BEST 4 Diabetes. Optimisation of insulin module
|
|
|
- Damon Mosley
- 5 years ago
- Views:
Transcription
1 BEST 4 Diabetes Optimisation of insulin module

2 Confidence and competence Where would you rate yourself?

3 Why do all of our patient not achieve optimal blood glucose control?
4 Insulin Therapy Goals and Purpose of Insulin Therapy Barriers to the use of Insulin Current Concepts in Insulin Therapy Basal/Bolus Insulin (Insulin Pump Therapy)

5
6
7 Why do patients delay insulin treatment? Concern about injections Worry over hypoglycaemia Fears for weight gain Stigma of insulin injections Concern about employment False previous family experience Strong negative cultural beliefs

8 Why do patients delay insulin?
9 Reasons for poor diabetic control Delay in commencing insulin treatment Insufficient dose titration Failure to control fasting blood sugar Inappropriate insulin mix False concerns about maximum insulin dose
10 Helping Patient Accept Insulin Therapy Address patient concerns Dispel fear by countering misconceptions Review rationale for insulin use Hypoglycaemia is infrequent, and can be easily treated, and that severe hypoglycaemia is rare Treatment need not be burdensome Weight gain can now be managed with adjuvant treatment Is a common course of treatment for this progressive disease Promise patient support and close follow-up Monitoring can prevent hypoglycemia Today s technology can facilitate daily injections and readings
11 Recap Insulin Time action profiles Group Work
12 Recap Insulin devices Insulin terminology

13 CSII Continuous Subcutaneous Insulin Infusion Insulin Pump A continuous infusion of rapid acting insulin, no requirement for long acting insulin. For Type 1 s under secondary care. Make sure patient has insulin pens and insulin in case of pump failure.
14 Choice of insulin treatments Once daily NPH/Analogue Basal with oral agents/glp1 T2DM and some T1 patients dependant on others for care Twice daily Either Combination bd/tds Biphasic insulin (Human or Analogue) T1 or T2 or bd (NPH/Analogue T2DM) Basal Bolus T1 or T2DM (Human-NPH/Analogue Bolus-Basal) Insulin pump treatment T1DM only
15 Injection technique: key messages injection sites insulin storage injecting process correct use of injection device use of pen needles or syringes once site rotation injecting into subcutaneous fatty tissue absorption rates needle length appropriate use of skin folds disposal of injecting material FIT (Oct 2011), The First UK Injection Technique Recommendations, 2 nd Edition
16 FIT (Forum for Injection Technique) Education topic areas At the beginning of injection therapy (and at least every year thereafter) the HCP should discuss: injection regimen choice and management of the devices used choice, care and self examination of injection sites correct injection technique (including site rotation, injection angle and possible use of skin folds) injection complications and how to avoid them optimal needle length safe disposal of used sharps FIT (Oct 2011), The First UK Injection Technique Recommendations, 2 nd Edition

17 Needle length/skin fold? mm thick Depth varies depending on site Image reproduced with permission from Becton Dickenson
18 Needle length/skin fold? Needle length Skin fold Comments 4,5,6mm No Unless injecting into slim limbs/abdomen 8mm Yes Shortest length available for an insulin syringe 12.7mm Yes No clinical reason to use this length
19 Absorption rates and injection sites Insulin type Most favoured injection sites Why? NPH insulin Thigh, buttocks Slowest absorption sites Short-acting insulin Abdomen Fastest absorption site Premixed insulin (human or analogue) Insulin analogues: rapid and longacting GLP-1 agonists Abdomen morning Thigh or buttock eve meal May be given at any injection site Follow manufacturer s instructions Increase speed of short /rapidacting insulin to cover post prandial breakfast Leads to slower absorption and decreases risk of nocturnal hypoglycaemia Absorption rates do not appear to be site specific More studies are needed FIT (Oct 2011), The First UK Injection Technique Recommendations, 2 nd Edition

20 Risks associated with lipohypertrophy Unpredictable and delayed insulin absorption Can result in larger insulin dosages being used May cause fluctuating glycaemic control with unpredictable hyperglycemia and hypoglycaemia Image reproduced with permission from Becton Dickenson

21 Management of lipohypertrophy Prevention Site rotation Fresh needle management Move away from the site for months/years Consider a reduction in insulin dosage Use blood glucose monitoring to assess need for further insulin dose alterations Encourage self inspection of sites and check at reviews Image reproduced with permission from Becton Dickenson


22 Images reproduced with permission from Becton Dickenson
23
24 Recap Hypoglycaemia BHFT Leaflet Hyperglycaemia and sick day rules Trend Leaflet






25 Berkshire West Insulin Optimisation Framework for Type 2 Diabetes Recommend initiation on human basal insulin Patient able to self titrate & have carb awareness Consider alternatives if ; District Nurse to Administer 60u BD Basal Bolus Steroid Patients Nursing Home Patients Erratic Eating Patterns In these cases contact DSN team for advice 60u BD 60u BD BD Human or 60u BD BD Mix 50/50 TDS Mix 50/50 30 units BD Analogue Mix Once Daily Human Basal Human Basal DSN Referral Recommended Low Skills and Capabilities High
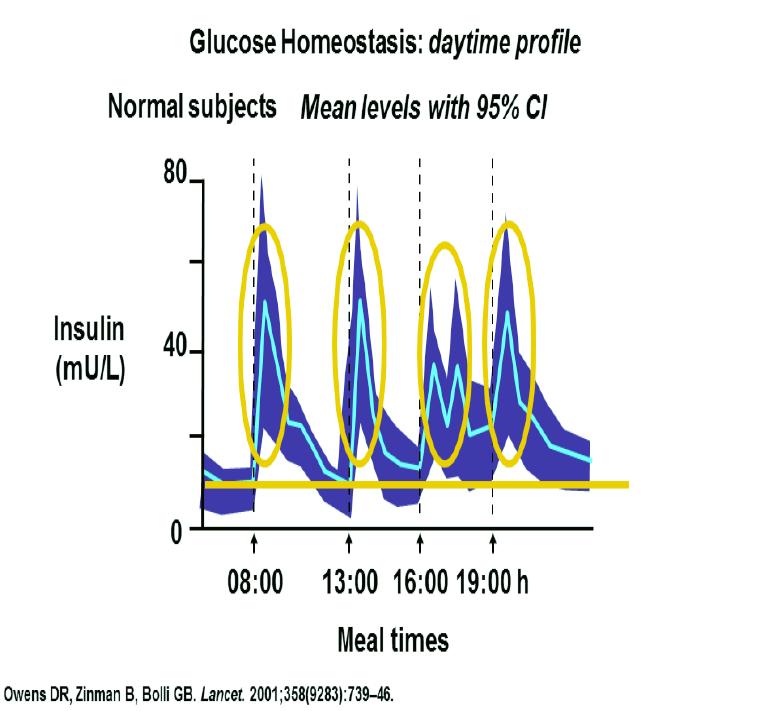
26 The Ideal Basal Insulin... Mimics normal pancreatic basal insulin secretion Long-lasting effect around 24 hours Smooth, peakless profile Reproducible and predictable effects Reduced risk of nocturnal hypoglycemia Once-daily administration for convenience 6-32
27 What are the problems with basal insulin treatment? Insufficient length of action requiring twice daily dosage Large intra-dose variability leading to increased hypoglycaemia or loss of daytime control Excess basal insulin treatment, leading to weight gain High dose volumes in insulin resistant and obese patients
28 Where is the appropriate place of newer basal insulin therapy? Patients who are demonstrated have problems with basal insulin treatment Patients who are having to split basal insulin therapies Patients with nocturnal hypoglycaemia?? Patients with excess weight gain Patients requiring third party administration of insulin treatment
29 Starting with Basal Insulin Continue oral agent(s) at same dosage (eventually stop secretagogue) Add single, evening insulin dose (around 10 U) Glargine (bedtime or anytime?) NPH (bedtime) Mixed Insulin 70/30 (evening meal) or 75/25 Adjust dose by fasting BG Increase insulin dose weekly as needed Increase 4 U if FBG >10 mmol Increase 2 U if FBG = 7-10 Treat to target (usually <7mg/dL) 6-59
30 What are the real unmet needs in insulin therapy Early recognition of failure of oral therapy Strong positive recommendation of benefits of insulin treatment to patients Reassurance concerning potential negative consequences in therapy Intense support to optimise insulin dosage Regular review to identify problems with insulin therapy Time
31 What you need to do in practice tomorrow Do a search for all your patients with HbA1C is >85 mmol per mole Refer those patients to Expert and For those on tablets, move them either to basal insulin and tablets, premixed insulin, or basal insulin and GLP1 combination therapy if they are obese For those refusing insulin treatment, reassure on the safety of insulin treatment, demonstrate injection, and explain that poor diabetic control is not an option For those already on insulin treatment, ask the diabetes specialist nurses to come work with you to titrate insulin doses. For those patients who are gaining weight, consider adjunctive therapy with SGLT/GLP1 For those with body mass index greater than 35 and less than 65 years old suggest refer to bariatric service Analogue insulin is expensive, so only use in clinically justified situations
32 Case Studies Put knowledge into practice.
33 Confidence and competence Where would you rate yourself?
34 Thank you
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Things you need to know about injections
 www.trend-uk.org Things you need to know about injections Injection sites: You can see from the picture below the best sites for injecting insulin or GLP-1 medications are: Back of the upper arms (difficult
www.trend-uk.org Things you need to know about injections Injection sites: You can see from the picture below the best sites for injecting insulin or GLP-1 medications are: Back of the upper arms (difficult
KEEPING SAFE WITH INSULIN THERAPY
 KEEPING SAFE WITH INSULIN THERAPY kk WHY IS THIS LEAFLET FOR YOU? Insulin treatment improves the quality of life in many people and saves the lives of others. It is used to lower blood glucose levels.
KEEPING SAFE WITH INSULIN THERAPY kk WHY IS THIS LEAFLET FOR YOU? Insulin treatment improves the quality of life in many people and saves the lives of others. It is used to lower blood glucose levels.
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Insulin Management. By Susan Henry Diabetes Specialist Nurse
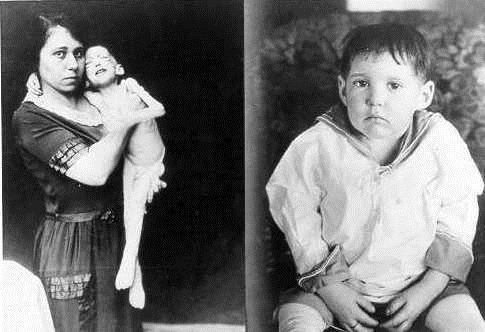
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
What do you need to know before you go home?
 What do you need to know before you go home? What is Insulin Types of Insulin Injection Sites How to Inject Insulin Correctly Low Blood Sugar and Treatment Sick Day Management After leaving the Hospital:
What do you need to know before you go home? What is Insulin Types of Insulin Injection Sites How to Inject Insulin Correctly Low Blood Sugar and Treatment Sick Day Management After leaving the Hospital:
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Correct Site Rotation
 Injection Techniques Questionnaire (ITQ) WorldWide Results 2014-2015 Correct Site Rotation BACKGROUND Correct Rotation = at least 1 cm between successive injections Lipohypertrophy and Observed Correct
Injection Techniques Questionnaire (ITQ) WorldWide Results 2014-2015 Correct Site Rotation BACKGROUND Correct Rotation = at least 1 cm between successive injections Lipohypertrophy and Observed Correct
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per
 4 times per") APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Diabetes Competencies
 Diabetes Competencies Name: Role: Base: Competency Statement: The participant demonstrates clinical knowledge and skill in diabetes nursing without assistance and/or direct supervision (level 3 - see level
Diabetes Competencies Name: Role: Base: Competency Statement: The participant demonstrates clinical knowledge and skill in diabetes nursing without assistance and/or direct supervision (level 3 - see level
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia
 CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
RDNS. Injection Therapy in injection therapy in diabetes. Type 2 Diabetes
 RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
This certificate-level program is non-sponsored.
 Program Name: Diabetes Education : A Comprehensive Review Module 5 Intensive Insulin Therapy Planning Committee: Michael Boivin, B. Pharm. Johanne Fortier, BSc.Sc, BPh.LPh, CDE Carlene Oleksyn, B.S.P.
Program Name: Diabetes Education : A Comprehensive Review Module 5 Intensive Insulin Therapy Planning Committee: Michael Boivin, B. Pharm. Johanne Fortier, BSc.Sc, BPh.LPh, CDE Carlene Oleksyn, B.S.P.
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Insulin Delivery System and Self Monitoring Blood Sugar (SMBG ) Leyden V. Florido, RN, MAN
 Leyden V. Florido, RN, MAN") Insulin Delivery System and Self Monitoring Blood Sugar (SMBG ) Leyden V. Florido, RN, MAN Management of Diabetes Mellitus Pharmacological Glucose Lowering Agents/Oral Antidiabetes Drug/Oral Hypogycemic
Insulin Delivery System and Self Monitoring Blood Sugar (SMBG ) Leyden V. Florido, RN, MAN Management of Diabetes Mellitus Pharmacological Glucose Lowering Agents/Oral Antidiabetes Drug/Oral Hypogycemic
MANAGING MEALTIME INSULIN
 MEDICATION MANAGING MEALTIME INSULIN kk WHY IS THIS LEAFLET FOR YOU? The blood glucose level in someone who does not have diabetes keeps remarkably steady despite variable meal sizes and amount of activity.
MEDICATION MANAGING MEALTIME INSULIN kk WHY IS THIS LEAFLET FOR YOU? The blood glucose level in someone who does not have diabetes keeps remarkably steady despite variable meal sizes and amount of activity.
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Pre-Dialysis Insulin Information for Patients with Type 2 Diabetes receiving haemodialysis
 Pre-Dialysis Insulin Information for Patients with Type 2 Diabetes receiving haemodialysis Exceptional healthcare, personally delivered 2 This leaflet is for patients with Type 2 diabetes who require insulin
Pre-Dialysis Insulin Information for Patients with Type 2 Diabetes receiving haemodialysis Exceptional healthcare, personally delivered 2 This leaflet is for patients with Type 2 diabetes who require insulin
Insulin Basic facts. Patient Education Patient Care Services. What is insulin? What types of insulin are there? Basal Insulin
 Patient Education Insulin Basic facts Insulin is a protein made by the pancreas that allows your cells to use glucose for energy. There are different types of insulin: Basal long-acting insulin that controls
Patient Education Insulin Basic facts Insulin is a protein made by the pancreas that allows your cells to use glucose for energy. There are different types of insulin: Basal long-acting insulin that controls
the person is intolerant of either metformin or a sulphonylurea, or treatment with metformin or a sulphonylurea is contraindicated, and
 Exenatide (Byetta) and Liraglutide (Victoza) prescribing guidance: Notes for initiation in primary care These incretin mimetics are given by subcutaneous injection once or twice daily. They have similar
Exenatide (Byetta) and Liraglutide (Victoza) prescribing guidance: Notes for initiation in primary care These incretin mimetics are given by subcutaneous injection once or twice daily. They have similar
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK. Optimising Glycaemic Control for Children and Young People with Diabetes
 EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK Optimising Glycaemic Control for Children and Young People with Diabetes Local diabetes teams need to take on the responsibility of ensuring
EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK Optimising Glycaemic Control for Children and Young People with Diabetes Local diabetes teams need to take on the responsibility of ensuring
The Wheel of Life Exercise. What s Happening? Where to start the beginning. What's in a meter- are they all the same?
 Wharfedale Hospital Otley Linda Clapham BSc Hons. RGN, SEN,Cert. Ed. The Wheel of Life Exercise An exercise to Encourage self management Work What s going on! Medication Helping patients succeed Diabetes
Wharfedale Hospital Otley Linda Clapham BSc Hons. RGN, SEN,Cert. Ed. The Wheel of Life Exercise An exercise to Encourage self management Work What s going on! Medication Helping patients succeed Diabetes
Monitoring in Type 2 Diabetes. Learning Outcomes. Type 2 Diabetes. Senga Hunter Community Diabetes Specialist Nurse
 Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Technology for Diabetes: 101 Basic Rules of the Road. Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE
 Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Pathogenesis of Type 1 Diabetes. Diabetes Mellitus Type 1. Pathogenesis. Pathogenesis of DM1. Type 2. Type 1. Genetics of Type 1 Diabetes
 Pathogenesis of Type 1 Diabetes Diabetes Mellitus Type 1 D G V A N ZYL Genetics of Type 1 Diabetes Pathogenesis Complex and poorly understood interplay between genetics and environmental factors Monozycotic
Pathogenesis of Type 1 Diabetes Diabetes Mellitus Type 1 D G V A N ZYL Genetics of Type 1 Diabetes Pathogenesis Complex and poorly understood interplay between genetics and environmental factors Monozycotic
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
COPYRIGHTED MATERIAL. Chapter 1 An Introduction to Insulin Pump Therapy WHAT IS INSULIN PUMP THERAPY?
 Chapter 1 An Introduction to Insulin Pump Therapy This chapter will provide information on what insulin pump therapy is, and how insulin pumps have developed from the early models introduced in the 1970s
Chapter 1 An Introduction to Insulin Pump Therapy This chapter will provide information on what insulin pump therapy is, and how insulin pumps have developed from the early models introduced in the 1970s
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations
 Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup
 1 Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup King s College London School of Medicine, Guy s Hospital, London SE1 9RT Experience of the technology I am the lead
1 Personal statement on Continuous Subcutaneous Insulin Infusion Professor John Pickup King s College London School of Medicine, Guy s Hospital, London SE1 9RT Experience of the technology I am the lead
Gentle and safe injections. Tips and tricks for injecting insulin.
 Gentle and safe injections. Tips and tricks for injecting insulin. Freedom. Confidence. With mylife. Gentle and safe injections The correct injection technique The insulin is injected into the subcutaneous
Gentle and safe injections. Tips and tricks for injecting insulin. Freedom. Confidence. With mylife. Gentle and safe injections The correct injection technique The insulin is injected into the subcutaneous
DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address:
 Name: Ward/Practice Area: Mailing Address:") 1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
Types of insulin. Your blood glucose levels. Types of insulin
 Different types of insulin are available for people with diabetes. If you need insulin, you and your diabetes team will look at the options and decide which type fits best with your lifestyle and blood
Different types of insulin are available for people with diabetes. If you need insulin, you and your diabetes team will look at the options and decide which type fits best with your lifestyle and blood
insulin and injections
 insulin and injections Insulin is a hormone made by the beta cells in the pancreas. Insulin allows sugar to go from the bloodstream into the body s cells and be used for energy. Insulin lowers blood sugar.
insulin and injections Insulin is a hormone made by the beta cells in the pancreas. Insulin allows sugar to go from the bloodstream into the body s cells and be used for energy. Insulin lowers blood sugar.
WHEN YOUR PANCREAS IS NOT A HAPPY CAMPER A PRESENTATION ON DIABETES MANAGEMENT IN THE CAMP SETTING AMANDA COSCHI, BSCN, RN, CDE
 WHEN YOUR PANCREAS IS NOT A HAPPY CAMPER A PRESENTATION ON DIABETES MANAGEMENT IN THE CAMP SETTING AMANDA COSCHI, BSCN, RN, CDE MAY 5, 2018 OBJECTIVES Strong understanding of diabetes and its management
WHEN YOUR PANCREAS IS NOT A HAPPY CAMPER A PRESENTATION ON DIABETES MANAGEMENT IN THE CAMP SETTING AMANDA COSCHI, BSCN, RN, CDE MAY 5, 2018 OBJECTIVES Strong understanding of diabetes and its management
LET S TALK INSULIN THE BASICS
 LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
Policy for the safe administration of Insulin
 Policy for the safe administration of Insulin This is a working document and any changes that become necessary to this policy must be Notified in writing to the Medicine Management Group via the Chief
Policy for the safe administration of Insulin This is a working document and any changes that become necessary to this policy must be Notified in writing to the Medicine Management Group via the Chief
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
Patient Education Pharmacy Services
 Patient Education This handout details the types of insulin. It also covers how to store, mix and inject insulin. What is insulin? Insulin is made by the pancreas and acts as a key to move glucose (sugar)
Patient Education This handout details the types of insulin. It also covers how to store, mix and inject insulin. What is insulin? Insulin is made by the pancreas and acts as a key to move glucose (sugar)
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
SCHOOL HEALTH PLAN: DIABETES
 BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
Safe and Gentle Injection of Insulin. Guide for correct injection technique. Englische Ausgabe
 Safe and Gentle Injection of Insulin Guide for correct injection technique Englische Ausgabe Insulin injection basics 1 Insulin has to be injected into the subcutaneous fat layer 3 Rotate the injection
Safe and Gentle Injection of Insulin Guide for correct injection technique Englische Ausgabe Insulin injection basics 1 Insulin has to be injected into the subcutaneous fat layer 3 Rotate the injection
Continuous Subcutaneous Insulin Infusion (CSII) pump therapy
 pump therapy") Page 1 of 14 Continuous Subcutaneous Insulin Infusion (CSII) pump therapy Introduction This booklet has been compiled by the Insulin Pump Therapy Team to standardise the information given to patients on
Page 1 of 14 Continuous Subcutaneous Insulin Infusion (CSII) pump therapy Introduction This booklet has been compiled by the Insulin Pump Therapy Team to standardise the information given to patients on
Gentle and safe injections. Tips and tricks for injecting insulin.
 Gentle and safe injections. Tips and tricks for injecting insulin. More freedom. More confidence. With mylife. Gentle and safe injections The correct injection technique The insulin is injected into the
Gentle and safe injections. Tips and tricks for injecting insulin. More freedom. More confidence. With mylife. Gentle and safe injections The correct injection technique The insulin is injected into the
Audit support for continuous subcutaneous insulin infusion for the treatment of diabetes mellitus (review of technology appraisal guidance 57)
") Audit support for continuous subcutaneous insulin (review of technology appraisal guidance 57) Issue date: 2008 Audit support Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus
Audit support for continuous subcutaneous insulin (review of technology appraisal guidance 57) Issue date: 2008 Audit support Continuous subcutaneous insulin infusion for the treatment of diabetes mellitus
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Workshop 4 Making the complex simple
 Workshop 4 Making the complex simple Goal of workshop Insulin commencement making the complex simple Ensure participants are confident with Selecting and using devices Troubleshooting injection issues
Workshop 4 Making the complex simple Goal of workshop Insulin commencement making the complex simple Ensure participants are confident with Selecting and using devices Troubleshooting injection issues
Injection Technique (I.T.), Glycemic Variability, and Lipohypertrophy. Why I.T. All Matters
, Glycemic Variability, and Lipohypertrophy. Why I.T. All Matters") Injection Technique (I.T.), Glycemic Variability, and Lipohypertrophy Why I.T. All Matters Larry Hirsch, MD Vice-President, Global Medical Affairs BD Diabetes Care Seoul, South Korea KDA-ICDM 29 September
Injection Technique (I.T.), Glycemic Variability, and Lipohypertrophy Why I.T. All Matters Larry Hirsch, MD Vice-President, Global Medical Affairs BD Diabetes Care Seoul, South Korea KDA-ICDM 29 September
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Insulin Optimisation Workshop. Theingi Aung & Claire Rowell
 Insulin Optimisation Workshop Theingi Aung & Claire Rowell Insulin initiation and titration Insulin Preparations Rapid-acting insulin analogues: onset of action of approximately 15 minutes and a duration
Insulin Optimisation Workshop Theingi Aung & Claire Rowell Insulin initiation and titration Insulin Preparations Rapid-acting insulin analogues: onset of action of approximately 15 minutes and a duration
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Lander County School District
 Lander County School District of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant
Lander County School District of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS
 TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
Diabetes Medical Management Plan
 Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
VICTORIA INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan
 VICTORIA INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. Student s Name: of Birth: of Diabetes
VICTORIA INDEPENDENT SCHOOL DISTRICT Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. Student s Name: of Birth: of Diabetes
What is the role of insulin pumps in the modern day care of patients with Type 1 diabetes?
 What is the role of insulin pumps in the modern day care of patients with Type 1 diabetes? Dr. Fiona Wotherspoon Consultant in Diabetes and Endocrinology Dorset County Hospital Fiona.Wotherspoon@dchft.nhs.uk
What is the role of insulin pumps in the modern day care of patients with Type 1 diabetes? Dr. Fiona Wotherspoon Consultant in Diabetes and Endocrinology Dorset County Hospital Fiona.Wotherspoon@dchft.nhs.uk
Case Study: Competitive exercise
 Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Complete this CE activity online at ProCE.com/InsulinPart2
 Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011
 DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards
9-A. Diabetes Medical Management Plan
 of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant school staff and copies should
of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant school staff and copies should
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
TO BE COMPLETED BY LICENSED HEALTH CARE PROFESSIONAL
 PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
Approach to the Young child & Parent with Child with DM Best Structure for Continued Care
 Approach to the Young child & Parent with Child with DM Best Structure for Continued Care M.S. Limbe MD Paediatric Endcocrinologist Aga Khan University Hospital, Nairobi Approach to the Young Child & Parent
Approach to the Young child & Parent with Child with DM Best Structure for Continued Care M.S. Limbe MD Paediatric Endcocrinologist Aga Khan University Hospital, Nairobi Approach to the Young Child & Parent
INSULIN INJECTION KNOW-HOW
 0-1- INSULIN INJECTION KNOW-HOW Learning how to Congratulations for making the move to insulin therapy. It won t be long before you start enjoying better blood sugar control, more energy, and a host of
0-1- INSULIN INJECTION KNOW-HOW Learning how to Congratulations for making the move to insulin therapy. It won t be long before you start enjoying better blood sugar control, more energy, and a host of
Managing Problematic Hypoglycaemia Pratik Choudary
 Managing Problematic Hypoglycaemia Pratik Choudary Control Hypoglycaemia What is normal? Rate per 100 years 100 80 60 40 Is tighter control associated with more severe hypoglycaemia? Intensive Conventional
Managing Problematic Hypoglycaemia Pratik Choudary Control Hypoglycaemia What is normal? Rate per 100 years 100 80 60 40 Is tighter control associated with more severe hypoglycaemia? Intensive Conventional
Diabetes Medical Management Plan
 SCHOOL DISTRICT OF LEE COUNTY HEALTH SERVICES Print Form Date of Plan Diabetes Medical Management Plan This plan should be completed by the student's personal health care team and parents/guardian. It
SCHOOL DISTRICT OF LEE COUNTY HEALTH SERVICES Print Form Date of Plan Diabetes Medical Management Plan This plan should be completed by the student's personal health care team and parents/guardian. It
Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011
 Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011 Dr Kingsley Nirmalaraj FRACP Endocrinologist BOPDHB Workshop goal To make participants comfortable in the timely
Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011 Dr Kingsley Nirmalaraj FRACP Endocrinologist BOPDHB Workshop goal To make participants comfortable in the timely
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Hypoglycemia a barrier to normoglycemia Are long acting analogues and pumps the answer to the barrier??
 Hypoglycemia a barrier to normoglycemia Are long acting analogues and pumps the answer to the barrier?? Moshe Phillip Institute of Endocrinology and Diabetes National Center of Childhood Diabetes Schneider
Hypoglycemia a barrier to normoglycemia Are long acting analogues and pumps the answer to the barrier?? Moshe Phillip Institute of Endocrinology and Diabetes National Center of Childhood Diabetes Schneider