Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance
|
|
|
- Shona Dawson
- 6 years ago
- Views:
Transcription

1 Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance

2 Hani Sabbour MD FACC FHRS Clinical Assistant Professor of Cardiology Brown University Rhode Island USA Consultant Cardiology Cleveland Clinic Abu Dhabi UAE
3 Update on Dyslipidemia Therapy in 2016 High potency statins were the sole focus of the 2013 guidelines due to lack of RCT for other therapies HDL has lost ground as a therapeutic target but remains a critical marker of CVD risk CETP is almost out ( waiting for anacetrapib REVEAL study ) since ACCELERATE / evacetrapib was halted Residual risk is well defined Statin intolerance is now well defined ( Gauss 2/3 studies) Combination therapy with niacin / fibrates is out Combination therapy with ezetimibe, BAS and PCSK9 is recommended
4 RESIDUAL RISK DESPITE MAXIMAL STATIN THERAPIES IN CLINICAL TRIALS Risk of CV mortality and MACE CV events are not eliminated ( but certainly better than placebo or less potent therapy ) estimated 60% residual risk Even after controlling for other risk factors there is a need to further reduce dyslipidemia dependent risk of CV events Over the last decade research into add on therapies or alternative therapies has become the HOLY GRAIL of risk reduction in Dyslipidemia

5
6 Why targets matter WHAT ABOUT THOSE PATIENTS WHO DON T ACHIEVE THEIR TARGET?

7 Approximately 70% of patients at the highest risk* are not at optional < 70 mg/dl (< 1.8 mmol/l)ldl-c goal * Very high risk defined as: CHD plus 2 major risk factors. Data shown are from a multinational survey, of which 2,334 patients were considered very high risk. Countries in this analysis included the United States, Canada, Spain, the Netherlands, France, Taiwan, Korea, Brazil, and Mexico. National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) US optional goal < 70 mg/dl (1.8 mmol/l)
8 Percent of Total Number of High Risk US Adults Achieving LDL-C Levels of < 100 mg/dl or LDL-C Levels of < 70 mg/dl, AN EVEN BIGGER PROBLEM FOR HIGH RISK PATIENTS At goal Not at goal NHANES Administrative claims data LDL-C < 100 mg/dl EMR NHANES Administrative claims data LDL-C < 70 mg/dl EMR High-risk patients were defined as patients older than 18 years with a history of CHD or CHD risk equivalent who had the latest complete lipid panel measurement and were treated with statin monotherapy for > 90 days. EMR = electronic medical record database collected from 40,000 clinicians and 20,000 NP and PA (GE Centricity); Administrative Claims Database of the medical and pharmacy claims for 42MM patients enrolled in a large US managed care plan (Clinformatics DataMart, a product of Optuminsight Life Sciences); NHANES=National Health and Nutrition Examination Survey, a national public health survey conducted by the CDC of a nationally representative sample of 5000 individuals each year across a country. As per NCEP ATP III, the LDL-C goal patients was <100 mg/dl. High-risk patients were also evaluated for the optional goal of LDL-C <70 mg/dl, as per the 2004 update to the NCEP ATP III Guidelines. Jones, PH, et al. J Am Heart Assoc. 2012;1:e

9
10 HOW DOES THIS HAPPEN & DOES IT MATTER? UNTREATED ( Not following Guidelines?) SUBOPTIMALLY TREATED UNABLE TO LOWER WITH STATIN( FAMILILAL HYPERLIPDEMIA) TREATMENT DISCONTINUED / STATIN INTOLERANCE WHEN SUB OPTIMAL LDL IS PRESENT RISK CLEARLY INCREASES!!!
11 Residual Risk Should we use ALTERNATE non LDL Therapy? Not taking a statin or unable to take a statin ( non adherence / intolerance ) therefore becomes a major cause of residual risk as the patient is unable to take the most effective therapy in CV risk prevention Can we lower risk by non LDL targeted therapy in combination or alone? Raising HDL niacin, fibrates, CETP Lowering TG- fibrates Inflammation methotrexate PCSk9 inhibition
12 Residual Risk & LDL Targets Combination therapy implies need for ADDITIONAL effectiveness Or should we just lower LDL even more :- Statin Combination with Ezetemibe Profound LDL lowering with PCSk9 WHAT IS THE EVIDENCE BASE?

13

14

15 ACCELERATE TRIAL


16

17
18 WHAT ABOUT COMBINATION WITH FIBRATES AND NIACIN?
19 ACCORD Lipid Primary Outcome: First occurrence of nonfatal MI, nonfatal stroke, or CV death 5518 pts T2DM treated with simvastatin randomized to fenofibrate or placebo The primary outcome was the first occurrence of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes. ACCORD Study Group. NEJM 2010; 362:

20
21


")
22 Fenofibrates Statins for Secondary Prevention Statins for Primary Prevention Niacin (HDL Hypothesis)
23 Patient Populations with HIGH Unmet Need for Additional LDL-C Lowering 24 FH Population in EU Genetic disorder High risk of early CHD HeFH prevalence 1:200 to 1:250 1,2 Untreated LDL-C of mg/dl 3 79% with HeFH not at goal (<100 mg/dl [2.6 mmol/l]) 4 High / Very High CV Risk Population Previous MI / stroke / CVD or multiple CV risk factors incl. T2DM Difficult to achieve LDL- C goals, despite current therapies 5 20% with CHD not at goal (<100 mg/dl [2.6 mmol/l]) 59% at very high CV risk not at goal (<70 mg/dl [1.8 mmol/l]) Statin-Intolerant Population 10-15% on highintensity statins show intolerance 6 Many discontinue due to muscle pain and/or weakness Nearly all patients who need considerable LDL-C reductions will not reach goal 1 Nordestgaard et al. Eur Heart J 2013;34: Sjouke et al. Eur Heart J Mar 1;36(9): ESC/EAS Guidelines for the management of dyslipidaemias Eur Heart J. 2011;32(14): Pijlman et al. Atherosclerosis 2010;209: Virani et al. Am Heart J 2011;161: Arca et al. Diabetes Metab Syndr Obes 2011;4:
24 Dyslipidemia in Familial Hypercholesterolemia PATIENTS WITH VERY HIGH BASELINE AND HYPORESPONDERS TO STATINS = UNABLE TO ACHIEVE TARGET WITH STATIN THERAPY
25 Familial Hypercholesterolemia Phenotypes FH Heterozygotes FH Homozygotes ~ 1 in 200 to 1:500 persons worldwide 1,4 ~ 1 in 1,000,000 persons worldwide 1 1 mutated allele 1 2 mutated alleles 1 TC: 350 to 500 mg/dl 3 TC: > 500 to > 1,000 mg/dl 1 LDL-C: mg/dl 1,2 LDL-C: > 600 mg/dl 2 Half the number of LDLR expressed 3 LDLR activity absent or dysfunctional 3 TC = total cholesterol 1. Rader DJ, et al. In: Longo DL, et al, eds. Harrison s Principles of Internal Medicine. Vol II.18th ed. New York, NY: McGraw Hill Medical. 2012: Robinson JG. J Manag Care Pharm. 2013;19: National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Circulation. 2002;106: Nordestgaard BG, et al. European Heart Journal. 2013;34:


26 % of Patients Achieving LDL-C Goal Per Risk Category Despite Maximal Treatment, A Low Percentage of Patients with HeFH Achieve LDL-C < 100 mg/dl In a Randomized Global Clinical Trial of HeFH Patients, A Low Percentage Achieved LDL-C Levels of < 100 mg/dl on Maximal Treatment* 100% 80% Statin 1 Statin 2 In Netherlands Estimates of HeFH Patients On Maximal Lipid Lowering Therapy Achieving LDL-C < 100 mg/dl** < 100 mg/dl > 100 mg/dl 60% p < 0.05, n = % 40% 20% n = 37 p < 0.001, n = % 0% n = 67 <130 mg/dl <100 mg/dl *NCEP Adult Treatment Panel III Risk Category: Medium Risk: <130 mg/dl (3.4 mmol/l); 2 risk factors,10-year risk of coronary artery disease 20%; High Risk: <100 mg/dl (2.6 mmol/l); coronary artery disease or its risk equivalents (atherosclerosis, diabetes, or 10-year risk > 20%).18 week RCT, double-blind parallel group where heterozygous (He) FH patients initiated statin treatment at 20 mg with forced titration to 40 and 80 mg in N = 623 randomized; p Values were obtained from a logistic regression model. Global population consisted of 31% US patients. **Adults with HeFH were part of a cross-sectional study. 96% were on statin treatment where 34% were on maximum dose. N = 1249 met inclusion criteria. n = 304 patients on maximal therapy; Maximum lipid-lowering therapy was defined as maximum statin doses in combination with ezetimibe. Using outpatient visits to Lipid Clinics after February Stein EA, et al. Am J Cardiol. 2003; 92: Pijlman AH, et al. Atherosclerosis. 2010; 209:
27
28 Mean percentage change in LDL-C (SE) from baseline (mg/dl) Reduction in LDL-C Level from Baseline at Week 12 According to Mutation Status for Heterozygous FH Patients Alirocumab 75 mg Q2W Alirocumab 150 mg Q2W Control SE, standard error Kastelein et al. Presented at ACC Poster number 1293M APOB defective LDLR defective LDLR negative PCSK9 GOF No known mutation n=21 n=6 n=18 n=133 n=99 n=132 n=172 n=93 n=148 n=5 n=1 n=0 n=88 n=111 n=73 29 CONFIDENTIAL NOT FOR PROMOTIONAL USE DO NOT COPY OR DISTRIBUTE 2015, Regeneron Pharmaceuticals, Inc.
29 THE PROMISE OF COMBINATION PCSK9 IN ATHEROSCLEROSIS FOR THE HIGH RISK PATIENT SHOULD WE NOW GO EVEN LOWER WITH LDL? AND HOW COULD WE ACHIEVE THIS GOAL?
30 Proportional reduction in event rate (SE) Cholesterol Trialist Collaboration Meta-Analysis of Dyslipidemia Trials 50% Major Vascular Events 40% 30% 20% 10% Every 1 mmol LDL reduction = 20% event rate reduction 0% -10% Reduction in LDL cholesterol (mmol/l) CTT Collaborators. Lancet. 2005; 366:


31 Percent Reduction vs. Treat-to-Target 32 NO TARGET TARGET CLEARLY DEFINED BY RISK GROUP Ray KK et al. Eur Heart J. 2014;35(15):960-8
32 Residual Risk Despite Statin Therapy in TNT effect of additional Risk Factors 33 The TNT study was a prospective, double blind, parallel-group trial done at 256 sites in 14 countries between April, 1998, and August, 2004, with a median follow-up of 4.9 years. 10,001 patients were enrolled aged years with clinically evident coronary heart disease. Our analysis includes 5584 patients with metabolic syndrome based on the 2005 NCEP ATP III criteria. Patients were randomly assigned to receive either atorvastatin 10 mg per day (n=2820) or 80 mg per day (n=2764). The primary outcome measure was time to first major cardiovascular event, defined as death from coronary heart disease, non-fatal nonprocedure-related myocardial infarction, resuscitated cardiac arrest, or fatal or non-fatal stroke. % patients with Major CV event Atorvastatin 10 mg Atorvastatin 80 mg HR = 1.35 (0.63, 2.90) Deedwania P et al. Lancet 2006;368: HR = 0.82 (0.57, 1.19) HR = 0.95 (0.72, 1.24) VERY HIGH RISK HR = 0.69 (0.54, 0.89) HR = 0.77 (0.60, 1.00) HR = 0.68 (0.48, 0.96) Number of metabolic syndrome components Atorvastatin 10 mg: 11/209 65/ / / / /465 Atorvastatin 80 mg: 16/223 52/ / / /965 54/457

 < 115 mg/dl (< 3 mmol/l) SCORE 10% Documented CVD Severe CKD (< 30) DM + 1 FR and/or")

33 Joint ESC Guidelines. Eur J Prev Cardiol 2012; 19: ESC/EAS Guidelines. Eur Heart J 2011; 32: ESC / EAS Guidelines Risk Based Targets LDL-C LDL-C LDL-C < 70 mg/dl (< 1.8 mmol/l) or > 50% LDL-C reduction < 100 mg/dl (<2.5 mmol/l) < 115 mg/dl (< 3 mmol/l) SCORE 10% Documented CVD Severe CKD (< 30) DM + 1 FR and/or TOD* DM 0 FR SCORE 10-5% Moderate CKD (30-60) Markedly elevated RF SCORE 5-1% SCORE < 1% Consider Drug if LDL > 190 mg/dl (> 4.9 mmol/l) Very High Risk High Risk * TOD= target organ damage (such as microalbuminuria mg/24h) Moderate Risk Low Risk
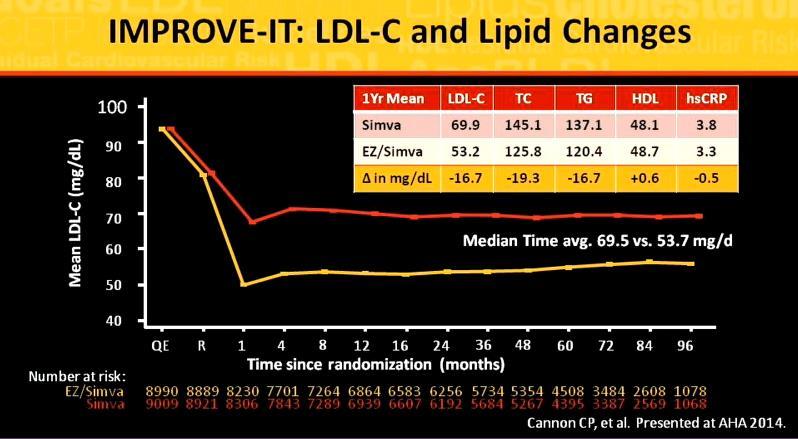
34 IMPROVE IT - LOWER IS BETTER REAFFIRMED Combination STATIN ( simvastatin 40 mg with Ezetimibe 10 mg ) REVISITED AGAIN IN IMPROVE IT IN HIGH and VERY HIGH RISK ASCVD AND ACS PATIENTS ACHIEVED LOWER LDL 53 MG/DL THAN THE HIGH INTENSITY STATIN 69 MG/DL SIGNIFICANT REDUCTION IN 7 POINT MACCE CV OUTCOME OVER 6 YEARS OF STUDY
35

36

37
38 THE TREATMENT GAP IT IS INSUFFIENT TO BE COMPLACENT ABOUT JUST BEING ON A STATIN THE GOALS FOR TRETAMENT HAVE BEEN REEMPHASIZED REACHING A GOAL OF LDL LESS THAN 70 HAS AN IMPACT ON ASCVD NEED TO RE FOCUS ON ACHIEVING THESE GOALS 1IN 3 DEATHS ARE DUE TO CVD AND 17 MILLION WORLDWIDE STATINS HAVE IMPACTED THIS SIGNIFICANTLY BUT INCOMPLTELY
39 Incremental Reduction of LDL New therapeutic strategies DOUBLING STATIN DOSE ONLY REDUCES LDL BY ADDITIONAL 6-7% ( CEILING EFFECT) It was not until 2015 that the ability to improve clinical CV outcomes by adding a non-statin lipid-lowering agent to a statin was confirmed in the IMPROVE IT STUDY This finding is particularly important in light of the conservative approach to adding non-statins in 2013 clinical guidelines. Moreover, the ability to improve clinical outcomes by incrementally reducing LDL-C levels has raised the expectations for other new classes of drugs, such as PCSK9 inhibitors.
40 OSLER-1 and -2 4,465 patients randomized open-label treatment with evolocumab (140 mg sq every 2 weeks or 420 mg monthly) vs standard therapy CV events nearly reduced by 50% OSLER Sabatine MS, et al. NEJM 2015

41 ODYSSEY Long-Term 2,300 patients randomized to 150 mg of alirocumab or placebo as a 1-mL subcutaneous injection every 2 weeks for 78 weeks. MACE reduced to 1.7% in the alirocumab group vs 3.3% in the placebo group (p=0.02)


42 Shift in Distribution of LDL-C in a Population of High-Risk Individuals With Use of PCSK9 Inhibitor MEAN LDL 47 Mean LDL 123 Am Coll Cardiol 2015;65:
 High-risk: <2.6 mmol/l (100 mg/dl) <1.")
43 % patients LONG TERM : Most Patients Receiving Alirocumab on Background Statin ± Other LLT Achieved LDL-C Goals 90 P< P< % 79% Proportion of patients reaching LDL-C goal at Week 24 Very high-risk: LDL-C <1.8 mmol/l (70 mg/dl) High-risk: <2.6 mmol/l (100 mg/dl) <1.8 mmol/l (70 mg/dl) regardless of risk Alirocumab Placebo % 8% 0 Intent-to-treat (ITT) analysis; LLT = lipid-lowering therapy Robinson et al. N Enl J Med 2015;372(16):
 at 12 weeks")
44 Proportion Achieving Goal (%) LDL Cholesterol Goals 73 % ACHIEVED <70 LDL Standard of care alone Evolocumab plus standard of care P<0.001 P< <100 <70 LDL-C Goal (mg/dl) at 12 weeks
45 Use of COMBINATION OR ALTERNATE THEARPY to address statin intolerance and statin non adherence CAN STATIN NON ADHERANCE AND INTOLERANCE AND ITS RESULTANT INCREASED CV RISK BE CHANGED?
46 Percent of patients continually refilling Rx Adherence to statins after two years, by condition EVEN IN HIGH RISK 50% 40% 30% 20% 10% 0% 40% Acute coronary syndrome 36% Chronic coronary artery disease 24% Primary prevention Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA 2002;288:
 Failure to understand the need for the medication High out-of-pocket costs Benner JS, Glynn RJ, Mogun H, Neumann")
47 Why don t patients adhere to their medication therapy? Complex therapies Side Effects ( WELL PUBLICIZED IN MEDIA) Failure to understand the need for the medication High out-of-pocket costs Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J. Long-term persistence in use of statin therapy in elderly patients. JAMA 2002;288:
 Non-adherence to cardioprotective medications increased risk of cardiovascular hospitalizations (10% to 40%) and mortality (50% to 80%) Poor adherence to heart failure medications")
48 Non-adherence Mortality, Hospitalizations, ED Visits Non-adherence causes ~30% to 50% of treatment failures and 125,000 deaths annually Non-adherence to STATINS increased relative risk for mortality (~12% to 25%) Non-adherence to cardioprotective medications increased risk of cardiovascular hospitalizations (10% to 40%) and mortality (50% to 80%) Poor adherence to heart failure medications increased the number of cardiovascular-related emergency department (ED) visits Sources: Ho 2009, Circulation; Edmondson 2013, Br J of Health Psychology; George & Shalansky 2006, Br J Clin Phar

49 Note the percentage in the placebo arm

50 Insurance criteria Statin Intolerance

51


52 The GAUSS-3 Trial Goal Achievement after Utilizing an anti-pcsk9 antibody in Statin Intolerant Subjects-3 Steven E. Nissen MD MACC* Erik Stroes MD PhD *Disclosure Study Sponsor: Amgen Consulting: Many pharmaceutical companies Clinical Trials: Amgen, AstraZeneca, Cerenis, Eli Lilly, Novartis, Novo Nordisk, The Medicines Company, Orexigen, Takeda, and Pfizer. Companies are directed to pay any honoraria, speaking or consulting fees directly to charity so that neither income nor tax deduction is received.
 of patients with a history of symptoms.")
53 SMS Controversy has surrounded the issue of statin- associated muscle symptoms because of large differences in the incidence of this disorder in randomized trials and observational studies. The GAUSS-3 trial demonstrates that muscle-related intolerance is reproducible during blinded statin rechallenge in a substantial fraction (about 40%) of patients with a history of symptoms. Accordingly, development of alternative approaches to LDL-C reduction for these patients represents an important medical priority.
54 Study Design: Two Double-Blind Phases Phase A 511 patients enrolled at 53 centers with a history of intolerance to multiple statins due to muscle-related adverse effects. 10 weeks Atorvastatin 20 mg Placebo 10 weeks Atorvastatin 20 mg Placebo Phase B 24 weeks Patients proceeded to Phase B only if they had intolerable muscle symptoms on atorvastatin, but not placebo, or CK 10 x ULN during prior statin treatment Monthly SC evolocumab 420 mg 2 1 Daily oral ezetimibe 10 mg
55 HDL-C (mg/dl) Selected Baseline Characteristics Characteristic Phase A (n=491) Phase B (n=218) Ezetimibe (n=73) Evolocuma b (n=145) Age (years) Male Gender 50% 47% 54% Coronary Heart Disease 35% 29% 33% NCEP-ATP III High Risk 63% 52% 58% Intolerance to 3 statins 82% 82% 82% Total Cholesterol (mg/dl) LDL-C (mg/dl)
56 Phase A: Study Drug Discontinuation Events Intolerable Muscle Symptoms N = 491 On atorvastatin, but not placebo 209 (42.6%)* On placebo, but not atorvastatin 130 (26.5%) On both placebo and atorvastatin 48 (9.8%) No symptoms on either treatment 85 (17.3%) Did not complete Phase A 20/511 Bypassed Phase A due to CK elevation 10 x ULN 19 (3.9%)* *218 of these 228 eligible patients proceeded to Phase B
57 Percent Change in LDL-C (%) LDL-C Values Over Time During Phase B Mean reduction 16.7% (LDL-C = 181 mg/dl) Ezetimibe Mean reduction 53.0% (LDL-C = 104 mg/dl) Weeks Following Randomization in Phase B

58 Percent of Patients (%) Percent of Patients (%) Achievement of Common LDL-C Target Levels 65% OF TRUE SMS PTS DID ACHIEVE A TARGET LDL-C < 70 mg/dl LDL-C < 100 mg/dl* 100% 100% 80% 80% P< % 60% 60% 40% P< % 40% 20% 20% 0% 1.4% Ezetimibe Evolocumab 0% 1.8% Ezetimibe Evolocumab *not a protocol prespecified analysis
59 Phase B: Time to Any Muscle-Related Cumulative Event Probability Ezetimibe Evolocumab Symptom HR = % CI, P =.17 Both drugs uncommonly 0 induced muscle symptoms leading to discontinuation (ezetimibe 6.8%, evolocumab 0.7%) Days Following Randomization 28.8% 20.7%
 report muscle-related symptoms when administered placebo, but not atorvastatin.")
60 Conclusions A substantial proportion (42.6%) of patients with a history of muscle-related statin intolerance have symptoms when rechallenged with atorvastatin 20 mg, but not placebo. A smaller fraction of patients (26.5%) report muscle-related symptoms when administered placebo, but not atorvastatin. In patients with statin-associated muscle symptoms, evolocumab, compared with ezetimibe, produced significantly larger reductions in LDL-C and other atherogenic lipoproteins. Both drugs uncommonly induced muscle symptoms leading to discontinuation (ezetimibe 6.8%, evolocumab 0.7%).
 4 High / Very High CV Risk Population Previous MI / stroke / CVD or multiple CV risk factors incl.")
![T2DM Difficult to achieve LDL- C goals, despite current therapies 5 20% with CHD not at goal (<100 mg/dl [2.6 mmol/l]) 59% at very high CV risk not at goal (<70 mg/dl [1.](/docs-images/75/72246550/images/61-2.jpg "8 mmol/l]) Statin-Intolerant Population 10-15% on highintensity statins show intolerance 6 Many discontinue due to muscle pain and/or weakness Nearly all patients who need considerable LDL-C")
61 Patient Populations with HIGH Unmet Need for Additional LDL-C Lowering 62 FH Population in EU Genetic disorder High risk of early CHD HeFH prevalence 1:200 to 1:250 1,2 Untreated LDL-C of mg/dl 3 79% with HeFH not at goal (<100 mg/dl [2.6 mmol/l]) 4 High / Very High CV Risk Population Previous MI / stroke / CVD or multiple CV risk factors incl. T2DM Difficult to achieve LDL- C goals, despite current therapies 5 20% with CHD not at goal (<100 mg/dl [2.6 mmol/l]) 59% at very high CV risk not at goal (<70 mg/dl [1.8 mmol/l]) Statin-Intolerant Population 10-15% on highintensity statins show intolerance 6 Many discontinue due to muscle pain and/or weakness Nearly all patients who need considerable LDL-C reductions will not reach goal 1 Nordestgaard et al. Eur Heart J 2013;34: Sjouke et al. Eur Heart J Mar 1;36(9): ESC/EAS Guidelines for the management of dyslipidaemias Eur Heart J. 2011;32(14): Pijlman et al. Atherosclerosis 2010;209: Virani et al. Am Heart J 2011;161: Arca et al. Diabetes Metab Syndr Obes 2011;4:


62
63 Guideline Update 2016 COMBINATION THERAPY Incorporates RCT data since 2013 as well as expert consensus Clearly addresses benefit in RCT from non statin therapies Re assesses the high risk groups that residual risk and further management of dyslipidemia that benefit from PCSK9 and Ezitimibe with no evidence of harm Niacin and fibrates as add on therapy remain out - lack of benefit and possible harm
64 HIGH RISK MARKERS The Committee identified several high-risk markers that may be informative, including: 10-year ASCVD risk 20%; Primary LDL-C 160 mg /dl at baseline; Other major ASCVD risk factor(s) that are poorly controlled Family history of premature ASCVD with or without elevated lipoprotein(a) Evidence of accelerated subclinical atherosclerosis (e.g., coronary artery calcification) Elevated hs-crp; and other risk-modifying conditions, such as CKD, HIV, and chronic inflammatory disorders.

65 1-SECONDARY PREVENTION CVD ALREADY ON STATIN


66 2-Patient with established ASCVD and Comorbiditites SECONDARY PREVENTION OF CVD ON STATIN ASCVD+DM VERY HIGH RISK= TARGET LDL<70

67 3-SECONDARY PREVENTION, LDL>190 ON STATIN (LIKELY HEFH)

68 4-PRIMARY PREVENTION & PRIMARY LDL >190, ON STATIN( LIKELY HEFH)

69 5-DIABETICS 40-75, LDL , ON STATIN FOR PRIMARY PREVENTION


70 6-PRIMARY PREVENTION, YEARS, LDL & CVD RISK >7.5%
71 Diagnose & manage secondary causes of dyslipidemia Optimally manage other ASCVD risk factors Implement appropriate nutrition and physical activity Administer maximally tolerated statin Lipid blood testing to assess if LDL-C level exceeds threshold LDL OF 70 (or 100) treatment level. If so... Add non-statin therapy DCV Medical Affairs Reassess &Treat to lipid goals
72 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk If, after these interventions, the patient still has <50% reduction in LDL-C (and may consider LDL-C 70 mg/dl), the patient and clinician should enter into a discussion focused on shared decision making regarding the addition of a non-statin medication to the current regimen. DCV Medical Affairs
73 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk In the opinion of the Expert Consensus Writing Committee, in a patient with ASCVD and baseline LDL-C 190 mg/dl* with <50% reduction in LDL-C (and may consider LDL-C 70 mg/dl) it is reasonable to consider a PCSK9 inhibitor as a first step rather than ezetimibe or BAS given PCSK9 inhibitors greater LDL-C lowering efficacy. *THESE ARE PROBABLE HEFH PTS DCV Medical Affairs
74 Combination Therapy Updates: Data indicate that combination therapy with ezetimibe also brings a benefit that is in line with the Cholesterol Treatment Trialists (CTT) Collaboration meta-analysis supporting the notion that LDL-C reduction is key to the achieved benefit independent of the approach used. They are recommended as combination therapy with statins in selected patients when a specific goal is not reached with the maximal tolerated dose of a statin. Patients with dyslipidaemia, particularly those with established CVD, DM or asymptomatic high-risk individuals, may not always reach treatment goals, even with the highest tolerated statin dose. Therefore, combination treatment may be needed. It must be stressed, however, that the only combination that has evidence of clinical benefit (one large RCT) is that of a statin combined with ezetimibe Downloaded from by guest on May 24,
75 PCSK9 Inhibitors Regarding new therapies, recent data from phase I III trials show that PCSK9 inhibitors sharply decrease LDL-C by up to 60%, either as monotherapy or in addition to the maximal statin dose. Whether this approach results in the predicted reduction in CV events is being addressed in large outcome trials; preliminary evidence suggests that this is the case.
76 When to consider PCSK9 Inhibitors 1. FH-Het. 2. High risk patients with ASCVD (recurrent ASCVD events). 3. Patients with ASCVD not attaining the goal on maximally tolerated Statin and Ezetimibe. 4. Statin Intolerance.

77 Thank You
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
PCSK9 inhibition across a wide spectrum of patients: One size fits all?
 PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Cholesterol; what are the future lipid targets?
 Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Management of LDL as a Risk Factor. Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil
 Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Management of LDL as a Risk Factor Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Consulting for: Merck, Astra Zeneca, ISIS- Genzyme, Novo-Nordisk, BMS, Pfizer,
Inhibition of PCSK9: The Birth of a New Therapy
 Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia. Prof. Alberto Corsini University of Milan, Italy
 Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
March 30, 2014, Joint ACC/JAMA Late-breaking Clinical Trials Session 402 American College of Cardiology, Washington DC
 A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
A Phase 3 Double-blind, Randomized Study to Assess Safety and Efficacy of Evolocumab (AMG 145) in Hypercholesterolemic Subjects Unable to Tolerate an Effective Dose of Statin Erik Stroes 1, David Colquhoun
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Familial Hypercholeterolaemia
 Familial Hypercholeterolaemia Is it all about statins? Gerald F Watts DSc PhD MD FRACP FRCP Professor and Head, Cardiometabolic Service, Department of Cardiology, Royal Perth Hospital School of Medicine,
Familial Hypercholeterolaemia Is it all about statins? Gerald F Watts DSc PhD MD FRACP FRCP Professor and Head, Cardiometabolic Service, Department of Cardiology, Royal Perth Hospital School of Medicine,
The ACCELERATE Trial
 The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
The ACCELERATE Trial Impact of the Cholesteryl Ester Transfer Protein Inhibitor Evacetrapib on Cardiovascular Outcome Stephen J Nicholls for the ACCELERATE investigators Disclosure Research support: AstraZeneca,
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
New Approaches to Lower LDL-C
 New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
 1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia
 for hypercholesterolemia") Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ). Following NCPE assessment of the applicant
Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ). Following NCPE assessment of the applicant
Nephrologisches Zentrum Göttingen GbR Priv. Doz. Dr. med. V. Schettler
 Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Cardiovascular Controversies: Emerging Therapies for Lowering Cardiovascular Risk
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Lipid Lowering in Patients at High Risk for Cardiovascular Disease
 Lipid Lowering in Patients at High Risk for Cardiovascular Disease Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Novel
Lipid Lowering in Patients at High Risk for Cardiovascular Disease Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Novel
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
Oppenheimer 29th Annual Healthcare Conference Mark Timney, Chief Executive Officer
 Oppenheimer 29th Annual Healthcare Conference Mark Timney, Chief Executive Officer New York City 20th March 2019 1 Safe Harbor Forward-looking statements Statements contained in this presentation about
Oppenheimer 29th Annual Healthcare Conference Mark Timney, Chief Executive Officer New York City 20th March 2019 1 Safe Harbor Forward-looking statements Statements contained in this presentation about
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
*Carbohydrate & Lipid Metabolism Research Unit, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa
 Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
Tuesday, May 26, 2015 Clinical Breakthroughs: Modifying LDL Cholesterol to Prevent CV Events International Society of Atherosclerosis, Amsterdam, Netherlands Long-term Treatment With Evolocumab in Patients
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE)
") Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
New Lipid Lowering Agents (PCSK9 Inhibitors, Bempedoic Acid, Apabetalone) in the Elderly? The State of the Recent Knowledge Prof.
 in the Elderly? The State of the Recent Knowledge Prof.") New Lipid Lowering Agents (PCSK9 Inhibitors, Bempedoic Acid, Apabetalone) in the Elderly? The State of the Recent Knowledge Prof. Maciej Banach Łódź, PL According to : Central Intelligence Agency". Retrieved
New Lipid Lowering Agents (PCSK9 Inhibitors, Bempedoic Acid, Apabetalone) in the Elderly? The State of the Recent Knowledge Prof. Maciej Banach Łódź, PL According to : Central Intelligence Agency". Retrieved
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Early Clinical Development #1 REGN727: anti-pcsk9
 Early Clinical Development #1 REGN727: anti-pcsk9 July 15, 2010 Neil Stahl, Ph.D. Senior Vice President Research and Development Sciences 1 Safe Harbor Statement Except for historical information, the
Early Clinical Development #1 REGN727: anti-pcsk9 July 15, 2010 Neil Stahl, Ph.D. Senior Vice President Research and Development Sciences 1 Safe Harbor Statement Except for historical information, the
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
2/10/2016. Patient-Centered Management of Dyslipidemia. No disclosures. What is Patient-Centered Management?
 Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine
 Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies
 Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
Efficacy, Safety and Tolerability of 150 mg Q2W Dose of the PCSK9 mab REGN727/SAR236553: Data from Three Phase 2 Studies Michael J. Koren, 1 Evan A. Stein, 2 Eli M. Roth, 3 James M. McKenney, 4 Dan Gipe,
2017 Update in Internal Medicine: Clinical Dyslipidemia Update
 2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia.
 for primary hypercholesterolemia and mixed dyslipidemia.") Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia. The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ) Following
Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia. The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ) Following
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Anne Carol Goldberg, MD, FACP, FAHA, FNLA Washington University, St. Louis, MO USA
 Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Efficacy and Safety of Bempedoic Acid Added to Maximally Tolerated Statins in Patients with Hypercholesterolemia and High Cardiovascular Risk: The CLEAR Wisdom Trial Anne Carol Goldberg, MD, FACP, FAHA,
Cholesterol Reduction Therapy in 2018 A Perspective Role Of Statins, Ezetimibe and PCSK9-Inhibitors
 USC-April 21, 2018, Los Angeles Cholesterol Reduction Therapy in 2018 A Perspective Role Of Statins, Ezetimibe and PCSK9-Inhibitors P.K.Shah, MD, MACC Shapell and Webb Chair in Clinical Cardiology, Director,
USC-April 21, 2018, Los Angeles Cholesterol Reduction Therapy in 2018 A Perspective Role Of Statins, Ezetimibe and PCSK9-Inhibitors P.K.Shah, MD, MACC Shapell and Webb Chair in Clinical Cardiology, Director,
Results of the GLAGOV Trial
 Results of the GLAGOV Trial Global Assessment of Plaque Regression with a PCSK9 Antibody as Measured by Intravascular Ultrasound Steven E. Nissen MD Stephen J. Nicholls MBBS PhD Consulting: Many companies
Results of the GLAGOV Trial Global Assessment of Plaque Regression with a PCSK9 Antibody as Measured by Intravascular Ultrasound Steven E. Nissen MD Stephen J. Nicholls MBBS PhD Consulting: Many companies
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Industry Relationships and Institutional Affiliations
 Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher
Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated daily statin: results from the ODYSSEY COMBO II study Christopher