Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011
|
|
|
- Darrell Wright
- 6 years ago
- Views:
Transcription
1 Insulin Initiation and titration in the Primary Care-KISS Rotorua GP CME Meeting June 2011 Dr Kingsley Nirmalaraj FRACP Endocrinologist BOPDHB
2 Workshop goal To make participants comfortable in the timely initiation and titration of insulin

3 Linda T2D 6 years

4 Linda 51-year-old laboratory technician (works day shifts) Presents for annual review of her T2D following a reminder letter triggered by the diabetes recall system Has completed the routine tests requested on the pathology slip that was included with the reminder letter in time for this visit Diagnosed with T2D 6 years ago Married with two sons in secondary school
5 History (1) You have managed Linda s diabetes on and off since diagnosis Her oral hypoglycaemic agents (OHAs) have been slowly increased to get better control Linda checks blood glucose most days mainly first thing in the morning; occasionally before dinner Comments that her morning test (i.e. fasting blood glucose [FBG]) is usually well over 8 mmol/l )
6 History (2) Eyes tested 2 months ago by optician no problems found Non-smoker who drinks alcohol at weekends A few Friday night drinks with work colleagues; occasional wine on Saturday evenings Led a sedentary life prior to diabetes diagnosis but has become more active with your help: Regular yoga class once a week Organises walks with friends once a week
7 Examination Height: Weight: 1.60 m 84 kg BMI: 33 kg/m 2 Waist: BP: Feet : 99 cm 135/90 mmhg Sensation adequate, pulses easily felt Urinanalysis: No abnormalities noted
8 Pathology results HbA 1c 11.2% TC 4.3 mmol/l TG 2.1 mmol/l HDL 1.1 mmol/l LDL 2.7 mmol/l egfr >60 ml/min ACR 40 mg/mmol Microalbuminuria 40 µg/24 h
9 Medications Metformin Gliclazide Aspirin Atorvastatin Cilazapril 1000 mg bd 160mg bd 100 mg daily 40 mg daily 5mg daily
10 Reviewing A1C target You previously set an A1c target of 7% with Linda, but her A1c has been slowly creeping up. Would you revise Linda s A1c target at this point? 1. Yes, I would give her an interim target of 8% 2. No, an A1c of 7% is still appropriate 3. No, leave for now and review later 4. Not sure
11 Setting an A1C target 1% fall in A1C reduces microvascular complications by 37%, 1 but risk of: 2 Hypoglycaemia Weight gain (approx 2kg) 1. Stratton IM et al. BMJ 2000; 321: ; 2. Phillips PJ. Medicine Today 2007; 8(4):
12 Setting an A1C target Recommended A1c target 7% but should be tailored to patient. Consider: 2 1. The individual s A1C value the higher the A1C, the more difficult it may be to achieve target of 7% 2. Patient s age may have to consider less tight glycaemic control if patient is old, frail, or has a failing memory 3. Patient s lifestyle hard to avoid weight gain if patient has conditions that make increasing physical activity or controlling diet difficult to do; conversely, if patient exercises a lot or lives alone, has higher risk of hypoglycaemia 1. Stratton IM et al. BMJ 2000; 321: ; 2. Phillips PJ. Medicine Today 2007; 8(4):
13 Improving glycaemic control You decide that an A1C target of 7% is still appropriate for Linda and discuss with her the best option for improving her glycaemic control. What treatment change would you recommend to Linda at this point? 1. Add acarbose to existing regimen 2. Add glitazone to existing regimen 3. (Add exenatide or sitagliptin to existing regimen) 4. Start insulin
14 2009 ADA/EASD treatment algorithm Tier 1: Well-validated therapies # At diagnosis: Lifestyle + metformin Lifestyle + met + basal insulin Lifestyle + met + sulfonylureas* Lifestyle + met + intensive insulin STEP 1 STEP 2 STEP 3 Tier 2: Less well-validated therapies # Lifestyle + met + pioglitazone No hypoglycaemia Oedema/CHF Bone loss Lifestyle + met + GLP-1 agonist No hypoglycaemia Weight loss Nausea/vomiting Nathan D et al. Diabetes Care 2009; 32: Lifestyle + met + pioglitazone + sulfonylurea* Lifestyle + met + basal insulin * Sulfonylureas other than glibenclamide (glyburide) Insufficient clinical use to be confident regarding safety # Check A1c every three months until A1c is <7% and then at least every 6 months. The interventions should be changed if A1c is 7%.
15 Actions of available drugs insulin peripheral insulin resistance liver insulin resistance carbohydrate absorption Sulphonylureas X Glitizones X Metformin X Acarbose X Insulin X
16 HbA1c decrease by agent Agent HbA1c reduction, % Diet Exercise Weight loss Even more Metformin Acarbose Sulphylurea Pioglitazone Insulin Even more Kenealy et al 2008
17
18 Initiating insulin therapy You think you need to start Linda on insulin because of her very elevated A1c, however you decide to check a few other things first. What else do you need to check before starting insulin therapy? 1. That the patient is compliant with all lifestyle measures and medication and whether any modifications could improve glycaemia 2. Any possible secondary causes of hyperglycaemia 3. Both 1 and 2 4. Nothing else
 Medical conditions (e.")
19 When to introduce insulin therapy A1C persistently above target Lifestyle Patient compliant with agreed modifications? Any further modifications that can be considered? Oral hypoglycaemic medication Is patient taking as prescribed? Can these be maximised further? Secondary causes for hyperglycaemia? Medications (e.g. contraceptive pill, thiazides,beta-blockers, oral corticosteroids) Medical conditions (e.g. hyperthyroidisim, urinary or dental infections, occult malignancy) A1C still above target Initiate insulin Philips P. Medicine Today 2007; 8:
20 Diabetes/insulin education Education on injecting insulin, BGL monitoring, hypos, activity/diet and life with insulin is essential to prepare patients for insulin therapy. Do you do it all yourself or engage other healthcare professionals to assist you? You discuss your plan with Linda and organise this through a Team Care Arrangement. In your current practice, how would you educate Linda? 1. Do it all yourself 2. Refer to a Specialist/DNS 3. Engage your practice nurse 4. Engage your practice nurse and a DNS 5. Other
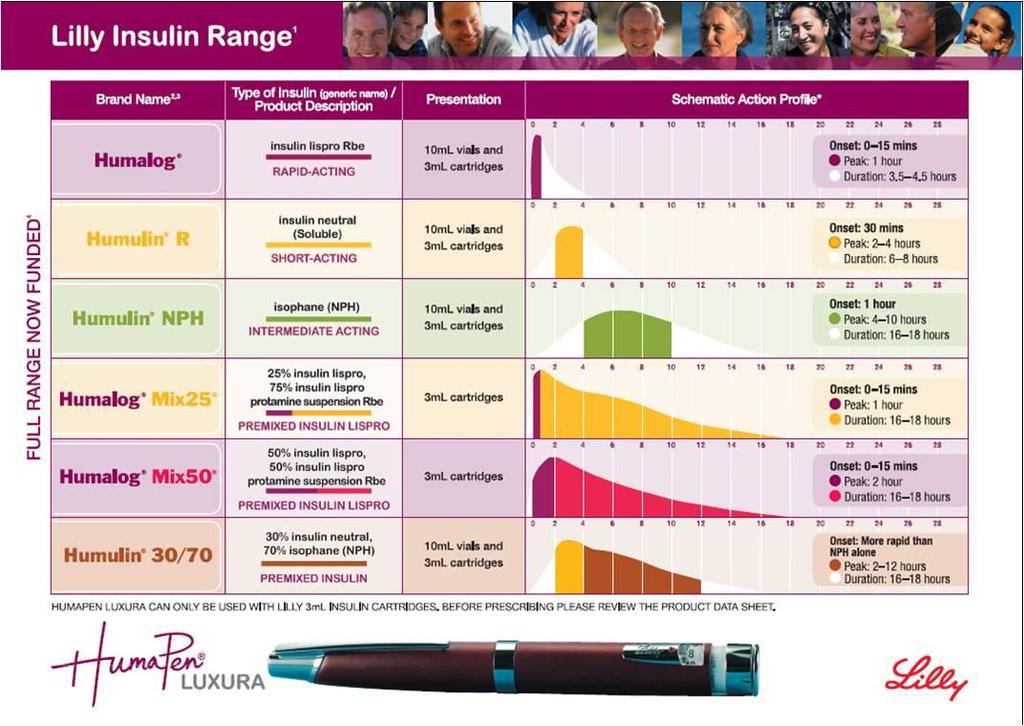
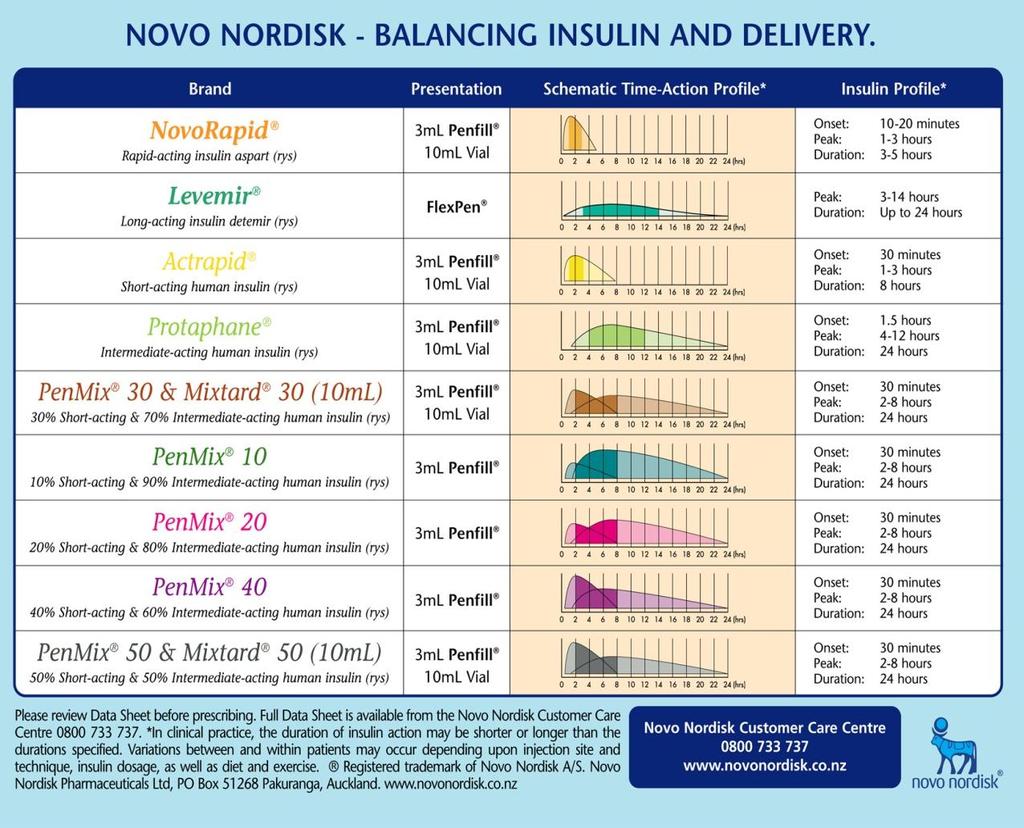
21 Selecting an insulin You decide to start Linda on insulin and discuss the different insulin profiles with her. Which insulin would you recommend for Linda and why? 1. Rapid-acting insulin to the meal with the highest preprandial BGL 2. Intermediate-acting insulin in the morning or night 3. Insulin premixed for ease of use 4. Basal insulin to reduce both postprandial and fasting BGLs

22
23
24 Selecting an insulin RACGP & ADA/EASD guidelines state Start with single daily dose (10 units) of bedtime intermediate-acting insulin or morning or bedtime longacting insulin 1,2 Rapid-acting insulin is not necessarily needed at initiation 1 Premixed insulin is not recommended during dosage adjustment period 2 Insulin regimens should be designed taking lifestyle and meal schedule into account 2 1. DA/RACGP Diabetes management in general practice 2009/ Nathan D et al. Diabetes Care 2009; 32:

25 Stepwise approach for T2D with progressive deterioration of beta cell function
26 Plasma glucose (mmol/l) Why start with basal insulin? Comparison of 24-hour glucose levels in untreated vs treated patients with diabetes T2DM Plasma glucose (mmol/l) Meal Meal Meal :00 10:00 14:00 18:00 22:00 02:00 06:00 Time of day (hours) Adapted from Hirsch I et al. Clin Diabetes 2005; 23:
27 Which basal insulin? You decide to start Linda on a basal insulin to address her fasting BGL. Which basal insulin would you recommend for Linda? Which basal insulin would you recommend for Linda and why? 1. Intermediate-acting, human ispophane/nph insulin 2. Long-acting insulin analogue, insulin glargine 3. Long-acting insulin analogue, insulin detemir 4. Not sure
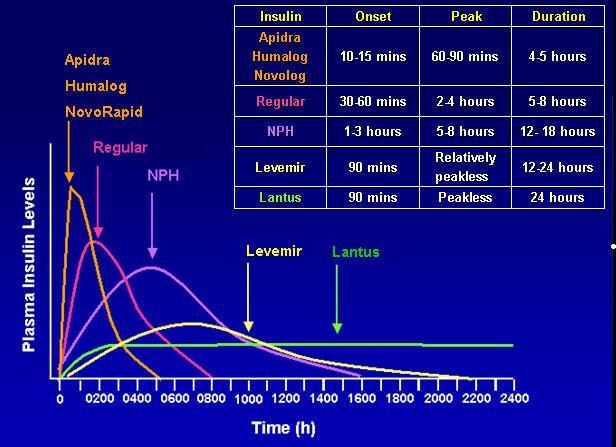
28 Intermediate-acting Which basal insulin? Onset Peak Duration Funded Isophane (OD/BD) Long-acting 1 2 h 4 12 h h Yes Glargine (OD) 2 4 h None 24 h Yes* Detemir (OD/BD) 1 2 h 6 12 h h No Adapted from Clinical Practice Guidelines: Type 1 Diabetes in Children and Adolescents by Australian Paediatric Endocrine Group. p58
29 Starting insulin dose You decide to start Linda on insulin NPH. What starting dose would you select? 1. 1 U/kg U/day U/day 4. Not sure

30 Linda s BGLs during past week (before starting insulin) 12 May Before Breakfast Before Dinner Before Breakfast Before Dinner
31 Initiating insulin therapy You decide to start Linda on 10 U of insulin NPH. Would it be best to start Linda on a morning or evening basal dose? 1. Morning 2. Evening 3. Not sure
32 Timing of single insulin dose Morning or evening is acceptable Timing depends on blood glucose profile: If fasting BGL is high give at bedtime If fasting BGL on target but evening BGL high give in morning If both are high give bd NPH or once daily glargine/detemir (not funded) Add basal insulin to OHAs Aim to achieve fasting BGL of 6.0 mmol/l* Starting dose: 10 units morning or at bedtime OHAs continued at same doses Monitor Fasting BGL * Usually the fasting BG target is 6.0mmol/L; however, targets may vary from one person to the next. 1. Phillips PJ Medicine Today, 2007; 8 (3): 23-34; 2. Davies M et al. Diabetes Care 2005; 28: ; 3. Rosenstock J et al. Diabetologia 2008; 51(3): Diabetes Australia/RACGP. Diabetes management in general practice. Guidelines for type 2 diabetes 15 th ed, 2009/10.
33 Insulin management next steps You start Linda on 10 U at bedtime of insulin NPH and discuss that her dose will need to increase over the next few months to achieve a target FBG of approx 6.0 mmol/l. This will be done with the help of your Practice Nurse You explain that it could take a very long time to reach a high enough insulin dose if the dose is increased slowly. Linda is a little concerned about potential weight gain and wants to increase the dose slowly initially and is willing to try a faster dose increase down the track.
34 Linda s summary to this point Elevated A1C on optimal doses of two (2) OHAs Lifestyle measures reviewed, no secondary causes of hyperglycaemia Insulin therapy is appropriate Basal insulin is most appropriate at this time Bedtime injection of 10 U insulin NPH to reduce Linda s fasting BGL Up-titration to be self-managed in consultation with Practice Nurse Linda to return for review in 3 months with lab tests completed prior to visit
35 Titrating insulin therapy Linda was started on 10 U of insulin NPH at bedtime. You instructed her to self-manage the dose up-titration in consultation with your Practice Nurse. Which schedule would you choose to advise Linda regarding uptitrating her dose in consultation with your Practice Nurse? 1. Slow schedule: increase 2 U every 3 days 2. Fast schedule: increase by 2-8 units of insulin depending on fasting BGL over previous 3 days 3. Not sure
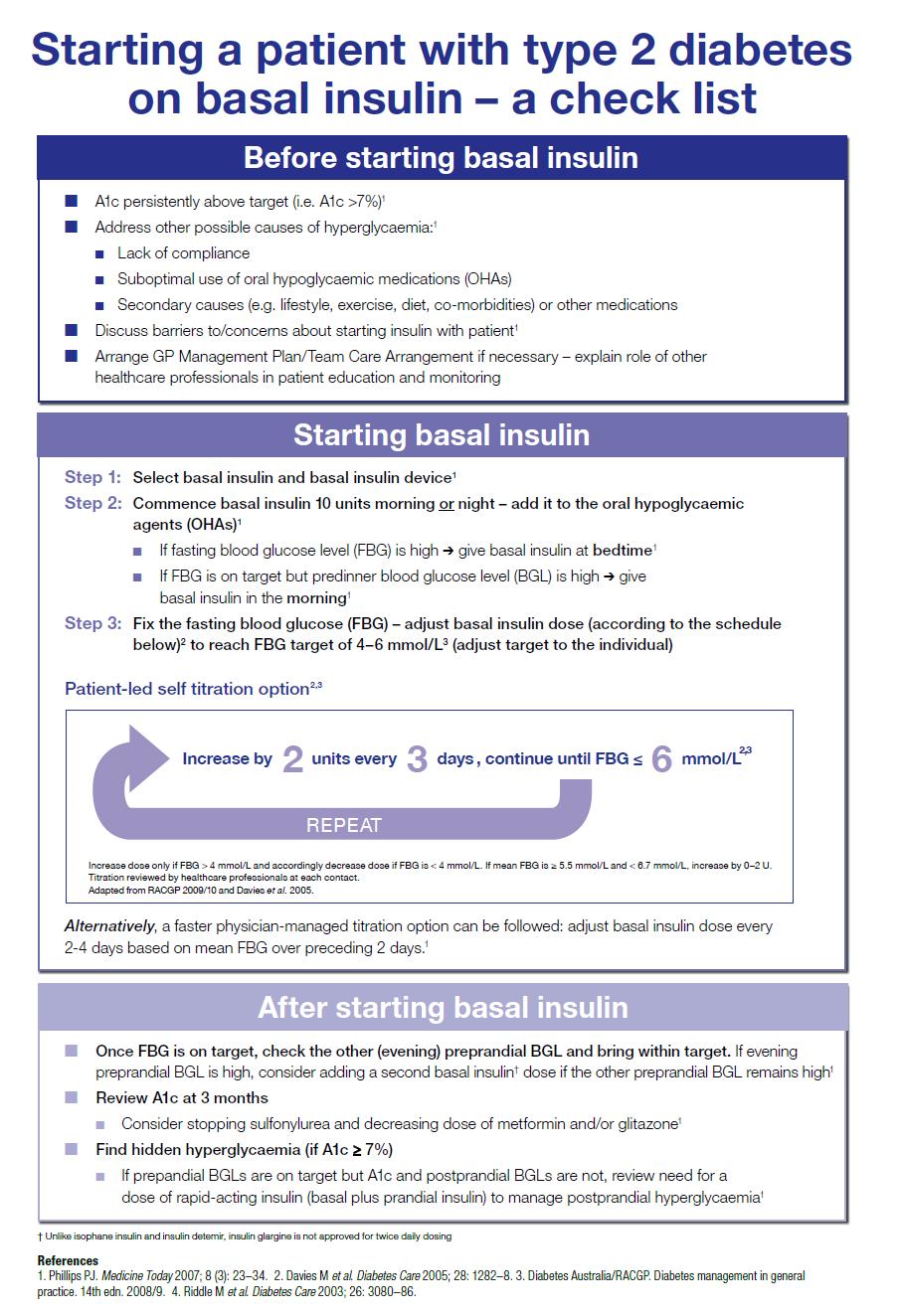
36 Dose adjustment first fix fasting Two dose adjustment schedules possible: 1. SLOW SCHEDULE (CAN BE PATIENT-LED) Increase by 2 units of insulin every 3 days continue until fasting BGL is 6.0 mmol/l Adapted from RACGP 2009/10 and Davies et al Increase dose only if FBG >4 mmol/l and accordingly decrease dose if FBG is <4 mmol/l. Titration reviewed by HCPs at each contact.
37 Dose adjustment first fix fasting 2. FAST SCHEDULE (PHYSICIAN-MANAGED) Increase by 2 8 units of insulin depending on fasting BGL over previous 2 3 days Mean fasting blood glucose (mmol/l) Increase in insulin dose <4 * See below No change units units units >10 8 units Starting dose 10 units, adjust dose twice weekly to reach the target FBG of <6mmol/L Insulin dose may be decreased (small decreases of 2 to 4 units) if there is severe hypoglycaemia (requiring assistance) or if BGL <3.0 mmol/l in preceding week. Do not increase insulin dose if fasting BGL <4 mmol/l at any time in preceding week. Adapted from Phillips PJ. Medicine Today 2007; 8(3):
38 Linda: 3 month review after starting insulin Presents for regular review of her type 2 diabetes following insulin initiation 3 months ago Medication: Insulin NPH Metformin Gliclazide Aspirin Atorvastatin cilazapril 30 U at bedtime 1000 mg bd 120 mg morning 100 mg daily 40 mg daily 10 mg daily
39 18 August Review: 3 months Linda s A1c is 8.9% (down from 11.2%) been on slow titration schedule Units of basal insulin Before Breakfast After Breakfast After Lunch Before Bed Before Breakfast Before Bed
40 Next steps Linda has increased her daily activity and only gained ½ kg since starting insulin and has enjoyed the support of the CDE during the up-titration process. She is however frustrated that her FBGs are still not in range. What would you do now? 1. Add a dose of bolus insulin? 2. Increase the dose of insulin NPH using a faster titration schedule 3. Increase the dose of insulin NPH using the slow titration schedule 4. Add a second dose of insulin NPH?
41 Next steps You organise for the Practice Nurse to work with Linda to more rapidly uptitrate the dose of insulin NPH to achieve a FBG of 6.0 mmol/l. You also ask the Practice Nurse to discuss hypoglycaemia and sick day management with Linda. Linda is requested to return to you in 3 months time.
42 Review: 6 months Linda returns to check lipid profile, A1c and spot urinary microalbumin test (ACR) Linda s FBG readings 6 mmol/l OHAs remain unchanged Insulin NPH 45 U Her BP, urinalysis all okay Pathology results: A1c 7.7% No evidence of microalbuminuria, and a satisfactory lipid profile
43 20 November Units of basal insulin Review: 6 months Linda s A1c is 7.7% (down from 8.9%) been on fast titration schedule Before Breakfast Before Lunch Before Bed Before Breakfast After Lunch Before Bed
44 Reviewing OHA use Linda is doing well on basal insulin and had no problems with the rapid up-titration process. Linda is now stable at 45 units of basal insulin daily. Linda asks if she still needs her OHAs. Would you rationalise Linda s OHAs at this point? 1. Stop all her OHAs straight away 2. Consider stopping one after A1C is under control 3. Definitely not to stop any OHAs 4. Not sure
45 Linda s OHAs Don t stop OHAs immediately Stopping OHAs may require more insulin Get A1c under control and consider stopping OHAs later Understand what each drug does Metformin [& glitazones] = insulin sensitisers should be continued Sulphonylureas = insulin secretagogues will need to be removed when ß-cells stop secreting insulin Discontinue if side effects are an issue Metformin: SU: Glitazone: fluid retention, weight gain, cardiovascular risks 1. Phillips PJ. Medicine Today 2007; 8(3): 23-34; 2. Phillips PJ. Aust Fam Physician, 2006; 35: ; 3. Phillips PJ. Medicine Today 2007; 8(6): 43-52; 4. Nathan D et al. Diabetologia 2008; 52: 8-11; 5. Nathan D et al. Diabetologia 2006: 49:

46 β-cell function (%) ß-cell failure defect in T2D Patients have only about 50% of normal β-cell function at time of diagnosis, and it continues to decline Diagnosis Years from diagnosis Dashed line represents extrapolation forward and backward from years 0 to 6 based on HOMA data from UKPDS. Lebovitz H. Diabetes Rev. 1999;7:
47 Improving glycaemic control You congratulate Linda on her fasting & bedtime BGLs, but you are still concerned that her A1C is still too high. What should you look for at this stage? 1. Nocturnal hypoglycaemia 2. Postprandial hypoglycaemia 3. Hidden hyperglycaemia 4. Not sure
48 Find hidden hypers Fasting preprandial BGL on target (4 6 mmol/l) 2 hour postmeal BGL on target (4 8 mmol/l) Is A1C 6-12 weeks later at target? Yes Continue with current schedule No Find and fix the hidden hyperglycaemia a) check 2 hours after breakfast & before bed to check for morning and evening postprandial hyperglycaemia b) check during the night (only if really necessary!) Diabetes Management in General Practice, 2009/10; Phillips (3): 23-34
49 Finding hidden hypers You discuss with Linda that you suspect that there are periods of hyperglycaemia causing her A1C to remain elevated. You discuss that she will need to monitor her BGLs at different times of the day to see when they are occurring. You suspect her large breakfast may be contributing to her elevated A1C. What BGL testing would you advise Linda to do over the next weeks? 1. 2 hours after breakfast 2. Before lunch 3. 2 hours after lunch 4. Before bed 5. Other

50 10 Feb Review: another 3 months later Linda s A1c remains elevated at 7.6% Units of basal insulin Before Breakfast After Breakfast After Lunch Before Bed Before Breakfast Before Bed
51 Improving glycaemic control You inform Linda that her BGLs 2 hours after breakfast are consistently high indicating hyperglycaemia after breakfast. What treatment options would you discuss with Linda? 1. Exercise after breakfast (brisk walk) 2. Seek dietitian s advice on carbohydrate intake for breakfast 3. Consider altering existing insulin therapy 4. All of the above
52 Adjusting insulin therapy You discuss options with Linda and agree that modifying the insulin schedule is the best option for her. What alterations in Linda s insulin schedule would you recommend? 1. Increasing the basal insulin dose 2. Add a single dose of rapid-acting insulin at lunch 3. Add a single dose of rapid-acting insulin at breakfast 4. Not sure
53 Starting second insulin injection A second injection can be added according to the when the glucose excursion is occurring. Time at which BG is out of range Type of Insulin When to add Pre-lunch Prandial Breakfast Pre-Dinner NPH Prandial Breakfast Lunch Pre-Bedtime Prandial Dinner
54 Plasma glucose (mmol/l) Then Tackle The Meal Responsible for the Greatest Glycaemic Excursion Time of day (h)
55 Starting prandial insulin You discuss treatment options and you both agree that adding a single dose of prandial insulin prior to the meal contributing most to hyperglycaemia would be appropriate as she finds it difficult to change her morning eating habits and exercise schedule. How would you calculate the initial dose of prandial or bolus insulin? 1. One-third the basal dose 2. 4 units 3. Start low, go slow 4. Not sure
56 Start prandial insulin at 4 Units Step 1: Add prandial insulin to meal most contributing to hyperglycaemia Starting dose: 4 units 1-4 to meal most contributing Monitor Postprandial BGLs Step 2: Step 3: If BGL off target (high) Adjust prandial insulin Titrate dose Increase by 2 U every 2 3 days Until postprandial for next meal is mmol/l 5, If A1C not at target after 3/12 Add prandial insulin to other meals* These dosing guidelines are based on recommendations from a number of authors. They are provided for guidance only. All insulin dosing and titration / adjustments require professional judgment and should be individualised to patient circumstances. Once prandial insulin is added, insulin secretagogues may be discontinued 1.Garg S, et al. J Fam Pract April Suppl_S1-S Raccah D, et al. Diabetes Metab Research and Reviews. 2007; 23: Tibaldi J, American Journal of Medicine. 2008; 121 (6A) S20-S29 4. Nathan D, et al. Diabetologia 2006; 51: RACGP/Diabetes Australia. Diabetes Management in General Practice, 2009/10.
 at breakfast Units of")

57 10 Feb Reviewing BGLs:4 weeks later Linda shows you her BGL readings after 3 weeks of prandial insulin (15U) at breakfast Units of rapid-acting insulin Units of basal insulin Before Breakfast After Breakfast After Lunch Before Bed Before Breakfast After Breakfast Before Bed
58 Reviewing BGLs: 4 weeks later (2) You congratulate Linda on achieving great readings Her BGLs are all within range Linda comments that she feels so much better You suggest Linda keep her basal dose at 45 U You ask Linda to maintain her bolus dose at 15 U With further review in 3 months Linda is asked to return in another 12 weeks You check that the CDE will remain in contact with her in the interim Reminder letter and pathology request will be sent prior to the next visit
59 Linda: summary Linda self-titrated insulin dose from 10 U to 45 U (slow titration schedule initially and changed to rapid titration) 6 months after starting basal insulin Linda s fasting BGLs were on target Hidden hyperglycaemia suspected with A1C slightly elevated Post-breakfast hyperglycaemia identified with more regular BGL testing Prandial insulin considered appropriate treatment 15 U at breakfast improved glycaemic control Regular review with Practice Nurse Linda to return for review in 3 months
60 Protaphane/Humulin N dose self-adjustment sheet Mean capillary blood glucose (mmol/l) Protaphane/Humulin N dose adjustment < 4 Return to previous dose tolerated Unchanged > Date Fasting blood glucose Mean fasting blood glucose Current dose New dose
61 Glargine/Detemir dose self-adjustment sheet Mean capillary blood glucose (mmol/l) Glargine/Detemir dose adjustment < 4 Return to previous dose tolerated Unchanged > Date Fasting blood glucose Mean fasting blood glucose Current dose New dose
62 Practice points Don t delay insulin initiation Keep it simple for you and patient 10 units basal insulin Ensure patient has expectation that basal dose will increase and what the dose may end up at Titrate! Fix the fasting first! Then look for hidden hypers
63
64 Other situations
65 Example -1 John is teacher Type 2 DM for 7 years HbA1c has been 8.5 to 9.7 % over the last 1-2 yrs on max OHAs Metformin 2.5g/d, Glipizide 10mg mane,15 mg nocte Seeing you for routine review He has been testing mainly before breakfast and occasionally before dinner
66 John s BG readings Fasting Pre-lunch Pre-dinner Postdinner Wednesday 9.1 Thursday Friday Saturday 10.4 Sunday Monday 7.9 Tuesday Wednesday 8.7
67 You ask him to bring more intensive SMBG test results
68 John s BG readings Fasting Pre-lunch Pre-dinner Postdinner Wednesday Thursday Friday Saturday Sunday Monday Tuesday Wednesday 8.7
69 What Insulin regime you are going to propose to John re: insulin therapy?
70 John s BG readings Fasting Pre-lunch Pre-dinner Postdinner Wednesday Thursday Friday Saturday Sunday Monday Tuesday Wednesday 8.7
71
72 Example 2 Matt is a 70 yr old, Type 2 diabetes for 5 yrs, well managed on Metformin 1g bid, Gliclazide 80mg bid Recently been diagnosed with temporal arteritis- started on high dose Prednisone His glycaemic control has deteriorated with previous A1c levels of 6.5% has risen to 9.7% His SMBGs test results show
73 Matt s BG readings show Fasting Pre-lunch Pre-dinner Postdinner Wednesday Thursday Friday Saturday Sunday Monday Tuesday Wednesday
74 What insulin regime would be suitable for him?
75 Thank you. Acknowledgement A/Prof Tim Kenealy Dr Brandon Orr- Walker
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008)
") Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Volume 2; Number 14 September 2008 NICE CLINICAL GUIDELINE 66: TYPE 2 DIABETES THE MANAGEMENT OF TYPE 2 DIABETES (MAY 2008) The purpose of this special edition of the PACE Bulletin is to summarize the
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia
 CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
Take Charge of Your Life With QuickChek
 monitor track manage A TRUEinsight Guide manage Take Charge of Your Life With QuickChek Better Understand Your Blood Glucose Results How to use your QuickChek Record Book Monitor Track Manage Blood glucose
monitor track manage A TRUEinsight Guide manage Take Charge of Your Life With QuickChek Better Understand Your Blood Glucose Results How to use your QuickChek Record Book Monitor Track Manage Blood glucose
RDNS. Injection Therapy in injection therapy in diabetes. Type 2 Diabetes
 RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
Case study for CME Diabetes up-to-date management
 Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
Complete this CE activity online at ProCE.com/InsulinPart2
 Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
Complete this CE activity online at ProCE.com/InsulinPart2 Case 1: A 67 year old male with T2DM History and Presentation John is a 67 year old retiree who has been visiting your pharmacy/clinic for over
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address:
 Name: Ward/Practice Area: Mailing Address:") 1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
MANAGEMENT OF DIABETES IN PREGNANCY
 MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
Insulin Intensification: A Patient-Centered Approach
 MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
Insulin Optimisation Workshop. Theingi Aung & Claire Rowell
 Insulin Optimisation Workshop Theingi Aung & Claire Rowell Insulin initiation and titration Insulin Preparations Rapid-acting insulin analogues: onset of action of approximately 15 minutes and a duration
Insulin Optimisation Workshop Theingi Aung & Claire Rowell Insulin initiation and titration Insulin Preparations Rapid-acting insulin analogues: onset of action of approximately 15 minutes and a duration
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Type 1 Diabetes & Continuous Glucose Monitoring. Dr Sheila Cook Director of Diabetes & Endocrinology Toowoomba Hospital
 Type 1 Diabetes & Continuous Glucose Monitoring Dr Sheila Cook Director of Diabetes & Endocrinology Toowoomba Hospital Let s consider the traditional diabetes clinic The Diabetes Clinic Whenever I check
Type 1 Diabetes & Continuous Glucose Monitoring Dr Sheila Cook Director of Diabetes & Endocrinology Toowoomba Hospital Let s consider the traditional diabetes clinic The Diabetes Clinic Whenever I check
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Patient empowerment and insulin titration
 Earn 3 CPD Points online Patient empowerment and insulin titration Introduction: Empowering patients to self-titrate Dr Ted Wu Endocrinologist Australia What is patient empowerment in insulin titration
Earn 3 CPD Points online Patient empowerment and insulin titration Introduction: Empowering patients to self-titrate Dr Ted Wu Endocrinologist Australia What is patient empowerment in insulin titration
Your Chart Review Data. Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine
 Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Your Chart Review Data Lara Zisblatt, MA Assistant Director Continuing Medical Education Boston University School of Medicine Participation 243 registered for the program 98 have completed the Practice
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes
 Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimal glucose control. DM Treatment. Glucose Control one out of many. Many guidelines: Confusing. Theorectically easy
 DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease
 Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease Authored by Paul Zimmet and Richard Nesto on behalf of the Global Partnership for Effective Diabetes Management.
Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease Authored by Paul Zimmet and Richard Nesto on behalf of the Global Partnership for Effective Diabetes Management.
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
Challenges in type 2 diabetes control: slipping control and weight gain
 control Earn 3 CPD Points online Case study Challenges in type 2 diabetes control: slipping control and weight gain Presenter Dr Sedeshan Govender Specialist Physician, Endocrinologist and Diabetologists
control Earn 3 CPD Points online Case study Challenges in type 2 diabetes control: slipping control and weight gain Presenter Dr Sedeshan Govender Specialist Physician, Endocrinologist and Diabetologists
BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH
 CHIEF OF MEDICINE, SOUTH WEST HEALTH") Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Intensification after basal insulin in type 2 diabetes
 Earn 3 CPD Points online Intensification after basal insulin in type 2 diabetes Introduction Professor Martin Pfohl Chief Physician Bethesda Hospital Duisburg, Germany It is vital to advise the type 2
Earn 3 CPD Points online Intensification after basal insulin in type 2 diabetes Introduction Professor Martin Pfohl Chief Physician Bethesda Hospital Duisburg, Germany It is vital to advise the type 2
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Mr Gavin Hendry. Mr Rab Burtun. Prof Jim Mann. Diabetes Nurse Facilitator, Auckland. Dunedin. Human Nutrition & Medicine University of Otago, Dunedin
 Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Case Study: Competitive exercise
 Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011
 DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards
DIABETES STRUCTURED EDUCATION IN WORCESTERSHIRE Information for Healthcare Professionals May 2011 What is Structured Education? Diabetes Structured Education is referred to in the Diabetes NSF standards
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Monitoring in Type 2 Diabetes. Learning Outcomes. Type 2 Diabetes. Senga Hunter Community Diabetes Specialist Nurse
 Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
More Than Just the Numbers:
 More Than Just the Numbers: Individualising Patient Care ADEA-QLD Branch Conference 20 April 2018 Case Study 1 Child with Type 1 Diabetes 2 Background and Social History 10 year old female with T1DM since
More Than Just the Numbers: Individualising Patient Care ADEA-QLD Branch Conference 20 April 2018 Case Study 1 Child with Type 1 Diabetes 2 Background and Social History 10 year old female with T1DM since
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Counting the Carbs, Fat and Protein in Type 1 Diabetes Translating the Research into Clinical Practice
 Welcome to Allied Health Telehealth Virtual Education Counting the Carbs, Fats and Protein in Type 1 Diabetes Translating the Research into Clinical Practice Dr Carmel Smart, PhD Senior Specialist Paediatric
Welcome to Allied Health Telehealth Virtual Education Counting the Carbs, Fats and Protein in Type 1 Diabetes Translating the Research into Clinical Practice Dr Carmel Smart, PhD Senior Specialist Paediatric
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
5/16/2018. Insulin Workshop. Disclosures to Participants. Learning Objectives. This presentation will cover the following learning objectives:
 Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Insulin Workshop Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA Holly Divine, PharmD, BCACP, BCGP, CDE,
Insulin and Post Prandial
 Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Insulin 301: Case, after case, after case
 Insulin 301: Case, after case, after case Learning objectives By the end of this session, you will be able to : 1. List the 3 types of insulin, 3 insulin regimens and pros/cons of each 2. Select the regimen
Insulin 301: Case, after case, after case Learning objectives By the end of this session, you will be able to : 1. List the 3 types of insulin, 3 insulin regimens and pros/cons of each 2. Select the regimen
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Diabetes mellitus. Treatment
 Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Diabetes mellitus Treatment Recommended glycemic targets for the clinical management of diabetes(ada) Fasting glycemia: 80-110 mg/dl Postprandial : 100-145 mg/dl HbA1c: < 6,5 % Total cholesterol: < 200
Insulin Therapy Management. Insulin Therapy
 Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Insulin Therapy Management Insulin Therapy Contents Insulin and its effect on glycemic control Physiology of insulin secretion Insulin pharmacokinetics and regimens Insulin dose adjustment for pregnancy
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Leicestershire Diabetes Guidelines: Insulin Therapy
 Endorsed by Leicestershire Medicines Strategy Group Leicestershire Diabetes Guidelines: Insulin Therapy These guidelines are designed for use by those trained and competent in insulin initiation and management
Endorsed by Leicestershire Medicines Strategy Group Leicestershire Diabetes Guidelines: Insulin Therapy These guidelines are designed for use by those trained and competent in insulin initiation and management
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
premix insulin and DPP-4 inhibitors what are the facts? New Sit2Mix trial provides first global evidence
 Earn 3 CPD Points online Using a premix insulin (BIAsp 30) with a DPP-4 inhibitor what are the facts? New Sit2Mix trial provides first global evidence An important trial using a premix insulin (BIAsp 30)
Earn 3 CPD Points online Using a premix insulin (BIAsp 30) with a DPP-4 inhibitor what are the facts? New Sit2Mix trial provides first global evidence An important trial using a premix insulin (BIAsp 30)
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Checking your. blood sugar. How frequent blood sugar checks can help you. When to check your blood sugar. Keeping a blood sugar tracker
 Checking your blood sugar How frequent blood sugar checks can help you Checking your blood sugar yourself is an important part of managing diabetes. Checking often will tell you: If your insulin or other
Checking your blood sugar How frequent blood sugar checks can help you Checking your blood sugar yourself is an important part of managing diabetes. Checking often will tell you: If your insulin or other
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Insulin use in Type 2 Diabetes
 Insulin use in Type 2 Diabetes 1 Conflict of Interest I have been on advisory boards or had speaker fees from the following pharmaceutical companies: - Eli Lilly - Novo Nordisk - Sanofi Aventis - MSD -
Insulin use in Type 2 Diabetes 1 Conflict of Interest I have been on advisory boards or had speaker fees from the following pharmaceutical companies: - Eli Lilly - Novo Nordisk - Sanofi Aventis - MSD -
Quick tips: initiating insulin in type 2 diabetes in primary care video 2 START AUDIO
 BMJ LEARNING VIDEO TRANSCRIPT Quick tips: initiating insulin in type 2 diabetes in primary care video 2 START AUDIO (Music) Martin Hadley-Brown: So usually when we re starting insulin, for someone with
BMJ LEARNING VIDEO TRANSCRIPT Quick tips: initiating insulin in type 2 diabetes in primary care video 2 START AUDIO (Music) Martin Hadley-Brown: So usually when we re starting insulin, for someone with
Dr Karen McNeil Consultant Endocrinologist
 Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Dr Karen McNeil Consultant Endocrinologist Aged 53 Type 2 Diabetes 2010 HbA1c 7.9% ACR 5.3 mg/mmol What treatment? MF 500 mg bd (misses midday dose) Control Symptoms, BGL Complications DR, DN, PN Associations
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Updated August /08/2020
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk
 Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Drug Therapy for Diabetes Mellitus. Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017
 Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Drug Therapy for Diabetes Mellitus Adj A/Prof Daniel Chew Dept of Endocrinology 8 th July 2017 Diabetes Subtypes Optimal Treatment Ominous Octet DeFronzo. DIABETES, VOL. 58, APRIL 2009 Schematic Overview
Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per
 4 times per") APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
28-Aug-15. RACGP guidelines 2014/15. ADS guidelines Part 1 T2D Guidelines. Part 2 What comes after metformin?
 Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi
Part 1 T2D Guidelines Oral therapies in T2 diabetes Dr Gary Kilov T2D Guidelines - What s New? What comes after metformin? 1 RACGP guidelines 2014/15 ADA-EASD: Anti-Hyperglycaemic therapy 2015 3 4 Inzucchi