Diabetes Management in New Brunswick Nursing Homes
|
|
|
- Gervais Stafford
- 5 years ago
- Views:
Transcription


1 Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016
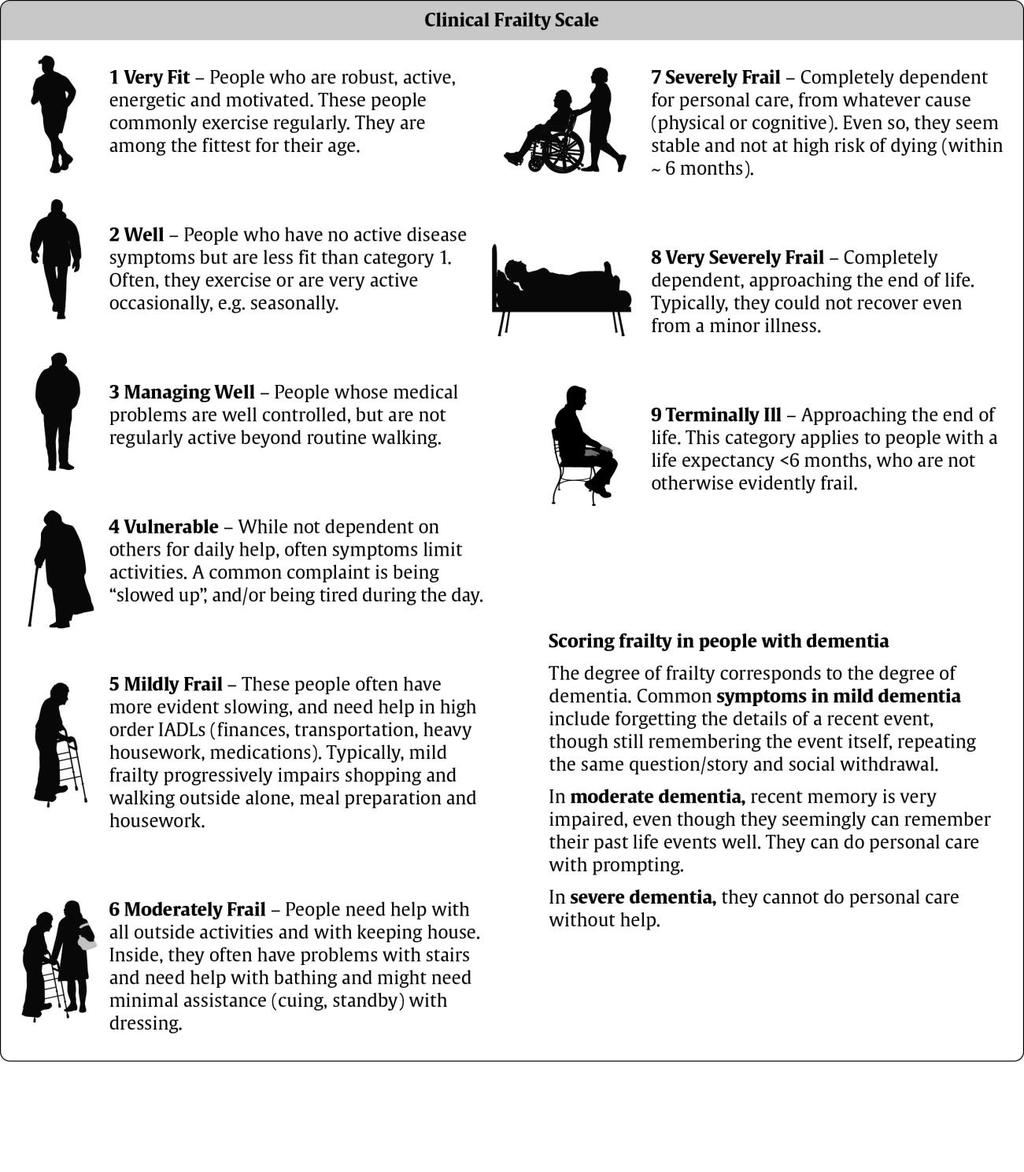
2 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with diabetes living in LTC facilities. The current complex care of diabetes has made it difficult to transition to appropriate goals and targets in this population which may have multiple comorbidities. In nursing homes, people with diabetes may range from those with limited functional dependence to those who are at the end of their life with a goal of palliation and comfort. Aggressive management of diabetes to avoid long term complication is no longer relevant for some. This document is meant to provide suggestions for those who care for New Brunswick residents living in nursing homes with the following purpose: 1. To ensure resident safety and quality of life is balanced with optimal diabetes management requirements, 2. To allow individualized care plans based on current knowledge, best practices and guidelines, 3. To recognize and avoid symptomatic hypoglycemia, 4. To avoid symptomatic hyperglycemia, 5. To allow rational glucose monitoring protocols when stable and increased monitoring when appropriate, 6. To optimize diabetes medication choices and insulin management practices Preparation of this document is based on several national guidelines including the Canadian Diabetes Association Clinical Practice Guidelines (CPGs) (1), American Diabetes Association guidelines (2) and International Diabetes Federation guidelines (3). The differences of development and recommendations in these three documents have been outlined by Sherifeli et al (4). In addition, there have been several provincial documents including those from Nova Scotia, Prince Edward Island, Newfoundland and Ontario that have been used as guides. In addition, there may be individual programs or facilities with guidelines, such as the Best Practice guidelines developed for alternate level of care patients in Saint John Regional Hospital. The Canadian Diabetes Association CPGs have utilized the Clinical Frailty Scale (Appendix A) to help clinicians identify those who are elderly with significant functional impairment (Moderately Frail level 6, Severely Frail level 7 or Very Severely Frail level 8) and whom a higher A1c (and blood glucose) is not only acceptable, but desired. The higher A1c target is most relevant for those residents on insulin or sulphonylureas who may have unacceptable hypoglycemia risk with tighter control and, in whom, medications may need to be reduced or stopped. As a great many residents with diabetes are managed with lifestyle or Metformin, the main intervention to avoid hypoglycemia is to liberalize the diet for the frail elderly (1). A review of New Brunswick prescription drug program for nursing homes in 2013 showed over 4000 residents with diabetes in nursing homes with 50% on diet or oral agents only. Approximately 50% of nursing home residents with diabetes are on insulin alone (30%) or in combination with oral agent (20%) and between 25 and 30% of these have an A1c <7% (Stuart Halpine, personal communication). A survey of Anglophone nursing homes showed that >50% of nursing homes allow sliding scale insulin for treatment of diabetes, 32% have no facility standing orders for diabetes glucose monitoring and 70% feel that provincial recommendation would be useful (McGibbon and Nicholson, unpublished results). Osman et al (5) have identified nursing time and knowledge as barriers to achieving individualized targets and goals for these residents in the frail elderly. This document will briefly summarize the recommendations for glucose monitoring, A1c use and targets, hypoglycemia, blood pressure and lipids, and some suggestions for optimizing medications and insulin management. This is not a comprehensive clinical guide for diabetes in the elderly and does not take the place of clinical and individualized assessment. It is meant to provide the care team with resources to make decisions appropriate for individual residents. 2
3 1. Rational Glucose monitoring Blood glucose monitoring is a key component of self-management behaviours instructed to patients with diabetes. Rational glucose monitoring refers to monitoring or checking the blood glucose only when the information will aid in decision making; such as how much insulin to take, effects of certain diet choices, assessing hyper or hypoglycemia with symptoms and for decision around treatment effectiveness. A blood glucose in people without diabetes may range from mmol/l. In those with diabetes, the expected or desired blood glucoses vary and will fluctuate depending illness, activity, pain, food intake, stress and other factors. Typically blood glucoses in the mid-teens can be associated with increased polyuria, the risk of dehydration and impaired wound healing. The suggested frequency of rational glucose monitoring has been reviewed by Canadian Association of Drugs and Therapeutics (CADTH) and the Canadian Diabetes Association. Suggested use of this information in the nursing home population (based on medical stability, clinical frailty index and treatment regimen) is summarized in Table 1. Suggestions for when to reassess the treatment schedule are offered. TABLE 1: Patient Description Clinical Frailty Scale >6 AND medically stable Clinical Frailty Scale > 6 and unwell/sick Clinical Frailty Scale 9 or active palliation/ end of life care Diabetes Management Categories Diet alone Metformin or DPP4 i.e. (Glucophage, Glumetza, Januvia, Onglyza, Trajenta ) Sulfonylureas i.e. Gliclazide (Diamicron ), Glimepiride (Amaryl ) Repaglanide (Gluconorm ) Insulin Once or twice daily injections Insulin - Multiple daily dose injections (not sliding scale) ANY ANY Recommendations for Blood Glucose Monitoring No blood glucose monitoring required unless symptomatic of hypoglycemia or hyperglycemia No blood glucose monitoring required unless symptomatic Once daily at alternating times initially and less frequently if stable. +Once or * twice daily at alternating times when stable. May require TID or QID monitoring when insulin adjustments are being made. *Twice daily alternating times, before meals. May require TID or QID monitoring when insulin adjustments are being made. Increase glucose monitoring to twice a day for 48 hours to rule out hyperglycemia or hypoglycemia. No glucose monitoring unless symptomatic (ex: shaking and tremulous, or thirsty and unusual urinary incontinence) Reassess when: glucose > 18 mmol/l More than one hypoglycemia event or persistent blood glucose > 18 mmol/l Example of: + Once daily alternating times = Day 1 before breakfast Day 2 before lunch Day 3 before supper Day 4 at bedtime 3
4 * Twice daily alternating times = Day 1 before breakfast and before supper Day 2 before lunch and at bedtime 2. A1c Use and Targets The A1c is not reliable in the older population for several reasons including renal dysfunction, a change in red blood cell turnover and other metabolic factors. A1c monitoring is generally not useful for those who meet a clinical frailty score of >8 or 9 or who have a very short life expectancy as the A1c is used primarily as predictor of long term complications. A low A1c in the elderly patient on diet alone is likely not clinically relevant (especially if the diet has been liberalized) and may signify declining renal or liver function if hypoglycemia is present. In those elderly residents who are on metformin, a low A1c (< 7-8%) is usually acceptable unless there are episodes of hypoglycemia or GI upset in which case the metformin should be reduced or discontinued. Given the potential for serious or prolonged hypoglycemia in elderly on sulphonylureas or insulin, the A1c target is most appropriately higher to avoid hypoglycemia. For those in whom an A1c is being used to assess glycemic control, the recommended A1c is approximately 8.5% (1, 2, 3). A higher A1c is acceptable in order to avoid hypoglycemia. For those on medications or insulin, consider liberalizing diet and reducing or stopping some medications or insulin when the A1c is < 8.0, particularly when there has been hypoglycemia symptoms. The optimal frequency of A1c monitoring is not known in LTC residents. In the absence of symptoms or changing treatment regimens, A1c monitoring may be done once every 6 months or even annually if stable. In some cases (very severely frail or terminally ill patients) the A1c will add little to the patients care and does not need to be tested. 3. Hypoglycemia Hypoglycemia is an important complication of diabetes management and must be avoided in nursing home residents. Hypoglycemia is defined as a blood glucose <4.0 in most people with diabetes but for some, symptoms occur at a higher blood glucose and should also be avoided. In nursing home residents on sulphonylureas or insulin, a blood glucose <5.0 may represent hypoglycemia. Residents on sulphonylureas may have prolonged hypoglycemia, particularly when there is declining renal function. Hypoglycemia is difficult to recognize in the elderly person, particularly those with cognitive impairment. Common symptoms of hypoglycemia are diaphoresis, trembling/shaking and confusion. Any change in resident behaviour may indicate abnormal blood glucose. A poster developed by CADTH and Western Health in Newfoundland to help recognize hypoglycemia is found in Appendix B. LTC facilities ideally have a hypoglycemia protocol for blood glucose less than 5.0 mmol/l. This does not apply to residents treated with lifestyle or diet treatment, however if these residents have frequent hypoglycemia, they should have a medical review. An example of a protocol for hypoglycemia is: Hypoglycemia protocol for residents with blood glucose <5.0 mmol/l with symptoms: For conscious patient who is able to take treatment orally: 20 g fast-acting carbohydrate (i.e. 250 ml unsweetened apple juice) Retest blood glucose in 15 minutes, If less than 5 mmol/l, treat with 20 g fast acting carbohydrate again Repeat every 15 minutes until blood glucose is greater than 5 mmol/l 4
5 Give protein and carbohydrate snack (2 tablespoons peanut butter or 1 ounce (30g) cheese or meat/fish along with 7 crackers or 1 slice of bread or 1 small muffin) if meal is greater than 30 minutes away For unconscious patient or patient unable to treatment orally: Give glucagon 1 mg subcutaneous x 1, check glucose in 15 minutes, repeat if necessary Notify physician if hypoglycemia persists 4. Blood Pressure and Lipids Nursing Home residents with diabetes have higher cardiovascular risk profiles and may benefit from treatment for hypertension however this must be balanced with the adverse events associated with drops in blood pressure including falls. The recommended blood pressure target for most frail elderly is <150/90. Statins should be considered if there is likely benefit from prevention of complications from dyslipidemia, particularly in regard to secondary prevention with a target LDL < 2.0 mg/dl (or 50% reduction from original LDL). In residents with dementia, lipid-lowering therapy may not be appropriate, especially if dementia is non-vascular in nature. 5. Optimizing Medications and insulin management Medication choices for the elderly available through the NB drug program coverage are: Medications Insulin Covered Metformin (Glucophage) Glyburide (Diabeta) Gliclazide (Diamicron and Diamicron MR) Glimepiride (Amaryl) Acarbose (Prandase) (*chlorpropamide, tolbutamide) Regular insulin Intermediate Acting insulin Premixed (30/70, 40/60 and 50/50) With Special Authorization Combination Metformin and Sitagliptin (Janumet) Sitagliptin (Januvia) Repaglanide (Gluconorm) Canaglifozin (Invokana) (**rosiglitazone and pioglitazone) Rapid acting insulin Basal analogues *Chlorpropamide and Tolbutamide older sulphonylures with a very high risk of hypoglycemia which should not be used in the LTC population. Glyburide is associated with a higher hypoglycemia risk than the other choices. **Rosiglitazone and Pioglitazone may be associated with weight gain, fluid retention, heart failure and other adverse effects. Generally not used except in younger patients with early diabetes. Metformin is first line therapy, but may cause nausea, GI upset or diarrhea. It should not be used in the setting of heart failure or renal disease (elevated creatinine) but does not cause hypoglycemia. Metformin doses may be reduced or stopped in the resident who has GI symptoms or changes in renal function. Gliclazide, Glimepiride and Repaglanide are sulphonylureas or insulin secretagogues which may cause hypoglycemia in residents with advanced renal failure or impaired oral intake. Acarbose can result in a small glucose reduction but is poorly tolerated. 5
6 Newer classes of oral medications may be approved with special authorization and the DPP4 class (such as Sitagliptin) has some potential benefits as the risk of hypoglycemia is low and there are generally few limiting side effects. The SGLT2 class (such as Canagliflozin) has not been well studied in the elderly person and may cause hypotension including postural hypotension; it would not be recommended for most residents in nursing homes. Many residents with type 2 diabetes (>95% of those with diabetes in LTC) and a consistent schedule can be well managed on the older regular and intermediate acting insulins. There may be some advantages to the simple twice daily schedule of premixed insulins; however, these are unlikely to result in glucose management that would meet targets for the healthy elderly. With special authorization, insulin analogues (humulog, novorapid, apridra, lantus and detemir ) may be considered, but the advantages in the elderly, clinically frail population are not clear (1). Proper insulin injection technique and regular site rotations are an important part of managing diabetes with insulin. Sliding scale insulin is not recommended for nursing home residents as a primary means of glucose management. There may be situations where a corrective dose of short acting insulin is appropriate for some residents who are otherwise well, have type 1 diabetes, or are having their blood glucose monitored regularly in order to make decisions about insulin dosing or during illness. The decision regarding the most appropriate medication or insulin treatments for the resident with diabetes in nursing homes can be difficult and is typically based on hypoglycemia risk, coverage, side effect profile and renal function. Residents with Type 1 diabetes, or insulin dependent diabetes, will always need some basal or long acting insulin even if the resident is not eating well. Residents with type 2 diabetes who refuse or skip meals may need to have sulphonylureas and insulin held or reduced temporarily or long term if there is a major decline in appetite or intake. Likewise, declining renal function often requires adjustment in medications (6). Metformin should be used with caution and at a reduced dose when CrCl is less than 60 and discontinued when Cr Cl is less than 30. Glyburide is used with caution at Cr Cl < 50 and should be discontinued when Cr Cl is less than 30 (see Appendix C). 6. Summary The goals and management strategies for residents in nursing homes with diabetes will be different than for the healthy elderly population. On or before admission, each resident should ideally be reviewed by a diabetes educator, physician or specialist with knowledge of the special considerations of diabetes in this population to determine if medication or insulin changes are required (such as stopping sliding scale insulin or switching glyburide to glyclazide for hypoglycemia risk reduction etc), and to determine a rationale glucose monitoring schedule for each resident and A1c target. Standing orders for hypoglycemia are encouraged for all facilities as well as a mechanism for ensuring medication adjustments are prompted when unacceptable hypoglycemia or hyperglycemia are experienced. Nursing Home staff should receive appropriate education that allows them to confidently assess and treat hypo and hyperglycemia in addition to knowing proper insulin injection techniques. For most nursing home residents, there is no benefit to maintaining dietary restrictions. Individualized management is ideal and many need to be adjusted over time. For many residents who are at the end of life, consideration can be given to discontinuing the diabetic regimen. 6

7 APPENDIX A: 7
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Glycemic Management Hypoglycemic & Hyperglycemic Treatment Continuing Care
 Approved by: Glycemic Management Hypoglycemic & Hyperglycemic Continuing Care Senior Operating Officer, Addiction & Mental Health and Continuing Care, Edmonton Senior Operating Officer, Rural Services
Approved by: Glycemic Management Hypoglycemic & Hyperglycemic Continuing Care Senior Operating Officer, Addiction & Mental Health and Continuing Care, Edmonton Senior Operating Officer, Rural Services
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Choosing a Diabetes Strategy Where to Start and Where to Go
 Choosing a Diabetes Strategy Where to Start and Where to Go Erin Keely, MD, FRCPC; and Sharon Brez, RN, BScN, MA(Ed), CDE As presented at the University of Ottawa's 52nd Annual Refresher Course for Family
Choosing a Diabetes Strategy Where to Start and Where to Go Erin Keely, MD, FRCPC; and Sharon Brez, RN, BScN, MA(Ed), CDE As presented at the University of Ottawa's 52nd Annual Refresher Course for Family
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Medications for Diabetes
 Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Medications for Diabetes Sweet, but not too sweet Colette Raymond, Pharm D June 15, 2011 Learning Objectives At the end of this presentation you should be able to: Understand the prevalence and types of
Frailty and Type 2 Diabetes Guidelines for clinicians
 H.G. WELLS PROJECT Frailty and Type 2 Diabetes Guidelines for clinicians Victoria Ruszala victoria.ruszala@nhs.net H.G. Wells Project team Dugal T, Partington E. Kernow CCG Diabetes and Frailty Guideline
H.G. WELLS PROJECT Frailty and Type 2 Diabetes Guidelines for clinicians Victoria Ruszala victoria.ruszala@nhs.net H.G. Wells Project team Dugal T, Partington E. Kernow CCG Diabetes and Frailty Guideline
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE GLYCEMIC MANAGEMENT - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT DOCUMENT
TITLE GLYCEMIC MANAGEMENT - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT DOCUMENT
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE TREATMENT OF HYPOGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity and Nutrition Strategic Clinical Network PARENT
TITLE TREATMENT OF HYPOGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity and Nutrition Strategic Clinical Network PARENT
End of Life Diabetes Care
 End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
Diabetes Medications: Oral Anti-Hyperglycemic Medications
 Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
Diabetes Medications: Oral Anti-Hyperglycemic Medications Medication Types 1. Biguanides 2. Sulfonylureas 3. Thiazolidinediones (TZDs) 4. Alpha-Glucosidase Inhibitors 5. D-Phenylalanine Meglitinides 6.
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
DIABETES AND RAMADAN FASTING
 DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
DIABETES AND RAMADAN FASTING Dr. A. Nigam, M.B.B.S., M.D. (Medicine) Specialist Internal Medicine Al Zahrawi Hospital, Ras Al Khaimah, U.A.E. It is estimated that UAE s population currently stands at approximately
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT)
") How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT) The Basics, New Concepts and Practical Pearls for Basal Bolus Insulin Therapy February 2018
How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT) The Basics, New Concepts and Practical Pearls for Basal Bolus Insulin Therapy February 2018
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Canadian Diabetes Association 2013
 Spring 2014 Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align to the guidelines? Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align
Spring 2014 Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align to the guidelines? Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Clinical Cases in Diabetes Management. Joseph Cook D.O.
 Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
Clinical Cases in Diabetes Management Joseph Cook D.O. Objectives State the prevalence of Diabetes Mellitus in Ohio State the percentage of diabetic patients in the U.S. treated by Primary Care Physicians
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
Oral Medication for the Management of Diabetes Mechanism of. Duration of Daily Dosing Action
 Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
Glyburide (Micronase, Diabeta, Glynase) Glipizide (Glucotrol) Glipizide XL (Glucotrol XL) Glimepiride (Amaryl) Prandin (Repaglinide) Starlix (Nateglinide) 1.25, 2.5, 5mg tabs, Dosing: 2.5-20 mg 12- (Glynase:
RN Diabetes Medication Titration Protocol
 Metformin (Glucophage) Biguanide Medication titration: Time 0 APC or MD Start Metformin 500mg (500mg in the morning, taken with food) Week 1 Week 2 Metformin 1000mg (500mg in the morning and 500mg in the
Metformin (Glucophage) Biguanide Medication titration: Time 0 APC or MD Start Metformin 500mg (500mg in the morning, taken with food) Week 1 Week 2 Metformin 1000mg (500mg in the morning and 500mg in the
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Non-Insulin Diabetes Medications Summary
 Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Non-Insulin Diabetes Medications Summary Medications marked with an asterisk (*) can cause hypoglycemia INSULIN SECRETAGOGUES Sulfonylureas* GLYBURIDE* (Diabeta) (Micronase) production. Side effects: Potential
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA
 LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Inpatient Diabetes 20/01/2015. What should I do? Hyperglycaemia why does it matter? Why are the BSLs unstable? BSL parameters
 Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
第十五章. Diabetes Mellitus
 Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Diabetes-1/9 第十五章 Diabetes Mellitus 陳曉蓮醫師 2/9 - Diabetes 羅東博愛醫院 Management of Diabetes mellitus A. DEFINITION OF DIABETES MELLITUS Diabetes Mellitus is characterized by chronic hyperglycemia with disturbances
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Diabetes Management in Palliative Care. Ryan Liebscher and Carolyn Wilkinson
 Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
Diabetes Management in Palliative Care Ryan Liebscher and Carolyn Wilkinson What are your learning needs? Objectives Review types and prevalence of diabetes Review what is unique to management in the palliative
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Let Them Eat Cake Clinical Practice Recommendations for Diabetes Management
 Let Them Eat Cake Clinical Practice Recommendations for Diabetes Management Mimi Cunningham, MA, RDN, CDE Idaho Health Care Association 2015 Winter Workshop Goals You Go Home With Confidence in your knowledge
Let Them Eat Cake Clinical Practice Recommendations for Diabetes Management Mimi Cunningham, MA, RDN, CDE Idaho Health Care Association 2015 Winter Workshop Goals You Go Home With Confidence in your knowledge
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH
 CHIEF OF MEDICINE, SOUTH WEST HEALTH") Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Sample Exam Questions
 Disclaimer These are not validated questions. They have been created to enhance your learning and provide practice in reading and answering multiple choice questions. Some questions have been created to
Disclaimer These are not validated questions. They have been created to enhance your learning and provide practice in reading and answering multiple choice questions. Some questions have been created to
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Diabetes Mellitus. Raja Nursing Instructor. Acknowledgement: Badil 09/03/2016
 Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
Diabetes Mellitus Raja Nursing Instructor 09/03/2016 Acknowledgement: Badil Objective: Define Diabetes Mellitus (DM) & types of DM. Understand the pathophysiology of Type-I & II DM. List the clinical features
This case study is supported by an educational grant from Abbott.
 Program Name: Planning Committee: When and How to Start or Intensify Insulin Therapy in Your Patients with Type 2 Diabetes Alice Cheng, MD, FRCPC Jean-Francois Yale, MD, CSPQ Lori Berard, RN, CDE Sol Stern,
Program Name: Planning Committee: When and How to Start or Intensify Insulin Therapy in Your Patients with Type 2 Diabetes Alice Cheng, MD, FRCPC Jean-Francois Yale, MD, CSPQ Lori Berard, RN, CDE Sol Stern,
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
FUNDING: MICIS mandated by Maine Legislature, funded by fees collected from pharmaceutical companies as a cost of doing business in the state.
 GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
GOAL: To improve clinical outcomes by delivering upto-date, evidence-based prescribing information, using data and guidelines developed by noncommercial sources FUNDING: MICIS mandated by Maine Legislature,
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Basics. Type 1 diabetes The body cannot make insulin Requires insulin injection Is not treated with oral diabetes medicines (pills)
") Diabetes Basics What is Diabetes? Diabetes is a disease in which the pancreas is unable to make insulin or the body is unable to use insulin or both. This leads to high blood sugar levels in the blood.
Diabetes Basics What is Diabetes? Diabetes is a disease in which the pancreas is unable to make insulin or the body is unable to use insulin or both. This leads to high blood sugar levels in the blood.
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
DIABETES INDICATIONS FOR INSULIN
 DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
Next Steps for Clinicians
 Controversies in the Management of Patients with Type 2 Diabetes The New England Comparative Effectiveness Public Advisory Council An Action Guide for Type 2 Diabetes Management Next Steps for Clinicians
Controversies in the Management of Patients with Type 2 Diabetes The New England Comparative Effectiveness Public Advisory Council An Action Guide for Type 2 Diabetes Management Next Steps for Clinicians
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Type II Diabetes Improving Blood Sugar Control. Geneva Clark Briggs, Pharm.D., BCPS
 Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Managing diabetes in Ramadan
 2nd EASD Postgraduate Course on Clinical Diabetes and its Complications Shiraz, Iran, 2-4 March 2017 Managing diabetes in Ramadan Fereidoun Azizi, M.D. Farhad Hosseinpanah, M.D. Research institute for
2nd EASD Postgraduate Course on Clinical Diabetes and its Complications Shiraz, Iran, 2-4 March 2017 Managing diabetes in Ramadan Fereidoun Azizi, M.D. Farhad Hosseinpanah, M.D. Research institute for
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Diabetes Treatment Guidelines
 Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Treatment Guidelines For more comprehensive information about current approaches to the diagnosis and treatment of diabetes, visit the American Diabetes Association Standards of Medical Care 2018
Diabetes Management: A diagnostic perspective
 Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Diabetes Management: A diagnostic perspective Images: http://www.engadget.com/2009/09/23/bayer-introduces-countour-usb-glucose-meter/ http://www.medtronicdiabetes.com/treatment-and-products/minimed-530g-diabetes-system-with-enlite
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES
 PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES α-glucosidase inhibitor Biguanide DPP-IV inhibitor Meglitinide Sulphonylurea SGLT-2 Inhibitors 1. What are these medicines used for? These medicines
PATIENT INFORMATION LEAFLET MEDICINE TO TREAT: DIABETES α-glucosidase inhibitor Biguanide DPP-IV inhibitor Meglitinide Sulphonylurea SGLT-2 Inhibitors 1. What are these medicines used for? These medicines
Insulin Intensification: A Patient-Centered Approach
 MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years