Biliopancreatic limb length is more important than the name of the Gastric bypass operation
|
|
|
- April Rich
- 5 years ago
- Views:
Transcription

 Adjunct Associate Professor of Surgery, UAE University COM Chief, Division of General,")
1 Biliopancreatic limb length is more important than the name of the Gastric bypass operation Abdelrahman A. Nimeri, MBBCh, ABS, FACS, FASMBS President, Pan Arab Society of Metabolic & Bariatric Surgery (PASMBS) Adjunct Associate Professor of Surgery, UAE University COM Chief, Division of General, Thoracic, & Vascular Surgery, SKMC Director, Bariatric & Metabolic Institute (BMI) Abu Dhabi, SKMC


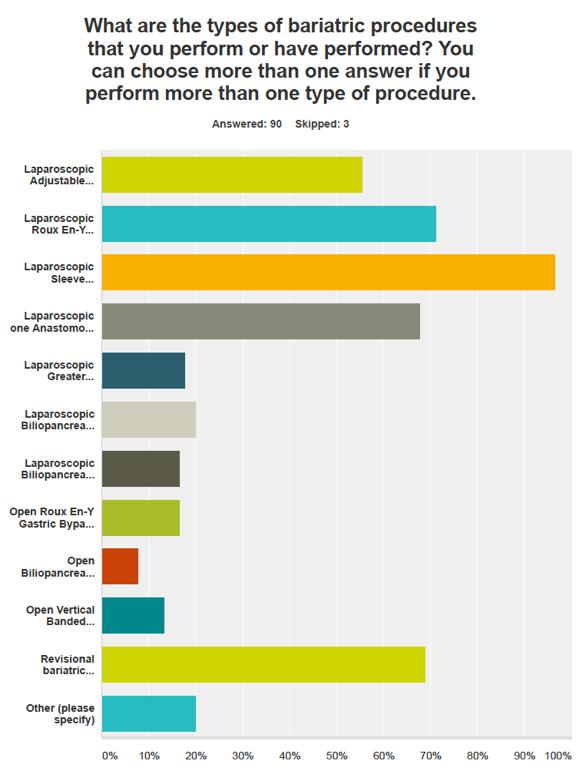
2 LAGB 2% Revision 17% Case Mix Disclosure No disclosures OAGB MGB 2% LoopDS 0% LSG LSG 33% RYGB LAGB Revision Communications Committee RYGB 46% OAGB MGB LoopDS
3 Take Home Message Why is RYGB becoming un-popular? Is it still the Gold standard? RYGB in it s standard short BPL is a restrictive operation with very little mal-absorption and not for every patient. Best candidates (Type II DM, GERD patients) & Worst candidates (BMI >50, weight regain after restrictive bariatric surgery). If you perform BPD, DS, SADI, DJB, OAGB/MGB you need to measure the common channel. Melton GB et al Suboptimal weight loss after RYGB J Gastrointestinal Surg 2008;12(2):250-5 Bessler M et al Frequency distribution of weight loss % after RYGB and LAGB SOARD 2008:4(4): Campos Good morning et al Factors associated with weight loss after RYGB. Arch Surg 2008:143(9):877-84
4 Take Home Message OAGB/MGB is more effective than RYGB for weight loss and comorbidity resolution because it has a longer BPL. RYGB patients with weight regain is not a dead end. Length of Roux limb is less important than BPL. In weight recidivism after RYGB: the answer is in judicial lengthening of the BPL & patients with BMI>50 & failure after restriction may benefit from a longer BPL.
5 The fall of RYGB, rise of LSG & OAGB/MGB

6 Bariatric surgery numbers in the USA
7 History of bariatric surgery in the US looks like this
8
9 World wide 2014
10 North American USA & Canada
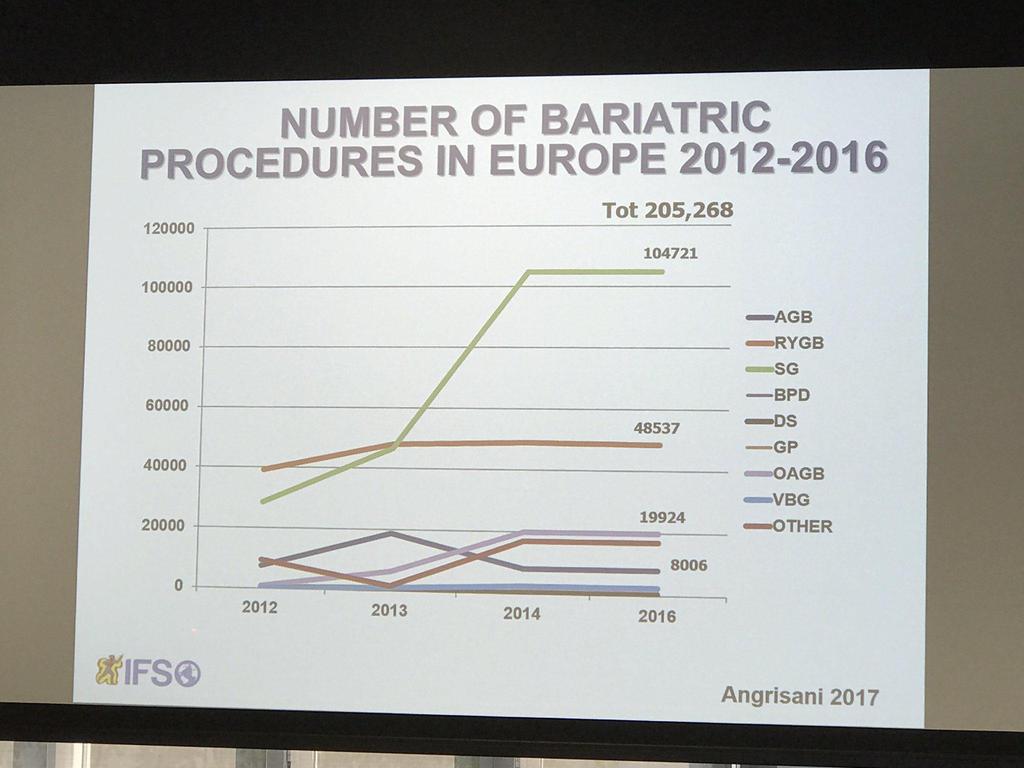
11 Europe
12 Asia Pacific
13
14
15 OAGB/MGB in the UAE is 13% in 2016 up from 7% Total LSG OAGB/MGB RYGB LAGB
16 Latin America
17 Why is RYGB becoming so un-popular and why are LSG and OAGB/MGB catching on? Poor long term outcomes. High incidence of complications. Ineffectiveness long term.
18
19
20
21 1156 patients with severe obesity comprised 3 groups: 418 patients After RYGB (surgery group), 417 patients who sought but did not undergo surgery (primarily for insurance reasons) (non-surgery group 1), and 321 patients who did not seek surgery (non-surgery group 2). We performed clinical examinations at baseline and at 2 years, 6 years, and 12 years to ascertain the presence of type 2 diabetes, hypertension, and dyslipidemia. The follow-up rate exceeded 90% at 12 years.
22
23
24
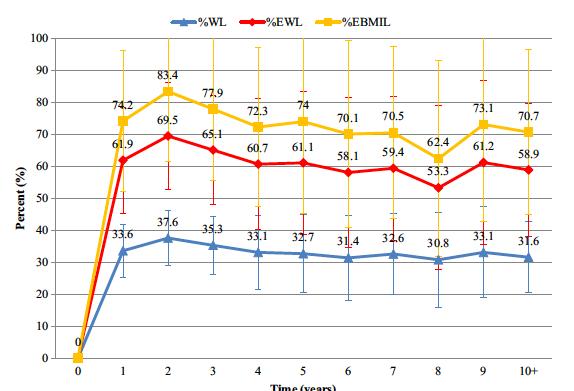
25 Long term FU years after RYGB in Italy 285 RYGB patients done between Mean BMI 45.3 (+5.9) kg/m2 went down to 33.5 (5.1) kg/m2 at 8 years, 33.8 (5) kg/m2 at 10 years, 30.5 (4.1) kg/m2 at 12 years & 32.6 (4.7) kg/m2 at 14 years (69% achieved BMI <35 kg/m2). Mean EWL% 66.3% (+21) at 8 years, 64.2% (+23) at 10 years, 76.7% (+21) at 12 years & 69.8% (+23) at 14 years. FU% was 91%, 84%, 72% and 63% at 8,10,12 & 14 years. Mortality 0.35%, leak 0.7%, stenosis 1%, IH 1.4%, SBO 7.3%. 60% of patients stopped taking supplements and 35.7% had nutritional deficiencies. R. Arnoux Dabadie Abstract IFSO London 2017
26
27
28
29 Diabetes resolution 6 years after LSG, RYGB, Medical therapy in France All patients undergoing bariatric surgery in France in 2009 & control group matched (age, gender BMI, DM) from French National Insurance. 15,650 (85% females, 10% had DM II) had bariatric surgery in Diabetes resolution after BS was 50% vs 9% medical therapy P< The main predictive for resolution were: RYGB 16.7 ( ), LSG 7.3 ( ), LAGB 4.3 ( ), No insulin 5.8 ( ), No dyslipidemia medications 1.3 ( ). DM recurrence at 6 years was least frequent with BS 1% vs 12% in control (P<0.001). RYGB 0.06 was the more effective than LSG 0.08 & LAGB J. Thereaux, A. Fagot-Campagna France Abstract IFSO London
30 5 year results of the Swiss RCT LSG vs RYGB (SM-BOSS) RCT of 217 patients LSG 107 vs RYGB 110 at 4 centers in Switzerland. Mean BMI 44+11, Age 43+5, 72% females, mean FU 5 years (95.4%). Patients with severe GERD or Hiatal hernia were excluded. Weight loss was similar at 1 year ( vs ) P=0.13, 3 years (71+23 vs ) P=0.3, 5 years ( vs 68+25) P=0.11. Weight loss after LSG at 5 years was inferior to RYGB (25+11 vs ) P Co-morbidity resolution was significantly reduced in both except GERD which was better with RYGB. QOL, number of complications and re-operations were similar. R. Peterli, M. Bueter Abstract IFSO London 2017
31 LAGB to RYGB is more effective than LAGB to LSG 192 patients LAGB to RYGB vs 283 LAGB to LSG. The baseline age and BMI were similar in both groups. At 2 years, BMI was lower in RYGB vs kg/m2 for LSG (P=0.0004), EBMIL% was lower in RYGB 57.8% vs 29.3% in LSG (P=0.0001), & %WL was lower in RYGB 23.4% vs 12.6% in LSG (P=0.001). Reoperation was higher in conversion to RYGB 7.3% vs 1.4% (P0=0022), OR time was longer in RYGB vs minutes in LSG (P<0.001), LOS was longer RYGB 3.33 vs 2.11 days (P<0.001). Readmission was similar in RYGB 7.3% vs 3.5% in LSG (P=0.087). M. Jenkins B Schwack Abstract IFSO London 2017
. The chance of developing de novo reflux after LSG was 47.8% (32/67).")
32 50% GERD from 17% at 8.5 years 100 LSG after long-term mean FU 8.5 years (%EWL) of 60%. A significant increase in GERD symptoms (50% from 17% pre op) (RR = , 95% CI [ ], & use of PPIs, p value = ). The chance of developing de novo reflux after LSG was 47.8% (32/67). Reflux disease was present in 7 of the 26 patients who underwent a secondary Roux- en-y gastric bypass (RYGB). In 4/7 patients, GERD disappeared completely after the secondary RYGB (57.1%).
33 68% GERD from 33% at 5 years 17.2% Barretts Esophagitis 69% Follow up A total of 110 patients after LSG, GERD symptoms(68.1% versus 33.6%: P , VAS mean score3 versus 1.8: P , and PPI intake significantly increased compared with preoperative values;57.2% versus 19.1%: P ) At EGD, an upward migration of the Z line and a biliary-like esophageal reflux was found in 73.6% and 74.5% of cases, respectively.
 43/53 patients were followed, 6 patients (14.0%) were converted to RYGB due to GERD over a period of 130 months. 10/26 (38.")
34 14% conversion to RYGB 23% weight regain 38.4% GERD15% Barretts metaplasia De novo GERD in 45% patients 100% Follow up 10.8 years Multi-Center study (3 centers) 43/53 patients were followed, 6 patients (14.0%) were converted to RYGB due to GERD over a period of 130 months. 10/26 (38.4%) not converted to RYGB also suffered from symptomatic reflux. Gastroscopies revealed de novo hiatal hernias in 45% of the patients & Barrett s metaplasia in 15%. SG patients suffering from symptomatic reflux scored significantly higher in the RSI (p = 0.04) and significantly lower in the GIQLI (p = 0.02) questionnaire.
35
36 Why is RYGB becoming so un-popular and why are LSG and OAGB/MGB catching on? Poor long term outcomes. High incidence of complications. Ineffectiveness long term.
 The perceived paucity of options to treat patients with weight recidivism especially when your are super obese.")
37 (1) The steep learning curve. (2)?Re routing of the small bowel (OAGB/MGB). (3) Potential known long term complications. (4) The perceived paucity of options to treat patients with weight recidivism especially when your are super obese. In contrast, (1) the short learning curve, (2) no re routing of the small bowel, (3) unknown long term complications and (4) the many options to revise a LSG to a duodenal switch or LRYGB are the reasons patients and surgeons are choosing the LSG over LRYGB.
38 Learning curve & adoption of laparoscopic colectomy less than 1/3 of colectomies 2.2% (878/38,264) for % (1175/42,166) for % (2336/44,817) for 2004 Publication of the COST Trial. 15% (7548/42,903) for % (14,610/31,888) for Ann Surg Aug;258(2): doi: /SLA.0b013e31828faa66. Growth of laparoscopic colectomy in the United States: analysis of regional and socioeconomic factors over time. Bardakcioglu O 1, Khan A, Aldridge C, Chen J.
39 Only patients with >50% EWL at 1 year postoperatively. A total of 1426 obese patients (15.8% male) after RYGB during January 2000 to 2012 (2 year FU). Weight regain was observed in 244 patients (17.1%). Preoperative BMI was similar between groups. BMI was significantly higher and percent excess weight loss was significantly lower in the Weight Regain (WR) group (P 0.001).
40 Univariate analysis found that older age, male gender, having hypertension, dyslipidemia, and insulin-treated type 2 diabetes were all factors associated with sustained weight loss. A longer duration after RYGB was associated with weight regain. Multivariate analysis revealed that younger age was a significant predictor of weight regain even after adjusting for time since RYGB.

41 Why do RYGB patients regain weight?
42 Small pouch & rapid emptying leads to better weight loss, less weight D Riccioppo I Cecconello abstract IFSO London 2017 regain and better food intolerance in RYGB 67 RYGB patients had pouch volumetry by 3D-CT, pouch emptying by 4hr Scintigraphy, food intolerance and weight loss measurement. Median FU was 47 months, median volume was 28 ml, %ret at 1,2,4 hours was 8%, 2%, 1%. There was association between V<40ml & higher emptying rates up to 2 hours (V<40 %Ret 1=6%, %Ret2=2%) P=0.009 vs (V>40 %Ret 1=44%, %Ret2=13.5%) P= Higher emptying speed at 1 hour correlated with higher weight loss (P=0.033) and less weight regain (P=0.036) (%Ret<12% vs >25%). Better food tolerance with lower %Ret 1 hour (0.003).
43
44
45 2 decades ago, if a patient was considering a surgery involving small bowel rerouting, it would have been (RYGB) or (BPD). In contrast, today, if a patient is considering a surgery that involves small bowel rerouting, this could mean any of the following bariatric surgeries: one anastomosis gastric bypass/mini gastric bypass (OAGB/MGB) BPD or BPD duodenal switch (DS) single anastomosis duodenoileostomy (SADI) single anastomosis gastroileostomy (SAGI) single anastomosis sleeve ileostomy (SASI) duodenojejunal bypass (DJB), or stomach intestinal pylorus sparing surgery (SIPS)
46 Assuming Small bowel length is 400 cm in length Approximate stomach size in ml BPD BPD/DS SADI OAGB MGB DJB RYGB Roux limb in cm NA NA NA 100 Common Channel Alimentary limb (Roux limb + CC) BPL
47 Assuming Small bowel length is 600 cm in length Approximate stomach size in ml BPD BPD/DS SADI OAGB MGB DJB RYGB Roux limb in cm NA NA NA 100 Common Channel Alimentary limb (Roux limb + CC) BPL
48 Assuming Small bowel length is 800 cm in length BPD BPD/DS SADI OAGB MGB DJB RYGB Approximate stomach size in ml Roux limb in cm NA NA NA 100 Common Channel Alimentary limb (Roux limb + CC) BPL
49 This is why you have to measure the common channel in patients undergoing any mal-absorptive surgery (BPD, BPD-DS, SADI, DJB, or OAGB/MGB) but not in RYGB with a short BPL

50 The concept of OAGB/MGB is valid & useful in: Super-obese, failure after restrictive surgery, failure after Roux-en Y gastric bypass

51 60 cm BPL 200 cm BPL
52
53
54
55
56
57 RCT long vs short BPL for type II DM patients 114 diabetic patients had RYGB with different BPL length: 73 had LBPL (200cm) & 41 had SBPL (84+2cm) & followed for 5 years. DM remission at 5 years was higher in LBPL 73.1% vs SBPL 55%, P<0.05), lower relapse rate (11.9% vs 32%, P<0.05) & less need for diabetic medications (P<0.05). Mixed meal test was done for 11 LBPL & 9 SBPL patients, patients with LBPL had higher GLP-1 at 45 minutes (P<0.05), higher AUC (P=0.01), lower GIP level at 15 minutes (P<0.01), lower insulin and C peptide at 30 minutes (P,0.001) compared to SBPL. M. Guimaraes MP Monteiro Abstract IFSO London 2017
58 RCT: conversion of LAGB to LBPL vs SBPL RYGB 146 patients had conversion of LAGB to RYGB with LBPL (150 cm) 73 patients vs SBPL (75 cm) 73 patients. Both groups were similar in baseline charachtaristics. At 3 years FU was 91%, total body weight loss was 24% for LBPL vs 20% for SBPL, P=0.039). Co-morbidity resolution was no different between two groups. Short term complications in 10% (6% LBPL & 4% SBPL) NS. A. Boerboom F Berends Abstract 0.158
59 RCT of 144 patients primary RYGB 70 patients with Roux/BPL vs 75/ patients with Roux/BPL 150/75 at 48 months (FU 90%). At 24 months, EWL% was better with long BPL 150 cm 84% vs 73% in short BPL 75 cm (P=0.002). EWL% was similar at 48 month 70% vs 62% (P=0.068). Type II DM was present in 33% (48 patients), complete remission was similar in both 78% vs 75% (P>0.05). Short and long term complications were similar. F. Berends I. Janssen Abstract IFSO London 2017




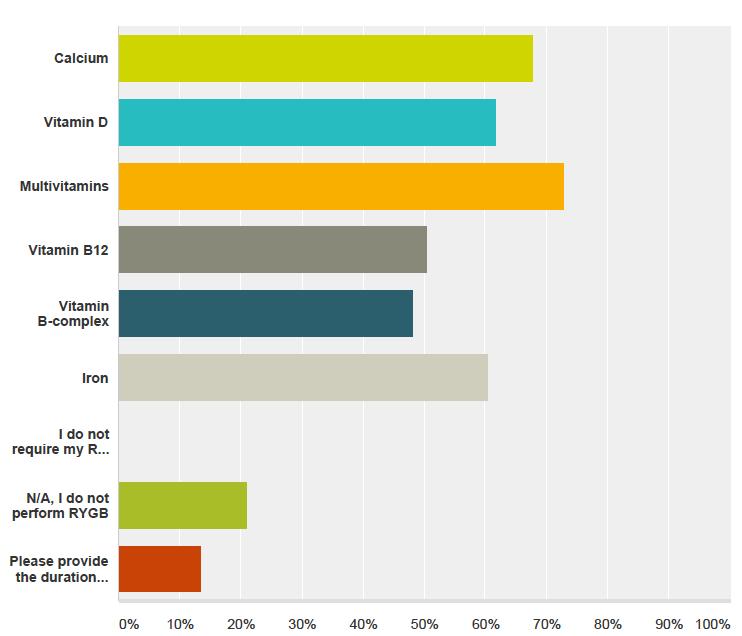
60 Nutritional deficiencies are unrecognized in approximately 50% of patients who undergo RYGB surgery. Routine supplements: Calcium. iron. Multivitamins. B 12 An ounce of prevention is better than a pound of cure John et al J Am Osteopath Assoc.2009;109:
61 Nutritional deficiencies 5 years after LSG 108 patients had LSG (81 females). Median EWL% 1 year 85.6% (weight loss maintained at 5 years) median EWL%74.5% Pre operative nutritional deficiencies Low Hgb 19.4%, iron 26.7%, ferritin 6% folate 2%, B12 3.1%, magnesium 34.4%, PTH elevation 3.4%. At 5 years, significantly more patients had anemia 40.1% (P=0.001), low ferritin 44% (P<0.001), low vitamin D 12.6% (P=0.07). This highlights the need for long term supplements for LSG. D. Karavias I. Kehagias abstract 0.074
62 Nutritional deficiencies 3 years after LSG 857 patients had LSG (609 females). Age 47+12, mean BMI Weight loss at 1,2,3 years was 37+14, & Kgs. Pre operative nutritional deficiencies Low Hgb 11%, low vit D 57 %, ferritin 14%, low B12 2% & PTH elevation 327%. At 3 years, significantly more patients had anemia 14% (P=0.02), low ferritin 23% (P<0.008), high PTH 16% (P value 0.008), low vitamin D 18% (P=0.005). This highlights the need for long term supplements for LSG. N. Zaeshenas Jjogensen abstract 0.071
63 Vitamin & mineral deficiencies 4 years after LSG Fit for me RCT of 150 patients after LSG standard multivitamin SMVS vs WLSO optimum (B12 400%, iron 150%, folic acid 150%). Weight, BMI, gender, iron, B12 folic acid vit D & total body weight loss were similar (28.8% for WLSO vs 28.6% for SMVS) P>0.48. At mean follow up of 4 years, vitamin B12 deficiency was lower for WLSO 14% vs 27%, ferritin 11% vs 23%, E Aarts F BeredsAbstract 0.168
64
65
66 Need for Intensive Nutrition Care After Bariatric Surgery: Is Mini Gastric Bypass at Fault? Patients at clinical nutrition ICU from 2013 to Twelve patients required enteral nutrition or parenteral nutrition (7 OAGB/MGB (58.3%), 2 underwent a RYGB, 2 had a LSG, and 1 had LAGB. OAGB led to more severe nutrition complications requiring intensive nutrition care and therefore cannot be considered a "mini" bariatric surgery. OAGB is often considered a simplified surgical technique, it obviously requires as the other standard bariatric procedures a close follow-up by experimented teams aware of its specific complications. Bétry C et al JPEN J Parenter Enteral Nutr Mar 9.
67 Laparoscopic reversal of mini-gastric bypass to original anatomy for severe postoperative malnutrition. A 10-year study of Reversal MGB for severe and refractory malnutrition syndrome after intensive nutritional support following MGB. 26 of 2934 patients had reversal 20.9 ± 13.4 months post-mgb. At presentation, mean (BMI) 22 ± 4.4 kg/m 2, (%EWL) ± 22.5%,, & albumin serum level 25.5 ± 3.6 gr/l. At surgical exploration, 8 of 12 (66.5%) patients had a biliary limb longer than 200 cm and 9 (34.6%) had bile reflux symptoms. After a mean follow-up of 8 ± 9.7 months, all patients experienced a complete clinical and biological regression of the SRMS after the RMGB despite a mean 13.9 kg weight regain in 16 (61.5%) patients. Overall reversal morbidity was 30.8% Langenbecks Arch Surg Aug 12. doi: /s [Epub ahead of print] Laparoscopic reversal of mini-gastric bypass to original anatomy for severe postoperative malnutrition. Genser L 1, Soprani A 2, Tabbara M 3, Siksik JM 4, Cady J 2, Carandina S 5.
68 Impact of BPL length on severe PCM requiring revisional surgery after one anastomosis (mini) gastric bypass The highest percentage of 0.51% (120/23,277) was recorded with formulae using >200 cm of BPL for some patients, and lowest rate of 0% was seen with 150 cm BPL. (survey study). J Minim Access Surg Jul 7. doi: /jmas.JMAS_198_16. [Epub ahead of print] Mahawar KK 1, Parmar C 1, Carr WRJ 1, Jennings N 1, Schroeder N 1, Small PK 1. Reply to "Key Features of an Ideal OAGB/MGB Pouch". Our study population consisted of the first patients that underwent a Mini Gastric Bypass (MGB) at our institution. At that time, we used a considerably long biliopancreatic (BP) limb ( cm), which proved to be too long for some patients in our series, and we have since then revised our technique accordingly Saarinen T, Juuti A. Obes Surg Jun;27(6):1632. doi: /s x.
69 70

70 Please Join our Facebook or Telegram groups 71


71
72
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
Long term laparoscopic Sleeve gastrectomy outcomes
 Long term laparoscopic Sleeve gastrectomy outcomes Gerhard Prager Department of General Surgery Metabolic and Bariatric Surgery Long-term results of gastric sleeve resection / Gerhard Prager Metabolic
Long term laparoscopic Sleeve gastrectomy outcomes Gerhard Prager Department of General Surgery Metabolic and Bariatric Surgery Long-term results of gastric sleeve resection / Gerhard Prager Metabolic
Disclosure. consultant to Ethicon Endosurgery. case mix disclosure. LRYGB sleeve BPD revisions OAGB ( minibp ), SADI: 0% 19% 55% 23%
, SADI: 0% 19% 55% 23%") Disclosure consultant to Ethicon Endosurgery case mix disclosure 3% 19% 23% 55% LRYGB sleeve BPD revisions OAGB ( minibp ), SADI: 0% Disclosure consultant to Ethicon Endosurgery case mix disclosure 3%
Disclosure consultant to Ethicon Endosurgery case mix disclosure 3% 19% 23% 55% LRYGB sleeve BPD revisions OAGB ( minibp ), SADI: 0% Disclosure consultant to Ethicon Endosurgery case mix disclosure 3%
ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass
 ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass WHICH OPERATION TO CHOOSE ANTHONY CLOUGH The options SURGICAL OPTIONS? - A MINEFIELD An explosion of operative variants Local technical variations Local
ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass WHICH OPERATION TO CHOOSE ANTHONY CLOUGH The options SURGICAL OPTIONS? - A MINEFIELD An explosion of operative variants Local technical variations Local
Current Status of Bariatric Surgery in Asia
 Emerald hall A, 1:2-1:5, November 7, 213 Current Status of Bariatric Surgery in Asia Go Wakabayashi, MD, PhD, FACS Professor and Chairman Department of Surgery Iwate Medical University Numbers of bariatric
Emerald hall A, 1:2-1:5, November 7, 213 Current Status of Bariatric Surgery in Asia Go Wakabayashi, MD, PhD, FACS Professor and Chairman Department of Surgery Iwate Medical University Numbers of bariatric
Welche Operation für welchen Patienten: Sleeve, Bypass oder?
 Welche Operation für welchen Patienten: Sleeve, Bypass oder?? Prof. Dr. med. Ralph Peterli Stv. Chefarzt Clarunis Leiter Forschungsplattform Viszeralchirurgie und bariatrisches Referenzzentrum Präsident
Welche Operation für welchen Patienten: Sleeve, Bypass oder?? Prof. Dr. med. Ralph Peterli Stv. Chefarzt Clarunis Leiter Forschungsplattform Viszeralchirurgie und bariatrisches Referenzzentrum Präsident
Management of the Bariatric. Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services. Surgery Patient 2017
 Management of the Bariatric Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services Surgery Patient 2017 Financial Disclosures None Objectives Identify the most commonly performed bariatric
Management of the Bariatric Farah A. Husain MD, FACS, FASMBS Division Chief, Bariatric Services Surgery Patient 2017 Financial Disclosures None Objectives Identify the most commonly performed bariatric
LONG TERM OUTCOMES OF SLEEVE GASTRECTOMY (LSG) Jacques Himpens, Gustavo Arman The European School of Laparoscopic Surgery Brussels Belgium
 Jacques Himpens, Gustavo Arman The European School of Laparoscopic Surgery Brussels Belgium") LONG TERM OUTCOMES OF SLEEVE GASTRECTOMY (LSG) Jacques Himpens, Gustavo Arman The European School of Laparoscopic Surgery Brussels Belgium DISCLOSURE DR HIMPENS IS A CONSULTANT WITH ETHICON ENDOSURGERY
LONG TERM OUTCOMES OF SLEEVE GASTRECTOMY (LSG) Jacques Himpens, Gustavo Arman The European School of Laparoscopic Surgery Brussels Belgium DISCLOSURE DR HIMPENS IS A CONSULTANT WITH ETHICON ENDOSURGERY
SLEEVEPASS RCT: SLEEVE vs. bypass 5-year results
 SLEEVEPASS RCT: SLEEVE vs. bypass 5-year results Thun 30.11.2018 Paulina Salminen MD, PhD, Professor of Surgery Turku University Hospital, Turku, Finland SLEEVEPASS trial PI Disclosures Lecture fees: Merck,
SLEEVEPASS RCT: SLEEVE vs. bypass 5-year results Thun 30.11.2018 Paulina Salminen MD, PhD, Professor of Surgery Turku University Hospital, Turku, Finland SLEEVEPASS trial PI Disclosures Lecture fees: Merck,
Technique. Matthew Bettendorf, MD Essentia Health Duluth Clinic. Laparoscopic approach One 12mm port, Four 5mm ports
 Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
Matthew Bettendorf, MD Essentia Health Duluth Clinic Technique Laparoscopic approach One 12mm port, Four 5mm ports Single staple line with no anastamosis 85% gastrectomy Goal to remove
SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS
 SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College
SURGICAL TREATMENT FOR OBESITY: WHAT S THE BEST OPTION? Natan Zundel, MD, FACS, FASMBS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College
The case for reductive surgery: a more efficient and cost-effective option
 Emil Loots MBChB (Pret), FCS (SA) Cert Gastro (SA) Surg PhD Candidate The case for reductive surgery: a more efficient and cost-effective option Big day in Pretoria Controversies Controversy around the
Emil Loots MBChB (Pret), FCS (SA) Cert Gastro (SA) Surg PhD Candidate The case for reductive surgery: a more efficient and cost-effective option Big day in Pretoria Controversies Controversy around the
SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS
 SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College of Medicine
SURGICAL TREATMENT FOR OBESITY: WHATS THE BEST OPTION? Natan Zundel, MD, FACS Professor of Surgery Vice-Chairman Department of Surgery Florida International University Herbert Wertheim College of Medicine
Commonly Performed Bariatric Procedures in Singapore. Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital
 Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Revision For Weight Regain
 Revision For Weight Regain When? Why? What? Ahmad Aly ANZMOSS Dietetics Workshop 2018 Reoperative Surgery What Is Reoperative? Reversal Correction Conversion } Revisional Surgery Revisional Surgery 4000
Revision For Weight Regain When? Why? What? Ahmad Aly ANZMOSS Dietetics Workshop 2018 Reoperative Surgery What Is Reoperative? Reversal Correction Conversion } Revisional Surgery Revisional Surgery 4000
Gastric bypass vs. Sleeve gastrectomy
 Gastric bypass vs. Sleeve gastrectomy SLEEVEPASS-study Sleeve gastrectomy Paulina Salminen, M.D., PhD Turku University Hospital Department of Surgery Stockholms Obesitasdagar 19.4.2012 Swedish Obese Subjects
Gastric bypass vs. Sleeve gastrectomy SLEEVEPASS-study Sleeve gastrectomy Paulina Salminen, M.D., PhD Turku University Hospital Department of Surgery Stockholms Obesitasdagar 19.4.2012 Swedish Obese Subjects
What we learned in 64 years of metabolic surgery. Bariatric surgery: predicting the future
 1 st Jordanian Society for Obesity Surgery (JSOS) & 2 nd Pan-Arab Society for Metabolic & Bariatric Surgery (PASMBS) Congress Program (July 25th - 27th) Day 1 - Wednesday July 25th: Hall 1 8:00-9:00 Welcome
1 st Jordanian Society for Obesity Surgery (JSOS) & 2 nd Pan-Arab Society for Metabolic & Bariatric Surgery (PASMBS) Congress Program (July 25th - 27th) Day 1 - Wednesday July 25th: Hall 1 8:00-9:00 Welcome
Benefits of Bariatric Surgery
 Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery
 Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS ACS NSQIP Surgeon Champion Chief of General, Thoracic & Vascular Surgery
Best Practices for Fast Track in Bariatric Surgery: Enhanced Recovery After Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS ACS NSQIP Surgeon Champion Chief of General, Thoracic & Vascular Surgery
7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004.
 7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004. DIMINISHING POSTOPERATIVE RISKS OF GASTRIC BYPASS Stenosis Stenosis Leak Leak Bleeding Bleeding Stenosis
7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004. DIMINISHING POSTOPERATIVE RISKS OF GASTRIC BYPASS Stenosis Stenosis Leak Leak Bleeding Bleeding Stenosis
Mandatory risk assessment reduces Venous Thromboembolism in Bariatric Surgery
 Mandatory risk assessment reduces Venous Thromboembolism in Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS President, Pan Arab Society for Metabolic & Bariatric Surgery Surgeon Champion, ACS
Mandatory risk assessment reduces Venous Thromboembolism in Bariatric Surgery Abdelrahman Nimeri, MBBCh, FACS, FASMBS President, Pan Arab Society for Metabolic & Bariatric Surgery Surgeon Champion, ACS
Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor
 Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
Current Trends in Bariatric Surgery
 Current Trends in Bariatric Surgery 9.28.2017 Abraham Krikhely, MD, FACS, FASMBS Assistant Professor of Surgery, CUMC Center of Minimal Access, Metabolic and Weight Loss Surgery Outline Why consider surgery
Current Trends in Bariatric Surgery 9.28.2017 Abraham Krikhely, MD, FACS, FASMBS Assistant Professor of Surgery, CUMC Center of Minimal Access, Metabolic and Weight Loss Surgery Outline Why consider surgery
Long-Term Care Updates
 Long-Term Care Updates August 2017 By Alyson Lozicki, PharmD As the prevalence of obesity continues to rise, and with now over one-third (36.5%) of American adults considered obese, the number of weight
Long-Term Care Updates August 2017 By Alyson Lozicki, PharmD As the prevalence of obesity continues to rise, and with now over one-third (36.5%) of American adults considered obese, the number of weight
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes
 Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
Effect of Bariatric Surgery on Cardio-Metabolic Outcomes Disclosure Research support from Bariatric Advantage (supplements donated for research study) Anne Schafer, MD Associate Professor of Medicine and
Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018
 Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018 Disclosures None Objectives Review expected weight loss from
Bariatric surgery: Impact on Co-morbidities and Weight Loss Expectations ALIYAH KANJI, MD FRCSC MIS AND BARIATRIC SURGERY SEPTEMBER 22, 2018 Disclosures None Objectives Review expected weight loss from
Lecture Goals. Body Mass Index. Obesity Definitions. Bariatric Surgery What the PCP Needs to Know 11/17/2009. Indications for bariatric Surgeries
 Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Long-Term Follow Up: The Burning Platform
 Long-Term Follow Up: The Burning Platform John Morton, MD, MPH, FACS, FASMBS Chief, Bariatric & Minimally Invasive Surgery Stanford School of Medicine Past-President, American Society of Metabolic and
Long-Term Follow Up: The Burning Platform John Morton, MD, MPH, FACS, FASMBS Chief, Bariatric & Minimally Invasive Surgery Stanford School of Medicine Past-President, American Society of Metabolic and
Choice Critria in Bariatric Surgery. Giovanni Camerini
 Choice Critria in Bariatric Surgery Giovanni Camerini Surgical vs Medical treatment Indications for Bariatric Surgery (WHO 1992) BMI of at least 40; BMI of 35 in case of serious diseases related to obesity;
Choice Critria in Bariatric Surgery Giovanni Camerini Surgical vs Medical treatment Indications for Bariatric Surgery (WHO 1992) BMI of at least 40; BMI of 35 in case of serious diseases related to obesity;
Obesity and Bariatric Surgery Michel M. Murr, MD, FACS
 Obesity and Bariatric Surgery Michel M. Murr, MD, FACS Director of Bariatric Center Chief of Surgery, TGH Professor of Surgery, USF Disclosure Covidien: educational grants Obesity and Bariatric Surgery
Obesity and Bariatric Surgery Michel M. Murr, MD, FACS Director of Bariatric Center Chief of Surgery, TGH Professor of Surgery, USF Disclosure Covidien: educational grants Obesity and Bariatric Surgery
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Policy Specific Section: April 14, 1970 June 28, 2013
 Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
SURGICAL MANAGEMENT OF OBESITY. Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery
 SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
SURGICAL MANAGEMENT OF OBESITY Anne Lidor, MD, MPH Professor of Surgery Chief, Division of Minimally Invasive and Bariatric Surgery Multi-Factorial Causes of Morbid Obesity include: Genetic Environmental
Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS
 Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS Disclosures No financial disclosures Medical Director Bariatric program at Lourdes Types
Nutritional deficiencies & vitamins after surgery. What needs to be monitored? Ratna Pallapothu, MD, FACS, FASMBS Disclosures No financial disclosures Medical Director Bariatric program at Lourdes Types
The First Annual GOSS Meeting
 invites you to Featuring The Fifth SKMC-Cleveland Clinic Obesity Symposium & The second Kuwait Society of Metabolic Surgery Meeting Symposia, Debates and Live Surgery Kuwait City, Kuwait December 12-14th
invites you to Featuring The Fifth SKMC-Cleveland Clinic Obesity Symposium & The second Kuwait Society of Metabolic Surgery Meeting Symposia, Debates and Live Surgery Kuwait City, Kuwait December 12-14th
JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial
 JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial Daniel DeUgarte, MD Division of Pediatric Surgery Surgical Director, UCLA FIT Program Bariatric
JAMA February 10, 2010 Laparoscopic Adjustable Banding in Severely Obese Adolescents: A Randomized Trial Daniel DeUgarte, MD Division of Pediatric Surgery Surgical Director, UCLA FIT Program Bariatric
Surgical Treatment of Obesity. 1. Understand who is an appropriate candidate for referral for surgical weight loss.
 Surgical Treatment of Obesity Learning Objectives: 1. Understand who is an appropriate candidate for referral for surgical weight loss. 2. Appreciate impact of operative weight reduction to improve co-morbid
Surgical Treatment of Obesity Learning Objectives: 1. Understand who is an appropriate candidate for referral for surgical weight loss. 2. Appreciate impact of operative weight reduction to improve co-morbid
The Surgical Management of Obesity
 The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
Bariatric Surgery Update
 Bariatric Surgery Update Alexander Perez, MD, FACS Professor of Surgery Chief, Division Minimally Invasive and Foregut Surgery Speaker Disclosure Dr. Perez has disclosed that the has no actual or potential
Bariatric Surgery Update Alexander Perez, MD, FACS Professor of Surgery Chief, Division Minimally Invasive and Foregut Surgery Speaker Disclosure Dr. Perez has disclosed that the has no actual or potential
DISCLOSURES. Laparoscopic Adjustable Gastric Banding (LAGB) As An Option For Failed Gastric Bypass Procedure In Obese Patients
 As An Option For Failed Gastric Bypass Procedure In Obese Patients") Laparoscopic Adjustable Gastric Banding (LAGB) As An Option For Failed Gastric Bypass Procedure In Obese Patients Presented By: Ali Hazrati, Md, Msc, FRCSC Co-authors: Patrick Yau, MD, Jamie Cyriac, MD
Laparoscopic Adjustable Gastric Banding (LAGB) As An Option For Failed Gastric Bypass Procedure In Obese Patients Presented By: Ali Hazrati, Md, Msc, FRCSC Co-authors: Patrick Yau, MD, Jamie Cyriac, MD
Viriato Fiallo, MD Ursula McMillian, MD
 Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Gastric Emptying Time after Laparoscopic Sleeve Gastrectomy
 International Journal of Current Research in Medical Sciences ISSN: 2454-5716 P-ISJN: A4372-3064, E -ISJN: A4372-3061 www.ijcrims.com Original Research Article Volume 4, Issue 7-2018 Gastric Emptying Time
International Journal of Current Research in Medical Sciences ISSN: 2454-5716 P-ISJN: A4372-3064, E -ISJN: A4372-3061 www.ijcrims.com Original Research Article Volume 4, Issue 7-2018 Gastric Emptying Time
Supplementary Online Content
 Supplementary Online Content Peterli R, Wölnerhanssen BK, Peters T, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity:
Supplementary Online Content Peterli R, Wölnerhanssen BK, Peters T, et al. Effect of laparoscopic sleeve gastrectomy vs laparoscopic Roux-en-Y gastric bypass on weight loss in patients with morbid obesity:
Goals 1/9/2018. Obesity over the last decade Surgery has become a safer management strategy Surgical options for management
 The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
The Current State of Surgical Intervention in Management of Morbid Obesity Goals Obesity over the last decade Surgery has become a safer management strategy Surgical options for management 1 Goals Obesity
Morbid Obesity A Curable Disease?
 Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
Morbid Obesity A Curable Disease? Piotr Gorecki, M.D. F.A.C.S. Associate Professor of Clinical Surgery Weill Medical College of Cornell University Chief of Laparoscopic Surgery New York Methodist Hospital
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Is laparoscopic sleeve gastrectomy safer than laparoscopic gastric bypass?
 Is laparoscopic sleeve gastrectomy safer than laparoscopic gastric bypass? A comparison of 30-day complications using the MBSAQIP data registry Sandhya B. Kumar MD, Barbara C. Hamilton MD, Soren Jonzzon,
Is laparoscopic sleeve gastrectomy safer than laparoscopic gastric bypass? A comparison of 30-day complications using the MBSAQIP data registry Sandhya B. Kumar MD, Barbara C. Hamilton MD, Soren Jonzzon,
Removal of a lap band and revision to an alternative bariatric procedure in one procedure.
 How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
The Bariatric and Heartburn Center of Northeast Ohio
 The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
Bariatric Surgery Update
 Friday General Session Bariatric Surgery Update Alex Perez, MD Chief, Division of Minimally Invasive and Foregut Surgery James E. Thompson, MD Family Distinguished Professor in Surgical Simulation Co Director,
Friday General Session Bariatric Surgery Update Alex Perez, MD Chief, Division of Minimally Invasive and Foregut Surgery James E. Thompson, MD Family Distinguished Professor in Surgical Simulation Co Director,
Medical Policy Bariatric Surgery. Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X
 Medical Policy Bariatric Surgery Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization Overview The purpose of this document is to describe
Medical Policy Bariatric Surgery Document Number: 042 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization Overview The purpose of this document is to describe
Medicare Part C Medical Coverage Policy
 Morbid Obesity Surgery Origination: June 30, 1988 Review Date: October 18, 2017 Next Review: October, 2019 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE OR SERVICE Bariatric surgery
Morbid Obesity Surgery Origination: June 30, 1988 Review Date: October 18, 2017 Next Review: October, 2019 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE OR SERVICE Bariatric surgery
Safety of Laparoscopic Vs Open Bariatric Surgery. Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat
 Safety of Laparoscopic Vs Open Bariatric Surgery 1 Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat Surgical Treatment of Obesity 2 Bariatrics is the branch of
Safety of Laparoscopic Vs Open Bariatric Surgery 1 Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat Surgical Treatment of Obesity 2 Bariatrics is the branch of
(1) Upper Gastrointestinal Surgical Unit, The Alfred Hospital (2) Monash University Centre for Obesity Research and Education (CORE)
 Upper Gastrointestinal Surgical Unit, The Alfred Hospital (2) Monash University Centre for Obesity Research and Education (CORE)") Yazmin Johari (1,2), Geri Ooi (1,2), Paul Burton (1,2), Shourye Dwivedi (2), Cheryl Laurie (2), Kalai Shaw (1), Richard Chen (1,2), Wendy Brown (1,2), Peter Nottle (1) (1) Upper Gastrointestinal Surgical
Yazmin Johari (1,2), Geri Ooi (1,2), Paul Burton (1,2), Shourye Dwivedi (2), Cheryl Laurie (2), Kalai Shaw (1), Richard Chen (1,2), Wendy Brown (1,2), Peter Nottle (1) (1) Upper Gastrointestinal Surgical
Overview. Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco
 GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
Bariatric Surgery. The Oregon Bariatric Center Surgical Team
 Bariatric Surgery The Oregon Bariatric Center Surgical Team Colin MacColl, MD, Medical Director, Bariatric Surgeon Jessica Folek, MD, Bariatric Surgeon I have no disclosures Disclosures Objectives What
Bariatric Surgery The Oregon Bariatric Center Surgical Team Colin MacColl, MD, Medical Director, Bariatric Surgeon Jessica Folek, MD, Bariatric Surgeon I have no disclosures Disclosures Objectives What
Is mini bypass as mini as we think it is? Nutritional consequences
 Is mini bypass as mini as we think it is? Nutritional consequences Mini/ single loop bypass What is a mini bypass? Single loop One anastomosis Mini Prevalence Increasing Who is the single loop bypass for?
Is mini bypass as mini as we think it is? Nutritional consequences Mini/ single loop bypass What is a mini bypass? Single loop One anastomosis Mini Prevalence Increasing Who is the single loop bypass for?
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page
 Vol. 72 (9), Page") The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page 5189-5194 Revisional Laparoscopic Mini-Gastric Bypass for Weight Loss Failure after Restrictive Procedures Hossam El-Din Hassan Hussein,
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page 5189-5194 Revisional Laparoscopic Mini-Gastric Bypass for Weight Loss Failure after Restrictive Procedures Hossam El-Din Hassan Hussein,
Update on Bariatric Surgery. Learning Objectives: At the end of this lecture you should be able to: Currently Available Options
 Update on Bariatric Surgery Dan Bessesen, MD Chief of Endocrinology; Denver Health Medical Center Professor of Medicine, University of Colorado School of Medicine Daniel.Bessesen@ucdenver.edu Learning
Update on Bariatric Surgery Dan Bessesen, MD Chief of Endocrinology; Denver Health Medical Center Professor of Medicine, University of Colorado School of Medicine Daniel.Bessesen@ucdenver.edu Learning
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery For Patients With End-Organ Failure
 Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
BARIATRIC SURGERY. Weight Loss Surgery. A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female
 BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
Bariatric Surgery MM /11/2001. HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient; Inpatient
 of Service: Outpatient; Inpatient") Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Bariatric Surgery Outcomes
 Bariatric Surgery Outcomes Kristoffel R. Dumon, MD a, Kenric M. Murayama, MD b, * KEYWORDS Bariatric surgery Outcomes Obesity Obesity is a global health problem and the exponential increase in obesity
Bariatric Surgery Outcomes Kristoffel R. Dumon, MD a, Kenric M. Murayama, MD b, * KEYWORDS Bariatric surgery Outcomes Obesity Obesity is a global health problem and the exponential increase in obesity
ADVANCE AT YOUR OWN PACE
 ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN
 OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN Nicole Basa, M.D., F.A.C.S., F.A.S.M.B.S Assistant Professor of Surgery Texas A&M Medical School Bariatric Medical Director- Cedar Park Regional
OBESITY AND WEIGHT LOSS SURGERY FOR THE PRIMARY CARE PHYSICIAN Nicole Basa, M.D., F.A.C.S., F.A.S.M.B.S Assistant Professor of Surgery Texas A&M Medical School Bariatric Medical Director- Cedar Park Regional
Obesity and Weight Loss Surgery for the Primary Care Physician
 Saturday General Session Obesity and Weight Loss Surgery for the Primary Care Physician Nicole Basa, MD Bariatric and General Surgeon Cedar Park Surgeons, PA Cedar Park, Texas Educational Objectives By
Saturday General Session Obesity and Weight Loss Surgery for the Primary Care Physician Nicole Basa, MD Bariatric and General Surgeon Cedar Park Surgeons, PA Cedar Park, Texas Educational Objectives By
Objectives. By the end of this educational encounter the learner will be able to:
 Complications of Bariatric Surgery WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG,
Complications of Bariatric Surgery WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG,
Corporate Medical Policy. Bariatric (Surgery for Morbid Obesity)
") Corporate Medical Policy Bariatric (Surgery for Morbid Obesity) File name: Bariatric (Obesity Surgery) Origination: 07/2008 Last Review: 07/2009 Next Review: 07/2010 Effective Date: 12/08/2008 Description
Corporate Medical Policy Bariatric (Surgery for Morbid Obesity) File name: Bariatric (Obesity Surgery) Origination: 07/2008 Last Review: 07/2009 Next Review: 07/2010 Effective Date: 12/08/2008 Description
NOTE: This policy is not effective until May 1, To view the current policy, click here. IMPORTANT REMINDER
 NOTE: This policy is not effective until May 1, 2018. To view the current policy, click here. Medical Policy Manual Surgery, Policy No. 58 Bariatric Surgery Next Review: December 2018 Last Review: January
NOTE: This policy is not effective until May 1, 2018. To view the current policy, click here. Medical Policy Manual Surgery, Policy No. 58 Bariatric Surgery Next Review: December 2018 Last Review: January
Disclosures. Weight Regain After Bariatric Surgery & Future Therapies. Objectives
 Weight Regain After Bariatric Surgery & Future Therapies Matthew Kroh, MD Assistant Professor of Surgery Cleveland Clinic Center for Surgical Innovation, Technology, and Education Digestive Disease Institute
Weight Regain After Bariatric Surgery & Future Therapies Matthew Kroh, MD Assistant Professor of Surgery Cleveland Clinic Center for Surgical Innovation, Technology, and Education Digestive Disease Institute
Sleeve Gastrectomy: Harmful. John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10
 Sleeve Gastrectomy: Harmful John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10 Background Obesity: Body Mass Index >30 Risk factor for CAD, DM, Cancers Obesity Trends*
Sleeve Gastrectomy: Harmful John C. Eun, PGY-5 General Surgery Grand Rounds University of Colorado Denver 11/22/10 Background Obesity: Body Mass Index >30 Risk factor for CAD, DM, Cancers Obesity Trends*
How can the surgeon help? M. Lannoo B. Navez
 How can the surgeon help? M. Lannoo B. Navez 1 Reimbursed indications > 18 year BMI > 40 BMI >35 in combination with: OSAS Hypertension with 3 anti-hypertensive drugs Diabetes type II Multidisciplinary
How can the surgeon help? M. Lannoo B. Navez 1 Reimbursed indications > 18 year BMI > 40 BMI >35 in combination with: OSAS Hypertension with 3 anti-hypertensive drugs Diabetes type II Multidisciplinary
Bariatric Surgery: The Primary Care Approach
 The 8 th Annual Conference of the Lebanese Society of Family Medicine October 25 th 2009 Bariatric Surgery: The Primary Care Approach Bassem Y. Safadi, MD, FACS Associate Professor of Clinical Surgery
The 8 th Annual Conference of the Lebanese Society of Family Medicine October 25 th 2009 Bariatric Surgery: The Primary Care Approach Bassem Y. Safadi, MD, FACS Associate Professor of Clinical Surgery
Roux-and-Y Gastric Bypass and its Metabolic Effects
 Roux-and-Y Gastric Bypass and its Metabolic Effects Nicola Di Lorenzo President elect of SICOb Italian Society for Bariatric Surgery and Metabolic Diseases Dept. of General Surgery-Università di Roma Tor
Roux-and-Y Gastric Bypass and its Metabolic Effects Nicola Di Lorenzo President elect of SICOb Italian Society for Bariatric Surgery and Metabolic Diseases Dept. of General Surgery-Università di Roma Tor
DEKAs after Bariatric Surgery*
 DEKAs after Bariatric Surgery* Once Daily All-in-one Multivitamin and Mineral Chewable Tablets with Enhanced Absorption for Dietary Management after Bariatric Surgery Roberto Jongejan, MD, PhD Gus Papas,
DEKAs after Bariatric Surgery* Once Daily All-in-one Multivitamin and Mineral Chewable Tablets with Enhanced Absorption for Dietary Management after Bariatric Surgery Roberto Jongejan, MD, PhD Gus Papas,
MBSAQIP Complex Clinical Scenarios & Variable Review
 MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
10/28/11. Bariatric Surgery: What the Primary Care Provider Should Know. Case Presentation: Rachelle
 Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes. Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018
 WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
WEIGHT LOSS SURGERY A Primer on Current Options and Outcomes Caitlin A. Halbert DO, MS, FACS, FASMBS April 5, 2018 A Little Bit About Me Bariatric Surgical Services Reflux Surgery General Surgery Overview
6/23/2011. Bariatric Surgery: What the Primary Care Provider Should Know. Case Presentation: Rachelle
 Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery: What the Primary Care Provider Should Know 2,000 B.C. 2,000 A.D. Case Presentation: Rachelle 35 year-old woman with morbid obesity. 5 1 236 lbs BMI 44.5 PMHx: mild depression obstructive
Bariatric Surgery Corporate Medical Policy
 Bariatric Surgery Corporate Medical Policy File name: Bariatric Surgery File code: UM.SURG.01 Origination: 07/2008 Last Review: 06/2018 Next Review: 06/2019 Effective Date: 10/01/2018 Description/Summary
Bariatric Surgery Corporate Medical Policy File name: Bariatric Surgery File code: UM.SURG.01 Origination: 07/2008 Last Review: 06/2018 Next Review: 06/2019 Effective Date: 10/01/2018 Description/Summary
FRESH START. Time For A BARIATRIC SURGERY! WHAT IS BARIATRIC SURGERY? UHS Medical Times EVERYTHING YOU NEED TO KNOW ABOUT علاج ال دانة وجراحة السمنة
 UHS Medical Times 1 Newsletter September 2018 علاج ال دانة وجراحة السمنة MINIMALLY INVASIVE Time For A FRESH START EVERYTHING YOU NEED TO KNOW ABOUT BARIATRIC SURGERY! While any surgical procedure carries
UHS Medical Times 1 Newsletter September 2018 علاج ال دانة وجراحة السمنة MINIMALLY INVASIVE Time For A FRESH START EVERYTHING YOU NEED TO KNOW ABOUT BARIATRIC SURGERY! While any surgical procedure carries
Endorsed by Executive Council June 17, American Society for Metabolic and Bariatric Surgery
 Endorsed by Executive Council June 17, 2007 American Society for Metabolic and Bariatric Surgery POSITION STATEMENT ON SLEEVE GASTRECTOMY AS A BARIATRIC PROCEDURE Clinical Issues Committee Preamble. The
Endorsed by Executive Council June 17, 2007 American Society for Metabolic and Bariatric Surgery POSITION STATEMENT ON SLEEVE GASTRECTOMY AS A BARIATRIC PROCEDURE Clinical Issues Committee Preamble. The
Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease
 Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease Erik Peltz, D.O. April 7 th, 2008 University of Colorado Health Science Center Department
Laparoscopic Adjustable Gastric Band The Safest, Effective Procedure for Treating Obesity and Obesity Related Disease Erik Peltz, D.O. April 7 th, 2008 University of Colorado Health Science Center Department
Disclosures OBESITY. Overview. Obesity: Definition. Prevalence of Obesity is Rising. Obesity as a Risk Factor. None
 Disclosures None OBESITY Florencia Halperin, M.D. Medical Director, Program for Management Brigham and Women s Hospital Instructor in Medicine, Harvard Medical School Overview Obesity: Definition Definition
Disclosures None OBESITY Florencia Halperin, M.D. Medical Director, Program for Management Brigham and Women s Hospital Instructor in Medicine, Harvard Medical School Overview Obesity: Definition Definition
Bariatric Surgery: A Cost-effective Treatment of Obesity?
 Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
Bariatric Surgery: A Cost-effective Treatment of Obesity? Shaneeta M. Johnson MD FACS FASMBS 2018 NMA Professional Development Seminar Congressional Black Caucus Foundation Annual Legislative Conference
Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy
 Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
Townhall: Assisting Patients Post Bariatric Surgery Katie McClendon, PharmD, BCPS, FCCP University of Mississippi School of Pharmacy Annual Meeting & Exposition Seattle, Washington March 22 25 Disclosures
You can lose weight.
 BARIATRIC CENTER You can lose weight. And our bariatric team will support your every step. Lauren 135 lb. weight loss Gastric Sleeve This was the best decision I ve made. My only regret was not doing it
BARIATRIC CENTER You can lose weight. And our bariatric team will support your every step. Lauren 135 lb. weight loss Gastric Sleeve This was the best decision I ve made. My only regret was not doing it
American Society for Metabolic & Bariatric Surgery
 American Society for Metabolic & Bariatric Surgery April 27, 2012 Louis Jacques, MD Director, Coverage and Analysis Group Centers for Medicare and Medicaid Services Mail Stop S3-02-01 7500 Security Boulevard
American Society for Metabolic & Bariatric Surgery April 27, 2012 Louis Jacques, MD Director, Coverage and Analysis Group Centers for Medicare and Medicaid Services Mail Stop S3-02-01 7500 Security Boulevard
Considering Bariatric Surgery?
 Considering Bariatric Surgery? minimally invasive LearnLearn aboutabout minimally invasive da Vinci da Vinci Surgery Surgery The Condit io n: Obesity Obesity is defined as having a body mass index (BMI)
Considering Bariatric Surgery? minimally invasive LearnLearn aboutabout minimally invasive da Vinci da Vinci Surgery Surgery The Condit io n: Obesity Obesity is defined as having a body mass index (BMI)
Sleeve Gastrectomy Debate: Everyone Needs a Sleeve!!! Dana Portenier, MD Assistant Professor of Surgery Duke University Medical Center
 Sleeve Gastrectomy Debate: Everyone Needs a Sleeve!!! Dana Portenier, MD Assistant Professor of Surgery Duke University Medical Center 1. Safety Two Year Excess Weight Loss Two Year Weight Loss and Mortality
Sleeve Gastrectomy Debate: Everyone Needs a Sleeve!!! Dana Portenier, MD Assistant Professor of Surgery Duke University Medical Center 1. Safety Two Year Excess Weight Loss Two Year Weight Loss and Mortality
Comparison Between Laparoscopic Sleeve Gastrectomy and Laparoscopic Adjustable Gastric Banding for Morbid Obesity: a Meta-analysis
 OBES SURG (2013) 23:980 986 DOI 10.1007/s11695-013-0893-3 REVIEW Comparison Between Laparoscopic Sleeve Gastrectomy and Laparoscopic Adjustable Gastric Banding for Morbid Obesity: a Meta-analysis Sen Wang
OBES SURG (2013) 23:980 986 DOI 10.1007/s11695-013-0893-3 REVIEW Comparison Between Laparoscopic Sleeve Gastrectomy and Laparoscopic Adjustable Gastric Banding for Morbid Obesity: a Meta-analysis Sen Wang
Bariatric Surgery. Options & Outcomes
 Bariatric Surgery Options & Outcomes Obesity Obesity now leading cause of premature death & illness in Australia 67% of Australians are overweight or obese Australia 4 th fattest nation in OECD Obesity
Bariatric Surgery Options & Outcomes Obesity Obesity now leading cause of premature death & illness in Australia 67% of Australians are overweight or obese Australia 4 th fattest nation in OECD Obesity
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery
 Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Surgery: Bariatric Surgery There are many non-surgical treatments for obesity such as dieting, exercise, and medicine.
Considering Bariatric Surgery? Learn about minimally invasive da Vinci Surgery The Surgery: Bariatric Surgery There are many non-surgical treatments for obesity such as dieting, exercise, and medicine.
Surgical Options for Weight Regain (or Poor Weight Loss) After Adjustable Gastric Banding
 After Adjustable Gastric Banding") Surgical Options for Weight Regain (or Poor Weight Loss) After Adjustable Gastric Banding Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center Jin.Yoo@duke.edu Financial Disclosures
Surgical Options for Weight Regain (or Poor Weight Loss) After Adjustable Gastric Banding Jin S. Yoo M.D. Assistant Professor of Surgery Duke University Medical Center Jin.Yoo@duke.edu Financial Disclosures
Bariatric Surgery and Bone Health
 Bariatric Surgery and Bone Health No conflicts of interest Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism July 26, 202 BMI and Fracture Risk Low BMI is associated
Bariatric Surgery and Bone Health No conflicts of interest Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism July 26, 202 BMI and Fracture Risk Low BMI is associated
Weight Loss Surgery. Outline 3/30/12. What Every GI Nurse Needs to Know. Define Morbid Obesity & its Medical Consequences. Treatments for Obesity
 3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
3/30/12 Weight Loss Surgery What Every GI Nurse Needs to Know Kenneth A Cooper, D.O. March 31, 2012 Outline Define Morbid Obesity & its Medical Consequences Treatments for Obesity Bariatric (Weight-loss)
See Policy CPT CODE section below for any prior authorization requirements
 Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
Marc Bessler, M.D.*, Amna Daud, M.D., M.P.H., Teresa Kim, M.D., Mary DiGiorgi, M.P.H.
 Surgery for Obesity and Related Diseases 3 (2007) 480 485 Original article Prospective randomized trial of banded versus nonbanded gastric bypass for the super obese: early results Marc Bessler, M.D.*,
Surgery for Obesity and Related Diseases 3 (2007) 480 485 Original article Prospective randomized trial of banded versus nonbanded gastric bypass for the super obese: early results Marc Bessler, M.D.*,