Accepted Manuscript. S (18) Reference: JACL To appear in:
|
|
|
- Aron Howard Paul
- 5 years ago
- Views:
Transcription

1 Accepted Manuscript Individualized low-density lipoprotein cholesterol reduction with alirocumab titration strategy in heterozygous familial hypercholesterolemia: Results from an open-label extension of ODYSSEY LONG TERM Robert Dufour, MD, MSc, CSPQ, G Kees Hovingh, MD, PhD, MBA, John R. Guyton, MD, Gisle Langslet, MD, Marie T. Baccara-Dinet, MD, MSc, Chantal Din-Bell, MSc, Garen Manvelian, MD, Michel Farnier, MD, PhD PII: DOI: Reference: JACL 1409 S (18) To appear in: Journal of Clinical Lipidology Received Date: 13 July 2018 Revised Date: 20 November 2018 Accepted Date: 24 November 2018 Please cite this article as: Dufour R, Hovingh GK, Guyton JR, Langslet G, Baccara-Dinet MT, Din- Bell C, Manvelian G, Farnier M, Individualized low-density lipoprotein cholesterol reduction with alirocumab titration strategy in heterozygous familial hypercholesterolemia: Results from an open-label extension of ODYSSEY LONG TERM, Journal of Clinical Lipidology (2018), doi: j.jacl This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 ODYSSEY OLE Objec ve: To characterise long-term efficacy and safety of two alirocumab dosages, in pa ents with HeFH ODYSSEY Open-label Extension LONG TERM Alirocumab provided steady 78 weeks Double-Blind Phase III Study Alirocumab 150 mg Q2W 214 pa ents with HeFH 8-week wash out period Star ng dose 75 mg Q2W Alirocumab 75 mg Q2W 150 mg Q2W Mean (SE) LDL-C change from baseline, % Mean (SD) LDL-C, mg/dl Alirocumab 150 mg Q2W (LONG TERM) Alirocumab 75 mg Q2W (OLE) Alirocumab 150 mg Q2W (LONG TERM) b Alirocumab 75 mg Q2W (OLE) c LDL-C reduc ons over a treatment dura on of up to 4 years (including 1.5 years of parent trial) In the same cohort of pa ents: Alirocumab 150 mg Q2W reduced LDL-C by 63.1% at week 8 of LONG TERM Alirocumab 75 mg Q2W reduced LDL-C by 47.3% at week 8 of OLE TEAEs leading to treatment discon nua on occurred in four pa ents (1.9%) Baseline (58.6) (59.5) Study demonstrates efficacy HeFH, heterozygous familial hypercholesterolemia; Week (42.9) 89.6 (54.9) and safety of both alirocumab LDL-C, low-density lipoprotein cholesterol; Q2W, every two weeks; Dose adjustment per physician dosages in pa ents with HeFH SD, standard devia on. judgment possible from week 12 for up to 4 years
3 Individualized low-density lipoprotein cholesterol reduction with alirocumab titration strategy in heterozygous familial hypercholesterolemia: Results from an open-label extension of ODYSSEY LONG TERM Robert Dufour MD, MSc, CSPQ a,, G Kees Hovingh MD, PhD, MBA b, John R Guyton MD c, Gisle Langslet MD d, Marie T Baccara-Dinet MD, MSc e, Chantal Din-Bell MSc f, Garen Manvelian MD g, Michel Farnier MD, PhD h a Institut de Recherches Cliniques de Montréal and Université de Montréal, Montréal, QC, Canada; b Department of Vascular Medicine, Academic Medical Center, Amsterdam, The Netherlands; c Duke University Medical Center, Durham, NC, USA; d Lipid Clinic, Oslo University Hospital, Oslo, Norway; e Clinical Development, R&D, Sanofi, Montpellier, France; f Biostatistics and Programming, Sanofi, Chilly-Mazarin, France; g Regeneron Pharmaceuticals, Tarrytown, NY, USA; h Lipid Clinic, Point Médical and Department of Cardiology, CHU Dijon-Bourgogne, Dijon, France Corresponding author: Michel Farnier, MD, PhD Point Médical, Lipid Clinic Rond-Point de la Nation Dijon, 21000, France michelfarnier@nerim.net; phone: ; fax:
4 The authors dedicate this report to the memory of Robert Dufour, who participated actively in the research and drafting of the manuscript. Dr Dufour passed away November 7, Target journal: Journal of Clinical Lipidology Word count: 3040 Figures/Tables: 4 Figures/4 Tables
5 Abstract Background: Patients with heterozygous familial hypercholesterolemia (HeFH) who completed the double-blind ODYSSEY LONG TERM parent trial and subsequently enrolled in the open-label extension ODYSSEY OLE (NCT ) provide a unique opportunity to investigate effects of 2 alirocumab dosages, a PCSK9 inhibitor, within the same patient cohort. Objective: To characterize long-term efficacy and safety of 2 alirocumab dosages, and utility of a dose titration strategy, in patients with HeFH. Methods: Following an 8-week wash-out period, patients with HeFH who completed the LONG TERM study (receiving alirocumab 150 mg every 2 weeks [Q2W]) were eligible to enroll in OLE (n=214) for up to 40 months treatment duration. In OLE, patients started on alirocumab 75 mg Q2W. From Week 12, dose adjustment from 75 to 150 mg Q2W or vice versa was possible, based on physician s clinical judgement. Results: During LONG TERM, alirocumab 150 mg Q2W reduced mean LDL-C from baseline (162.3 mg/dl) to Week 8 by 63.1%; during OLE, alirocumab 75 mg Q2W reduced mean LDL-C from baseline (166.6 mg/dl) by 47.3% within the same patient cohort. At Week 96, mean LDL-C reduction from OLE baseline was 55.4% vs 46.8% for patients with or without alirocumab dose increase, respectively. Treatmentemergent adverse events leading to permanent treatment discontinuation were observed in 4 patients (1.9%). Conclusions: In patients with HeFH, both alirocumab dosages provided consistent LDL-C reductions over a treatment duration of up to 4 years (including 1.5 years of 3
6 LONG TERM), allowing an individualized approach to LDL-C lowering, depending on baseline LDL-C levels. Word count: 249/250 words maximum Clinical Trial Registration: NCT ; clinicaltrials.gov Keywords: alirocumab; familial hypercholesterolemia; LDL-C; open-label extension; PCSK9 4
7 Introduction Patients with heterozygous familial hypercholesterolemia (HeFH) are characterized by high levels of low-density lipoprotein cholesterol (LDL-C) and elevated risk of atherosclerotic cardiovascular disease. 1-3 Patients with HeFH are typically initiated on maximally tolerated statin therapy with or without ezetimibe, but may require additional lipid-lowering therapies (LLTs) to reach their guidelinerecommended LDL-C treatment goals. 4-8 In the recent European Atherosclerosis Society/European Society of Cardiology consensus statement and a number of guidelines, it has been emphasized that monoclonal antibodies directed against proprotein convertase subtilisin/kexin type 9 (PCSK9), such as alirocumab, should be considered for patients with HeFH at very-high cardiovascular risk, a family history of coronary artery disease at a very young age, or an LDL-C level far from goal despite being on other maximally tolerated LLT. 4,5,9-11 As alirocumab can be administered at a dose of 75 or 150 mg every 2 weeks (Q2W), it offers a flexible dose titration strategy, with dose adjustments possible depending on the level of LDL-C reduction required. Overall, across the ODYSSEY clinical trial program, alirocumab 75 and 150 mg Q2W dose regimens have demonstrated consistent LDL-C reductions of % and 61.0%, respectively, regardless of baseline LDL-C levels ,16 As patients with HeFH generally require ongoing LLT, it is important to characterize the long-term safety and efficacy of alirocumab in these individuals. In ODYSSEY LONG TERM, 18 alirocumab 150 mg Q2W was chosen to enable an assessment of the long-term safety and efficacy of the highest available alirocumab dose. However, some patients may only require the lower dose of alirocumab 75 mg 5
8 Q2W to achieve their cardiovascular risk-based LDL-C goals. In the FH I and FH II parent studies, 56.6% and 61.4% of patients achieved pre-defined LDL-C goals at week 12, respectively, and so were maintained on alirocumab 75 mg Q2W throughout. 14 Patients with HeFH who received alirocumab 150 mg Q2W during the ODYSSEY LONG TERM trial could opt to enroll in the open-label extension study, ODYSSEY OLE study, and receive alirocumab 75 mg Q2W at OLE entry. This affords us the unique opportunity to investigate the effects of the 2 alirocumab doses in the same group of patients, in the initial absence of the effects of alirocumab dose adjustment. We set out to investigate the effects of the 2 approved doses of alirocumab (75 and 150 mg Q2W) administered sequentially in the same HeFH patient cohort, who had relatively high baseline LDL-C levels (in both LONG TERM, and, following wash-out, in OLE), despite maximally tolerated statin therapy. 6
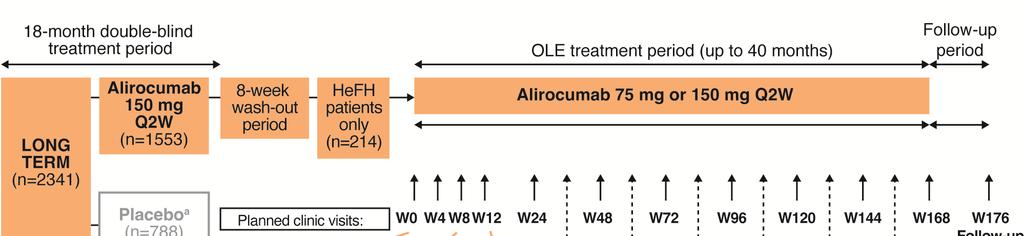
9 Methods Overview of the parent study The protocol of the ODYSSEY LONG TERM (NCT ) parent study has been described previously. 18 Briefly, ODYSSEY LONG TERM was a randomized, multinational, placebo-controlled phase 3 study which included patients ( 18 years) with HeFH, or with established coronary heart disease or a coronary heart disease risk equivalent, and LDL-C 70 mg/dl (1.8 mmol/l) at screening. All participants (n = 2341) were to be receiving high-intensity statin therapy or maximum tolerated dose of statin, with or without other LLT. Patients were randomized 2:1 to receive alirocumab 150 mg Q2W or placebo administered subcutaneously (1 ml injection volume) throughout the 18-month double-blind treatment period; as such, no dose adjustment strategy was utilized during LONG TERM. Of the 2341 randomized participants in LONG TERM, 318 with HeFH who completed the trial and were eligible opted to enroll in ODYSSEY OLE. Open-label extension study design ODYSSEY OLE (986 patients enrolled, of whom 985 received alirocumab) is an open-label extension (OLE) study of patients with HeFH who had completed 1 of 4 phase 3 double-blind clinical trials (FH I, 14 FH II, 14 HIGH FH, 19 and LONG TERM 18 ), conducted over a treatment period of up to 40 months. Following an 8-week wash-out period (off-treatment), patients with a diagnosis of definite HeFH who completed LONG TERM were eligible to enter OLE for a treatment period of up to 40 months (Figure 1). At entry to OLE, patients (the majority of whom had baseline LDL-C >70 mg/dl when they entered the LONG 7
10 TERM parent study) received open-label alirocumab 75 mg Q2W. The starting dose of 75 mg Q2W was chosen because the characteristics of LONG TERM patients enrolled in OLE were similar to those of the overall ODYSSEY population, where the majority achieved their pre-defined LDL-C goals on the 75 mg Q2W dose. In OLE, LDL-C was measured at Day 1 and Weeks 8, 24, 48, 72, 96, 120, 144, and 168. From Day 1 until Week 8 of OLE, LDL-C values were blinded to the physician and patient; from Week 8, the values were communicated to the physician. From Week 12, physicians could adjust the alirocumab dose from 75 mg Q2W to 150 mg Q2W, and vice versa, depending on their clinical judgement and the patient s LDL-C level. Thus, the strategy for dose adjustment in OLE differs from the automatic blinded algorithm for dose adjustment used in most previous ODYSSEY double-blind studies ,20 Throughout OLE, background statin therapies, including maximally tolerated statin dose ± other LLTs, were to be kept stable if possible; reasons for any background LLT dose adjustments were to be recorded by the investigator. For dose adjustments based on LDL-C values, simultaneous adjustments in any LLT and alirocumab dose were avoided. In the current analysis, only patients with HeFH who received alirocumab in the LONG TERM parent study and subsequently entered OLE are included (n = 214). The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Guidelines for Good Clinical Practice. The study protocol was approved by the appropriate independent review board/ethics committee, and written informed consent was obtained from each participant. The trial was registered with clinicaltrials.gov (NCT ). 8
11 Endpoints and assessments The primary objective of this OLE study was to assess the long-term safety of alirocumab when added to background LLTs in patients diagnosed with HeFH. Safety was assessed through treatment-emergent adverse events (TEAEs), laboratory data, and vital signs. TEAEs were assessed from baseline (first dose of alirocumab in OLE) until 10 weeks after the last dose of alirocumab received during OLE. Secondary objectives included the evaluation of the long-term efficacy and immunogenicity of alirocumab. Statistical analysis The safety population included patients who received at least 1 dose or partial dose of the study drug. Safety was analyzed by descriptive statistics. The efficacy analysis was performed on the modified intention-to-treat (mitt) population, which included all patients who received at least 1 dose or partial dose of the study drug, had baseline LDL-C data available from the parent LONG TERM study, and had at least 1 LDL-C value available during OLE (and at least the Week 8 value) from the period of the first study drug injection in OLE up to the 3 weeks following the last study drug injection. Efficacy parameters were assessed by descriptive statistics. Alirocumab anti-drug antibody (ADA) analyses were performed on all treated patients (safety population) who had a blood sample at the parent study baseline and at least 1 evaluable blood sample post study drug injection in OLE. 9
12 Results Patient characteristics A total of 214 patients with HeFH who received alirocumab during the LONG TERM parent study entered OLE, of whom 213 were included in the mitt population. During OLE, 16 patients (7%) prematurely discontinued the study treatment: 2 due to death, 4 due to adverse events, 3 due to poor compliance, and 7 due to other reasons. Baseline characteristics are presented in Table 1; of note, 50% of patients had atherosclerotic cardiovascular disease. Mean (standard deviation [SD]) LDL-C at OLE baseline was (58.3) mg/dl (safety population; Table 1), despite patients being on maximally tolerated statins ± other LLTs (for example, 71.5% and 54.7% of patients were receiving high-intensity statin doses and ezetimibe at OLE baseline, respectively); the lipid parameters at OLE baseline reflect the 8-week wash-out period prior to the start of OLE. Overall median (minimum:maximum) exposure to alirocumab in OLE was 132 (4:168) weeks (2.5 years). Comparison of alirocumab 75 mg in OLE vs 150 mg dose in the LONG TERM parent study in the same cohort of patients All patients with HeFH considered in this analysis received alirocumab 150 mg Q2W in the LONG TERM parent study, entered OLE following an 8-week wash-out period, and received alirocumab 75 mg Q2W for the first 8 weeks of OLE (prior to potential dose increase). Examining LDL-C reductions at Week 8 in the LONG TERM parent study and at Week 8 in OLE therefore allows for investigation of the effects of exposure to the 2 alirocumab doses in the same cohort of HeFH patients, 10
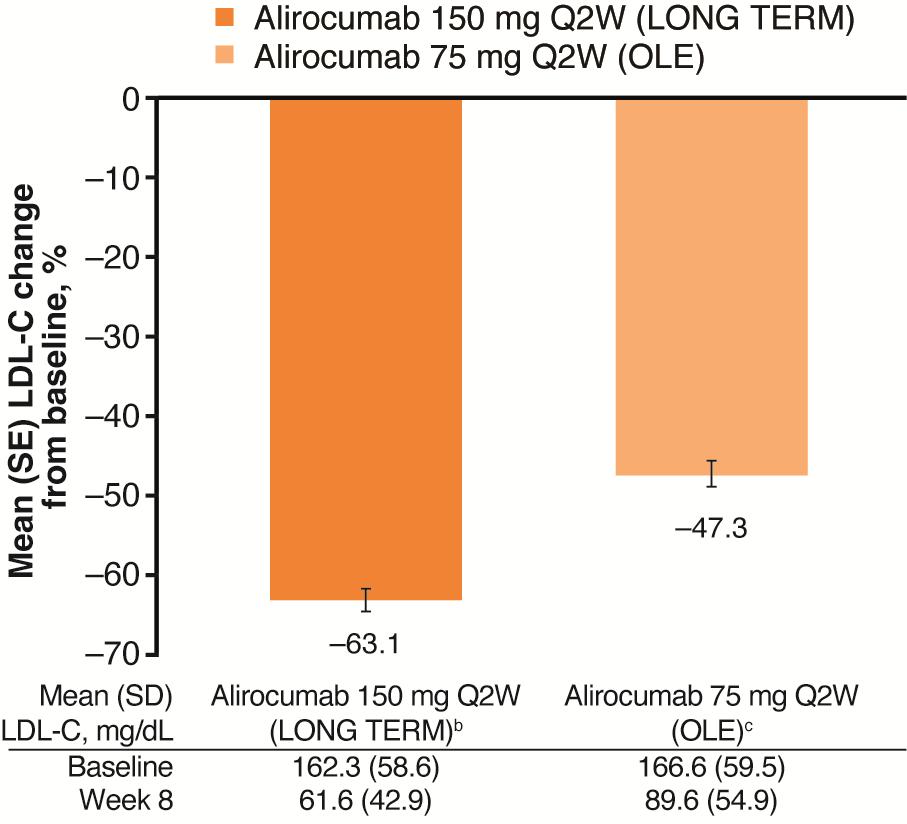
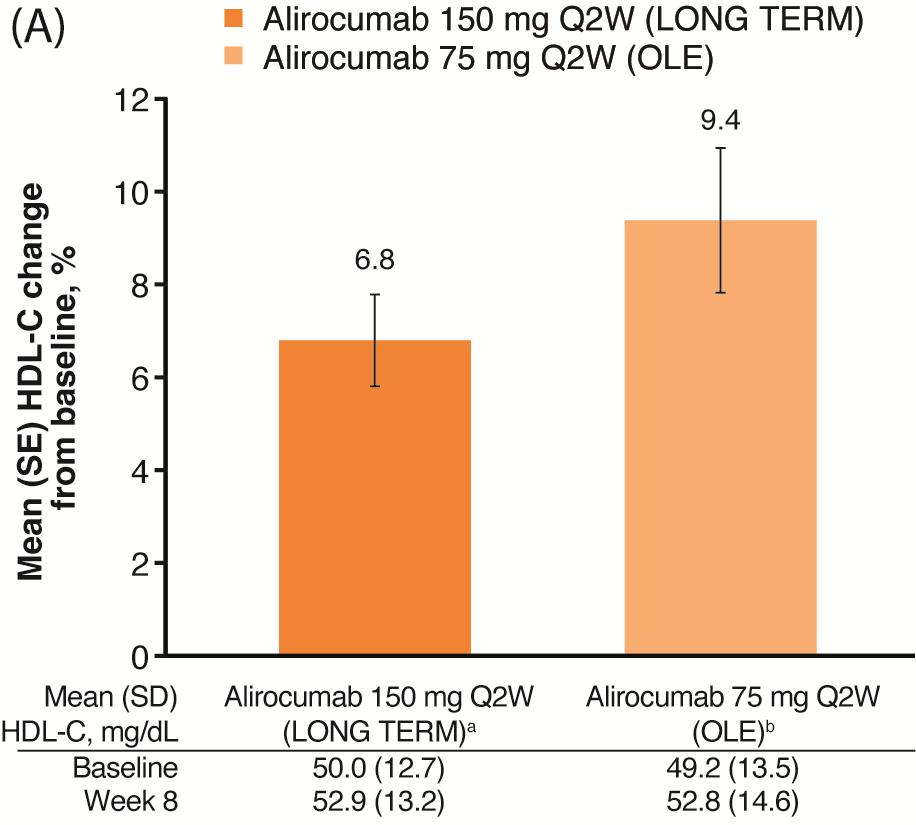
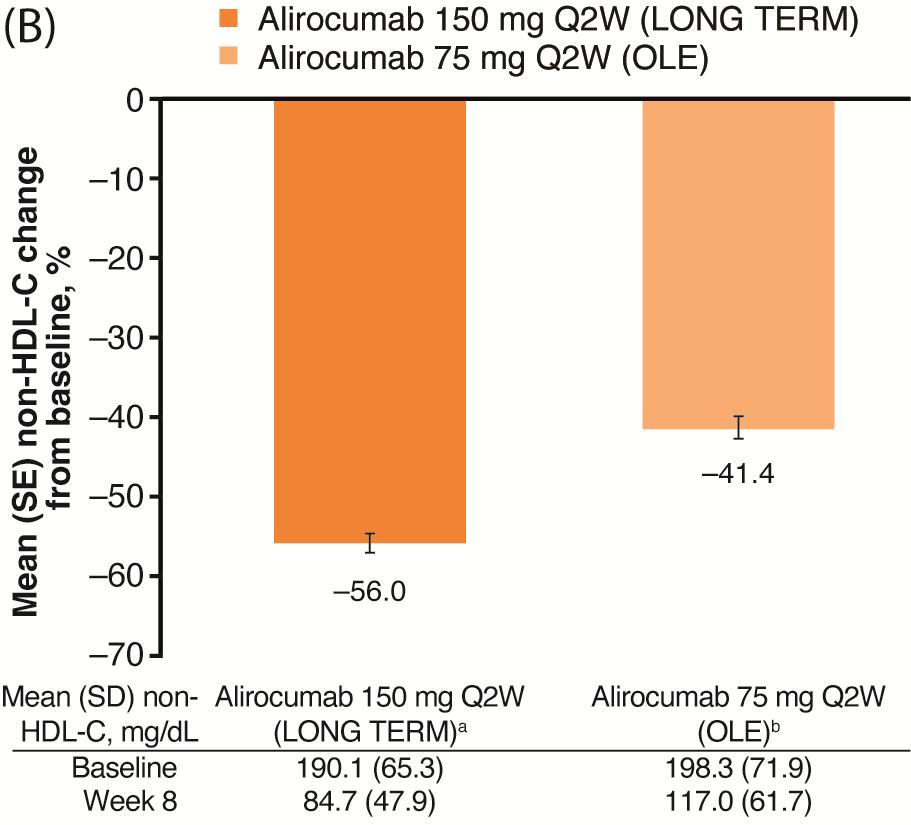
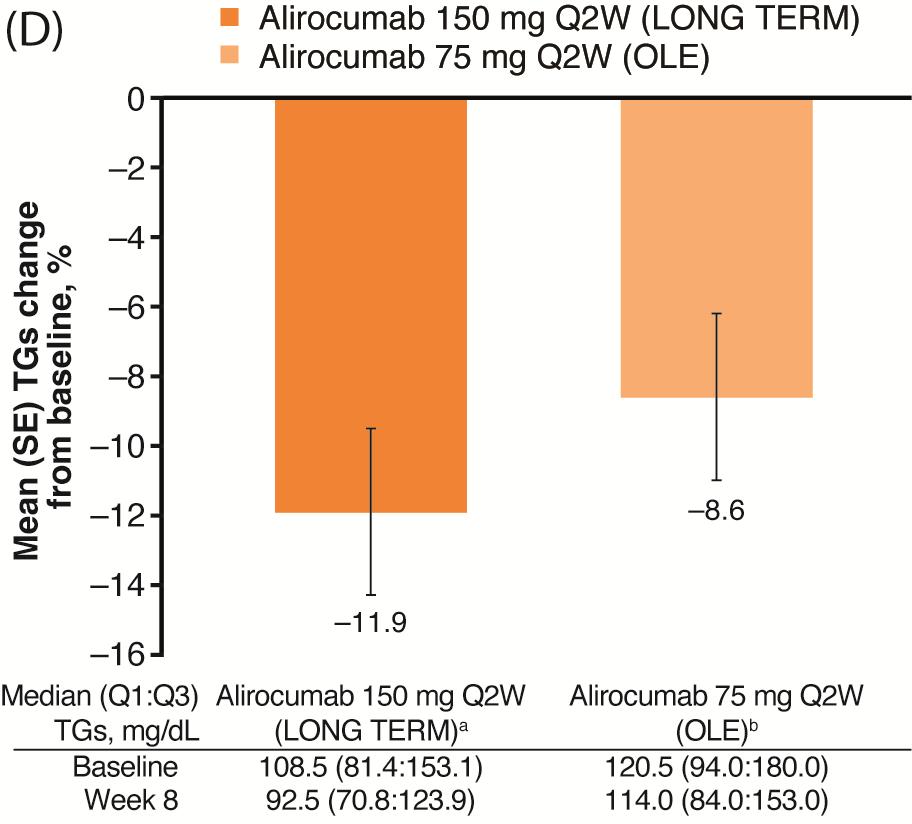
13 without the confounding effects of dose adjustments. For the mitt population, mean (SD) LDL-C at parent study baseline was (58.6) mg/dl, compared with (59.5) mg/dl at OLE baseline (following the 8-week wash-out period) for the same patient cohort (Figure 2). At Week 8 of the LONG TERM study (all patients with HeFH in this cohort receiving alirocumab 150 mg Q2W), mean (SD) LDL-C was 61.6 (42.9) mg/dl (63.1% reduction from LONG TERM baseline). By comparison, at Week 8 of OLE (all patients receiving alirocumab 75 mg Q2W), mean (SD) LDL-C was 89.6 (54.9) mg/dl (47.3% reduction from OLE baseline). Mean percent changes observed in other lipid parameters from baseline following 8 weeks of alirocumab 150 mg Q2W during LONG TERM versus 8 weeks of alirocumab 75 mg Q2W during OLE in this HeFH cohort were as follows: highdensity lipoprotein cholesterol (HDL-C) increased by 6.8% (LONG TERM) versus 9.4% (OLE); non-hdl-c decreased by 56.0% (LONG TERM) versus 41.4% (OLE), total cholesterol (TC) decreased by 42.3% (LONG TERM) versus 30.9% (OLE), and triglycerides (TGs) decreased by 11.9% (LONG TERM) versus 8.6% (OLE; Figures 3A to 3D, respectively). Dose adjustment during OLE During the OLE study, in this subgroup of patients with mean LDL-C at OLE baseline of mg/dl, the alirocumab dose was increased from 75 mg to 150 mg Q2W in 51.9% of patients (n = 111), with a median time to dose increase of 14.1 weeks (Table 2). In most cases (n = 110, 99.1%), alirocumab dose increase was due to high LDL-C values (mean [SD] LDL-C value for dose increase decision of [51.1] mg/dl), as per investigator judgement; in one patient (0.9%), alirocumab dose increase was due to high triglyceride levels, and LDL-C values were 11
14 unavailable at the time of dose decision. A comparable proportion of the patients who were either maintained on alirocumab 75 mg Q2W or who had dose increase to 150 mg Q2W were receiving high-intensity statin therapy or ezetimibe (71.7% vs 71.2% and 55.3% vs 54.1%, respectively) at entry to OLE (safety population). Among patients who had an alirocumab dose increase during OLE, alirocumab dose was subsequently decreased from 150 mg to 75 mg Q2W in 7 individuals (6.3%); the median time from first study treatment to first dose adjustment from 150 mg to 75 mg Q2W was 96.1 weeks (Table 2). The main reason for alirocumab dose adjustment from 150 mg to 75 mg Q2W was reported as low LDL-C values (n = 5, 71.4%; mean [SD] LDL-C value for dose decrease decision of 49.8 [29.2] mg/dl), as per investigator judgement. Two other patients (28.6%) also had dose adjustment from 150 to 75 mg Q2W, one due to an adverse event (memory loss of unknown etiology) and one due to other reasons (further details provided as a footnote to Table 2). Efficacy by dose during OLE In patients who had dose increase to 150 mg Q2W during OLE (n = 111; mitt population), mean (SD) LDL-C decreased from (59.3) mg/dl at OLE baseline to (55.0) mg/dl at Week 8 with 75 mg Q2W, and decreased further to 84.7 (57.2) mg/dl at Week 96 with 150 mg Q2W (55.4% reduction from baseline; mg/dl absolute reduction from baseline; Figure 4). For patients who were maintained on alirocumab 75 mg Q2W throughout OLE (n = 102; mitt population), mean (SD) LDL-C decreased from (42.6) mg/dl at OLE baseline to 59.7 (36.5) mg/dl at Week 8, and was 69.7 (36.8) mg/dl at Week 12
15 96 (46.8% reduction from baseline; 62.8 mg/dl absolute reduction from baseline; Figure 4). Overall, for patients with and without dose increase (dose increase mainly dependent on the value of baseline LDL-C), LDL-C reductions were maintained over time from Week 8 through to Week 96 of OLE. At Week 96 of OLE, the proportion of patients in the overall cohort with prior atherosclerotic cardiovascular disease (ASCVD) achieving LDL-C <70 mg/dl or 50% reduction in LDL-C from OLE baseline was 65.8% and 1.4%, respectively; 67.1% achieved LDL-C <70 mg/dl or 50% reduction from OLE baseline (on-treatment analysis; Table 3). For patients without prior ASCVD, 74.1% achieved LDL-C <100 mg/dl and 1.3% achieved 50% reduction in LDL-C from OLE baseline at Week 96 of OLE (on-treatment analysis; Table 3). Safety During OLE, 185 patients (86.4%) reported a TEAE, while 4 patients (1.9%) discontinued treatment due to a TEAE (Table 4). The TEAEs leading to treatment discontinuation (1 event each) included pregnancy, metastatic colon cancer, worsening myalgia in both legs, and grade I transitional meningioma. Three deaths (1.4%) due to TEAEs occurred during OLE, including sudden cardiac death (22 weeks after start of OLE), acute myocardial infarction (2.7 years after start of OLE), and metastatic colon cancer (Table 4). None of the three TEAEs leading to death were considered by the investigator to be related to the study treatment. Common TEAEs were viral upper respiratory tract infection (13.1%), influenza (10.3%), and bronchitis (8.9%; Table 4). 13
16 Local injection-site reactions were reported by 11 patients (5.1%); the majority of cases were mild in intensity, with only 1 report of a moderate-intensity local injectionsite reaction. Other TEAEs of special interest that were reported included; 26 patients (12.1%) with general or local allergic TEAEs; 7 patients (3.3%) with hepatic disorders, of whom 2 patients experienced serious hepatic disorders; 2 patients with neurocognitive disorders (0.9%); 10 patients (4.7%) with neurological disorders, of whom 1 patient experienced a serious neurological disorder; 5 patients (2.3%) with ophthalmological disorders, of whom 1 patient experienced a serious ophthalmological TEAE; 5 patients (2.3%) with an overdose with study treatment (accidental or intentional; defined as at least twice the intended dose within the intended therapeutic interval, ie, 2 injections in <7 calendar days); and 10 patients (4.7%) with diabetes mellitus or diabetic complications TEAEs, of whom 4 patients had diabetes mellitus at OLE baseline and 6 patients did not. Of the 6 patients without diabetes mellitus at OLE baseline who reported diabetes mellitus or diabetic complications TEAEs, these TEAEs included 5 patients with type 2 diabetes mellitus, 1 patient with hyperglycemia, 1 patient with diabetic neuropathy and 1 patient with increased blood glucose. While only the safety data for this cohort during OLE is presented here, a complete safety description for the overall OLE population can be found in the paper by Farnier and colleagues. 21 Anti-drug antibodies During OLE, 5/209 patients (2.4%) had a treatment-emergent positive ADA response: 3 patients had a negative ADA status for the duration of the parent study, and 2 patients had a positive treatment-emergent ADA response during the parent 14
17 study. For the 3 patients who had a negative ADA status during the parent study, all ADAs recorded during OLE were of a low titer, with no consistent pattern between ADA status and efficacy of LDL-C lowering; furthermore, no TEAEs were considered by investigators to be related to the study drug. Of patients with a positive ADA response during OLE, 1/5 had a persistent positive ADA response (0.5% of total cohort). No neutralizing ADAs were observed in the overall population during OLE. Finally, none of the 5 patients who had a treatment-emergent positive ADA response reported injection site reactions. 15
18 Discussion As patients with HeFH require long term treatment with LLTs to achieve their guideline-recommended target LDL-C levels, 4,5 the characterization of the long-term efficacy and safety of alirocumab is of importance. In particular, the use of investigator judgement to decide on potential alirocumab dose adjustment is of interest. The present analysis investigating the HeFH LONG TERM cohort of the ODYSSEY OLE trial also provides a unique opportunity to explore the efficacy of both alirocumab doses (75 and 150 mg Q2W) within the same patient group with particularly high baseline LDL-C levels. During the LONG TERM parent study, 18 for this cohort of HeFH patients who entered OLE, alirocumab 150 mg Q2W was shown to reduce LDL-C levels by 63.1% from baseline at Week 8; in contrast, for the same patient group receiving alirocumab 75 mg Q2W during OLE, LDL-C was reduced from baseline by 47.3% at Week 8. The difference in percentage LDL-C reduction between the 2 doses of alirocumab (15.8%) is as expected by simulation when designing the ODYSSEY phase 3 clinical trial program, 22 and is also consistent with that observed in previous double-blind trials ,22 In comparison, doubling the dose of a statin typically leads to an additional LDL-C reduction of ~6%. 23 Although the corresponding absolute mean LDL-C level at Week 8 was higher in this HeFH cohort in OLE than for the parent study (89.6 vs 61.6 mg/dl), subsequent alirocumab dose increase from 75 to 150 mg Q2W was possible during OLE for those patients requiring further reduction in LDL-C levels. Alirocumab was shown to produce a sustained reduction in LDL-C levels, both for patients with HeFH maintained on alirocumab 75 mg Q2W (46.8% reduction from baseline at Week 96) and for those with dose increase to alirocumab 16
19 150 mg Q2W (55.4% reduction from baseline at Week 96); the main driver for alirocumab dose increase is the level of baseline LDL-C, based on the clinical judgement of the physician. As all patients received alirocumab 150 mg during LONG TERM, irrespective of baseline LDL-C level, this may explain why the mean LDL-C reduction observed with alirocumab 150 mg Q2W is greater in LONG TERM than as reported here for OLE, in which 102 patients were maintained on alirocumab 75 mg (63.1% vs 55.4%, respectively). A pooled analysis of 4 double-blind phase 3 ODYSSEY trials showed that, for patients with HeFH receiving alirocumab 75 mg Q2W (with possible dose increase to 150 mg Q2W at Week 12 if Week 8 LDL-C >70 mg/dl), LDL-C reduction from baseline was 48.8% at Week 24, 24 comparable to that observed during OLE. Of note, the comparable LDL-C reductions were observed despite different mechanisms for dose decisions being employed for the 2 analyses; dose decisions were determined by a blinded algorithm in the pooled double-blind studies and by using investigator judgement during OLE. Patients with HeFH who received blinded alirocumab dose increase from 75 mg to 150 mg Q2W during phase 3 trials (41.8% of patients from FH I and FH II combined) were found to have higher baseline LDL-C levels than patients maintained on 75 mg Q2W (164.9 mg/dl and mg/dl vs mg/dl and mg/dl for patients from FH I and FH II, respectively). 24 A similar result was observed in the current analysis (mean baseline LDL-C of vs mg/dl for patients with vs without dose increase, respectively), although, as mentioned above, dose adjustment decisions (51.9% of all patients with dose increase) were based on investigator judgement rather than a blinded algorithm. In almost all cases during 17
20 OLE, the decision to increase the dose was based on the LDL-C level attained. Nevertheless, the observation of higher baseline LDL-C in patients titrating to the higher dose suggests that in some HeFH cases initial dosing at 150 mg Q2W might be considered. Previously, it has been reported that a common reason for not adopting maximum dose drug regimens is the acceptance by physicians of a higher than target LDL-C level, with the justification that patient LDL-C levels had already been reduced by more than 50% from baseline. 25 This follows current guideline recommendations, which suggest that for patients with clinical ASCVD a realistic treatment goal is a 50% reduction in LDL-C from baseline, and ideally the achievement of LDL-C <70 mg/dl. 26 Here, with the cohort of HeFH patients who received alirocumab during LONG TERM, the proportion of patients with ASCVD achieving LDL-C <70 mg/dl or a 50% reduction in LDL-C from baseline at Week 96 of OLE was 67.1%. Alirocumab was generally well tolerated, and the safety data are consistent with data from the 18-month double-blind placebo-controlled parent study. 18 During OLE, the incidences of treatment-emergent ADAs and persistent treatment-emergent ADAs were similar to those previously reported from a pooled analysis of 10 phase 3 alirocumab trials, which showed that LDL-C reductions were maintained for the duration of the trials, regardless of ADA status. 27 Limitations of this analysis include the relatively small sample size (n = 214), the lack of a comparative control, and, as a result of the open-label treatment design, the possible introduction of bias. 18
21 In conclusion, both alirocumab dosages provide substantial and consistent LDL- C reductions over a treatment duration of up to 4 years, allowing for an individualized approach to LDL-C-lowering, depending on baseline LDL-C levels, in patients with HeFH. 19
22 Acknowledgements The authors would like to thank the participants, their families, and all investigators involved in this study. The following people from the study sponsors reviewed and provided editorial comments on the manuscript: Corinne Hanotin, MD, and Michael Howard, MBA (Sanofi); and Robert Pordy, MD, and Carol Hudson, MS (Regeneron Pharmaceuticals, Inc.). The sponsor was involved in the study design and collection, analysis, and interpretation of data, as well as data checking of information provided in the manuscript. The authors had unrestricted access to study data, were responsible for all content and editorial decisions, and received no honoraria related to the development of this publication. Medical writing and editorial support, under the direction of the authors, was provided by Rachel Dunn, PhD, of Prime, Knutsford, UK, funded by Sanofi and Regeneron Pharmaceuticals, Inc. Responsibility for all opinions, conclusions, and data interpretation lies with the authors. Qualified researchers may request access to patient level data and related study documents including the clinical study report, study protocol with any amendments, blank case report form, statistical analysis plan, and dataset specifications. Patient level data will be anonymized and study documents will be redacted to protect the privacy of trial participants. Further details on Sanofi s data sharing criteria, eligible studies, and process for requesting access can be found at: Funding The ODYSSEY OLE study was funded by Sanofi and Regeneron Pharmaceuticals, Inc. 20
23 Financial Disclosure Robert Dufour has received research support from Sanofi, Regeneron Pharmaceuticals, Inc., Amgen, Orion, and Akcea; has served as a consultant for Sanofi, Regeneron Pharmaceuticals, Inc., Amgen, Janssen, Aegerion, and Akcea; and has received speaker fees from Amgen and Sanofi. G Kees Hovingh is a holder of a Vidi grant [ ] from the Netherlands Organisation for Scientific Research (NWO), and is supported by CardioVascular Research Initiative [CVON ; Genius] and the European Union [Resolve: FP and TransCard: FP ]; has received research support from Aegerion, Amgen, and Sanofi; and has served as a consultant and received speaker fees from Amgen, Aegerion, Sanofi, Regeneron Pharmaceuticals, Inc., and Pfizer. John R Guyton has received research support from Sanofi, Regeneron Pharmaceuticals, Inc., Amgen, and Amarin; and has served as a consultant for Amgen and FH Foundation. Gisle Langslet has received speaker and expert witness fees from Sanofi, Amgen, Boehringer Ingelheim, and Janssen. Marie T Baccara-Dinet is a stockholder and an employee of Sanofi. Chantal Din-Bell is a stockholder and an employee of Sanofi. Garen Manvelian is a stockholder and an employee of Regeneron Pharmaceuticals, Inc. Michel Farnier has received research support from Sanofi/Regeneron Pharmaceuticals, Inc., Amgen, and Merck and Co; has served as a consultant for 21
24 Sanofi/Regeneron Pharmaceuticals, Inc., Pfizer, Amgen, Merck and Co, Eli Lilly, AstraZeneca, Kowa, Akcea/Ionis, Amarin and Servier; and has received speaker fees from Sanofi/Regeneron Pharmaceuticals, Inc., Abbott, Amgen, Merck and Co, Pfizer, and Mylan. Author contributions R.D., G. K. H., J. R. G. and G. L. were investigators who contributed to the data acquisition in the ODYSSEY OLE trial; M. F. was an investigator who contributed to the data acquisition in LONG TERM. M. T. B.-D., C. D.-B., G. M. and M. F. contributed to the concept or design of the analysis. C. D.-B. contributed to the statistical analyses. All authors contributed to the analysis and interpretation of data and critically reviewed and edited the manuscript. All authors approved the final version. In addition, all authors had full access to the study data and were responsible for the final decision to submit the manuscript, and are accountable for the accuracy and integrity of the submitted work. 22
25 References 1. Arca M. Old challenges and new opportunities in the clinical management of heterozygous familial hypercholesterolemia (HeFH): The promises of PCSK9 inhibitors. Atherosclerosis. 2017;256: Nordestgaard BG, Chapman MJ, Humphries SE, et al. Familial hypercholesterolaemia is underdiagnosed and undertreated in the general population: guidance for clinicians to prevent coronary heart disease: consensus statement of the European Atherosclerosis Society. Eur Heart J. 2013;34: a. 3. Gidding SS, Champagne MA, de Ferranti SD, et al. The Agenda for Familial Hypercholesterolemia: A Scientific Statement From the American Heart Association. Circulation. 2015;132: Catapano AL, Graham I, De Backer G, et al ESC/EAS Guidelines for the Management of Dyslipidaemias: The Task Force for the Management of Dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Assocciation for Cardiovascular Prevention & Rehabilitation (EACPR). Atherosclerosis. 2016;253: Lloyd-Jones DM, Morris PB, Ballantyne CM, et al ACC Expert Consensus Decision Pathway on the role of non-statin therapies for LDLcholesterol lowering in the management of atherosclerotic cardiovascular 23
26 disease risk: A report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2016;68: Huijgen R, Kindt I, Verhoeven SB, et al. Two years after molecular diagnosis of familial hypercholesterolemia: majority on cholesterol-lowering treatment but a minority reaches treatment goal. PLoS One. 2010;5:e Béliard S, Carreau V, Carrie A, et al. Improvement in LDL-cholesterol levels of patients with familial hypercholesterolemia: can we do better? Analysis of results obtained during the past two decades in 1669 French subjects. Atherosclerosis. 2014;234: Perez de Isla L, Alonso R, Watts GF, et al. Attainment of LDL-cholesterol treatment goals in patients with familial hypercholesterolemia: 5-Year SAFEHEART registry follow-up. J Am Coll Cardiol. 2016;67: Anderson TJ, Grégoire J, Pearson GJ, et al Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can J Cardiol. 2016;32: Landmesser U, Chapman MJ, Stock JK, et al Update of ESC/EAS Task Force on practical clinical guidance for proprotein convertase subtilisin/kexin type 9 inhibition in patients with atherosclerotic cardiovascular disease or in familial hypercholesterolaemia. Eur Heart J. 2018;39:
27 11. Bays HE, Jones PH, Orringer CE, Brown WV, Jacobson TA. National Lipid Association Annual Summary of Clinical Lipidology J Clin Lipidol. 2016;10:S Bays H, Gaudet D, Weiss R, et al. Alirocumab as add-on to atorvastatin versus other lipid treatment strategies: ODYSSEY OPTIONS I randomized trial. J Clin Endocrinol Metab. 2015;100: Cannon CP, Cariou B, Blom D, et al. Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated doses of statins: the ODYSSEY COMBO II randomized controlled trial. Eur Heart J. 2015;36: Kastelein JJ, Ginsberg HN, Langslet G, et al. ODYSSEY FH I and FH II: 78 week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolaemia. Eur Heart J. 2015;36: Kereiakes DJ, Robinson JG, Cannon CP, et al. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: The ODYSSEY COMBO I study. Am Heart J. 2015;169: e Moriarty PM, Thompson PD, Cannon CP, et al. Efficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge 25
28 arm: The ODYSSEY ALTERNATIVE randomized trial. J Clin Lipidol. 2015;9: Farnier M, Jones P, Severance R, et al. Efficacy and safety of adding alirocumab to rosuvastatin versus adding ezetimibe or doubling the rosuvastatin dose in high cardiovascular-risk patients: The ODYSSEY OPTIONS II randomized trial. Atherosclerosis. 2016;244: Robinson JG, Farnier M, Krempf M, et al. Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372: Ginsberg HN, Rader DJ, Raal FJ, et al. Efficacy and safety of alirocumab in patients with heterozygous familial hypercholesterolemia and LDL-C of 160 mg/dl or higher. Cardiovasc Drugs Ther. 2016;30: Roth EM, Taskinen MR, Ginsberg HN, et al. Monotherapy with the PCSK9 inhibitor alirocumab versus ezetimibe in patients with hypercholesterolemia: results of a 24 week, double-blind, randomized Phase 3 trial. Int J Cardiol. 2014;176: Farnier M, Hovingh GK, Langslet G, et al. Long-term safety and efficacy of alirocumab in patients with heterozygous familial hyphercholesterolemia: An open-label extension of the ODYSSEY program. Atherosclerosis. 2018;(In press). 26
29 22. Kastelein JJ, Kereiakes DJ, Cannon CP, et al. Effect of alirocumab dose increase on LDL lowering and lipid goal attainment in patients with dyslipidemia. Coron Artery Dis. 2017;28: Nicholls SJ, Brandrup-Wognsen G, Palmer M, Barter PJ. Meta-analysis of comparative efficacy of increasing dose of atorvastatin versus rosuvastatin versus simvastatin on lowering levels of atherogenic lipids (from VOYAGER). Am J Cardiol. 2010;105: Kastelein JJ, Hovingh GK, Langslet G, et al. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 monoclonal antibody alirocumab vs placebo in patients with heterozygous familial hypercholesterolemia. J Clin Lipidol. 2017;11: e Pijlman AH, Huijgen R, Verhagen SN, et al. Evaluation of cholesterol lowering treatment of patients with familial hypercholesterolemia: a large crosssectional study in The Netherlands. Atherosclerosis. 2010;209: Farnier M, Civeira F, Descamps O, FH Expert Working Group. How to implement clinical guidelines to optimise familial hypercholesterolaemia diagnosis and treatment. Atheroscler Suppl. 2017;26: Roth EM, Goldberg AC, Catapano AL, et al. Antidrug Antibodies in Patients Treated with Alirocumab. N Engl J Med. 2017;376:
30 Table 1. Baseline characteristics at OLE entry (safety population) All patients (n = 214) Age, years, mean (SD) 55.8 (10.7) Male, n (%) 121 (56.5) BMI, kg/m 2, mean (SD) 29.6 (5.4) ASCVD, a n (%) 107 (50.0) Very-high CV risk, b n (%) 118 (55.1) High CV risk, c n (%) 96 (44.9) Hypertension, n (%) 93 (43.5) Type 1 or type 2 diabetes mellitus 27 (12.6) High-intensity statin therapy, d n (%) 153 (71.5) Ezetimibe, n (%) 117 (54.7) Lipid parameters, mg/dl LDL-C, mean (SD) (58.3) Non-HDL-C, mean (SD) (70.0) Total cholesterol, mean (SD) (68.7) HDL-C, mean (SD) 49.2 (13.3) Triglycerides, median (Q1:Q3) (96.0:180.0) Lipoprotein (a), median (Q1:Q3) 27.0 (10.0:63.0) Apolipoprotein B, mean (SD) (35.8) Apolipoprotein A1, mean (SD) (27.6) a ASCVD defined as coronary heart disease, ischemic stroke, or peripheral arterial disease. b Very-high CV risk defined as patients with coronary heart disease or coronary heart disease risk equivalents. c High CV risk defined as all other patients. d High-intensity statin therapy defined as atorvastatin mg, or rosuvastatin mg daily. ASCVD, atherosclerotic cardiovascular disease; BMI, body mass index; CV, cardiovascular; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SD, standard deviation. 28
31 Table 2. Dose adjustment during OLE a (safety population) All patients (n = 214) Patients maintained on 75 mg Q2W during OLE, n (%) 103 (48.1) Patients with dose adjustment to 150 mg Q2W, n (%) 111 (51.9) Time to first dose adjustment to 150 mg Q2W, weeks, mean (SD) [median (min:max)] Reason for first dose adjustment to 150 mg Q2W, n (%) 28.6 (25.3) [14.1 (10.0:120.0)] LDL-C value too high as per investigator judgement 110 (99.1) Other b 1 (0.9) Patients with dose adjustment from 150 mg Q2W to 75 mg Q2W, c n (%) Time to first dose adjustment from 150 mg Q2W to 75 mg Q2W, weeks, mean (SD) [median (min:max)] Reason for first dose adjustment from 150 mg Q2W to 75 mg Q2W, n (%) 7 (6.3) 86.1 (45.7) [96.1 (24:132)] Adverse event d 1 (14.3) LDL-C value too low as per investigator judgement 5 (71.4) Other e 1 (14.3) a A patient can be counted in both dose adjustment categories as appropriate. b Patient had dose increase from alirocumab 75 mg to 150 mg Q2W due to high triglyceride levels; LDL-C values were unavailable at time of dose decision. c For those patients who had previously had dose increase. d Memory loss of unknown etiology. e Physician previously decided to increase the dose as they were unsure if the patient was properly compliant with diet; later, the physician decided to return the dose to alirocumab 75 mg Q2W. LDL-C, low-density lipoprotein cholesterol; Q2W, every 2 weeks; SD, standard deviation 29
32 Table 3. Proportion of patients achieving LDL-C goals at week 96 according to ASCVD status at OLE entry (on-treatment population) 50% reduction in LDL-C a LDL-C <70 mg/dl LDL-C <100 mg/dl 50% reduction in LDL-C a ASCVD status at OLE entry or LDL-C <70 mg/dl Yes, % (n/n) 1.4 (1/70) 65.8 (50/76) 81.6 (62/76) 67.1 (51/76) No, % (n/n) 1.3 (1/77) 55.6 (45/81) 74.1 (60/81) 56.8 (46/81) a Compared to OLE baseline. ASCVD, atherosclerotic cardiovascular disease; LDL-C, low-density lipoprotein cholesterol. 30
33 Table 4. Adverse events in OLE (safety population) n (%) All patients (n = 214) Any TEAE 185 (86.4) Treatment-emergent SAE 54 (25.2) TEAE leading to death 3 (1.4) TEAE leading to permanent treatment discontinuation 4 (1.9) Most frequently reported TEAEs by preferred term ( 5% of participants) Viral upper respiratory tract infection 28 (13.1) Influenza 22 (10.3) Bronchitis 19 (8.9) Influenza-like illness 19 (8.9) Arthralgia 17 (7.9) Back pain 17 (7.9) Hypertension 16 (7.5) Upper respiratory tract infection 16 (7.5) Diarrhea 15 (7.0) Myalgia 14 (6.5) Gastroenteritis 12 (5.6) Pain in extremity 12 (5.6) Injection-site reaction 11 (5.1) SAE, serious adverse event; TEAE, treatment-emergent adverse event. 31
34 Figure 1. OLE study design a Patients receiving placebo were part of the OLE study but were not included in this analysis. b Post-treatment follow-up call to be performed 10 weeks after the last injection. HeFH, heterozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LLT, lipid-lowering therapy; NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III; OLE, open-label extension; Q2W, every 2 weeks; TLC, therapeutic lifestyle changes; W, week. Figure 2. Percent LDL-C change from baseline to Week 8 in the LONG TERM parent study and OLE study, in the same cohort of HeFH patients (mitt analysis) a a Only patients who have all 4 LDL-C measurements (parent-study baseline, OLE baseline, week 8 parent-study, and week 8 OLE study) are included in this analysis. b Results for patient cohort during the LONG TERM study (n = 179). c Results for patient cohort during the OLE study (n = 179). LDL-C, low-density lipoprotein cholesterol; Q2W, every 2 weeks; mitt, modified intent-to-treat; SD, standard deviation; SE, standard error. Figure 3. Percent change in (A) HDL-C, (B) non-hdl-c, (C) TC, and (D) TGs from baseline to Week 8 in the LONG TERM parent study and OLE study, in the same cohort of HeFH patients (mitt analysis) Patient numbers for each lipid parameter are as follows: HDL-C, non-hdl-c, and TC, n = 185; TGs, n = 182. a Results for patient cohort during the LONG TERM study. b Results for patient cohort during the OLE study. HDL-C, high-density lipoprotein cholesterol; mitt, modified intention-to-treat; Q2W, every 2 weeks; SD, standard deviation; SE, standard error; TC, total cholesterol; TGs, triglycerides. 32
35 Figure 4. Mean (SD) LDL-C levels over time according to alirocumab dose increase status in OLE (mitt analysis) LDL-C, low-density lipoprotein cholesterol; mitt, modified intention-to-treat; Q2W, every 2 weeks; SD, standard deviation. 33
36
37
38
39
40
41
42
43 Highlights Alirocumab 150 mg Q2W reduced LDL-C by 63.1% at week 8 of LONG TERM (HeFH cohort) Alirocumab 75 mg Q2W reduced LDL-C by 47.3% at week 8 of OLE (same cohort, n=214) Choice of alirocumab dose allowed for an individualized approach to LDL-C lowering Alirocumab provided steady LDL-C reductions over 3 years of treatment TEAEs leading to treatment discontinuation occurred in 4 patients (1.9%)
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study
 Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study Erik Stroes, 1 John Guyton, 2 Michel Farnier, 3 Norman Lepor, 4 Fernando Civeira,
Efficacy and Safety of Alirocumab in Patients with Hypercholesterolemia not on Statin Therapy: the ODYSSEY CHOICE II Study Erik Stroes, 1 John Guyton, 2 Michel Farnier, 3 Norman Lepor, 4 Fernando Civeira,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies
 Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Industry Relationships and Institutional Affiliations
 Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher
Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM
 Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM Efficacy by subgroup, and safety when LDL-C
Long-term safety, tolerability and efficacy of alirocumab in high cardiovascular risk patients: ODYSSEY LONG TERM Efficacy by subgroup, and safety when LDL-C
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Effect of alirocumab on the frequency of lipoprotein apheresis: A randomised Phase III trial
 Effect of alirocumab on the frequency of lipoprotein apheresis: A randomised Phase III trial Patrick M. Moriarty, Klaus G. Parhofer, Stephan P. Babirak, Marc-Andre Cornier, P. Barton Duell, Bernd Hohenstein,
Effect of alirocumab on the frequency of lipoprotein apheresis: A randomised Phase III trial Patrick M. Moriarty, Klaus G. Parhofer, Stephan P. Babirak, Marc-Andre Cornier, P. Barton Duell, Bernd Hohenstein,
PCSK9 inhibition across a wide spectrum of patients: One size fits all?
 PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
Alirocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia
 Alirocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Alirocumab (Praluent,
Alirocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Stephen Erhorn Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Alirocumab (Praluent,
Anne Carol Goldberg, MD, FACP, FAHA, FNLA Washington University, St. Louis, MO USA
 Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Introduction. Harold E. Bays 1 & Robert S. Rosenson 2 & Marie T. Baccara-Dinet 3 & Michael J. Louie 4 & Desmond Thompson 4 & G.
 Cardiovascular Drugs and Therapy (2018) 32:175 180 https://doi.org/10.1007/s10557-018-6784-z SHORT COMMUNICATION Assessment of the 1% of Patients with Consistent < 15% Reduction in Low-Density Lipoprotein
Cardiovascular Drugs and Therapy (2018) 32:175 180 https://doi.org/10.1007/s10557-018-6784-z SHORT COMMUNICATION Assessment of the 1% of Patients with Consistent < 15% Reduction in Low-Density Lipoprotein
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Industry Relationships and Institutional Affiliations
 Long-term safety, tolerability and efficacy of alirocumab versus placebo in high cardiovascular risk patients: first results from the ODYSSEY LONG TERM study in 2,341 patients Jennifer G. Robinson, 1 Michel
Long-term safety, tolerability and efficacy of alirocumab versus placebo in high cardiovascular risk patients: first results from the ODYSSEY LONG TERM study in 2,341 patients Jennifer G. Robinson, 1 Michel
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Patient and Physician Perspectives on Administration of the PCSK9 Monoclonal Antibody Alirocumab, an Injectable Medication to Lower LDL-C Levels
 Patient and Physician Perspectives on Administration of the PCSK9 Monoclonal Antibody Alirocumab, an Injectable Medication to Lower LDL-C Levels Bertrand Cariou, 1 Maja Bujas-Bobanovic, 2 Michael J Louie,
Patient and Physician Perspectives on Administration of the PCSK9 Monoclonal Antibody Alirocumab, an Injectable Medication to Lower LDL-C Levels Bertrand Cariou, 1 Maja Bujas-Bobanovic, 2 Michael J Louie,
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Patient Lists. Epic ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION. Please see accompanying full Prescribing Information
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
Inhibition of PCSK9: The Birth of a New Therapy
 Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Patient List Inquiries
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient List Inquiries in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient List Inquiries in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject PCSK9 Inhibitors Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 9 References... 9 Effective Date... 01/15/2018
Cigna Drug and Biologic Coverage Policy Subject PCSK9 Inhibitors Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 9 References... 9 Effective Date... 01/15/2018
Patient Action Sets. Allscripts Touchworks ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Action Sets in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Action Sets in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Praluent (alirocumab)
") Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
Praluent (alirocumab) Policy Number: 5.01.600 Last Review: 06/2018 Origination: 07/2015 Next Review: 06/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Praluent
Patient Lists. Allscripts Professional ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Registry Processor Reports
 ABOUT THIS GUIDE This Guide provides a high-level overview of Registry Processor Reports in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates
ABOUT THIS GUIDE This Guide provides a high-level overview of Registry Processor Reports in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
PCSK9 Inhibitors: A View of Clinical Studies
 PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
Reports. NextGen ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION. Please see accompanying full Prescribing Information
 ABOUT THIS GUIDE This Guide provides a high-level overview of in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT (alirocumab)
ABOUT THIS GUIDE This Guide provides a high-level overview of in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT (alirocumab)
Cholesterol; what are the future lipid targets?
 Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
IR Thematic Call on Alirocumab. September 2 nd, 2014
 IR Thematic Call on Alirocumab September 2 nd, 2014 Sanofi Forward Looking Statements This presentation contains forward-looking statements as defined in the Private Securities Litigation Reform Act of
IR Thematic Call on Alirocumab September 2 nd, 2014 Sanofi Forward Looking Statements This presentation contains forward-looking statements as defined in the Private Securities Litigation Reform Act of
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
Registry Reports. eclinicalworks ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION
 ABOUT THIS GUIDE This Guide provides a high-level overview of Registry Reports in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Registry Reports in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
Guidelines for the management of dyslipidemia have
 ORIGINAL RESEARCH Alirocumab Treatment and Achievement of Non-High-Density Lipoprotein Cholesterol and Apolipoprotein B Goals in Patients With Hypercholesterolemia: Pooled Results From 10 Phase 3 ODYSSEY
ORIGINAL RESEARCH Alirocumab Treatment and Achievement of Non-High-Density Lipoprotein Cholesterol and Apolipoprotein B Goals in Patients With Hypercholesterolemia: Pooled Results From 10 Phase 3 ODYSSEY
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update. November 17 th, 2018
 CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
PCSK9 Inhibitors DRUG POLICY BENEFIT APPLICATION
 DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study
 Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study Michael J Koren 1, Robert P Giugliano 2, Frederick Raal 3, David
Randomized Comparison of the Safety, Tolerability, and Efficacy of Long-term Administration of AMG 145: 52-Week Results From the OSLER Study Michael J Koren 1, Robert P Giugliano 2, Frederick Raal 3, David
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
LDL-C treatment goals were introduced in the first National
 Point/Counterpoint Counterpoint: Low-Density Lipoprotein Cholesterol Targets Are Not Needed in Lipid Treatment Guidelines Jennifer G. Robinson, Kausik Ray Abstract On the basis of accumulating evidence,
Point/Counterpoint Counterpoint: Low-Density Lipoprotein Cholesterol Targets Are Not Needed in Lipid Treatment Guidelines Jennifer G. Robinson, Kausik Ray Abstract On the basis of accumulating evidence,
Class Update PCSK9 Inhibitors
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Supplementary Online Content
 Supplementary Online Content Cannon CP, Khan I, Klimchak AC, Reynolds MR, Sanchez RJ, Sasiela WJ. Simulation of lipid-lowering therapy intensification in a population with atherosclerotic cardiovascular
Supplementary Online Content Cannon CP, Khan I, Klimchak AC, Reynolds MR, Sanchez RJ, Sasiela WJ. Simulation of lipid-lowering therapy intensification in a population with atherosclerotic cardiovascular
Nephrologisches Zentrum Göttingen GbR Priv. Doz. Dr. med. V. Schettler
 Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
PCSK9 Inhibitors for Lowering Cholesterol: Ready for Prime Time?
 Original Article Thomas Knickelbine, MD, FACC, FSCCT, FSCAI From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Thomas Knickelbine, MD, FACC,
Original Article Thomas Knickelbine, MD, FACC, FSCCT, FSCAI From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Thomas Knickelbine, MD, FACC,
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials?
 PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
Approximately 34% of adults in the United States
 RESEARCH Ezetimibe Use and LDL-C Goal Achievement: A Retrospective Database Analysis of Patients with Clinical Atherosclerotic Cardiovascular Disease or Probable Heterozygous Familial Hypercholesterolemia
RESEARCH Ezetimibe Use and LDL-C Goal Achievement: A Retrospective Database Analysis of Patients with Clinical Atherosclerotic Cardiovascular Disease or Probable Heterozygous Familial Hypercholesterolemia
Efficacy and Safety of Alirocumab 150 mg Every 4 Weeks in Patients With Hypercholesterolemia Not on Statin Therapy: The ODYSSEY CHOICE II Study
 ORIGINAL RESEARCH Efficacy and Safety of Alirocumab 150 mg Every 4 Weeks in Patients With Hypercholesterolemia Not on Statin Therapy: The ODYSSEY CHOICE II Study Erik Stroes, MD, PhD; John R. Guyton, MD;
ORIGINAL RESEARCH Efficacy and Safety of Alirocumab 150 mg Every 4 Weeks in Patients With Hypercholesterolemia Not on Statin Therapy: The ODYSSEY CHOICE II Study Erik Stroes, MD, PhD; John R. Guyton, MD;
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
DYSLIPIDEMIA. Michael Brändle, Stefan Bilz
 DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Disclosures. Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA. Learning Objectives. Atherogenesis. Acceptable Values
 39 th National Conference on Pediatric Health Care Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA March 19-22, 2018 CHICAGO Disclosures Speakers Bureau Sanofi and Regeneron Learning Objectives
39 th National Conference on Pediatric Health Care Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA March 19-22, 2018 CHICAGO Disclosures Speakers Bureau Sanofi and Regeneron Learning Objectives
Lowering elevated levels of low-density lipoprotein cholesterol
 Lower On-Treatment Low-Density Lipoprotein Cholesterol and Major Adverse Cardiovascular Events in Women and Men: Pooled Analysis of 10 ODYSSEY Phase 3 Alirocumab Trials Antonio J. Vallejo-Vaz, MD, PhD;
Lower On-Treatment Low-Density Lipoprotein Cholesterol and Major Adverse Cardiovascular Events in Women and Men: Pooled Analysis of 10 ODYSSEY Phase 3 Alirocumab Trials Antonio J. Vallejo-Vaz, MD, PhD;
Study 2 ( ) Pivotal Phase 3 Study Top-Line Results. October 29, 2018
 Pivotal Phase 3 Study Top-Line Results. October 29, 2018") Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
Results of ODYSSEY OUTCOMES Trial
 Results of ODYSSEY OUTCOMES Trial Evaluation of long-term cardiovascular outcomes after Acute Coronary Syndrome (ACS) during treatment with Praluent (alirocumab) Investor call at ACC, Orlando, March 10,
Results of ODYSSEY OUTCOMES Trial Evaluation of long-term cardiovascular outcomes after Acute Coronary Syndrome (ACS) during treatment with Praluent (alirocumab) Investor call at ACC, Orlando, March 10,
Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab
 Original Article Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab Paul M Ridker, M.D., Jean Claude Tardif, M.D., Pierre Amarenco, M.D., William Duggan, Ph.D., Robert J. Glynn,
Original Article Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab Paul M Ridker, M.D., Jean Claude Tardif, M.D., Pierre Amarenco, M.D., William Duggan, Ph.D., Robert J. Glynn,
ABSTRACT. n engl j med 372;16 nejm.org april 16,
 The new england journal of medicine established in 1812 april 16, 2015 vol. 372 no. 16 Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events Jennifer G. Robinson, M.D., M.P.H.,
The new england journal of medicine established in 1812 april 16, 2015 vol. 372 no. 16 Efficacy and Safety of Alirocumab in Reducing Lipids and Cardiovascular Events Jennifer G. Robinson, M.D., M.P.H.,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
*Carbohydrate & Lipid Metabolism Research Unit, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa
 Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
What s our starting point? New Lipid-Lowering Drugs: PCSK9 Inhibitors. Why You Should Care. Outline ATPIII Guidelines 1
 New Lipid-Lowering Drugs: Inhibitors Blockbusters or Bust? Jody Mallicoat, BS, PharmD PGY1 Pharmacy Resident OSF Saint Francis Medical Center, Peoria, IL What s our starting point? Had you heard of inhibitors
New Lipid-Lowering Drugs: Inhibitors Blockbusters or Bust? Jody Mallicoat, BS, PharmD PGY1 Pharmacy Resident OSF Saint Francis Medical Center, Peoria, IL What s our starting point? Had you heard of inhibitors
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
QUANTITY LIMIT TARGET DRUGS- RECOMMENDED LIMITS Brand (generic) GPI Multisource Code Quantity Limit
 GPI Multisource Code Quantity Limit") Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Criteria- Through Preferred Agent(s) Program Summary This program applies to Commercial, Netresults
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Criteria- Through Preferred Agent(s) Program Summary This program applies to Commercial, Netresults
IR Thematic Call on Alirocumab. March 31 st, 2014
 IR Thematic Call on Alirocumab March 31 st, 2014 Sanofi Forward Looking Statements This presentation contains forward-looking statements as defined in the Private Securities Litigation Reform Act of 1995,
IR Thematic Call on Alirocumab March 31 st, 2014 Sanofi Forward Looking Statements This presentation contains forward-looking statements as defined in the Private Securities Litigation Reform Act of 1995,
March 30, 2014, Joint ACC/JAMA Late-breaking Clinical Trials Session 402 American College of Cardiology, Washington DC
 A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia
 Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia The trial ClinicalTrials.gov number: NCT00552097 John J.P. Kastelein, MD, PhD* Department of Vascular Medicine Academic Medical Center
Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia The trial ClinicalTrials.gov number: NCT00552097 John J.P. Kastelein, MD, PhD* Department of Vascular Medicine Academic Medical Center
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a
: Results from a") Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
Goal Achievement after Utilizing an Anti-PCSK9 Antibody in Statin-Intolerant Subjects (GAUSS): Results from a Randomized, d Double-blind, bli Placebo- Controlled Study Evan A. Stein 1, David Sullivan 2,
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance
 Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance Hani Sabbour MD FACC FHRS Clinical Assistant Professor of Cardiology Brown University Rhode Island USA Consultant Cardiology
Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance Hani Sabbour MD FACC FHRS Clinical Assistant Professor of Cardiology Brown University Rhode Island USA Consultant Cardiology
Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia
 Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Evolocumab (Repatha,
Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Evolocumab (Repatha,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2/10/2016. Patient-Centered Management of Dyslipidemia. No disclosures. What is Patient-Centered Management?
 Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Treatment of severe Familial Hypercholesterolemia PCSK9 inhibitors
 Treatment of severe Familial Hypercholesterolemia PCSK9 inhibitors 2 nd Severe FH Course: Recognize, Diagnose and Treat Severe Familial Hypercholesterolemia December 2-3, 2018 Muscat, Oman Dr. Khalid Al-Waili,
Treatment of severe Familial Hypercholesterolemia PCSK9 inhibitors 2 nd Severe FH Course: Recognize, Diagnose and Treat Severe Familial Hypercholesterolemia December 2-3, 2018 Muscat, Oman Dr. Khalid Al-Waili,
ADVANCES IN CARDIAC ARRHYTMIAS AND GREAT INNOVATIONS IN CARDIOLOGY Torino, October 13 15, 2016
 ADVANCES IN CARDIAC ARRHYTMIAS AND GREAT INNOVATIONS IN CARDIOLOGY Torino, October 13 15, 2016 PCSK9 INHIBITORS: A HUGE LITERATURE, NOW WE ARE READY TO USE THEM Pasquale Perrone Filardi Federico II University
ADVANCES IN CARDIAC ARRHYTMIAS AND GREAT INNOVATIONS IN CARDIOLOGY Torino, October 13 15, 2016 PCSK9 INHIBITORS: A HUGE LITERATURE, NOW WE ARE READY TO USE THEM Pasquale Perrone Filardi Federico II University
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Class Update PCSK9 Inhibitors
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab
 The new england journal of medicine Original Article Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab Paul M Ridker, M.D., Jean Claude Tardif, M.D., Pierre Amarenco, M.D.,
The new england journal of medicine Original Article Lipid-Reduction Variability and Antidrug- Antibody Formation with Bococizumab Paul M Ridker, M.D., Jean Claude Tardif, M.D., Pierre Amarenco, M.D.,
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;