Hospital Dermatology: Pearls and Pitfalls
|
|
|
- Christian Wilkins
- 6 years ago
- Views:
Transcription

1 Hospital Dermatology: Pearls and Pitfalls Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship ASDP Alternate Advisor to the AMA-RUC Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo Clinic, Rochester
2 Disclosures Relevant Financial Relationships None Off Label Usage Yes
3 What is Hospital Dermatology? Long-standing unique tradition at Mayo, a tertiary care center with a large referral service We preserved and improved on the quality of care rendered our patients with difficult skin diseases in our hospital program Hospital core group Clinical Division MDP Davis, R El Azhary, D. Wetter, M McEvoy, J Sartori Laboratory Division AG Bridges, MC Camilleri
4 Role of Dermatology Hospitalist Hospitalist Inpatient Dermatology Lymphoma, Autoimmune bullous disorders, Ulcers, PG, Calciphylaxis, Vasculitis, CTD, Erythroderma, Generalized dermatitis, Hypersensitivity reactions, Cellulitis, Psoriasis Outpatient - Hospital based Psoriasis Goeckerman Phototherapy Consult Service Pediatrics/Neonatal medicine, Drug eruptions, GVHD, Dermatitis, Lesions, Vasculitis/vasculopathy, Autoimmune diseases, Infection, Ulcers, Lymphoma
5 Pearls and Pitfalls of Hospital Dermatology Goals of this lecture Review clinical and histopathological presentations, differential diagnosis, evaluation and management of major categories of dermatologic diseases in hospitalized patients 1. Help! Red and Scaly All Over 2. I itch and nothing helps! 3. I think it s a drug eruption. Now what do I do? 4. Bugs What bugs you? 5. Oh no! The patient has purpura 6. Yikes! The flesh eating ulcer
6 HELP! Red and Scaly All Over

7 91 year old woman admitted to Ortho for left hip replacement HTN, hyperlipidemia, GERD and dermatitis Worsening dermatitis for 3 months Hip replacement cancelled Admitted to Derm service 2011 MFMER slide-7



8 2011 MFMER slide-8


9

10 2011 MFMER slide-10
 C. Psoriasis D.")
11 What is your diagnosis? A. Dermatitis B. Pityriasis Rubra Pilaris (PRP) C. Psoriasis D. Drug reaction E. Lymphoma

12 2011 MFMER slide-12

13 2011 MFMER slide-13


14 CD4 CD7
15 Sézary syndrome Clonal T-cell receptor gene rearrangement detected in skin biopsy Lymphadenopathy Convoluted lymphocytes on peripheral smear Patient declined aggressive management and methotrexate initiated up to 25mg weekly
16 Psoriasis Erythroderma Pityriasis rubra pilaris Dermatitis Drug eruption Lymphoma Infection Autoimmune bullous disorder



17 I itch and nothing helps!!
18 54 y/o F with severe pruritic eruption x 1.5 years Admitted to Dermatology inpatient service for wet dressings Outside skin biopsies non-specific dermatitis DIF? DH (negative anti-gliadin and TTG antibodies, duodenum biopsy negative for celiac disease) Prior treatments: - Topical corticosteroids (poor response) - Dapsone gel (poor response) - UVB (some benefit) - Dapsone 50 mg QD x 8 months (initially helpful) - Systemic corticosteroids ( 30 day course w/ taper) - Hydroxyzine and doxepin (some benefit)




19

20 2011 MFMER slide-20
21 What is your diagnosis? A. Scabies B. Prurigo Nodularis C. Dermatitis Herpetiformis D. Bullous Pemphigoid E. Lymphoma
22 Pruritus Evaluation Normal or negative: CBC, peripheral smear, ESR, SPEP, IgA, IgM, IgG, TSH, ANA, gliadin Ab, endomysial Ab, TTG, Hep B/C, HIV, CXR AST 51 and ALT 111: known steatohepatitis Skin swab: Methicillin sensitive Staph aureus Biopsies for H&E and DIF obtained

")

23 DIF: Linear deposition of IgG along BMZ IIF: 1:640 BMZ titer on monkey esophagus with epidermal pattern on salt-split skin Elevated BP180 (90) and BP230 (90) Final diagnosis: Bullous pemphigoid (pemphigoid nodularis)
24 Pearl: Atypical presentations of bullous pemphigoid 20% non-bullous Eczematous, dyshidrosiform, urticarial, erythrodermic, nodular, lichenoid, or targetoid Include evaluation for autoimmune bullous disorders in erythroderma and pruritus work-up
25 Pruritus Xerosis Dermatitis Hypersensitivity reaction Dermatophytosis Folliculitis Scabies Autoimmune bullous disease Liver disease Renal disease Thyroid disease Anemia Lymphoproliferative disorders

26 I think it s a drug eruption. Now what do I do?
27 Drug Eruptions Simple Complex Other No systemic symptoms Systemic involvement Life threatening Morbilliform Urticarial Drug hypersensitivity reaction Stevens-Johnson syndrome (SJS) Toxic epidermal necrolysis (TEN)
28 Drug Reactions 3 things you need to know 1. Type of drug reaction 2. Statistics What drugs are most likely to cause that type of reaction? 3. Timing How long after the drug was started did the reaction begin?
29 Drug Timeline Patient Name: Clinic Number: DATES % Rxn RASH Reaction Type for Drug Drug 2/5 Morbilliform ASA x x x x x x x x x x x x x x x x Urticarial Colace x x x x x x Fixed Drug Bactrim x x x x Erythroderma Tetracycline x x x x x x EM PCN x x x x x x SJS Vancomycin x x x x x x TEN HCTZ x x x x x x x AGEP Dilantin x x x x x x x x x x DRESS Vasculitis LCV HSP Other Lupus-like Blistering Pemphigus LABD PseudoPCT Pseudolymphoma Cytotoxic OTHER UserName = Mayo1 Password = Physicians MR = Many Reports R = Reported NR = Not Reported
 C. Find out what drug was recently started and stop that drug D. Arrange for an urgent skin biopsy to find out what the rash is due to E.")
30 This patient is hospitalized for a pneumonia and has developed this pruritic eruption. What is the most important intervention that will lead to resolution of the rash? A. Topical corticosteroids B. Systemic Corticosteroids (prednisone mg/kg/day) C. Find out what drug was recently started and stop that drug D. Arrange for an urgent skin biopsy to find out what the rash is due to E. Oral antihistamines
31 Clinical Pearls Drug eruptions are extremely common Tend to be generalized Maculopapular/morbilliform most common Best intervention: Stop the offending drug How to spot the culprit? Drug started within days to a week prior to rash Can be difficult! Tip: can generally exclude all drugs started after onset of rash! Drug eruptions can continue for 1-2 weeks even after stopping culprit drug
32 CASE

33 Patient just admitted BP 80/50 mmhg Your diagnosis?

34

35 TEN epidermal necrosis & dermal infiltrate compared to SJS

36 TEN Most severe presentation in spectrum which includes EM & SJS Generalized erythema, purpura & flaccid bullae Widespread epidermal detachment 10% of BSA Extensive mucous membrane involvement No target lesions
37 Drug-related TEN/SJS Extracutaneous involvement Fever Leukopenia Poor prognostic factor Involvement of GI, renal & respiratory mucosa
38 TEN/SJS Drug-related Sulfonamides Slow acetylator phenotype Anticonvulsants Dilantin, phenobarbital, carbamazepine, lamotrigine Penicillin derivatives NSAIDS Allopurinol


39 Target lesions SJS


40 SJS Generalized erythema or purpura <10% epidermal detachment


41 Extensive ulceration of oral, genital, &/or ocular mucous membranes ( 2 surfaces) SJS
42 TEN/SJS Bottom Line (Personal View) TEN/SJS are both associated with high mortality rates (up to 25%) from sepsis and multiorgan failure Require intensive supportive management in ICU/Burn unit Discontinue the causative drug or treat underlying infection Mycoplasma in 25% of pediatric patients with SJS Bulk of evidence Supports use of intravenous immunoglobulin 0.5-1gm/kg/d X 4 days IVIG blocks Fas mediated apoptosis in vitro and arrests development of TEN in vivo Does not support use of systemic corticosteroids Cyclosporine 3mg/kg X 10days, then 1 mg/kg X 10 days; go back up if you taper too quickly & the patient flares
43 CASE

44 33 yo F G1P1, 2 weeks postpartum Persistent, painful generalized eruption X 3 months Severe head, ear and mouth pain with dysphagia Reported NO medications Received systemic and topical steroids


45


46


47

48 2011 MFMER slide-48


49
50 What is your diagnosis? A. Scabies B. Drug reaction with eosinophilia and systemic disease (DRESS) C. Polymorphic eruption of pregnancy D. Connective tissue disease (CTD) E. Psoriasis F. Autoimmune bullous disorder
51 Laboratory evaluation Oral swab: + HSV-1 & Candida Cutaneous swab: MSSA Leukocytosis (18.9) with eosinophilia (4.47) aldolase, LDH, ALT, AST PCR HHV-6 negative CT chest/ abdomen/ pelvis B/L axillary & inguinal lymphadenopathy zinc TSH wnl EKG normal
52 Latent TB + PPD 7 months ago INH initiated Onset of rash 4 months later Rash persisted and 1 month later INH discontinued
53 Hospital course 3 consecutive days high dose methylprednisolone (1.5 gm/day) followed by transition to prednisone Mycophenolate mofetil and IVIG aldolase, LDH, LFTs, eosinophils Improvement in skin, symptoms

54 Drug Reaction with Eosinophilia and Systemic Symptoms DRESS Syndrome
55 AKA: DRESS Syndrome Anticonvulsant Hypersensitivity Syndrome Drug-induced Pseudolymphoma Drug-induced Hypersensitivity Syndrome Hypersensitivity syndrome Drug-induced Delayed Multiorgan Hypersensitivity Syndrome
56 DRESS Syndrome Severe, idiosyncratic drug reaction Commonly implicated drugs: anticonvulsants, sulfonamides, allopurinol, NSAIDS, azithromycin, azathioprine, and anti-retrovirals Most cases present after delay of 2-8 weeks, but onset has been reported from days after drug initiation Time to abnormally metabolize the drug leading to toxic drug metabolites Reactivation of HHV-6 has been observed
57 Clinical Features of DRESS Fever, leukocytosis, eosinophilia Huge variability in presentation Each class of drug causes a slightly different clinical picture Facial edema mimicking angioedema Generalized eruption: erythematous edematous papules, vesicles, bullae, pustules, purpura, target lesions and erythroderma
58 Clinical Features of DRESS Lymphadenopathy Myositis Liver function test abnormalities May result in severe hepatocellular or cholestatic damage, necessitating transplant 10% mortality typically from liver failure Variable lung, kidney, heart, thyroid involvement
59 Treatment of DRESS Withdrawal of offending medication Avoid cross-reacting medications High-dose systemic steroids mg/kg tapering dose over 1-3 months LFTs should be followed until resolved Supportive care ICU/Burn unit care is not required
60 Miscellaneous Drug Eruptions You Should Know About Acute generalized exanthematous pustulosis (AGEP) Linear IgA bullous dermatosis (LABD) Symmetric drug-related intertriginous and flexural exanthema (SDRIFE) TNF-alpha antagonist-induced lupuslike drug eruption/syndrome (TAILS)
61 CASE

62 31 year old woman admitted to Medicine 1 week history of generalized erythema and edema Following uncomplicated Caesarian delivery Given Clindamycin Tachycardia, leukocytosis, elevated ESR and CRP Systemic steroids given


63


64

65

66
67 Acute Generalized Exanthematous Pustulosis (AGEP) Also known as a pustular drug eruption Fever and leukocytosis with neutrophilia and eosinophilia are often present Many implicated drugs: macrolide & beta-lactam antibiotics, cephalosporins, tetracyclines, vancomycin, sulfonamides, carbamazepine, allopurinol, furosemide, antifungals, calcium channel blockers, ACE inhibitors, acetaminophen Sudden onset 2-5 days after drug started Begins on the face and intertriginous areas Disseminates in a few hours
68 Treatment of AGEP Discontinuation of drug Topical care Eruption usually resolves rapidly in 3-5 days with desquamation May be due to a specific T-cell reaction Neutrophils may be recruited by local cytokines
69 CASE

70 19-yo man with pruritic eruption Began shortly after starting vancomycin

71
72
73


74

75

76 DIF- Linear deposition of IgA along the BMZ
77 Drug-induced LABD Various clinical presentations Vesiculobullous eruption on trunk/extremities Herpetiform or rosette-like bullae Morbilliform, urticarial Can resemble DH, BP, CP, PV, LP, EM or TEN 40% with mucosal involvement
78 Drug-induced LABD Drug-induced Vancomycin most common drug Others: Penicillins, cephalosporins, captopril, trimethoprim/sulfamethoxazole, phenytoin, furosemide, glyburide, diclofenac Onset:3-14 days after exposure Target Ag- BPAg2 (BP180)
79 Drug-induced LABD Treatment Removal of the offending agent Dapsone, Sulfapyridine, Corticosteroids Dialysis
80 CASE

81 84 yo male 2 day intertriginous eruption On Levaquin, Cefepime, and Hydroxyzine

82 2011 MFMER slide-82

83 2011 MFMER slide-83
84 What is Your Diagnosis? A. Acute generalized exanthematous pustulosis (AGEP) B. Intertrigo C. Hailey-Hailey disease D. Cellulitis E. Symmetric drug-related intertriginous and flexural exanthema (SDRIFE)

85 2011 MFMER slide-85

86 2011 MFMER slide-86
87 Symmetric Drug-Related Intertriginous and Flexural Exanthema (SDRIFE) Diagnostic criteria Exposure to systemic drug predominantly aminopenicillins and B-lactams at first or repeated dose (contact allergens excluded) Erythema of the gluteal/perineal area Involvement of at least one other intertriginous/flexural localization Symmetry of the affected areas Absence of systemic symptoms and signs
88 CASE
89 18 year old female with juvenile RA in the MICU Fever, chills, hypotension, headache, N/V, fatigue, weakness Etanercept 0.98mL of 50 mg/ml SC weekly Started 1 year ago and last injection 4 wks ago Methotrexate 2.5 mg weekly Discontinued 8 wks ago Prednisone 5 mg qam Increased to 20 mg Started on amoxicillin 2 days after rash



90 2011 MFMER slide-90


91 2011 MFMER slide-91


92 2011 MFMER slide-92

93

94 2011 MFMER slide-94
95 The most likely diagnosis for this patient s skin eruption is: A. Stevens Johnson syndrome (SJS) B. Infectious mononucleosis from EBV C. Lupus erythematosus or lupus-like reaction secondary to etanercept D. Secondary syphilis E. DRESS (drug reaction with eosinophilia and systemic symptoms)
96 Pancytopenia Laboratory Evaluation Anemia and thrombocytopenia (3 months prior); leukopenia; normal peripheral smear; no eosinophilia Elevated ANA (>12) Elevated ds-dna (>1000) ENA: Elevated Scl70 Ab (1.8) Decreased Complement Total C (8), C4 (9) SPEP: Polyclonal hypergammaglobulinemia

97 Vacuolar interface dermatitis consistent with lupus-like reaction secondary to etanercept or LE
98 TNF-alpha Inhibitors Using more of these agents to treat chronic inflammatory diseases RA, AS, psoriasis, PsA, and IBD Infliximab Chimeric monoclonal Ab (IV) Etanercept Recombinant TNF-alpha soluble receptor fused to the Fc fragment of IgG2 (SC) Adalimumab Recombinant human IgG1 monoclonal Ab (SC) Golimumab Human IgG1 monoclonal Ab (SC) Certolizumab Recombinant humanized monoclonal Ab Fab fragment (SC)
99 TAILS Incidence % Difficult to establish Based on post-marketing studies As use of these agents increases, incidence of cutaneous reactions will increase Most cases caused by the agents that have been more widely used Onset: <1 month 4 years Diagnostic and therapeutic challenge
100 TAILS: Pathogenesis TNF-alpha inhibitor leads to production of autoantibodies Disruption in cytokine balance Suppression in production of Th1 cytokines, driving the immune response to Th2 cytokine production Interference with apoptosis by decreasing CD44 expression Inhibition of cytotoxic T-cells
101 Drug-induced autoimmunity Patients treated with TNF-alpha inhibitors develop antibodies found in patients with SLE (ANA, ds-dna, ENA) in the absence of clinical features of SLE Not an indication to stop drug

102 Drug-induced autoimmunity Use of these agents may trigger or unmask SLE in some patients
103 TNF-alpha Inhibitor Induced SLE: Diagnosis In the setting of ongoing treatment with TNF-alpha inhibitor No prior history of SLE Cutaneous findings of SLE Malar rash, photosensitive rash, mucosal ulcers, alopecia Systemic findings of SLE Constitutional symptoms fever, malaise, weight loss Arthralgias, arthritis + Serology ANA, ds-dna Low complement Negative anti-histone antibodies Resolution of symptoms when drug is discontinued
104 TNF-alpha Inhibitor Induced SLE: Management Stop the drug Resolution of symptoms in 3 weeks to 6 months Patients may require systemic therapy Corticosteroids and steroid sparing immunosuppressive agents (methotrexate, azathioprine, mycophenolate mofetil)
105 Regarding TNF-alpha Inhibitors which statement is INCORRECT: A. It is contraindicated to use these drugs in patients with SLE B. Re-challenging patients who develop anti-tnf alpha induced SLE with alternative TNF-alpha inhibitor agents is safe. C. It is recommended to perform baseline serologic testing for CTD prior to starting therapy D. It is recommended to perform baseline CXR and TB testing prior to starting therapy. E. Patients should be followed closely after initiation of therapy to assess for development of lupus-like reactions and other cutaneous reactions
106 TNF-alpha inhibitors can cause the following cutaneous reaction: A. Psoriasiform dermatitis B. Granulomatous dermatitis C. Vasculitis D. Alopecia areata E. All of the above

107 Psoriasiform dermatitis and palmoplantar pustulosis indistinguishable from psoriasis
108 Cutaneous Reactions to TNF-alpha Injection site reaction Urticaria Cellulitis Psoriasiform dermatitis Granulomatous dermatitis LE-like syndrome Inhibitors Vasculitis Alopecia areata Erythema nodosum SJS Morphea Erythroderma
109 CASE
110 70 yo F, 2 month h/o recurrent follicular lymphoma, treated 2 yrs ago Transferred from outside hospital for worsening desquamating eruption and severe mucositis for 1 month Skin and mucosal biopsies showed lichenoid dermatitis and mucositis c/w SJS/TEN 1 month prior to the eruption developing, she received 1 dose of a cefazolin as well a course of trimethoprim/sulfa and levofloxacin for URI She has not responded to systemic steroids and IVIG


111

112

113
114 What is the likely diagnosis? A. Stevens Johnson syndrome/ toxic epidermal necrolysis (SJS/TEN) B. Drug reaction with eosinophilia and systemic symptoms (DRESS) C. Lymphoma D. Infection E. Paraneoplastic pemphigus

115 Paraneoplastic pemphigus DIF- Cell surface staining along with linear to granular deposition along the BMZ with IgG and C3 IIF - + ICS titer 1:80 Dsg 3 + Dsg 1 -
116 Pitfall Not considering other diseases associated with mucosal lesions, blisters, and sloughing when evaluating a patient for possible SJS/TEN

117 BUGS: What bugs you?

118 77 yo male with CLL most recently treated with ibrutinib (EGFR inhibitor) Abdominal pain secondary to acute pancreatitis Worsening skin eruption involving head, neck, chest, and back 2-3 weeks after ibrutinib started

119

120
121 What is your diagnosis? A. Ibrutinib drug eruption B. Scabies C. Varicella-Zoster infection D. Deep fungal infection E. Impetigo
122 Disseminated VZV Lesion swab - Bacterial culture: Staph aureus 4+ - HSV1/HSV2 PCR: negative - PCR VZV: Positive Reactivation of VZV infection: started on IV Acyclovir 10mg/kg Q8H until lesions have crusted. Negative pressure room. Mupirocin 2% oint TID Ophthalmology: no ocular involvement Pancreatitis due to visceral involvement Cholecystectomy deferred
123 Disseminated Zoster Pearls Definition > 20 lesions outside of 2 contiguous dermatomes At risk group Elderly, immunosuppressed Viscera can be affected Hutchinson s sign Call ophthalmology Contact and airborne precautions Treatment IV Acyclovir until lesions healed over or clear
124 Cutaneous adverse effects of targeted therapies Epidermal growth factor (EGFR) inhibitors Papulopustular eruption in a seborrheic distribution Most common cutaneous side effect Dose-dependent 1-2 weeks after therapy Pruritus, xerosis Paronychia Mucositis Pattern or cicatricial alopecia


125
126 What is the best management for papulopustular eruption from an EGFR inhibitor? A. Systemic steroids B. Topical retinoids C. Low potent topical steroids and topical clindamycin D. Systemic antihistamines for pruritus and systemic antibiotics (tetracyclines) for severe eruptions E. C and D
127 Pearl Dermatologists need to be familiar with the skin-related toxicities associated with targeted therapies
128 CASE

129 72 yo F with psoriasis and psoriatic arthritis Worsening skin eruption on extremities x 1 month Infliximab Methotrexate Prednisone Methylprednisolone Fever, tachypnea, tachycardia Admitted for possible sepsis Started on Vancomycin and Cefepime


130


131 2011 MFMER slide-131


132

133 What is your diagnosis? A. Occlusive vasculopathy B. Infection C. Lupus-like reaction to TNF inhibitors D. Psoriasis E. Lymphoma
134

135 2011 MFMER slide-135

136 2011 MFMER slide-136


137 2011 MFMER slide-137
138 Which organism is this? A. Blastomycosis B. Coccidiomycosis C. Cryptococcus D. Histoplasmosis
139 Disseminated Histoplasmosis Cutaneous, pulmonary, and intestinal involvement Histoplasma antibody and urine antigen positive Fungal blood cultures positive All immunosuppressants discontinued Responded to treatment with amphotericin X 2 weeks, followed by itraconazole Monitor itraconazole levels and Histoplasma urine antigen
140 Disseminated Histoplasmosis Histoplasma capsulatum Grows in soil which contains bird and bat feces Endemic in Mississippi and Ohio river basins; Central and South America; Southern Europe; Africa; South and Southeast Asia Hematogenous dissemination in patients with suppressed immune systems
141 Disseminated Histoplasmosis Patients may present with ill-defined symptoms Fevers, weight loss Up to 20% may present in septic shock and multisystem organ failure Variable clinical presentation Papules & nodules with necrosis & hyperkeratosis; ulcers; bullous EM-like; erysipelas-like; petechiae/purpura; acneiform & folliculopustular papules; vesicles, herpetiform; exfoliative, nummular or psoriasiform dermatitis; morbilliform eruption Gold standard for diagnosis Tissue cultures
142 Pearls Infection MUST be excluded in an immunocompromised patient!!! Recently described phenomenon of immune reconstitution syndrome In the setting of disseminated histoplasmosis in patients who have been on a biologic agent or had reduced cellular immunity Patients do well clinically and have therapeutic itraconazole levels with decrease in histoplasma urine antigens Develop new skin or LN lesions with negative cultures but organisms still present on biopsy Tx with prednisone taper and continue itraconazole
143 CASE


144 3 month boy with fever, irritability & rapidly progressing generalized blisters over past 24 hours 2011 MFMER slide-144


145 2011 MFMER slide-145


146 2011 MFMER slide-146
147 What is your diagnosis? A. Erythema multiforme (EM) B. Herpes infection C. Stevens Johnson syndrome/ Toxic epidermal necrolysis (SJS/TEN) D. Staphylococcal scalded skin syndrome (SSSS) E. Toxic shock syndrome (TSS)
148 Staphylococcal Scalded Skin Syndrome (SSSS) Common in infants and children Secondary to extracutaneous S. aureus, phage grp II, infection Produce exfoliative toxins, bind to dsg 1 leading to acantholysis of the upper epidermis Fever, irritability, purulent rhinorrhea and conjunctivitis, painful, tender skin Periorificial edema and scale crusts Confluent erythema, superficial erosions and flaccid bullae, esp. in intertriginous sites
149 Treatment Throat culture positive for MSSA IV antibiotics Vancomycin (per ID) stopped after 5 days, Clindamycin 80 mg IV q8h and Oxacillin 300 mg IV q6h Plastibase ointment Zinc oxide ointment to groin and neck Mupirocin ointment to nares and severe areas
150 CASE

151 7 month male Atopic dermatitis 24 hours of explosive worsening of AD VSS Non-toxic, happy, no change in temperament


152 2011 MFMER slide-152


153 2011 MFMER slide-153


154


155 2011 MFMER slide-155
156 What is your diagnosis? A. Eczema Coxsackium B. Eczema Herpeticum C. Gianotti Crosti syndrome D. Secondary bacterial infection in setting of atopic dermatitis
157 Eczema Coxsackium Enterovirus PCR swabs from both tongue and skin positive HSV/VZV PCR swab negative Bacterial swab culture grew 2+ Staph aureus After 30 hrs of wet dressings, he had 75% improvement
158 Eczema Coxsackium Coxsackievirus A6 infection Widespread vesiculobullous exanthem favoring the perioral area, trunk and areas of previous dermatitis or injury as well as classic sites of hand, foot and mouth disease Young children Summer and Fall Spread via fecal-oral and respiratory routes

159

160 66 y/o male with no prior medical history Blisters of mouth and skin for 1.5 months Seen by outside derm: biopsies pemphigus vulgaris Prednisone 60 mg x 2 wks, worsening Prednisone 80 mg Mayo referral Admitted for wet dressings/wound care Plan for therapy with Rituximab


161 2011 MFMER slide-161


162


163

164 DIF: Cell surface staining with IgG and C3; IIF:1:1280 ICS; DSG1 131 DSG3 203

165 2011 MFMER slide-165
166 CBC, chem 20 panel Evaluation Negative CXR, Hepatitis screen, HIV, syphilis serologies QuantiFERON-TB POSITIVE!!! Vaccination status Influenza and Pneumococcal vaccine: past fall Herpes zoster: no DTaP: unknown
167 What would you do next? A. Continue steroids alone B. Continue steroids, vaccinate, and wait 4 weeks to give Rituximab C. Continue steroids, vaccinate and wait 2 weeks to give Rituximab D. Continue steroids, hold vaccination, and give Rituximab E. Continue steroids, start mycophenolate mofetil
168 Infectious Disease Consult No signs/symptoms of active disease latent TB Started on isoniazid and pyridoxine x 9 months QFT +: likely because of systemic steroids Delay Rituximab for at least 2 wks (ideally 4wks) Give DTaP

169 Inactivated vaccines are safe; effectiveness might be lower. If vaccination within 2 wks of therapy or while on therapy, should revaccinate (at least 3 months post-therapy if immunity restored). YES MAYBE NO Live vaccines should be administered 4 wks prior to therapy otherwise need wait at least 3 months after therapy. Influenza (inactivated) yearly Meningococcal Varicella Tdap once, Td booster every 10 years Hepatitis A Zoster Pneumococcal (PCV13 or PPSV23) Hepatitis B MMR HPV, if < 26 y/o
170

171 The Patient has Purpura!
172 Clinical Erythema Purpura Purpura Definitions Histologic Inflammation of blood vessel walls RBC extravasation Subepidermal vesicles/bullae, ulcers Necrosis, occlusion or destruction of blood vessel walls Nonpalpable and palpable purpura Petechiae purpuric macules Ecchymoses purpuric patches Retiform purpura livedo reticularis (lacelike) or racemosa (net-like)
173 Purpura Etiopathogenesis guides the differential diagnosis Purpura Immunologic or Allergic Infectious or Septic Occlusive Bleeding diathesis thrombocytopenia
174 CASE


175
176 22 year old male developed leg ulcers associated with a rash. Intensive wound care has been initiated. Which of the following would you recommend in addition? A. Observation B. Topical corticosteroids C. Systemic corticosteroids D. ACE wraps E. Surgical consultation for possible revascularization procedure


177


178 LCV Immunofluorescence Findings IgM IgG C3 F IgM > IgG, C3, & fibrinogen in blood vessels in the superficial dermis
179 Immunologic or Allergic Palpable purpura LCV and its Variants ANCA-associated vasculitis HSP or IgA vasculitis Mixed cryoglobulinemia Types II and III Urticarial vasculitis
180 LCV- Etiology Vasculitis is a clinical sign Ask what underlies the diagnosis Idiopathic (45-55%) Infection (15-20%) Inflammatory diseases/systemic diseases (15-20%) Connective tissue diseases: Lupus erythematosus, rheumatoid arthritis, Sjögren's syndrome Drugs ( 10-15%) PCN, sulfas, PTU, allopurinol, thiazides Malignancy (<5%)
181 Evaluation Possible causes & extent of involvement H & P, hemoccult, CBC, UA, ESR, CRP, ANA, ENA, ANCA, complement studies, RF, SPEP, TSH, cryoproteins, hepatitis serologies, thrombophilia workup, pan cx, CXR Skin biopsies 1 2 day old lesion for routine histology < 24 hour old macule for DIF Do not biopsy ulcers


182 HSP, Types II & III cryoglobulinemia, ACNAassociated vasculitis Clinical Features Similar to LCV Involvement above waist


183 HSP, Types II & III cryoglobulinemia, ACNAassociated vasculitis Clinical Features Larger lesions with figurate, retiform, or stellate shapes

184 HSP Histologic Findings Similar to LCV Immunofluorescence Findings IgA in blood vessel walls in the superficial dermis in >90%
185 Clinical Pearl When to treat? If mild and nonprogressive Many do not treat Supportive tx, compression If painful, severe or rapidly progressive Treat! Associated with systemic disease Associated with ulcerations
186 Pitfall Treating the ulcer as something other than vasculitis
187 CASE


188 The college student was well earlier today. 6 hours ago she developed a bad sore throat and muscle pains I feel awful Now prostrate, febrile, hypotensive, & tachycardic
189 The most important & lifesaving measure initiated was A. Supportive management alone B. Intravenous ceftriaxone C. Systemic corticosteroids (dexamethasone) D. Activated Protein C E. Lumbar puncture

190
191 Clinical Pearl Purpura fulminans Due to DIC Induced by meningococcemia Emergency! No more than 30 minutes should elapse before the administration of appropriate antibiotics Treat empirically, don t wait for the results of tests
192 Pearl Purpura fulminans? Identify cause of DIC, manage cause Think meningococcus or other underlying infection Medical emergency requiring intensive supportive management in an ICU Dermatologists can be valuable in guiding appropriate diagnosis and management Pitfall: Thinking this is LCV and starting systemic corticosteroids Purpura fulminans with symmetrical peripheral gangrene is an ominous clinical presentation affecting all age groups Outcome: Death/Amputation


193




194
195 Occlusive Intraluminal Vessel Wall Thrombosis Embolism Coagulation disorders Fibrin Cryoprotein- Type I cryoglobulinemia Degos disease or malignant atrophic papulosis Livedoid vasculopathy


196 Occlusive Vasculitis Intraluminal Thrombosis- Embolism Atherosclerosis Cholesterol emboli Thrombotic thrombocytopenic purpura (TTP)
197 Occlusive Vasculitis Intraluminal Coagulation Disorder - Fibrin DIC/purpura fulminans Coumadin necrosis Heparin necrosis Protein C deficiency Protein S deficiency Antithrombin III deficiency Antiphospholipid antibody syndrome Mutation in factor V Leiden G20210A mutation in prothrombin gene


198 Occlusive Vasculitis Intraluminal Coagulation Disorder - Fibrin


199 Occlusive Vasculitis Intraluminal Coagulation Disorder - Fibrin
200 Occlusive Vasculitis Intraluminal Cryoproteins Cryoglobulins Cryofibrinogens Type I cryoglobulinemia Monoclonal Ig, most commonly IgM Associated with lymphoproliferative disorders

201 Type I Cryoglobulinemia Clinical Features Purpuric macules & papules Small, punched-out ulcers on acral sites


202 Type I Cryoglobulinemia Histologic Features Deeply eosinophilic, homogeneous, hyalin, amorphous, PAS+ material in lumina of vessels
203 Infectious or Septic Vasculitis Pathogenesis Direct infection of blood vessel wall Interaction of the host immune response with microorganism in the blood vessel wall
204 Infectious Vasculitis Clinical Variants Ecthyma gangrenosum (Pseudomonas) Gonococcemia (Neisseria gonorrhoeae) Bacterial endocarditis Rocky Mountain Spotted Fever (Rickettsia rickettsii) Fungal sepsis (Candida, Aspergillus)
205 Infectious Vasculitis Histologic Features Involvement of deeper vessels Prominent thrombosis Usually cell-poor infiltrate Organisms may be visualized in & around blood vessel walls in acute but not chronic septic vasculitis


206 Infectious Vasculitis Histologic Features
207 CASE

208 A patient on hemodialysis
209 A patient on dialysis for chronic renal failure suddenly develops extraordinarily tender ulcerations involving legs, thighs and abdominal pannus Which of the following statements are most accurate about this condition? A. Corticosteroids are the treatment of choice. B. Surgical excision of the affected areas should be immediately performed C. The prognosis of this condition is dismal, and there is no treatment that consistently works. D. Sodium thiosulfate leads to a predictable improvement in this condition. E. Parathyroidectomy will usually be curative.


210

211

212

213
214 Occlusive Intraluminal Thrombosis Embolism Coagulation disorders Fibrin Cryoprotein- Type I cryoglobulinemia Calciphylaxis

215 Soft tissue X-ray Net-like pattern of calcification 90% specificity
216 Clinical Pearls Calciphylaxis is multifactorial and usually fatal The prognosis is dismal 1-year survival: 46% 2-year survival: 20%



217 One of the worst ways to die
218 Clinical Pearls Under-recognized syndrome Occurs in 4% of hemodialysis patients Non uremic cases associated with Warfarin therapy, CTD, hematologic malignancies, DM, primary hyperparathyroidism, vitamin D deficiency, protein C and S deficiency, factor V Leiden deficiency, Crohn disease, and liver disease No clearly effective treatments
219 Calciphylaxis treatment strategies Correct calcium-phosphate balance Improve tissue perfusion & oxygenation Wound Care Debridement Pain control Palliative care Sodium thiosulfate TPA Surgical Cinacalcet Hyperbaric oxygen Whirlpool Low calcium dialysate Avoid warfarin for anticoagulation Maggot Multidisciplinary approach Mechanism - Thrombotic tissue ischemia; Must address the clot & prevent more



220 ESRD from focal segmental GN on HD Calciphylaxis One month later Before low dose TPA X 14 days 6 months later
221 CASE
222 70 yo M with DM, HTN, hyperlipidemia, peripheral neuropathy, pancytopenia, CAD s/p CABG and MI Transfemoral, endovascular aortic valve insertion for CHF secondary to aortic stenosis Complicated intraoperatively by cardiac arrest, requiring transcatheter placement of another aortic valve Postoperatively, he developed fever, leukocytosis, anemia, and thrombocytopenia (43) followed 4 days later by cerebral infarction Consulted for LLE nonpalpable purpura that developed 9 days after the procedure


223

224

225
226 What is your diagnosis? A. Cholesterol emboli B. Thrombocytopenia C. Infectious emboli D. Polymer gel emboli E. Vasculitis

227

228

229 2011 MFMER slide-229

230 What is this material? Colloidal iron stain established this was hydrophilic material X-ray probe microanalysis of the material Phosphorus, sulfur and iron


231
232 Hydrophilic Polymer Coating Purpose: Decrease friction Reduce arterial spasm & pain Reduce thrombosis Must be meticulously cleaned and moistened in order to avoid drying out and becoming tacky Not to be used for initial vascular access, because passage through entry needles can shear off the hydrophilic coating


233 2010 Clinical sequelae ranged from undetectable (no symptoms) to renal failure, myocardial infarction, pulmonary infarction, stroke, ongoing gangrene, and/or death occurring within days to weeks of suspected embolization of foreign material MFMER slide-233
234 Review Article Polymer coating embolism from intravascular medical devices a clinical literature review Author links open overlay panelamitabh M.Chopra a MonikMehta b JeanBismuth c MaksimShapiro d Michael C.Fishbein e Alina G.Bridges f Harry V.Vinters g rights and content Under a Creative Commons license open access Highlights Recent literature associates polymer coating embolism with a range of adverse clinical sequelae. The elusive, microscopic phenomenon has been difficult to detect for almost three decades. Major polymer-emboli-related conditions include obstructions of blood flow in small vessels. Polymer emboli incidence is dependent on device coating integrity measured by particulate release. Regulators may default to controlling particulate release from intravascular devices. Research highlights the potential of using low-particulate-release coatings on intravascular devices.




235 Hydrophilic Polymer Gel Emboli: An Epidemic 2011 MFMER slide-235

236 Occlusive Intraluminal Thrombosis Embolism Coagulation disorders Fibrin Cryoprotein- Type I cryoglobulinemia Calciphylaxis Hydrophilic gel coating
237 Pearls: Hydrophilic Polymer Gel Emboli Can embolize to the skin and cause microvascular occlusion presenting as purpura, livedo racemosa, livedo reticularis, hemorrhagic panniculitis, or ulceration Recent interventional procedure Treatment is supportive Lesions gradually improve Be aware of internal organ involvement of emboli

238 Yikes! The flesh eating ulcer

239
240 58-year-old woman with multiple ulcerations and abscesses involving both breasts x 5 months Started after breast reduction surgery for pendulous breasts Ulcerations began at the incision sites 3 weeks postoperatively Multiple admissions to plastic surgery for incision and drainage of breast abscesses Several admissions to infectious diseases service for intravenous antibiotics Ulcerations have progressed
241 The treatment that led to resolution of these abscesses was: A. Readmission of patient for incision and drainage of abscesses B. Bilateral mastectomy C. Long-term suppressive oral antibiotic treatment depending on antimicrobial susceptibilities D. Oral prednisone E. Skin grafting of ulcerations




242
243 Discussion Pyoderma Gangrenosum There are many weird causes of ulcerations Weirdest of all: pyoderma gangrenosum Clues in this patient: Irregular, violaceous undermined border Pathergy (triggered by trauma, surgical debridement, and attempts to graft)
244 Clinical Pearls Pyoderma gangrenosum can occur anywhere on body including the breasts Characteristic clinical presentation Rapidly progressive ulcerative process Begins as a small pustule which breaks down forming an ulcer Satellite papules may appear at the border, break down, and then fuse with the central ulcer Fully developed: painful, undermined ulcer with blue/purple border Heals with atrophic scar

245 CP
246 Associated conditions 50% have no underlying cause Associations (50%) IBD - Most common(1.5%-5% of IBD patients get PG) RA, seronegative arthritis (>1/3 PG pts have arthritis Hematologic abnormalities, malignancies

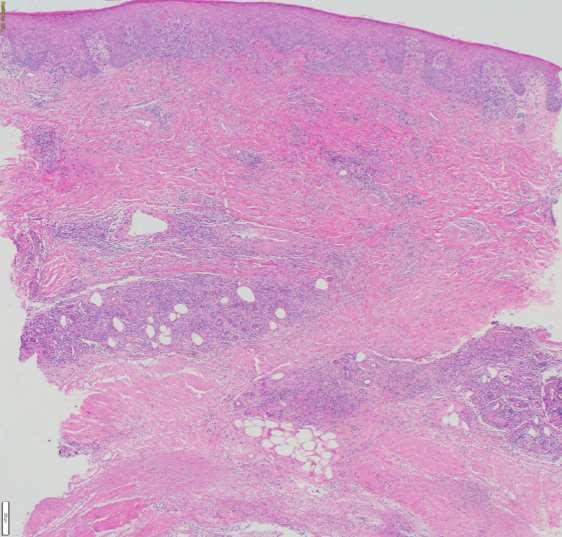
247 Edge of the ulcer, dense infiltrate of PMN undermining the epidermis.

248 All special stains and tissue cultures fail to reveal infection c/w pyoderma gangrenosum.
249 CASE

250 59 yo woman admitted with 1 yr. history of expanding leg ulcers On prednisone, cyclosporine and azathioprine for presumed diagnosis of pyoderma gangrenosum No biopsy


251
252 What is your diagnosis? A. Pyoderma gangrenosum B. Lymphoma C. Infection D. Occlusive vasculopathy E. Calciphylaxis


253



254 Sporotrichosis Admission 4 months 1 year
255 Bottom Line with PG Diagnosis of exclusion BUT! It s important to do our best since treating a patient for PG when they DON T have it with steroids and/or immunosuppression has it s own set of associated risks, and can certainly aggravate the actual condition

256 Common diseases misdiagnosed as PG Vascular occlusive disease Chronic venous disease Vasculitis Neoplasm Exogenous tissue injury/factitial Disease Spider bite Infection
257 Lessons learned Pyoderma gangrenosum can be underdiagnosed Pyoderma gangrenosum can be overdiagnosed
258 Summary: Pearls and Pitfalls in Hospital Dermatology Erythroderma Pruritus Drugs Simple, Complex, Misc BUGS: Infection and infection prevention Purpura Neutrophilic dermatoses PG Handout


259 Thank you!


260 Comments/questions?
S003 CPC Self-Assessment
 S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Five things not to miss in Dermatology. Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine
 Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
DERMATOLOGICAL EMERGENCIES. DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE
, DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE") DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Concentrate on Descriptors. An Approach to Skin Diseases in the ER
 Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
DERMATOLOGIC EMERGENCIES. Mary Evers D.O., F.A.O.C.D. Georgetown, Texas
 DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
Goals of this talk. Morbilliform. Common Morphologies in the Hospital 11/7/2017. Hospital Based Dermatology: Common and Tough Consult Cases
 Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Bacterial Infections in Pediatric Dermatology. Patrick McMahon, MD Children s Hospital of Philadelphia
 Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Emergency Dermatology. Emergency Dermatology
 Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
GOOD MORNING! AUGUST 5, 2014
 GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
Index. derm.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abatacept for DLE, 493 for SLE, 497 Ablative therapies, localized, for cutaneous T-cell lymphoma, 502 506. See also Cutaneous T-cell lymphoma,
Note: Page numbers of article titles are in boldface type. A Abatacept for DLE, 493 for SLE, 497 Ablative therapies, localized, for cutaneous T-cell lymphoma, 502 506. See also Cutaneous T-cell lymphoma,
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES. R e g i S C A R PATIENT'S DATA. Age country of birth
 REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
SJS/TEN spectrum. Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) 10/7/2016
 /Toxic Epidermal Necrolysis (TEN) 10/7/2016") Jesse Keller MD Assistant Professor Oregon Health & Science University Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) Drug induced dermemergencies that exist on a spectrum Delayed reaction:
Jesse Keller MD Assistant Professor Oregon Health & Science University Stevens-Johnson syndrome (SJS) /Toxic Epidermal Necrolysis (TEN) Drug induced dermemergencies that exist on a spectrum Delayed reaction:
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes
 Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Skin Manifestations of Systemic Disease. Approach to Dermatalogic Diagnosis 9/6/2016. Go Ahead---Judge a Book by its Cover!
 Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Inpatient dermatopathology. Inpatient dermatopathology. Inpatient dermatopathology: Histologic patterns that matter most
 Inpatient dermatopathology: Histologic patterns that matter most Beth S. Ruben, M.D. Associate Clinical Professor University of California, San Francisco Departments of Dermatology and Pathology Dermatopathology
Inpatient dermatopathology: Histologic patterns that matter most Beth S. Ruben, M.D. Associate Clinical Professor University of California, San Francisco Departments of Dermatology and Pathology Dermatopathology
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
Drug Allergy A Guide to Diagnosis and Management
 Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
Hospital-based Dermatopathology. Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM
 Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
Hospital-based Dermatopathology Janis M. Taube, MD Director of Dermatopathology Johns Hopkins University SOM Overview Drug-eruptions Erythroderma Manifestations of renal disease Blistering disorders Vasculitis/Vasculopathy
Big rashes in little patients:
 ! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
Case 1. Debridement Cultures Keflex Silvadene
 The Red Breast Beth McLellan, M.D. Assistant Professor Division of Dermatology Albert Einstein College of Medicine Montefiore Medical Center Jacobi Medical Center Case 1 48 year old radiation oncologist
The Red Breast Beth McLellan, M.D. Assistant Professor Division of Dermatology Albert Einstein College of Medicine Montefiore Medical Center Jacobi Medical Center Case 1 48 year old radiation oncologist
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]
![Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]](/thumbs/83/87318178.jpg "Clinical Pearls Infectious Diseases. Pritish K. Tosh, MD MN ACP Nov 7, [Answers and discussion slides will be posted after the meeting]") Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Clinical Pearls Infectious Diseases Pritish K. Tosh, MD MN ACP Nov 7, 2014 [Answers and discussion slides will be posted after the meeting] Case 1 A 33-year-old male with diffuse large B-cell lymphoma
Management of Pyoderma Gangrenosum Mentoring in IBD XVII
 Management of Pyoderma Gangrenosum Mentoring in IBD XVII Scott Walsh MD PhD FRCPC Division of Dermatology Sunnybrook Health Sciences Centre University of Toronto Pyoderma Gangrenosum: A pathological
Management of Pyoderma Gangrenosum Mentoring in IBD XVII Scott Walsh MD PhD FRCPC Division of Dermatology Sunnybrook Health Sciences Centre University of Toronto Pyoderma Gangrenosum: A pathological
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Dermatology Pearls for Inpatient Medicine. Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University
 Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Background information of DIF
 Napa Dermatopathology Meeting 2018: Immunobullous Disease Whitney A. High, MD, JD, MEng whitney.high@ucdenver.edu Professor of Dermatology & Pathology Vice-Chairman, Dermatology Director of Dermatopathology
Napa Dermatopathology Meeting 2018: Immunobullous Disease Whitney A. High, MD, JD, MEng whitney.high@ucdenver.edu Professor of Dermatology & Pathology Vice-Chairman, Dermatology Director of Dermatopathology
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Bugs and Drugs: What s New in Hypersensitivity Reactions?
 Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions
 PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
PHM142 Autoimmune Disorders + Idiosyncratic Drug Reactions 1 Autoimmune Disorders Auto-reactivity: low physiological levels (e.g. tolerance) vs. pathogenic levels 80+ types of autoimmune diseases affect
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123
 BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
BSD Self Assessment Workshop 7 th July 2013 CASE 27 RAC6123 M55. 4/7 tender lesions on knee, legs and arms. Also iritis/ weight loss/headache, synovitis.?vasculitis. Sarcoidosis. Biopsy from left elbow
Bacterial Infections. Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas
 Bacterial Infections Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas Conflict of interest statement: Book royalties- Elsevier
Bacterial Infections Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas Conflict of interest statement: Book royalties- Elsevier
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
CASE REPORT ATYPICAL BULLOUS PYODERMA GANGRENOSUM WITH EARLY LESIONS MIMICKING CHICKEN POX
 ATYPICAL BULLOUS PYODERMA GANGRENOSUM WITH EARLY LESIONS MIMICKING CHICKEN POX Ramesh M 1, Kavya Raju Nayak 2, M.G. Gopal 3, Sharath Kumar B.C 4, Nandini A.S 5 HOW TO CITE THIS ARTICLE: Ramesh M, Kavya
ATYPICAL BULLOUS PYODERMA GANGRENOSUM WITH EARLY LESIONS MIMICKING CHICKEN POX Ramesh M 1, Kavya Raju Nayak 2, M.G. Gopal 3, Sharath Kumar B.C 4, Nandini A.S 5 HOW TO CITE THIS ARTICLE: Ramesh M, Kavya
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
VARICELLA. Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara
 VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
A case of bullous pemphigoid following pemphigus foliaceus
 #2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
#2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving
 Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Skin Manifestations of Drug Reactions
 Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India.
 Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Cutaneous Conditions Associated with Systemic Disease
 Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
Cutaneous Conditions Associated with Systemic Disease Johnnie M Woodson, M.D., F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates,
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD
 CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
Vulval dermatoses. Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough
 Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT
 HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
HEMORRHAGIC BULLOUS HENOCH- SCHONLEIN PURPURA: A CASE REPORT Nirmala Ponnuthurai, Sabeera Begum, Lee Bang Rom Paediatric Dermatology Unit, Institute of Paediatric, Hospital Kuala Lumpur, Malaysia Abstract
Herbal and homeopathic products, often considered natural and non-toxic, can also cause adverse drug reactions.
 Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Right type of lesions for topicals. Onychomycosis. Common Diseases and Infections of the SKIN. Toby Maurer, MD University of California, San Francisco
 Common Diseases and Infections of the SKIN Toby Maurer, MD University of California, San Francisco Onychomycosis Topical treatment use for the right type of lesions Naftin gel for small superficial lesions
Common Diseases and Infections of the SKIN Toby Maurer, MD University of California, San Francisco Onychomycosis Topical treatment use for the right type of lesions Naftin gel for small superficial lesions
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
What's New in Oncodermatopathology: Immunotherapy Reactions
 What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
Dermatology GP Referral Guidelines
 Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
DESCRIPTIONS FOR MED 3 ROTATIONS Dermatology A3S
 Regardless of your future field of practice, you will be exposed to a considerable amount of dermatology and this rotation provides you the chance to see a range of skin diseases. You will have the opportunity
Regardless of your future field of practice, you will be exposed to a considerable amount of dermatology and this rotation provides you the chance to see a range of skin diseases. You will have the opportunity
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS LUPUS 101 SLE SUBSETS AUTOIMMUNE DISEASE 11/4/2013 HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS
 LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
LUPUS 101 LUPUS CAN DO EVERYTHING, BUT NOT EVERYTHING IS LUPUS HOWARD HAUPTMAN, MD IDIOPATHIC DISCOID LUPUS SLE SUBSETS SUBACUTE CUTANEOUS LUPUS DRUG INDUCED LUPUS NEONATAL LUPUS LATE ONSET LUPUS ANTI-PHOSPHOLIPID
-> Education -> Excellence
 Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
Quality Conference 5/2557 Extravasations: Event -> Education -> Excellence รศ.นพ. รว ศ เร องตระก ล สาขาว ชาก มารศ ลยศาสตร ภาควชาศลยศาสตร Extravasations: Event 1. Thrombophlebitis - superficial vein 2.
B. Autoimmune blistering diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details formation immediately above the basal layer. The dermal papillae, which are covered by basal cells in the single layer that is left in
Go Back to the Top To Order, Visit the Purchasing Page for Details formation immediately above the basal layer. The dermal papillae, which are covered by basal cells in the single layer that is left in
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Recalcitrant Warty Erythroderma With Severe Pruritus. Gil Yosipovitch Professor & Chair Department of Dermatology & Itch Center Temple University
 Recalcitrant Warty Erythroderma With Severe Pruritus Gil Yosipovitch Professor & Chair Department of Dermatology & Itch Center Temple University DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Gil Yosipovitch,
Recalcitrant Warty Erythroderma With Severe Pruritus Gil Yosipovitch Professor & Chair Department of Dermatology & Itch Center Temple University DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Gil Yosipovitch,
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA
 THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
THE TIP OF THE ICEBERG SAMER BOLIS, DO PGY-3 LEHIGH VALLEY HEALTH NETWORK, ALLENTOWN PA Case The patient is a 48 year-old female, who recently returned from a trip to Puerto Rico. She presents to the ED
Immunobullous Diseases: Review and Update. May P. Chan, MD Associate Professor of Pathology and Dermatology University of Michigan
 Immunobullous Diseases: Review and Update May P. Chan, MD Associate Professor of Pathology and Dermatology University of Michigan Diagnosis of Immunobullous Diseases Clinical H&E DIF DIAGNOSIS IIF ELISA
Immunobullous Diseases: Review and Update May P. Chan, MD Associate Professor of Pathology and Dermatology University of Michigan Diagnosis of Immunobullous Diseases Clinical H&E DIF DIAGNOSIS IIF ELISA
Objectives. 3HP and Flu Syndrome What is the Underlying Mechanism? Case #1 3/23/2016. Christina T. Fiske, MD MPH March 30, 2016
 Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
Objectives 3HP and Flu Syndrome What is the Underlying Mechanism? Christina T. Fiske, MD MPH March 30, 2016 Illustrate the side effect of 3HP flu like syndrome after its initiation to raise awareness in
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Drug allergy and Skin Disorders. Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey
 Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
Drug allergy and Skin Disorders Timothy Craig, DO, FACOI Professor of Medicine and Pediatrics Distinguished Educator Penn State University, Hershey The best screening test for anaphylaxis is? A. histamine
PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION
 JAN 18 2018 ASP ECHO CLINIC CHARLES KRASNER, M.D. PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION FIRST HOSPITALIZATION: 62 YEAR OLD MALE ADMITTED WITH DIAGNOSIS OF CELLULITIS Hx of AODM, Morbid Obesity,
JAN 18 2018 ASP ECHO CLINIC CHARLES KRASNER, M.D. PSEUDO-CELLULITIS - ALL THAT S RED IS NOT INFECTION FIRST HOSPITALIZATION: 62 YEAR OLD MALE ADMITTED WITH DIAGNOSIS OF CELLULITIS Hx of AODM, Morbid Obesity,
Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center
 Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
CUTANEOUS VASCULITIS. Katharine Warburton ST6 Dermatology
 CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
SKIN, SOFT TISSUE, AND BONE INFECTIONS. Clinical Correlation Series
 SKIN, SOFT TISSUE, AND BONE INFECTIONS Clinical Correlation Series impetigo Ecthyma Erysipelas Cellulitis Panniculitis Necrotizing fasciitis CONSIDERATIONS IN SKIN AND SOFT TISSUE INFECTION Localization
SKIN, SOFT TISSUE, AND BONE INFECTIONS Clinical Correlation Series impetigo Ecthyma Erysipelas Cellulitis Panniculitis Necrotizing fasciitis CONSIDERATIONS IN SKIN AND SOFT TISSUE INFECTION Localization
Rayos Prior Authorization Program Summary
 Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Rayos Prior Authorization Program Summary FDA APPROVED INDICATIONS AND DOSAGE FDA-Approved Indications: 1 Agent Indication Dosage Rayos (prednisone delayedrelease tablet) as an anti-inflammatory or immunosuppressive
Infectious Disease. Chloe Duke
 Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
Infectious Disease Chloe Duke Learning Objectives Essential - Causes, recognition and Treatment of: Meningitis Sepsis Purpura Important Cervical Adenopathy Tonsillitis and Pharyngitis Otitis Media Pneumonia
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Cases I have Learned From. Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville
 University of Louisville") Cases I have Learned From Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville Jeffrey P. Callen, MD Disclosure (previous 12 months) Consultant/Advisory board Auxilium Consultant
Cases I have Learned From Jeffrey P. Callen, MD Professor of Medicine (Dermatology) University of Louisville Jeffrey P. Callen, MD Disclosure (previous 12 months) Consultant/Advisory board Auxilium Consultant
To provide guidance on prevention and control of illness caused by varicella-zoster virus (VZV).
.") Effective Date: 04/18 Replaces: 0 4 / 1 3 / 1 7 Page 1 of 4 POLICY: To provide guidance on prevention and control of illness caused by varicella-zoster virus (VZV). DEFINITIONS Two syndromes occur from
Effective Date: 04/18 Replaces: 0 4 / 1 3 / 1 7 Page 1 of 4 POLICY: To provide guidance on prevention and control of illness caused by varicella-zoster virus (VZV). DEFINITIONS Two syndromes occur from
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Index. Angiosarcoma diagnosis, 47 lymphedema-related vs. non-lymphedemarelated, 48
 A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
Psoriasiform pemphigus foliaceus: a report of two cases
 J Cutan Pathol 2012: 39: 549 553 doi: 10.1111/j.1600-0560.2012.01866.x John Wiley & Sons. Printed in Singapore Copyright 2012 John Wiley & Sons A/S Journal of Cutaneous Pathology Psoriasiform pemphigus
J Cutan Pathol 2012: 39: 549 553 doi: 10.1111/j.1600-0560.2012.01866.x John Wiley & Sons. Printed in Singapore Copyright 2012 John Wiley & Sons A/S Journal of Cutaneous Pathology Psoriasiform pemphigus
My Method for Approaching Skin Biopsies
 My Method for Approaching Skin Biopsies P A U L H A U N, MD, MS, F A A D A S S I S T A N T P R O F E S S O R D E R M A T O L O G Y A N D D E R M A T O P A T H O L O G Y D E P A R T M E N T O F D E R M
My Method for Approaching Skin Biopsies P A U L H A U N, MD, MS, F A A D A S S I S T A N T P R O F E S S O R D E R M A T O L O G Y A N D D E R M A T O P A T H O L O G Y D E P A R T M E N T O F D E R M
From. The Department of Pediatrics Dr. Mehtas Hospital
 From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
Objectives. Routine to Rare: Complex Wound and Skin Conditions 8/29/2017
 Routine to Rare: Complex Wound and Skin Conditions Debbie Harrell RN, MSN Objectives Describe various pediatric complex wound and skin conditions. Identify the root causes of complex wound and skin conditions
Routine to Rare: Complex Wound and Skin Conditions Debbie Harrell RN, MSN Objectives Describe various pediatric complex wound and skin conditions. Identify the root causes of complex wound and skin conditions
MabThera. SC. The wait is over. MabThera delivered in just 5 minutes. SC= subcutaneous injection
 MabThera SC. The wait is over. MabThera delivered in just 5 minutes Abbreviated Prescribing Information MabThera 1400 mg solution for subcutaneous (SC) injection (Rituximab) Indications: Indicated in adults
MabThera SC. The wait is over. MabThera delivered in just 5 minutes Abbreviated Prescribing Information MabThera 1400 mg solution for subcutaneous (SC) injection (Rituximab) Indications: Indicated in adults
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update
 Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Stevens-Johnson s Syndrome / Toxic Epidermal Necrolysis: An update Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis Center
Department of Dermatology, Nippon Medical School, 1-1-5, Sendagi, Bunkyo-ku, Tokyo , Japan 2
 Dermatology Research and Practice Volume 2010, Article ID 931340, 5 pages doi:10.1155/2010/931340 Case Report Paraneoplastic Pemphigus Presenting as Mild Cutaneous Features of Pemphigus Foliaceus and Lichenoid
Dermatology Research and Practice Volume 2010, Article ID 931340, 5 pages doi:10.1155/2010/931340 Case Report Paraneoplastic Pemphigus Presenting as Mild Cutaneous Features of Pemphigus Foliaceus and Lichenoid
Case 1 History. William Tremaine, M.D. CP
 Extraintestinal Manifestations of IBD Case Studies William Tremaine, M.D. Case 1 History 18 year-old woman with Crohn s disease Onset at age 5: colonic & perianal Sulfasalazine, prednisone, mercaptopurine
Extraintestinal Manifestations of IBD Case Studies William Tremaine, M.D. Case 1 History 18 year-old woman with Crohn s disease Onset at age 5: colonic & perianal Sulfasalazine, prednisone, mercaptopurine
Psoriasis management. A/Prof Amanda Oakley Dermatologist, Waikato
 Psoriasis management A/Prof Amanda Oakley Dermatologist, Waikato AbbVie Breakfast Session, 14 June 2014 Disclosure This breakfast session is sponsored by Abbvie Autoimmune skin disorders Psoriasis Eczema
Psoriasis management A/Prof Amanda Oakley Dermatologist, Waikato AbbVie Breakfast Session, 14 June 2014 Disclosure This breakfast session is sponsored by Abbvie Autoimmune skin disorders Psoriasis Eczema
ERYTHRODERMA. ASAPA 2018 Fall Conference Tucson, AZ 10/12/2018. Andrew Newman, DO Pgy-3, Affiliated Dermatology/Honor Health
 ERYTHRODERMA ASAPA 2018 Fall Conference Tucson, AZ 10/12/2018 Andrew Newman, DO Pgy-3, Affiliated Dermatology/Honor Health OBJECTIVES Define Erythroderma Name common diseases and medications that cause
ERYTHRODERMA ASAPA 2018 Fall Conference Tucson, AZ 10/12/2018 Andrew Newman, DO Pgy-3, Affiliated Dermatology/Honor Health OBJECTIVES Define Erythroderma Name common diseases and medications that cause
Case No. 5; Slide No. B13/8956/2
 Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Interface diseases Case No. 5; Slide No. B13/8956/2 Histological findings Severe hydropic vacuolation of epidermal and follicular basal cells/ interface dermatitis Multifocally apoptotic keratinocytes
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.