 Adult (>18 years) Depression Flow Chart (Generic) Two Question Screen: PHQ-2 Annually, new adult patients, and when suspect
Treatment Algorithm Treatment Algorithm Primary Care Toolkit September 2015 Page 2 Adult (>18 years) Depression Flow Chart (Generic) Two Question Screen: PHQ-2 Annually, new adult patients, and when suspect
Pediatrics Grand Rounds 5 March University of Texas Health Science Center at San Antonio I-1
 Diagnosis and Treatment of Depression in Children and Adolescents Steven R. Pliszka, M.D. Professor and Vice Chair Chief, Division of Child and Adolescent Psychiatry Department of Psychiatry The Disclosures
Diagnosis and Treatment of Depression in Children and Adolescents Steven R. Pliszka, M.D. Professor and Vice Chair Chief, Division of Child and Adolescent Psychiatry Department of Psychiatry The Disclosures
Enhancing Treatment. Recognizing Depression and. Tools for successful patient management. Provider Communications. Health Net. Christian Aparicio,
 Provider Communications Recognizing Depression and Enhancing Treatment Tools for successful patient management Christian Aparicio, Health Net We offer tools and resources for improving member health. Contents
Provider Communications Recognizing Depression and Enhancing Treatment Tools for successful patient management Christian Aparicio, Health Net We offer tools and resources for improving member health. Contents
Appendix C: Algorithms. Algorithm C-1: Enhanced Screening Algorithm
 Appendix C: Algorithms Algorithm C-1: Enhanced Screening Algorithm PCC Depression Screening Neg Annual Screening Pos CPRS Alert to Team Enhanced Screening Via Telephone Unable To Contact Telephone Introduction
Appendix C: Algorithms Algorithm C-1: Enhanced Screening Algorithm PCC Depression Screening Neg Annual Screening Pos CPRS Alert to Team Enhanced Screening Via Telephone Unable To Contact Telephone Introduction
Comparison of Depression Interventions after Acute Coronary Syndrome
 Comparison of Depression Interventions after Acute Coronary Syndrome Funded by the National Heart Lung and Blood Institute RC2-HL HL-101663 Depressive Symptoms are Related to Acute Coronary Events Increased
Comparison of Depression Interventions after Acute Coronary Syndrome Funded by the National Heart Lung and Blood Institute RC2-HL HL-101663 Depressive Symptoms are Related to Acute Coronary Events Increased
Webinar Agenda. Terminology. What Is It? How this fits for depression. Social Innovation Fund. Relapse Prevention Planning. Relapse Prevention
 SIF Webinar: Relapse Prevention 3/11/15 Webinar Agenda Relapse Prevention Social Innovation Fund Relapse Prevention Planning Rita Haverkamp Lori Higa What it is Why it s important Common and best practices
SIF Webinar: Relapse Prevention 3/11/15 Webinar Agenda Relapse Prevention Social Innovation Fund Relapse Prevention Planning Rita Haverkamp Lori Higa What it is Why it s important Common and best practices
INSTRUCTION MANUAL Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures
 and GAD-7 Measures") PHQ and GAD-7 Instructions P. 1/9 INSTRUCTION MANUAL Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures TOPIC PAGES Background 1 Coding and Scoring 2, 4, 5 Versions 3 Use as Severity
PHQ and GAD-7 Instructions P. 1/9 INSTRUCTION MANUAL Instructions for Patient Health Questionnaire (PHQ) and GAD-7 Measures TOPIC PAGES Background 1 Coding and Scoring 2, 4, 5 Versions 3 Use as Severity
Managing Depression as a Chronic Condition. D. Green MD TOH/Bruyere Shared Care Program
 Managing Depression as a Chronic Condition D. Green MD TOH/Bruyere Shared Care Program None Financial disclosure Objectives To review key concepts relevant to understanding the course of depression To
Managing Depression as a Chronic Condition D. Green MD TOH/Bruyere Shared Care Program None Financial disclosure Objectives To review key concepts relevant to understanding the course of depression To
A Randomized Controlled Trial of In-Person and Telephone Cognitive Behavioral Therapy for Major Depression after Traumatic Brain Injury
 A Randomized Controlled Trial of In-Person and Telephone Cognitive Behavioral Therapy for Major Depression after Traumatic Brain Injury Josh Dyer, PhD Department of Rehabilitation Medicine University of
A Randomized Controlled Trial of In-Person and Telephone Cognitive Behavioral Therapy for Major Depression after Traumatic Brain Injury Josh Dyer, PhD Department of Rehabilitation Medicine University of
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Care management for depression and osteoarthritis pain in older primary care patients: a pilot study
 University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Spring April 8, 2008 Care management for depression and osteoarthritis pain in older primary care patients: a pilot study Ju
University of Massachusetts Boston From the SelectedWorks of Steven D Vannoy Spring April 8, 2008 Care management for depression and osteoarthritis pain in older primary care patients: a pilot study Ju
Denver Health s Roadmap to Reduce Racial Disparities: Telephonic Counseling for Depression and Anxiety
 Denver Health s Roadmap to Reduce Racial Disparities: Telephonic Counseling for Depression and Anxiety David Brody, MD Medical Director Denver Health Managed Care Plans Professor of Medicine University
Denver Health s Roadmap to Reduce Racial Disparities: Telephonic Counseling for Depression and Anxiety David Brody, MD Medical Director Denver Health Managed Care Plans Professor of Medicine University
Linda Parisi, BSN, MA, RN BC; David Karcher, MSN, PMH CNS, RN 1
 APNA National Conference Depression Matters: Advocating for the Best Care The presenters have no conflicts of interest to disclose Linda Parisi, BSN, MA, RN-BC David Karcher, MSN, PMH-CNS, RN (Permission
APNA National Conference Depression Matters: Advocating for the Best Care The presenters have no conflicts of interest to disclose Linda Parisi, BSN, MA, RN-BC David Karcher, MSN, PMH-CNS, RN (Permission
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System
 Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Kaiser Telecare Program for Intensive Community Support Intensive Case Management Exclusively for Members within a Managed Care System 12-Month Customer Report, January to December, 2007 We exist to help
Depression Screening: An Effective Tool to Reduce Disability and Loss of Productivity
 Depression Screening: An Effective Tool to Reduce Disability and Loss of Productivity Kay n Campbell. EdD. RN-C. COHN-S, FAAOHN ICOH Cancun, Mexico March, 2012 What Is It? Common mental disorder Affects
Depression Screening: An Effective Tool to Reduce Disability and Loss of Productivity Kay n Campbell. EdD. RN-C. COHN-S, FAAOHN ICOH Cancun, Mexico March, 2012 What Is It? Common mental disorder Affects
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans
 Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans Steve Bartels MD, MS Professor of Psychiatry, Community and Family Medicine, and The Dartmouth Institute Geisel
Closing the Gap: Implementing Evidence-based Behavioral Health Practices for Older Americans Steve Bartels MD, MS Professor of Psychiatry, Community and Family Medicine, and The Dartmouth Institute Geisel
STAR-CENTER PUBLICATIONS. Services for Teens at Risk
 STAR-CENTER PUBLICATIONS Services for Teens at Risk Teen Handbook on Depression Services for Teens at Risk (STAR-Center) Western Psychiatric Institute and Clinic (412)864-3346 All Rights Reserved - 2018
STAR-CENTER PUBLICATIONS Services for Teens at Risk Teen Handbook on Depression Services for Teens at Risk (STAR-Center) Western Psychiatric Institute and Clinic (412)864-3346 All Rights Reserved - 2018
Principles in Action Case Example
 1 Principles in Action Case Example Patient Centered Team Care / Collaborative Care Co-location is not Collaboration. Team members learn to work differently. Population-Based Care All patients tracked
1 Principles in Action Case Example Patient Centered Team Care / Collaborative Care Co-location is not Collaboration. Team members learn to work differently. Population-Based Care All patients tracked
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
8. DEPRESSION 1. Eve A. Kerr, M.D., M.P.H. and Kenneth A. Clark, M.D., M.P.H.
 8. DEPRESSION 1 Eve A. Kerr, M.D., M.P.H. and Kenneth A. Clark, M.D., M.P.H. We relied on the following sources to construct quality indicators for depression: the AHCPR Clinical Practice Guideline in
8. DEPRESSION 1 Eve A. Kerr, M.D., M.P.H. and Kenneth A. Clark, M.D., M.P.H. We relied on the following sources to construct quality indicators for depression: the AHCPR Clinical Practice Guideline in
BREAKING FREE FROM DEPRESSION AND DIABETES 10 THINGS YOU NEED TO KNOW AND DO
 BREAKING FREE FROM DEPRESSION AND DIABETES 10 THINGS YOU NEED TO KNOW AND DO Depression is like a black hole. It can take the joy out of life, drain your energy and motivation, and cause you to feel hopeless
BREAKING FREE FROM DEPRESSION AND DIABETES 10 THINGS YOU NEED TO KNOW AND DO Depression is like a black hole. It can take the joy out of life, drain your energy and motivation, and cause you to feel hopeless
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Pain Psychology: Disclosure Slide. Learning Objectives. Bio-psychosocial Model 8/12/2014. What we won t cover (today) What influences chronic pain?
 What influences chronic pain?") Disclosure Slide Pain Psychology: No commercial interests to disclose Screening for distress and maladaptive attitudes and beliefs Paul Taenzer PhD, CPsych Learning Objectives At the end of the session,
Disclosure Slide Pain Psychology: No commercial interests to disclose Screening for distress and maladaptive attitudes and beliefs Paul Taenzer PhD, CPsych Learning Objectives At the end of the session,
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS
 Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
Taking Care: Child and Youth Mental Health TREATMENT OPTIONS Open Learning Agency 2004 TREATMENT OPTIONS With appropriate treatment, more than 80% of people with depression get full relief from their symptoms
TEAMcare at The Polyclinic: Collaborative Care for Diabetes and Depression
 TEAMcare at The Polyclinic: Collaborative Care for Diabetes and Depression Michael J. Tronolone, MD, MMM CMO, The Polyclinic Seattle, WA April 3, 2014 1 The Multi-Condition Patient JAMA, April 7, 2010
TEAMcare at The Polyclinic: Collaborative Care for Diabetes and Depression Michael J. Tronolone, MD, MMM CMO, The Polyclinic Seattle, WA April 3, 2014 1 The Multi-Condition Patient JAMA, April 7, 2010
Screening for Depression and Suicide
 Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
Depression intervention via referral, education, and collaborative treatment (Project DIRECT): a pilot study
: a pilot study") Executive summary of completed research Depression intervention via referral, education, and collaborative treatment (Project DIRECT): a pilot study Principal Investigator Jane McCusker, MD DrPH Co-investigators
Executive summary of completed research Depression intervention via referral, education, and collaborative treatment (Project DIRECT): a pilot study Principal Investigator Jane McCusker, MD DrPH Co-investigators
Anxiety and Depression Association of America 34 th Annual Conference March 27-30, 2014
 Anxiety and Depression Association of America 34 th Annual Conference March 27-30, 2014 Inger E. Burnett-Zeigler, Ph.D. Assistant Professor Asher Center for the Study and Treatment of Depressive Disorders
Anxiety and Depression Association of America 34 th Annual Conference March 27-30, 2014 Inger E. Burnett-Zeigler, Ph.D. Assistant Professor Asher Center for the Study and Treatment of Depressive Disorders
10 INDEX Acknowledgements, i
 INDEX 10 INDEX Acknowledgements, i Acute Care, Admissions to, 3.83 Discharge Planning, 3.86 Involuntary Admission Criteria, 3.84 List of Designated Provincial and Regional Mental Health Facilities, 3.83
INDEX 10 INDEX Acknowledgements, i Acute Care, Admissions to, 3.83 Discharge Planning, 3.86 Involuntary Admission Criteria, 3.84 List of Designated Provincial and Regional Mental Health Facilities, 3.83
Epidemiological and clinical studies consistently indicate that
 Depression and Comorbid Illness in Elderly Primary Care Patients: Impact on Multiple Domains of Health Status and Well-being Polly Hitchcock Noël, PhD 1,2 John W. Williams Jr, MD, MHS 3,4 Jürgen Unützer,
Depression and Comorbid Illness in Elderly Primary Care Patients: Impact on Multiple Domains of Health Status and Well-being Polly Hitchcock Noël, PhD 1,2 John W. Williams Jr, MD, MHS 3,4 Jürgen Unützer,
Depressive disorders are common in primary care,
 Do Clinician and Patient Adherence Predict Outcome in a Depression Disease Management Program? Catherine J. Datto, MD, Richard Thompson, PhD, David Horowitz, MD, Maureen Disbot, RN, Hillary Bogner, MD,
Do Clinician and Patient Adherence Predict Outcome in a Depression Disease Management Program? Catherine J. Datto, MD, Richard Thompson, PhD, David Horowitz, MD, Maureen Disbot, RN, Hillary Bogner, MD,
Diabetes and Depression. Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C
 Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)
 Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017)") Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Protocol Title: Depression & Generalized Anxiety Disorder Effective Date: 5/28/2014 Version: 2.0 (Revised: 10/12/2015) Approval By: CCC Clinical Delivery Steering Planned Review Date: (04/47/2017) Group
Long-Term Effects on Medical Costs of Improving Depression Outcomes in Patients With Depression and Diabetes
 Epidemiology/Health Services Research O R I G I N A L A R T I C L E Long-Term Effects on Medical Costs of Improving Depression Outcomes in Patients With Depression and Diabetes WAYNE J. KATON, MD 1 JOAN
Epidemiology/Health Services Research O R I G I N A L A R T I C L E Long-Term Effects on Medical Costs of Improving Depression Outcomes in Patients With Depression and Diabetes WAYNE J. KATON, MD 1 JOAN
Appendix B: Screening and Assessment Instruments
 Appendix B: Screening and Assessment Instruments Appendix B-1: Quick Guide to the Patient Health Questionnaire (PHQ) Purpose. The Patient Health Questionnaire (PHQ) is designed to facilitate the recognition
Appendix B: Screening and Assessment Instruments Appendix B-1: Quick Guide to the Patient Health Questionnaire (PHQ) Purpose. The Patient Health Questionnaire (PHQ) is designed to facilitate the recognition
BIPOLAR DISORDER. BIPOLAR DISORDER is. a lifelong illness. It affects. millions of people each. year. With proper treatment,
 BIPOLAR DISORDER is a lifelong illness. It affects millions of people each year. With proper treatment, people with bipolar disorder can live normal lives. Work with your doctor to find treatment that
BIPOLAR DISORDER is a lifelong illness. It affects millions of people each year. With proper treatment, people with bipolar disorder can live normal lives. Work with your doctor to find treatment that