Managing diabetes in Ramadan
|
|
|
- Jordan Hampton
- 5 years ago
- Views:
Transcription

1
2 2nd EASD Postgraduate Course on Clinical Diabetes and its Complications Shiraz, Iran, 2-4 March 2017 Managing diabetes in Ramadan Fereidoun Azizi, M.D. Farhad Hosseinpanah, M.D. Research institute for Endocrine Sciences Shahid Beheshti University of Medical Sciences Tehran, I.R. Iran
3 Objectives To review changes in metabolism of carbohydrates during fasting of Ramadan To present the evidence-based management of diabetic patients during Ramadan To discuss practical management of diabetic cases during Ramadan
4 Introduction There are over 1.6 billion Muslims world-wide, constituting 23% of the total global population Observance of Ramadan requires fasting from dawn to sunset, abstaining from eating and drinking during daylight hours, most Muslimsm will consume two meals each day The timing of Ramadan follows the lunar calendar, therefore the length of the fast varies depending on the time of year and the geographical location but is usually between hours.
5 Differences of fasting in Ramadan and experimental fasting 1. Intermittent in Ramadan 2. Fasting hours daily 3. Avoidance of liquid intake 4. Various effects of temperature in each region 5. Difference in food habits in various regions 6. Change in sleep pattern 7. Difference in aim of fasting and moral issues
6 Up to 79% of Muslims with diabetes fast for at least 15 days during Ramadan Salti I, Benard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004;27:
7 Introduction Globally it is estimated that 50 million Muslims with T2DM fast during Ramadan However, the proportion of those with T2DM who observe Ramadan varies considerably between 58% to 90% amongst different Islamic countries Salti I, et al. (2004) Diabetes care 27:
8 Introduction Many Muslims, even those who could seek exemption, have an intense desire to participate in fasting during Ramadan. Most of the guidance available for the management of diabetes during Ramadan represents expert opinion rather than medical evidence. Generating optimized Ramadan-specific treatment regimens for each patient is essential if a physician is to offer the best possible care.
9 Changes in Carbohydrates Metabolism During Fasting of Ramadan
10 Effects of fasting on glucose homeostasis in healthy individuals
11 Fasting state In a healthy individual, fasting causes the release of glucose from glycogen stores (glycogenolysis) and the formation of glucose from noncarbohydrate substrates (gluconeogenesis)
12 Fasting state Liver glycogen can provide enough glucose for the brain and peripheral tissues for around 12 hours. When glycogen stores are depleted and levels of insulin are low, fatty acids are released from adipocytes and oxidised to generate ketones,which can be used as fuel by many organs, preserving glucose for the brain and erythrocytes.
13
14 Carbohydrate metabolism in healthy persons Most of the studies show slight decrease in serum glucose (60 mg/dl to 70 mg/dl) occurs in normal adults Changes in serum glucose may occur in individuals depending upon food habits and individual differences in metabolism and energy regulation.

15
16 Fasting in Ramadan During Ramadan, each fasting period is often longer than 12 hours, most subjects who take their first meal at dawn are in a state of glycogen depletion by late afternoon, at which point ketogenesis occurs
17 Pathophysiology of fasting in patients with diabetes diabetes
18 Fasting in Type 1 During the fast, patients with T1DM may fail to secrete adequate levels of glucagon in response to hypoglycaemia, leading to further decreases in blood glucose levels In addition, as a result of autonomic neuropathy, some patients with DM may have a defective adrenaline response and therefore an inadequate response to hypoglycaemia.

19
20 Importance of sahur During longer fasting days of >16 h, which follow a rather heavy meal taken before dawn (Sahur), the stores of glycogen, along with some degree of gluconeogenesis, maintain serum glucose levels within normal limits. Since gluconeogenesis becomes the only source of glucose after h of fasting, it is recommended that observers of fasts do not skip Sahur, their predawn meal, because of the possibility of extended gluconeogenesis.


21 Changing in lifestyle during Ramadan Dietary Habits Daily Physical Activity Sleeping Pattern Glycemic Control Lipid Profile Weight & Dietary Intakes
22 Major risks associated with fasting in patients with diabetes Hypoglycemia Hyperglycemia Diabetic ketoacidosis Dehydration and thrombosis Diabetes Care 2004; 28: 2305 Al-Arouj et al. Diabetes Care 2010; 33: 1895

23 EPIDIAR study: mean numbers of severe glycemic events/month during Ramadan compared with before Ramadan Salti I, Benard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care 2004;27:
24 Evidence- Based Management of Diabetes During Ramadan


25
26 Education as a cornerstone for Ramadan diabetes management
27 Ramadan-focused diabetes education Ramadan-focused diabetes education is an extension of structured diabetes education aiming to give patients the knowledge to make informed decisions regarding their behavior and enabling them to effectively self-manage their condition. [1] enables patients with diabetes to maintain and improve glycemic control during and after fasting. [1] raises awareness of the risks associated with diabetes and fasting, and provides strategies to minimize them. [2] Education should be simple, engaging, and delivered with cultural sensitivity by well informed individuals. [2] 1) American Diabetes Association. 4. Foundations of care: Diabetes Care 2015;38:S ) IDF Diabetes and Ramadan guideline 2016; p:64. 1) American Diabetes Association. 4. Foundations of care: Diabetes Care 2015;38:S ) IDF Diabetes and Ramadan guideline 2016; p:64.


28 Targets of Ramadan-focused diabetes education Health Care Professionals General Public Patients with Diabetes IDF Diabetes and Ramadan guideline 2016; p:65
29 Key components of a Ramadan-focused educational program Risk quantification When to break the fast Medication adjustments Key components of a Ramadanfocused educational program Exercise advice Blood glucose monitoring Fluids and dietary advice IDF Diabetes and Ramadan guideline 2016; p:66

Al-Arouj M, et al. Update 2010. Diabetes Care 2010;33:1895-902. 2) Beshyah SA. IJMBS 2009;1:58-60.")
30 Key components of a Ramadan-focused educational program Risk Quantification Medical assessment: 6-8 weeks before Ramadan Risk quantification: The type of diabetes, current diabetes medication, individual social and work circumstances, individual hypoglycemic risk, self management capabilities and the presence of any complications and/or co-morbidities Risk Stratifications Providing advices: appropriate knowledge to minimize the risks [1,2,3] 1)Al-Arouj M, et al. Update Diabetes Care 2010;33: ) Beshyah SA. IJMBS 2009;1: ) IDF Diabetes and Ramadan guideline 2016; p:66.

31 Risk Quantification: IDF Diabetes and Ramedan guideline 2016; p:44


32 Category Red: Very High Risk IDF Diabetes and Ramedan guideline 2016,p:47


33 IDF Diabetes and Ramedan guideline 2016,p:47 Category Yellow: High Risk


34 Category Green: Moderate/low risk IDF Diabetes and Ramedan guideline 2016,p:47
35 Key components of a Ramadan-focused educational program Blood glucose monitoring Pricking the skin for blood glucose testing does not invalidate the Ramadan fast. [1] Having the skills to do SMBG can empower patients with diabetes to effectively self-manage their disease. [2] The frequency of SMBG depends on many factors including the type of diabetes and current medications but should be carried out regularly by all: moderate or low risk: once or twice a day high or very high risk: several times a day Patients should check blood glucose levels whenever they experience symptoms of hypoglycemia. [2] 1) Masood S, et al. Diabetes Care 2014;37:e ) IDF Diabetes and Ramadan guideline 2016; p:66.
36 Recommended timings to check blood glucose levels during Ramadan fasting IDF, Diabetes and Ramadan: Practical Guidelines, April 2016
 Include low glycemic index, high fiber foods that release energy slowly before and after fasting (granary bread, beans,")
37 Key components of a Ramadan-focused educational program Fluids and dietary advice Divide daily calories between Suhoor and Iftar, plus 1 2 snacks if necessary Ensure meals are well balanced 45 50% carbohydrate 20 30% protein <35% fat (preferably mono- and polyunsaturated) Include low glycemic index, high fiber foods that release energy slowly before and after fasting (granary bread, beans, rice, ) Keep hydrated between sunset and sunrise by drinking water or other nonsweetened beverages Minimize foods that are high in saturated fats (ghee, samosas, pakoras, ) Use small amounts of oil when cooking (olive, rapeseed) Include plenty of fruit, vegetables and salads Avoid caffeinated and sweetened drinks Avoid sugary desserts IDF Diabetes and Ramadan guideline 2016; p:66.
 IDF Diabetes and Ramadan guideline")
38 Key components of a Ramadan-focused educational program Exercise Maintain normal level of physical activity Beware that excessive physical activity may increase risk of hypoglycemia (especially before Iftar) IDF Diabetes and Ramadan guideline 2016; p:66.
39 Individualization of treatment options Pre-Ramadan patient assessment Medication adjustment during Ramadan Post-Ramadan follow-up
:639-48 Medicine Volume 95,")
40 Diabetes Obes Metab Jul;17(7): Medicine Volume 95, Number 2, January 2016
41 To determine which non-insulin glucose lowering treatment regimens : are most appropriate in people with type 2 diabetes who choose to fast during Ramadan Sixteen studies included; nine RCTs(2,927 participants) and seven observational studies(1,775 participants) Diabetes Obes Metab Jul;17(7):639-48
42 Outcomes Number of participants having one or more hypoglycemic episodes during Ramadan Number of participants having one or more severe hypoglycemia episodes during Ramadan HbA1c change post Ramadan Weight change post ramadan Ramadan

43
44 Key messages This systematic review and meta-analysis suggests that DPP-4 inhibitors and possibly GLP-1 receptor agonists could be used during Ramadan over sulfonylureas for fewer hypoglycemic episodes and a greater reduction in weight and possibly HbA1c. The results should be interpreted with caution however given the variable quality of the studies included
45 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
46 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM

47
48 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM

49
50 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM


51
52 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
53 Short-acting insulin secretagogues In two small observational studies, no hypoglycemic events were reported in patients treated with repaglinide during Ramadan, while a third demonstrated no difference in hypoglycemia when compared with insulin glargine or glimepiride, a sulphonylurea (SU) therapy In two randomized parallel-group trials, a low incidence of hypoglycemic events was associated with repaglinide treatment during Ramadan, occurring in similar proportions of patients treated with glibenclamide and glimepiride.

54 Short-acting insulin secretagogues The short duration of action of these agents make them appealing for use during Ramadan as they can be taken before iftar and suhoor and carry a low risk of hypoglycemia
55 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfonylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
56 Sulfonylureas SUs are widely used as second-line treatment for T2DM after metformin and so there is a wealth of evidence and experience with this low cost efficacious drug class
 followed by glimepiride (16.8%) and gliclazide (14.")
57 Sulfonylureas In a multinational observational study of 1,378 patients with T2DM treated with SUs, approximately one fifth of patients experienced a symptomatic hypoglycemic event during Ramadan. When this was broken down by drug, the highest incidence was associated with glibenclamide (25.6%) followed by glimepiride (16.8%) and gliclazide (14.0%)
58 Sulfonylureas More recent SUs such as glimepiride, glipizide and gliclazide are therefore preferred over conventional SUs, such as glibenclamide, because of their more favorable safety profile in terms of hypoglycemia To date, no trials have been conducted looking at the modified-release formulation of gliclazide during Ramadan
59
60 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
61

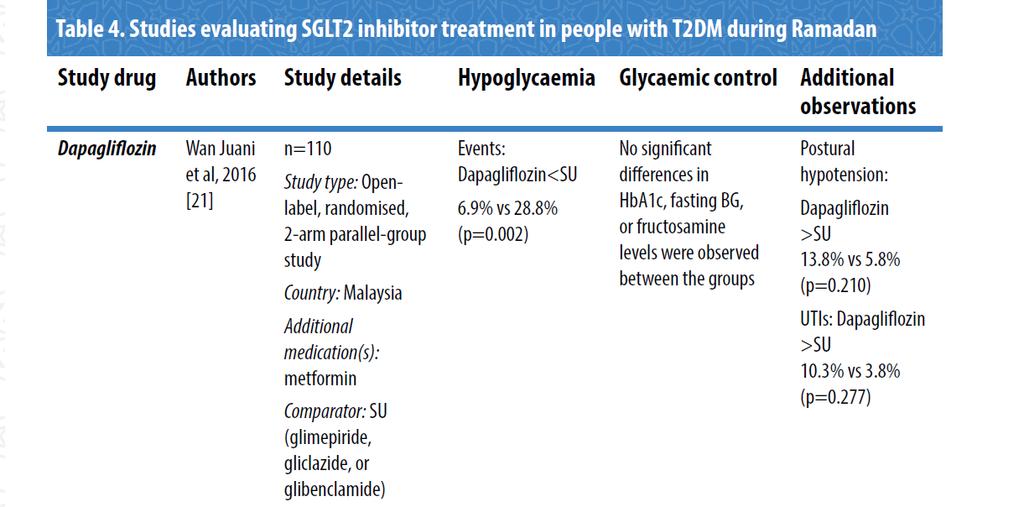
62 SGLT2 inhibitors Further studies are warranted in order to prove the efficacy and safety of SGLT2 inhibitors during Ramadan Those that are deemed more at risk of complications such as the elderly, patients with renal impairment, hypotensive individuals, those at risk of dehydration or those taking diuretics should not be treated with SGLT2 inhibitors
63 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
64 DPP4 inhibitors Four RCTs and five observational studies have examined the efficacy and safety of DPP-4 inhibitor treatment during Ramadan Specifically, the four RCTs examined the effects of switching from SU therapy to either vildagliptin or sitagliptin prior to Ramadan compared with continuing on SU. The largest of these studies compared the incidence of selfreported hypoglycaemic events in 1,066 patients with T2DM treated with sitagliptin or SUs during Ramadan. Overall, the risk of hypoglycemia significantly decreased on the sitagliptin-based regimen compared to continuing with SU treatment (relative risk ratio [95% CI]= 0.51[0.34, 0.75]; p<0.001)
65 DPP4 inhibitors The results of the studies described above indicate that vildagliptin is effective in improving glycemic control and that both vildagliptin and sitagliptin are associated with low rates of hypoglycemia during fasting, making them attractive treatment options during Ramadan. These drugs do not require any treatment modifications during Ramadan
66 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
67
68

69 GLP-1 Ras These studies demonstrate that liraglutide is safe as an add-on treatment to metformin and can be effective in reducing weight and HbA1c levels during Ramadan. Data on exenatide is limited to one study but the short duration of action and dosing of exenatide suggest that, like liraglutide, the risk of hypoglycemia during Ramadan is low.
70 Pharmacological management of people with T2DM Metformin Acarbose TZDs Short-acting insulin secretagogues Sulfunylureas SGLT2 inhibitors DPP4 inhibitors GLP-1 Ras Insulin treatment for T2DM
71 Insulin treatment for T2DM Insulin use during prolonged fasting carries an increased risk of hypoglycemia, particularly for those with T1DM but also for those with T2DM. The use of insulin analogues is recommended over regular human insulin due to a number of advantages that include less hypoglycemia Although a number of small randomized trials and observational studies have been conducted to assess some insulin regimens during Ramadan, large RCT data in this area are lacking.

72 Insulin treatment for T2DM There are limited data available regarding the optimal insulin type or regimen for patients with T2DM during Ramadan but results from the studies described above indicate it may be safe to fast while on insulin, however treatment must be appropriately individualized

73

74
75 Individualization of treatment options Pre-Ramadan patient assessment Medication adjustment during Ramadan Post-Ramadan follow-up
76 Post-Ramadan follow-up Patients with diabetes should be made aware of the risks of overindulgence during this time A post- Ramadan follow-up meeting with HCPs is advisable in order to discuss medication and regimen readjustments and assess how the patient handled the fasting It should be stressed to the patient that a safe fast one year does not automatically make them a low risk for the next year due to the progressive nature of the disease
77 Recommendations for prevention of hypoglycaemia during Ramadan Blood glucose monitoring Record blood glucose to determine pattern of hypoglycaemia Medication adjustment (1-2 month before) Avoid skipping Sahur meals Avoid strenuous physical activity during fasting Breaking fast if there is hypoglycaemia

78 Key components of a Ramadan-focused educational program When to break the fast? IDF Diabetes and Ramadan guideline 2016; p:66
79 Conclusion Diabetics with complications and those who are high risk should not fast Diabetics must visit the physician at least one month prior to Ramadan Only those with appropriate diets and physical activity, having controlled diabetes could fast during Ramadan Patient education must be conducted before entering Ramadan Management of diabetics in Ramadan is a good example of Patient Centered Care (PCC). Appropriate self management is the key to Ramadan fasting for diabetics.

80
Diabetes and Ramadan: Practical guidelines
 Diabetes and Ramadan: Practical guidelines 1. Introduction Fasting during Ramadan is one of the five pillars of Islam and is obligatory for all healthy adult Muslims. The timing of Ramadan is based on
Diabetes and Ramadan: Practical guidelines 1. Introduction Fasting during Ramadan is one of the five pillars of Islam and is obligatory for all healthy adult Muslims. The timing of Ramadan is based on
Diabetes and Ramadan: A Challenge and an Opportunity?
 Diabetes and Ramadan: A Challenge and an Opportunity? Dr Mohamed Hassanein Endocrinology Department, Dubai Hospital, UAE Chair of DAR International Alliance H Senior Lecturer, Cardiff University, UK mhassanein148@hotmail.com
Diabetes and Ramadan: A Challenge and an Opportunity? Dr Mohamed Hassanein Endocrinology Department, Dubai Hospital, UAE Chair of DAR International Alliance H Senior Lecturer, Cardiff University, UK mhassanein148@hotmail.com
DIABETES AND RAMADAN FASTING
 DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر
 بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر فليصمه Najat Buzaid Introduction Ramadan is a lunar-based month, and its duration varies between 29 and 30 days. The fasting hours vary from 10 hours in a temperature
بسم اهلل الرمحن الرحيم فمن شهد منكم الشهر فليصمه Najat Buzaid Introduction Ramadan is a lunar-based month, and its duration varies between 29 and 30 days. The fasting hours vary from 10 hours in a temperature
Ramadaan and Diabetes : South Africa
 Ramadaan and Diabetes : South Africa M.A.K. Omar Dept. of Diabetes and Endocrinology Nelson R Mandela School of Medicine University of KwaZulu Natal South Africa Conflict of Interest Statement - Nil Acted
Ramadaan and Diabetes : South Africa M.A.K. Omar Dept. of Diabetes and Endocrinology Nelson R Mandela School of Medicine University of KwaZulu Natal South Africa Conflict of Interest Statement - Nil Acted
Between health and faith - Managing diabetes during Ramadan. Ahmed Hussein Endocrine and Diabetes Registrar Blacktown-Mt Druitt Hospital
 Between health and faith - Managing diabetes during Ramadan Ahmed Hussein Endocrine and Diabetes Registrar Blacktown-Mt Druitt Hospital Acknowledgment Dr Ibrahim Abu Muhammed Grand Mufti of Australia Professor
Between health and faith - Managing diabetes during Ramadan Ahmed Hussein Endocrine and Diabetes Registrar Blacktown-Mt Druitt Hospital Acknowledgment Dr Ibrahim Abu Muhammed Grand Mufti of Australia Professor
THE FACTS ABOUT FASTING DURING RAMADAN FOR PEOPLE WITH TYPE 2 DIABETES
 THE FACTS ABOUT FASTING DURING RAMADAN FOR PEOPLE WITH TYPE 2 DIABETES 1 Introduction Ramadan; one of the five pillars of Islam Fasting is an important spiritual aspect of many religions. The Islamic month
THE FACTS ABOUT FASTING DURING RAMADAN FOR PEOPLE WITH TYPE 2 DIABETES 1 Introduction Ramadan; one of the five pillars of Islam Fasting is an important spiritual aspect of many religions. The Islamic month
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Chapter 4. Risk Stratification of Individuals with Diabetes before Ramadan Monira Al-Arouj, Abdullah Ben-Nakhi & Mohamed Hassanein
 Chapter 4. Risk Stratification of Individuals with Diabetes before Ramadan Monira Al-Arouj, Abdullah Ben-Nakhi & Mohamed Hassanein 41 4.1 Risks associated with fasting in people with diabetes During Ramadan,
Chapter 4. Risk Stratification of Individuals with Diabetes before Ramadan Monira Al-Arouj, Abdullah Ben-Nakhi & Mohamed Hassanein 41 4.1 Risks associated with fasting in people with diabetes During Ramadan,
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Chapter 1. Introduction to the IDF-DAR Practical Guidelines
 Chapter 1. Introduction to the IDF-DAR Practical Guidelines Mohamed Hassanein, Khalifa Abdallah & Mehmet Akif Buyukbese 7 1.1 Ramadan fasting regulations Fasting during Ramadan is one of the five pillars
Chapter 1. Introduction to the IDF-DAR Practical Guidelines Mohamed Hassanein, Khalifa Abdallah & Mehmet Akif Buyukbese 7 1.1 Ramadan fasting regulations Fasting during Ramadan is one of the five pillars
THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES
 THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES INTRODUCTION This information kit is designed to provide you with facts and practical advice about fasting during
THE FACTS ABOUT FASTING DURING RAMADAN INFORMATION KIT FOR PEOPLE WITH TYPE 2 DIABETES INTRODUCTION This information kit is designed to provide you with facts and practical advice about fasting during
Guidelines for managing diabetes in Ramadan
 Guidelines for managing diabetes in Ramadan Sarah Ali 1, Melanie J Davies 2,3, Emer M Brady 3, Laura J Gray 4,, Kamlesh Khunti 2,3, Salem A Beshyah 5, Wasim Hanif 6 1. Department of Diabetes & Endocrinology,
Guidelines for managing diabetes in Ramadan Sarah Ali 1, Melanie J Davies 2,3, Emer M Brady 3, Laura J Gray 4,, Kamlesh Khunti 2,3, Salem A Beshyah 5, Wasim Hanif 6 1. Department of Diabetes & Endocrinology,
Sitagliptin: A component of incretin based therapy. Rezvan Salehidoost, M.D., Endocrinologist
 Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
PLEASE CHECK FULL SPECIFIC PRODUCT CHARACTERISTICS FOR MORE DETAILED AND CURRENT INFORMATION:
 Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
Metformin Standard tablets Modified-release tablets Metformin 1g sachets Metformin liquid 500mg/5ml (avoid use as expensive) < 2.00 5.32 for 56 tabs 500mg 13.16 for 60 sachets > 120 Ketoacidosis General
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Fasting and Diabetes: An experience with safety of fasting in peoples with type II diabetes
 : An experience with safety of fasting in peoples with type II diabetes Ahmed Bilal 1, Muhammad Sohail Anjum 2, Zaheer Ahmed 3 1 Chief Endocrinologist and Professor of Medicine, Head of Medical Unit II,
: An experience with safety of fasting in peoples with type II diabetes Ahmed Bilal 1, Muhammad Sohail Anjum 2, Zaheer Ahmed 3 1 Chief Endocrinologist and Professor of Medicine, Head of Medical Unit II,
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption),
,") Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Management of Diabetes in Ramadan Fasting
 REVIEW ARTICLE Management of Diabetes in Ramadan Fasting Masoud Rahmanian 1*, Fateme Sadat Haghighi 2, Nasim Namiranian 3 1. Assistant Professor of Yazd Diabetes Research Center, Shahid Sadoughi University
REVIEW ARTICLE Management of Diabetes in Ramadan Fasting Masoud Rahmanian 1*, Fateme Sadat Haghighi 2, Nasim Namiranian 3 1. Assistant Professor of Yazd Diabetes Research Center, Shahid Sadoughi University
Ramadan. Health Advice
 Ramadan Health Advice Background The Holy month of Ramadan is the ninth month of the Islamic calendar in which Muslim adults observe the fast from dawn to sunset every year. Muslims observing the fast
Ramadan Health Advice Background The Holy month of Ramadan is the ninth month of the Islamic calendar in which Muslim adults observe the fast from dawn to sunset every year. Muslims observing the fast
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND THE OLDER ADULT Objectives u At conclusion of the presentation the participant will: 1. Discuss challenges to glycemic control unique in the older population
Diabetes Management in New Brunswick Nursing Homes
 Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
WHO Guidelines for Management of Diabetes in Low Resource Settings
 WHO Guidelines for Management of Diabetes in Low Resource Settings 24 th November, 2018 Dr. Alok Shetty K Senior Resident Department of Medicine St. John s Medical College & Hospital WHO vs ADA-EASD Revisiting
WHO Guidelines for Management of Diabetes in Low Resource Settings 24 th November, 2018 Dr. Alok Shetty K Senior Resident Department of Medicine St. John s Medical College & Hospital WHO vs ADA-EASD Revisiting
Nutritional Recommendations for the Diabetes Managements
 In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes
 in combination with basal insulin for type 2 diabetes") Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals
 Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals 1. Which one of the agents listed here is widely considered the first-line therapy in type 2 diabetes
Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals 1. Which one of the agents listed here is widely considered the first-line therapy in type 2 diabetes
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Managing your Diabetes during Ramadan
 Managing your Diabetes during Ramadan A Guide for Patients Introduction The holy month of Ramadan is a period of prayer, routine work, and charitable activities, with strict fasting where no food or drink
Managing your Diabetes during Ramadan A Guide for Patients Introduction The holy month of Ramadan is a period of prayer, routine work, and charitable activities, with strict fasting where no food or drink
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, :15 a.m. 11:00 a.m.
 Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
The effects of long term fasting in Ramadan on glucose regulation in type 2 Diabetes Mellitus
 European Review for Medical and Pharmacological Sciences The effects of long term fasting in Ramadan on glucose regulation in type 2 Diabetes Mellitus C. KARATOPRAK, S. YOLBAS, M. CAKIRCA, A. CINAR, M.
European Review for Medical and Pharmacological Sciences The effects of long term fasting in Ramadan on glucose regulation in type 2 Diabetes Mellitus C. KARATOPRAK, S. YOLBAS, M. CAKIRCA, A. CINAR, M.
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Questions may not always match the order of those online. Please be sure to read the questions when completing the online test.
 Module 13 Part 1 Questions may not always match the order of those online. Please Case #1 Fred W. Fred W. is in to see you for a referral from his family physician. In the referral letter, the family physician
Module 13 Part 1 Questions may not always match the order of those online. Please Case #1 Fred W. Fred W. is in to see you for a referral from his family physician. In the referral letter, the family physician
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Diabetes Mellitus. Medical Management and Latest Developments Dr Ahmad Abou-Saleh
 Diabetes Mellitus Medical Management and Latest Developments Dr Ahmad Abou-Saleh What is Diabetes Mellitus? A disease characterised by a state of chronic elevation of blood glucose levels due to: - The
Diabetes Mellitus Medical Management and Latest Developments Dr Ahmad Abou-Saleh What is Diabetes Mellitus? A disease characterised by a state of chronic elevation of blood glucose levels due to: - The
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
National Horizon Scanning Centre. Saxagliptin (BMS ) for type 2 diabetes. April 2008
 for type 2 diabetes. April 2008") Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY
 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
Diabetes Mellitus and Ramadan: Physiopathological, Clinical and Therapeutic Aspects
 Cloud Publications International Journal of Advanced Nutritional and Health Science 2017, Volume 5, Issue 1, pp. 256-265 ISSN 2348-5140, Crossref: 10.23953/cloud.ijanhs.322 Review Article Diabetes Mellitus
Cloud Publications International Journal of Advanced Nutritional and Health Science 2017, Volume 5, Issue 1, pp. 256-265 ISSN 2348-5140, Crossref: 10.23953/cloud.ijanhs.322 Review Article Diabetes Mellitus
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
British Islamic Medical Association (BIMA) presents. Healthy Ramadan. Name of Speaker
 presents. Healthy Ramadan. Name of Speaker") British Islamic Medical Association (BIMA) presents Healthy Ramadan Name of Speaker Special thanks Dr M Ali Karamat (Consultant Endocrinologist) Dr Ateeq Syed (Consultant Endocrinologist) Dr Ahmed Helmy
British Islamic Medical Association (BIMA) presents Healthy Ramadan Name of Speaker Special thanks Dr M Ali Karamat (Consultant Endocrinologist) Dr Ateeq Syed (Consultant Endocrinologist) Dr Ahmed Helmy
Type Two Diabetes Mellitus Prescribing in New Zealand - What are we dispensing?
 Type Two Diabetes Mellitus Prescribing in New Zealand - What are we dispensing? Dr Bryan Betty Deputy Medical Director PHARMAC GP Cannons Creek, East Porirua Type 2 Diabetes in NZ: The Numbers 250,000
Type Two Diabetes Mellitus Prescribing in New Zealand - What are we dispensing? Dr Bryan Betty Deputy Medical Director PHARMAC GP Cannons Creek, East Porirua Type 2 Diabetes in NZ: The Numbers 250,000
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
FASTING DURING RAMADAN
 FASTING DURING RAMADAN Dr Neesha Patel University of Manchester 21 st May 2014 Accrington Sponsored by Sanofi Key Objectives By the end of this session you will understand and learn about: Importance of
FASTING DURING RAMADAN Dr Neesha Patel University of Manchester 21 st May 2014 Accrington Sponsored by Sanofi Key Objectives By the end of this session you will understand and learn about: Importance of
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
VICTOSA and Renal impairment DR.R.S.SAJAD
 VICTOSA and Renal impairment DR.R.S.SAJAD February 2019 Main effect of GLP-1 is : Stimulating glucose dependent insulin release from the pancreatic islets. Slow gastric emptying Inhibit inappropriate
VICTOSA and Renal impairment DR.R.S.SAJAD February 2019 Main effect of GLP-1 is : Stimulating glucose dependent insulin release from the pancreatic islets. Slow gastric emptying Inhibit inappropriate
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Initial Mono Versus Combination Therapy for Type 2 Diabetes
 Initial Mono Versus Combination Therapy for Type 2 Diabetes The Case for Combination Therapy ALAN J. GARBER, MD, PHD, FACE Professor Departments of Medicine, Biochemistry, Molecular and Cellular Biology
Initial Mono Versus Combination Therapy for Type 2 Diabetes The Case for Combination Therapy ALAN J. GARBER, MD, PHD, FACE Professor Departments of Medicine, Biochemistry, Molecular and Cellular Biology
Xultophy 100/3.6. (insulin degludec, liraglutide) New Product Slideshow
 New Product Slideshow") Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION
 OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca
 SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca") dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 September 2012 (Issued 07 December 2012) The Scottish Medicines Consortium (SMC) has completed
dapagliflozin 5mg and 10mg film-coated tablets (Forxiga ) SMC No. (799/12) Bristol-Myers Squibb / AstraZeneca 07 September 2012 (Issued 07 December 2012) The Scottish Medicines Consortium (SMC) has completed
Chapter 1: Food, Nutrition, and Health Test Bank
 Chapter 1: Food, Nutrition, and Health Test Bank MULTIPLE CHOICE 1. Promoting a health care service that improves diabetes management for the elderly in a community would assist in which of the following?
Chapter 1: Food, Nutrition, and Health Test Bank MULTIPLE CHOICE 1. Promoting a health care service that improves diabetes management for the elderly in a community would assist in which of the following?
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Diabetes Mellitus. Raja Nursing Instructor. Acknowledgement: Badil 09/03/2016
 Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
What systems are involved in homeostatic regulation (give an example)?
?") 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
Case Study. Patient Profile. Baseline Report - Daily Patterns. Insights
 Case Study Patient Profile Sex/Age: Male, elderly Disease diagnosis: Type 2 for the past 30 years, recurrent episodes of hunger HbA1c: 6.2% Diabetes medication profile: DPP-4 inhibitor 50 mg twice a day,
Case Study Patient Profile Sex/Age: Male, elderly Disease diagnosis: Type 2 for the past 30 years, recurrent episodes of hunger HbA1c: 6.2% Diabetes medication profile: DPP-4 inhibitor 50 mg twice a day,
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including