Jessica Kaffenberger, MD
|
|
|
- Melanie Gaines
- 5 years ago
- Views:
Transcription
1 Dermatology: What you need to know in primary care Part I Jessica Kaffenberger, MD Assistant Professor Clinical Division of Dermatology The Ohio State University Wexner Medical Center 20 most common dermatology diagnoses 1. acne 11. hemangiomas/port-wine 2. rosacea stain 3. psoriasis 12. verruca/condyloma 13. molluscum contagiosum 4. seborrheic dermatitis 14. seborrheic keratosis 5. atopic dermatitis 15. actinic keratosis 6. contact dermatitis 16. melanocytic nevi 7. stasis 17. impetigo, folliculitis, dermatitis/ulcers abscess 8. urticaria 18. herpesvirus infections 9. dermatophyte 19. scabies infections 20. pityriasis rosea 10. tinea versicolor 1
2 20 most common dermatology diagnoses 1. acne 11. hemangiomas/port-wine 2. rosacea stain 3. psoriasis 12. verruca/condyloma 13. molluscum contagiosum 4. seborrheic dermatitis 14. seborrheic keratosis 5. atopic dermatitis 15. actinic keratosis 6. contact dermatitis 16. melanocytic nevi 7. stasis 17. impetigo, folliculitis, dermatitis/ulcers abscess 8. urticaria 18. herpesvirus infections 9. dermatophyte 19. scabies infections 20. pityriasis rosea 10. tinea versicolor HEAD SHOULDERS KNEES TOES 2
3 HEAD SHOULDERS KNEES TOES PSORIASIS 3




4 Psoriasis Four Main types: Plaque Guttate Pustular Inverse Arthritis can be seen with any type Plaque Psoriasis OSUDERM.org 4









5 Plaque Psoriasis Most common type Scalp, Elbows, Knees, Sacrum Usually itches OSUDERM.org Guttate Psoriasis More common in children Related to strep infections Trunk most involved May resolve spontaneously OSUDERM.org OSUDERM.org 5




6 Inverse Psoriasis Usually macerated scale NOT visible Photo from J.Kaffenberger Photo from J.Kaffenberger Pustular Psoriasis Most acute type Can be life threatening May have fevers, high WBC Can be caused by withdrawal of systemic steroids OSUDERM.org OSUDERM.org 6

 - Ultraviolet light: 2-3x weekly Systemic Other: - Pustular pso: call derm - AVOID systemic steroids")
 Pso")
7 Treatment Topical Psoriasis - Acitretin, cyclosporine, biologics (call dermatologist) - Steroids: mid-strong potency - Triamcinolone 0.1% (only one that comes in a tub) - Calcipotriene - Tacrolimus/Pimecrolimus: usually for inverse pso (off- label) - Ultraviolet light: 2-3x weekly Systemic Other: - Pustular pso: call derm - AVOID systemic steroids can cause severe flare when stopped OSUDERM.org Psoriasis Pearls: Give appropriate amount of topical medication (Whole body application approx 30g) Pso = lifelong condition choose therapies accordingly Make sure correct vehicle for all pso locations Scalp = oil, solution, foam Body = cream, ointment 7

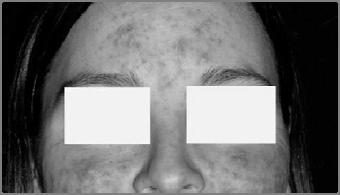
8 SEBORRHEIC DERMATITIS Most common = Face and scalp butterfly rash Can affect intertriginous areas esp in children Yellow/greasy scale OSUDERM.org Cause: Pityrosporum ovale +/- itch 8


 hydrocortisone 1-2.")
9 Photo from J.Kaffenberger Photo from J.Kaffenberger Seborrheic dermatitis Treatment Zinc, selenium sulfide, or ketoconazole shampoos Leave in for 3-5 min before rinsing Use on side of nose and eyebrows too Scalp: Clobetasol solution Face: Intermittent t (minimize i i use) hydrocortisone 1-2.5%, or tacrolimus/pimecrolimus 9
10 Seborrheic dermatitis pearls Manage expectations: can t cure, can control Assoc with Parkinson s and AIDs Can overlap with psoriasis sebopsoriasis ACNE 10

11 One size fits all Photo from J.Kaffenberger Photo from J.Kaffenberger One size fits all Photo from J.Kaffenberger 1. Non-inflammatory: Comedones Photo from J.Kaffenberger 11





12 One size fits all Photo from J.Kaffenberger 1. Non-inflammatory: Comedones 2. Inflammatory Papules Pustules Nodules Cysts Photo from J.Kaffenberger Pathogenesis of acne. 12




13 Non-inflammatory acne - abnormal keratinization - increased sebum production OSUDERM.org OSUDERM.org Open comedones = blackheads Closed comedones = whiteheads Non-inflammatory acne Treatment: - **Retinoid** - Adapalene - Tretinoin - Tazarotene - Benzoyl peroxide wash or gel - Salicyclic acid 13


14 Inflammatory Acne OSUDERM.org Pathogenesis: Abnormal keratinization Increased sebum production Inflammation P. acnes Lesions: Papules Pustules Nodules Cysts Inflammatory acne Treatment target all causes! Triple therapy 1. Antibiotics Doxycycline 100mg PO BID Minocycline 100mg PO BID Minimizecouseto36 course 3-6 months 2. Retinoid 3. BPO 14





15 SPECIAL CASES Inflammatory acne - severe OSUDERM.org OSUDERM.org - Nodules > 0.5cm in diameter and depth - Cysts - Scars 15
16 Severe inflammatory acne Treatment - Isotretinoin - Synthetic Vitamin A Derivative - Highly teratogenic controlled by gov t - Numerous A/E: - Xerosis - Hyperlipidemia -? depression/suicide -? IBD - Send to derm if not part of Ipledge program Inflammatory acne adult female O distribution Treatment: - Hormonal therapy - OCPs - 3 approved - Reality: all likely work, - Ideally pick one w/ low androgenic progestin - (norgestimate, desogestrel, drospirenone, 3 rd gen progestins) - Spironolactone (off-label) - Blocks androgens - Dose: 50mg BID, can increase to 100mg PO BID - S.E.: Breast tenderness, irreg periods, headache, feminization of male fetus 16
17 Acne pearls Biggest cause of treatment failure: Poor compliance * Counsel takes 2-3 months for therapy to work! Diet and acne..the jury is still out ROSACEA 17





18 Rosacea OSUDERM.org OSUDERM.org Rosacea 4 Types: 1. Erythrotelangiectatic 2. Papulopustular 3. Phymatous 4. Ocular OSUDERM.org 18




")


19 Rosacea Treatment: 1. Erythrotelangiectatic Aug 2013: Brimonidine topical gel, 0.33% Alpha-2 adrenergic agonist 2. Papulopustular Metrogel or metrocream Oral doxycycline (off-label) Anti-inflammatory dosing 3. Ocular Oral doxycycline (off-label) 4. Phymatous Surgery/ Shaw scalpel Rhinophyma OSUDERM.org OSUDERM.org 19
20 Rosacea pearls Anti-inflammatory dosing of doxycycline Doxycycline 20mg PO BID, 40mg PO daily, 50mg PO BID Effective Lower incidence of GI side effects Ask about eye symptoms Dry, gritty eyes Need oral doxycycline ACTINIC KERATOSES 20



21 OSUDERM.org Actinic Keratoses Treatment: Cryotherapy Field therapy : 5-fluorouracil, imiquimod, diclofenac New therapy: ingenol mebutate Intracellular protein kinase C agonist cellular necrosis Also immunostimulatory get cytotoxic t Ts against dysplastic cells Face 0.015% x 3 days, Trunk/extremities 0.05% x 2 days Face/scalp: 83% median reduction, Trunk: 75% median reduction 21
22 Actinic keratoses pearls Don t need to treat them all treat bothersome areas Field therapy can be difficult esp for elderly pts IMPETIGO 22

23 Photo from J.Kaffenberger Impetigo Most common: S. aureus Honey-colored crusts more than pustules More superficial than ecthyma More likely in kids w/ atopic derm Treatment: Topical antibiotic, antibacterial wash More severe: oral antibiotic (cephalexin) When to consult your local dermatologist? 23
24 Managing g the STAT acne consult Common rashes in primary care Part 2: Ben Kaffenberger, MD Assistant Professor Division of Dermatology The Ohio State University Wexner Medical Center 24
25 Objectives (I can Identify common patterns of) 1. Dermatitis/Eczemas A. Atopic Dermatitis B. Asteatotic eczema (Eczema craquele) C. Allergic/Irritant Contact Dermatitis D. Stasis Dermatitis E. Dermatophyte infections F. Tinea Versicolor G. Scabies 2. Urticaria 3. Hidradenitis Suppurativa 4. Severe cutaneous adverse reactions from drugs Topical Steroids You need to know Low: Hydrocortisone 2.5% crm/oint Medium: Body Triamcinolone 0.1% crm/oint High Potency: Body thick plaques High Potency: Body, thick plaques Betamethasone dipropionate augmented 0.05% crm/oint/lot 25





26 Psoriasis Atopic Dermatitis Atopic Dermatitis 26




27 Childhood Atopic Dermatitis Treatment of Atopic Dermatitis (AD) Moisturization (most important) Avoid triggers (food allergens, infections, airborne allergens) Antihistamines Topical steroids For severe disease: Send to dermatologist! 27

")
28 Asteatotic Eczema Eczema craquele Asteatotic Eczema Always elderly patients Always on the legs Worst in the wintertime B t t t t i t i ti Best treatment moisturization (ammonium lactate although triamcinolone can be beneficial initially) 28







29 Contact Dermatitis Contact Dermatitis Poison Ivy 29



30 Contact Dermatitis Poison Ivy Toxicodendron radicans. Very common, probably 75% of the population is sensitized Streaky Dermatitis New spots can appear for days after rash starts Blister fluid does not spread the rash Treat with 3 weeks of prednisone if severe ere otherwise high-potency topical steroids Contact Dermatitis Nickel 30



 Clothing (belts,")



31 Contact Dermatitis Nickel Most common cause of chronic allergic contact Common sources of exposure: Jewelry (earrings, watches, etc) Clothing (belts, snaps, rivets, etc) Coins, Keys, Eyeglasses Internet for sources of nickel free jewelry Contact Dermatitis Triple Antibiotic ointment (neomycin or bacitracin) 31









32 Contact Dermatitis - Neomycin Very common, up to 10% of the population is allergic Both Neomycin (most common cause of allergic contact dermatitis from topical medications) and Bacitracin - If a patient has used neomycin/bacitracin, have patient perform a repeat open application test Contact Dermatitis Fragrance and Preservatives 32


33 Contact Dermatitis Fragrance and Preservatives Face, Neck, Hands Common exposures: Shampoo, soap, conditioner, hair products, moisturizer, perfume, deodorant Very difficult to avoid these substances as even products that say hypoallergenic or dermatologist tested often have fragrances Allergic patients only react to some fragrances and preservatives Contact Dermatitis Perianal - Ask about diarrhea and use of diaper wipes - If using diaper wipes stop and give high potency steroid 33





34 Irritant Hand Dermatitis Irritant Hand Dermatitis Most commonly due to repetitive exposure to soap and water Interdigital and dorsal hands - Ask about frequency of handwashing Hand sanitizer is less damaging than soap g g p Need thick ointment to protect 34



35 Stasis Dermatitis Stasis Dermatitis For mild cases, compression is key Predisposed by lower limb injury, surgery, obesity, lymphedema, and increased age May apply Triamcinolone underneath stockings Contact dermatitis is common 35






36 Lymphedema ->Stasis Dermatitis Elephantiasis Tinea Ask about known Triggers. If none pinpointed, Titrate cetirizine to 20 mg daily. daily Can start H2 blocker as well. If no improvement Refer to derm, can consider further immunosuppressio n 36



37 Tinea Look for annular/arcuate appearance Also look for interdigital scale, mild tinea pedis KOH examination or skin biopsy will confirm Treat with Ketoconazole 2% cream bid UNLESS features suggestive for hair-follicle involvement 37


 as body")
38 Tinea Versicolor Tinea Versicolor Upper body, summer time, young-adults, typically in humid environments Scrape with slide or fingernail, scaling can confirm it Treat: Fluconazole 300 mg x 2, 1 wk apart For maintenance, have patient use OTC dandruff shampoo (zinc pyrithione, selenium, or ketoconazole) as body wash tiw 38




!")
39 Scabies Ask about known Triggers Triggers. If none pinpointed, Titrate cetirizine to 20 mg daily. Can start H2 blocker as well. If no improvement Refer to derm, can consider further immunosuppression Scabies Finger webs Antecubital fossa Axilla Breasts/Groin Permethrin (5%)! Neck down full body Everyone in house Everything washed in a hot cycle the following AM 39






40 Urticaria Ask about known Triggers. If none pinpointed, daily Titrate cetirizine to 20 mg daily. Can start H2 blocker as well. If no improvement Refer to derm, can consider further immunosuppression Urticaria - Hives Ask about known Triggers. If none pinpointed, Titrate cetirizine to 20 mg daily. Can start H2 blocker as well. If no improvement Refer to derm, can consider further immunosuppression 40



 for")
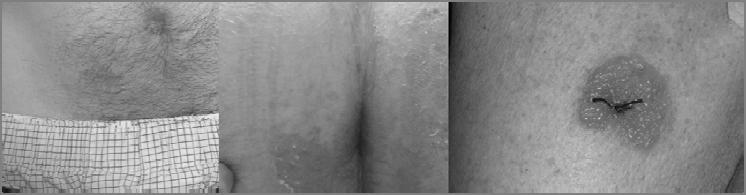
41 Urticaria Itchy, evanescent, and transient wheels *If greater than 24 hrs in one place, it is not urticaria!! not urticaria!! Common causes include strep infections, drugs, hymenoptera envenomations Never scaly Titrate cetirizine (start 10 mg bid) for treatment Hidradenitis suppurativa 41






42 Hidradenitis suppurativa Treatments: Topical acne treatments Weight loss Chronic antibiotics (Doxycycline 100 mg bid)??adalimumab, infliximab?? Needs referral to dermatology. If severe and can t get into dermatology consider referral to plastics/gen surg for excision and skin grafting Severe Cutaneous Adverse Reactions Stevens-Johnson Syndrome 42
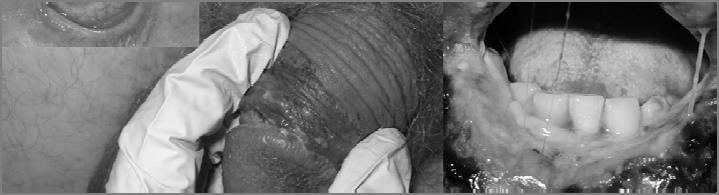




43 Stevens-Johnson Syndrome Stevens-Johnson Syndrome 43


44 Stevens-Johnson Syndrome Acute death of epidermis due to exposure to a medication Key early finding is pain/involvement of multiple mucous membranes, followed by sloughing of the skin Usually within 1-3 weeks of starting med Aromatic Anticonvulsants, allopurinol, Sulfa, NSAIDS, High Mortality - Stop med, call dermatology/hospital with dermatology capabilities Lastly Bed Bugs or Cimex lectularius C. Wayne Elliott Plant and Pest diagnostic center. - ppdc@cfaes.osu.edu, Thanks Everyone 44
No Disclosures. Objectives 12/13/2016. Pregnancy-Associated and Other Dermatoses of Young Women
 Pregnancy-Associated and Other Dermatoses of Young Women Kelly Tyler, MD, FACOG Division of Dermatology The Ohio State University 1 No Disclosures I have no financial interest or other conflict of interest
Pregnancy-Associated and Other Dermatoses of Young Women Kelly Tyler, MD, FACOG Division of Dermatology The Ohio State University 1 No Disclosures I have no financial interest or other conflict of interest
The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis
 Dermatology The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis The image to the left shows an image of skin cells and the proteins which
Dermatology The skin is the largest organ of the human body. Functions: protection sensation maintain temperature vitamin synthesis The image to the left shows an image of skin cells and the proteins which
Psoriasis. Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center
 Psoriasis Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center Learning objectives Recognize the different types of psoriasis
Psoriasis Jessica Kaffenberger, M.D. Assistant Professor of Dermatology Division of Dermatology The Ohio State University Wexner Medical Center Learning objectives Recognize the different types of psoriasis
Dermatology Pearls. Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018
 Dermatology Pearls Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018 What s on the agenda? Common skin conditions and where to start with treatment Gentle skin care regimen PCP and Biologics
Dermatology Pearls Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018 What s on the agenda? Common skin conditions and where to start with treatment Gentle skin care regimen PCP and Biologics
COMMON SKIN CONDITIONS IN PRIMARY CARE. Ibrahim M. Zayneh, MD Dermatology Private Practice, Portsmouth, Ohio
 COMMON SKIN CONDITIONS IN PRIMARY CARE Ibrahim M. Zayneh, MD Dermatology Private Practice, Portsmouth, Ohio DISCLOSURE The Speaker and members of the planning committee do not have a conflict of interest
COMMON SKIN CONDITIONS IN PRIMARY CARE Ibrahim M. Zayneh, MD Dermatology Private Practice, Portsmouth, Ohio DISCLOSURE The Speaker and members of the planning committee do not have a conflict of interest
Types of Skin Infections
 Anatomy of Skin Types of Skin Infections Bacterial Impetigo Folliculitis Acne Fungal /Parasitic Tinea Pedis Tinea Cruris Tinea Versicolor Tinea Corporis Toenail fungus Allergic/Irritation conditions Dermatitis
Anatomy of Skin Types of Skin Infections Bacterial Impetigo Folliculitis Acne Fungal /Parasitic Tinea Pedis Tinea Cruris Tinea Versicolor Tinea Corporis Toenail fungus Allergic/Irritation conditions Dermatitis
Dermclinic
 Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
ACNE UPDATE 2017 FACULTY DISCLOSURE ACNE UPDATE
 ACNE UPDATE 2017 PATRICIA TREADWELL, M.D. PROFESSOR OF PEDIATRICS AND DERMATOLOGY IU SCHOOL OF MEDICINE FACULTY DISCLOSURE I have no relevant financial relationships with the manufacturer(s) of any commercial
ACNE UPDATE 2017 PATRICIA TREADWELL, M.D. PROFESSOR OF PEDIATRICS AND DERMATOLOGY IU SCHOOL OF MEDICINE FACULTY DISCLOSURE I have no relevant financial relationships with the manufacturer(s) of any commercial
Learning Circle: Jan 26, 2011 Childhood Eczema
 Learning Circle: Jan 26, 2011 Childhood Eczema Wingfield Rehmus, MD MPH BC Children s Hospital Clinical Assistant Professor, UBC Department of Paediatrics Associate Member, UBC Department of Dermatology
Learning Circle: Jan 26, 2011 Childhood Eczema Wingfield Rehmus, MD MPH BC Children s Hospital Clinical Assistant Professor, UBC Department of Paediatrics Associate Member, UBC Department of Dermatology
Dermatology for the Internist DREW M ANDERSON, MD VOLUNTEER CLINICAL ASSISTANT PROFESSOR OF MEDICINE, INDIANA UNIVERSITY SCHOOL OF MEDICINE
 Dermatology for the Internist DREW M ANDERSON, MD VOLUNTEER CLINICAL ASSISTANT PROFESSOR OF MEDICINE, INDIANA UNIVERSITY SCHOOL OF MEDICINE Why Should I Care? 53% of all skin related visits are to non
Dermatology for the Internist DREW M ANDERSON, MD VOLUNTEER CLINICAL ASSISTANT PROFESSOR OF MEDICINE, INDIANA UNIVERSITY SCHOOL OF MEDICINE Why Should I Care? 53% of all skin related visits are to non
Pediatric Dermatology. Wingfield Rehmus, MD MPH BC Children s Hospital
 Pediatric Dermatology Wingfield Rehmus, MD MPH BC Children s Hospital Conflict of interest! No financial conflict of interest! Individual products shown are examples only not a product endorsement Pediatric
Pediatric Dermatology Wingfield Rehmus, MD MPH BC Children s Hospital Conflict of interest! No financial conflict of interest! Individual products shown are examples only not a product endorsement Pediatric
Time to Learn. 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service
 Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
COMMON CHILDHOOD SKIN DISEASES. Sharon Seguin MD FAAD
 COMMON CHILDHOOD SKIN DISEASES Sharon Seguin MD FAAD COMMON CHILDHOOD SKIN DISEASES Rashes Infections And Infestations RASHES Dermatitis- Inflammation of the skin Eczema- Atopic Dermatitis Psoriasis Pityriasis
COMMON CHILDHOOD SKIN DISEASES Sharon Seguin MD FAAD COMMON CHILDHOOD SKIN DISEASES Rashes Infections And Infestations RASHES Dermatitis- Inflammation of the skin Eczema- Atopic Dermatitis Psoriasis Pityriasis
ACNE. Jason M Cheyney, MPAS, PA-C Dermatologic Surgery Specialists Macon, Ga 31211
 ACNE Jason M Cheyney, MPAS, PA-C Dermatologic Surgery Specialists Macon, Ga 31211 Pathogenesis of Acne Causative Factors Therapy On the horizon Approximately 45 million Americans have acne It is often
ACNE Jason M Cheyney, MPAS, PA-C Dermatologic Surgery Specialists Macon, Ga 31211 Pathogenesis of Acne Causative Factors Therapy On the horizon Approximately 45 million Americans have acne It is often
Vulval dermatoses. Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough
 Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Subspecialty Rotation: Dermatology
 Subspecialty Rotation: Dermatology Faculty: Wesley Galen, M.D. GOAL: Prevention, Counseling and Screening (Dermatology). Understand the pediatrician's role in preventing illness and dysfunction related
Subspecialty Rotation: Dermatology Faculty: Wesley Galen, M.D. GOAL: Prevention, Counseling and Screening (Dermatology). Understand the pediatrician's role in preventing illness and dysfunction related
Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada. Catherine Zip Nov 10, 2016
 Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada Catherine Zip Nov 10, 2016 Acne Acne Classification Type Comedonal Mild-to-moderate papulopustular acne Severe Description
Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada Catherine Zip Nov 10, 2016 Acne Acne Classification Type Comedonal Mild-to-moderate papulopustular acne Severe Description
ACNE VULGARIS: DIAGNOSIS AND TREATMENT
 ACNE VULGARIS: DIAGNOSIS AND TREATMENT Federal Bureau of Prisons Clinical Guidance DECEMBER 2017 Clinical guidance is made available to the public for informational purposes only. The Federal Bureau of
ACNE VULGARIS: DIAGNOSIS AND TREATMENT Federal Bureau of Prisons Clinical Guidance DECEMBER 2017 Clinical guidance is made available to the public for informational purposes only. The Federal Bureau of
Diagnosis And Treatment Of Seborrheic Dermatitis
 Diagnosis And Treatment Of Seborrheic Dermatitis 1 / 5 2 / 5 3 / 5 Diagnosis And Treatment Of Seborrheic Seborrheic dermatitis Diagnosis. Your doctor will likely be able to determine whether you have seborrheic
Diagnosis And Treatment Of Seborrheic Dermatitis 1 / 5 2 / 5 3 / 5 Diagnosis And Treatment Of Seborrheic Seborrheic dermatitis Diagnosis. Your doctor will likely be able to determine whether you have seborrheic
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
PHARMACY PRACTICE I PHCY280 (2 CREDITS); PHCY280L (1CREDIT) SUMMER Christy Mary Sam
; PHCY280L (1CREDIT) SUMMER Christy Mary Sam") PHARMACY PRACTICE I PHCY280 (2 CREDITS); PHCY280L (1CREDIT) SUMMER 2014-15 1 Christy Mary Sam COMMUNICATION SKILLS Communication is the process involved with the exchange of any kind of information between
PHARMACY PRACTICE I PHCY280 (2 CREDITS); PHCY280L (1CREDIT) SUMMER 2014-15 1 Christy Mary Sam COMMUNICATION SKILLS Communication is the process involved with the exchange of any kind of information between
RASHES- Dermatitis nonspecific term for inflammation of the skin. 1. ECZEMA Atopic Dermatitis- specific form of eczema starting in childhood
 COMMON CHILDHOOD SKIN DISEASES Sharon Seguin MD Dermatology- Confluence Health Wenatchee Rashes Infections and Infestations RASHES- Dermatitis nonspecific term for inflammation of the skin 1. ECZEMA Atopic
COMMON CHILDHOOD SKIN DISEASES Sharon Seguin MD Dermatology- Confluence Health Wenatchee Rashes Infections and Infestations RASHES- Dermatitis nonspecific term for inflammation of the skin 1. ECZEMA Atopic
My Algorithm. Questions to ask. Do you or your family have a history of?... Allergic rhinitis, Sensitive skin, Asthma Skin Cancer
 Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Acne vulgaris is a disease of the pilosebaceous unit (i.e., the sebaceous glands and adjacent hair follicle).
.") Dr. Ghassan Salah Acne is a common, chronic inflammatory disorder of the pilosebaceous unit in which a microcomedo develops as the initial condition. The most common form of acne is acne vulgaris. Other
Dr. Ghassan Salah Acne is a common, chronic inflammatory disorder of the pilosebaceous unit in which a microcomedo develops as the initial condition. The most common form of acne is acne vulgaris. Other
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level
 Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Treatments used Topical including cleansers and moisturizer Oral medications:
 Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Case Studies From econsults Lessons Learned
 Case Studies From econsults Lessons Learned Karolyn (Kari) Wanat, MD Department of Dermatology and Pathology University of Iowa karolyn-wanat@uiowa.edu econsults Health care innovation award for controlled
Case Studies From econsults Lessons Learned Karolyn (Kari) Wanat, MD Department of Dermatology and Pathology University of Iowa karolyn-wanat@uiowa.edu econsults Health care innovation award for controlled
Clinico Pathological Test SCPA605-Essential Pathology
 Clinico Pathological Test SCPA605-Essential Pathology Somphong Narkpinit, M.D. Department of Pathogbiology, Faculty of Science, Mahidol University e-mail : somphong.nar@mahidol.ac.th Pathogenesis of allergic
Clinico Pathological Test SCPA605-Essential Pathology Somphong Narkpinit, M.D. Department of Pathogbiology, Faculty of Science, Mahidol University e-mail : somphong.nar@mahidol.ac.th Pathogenesis of allergic
Dermatology for the PCP
 Dermatology for the PCP Laura S. Winterfield, MD MPH Associate Professor Medical University of South Carolina I have no relevant conflicts of interest. 1 Learning Objectives Identify common skin conditions
Dermatology for the PCP Laura S. Winterfield, MD MPH Associate Professor Medical University of South Carolina I have no relevant conflicts of interest. 1 Learning Objectives Identify common skin conditions
F r e q u e n t l y A s k e d Q u e s t i o n s
 Acne who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. Q: What is acne? A: Acne is a disorder that causes outbreaks of skin lesions commonly
Acne who specializes in treating skin problems) about how you can help prevent acne and if treatment would help you. Q: What is acne? A: Acne is a disorder that causes outbreaks of skin lesions commonly
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
Commonly Coded Conditions in Dermatology
 Commonly Coded Conditions in Dermatology No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or mechanically, including photocopying,
Commonly Coded Conditions in Dermatology No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or mechanically, including photocopying,
Atopic Eczema with detail on how to apply wet wraps
 Atopic Eczema with detail on how to apply wet wraps Dr Carol Hlela Consultant Dermatologist Head of Unit, Department of Dermatology, Paediatrics Red Cross Children s Hospital, UCT Red Cross War Memorial
Atopic Eczema with detail on how to apply wet wraps Dr Carol Hlela Consultant Dermatologist Head of Unit, Department of Dermatology, Paediatrics Red Cross Children s Hospital, UCT Red Cross War Memorial
Interesting Cases in Dermatology: Clinical Pearls for Primary Care Providers
 Interesting Cases in Dermatology: Clinical Pearls for Primary Care Providers 26 th Annual Southwestern Conference on Medicine Tucson, Arizona Friday, April 28 th, 2017 Shannon C. Trotter DO, FAOCD, FAAD
Interesting Cases in Dermatology: Clinical Pearls for Primary Care Providers 26 th Annual Southwestern Conference on Medicine Tucson, Arizona Friday, April 28 th, 2017 Shannon C. Trotter DO, FAOCD, FAAD
Cutaneous reactions to targeted therapies. Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017
 Cutaneous reactions to targeted therapies Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017 Disclosures I have no relevant disclosures Papulopustular Eruption
Cutaneous reactions to targeted therapies Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017 Disclosures I have no relevant disclosures Papulopustular Eruption
ACNE. What are the aims of this leaflet?
 ACNE What are the aims of this leaflet? This leaflet has been written to help you understand more about acne - what it is, what causes it, what can be done about it and where you can find out more about
ACNE What are the aims of this leaflet? This leaflet has been written to help you understand more about acne - what it is, what causes it, what can be done about it and where you can find out more about
Teledermatology. Acne. What the primary care physician needs to know in the world of increased access
 Teledermatology What the primary care physician needs to know in the world of increased access Toby Maurer, MD University of California, San Francisco In the world of dermatology-teledermatology is powering
Teledermatology What the primary care physician needs to know in the world of increased access Toby Maurer, MD University of California, San Francisco In the world of dermatology-teledermatology is powering
Issues in Dermatology. Rhonda Lesniak, PhD, ARNP, FNP-BC, NCSN
 Issues in Dermatology Rhonda Lesniak, PhD, ARNP, FNP-BC, NCSN Anatomy of the Skin Functions Protect Fluid balance Absorption Synthesis of Vitamin D Sensation/communication with external environment Thermoregulation
Issues in Dermatology Rhonda Lesniak, PhD, ARNP, FNP-BC, NCSN Anatomy of the Skin Functions Protect Fluid balance Absorption Synthesis of Vitamin D Sensation/communication with external environment Thermoregulation
Objectives. 1. Recognizing benign skin lesions. 2.Know which patients will likely need surgical intervention.
 The Joy of Pediatric Skin Dr. Claire Sanger University of Kentucky Plastic & Reconstructive Surgery Objectives 1. Recognizing benign skin lesions 2.Know which patients will likely need surgical intervention.
The Joy of Pediatric Skin Dr. Claire Sanger University of Kentucky Plastic & Reconstructive Surgery Objectives 1. Recognizing benign skin lesions 2.Know which patients will likely need surgical intervention.
Common Skin Diseases. MdAhadAli Khan Department of Pharmacy SUB
 Common Skin Diseases MdAhadAli Khan Department of Pharmacy SUB Intact: Skin is unbroken Contusion: Injury in which skin is unbroken Excoriation: Removal of an area of the skin Abrasion: Spot rubbed bare
Common Skin Diseases MdAhadAli Khan Department of Pharmacy SUB Intact: Skin is unbroken Contusion: Injury in which skin is unbroken Excoriation: Removal of an area of the skin Abrasion: Spot rubbed bare
Psoriasis. What is Psoriasis? What causes psoriasis? Medical Topics Psoriasis
 1 Psoriasis What is Psoriasis? Psoriasis is a long standing inflammatory non-contagious skin disease which waxes and wanes with triggering factors. There is a genetic predisposition in psoriasis. Internationally,
1 Psoriasis What is Psoriasis? Psoriasis is a long standing inflammatory non-contagious skin disease which waxes and wanes with triggering factors. There is a genetic predisposition in psoriasis. Internationally,
Psoriasis: Causes, Symptoms, And Treatment
 Psoriasis: Causes, Symptoms, And Treatment We all know that a healthy immune system is good. But, do you know that an overactive immune system can cause certain conditions like Psoriasis? Read on to find
Psoriasis: Causes, Symptoms, And Treatment We all know that a healthy immune system is good. But, do you know that an overactive immune system can cause certain conditions like Psoriasis? Read on to find
Eczema. By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University
 Eczema By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University Dermatitis= Eczema =Spongiosis Eczema Atopic Seborrheic Contact Allergic Irritant Nummular Asteatotic Stasis Neurodermatitis/Lichen Simplex
Eczema By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University Dermatitis= Eczema =Spongiosis Eczema Atopic Seborrheic Contact Allergic Irritant Nummular Asteatotic Stasis Neurodermatitis/Lichen Simplex
Dermatology elective for yr. 5. Natta Rajatanavin, MD. Div. of dermatology Dep. Of Medicine, Ramathibodi Hospital Mahidol University 23 rd Feb 2015
 Dermatology elective for yr. 5 Natta Rajatanavin, MD. Div. of dermatology Dep. Of Medicine, Ramathibodi Hospital Mahidol University 23 rd Feb 2015 How to diagnosis and manage eczema and psoriasis. Objectives
Dermatology elective for yr. 5 Natta Rajatanavin, MD. Div. of dermatology Dep. Of Medicine, Ramathibodi Hospital Mahidol University 23 rd Feb 2015 How to diagnosis and manage eczema and psoriasis. Objectives
X-Plain Acne Reference Summary
 X-Plain Acne Reference Summary Nearly 17 million people in the United States have acne, making it one of the most common skin diseases in the USA. Although acne is not a serious health threat, severe acne
X-Plain Acne Reference Summary Nearly 17 million people in the United States have acne, making it one of the most common skin diseases in the USA. Although acne is not a serious health threat, severe acne
INFLAMMATORY BOWEL DISEASE AND SKIN HEALTH KARA N. SHAH, MD, PHD KENWOOD DERMATOLOGY MARCH 4, 2018
 INFLAMMATORY BOWEL DISEASE AND SKIN HEALTH KARA N. SHAH, MD, PHD KENWOOD DERMATOLOGY MARCH 4, 2018 DISCLOSURES I HAVE NO RELEVANT FINANCIAL DISCLOSURES INTRODUCTION Structure and function of the skin IBD
INFLAMMATORY BOWEL DISEASE AND SKIN HEALTH KARA N. SHAH, MD, PHD KENWOOD DERMATOLOGY MARCH 4, 2018 DISCLOSURES I HAVE NO RELEVANT FINANCIAL DISCLOSURES INTRODUCTION Structure and function of the skin IBD
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Facial Rash. Facial Rash 10/14/2013. Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program
 Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program Facial Rash Facial Rash Case 1 28 year female Progressive development of erythematous facial lesions
Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program Facial Rash Facial Rash Case 1 28 year female Progressive development of erythematous facial lesions
Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD)
") Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
Diagnosis: ATOPIC DERMATITIS (AD) Texas Children's Hospital Dermatology Service PCP Referral Guidelines- Atopic Dermatitis (AD) PATIENT ADVICE: Unfortunately, there is no cure for atopic dermatitis, so
Common Superficial Fungal Infections
 How to recognise and treat Common Superficial Fungal Infections Dr Lilianne Scholtz (MBBCh) Types of superficial fungal infections Ringworm (Tinea) Candida (Thrush) Body Groin Feet Skin Nappy rash Vagina
How to recognise and treat Common Superficial Fungal Infections Dr Lilianne Scholtz (MBBCh) Types of superficial fungal infections Ringworm (Tinea) Candida (Thrush) Body Groin Feet Skin Nappy rash Vagina
Rash Decisions Approach to the patient with a skin condition
 National Conference for Nurse Practitioners April 25, 2014 Rash Decisions Approach to the patient with a skin condition Margaret A. Bobonich, DNP, FNP C, DCNP, FAANP Assistant Professor, Case Western Reserve
National Conference for Nurse Practitioners April 25, 2014 Rash Decisions Approach to the patient with a skin condition Margaret A. Bobonich, DNP, FNP C, DCNP, FAANP Assistant Professor, Case Western Reserve
Recognizing common Dermatologic conditions. Case presentations. CAPA 2015 Annual Conference. Tanya Nino, MD St. Joseph Heritage Medical Group
 Recognizing common Dermatologic conditions Tanya Nino, MD St. Joseph Heritage Medical Group Case presentations 65 year old female referred for rule out melanoma a lesion on back 30 year old female has
Recognizing common Dermatologic conditions Tanya Nino, MD St. Joseph Heritage Medical Group Case presentations 65 year old female referred for rule out melanoma a lesion on back 30 year old female has
Eczema & Dermatitis Clinical features: Histopathological features: Classification:
 Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Eczema & Dermatitis Eczema is an inflammatory reactive pattern of skin to many and different stimuli characterized by itching, redness, scaling and clustered papulovesicles. Eczema and dermatitis are synonymous
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
The Itch That Rashes. Sarah D. Cipriano, MD, MPH, MS Resident, Dermatology University of Utah
 The Itch That Rashes Sarah D. Cipriano, MD, MPH, MS Resident, Dermatology University of Utah 1 Conflict of Interest No conflict of interest Will discuss off label use of medications 2 3 Most likely diagnosis?
The Itch That Rashes Sarah D. Cipriano, MD, MPH, MS Resident, Dermatology University of Utah 1 Conflict of Interest No conflict of interest Will discuss off label use of medications 2 3 Most likely diagnosis?
PROCEEDINGS PRACTICAL APPLICATIONS: CASE STUDY REVIEWS* Bernard A. Cohen, MD, FAAP
 PRACTICAL APPLICATIONS: CASE STUDY REVIEWS* Bernard A. Cohen, MD, FAAP A HEALTHY 4-WEEK-OLD INFANT WITH ACNE A 4-week-old infant was brought to the pediatrician s office by his parents following the appearance
PRACTICAL APPLICATIONS: CASE STUDY REVIEWS* Bernard A. Cohen, MD, FAAP A HEALTHY 4-WEEK-OLD INFANT WITH ACNE A 4-week-old infant was brought to the pediatrician s office by his parents following the appearance
GROUP 15 TOPICAL PREPARATIONS
 - 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
- 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
The Integumentary System. Disorders, Conditions, and Diseases
 The Integumentary System Disorders, Conditions, and Diseases Definitions Disease- an abnormal condition of the body or the mind that causes dysfunction or discomfort. Disorder- a functional abnormality,
The Integumentary System Disorders, Conditions, and Diseases Definitions Disease- an abnormal condition of the body or the mind that causes dysfunction or discomfort. Disorder- a functional abnormality,
Top 10 Skin Problems
 THE UK GUIDE Top 10 Skin Problems Learn how a Dermatologist can solve your frustrating challenges with skin, scalp, hair and nails Jennifer Crawley MBChB, BSc (Hons), MRCP (Derm) BAD British Association
THE UK GUIDE Top 10 Skin Problems Learn how a Dermatologist can solve your frustrating challenges with skin, scalp, hair and nails Jennifer Crawley MBChB, BSc (Hons), MRCP (Derm) BAD British Association
Dermatology GP Referral Guidelines
 Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
(5). (1, 5) Table 1:Appearance and location of dandruff, psoriasis and seborrhoeic dermatitis
. (1, 5) Table 1:Appearance and location of dandruff, psoriasis and seborrhoeic dermatitis") A-Dandruff(pityriasis capitis) 1-Dandruff is a chronic relapsing condition of the scalp which respond to treatment, but return when the treatment is stopped (1). Increased cell turnover rate (twice the
A-Dandruff(pityriasis capitis) 1-Dandruff is a chronic relapsing condition of the scalp which respond to treatment, but return when the treatment is stopped (1). Increased cell turnover rate (twice the
Disclosures. Poll Everywhere. Learning Objectives. Atopic Dermatitis. Atopic Dermatitis
 39 th National Conference on Pediatric Health Care March 19-22, 2018 CHICAGO Disclosures When It s Not Eczema: Reviewing common and not so common differential diagnosis for Atopic Dermatitis No disclosures
39 th National Conference on Pediatric Health Care March 19-22, 2018 CHICAGO Disclosures When It s Not Eczema: Reviewing common and not so common differential diagnosis for Atopic Dermatitis No disclosures
Identifying and managing dermatologic toxicities associated with EGFR-inhibitor therapy. An educational resource for healthcare professionals
 Identifying and managing dermatologic toxicities associated with EGFR-inhibitor therapy An educational resource for healthcare professionals What to expect from EGFR-inhibitor therapy The goal of EGFR-inhibitor
Identifying and managing dermatologic toxicities associated with EGFR-inhibitor therapy An educational resource for healthcare professionals What to expect from EGFR-inhibitor therapy The goal of EGFR-inhibitor
Tinea: Head to Toe A dermatophyte tour of human skin. Tour de Tinea Head to Toe. Tips for Tinea Head to Toe. Psoriasis. Non-inflammatory Tinea Capitis
 Tinea: Head to Toe A dermatophyte tour of human skin Renee Howard, MD Assistant Clinical Professor of Dermatology, UCSF Tour de Tinea Head to Toe Tips for Tinea Head to Toe Capitis Faciei Corporis Pedis
Tinea: Head to Toe A dermatophyte tour of human skin Renee Howard, MD Assistant Clinical Professor of Dermatology, UCSF Tour de Tinea Head to Toe Tips for Tinea Head to Toe Capitis Faciei Corporis Pedis
Molluscum Contagiosum in Adults & Kids
 How to care for Molluscum Contagiosum in Adults & Kids 1 e-book edition 2 TOPICS Common Treatments for Molluscum Contagiosum How to Stop Molluscum Contagiosum from Spreading to Other Parts of Your Body
How to care for Molluscum Contagiosum in Adults & Kids 1 e-book edition 2 TOPICS Common Treatments for Molluscum Contagiosum How to Stop Molluscum Contagiosum from Spreading to Other Parts of Your Body
(NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122)
") (NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122) Bacteria Bacteria are microscopic, single-celled forms of plant life, containing no chlorophyll. They live on the skin, on the surface of the stratum
(NATO STANAG 2122, CENTO STANAG 2122, SEATO STANAG 2122) Bacteria Bacteria are microscopic, single-celled forms of plant life, containing no chlorophyll. They live on the skin, on the surface of the stratum
Integumentary System
 Integumentary System Integumentary System Skin, hair, and nails. Skin: Epidermis: outer layer. Dermis: also called corium, or true skin. Subcutaneous fascia: innermost layer. Integumentary Glands Sudoriferous:
Integumentary System Integumentary System Skin, hair, and nails. Skin: Epidermis: outer layer. Dermis: also called corium, or true skin. Subcutaneous fascia: innermost layer. Integumentary Glands Sudoriferous:
Therapeutic Agents for the Dermatological System
 Therapeutic Agents for the Dermatological System Chapter 25 1 Anatomy of the Skin Skin is made of various layers that contain nerves, glands, hair, and blood vessels Function is to protect the body against
Therapeutic Agents for the Dermatological System Chapter 25 1 Anatomy of the Skin Skin is made of various layers that contain nerves, glands, hair, and blood vessels Function is to protect the body against
Panel: Practice Pearls from the Pros. Prescription Medication: Office Protocols. Kathy Jones, BSN, RN, CPSN
 24TH Annual Meeting Panel: Practice Pearls from the Pros Prescription Medication: Office Protocols Kathy Jones, BSN, RN, CPSN Upon completion of this presentation, the participants will self-report an
24TH Annual Meeting Panel: Practice Pearls from the Pros Prescription Medication: Office Protocols Kathy Jones, BSN, RN, CPSN Upon completion of this presentation, the participants will self-report an
Skin Deep: Or is It? Practical Pearls from a Pediatric Dermatologist
 Skin Deep: Or is It? Practical Pearls from a Pediatric Dermatologist I have no conflicts of interest 6 yo boy referred for AD. On topical HC and food elimination diet s/p topical triamcinolone to body
Skin Deep: Or is It? Practical Pearls from a Pediatric Dermatologist I have no conflicts of interest 6 yo boy referred for AD. On topical HC and food elimination diet s/p topical triamcinolone to body
Review Acne Pathogenesis Clinical Evaluation Treatment Guidelines
 Tiffany Herd, MD Pediatric Dermatology Fellow Baylor College of Medicine/Texas Children's Hospital Review Acne Pathogenesis Clinical Evaluation Treatment Guidelines Psychosocial Impact of Acne Acne is
Tiffany Herd, MD Pediatric Dermatology Fellow Baylor College of Medicine/Texas Children's Hospital Review Acne Pathogenesis Clinical Evaluation Treatment Guidelines Psychosocial Impact of Acne Acne is
Thursday 21 st August Skin Problems
 Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
4 th Annual SKIN: Practical Dermatology for the Generalist Program Schedule
 4 th Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
4 th Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
Disclosures. Outline. Goals of this lecture. Common Dermatologic Disorders: Tips for Diagnosis and Management Part 2 3/26/2014
 Common Dermatologic Disorders: Tips for Diagnosis and Management Part 2 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service
Common Dermatologic Disorders: Tips for Diagnosis and Management Part 2 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service
Derm quiz. Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52. bit.ly/2a8asoy. Scan the QR code with your phone
 Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Index. derm.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abnormal wound healing Acne and cybereducation, 131 and Google, 129 131 and online dangers, 131, 132 reliable online resources on, 130 self-proclaimed
Note: Page numbers of article titles are in boldface type. A Abnormal wound healing Acne and cybereducation, 131 and Google, 129 131 and online dangers, 131, 132 reliable online resources on, 130 self-proclaimed
Common Skin Diseases. Md Ahad Ali Khan Department of Pharmacy SUB
 Common Skin Diseases Md Ahad Ali Khan Department of Pharmacy SUB Intact: Skin is unbroken Contusion: Injury in which skin is unbroken Excoriation: Removal of an area of the skin Abrasion: Spot rubbed bare
Common Skin Diseases Md Ahad Ali Khan Department of Pharmacy SUB Intact: Skin is unbroken Contusion: Injury in which skin is unbroken Excoriation: Removal of an area of the skin Abrasion: Spot rubbed bare
9/9/17. Disclosures" Dermatology in Primary Care: Recognition and treatment of common disorders of the skin" A preview" Classic skin infections"
 Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
ATOPIC DERMATITIS: A BLUEPRINT FOR SUCCESS. Sierra Wolter MD, FAAD Pediatric Dermatology University of Arizona, College of Medicine
 ATOPIC DERMATITIS: A BLUEPRINT FOR SUCCESS Sierra Wolter MD, FAAD Pediatric Dermatology University of Arizona, College of Medicine THE PLAN Is it atopic dermatitis? What is atopic dermatitis? Guidelines
ATOPIC DERMATITIS: A BLUEPRINT FOR SUCCESS Sierra Wolter MD, FAAD Pediatric Dermatology University of Arizona, College of Medicine THE PLAN Is it atopic dermatitis? What is atopic dermatitis? Guidelines
3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule
 3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
HIDRADENITIS SUPPURATIVA
 Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright 2004-2005 The McGraw-Hill Companies. All rights reserved. Fitzpatrick Color Atlas, 5e
Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright 2004-2005 The McGraw-Hill Companies. All rights reserved. Fitzpatrick Color Atlas, 5e
LNE & Spa the magazine for skin care and spa professionals December 2017 $7.50
 LNE & Spa the magazine for skin care and spa professionals December 2017 $7.50 18 December2017 LNEonline.com Psoriasis Spa Therapy Calm your clients sensitive skin with these psoriasis spa therapy tips
LNE & Spa the magazine for skin care and spa professionals December 2017 $7.50 18 December2017 LNEonline.com Psoriasis Spa Therapy Calm your clients sensitive skin with these psoriasis spa therapy tips
What s causing this rash?
 Case 1 What s causing this rash? A 38-year-old woman presents with a pruritic, tender rash on the trunk and extremities that has not changed over the past few days (Figure 1). She has taken fluvastatin
Case 1 What s causing this rash? A 38-year-old woman presents with a pruritic, tender rash on the trunk and extremities that has not changed over the past few days (Figure 1). She has taken fluvastatin
Can You Take a Look at This? Objectives 4/18/12. Shane Scott, DO Internal Medicine & Pediatrics The
 Can You Take a Look at This? Shane Scott, DO Internal Medicine & Pediatrics The Objectives! Identify Common Presentations of Rashes in the Pediatric Patient! Decide if the rash is Communicable! Decide
Can You Take a Look at This? Shane Scott, DO Internal Medicine & Pediatrics The Objectives! Identify Common Presentations of Rashes in the Pediatric Patient! Decide if the rash is Communicable! Decide
Didactic Series. Dermatologic Manifestations Associated with HIV/AIDS. Ankita Kadakia, MD UCSD Owen Clinic 12/11/2014
 Didactic Series Dermatologic Manifestations Associated with HIV/AIDS Ankita Kadakia, MD UCSD Owen Clinic 12/11/2014 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited
Didactic Series Dermatologic Manifestations Associated with HIV/AIDS Ankita Kadakia, MD UCSD Owen Clinic 12/11/2014 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited
Conflicts of interest
 Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Chapter 29. Learning Objectives. Learning Objectives (Cont d) 9/10/2012. Cutaneous Disorders
 9/10/2012. Cutaneous Disorders") Chapter 29 Cutaneous Disorders Learning Objectives Describe the three layers of skin, and their composition and functions Describe the morphology of primary skin lesions Describe the morphology of secondary
Chapter 29 Cutaneous Disorders Learning Objectives Describe the three layers of skin, and their composition and functions Describe the morphology of primary skin lesions Describe the morphology of secondary
Can steroids cause rash on arms
 Can steroids cause rash on arms Prednisone is a steroid that may be used to treat cancer. This drug is. Skin reactions such as rash, acne, facial redness, reddish-purple lines on the skin, or shiny skin..
Can steroids cause rash on arms Prednisone is a steroid that may be used to treat cancer. This drug is. Skin reactions such as rash, acne, facial redness, reddish-purple lines on the skin, or shiny skin..
Acne Workshop Pediatric Acne: What s Erupting? AZAAP. Marcia Hogeling, MD, FAAD, FAAP
 Acne Workshop Pediatric Acne: What s Erupting? AZAAP Marcia Hogeling, MD, FAAD, FAAP Disclosures Advisory Board Leo Pharma & Anacor Off label use of acne medicines Objectives Diagnose comedonal, inflammatory
Acne Workshop Pediatric Acne: What s Erupting? AZAAP Marcia Hogeling, MD, FAAD, FAAP Disclosures Advisory Board Leo Pharma & Anacor Off label use of acne medicines Objectives Diagnose comedonal, inflammatory
3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule
 3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
3rd Annual SKIN: Practical Dermatology for the Generalist Program Schedule PHARMACOLOGY CONTENT Select presentations will contain pharmacology content as noted in the program. Identified presentations
29a Pathology - Integumentary System
 29a Pathology - Integumentary System 29a Pathology - Integumentary System! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders 10 minutes Lecture: 25 minutes Lecture: 15 minutes Active
29a Pathology - Integumentary System 29a Pathology - Integumentary System! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders 10 minutes Lecture: 25 minutes Lecture: 15 minutes Active
Richard Turner Consultant Dermatologist
 Old Problems & New Treatments Photo Album by Administrator Richard Turner Consultant Dermatologist Plan for tonight? Refresher on SCC and solar keratosis How to distinguish the two Classic therapy than
Old Problems & New Treatments Photo Album by Administrator Richard Turner Consultant Dermatologist Plan for tonight? Refresher on SCC and solar keratosis How to distinguish the two Classic therapy than
Dermatology. Women and Children s Services
 Women and Children s Services Dermatology Disclaimer: The recommendations contained in this guideline do not indicate an exclusive course of action, or serve as a standard of medical care. Variations,
Women and Children s Services Dermatology Disclaimer: The recommendations contained in this guideline do not indicate an exclusive course of action, or serve as a standard of medical care. Variations,
COMMON SKIN INFECTIONS. Sports Medicine
 COMMON SKIN INFECTIONS Sports Medicine IMPETIGO IS A SUPERFICIAL BACTERIAL INFECTION CAUSED BY: STREPTOCOCCI OR STAPHYLOCOCCUS AUREUS BOULOUS IMPETIGO IMPETIGO COMES IN TWO FORMS: BOULOUS OR NON- BOULOUS
COMMON SKIN INFECTIONS Sports Medicine IMPETIGO IS A SUPERFICIAL BACTERIAL INFECTION CAUSED BY: STREPTOCOCCI OR STAPHYLOCOCCUS AUREUS BOULOUS IMPETIGO IMPETIGO COMES IN TWO FORMS: BOULOUS OR NON- BOULOUS
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Site and distribution: symmetrical, asymmetrical. Surface characteristics: smooth, scaly, warty
 B I O T E R R O R I S M PRINCIPLES AND PRACTICE OF DERMATOLOGY Dr Matthew Ng Joo Ming INTRODUCTION Medical schools and textbooks teach us dermatology by subjects such as eczema and psoriasis. This is useful
B I O T E R R O R I S M PRINCIPLES AND PRACTICE OF DERMATOLOGY Dr Matthew Ng Joo Ming INTRODUCTION Medical schools and textbooks teach us dermatology by subjects such as eczema and psoriasis. This is useful