"To Replace or Not to Replace, that is the Question"
|
|
|
- Caitlin Merritt
- 5 years ago
- Views:
Transcription

1 "To Replace or Not to Replace, that is the Question" Timothy Bailey, MD, FACE, CPI Director, AMCR Institute Clinical Associate Professor, UCSD School of Medicine

2 Disclosures Research: Abbott, Ascensia, BD, Boehringer Ingelheim, Companion Medical, Dexcom, Elcelyx, Glysens, Insulet, Janssen, Lexicon, Lilly, Medtronic, Novo Nordisk, Sanofi, Senseonics, Versartis, Yofimeter Consulting: Astra Zeneca, Bayer, Calibra, Lilly, Medtronic, Novo Nordisk, Sanofi Speaking: Abbott, Insulet, Medtronic, Novo Nordisk, Sanofi This slide deck: Dr. Herb Rettinger, MD, FACE
3 FEMALE HORMONE THERAPY
4 Estrogen Deficiency Menopause = 1 year without menses Can be gradual - begin in the late 30s with complete loss of production in the mid-50s Oophorectomy / Hysterectomy Presents with symptoms of hot flashes, sweating, insomnia, vaginal dryness/discomfort Affects 85% menopausal women; (nearly 100% of women with surgical menopause) Symptoms cease within 5 years for most individuals Endocr Pract. 2011; 17 (supp 6)
5 Hormone Therapy (HRT) Most effective means to minimize symptoms Estrogen therapy or Estrogen and a progesterone agent (E+P) To replace or not to replace? Risk-benefit ratio must be determined individually Menopause is NOT a disease

6 The WHI was TWO trials!
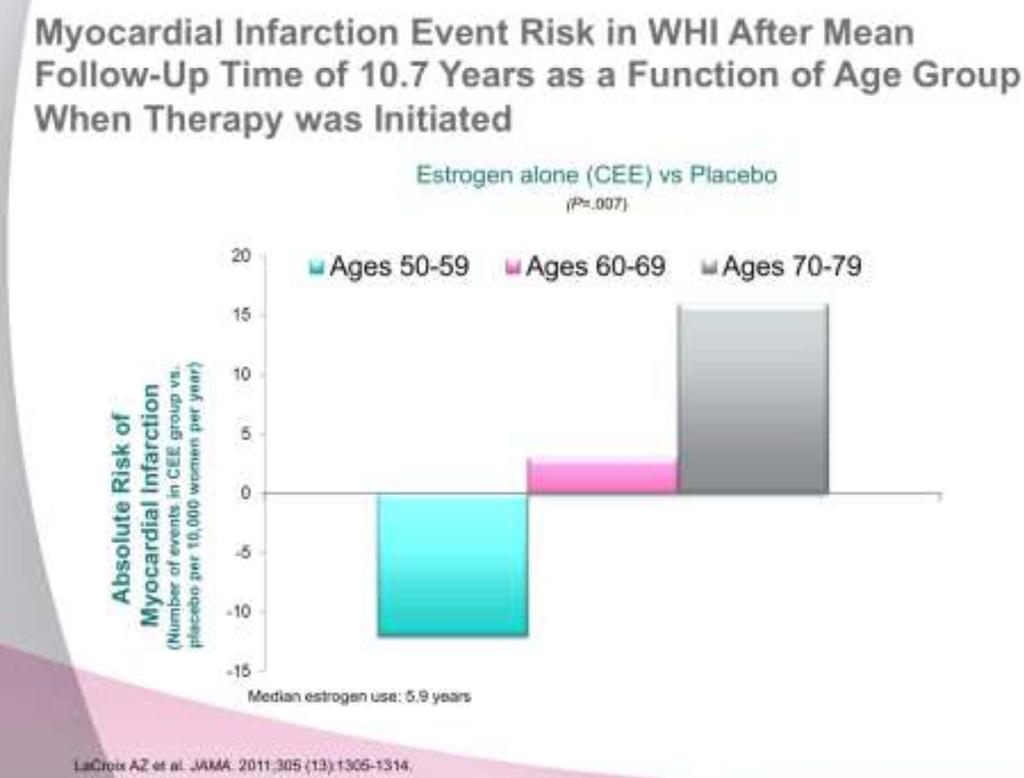
7 Women s Health Initiative (WHI) NIH sponsored multi-outcome study Most women were largely asymptomatic Women up to the age of 79 were treated Average age 63 (12 years postmenopausal) Oral CEE used ( +/- Progesterone) In 2002, E+P trial was terminated after 5.6 years as rate of breast cancer crossed preset boundaries JCEM, May 2013, 98(5): JCEM, July 2010, 95 (S1)s1-66

8 WHI Update (Hysterectomized Group)
9 9
10 Risks: Coronary Heart Disease Evidence for early harm among the older women in the E+P trial in WHI No increase in younger women; instead a trend to benefit Older women who are distant from menopause, who have established atherosclerosis and who receive standard doses of oral hormone therapy are at increased risk of coronary plaque instability, mural rupture and thrombosis JCEM, May 2013, 98(5):
11 Benefits of Hormone Therapy Improves hot flashes Relieves symptoms and normalizes vaginal atrophy, reduces incidence of UTI Prevents early postmenopausal bone loss and augments bone mass in late postmenopause Decreases colon cancer risk Associated with a decrease in diabetes risk Exerts a protective effect on osteoarthritis Improves quality of life JCEM, July 2010, 95 (S1)s1-66
12 Absolute Contraindications to Hormone Therapy Current, past, or suspected breast cancer Known or suspected estrogen sensitive malignant conditions Undiagnosed genital bleeding Untreated endometrial hyperplasia Previous idiopathic or current venous thromboembolism Active or recent arterial thromboembolic disease (angina, MI) Untreated hypertension Active liver disease Known hypersensitivity to the active substances of HT Porphyria cutanea tarda Endocr Pract. 2011; 17 (supp 6)
13 Risks of Hormone Therapy Cholecystitis Endometrial cancer (4.5-9x without P - Use if Uterus) Venous thromboembolic disease (smokers, clotting disorders, age, obesity) Use Transdermal Stroke (1-2 more cases/ 10,000 women-years) Breast cancer (NOT menpause) -? lower P agent Coronary Heart Disease timing & vascular state Endocr Pract. 2011; 17 (supp 6) JCEM, May 2013, 98(5): JCEM, July 2010, 95 (S1)s1-66
14 Special Populations: Status Post Hysterectomy Hysterectomy is the 2 nd most common major surgery in women (after cesarean) More than 6 million hysterectomies in the last 10 years Ovaries removed in 54% surgical menopause In these patients, HT can decrease mortality and may be overwhelmingly beneficial Vital Health Stat ; 92:1-32

15 Special Populations: Status Post Hysterectomy

16 Oophorectomized Women are Different! 16
17 Clinical Considerations Transdermal route of estrogen may theoretically decrease the risk of thromboembolic disease as it avoids the hepatic first pass effect History of VTE is not a complete contraindication to HT. Consider transdermal in symptomatic patients with history of VTE Also consider transdermal in patients with gallstones, hypertriglyceridemia and hypertension Transvaginal estrogen may be considered to have less systemic absorption Best for localized symptoms of vaginal atrophy, urinary incontinence Endocr Pract. 2011; 17 (supp 6)
18 Clinical Considerations Progestional agents for minimum of days per month Can consider 14 days every 3 months to decrease breast exposure to progesterone Some women may experience premenstrual like symptoms of progesterone i.e. mood swings, bloating, fluid retention switch to a different progesterone agent.
19 Clinical Considerations Hormone replacement therapy not recommended for prevention of dementia Not recommended for primary and secondary prevention of cardiovascular disease Not recommended as a 1 st line agent for osteoporosis treatment Bio-identical = buzzword - Beneficial? Compounded = unregulated
20 Bioidentical Hormones Compounding of plant derived hormones that are marketed as identical in structure to human endogenous hormones Not subjected to FDA regulations for safety and effectiveness Different mixtures of estrogens Estradiol (predominant estrogen before menopause) Estrone (predominant estrogen after menopause Estriol (from placenta) Triest has all 3. Endocr Pract. 2011; 17 (supp 6)
21 Bioidentical Hormones Variable potency leading to over and under dosing Cross contamination and concerns over sterility of preparations Compounded HTs have the same risks as FDA-approved therapies Recommendations against bioidentical hormones Endocr Pract. 2011; 17 (supp 6)
22 Approach to a Patient Identify if a patient is an appropriate candidate for HT Symptoms? Past medical history? Discuss treatment options with patient Hormone therapies Nonhormonal therapies (i.e. SSRi, SSNRs, gabapentin, clonidine) Review risks and adverse events If pt would like to try HT, use the lowest effective dose for symptom control Relief of clinical symptoms is used to determine dosing decisions; RARELY need lab tests!
23 Conclusions Menopause and aging are associated with many chronic illnesses including CAD, stroke, osteoporosis, dementia, and cancer Timing of therapy initiation may be critical Disease prevention may be possible in early menopause; may be detrimental in later periods.
24 Conclusions Treatment should be absolutely considered in appropriate women <60 years of age Would not consider starting HT in patients>70 years of age and >10 years post menopause All appropriate patients with surgical menopause should be considered for HT Duration of course should be based on a discussion between provider and patient, including risk factors, comorbidities, symptom relief.
25 MALE HORMONE THERAPY
26
27 The Massachusetts Male Aging Study The largest review of the effect of T levels on overall mortality 3,518 men were followed for 17 years Total testosterone levels were measured and divided into five categories at 200 ng/dl increments Multivariate analysis depicting the association with overall mortality, CVD, and prostate cancer specific mortalities was conducted Araujo AB, et al: Total Testosterone as a Predictor of Mortality in Men. The Endocrine Society 2005 Annual Meeting, San Diego, CA, June 4-7.
28 Estimates of the Cumulative Probability of Mortality, CVD Death, and Cancer Death Findings from follow up of 17 years: Age adjusted HR s* for men with Total T < 200 ng/dl vs. men with Total T of ng/dl 1.93 or two fold for all mortalities (p=.03) 3.30 or three fold for Cancer death (p=.03) 1.93 or two fold for CVD death (p=.28) * Hazard Ratio Araujo AB, et al: Total Testosterone as a Predictor of Mortality in Men. The Endocrine Society 2005 Annual Meeting, San Diego, CA, June 4-7.
29 Production and Regulation of Testosterone CNS Stimulation Hypothalamus _ GnRH Hypothalamic-Pituitary Portal System Posterior Pituitary Anterior Pituitary _ Testis FSH LH + + Sertoli Cells Sperm Inhibin Leydig Cells Testosterone
30 Pathophysiology of Testosterone Deficiency: Testicular Dysfunction (Primary Hypogonadism) GnRH LH Hypothalamus Pituitary Testes T Reduced Feedback 30 Hormone Levels: T, LH/FSH, GnRH Causes: Klinefelter s syndrome (47 XXY), undescended testes, orchiectomy, trauma, testicular cancer, radiation, chemotherapy, virus, hemochromatosis, EtOH, other drugs.

31 Pathophysiology of Testosterone Deficiency: Pituitary Dysfunction (Secondary Hypogonadism) GnRH or normal LH (Normal ) Hypothalamus Pituitary Testes T Reduced Feedback Hormone Levels: T, or inapprop. normal LH, FSH Causes: Pituitary tumors (eg, prolactinoma, acromegaly), radiation, craniopharyngioma, sarcoidosis, -thalassemia major, Trauma.

32 Hypothalamic Dysfunction (Secondary/Tertiary) GnRH (Normal) or normal LH (Normal) Hypothalamus Pituitary Testes T Reduced Feedback Hormone Levels: T, or inapprop. normal LH, GnRH Causes: Kallman s syndrome (with anosmia), idiopathic hypogonadotropic hypogonadism, head trauma, nutritional, chronic disease states, drugs.
33 Certain Substances May Cause Low Testosterone Alcohol Amiodarone Antivirals Cimetidine Cyclophosphamide Estrogens/progestins Anabolic Steroids Ganciclovir Glucocorticoids Ketoconazole Marijuana Megestrol acetate Opiates Spironolactone Adapted from Bhasin, S.in Harrison's Principles of Internal Medicine, 16 th edit. 2005;

34 The Influence of Testosterone Skin Hair growth, balding, sebum production Liver Synthesis of serum proteins Bone Accelerated linear growth, closure of epiphyses Male sexual organs Penile growth, spermatogenesis, prostate growth and function Brain Libido, Mood Muscle Increase in strength and volume Kidney Stimulation of erythropoietin production Bone marrow Stimulation of stem cells Morley JE, et al. Metab. 2000;49: AACE Hypogonadism Task Force Endocrinol Pract. 2002;8:
35 Low Testosterone is Frequently Seen in Patients with the Following Conditions Aging ( 1-2%/yr after age 30) Erectile Dysfunction (ED) Type II Diabetes HIV/AIDS Cancer Osteoporosis Depression Chronic pain treated with opioids Head Trauma Obesity Metabolic Syndrome Chronic renal failure COPD, OSA Alcohol abuse Anabolic steroid abuse Glucocorticosteroid use Chronic Infection Chronic Inflammatory Disease Griffen JE. Harrison s Principles of Internal Medicine Benito M, et al. J Clin Endocrinol Metab 2003;88: Winters SJ. Arch Fam Med. 1999;8: Tenover JL. Endocrinol Metab Clin North Am. 1998;27: Shores M. Arch Gen Psychiatry, 2004;61: Handelsman DJ. Endocrinol Metab Clin North Am Mar;22(1): Laghi F, et al. Am J Respir Crit Care Med Apr 1;171(7): van Breda E, et al. Int J Sports Med Apr;24(3):195-6
36 Signs and Symptoms of Low Testosterone (Hypogonadism) 1 Loss of libido* Erectile dysfunction* Depression, irritability Lethargy, loss of motivation Osteoporosis Loss of muscle mass Regression of secondary sexual characteristics Oligospermia or azoospermia Insulin Resistance 1.Tenover JL. Endocrinol Metab Clin North Am. 1998;27: * Hallmarks of hypogonadism
37 HIM Study*: Overall Conclusions Age-adjusted prevalence rate of low total testosterone levels was 38.4%; in Diabetics, 52% had low Testosterone! Odds of having total testosterone <300 ng/ml or currently being treated for low testosterone are: 2.5 x higher if BMI 25 kg/m2 2.0 x higher for diabetes 1.8 x higher for hypertension 1.4 x higher for asthma/copd 1.2 x higher for age x higher with each decade increase *Mulligan T, et al. The HIM Study (Hypogonadism In Males): An Epidemiological Program to Estimate the Population Prevalence of Hypogonadism in Men over 45. Poster presented at the Annual Scientific Assembly of the American Academy of Family Physicians. October 13-17, 2004; Orlando, FL.
38 How Do We Identify Patients? Serum Testosterone Levels Total Testosterone < 300 ng/dl* Free Testosterone < 50 pg/ml(may be better test in older men) Bioavailable Testosterone < 70 ng/dl *Total Testosterone is the most frequently used lab test for the diagnosis of hypogonadism Brawer, M. Reviews in Urology Vol 6, Supp 6, 2004; pgs. S9-S15 AACE Hypogonadism Task Force. Endocrinol Pract. 2002;8:
39 Low Testosterone Diagnosis and Treatment Algorithm Suspected or At Risk for Low Testosterone Assess Symptoms If Present If Low Testosterone Total < 300 ng/dl; Bioavail < 70 ng/dl; Free <50 pg/dl Testosterone Levels Repeat T with LH,FSH, Prolactin* Digital Rectal Exam, PSA Abnormal Normal Seek Other Causes Normal TRT Evaluate Further by Urologist *Pituitary MRI and/or refer to endocrinologist for further testing Adapted from Morales A et al. J Urol. 2000;163:
40 Potential Risks of Testosterone Replacement Therapy Polycythemia (more common in IM injections and/or smokers) Increased PSA (BPH and prostate cancer- elderly pts) Edema in patients with or without pre-existing cardiac, renal, or hepatic disease Precipitation or worsening of sleep apnea Acne Decrease in testicular size Decrease in sperm count / Infertility Gynecomastia (more common with IM injections) Hepatotoxicity only with oral therapy (increase in liver enzymes, cholestasis, and hepatic tumors) Hypertension Brawer, M. Reviews in Urology Vol 6, Supp 6, 2004; pgs. S9-S15 Hypogonadism Task Force. Endocrinol Pract. 2002;8: Package insert- Testim gel.
41 Testosterone Replacement Therapy (TRT): Prostate Issues Does TRT Cause Prostate Cancer? To date, there is no conclusive evidence that TRT causes prostate cancer Geriatric patients treated with androgens may be at an increased risk for development of prostatic hyperplasia and prostatic cancer (monitor PSA and DRE) Before initiation of TRT, pre-existing prostate cancer should be ruled out Testosterone should not be given to any man with suspected or current prostate cancer Rhoden EL and Morgentaler A. N Engl J Med 2004;350:
42 Goals and Benefits of Testosterone Replacement Therapy Improve libido and improve erectile function Improve body mass and strength Improve bone mineral density Improve energy level Improve mood/sense of well-being Petak SM, et al. AACE Clinical Practice Guidelines. Available at: Tenover JL. Endocrinol Metab Clin North Am. 1998;27: Wang C, et al. J Clin Endocrinol Metab. 2000;85: Katznelson L. Baillières Clin Endocrinol Metab. 1998;12:
43 Testosterone Therapy Delivery Systems Intramuscular injections Pellet implants Transdermal patches Applied to scrotal or non-scrotal areas Transdermal gel (most common) Chorionic gonadotropin or pulsatile GnRH for men interested in retaining fertility Petak SM, et al. AACE Clinical Practice Guidelines. Available at: Bals-Pratsch M, et al. Acta Endocrinol. 1988;118:7-13. Wang C, et al. J Clin Endocrinol Metab. 2000;85: Arver S, et al. J Urol. 1996;155:
44 Testosterone Levels after Replacement Therapy with Patch, Gel or Injection T Testosterone ng/dl Patch or Gel Normal range Injection Day Adapted from Bhasin and Bremner. J Clin Endocrinol Metab. 1997;82:3-8 Testosterone gel (AndroGel 1%) Solvay Pharmaceuticals, 2002
45 Considerations for Referral to Endocrinologist Signs and symptoms of pituitary tumor, including: Visual field abnormalities Headaches Hyperprolactinemia or hypopituitarism Testosterone <150 with normal LH, FSH Other pituitary abnormalities Interest in fertility Unclear etiology, signs/symptoms of estrogen excess. 45 Comments and Directions from Endocrinology Key Opinion Leaders
46 Considerations for Referral to Urologist Abnormal DRE History of prostate cancer Rapid rise in PSA velocity 0.75ng/ml/year or 1.5ng/ml/2 years Interest in fertility (primary hypogonadism) Comments and Directions from Urology Key Opinion Leaders
47 Summary Low testosterone is common with aging but rare in youth (where is is always a disease ) It may be both: Under (mis)-diagnosed Over (mis)-treated Symptom improvement is seen if testosterone levels are raised to within normal range Requires patient monitoring and an understanding of underlying etiology. (Endocrine referral if etiology unclear).
48 HRT - BOTTOM LINE Make a correct diagnosis (not issue in menopause) Therapy safe and available Individualize therapy don t mis-, over-, or under- treat duration Monitor therapy Physiologic (safety with androgens) Quality of life Your patients will thank you!
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Disclosures. Learning Objectives. Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease. None
 Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
Effects of Hormone Therapy on the Metabolic Syndrome and Cardiovascular Disease Micol S. Rothman, MD Associate Professor of Medicine Endocrinology, Diabetes and Metabolism Clinical Director Metabolic Bone
A dro r gen e R e R p e lac a e c m e e m n e t t T her e a r p a y Androgen Replacement Therapy in the Aging O j b ecti t ve v s Male
 Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Androgen Replacement Therapy in the Aging Male Thomas J. Walsh, MD, MS Department of Urology University of California, San Francisco Objectives 1. List 3 effects of androgens on normal male physiology.
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
Androderm patch, AndroGel packets and pump, Axiron solution, First- Testosterone, First-Testosterone MC, Fortesta gel, Testim gel, Vogelxo
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.31 Subject: Testosterone Topical Page: 1 of 9 Last Review Date: September 23, 2016 Testosterone topical
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Consent for Testosterone Therapy-Men Revised 4/10/18
 Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Endocrine Update Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh
 Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
Endocrine Update 2016 Mary T. Korytkowski MD Division of Endocrinology University of Pittsburgh Disclosure of Financial Relationships Mary Korytkowski MD Honoraria British Medical Journal Diabetes Research
What Is the Low T Syndrome? Is Testosterone Supplementation Safe?
 What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
What Is the Low T Syndrome? Is Testosterone Supplementation Safe? UCSF Osher Mini Medical School March 7, 2018 Dolores Shoback, MD Staff Physician SF-VAMC Professor of Medicine, UCSF No disclosures or
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN
 International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
International Society for Sexual Medicine - www.issm.info ISSM QUICK REFERENCE GUIDE ON TESTOSTERONE DEFICIENCY FOR MEN Version: September 2015 What is testosterone deficiency? Testosterone deficiency
ANDROGEN DEFICIENCY Update on Evaluation and Management
 ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
ANDROGEN DEFICIENCY Update on Evaluation and Management Kristen Gill Hairston, MD, MPH Associate Professor of Internal Medicine Section of Endocrinology and Metabolism Wake Forest University School of
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA
 Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
Prof Dato Dr TAN Hui Meng University of Malaya, Kuala Lumpur University of Pennsylvania, USA Prevailing context Increase number of men who are potential candidates for Testosterone Replacement Therapy
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc.
 OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
Testosterone Replacement in Adults. John A. Seibel, MD, FACP, MACE
 Testosterone Replacement in Adults John A. Seibel, MD, FACP, MACE Disclosures None! *Privately Authenticated Definition of Male Hypogonadism inadequate gonadal function, as manifested by deficiencies in
Testosterone Replacement in Adults John A. Seibel, MD, FACP, MACE Disclosures None! *Privately Authenticated Definition of Male Hypogonadism inadequate gonadal function, as manifested by deficiencies in
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Menopause & HRT. Rosie & Alex. Image:
 Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Men Getting Older Will Testosterone Keep Him Young?
 Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Men Getting Older Will Testosterone Keep Him Young? Alvin M. Matsumoto, M.D. Associate Director, GRECC V.A. Puget Sound Health Care System Professor, Department of Medicine Division of Gerontology and
Hypogonadism in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Hypogonadism in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
OVERVIEW OF PRESENTATION
 Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Testosterone Therapy in Men An update
 Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
Testosterone Therapy in Men An update SANDEEP DHINDSA Associate Professor of Medicine Director, Division of Endocrinology and Metabolism, Saint Louis University, St. Louis, MO Presenter Disclosure None
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Androgens. Medication Strengths Quantity Limit Comments Androderm (testosterone patch) 1% pump 2 pump bottles per Non-Preferred
 1% pump 2 pump bottles per Non-Preferred") Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Low Testosterone Consultation Information
 T Low Testosterone Consultation Information www.urologyaustin.com Andropause or Male Menopause This syndrome has been nicknamed ADAM, which stands for androgen deficiency of the aging male. It differs
T Low Testosterone Consultation Information www.urologyaustin.com Andropause or Male Menopause This syndrome has been nicknamed ADAM, which stands for androgen deficiency of the aging male. It differs
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone Oral Buccal Nasal Description
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice
 Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice JoAnn E. Manson, MD, DrPH, FACP Chief, Division of Preventive Medicine Interim Executive Director, Connors Center Brigham and
Lessons from the WHI HT Trials: Evolving Data that Changed Clinical Practice JoAnn E. Manson, MD, DrPH, FACP Chief, Division of Preventive Medicine Interim Executive Director, Connors Center Brigham and
OVERVIEW OF MENOPAUSE
 OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Sexual dysfunction of chronic kidney disease. Razieh salehian.md psychiatrist
 Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Sexual dysfunction of chronic kidney disease Razieh salehian.md psychiatrist Disturbances in sexual function are a common feature of chronic renal failure. Sexual dysfunction is inversely associated with
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone Oral Buccal Nasal
Testosterone Oral Buccal Nasal. Android, Androxy, Methitest, Natesto, Striant, Testred. Description
 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.32 Subject: Testosterone Oral Buccal Nasal Page: 1 of 10 Last Review Date: June 24, 2016 Testosterone Oral Buccal Nasal Description
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: December 8, 2017 Testosterone
Managing Testosterone Deficiency: A Practical Guide. John Grantmyre MD Professor of Urology Dalhousie University
 Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Managing Testosterone Deficiency: A Practical Guide John Grantmyre MD Professor of Urology Dalhousie University 1 2 Case Study #1 A 59-Year-Old Man with Erectile Dysfunction 3 Case History Robert is a
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.37 Subject: Testosterone Powder Page: 1 of 12 Last Review Date: November 30, 2018 Testosterone powder
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Testosterone (cypionate, enanthate, and propionate) powder, Fluoxymesterone powder, Methyltestosterone powder
 powder, Fluoxymesterone powder, Methyltestosterone powder") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.08.37 Subject: Testosterone Powder Page: 1 of 11 Last Review Date: September 18, 2015 Testosterone powder
Hormone Replacement Therapy
 Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Hormone Replacement Therapy What Role Should It Play With Our Patients? Noel R. Williams MD, FACOG TESTOSTERONE FOR MEN: SALVATION OR SNAKE OIL? Definition Male hypogonadism means the testicles don't produce
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Therapeutic Cohort Results
 Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
Patient: JANE DOE DOB: December 31, 1968 Sex: F MRN: Order Number: Completed: February 26, 2016 Received: February 26, 2016 Collected: February 26, 2016 One Day Hormone Check - Salivary Profile Therapeutic
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK
 2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
Testosterone Injection / Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Testosterone Injection / Implant Page: 1 of 9 Last Review Date: December 5, 2014 Testosterone
Women s Health: Managing Menopause. Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School
 Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: November 30, 2018 Testosterone
Peter J. Burrows MD FACS
 Testosterone Supplementation, Prostate Cancer Screening and Vitamins Peter J. Burrows MD FACS Clinical Assistant Professor of Urology University of Arizona, College of Medicine Adjunct Assistant Professor
Testosterone Supplementation, Prostate Cancer Screening and Vitamins Peter J. Burrows MD FACS Clinical Assistant Professor of Urology University of Arizona, College of Medicine Adjunct Assistant Professor
The Adolescent: A Patient at Risk: Ovarian Failure in Adolescent Cancer Survivors
 The Adolescent: A Patient at Risk: Ovarian Failure in Adolescent Cancer Survivors Avner Hershlag MD Professor and Chief Center for Human Reproduction North Shore LIJ Hofsra university School of Medicine
The Adolescent: A Patient at Risk: Ovarian Failure in Adolescent Cancer Survivors Avner Hershlag MD Professor and Chief Center for Human Reproduction North Shore LIJ Hofsra university School of Medicine
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Appendix: Reference Table of HT Brand Names
 Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
presents with Ken Sekine, MD
 presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice
presents Pioneering Technologies For Pellet Hormone Therapy Lifestyle Based Medicine A Primer for Clinicians with Ken Sekine, MD Dr. Sekine is a board certified OB-GYN who has been in private practice
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Testosterone Injection and Implant
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.33 Subject: Testosterone Injection Implant Page: 1 of 10 Last Review Date: March 17, 2017 Testosterone
Menopause: diagnosis and management NICE guideline NG23. Published November 2015
 Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Recognizing and Managing Testosterone Deficiency
 Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
Recognizing and Managing Testosterone Deficiency J. Bruce Redmon, M.D. Professor Division of Endocrinology Departments of Medicine and Urologic Surgery Disclosure Information I have no financial relationships
MENOPAUSAL HORMONE THERAPY 2016
 MENOPAUSAL HORMONE THERAPY 2016 Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA NICE provides the National Health Service advice on effective, good value healthcare.
MENOPAUSAL HORMONE THERAPY 2016 Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA NICE provides the National Health Service advice on effective, good value healthcare.
BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE
 Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
Authoriser: Moya O Doherty Page 1 of 7 BIOCHEMICAL TESTS FOR THE INVESTIGATION OF COMMON ENDOCRINE PROBLEMS IN THE MALE The purpose of this protocol is to describe common tests used for the investigation
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Hormone Replacement Therapy For Men Consultation Information
 Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Current Topics in Hormone Replacement Therapy
 Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
PERIMENOPAUSE. Objectives. Disclosure. The Perimenopause Perimenopause Menopause. Definitions of Menopausal Transition: STRAW.
 PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
Post-menopausal hormone replacement therapy. Evan Klass, MD May 17, 2018
 Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Male History, Clinical Examination and Testing
 Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
Male History, Clinical Examination and Testing Dirk Vanderschueren, MD, PhD Case Jan is 29 years old and consults for 1 year primary subfertility partner 28 years old and normal gynaecological investigation
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
HT: Where do we stand after WHI?
 HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
HT: Where do we stand after WHI? Hormone therapy and cardiovascular disease risk Experimental and clinical evidence indicate that hormone therapy (HT) reduces the risk of cardiovascular disease (CVD) Women
Implantable Hormone Pellets
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
Orals,Transdermals, and Other Estrogens in the Perimenopause
 Orals,Transdermals, and Other Estrogens in the Perimenopause Cases Denise Black, MD, FRCSC Assistant Professor, Obstetrics, Gynecology and Reproductive Sciences University of Manitoba 6/4/18 197 Faculty/Presenter
Orals,Transdermals, and Other Estrogens in the Perimenopause Cases Denise Black, MD, FRCSC Assistant Professor, Obstetrics, Gynecology and Reproductive Sciences University of Manitoba 6/4/18 197 Faculty/Presenter
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Reproductive physiology. About this Chapter. Case introduction. The brain directs reproduction 2010/6/29. The Male Reproductive System
 Section Ⅻ Reproductive physiology Ming-jie Wang E-Mail: mjwang@shmu.edu.cn About this Chapter The reproductive organs and how they work the major endocrine functions of sexual glands actions of sex hormones
Section Ⅻ Reproductive physiology Ming-jie Wang E-Mail: mjwang@shmu.edu.cn About this Chapter The reproductive organs and how they work the major endocrine functions of sexual glands actions of sex hormones
Before you prescribe
 Initiating hormone replacement therapy (HRT) / menopausal hormone therapy (MHT) Dr Sonia Davison Jean Hailes Consultant Endocrinologist Before you prescribe Ensure there are no contraindications to HRT/MHT
Initiating hormone replacement therapy (HRT) / menopausal hormone therapy (MHT) Dr Sonia Davison Jean Hailes Consultant Endocrinologist Before you prescribe Ensure there are no contraindications to HRT/MHT
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
Hormone Replacement Therapy For Women
 Hormone Replacement Therapy For Women Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Women Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Therapy Overview for the Behavioral Health Provider. Julie Thompson, PA Fenway Health
 Hormone Therapy Overview for the Behavioral Health Provider Julie Thompson, PA Fenway Health Continuing Medical Education Disclosure Program Faculty: Julie Thompson, PA Current Position: Physician s Assistant,
Hormone Therapy Overview for the Behavioral Health Provider Julie Thompson, PA Fenway Health Continuing Medical Education Disclosure Program Faculty: Julie Thompson, PA Current Position: Physician s Assistant,
Practical recommendations for hormone replacement therapy in the peri- and postmenopause
 CLIMACTERIC 2004;7:in press Practical recommendations for hormone replacement therapy in the peri- and postmenopause Recommendations from an Expert Workshop, February 2004 Henry Burger, Australia; David
CLIMACTERIC 2004;7:in press Practical recommendations for hormone replacement therapy in the peri- and postmenopause Recommendations from an Expert Workshop, February 2004 Henry Burger, Australia; David
Imvexxy (estradiol) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Imvexxy (estradiol) NEW PRODUCT SLIDESHOW Introduction Brand name: Imvexxy Generic name: Estradiol Pharmacological class: Estrogen Strength and Formulation: 4mcg, 10mcg; vaginal inserts Manufacturer: TherapeuticsMD,
Imvexxy (estradiol) NEW PRODUCT SLIDESHOW Introduction Brand name: Imvexxy Generic name: Estradiol Pharmacological class: Estrogen Strength and Formulation: 4mcg, 10mcg; vaginal inserts Manufacturer: TherapeuticsMD,
Menopause & HRT. Matt McKenna Elliot Davis
 Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
Why is my body not changing? Conflicts of interest. Overview 11/9/2015. None
 Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Why is my body not changing? Murthy Korada Pediatrician, Pediatric Endocrinologist Ridge Meadows Hospital Surrey Memorial Hospital None Conflicts of interest Overview Overview of normal pubertal timing
Does TRT Induce Prostate Cancer?
 Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
Does TRT Induce Prostate Cancer? Prism VI, Bruges, Belgium 21-22November 2014 Herman Leliefeld, Urologist, Utrecht The Netherlands Does TRT Induce Prostate Cancer? Why is it a controversial topic? Is there
MALE INFERTILITY & SEMEN ANALYSIS
 MALE INFERTILITY & SEMEN ANALYSIS DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential
MALE INFERTILITY & SEMEN ANALYSIS DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential
Original Policy Date
 MP 5.01.30 Implantable Hormone Pellets Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Local Policy created with literature search/12:2013 Return
MP 5.01.30 Implantable Hormone Pellets Medical Policy Section Prescription Drug Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Local Policy created with literature search/12:2013 Return
Prior Authorization Criteria Update: Androgens, Topical and Parenteral
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
A Practitioner s Toolkit for the Management of the Menopause
 Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Late Onset Hypogonadism. Toh Charng Chee Hospital Selayang
 Late Onset Hypogonadism Toh Charng Chee Hospital Selayang Introduction Although suppressed serum testosterone (T) is common in ageing men, only a small proportion of them develop the genuine syndrome of
Late Onset Hypogonadism Toh Charng Chee Hospital Selayang Introduction Although suppressed serum testosterone (T) is common in ageing men, only a small proportion of them develop the genuine syndrome of
Current Data and Considerations Novel Testosterone Formulations
 Current Data and Considerations Novel Testosterone Formulations 1 Hypogonadism: Treatment Safety and Prostate Health 2 Monitoring for Testosterone Therapy DRE 1,2 PSA Parameter Voiding/IPSS 1,2 Hemoglobin
Current Data and Considerations Novel Testosterone Formulations 1 Hypogonadism: Treatment Safety and Prostate Health 2 Monitoring for Testosterone Therapy DRE 1,2 PSA Parameter Voiding/IPSS 1,2 Hemoglobin