HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT SEPTEMBER 2011 MELBOURNE, AUSTRALIA
|
|
|
- Sharyl Pitts
- 5 years ago
- Views:
Transcription


1 HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT SEPTEMBER 2011 MELBOURNE, AUSTRALIA

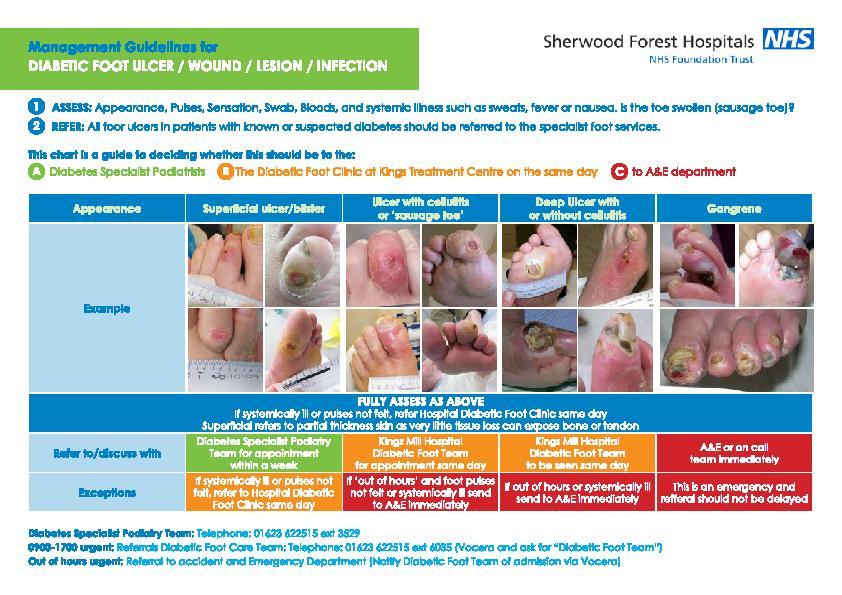
2 THE IMPACT OF A DECISION SUPPORT TOOL LINKED TO AN ELECTRONIC MEDICAL RECORD, ON GLYCAEMIC BURDEN IN PEOPLE WITH TYPE 2 DIABETES PROFESOR DEVAKA FERNANDO CONSULTANT ENDOCRINOLOGIST AND HONORARY PROFESSOR ASSOCIATE MEDICAL DIRECTOR SHERWOOD FOREST HOSPITALS NHS FOUNDATION TRUST 9/22/ Healthcare Information and Management Systems Society 2
3 The Clinical Problem Clinical Decision Support Systems The Evaluation 9/22/ Healthcare Information and Management Systems Society 3
4 High Cholesterol Excess food Genetics DM type 2 Heart Attacks Stroke Kidney failure Blindness Gout Lack of excercise Sociocultural factors High Blood Pressure Obesity The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997; 20 (7):
5 7-year incidence of cardiovascular events (%) High Risk of Cardiovascular Events in Type 2 Diabetes Myocardial infarction Stroke Cardiovascular deaths No diabetes Type 2 diabetes Prior myocardial infarction Haffner, NEJM 1998,
6 Rrisk of cardiovascular complications CVD risk based on diabetes duration 1,4 1,2 1 0,8 High risk 0,6 0, Diabetes Duration (years) VADT: ADA (2008) San Francisco and N Engl J Med (2009) 360:

7 Visceral adiposity is the basis of the metabolic syndrome The hidden effect of abdominal obesity

8
9 All other drugs 16% Oral antidiabetic agents 2% Primary care 11% In-patient care 41% NHS costs in Type 2 diabetes are mainly due to in-patient care Insulin 16% Outpatient care 14% Hospital costs: 55% 1. T 2 ARDIS. A satellite symposium at the BDA Annual Professional Conference, 2000.
10 World Health Organization, 2002 Non-modifiable Risk Factors Age Sex Genes BEHAVIOURAL RISK FACTORS Tobacco Diet Alcohol Physical Activity CVD, Risk Factors INTERMEDIATE RISK FACTORS Hypertension Diabetes Obesity ENDPOINTS Coronary heart disease Stroke Peripheral vascular disease Socio-economic, cultural & environmental factors
11 Tertiary care Industrial Age Secondary care Primary care Self care family/friends Information Age Self help networks Professional as teacher Professional as partner Professional as authority

12 Factors Influencing HbA1c GLYCATION 3 2 HEMOGLOBIN 4 1 ERYTHROPOIESIS ERYTHROCYTE DESTRUCTION 5 ASSAY Gallagher EJ, et al. J Diabetes. 2009;1:9-17.
13 Incidence per 1000 person-years (%) The relationship between glycaemia and the risk of complications in Type 2 diabetes MI Microvascular complications Mean HbA 1c concentration (%) Stratton IM et al. BMJ 2000; 321:
14 UKPDS: Tight Glycaemic Control Reduces Complications Epidemiological extrapolation showing benefit of a 1% reduction in mean HbA 1c HbA 1c 1% 21% 37% 14% Deaths related to diabetes * Microvascular complications e.g. kidney disease and blindness * Heart attack * * p< ** p=0.035 Stratton IM et al. UKPDS 35. BMJ 2000; 321: % 12% Amputation or fatal peripheral blood vessel disease * Stroke **
15 The Benefits of Early Tight Control- UKPDS 10 year Post-Trial Follow-Up Randomisation Intensive vs Conventional Treatment 10 yr Post Trial Follow Up (Non Interventional) 1997 (20 yrs) 2007 Trial End 1 (30 yrs) 2 Any diabetes related endpoint Microvascular disease Myocardial Infarction 12%* 9%* 16%*** 15%* 25%* 24%* *P<0.05 ***P= Unnikrishnan AG et al. UKPDS 33. Lancet, 1998: 352; Holman RR et al. UKPDS 80. NEJM (15):

16 Natural history of Type 2 diabetes: a progressive disease Insulin sensitive Normal Impaired glucose tolerance Type 2 diabetes Late Type 2 diabetes complications Normoglycaemia Hyperglycaemia Normal insulin secretion Insulin resistance β-cell exhaustion Insulin resistance Fasting plasma glucose Adapted from Bailey CJ et al. Int J Clin Pract 2004; 58: Insulin resistance
17 Pathophysiology of diabetes complications Activation of oxidative stress Glucose fluctuations (MAGE) Activation of oxidative stress Risk of complications PPG FPG HbA 1 c (glycation) L Monnier, C Colette. Diabetes Care 2008; 31: S
18 Problem Type 2 Diabetes Which Blood Glucose level Contributes most glucose PP-glucose Fasting glucose Blood glucose NGT Normal Glucosetolerance IFG IGT IFG IGT Diabetes modified from DeFronzo RA et al., Diabetes Care 1998
19
20 HbA 1c (%) Initiation of diet and exercise Total glycaemic burden the need for improved intervention Initiation of monotherapy Additional intervention Time since diagnosis Glycaemic burden 6 Adapted from Brown JB et al. Diabetes Care 2004; 27:
21 HbA 1c (%) Diet A conservative target-based approach 8.5 OAD monotherapy OAD combination OAD combination up-titration OAD + insulin 8 Glycaemic burden Target HbA 1c 6 Time since diagnosis 6 Adapted from Campbell IW. Br J Cardiol 2000; 7:
22 What could an early, intensive, target-based approach achieve? 10 Diet 9 Monotherapy Combination therapy 8 7 Target HbA 1c 6 Time since diagnosis
23 Treatment summary Newly Newly diagnosed Type Type 2 2 diabetes Lifestyle modification Lifestyle modification Diet Diet Physical activity Physical activity Smoking cessation Smoking cessation Test HbA 1c 3 months after initial diagnosis STEP 1 Start Metformin Titrate to maximal tolerated dose or if: unable to tolerate metformin metformin contraindicated Use an insulin sensitiser ( (glitazone) or Use a sulphonylurea *** STEP 2 Add Add an an insulin sensitiser Particularly if BMI if BMI > 27 > 27 or add a sulphonylurea * or post - prandial glucose regulator* ** STEP 3 Add additional oral hypoglycaemic agents or convert to insulin therapy* +/ - oral agent Test HbA 1c 3 months after initial diagnosis Review Review patient patient every every months If HbA If HbA 1c 1c remains > 7% > 7% move move on on to the to the next next treatment step step Diet and exercise Blood pressure and lipid management * Clinicians should be alert to the risk of hypoglycaemia with ins ulin, sulphonylureasand post - prandialglucose regulators Post - prandialglucose regulators may be of particular use in patients with no n-routine daily patterns *Clinicians Acarbosemay should be be considered alert to the as an risk alternative of hypoglycaemia agent in patients with insulin, unable sulphonylurea to use and other post-prandial oral therapies. glucose regulators Insulin sensitisersare not licensed for triple therapy or in combination with insulin **Post-prandial glucose regulators may be of particular use in patients with non-routine daily patterns Acarbose may be considered as an alternative agent in patients unable to use other oral therapies. Insulin sensitisers are not licensed in combination with insulin
24 High risk approach Population approach Risk factor distribution Identify and treat those beyond a threshold for risk factor Resource intensive Screening necessary Provable in RCT Large effect in small number of people Risk factor distribution Shift the whole population distribution of risk factor lower Less resource intensive Less amenable to RCT No spec. need to identify high risk subjects Small effect in large number of people
25 Managing diabetes is neither an art nor a science but an interpretive practice with the patient at its core. It draws on science to inform reasoning but practice of medicine cannot be a universally replicable, invariant process.
26 The clinical Problem Complex Disorder Many contributing variables Treatment needs to be individualised and not one size fits all Increasing frequency Specialist care too expensive. Training Generalists to critical knowledge and skill base takes time. 9/22/ Healthcare Information and Management Systems Society 26
27 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? How can they be put to use? Do they work?
28 Decision Support Systems Decision support systems are a class of computer-based information systems including knowledge based systems that support decision making activities. -Wikipedia
29 Clinical Decision Support Systems Employing a knowledge base Used by a clinician Involved in patient care Direct aid to clinical decision making
30 Clinical Decision Support Systems Knowledge-based tools Fully integrated with both the clinician workflow components of a computerized patient record Repository of complete and accurate data
31 Clinical Decision Support Systems : Clinician and Patient-related information Presented at appropriate times
32 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? How can they be put to use? Do they work?
33 Why do we need them? Increasing need to keep up to-date Millions of facts needed to practice. Covell DG, Annals of Intern Med Oct;103(4):596-9
34 Why do we need them? A single prescription requires adjustment for: Age Weight Height Kidney function Liver function Results of lab tests Concurrent use of other medicines Patient history of allergies Co existing health conditions
35 Case History: 48 year old Patient with a BMI of 37, type 2 diabetes who has had diabetes for 15 years and has impaired kidney function and nerve damage and has had a heart attack last year. Current tablets are not working and he has poor blood glucose control HBA1c 10%. Which medication?
36 Clinical Coding used to assess quality Data Entry The process Written Clinical Record Refer Clinical Guideline protocol Or Take History Examine Take History Examine Refer Clinical guideline or protocol Data Entry Electronic Health Records Ask expert by phone Decision Support Integration Better Practice




37
38 38 Clinical decision support Gives clinicians, patients, and others relevant information in context, that helps them make better decisions, prevent errors, and improve care quality and outcomes CDS interventions include guidelines, alerts, order sets, tools to interpret patient data
39
40 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? Do they work? How can they be put to use?
41 Do They work? Evidence? Facilitating use of Guidelines and Management Protocols? Prescribing Protocol based care Referral Diagnosis? 9/22/ Healthcare Information and Management Systems Society 41

42 Better care for diabetes in the VA system than for patients in commercial managed care. Annals of Internal Medicine, August 17, 2004
43 Benefits of integration with Electronic Medical Record Improve healthcare outcomes Real time decision support for clinicians at point of care reminders, alerts Avoid reliance on memory, clinician vigilance Reduce errors (omissions, transcriptions, etc) Facilitate documentation for performance measurement and improvement efforts
44 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? Do they work? How can they be put to use?
45 Types of Decision Support Systems Informative Guidelines Literature search Triggers and warnings Guidance and advice
46 Decision Support Systems: how do they interact with user? Passive decision support: make information available when specifically requested Active decision support: process information and interact with clinical data Co-operative: user interface
47 1. Trigger Components of active decision support 2. Output 3. Relevant Data available in the system
48 Active decision support: The medication list you generated is a repeat prescription Her current Glycaemic Burden is.. Glycaemic burden displayed graphically Please list reason for exclusion from treatment to target glycaemic control Dialogue box
49 Clinical Reminders 1. Direct Patient care Real time decision support Targeted to specific patient Targeted to specific clinician Patient recall if missed intervention 2. Clinical Governance Performance improvement feedback against benchmarks Reports for appraisal documentation Targeting outlier clinicians for educational intervention
50 Clinical Reminders 2 Administrative Reminder Reports related to Patient care: Future Appointments Which patients need an intervention (medication change, referral)? Past Visits Which patients missed an intervention? Action Lists - What results need review and action?
51 Clinical Reminder Reports Identify patients for case management People with Diabetes who have poor glycaemic, blood Pressure control Identify patients with incomplete task completion lists (especially non medic actions) Identify high risk patients needing frequent intervention Identify low risk patients for discharge to primary care Track annual review.
52 The setting


53
54 Telemedicine The module permits a tele-medicine consultation through , video images and data, to enable specialist interpretation and expert advice from specialists based in the UK.

55
56 E-education The Network enhances and supports the ongoing educational collaboration that exists between the University in Sri Lanka, Teaching Hospital Kandy, Teaching Hospital Peradeniya, Endocrine Metabolic Disease Trust, Sheffield Hallam University and the Sherwood Forest Hospitals NHS Trust.
57
58 The Clinical Problem Clinical Decision Support Systems The Evaluation 9/22/ Healthcare Information and Management Systems Society 58
59 Safety Testing As to disease, make a habit of two things to help, or at least do no harm- Hippocrates, Epidemics (book I Chapter XI) c 400 BC Medicine used to be simple, ineffective and relatively safe. It is now complex, effective and potentially dangerous. 9/22/ Healthcare Information and Management Systems Society 59
60 Safety Testing Health Informatics Before disseminating any biomedical information resource designed to influence real-world practice decisions check that it is safe Friedman and Wyatt Evaluation Methods in Biomedical Informatics 2006
61 Meeting the Challenge A work in progress Design and re-designing the system after input from key stakeholders Pre tests offline Pilots tested with early physician adopters Later tested with typical users (early adopters at pilot stage excluded from analysis)
62 Stages in Evaluating Clinical Decision Support Systems (CDSS) Eval Type Explore Feasibility, Reliability, safety informally More Formal Test of components Tests in Actual use; External reviewers Large Clinical trial,? RCT Postimplementation surveillance Stage Early Design And development Intermed Development More Mature System Wider Implementation
63 Benefits of the Offline Testing Offline testing successful in identifying errors Knowledge base Updates made before deployment
64 Comparison Method Comparing CDSS vs Clinician decision: Comparison for discrepancies in instructions / advice Manual review of all cases Reviewing discrepancies Review by specialist clinician panel
65 Stages in Evaluating Clinical Decision Support Systems Eval Type Explore Feasibility, Reliability, safety informally More Formal Test of components Tests in Actual use; External reviewers Large Clinical trial,? RCT Post- Implementation surveillance Stage Early Design And develop Intermed Development More Mature System Wider Implementation
66 Evaluator General Physician with experience in treating diabetes in primary care setting No previous involvement with EMR or CDSS project Guidelines available during evaluation of test cases
67 CDSS Methods Clinician EMR Electronic patient data: Test cases Clinician + Rules System recommendations Comparison Clinician recommendations
68 Stages in Evaluating Clinical Decision Support Systems Eval Type Explore Feasibility, Reliability, Safety informally More Formal Test of Components Tests in Actual use; External reviewers Large Clinical trial,? RCT Post- Implementation surveillance Stage Early Design And Develop Intermed Development More Mature System Wider Implementation
69 HbA 1c (%) Initiation of diet and exercise Total glycaemic burden the need for improved intervention Initiation of monotherapy Additional intervention Time since diagnosis Glycaemic burden 6 Adapted from Brown JB et al. Diabetes Care 2004; 27:

70 HbA 1c (%) Diet A conservative target-based approach 8.5 OAD monotherapy OAD combination OAD combination up-titration OAD + insulin 8 Glycaemic burden Target HbA 1c 6 Time since diagnosis 6 Adapted from Campbell IW. Br J Cardiol 2000; 7:
71 What could an early, intensive, target-based approach achieve? 10 Diet 9 Monotherapy Combination therapy 8 7 Target HbA 1c 6 Time since diagnosis
72 Glycaemic burden before and after specialist supported Observed HBa1c -7.5 intermediate care Without Consultant Support Community Based Consultant and DSN 0-0.5
73 Observed HBa1c -7.5 Impact on Glycaemic Burden using a clinical decision support system in patients discharged from specialist care With Decision support Without Decision support Time (months)
74 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? How can they be put to use? Do they work? What can de done to make this one work in a wider environment?
75 What is needed to successfully implement CDSS in a health community? Best knowledge made available when needed at clinician patient encounter. High adoption rate in health care community. Effective use by clinicians and patients Continuous Improvement through a governance mechanism (Industry may regard this as regulatory) 9/22/ Healthcare Information and Management Systems Society 75
76 Implementing an integrated CDSS Management team Informatics department Awareness Acceptance Adoption Adherence Present research data and Baseline audits of performance against benchmarks Clinician education and training Ensuring concordance with clinic workflow Audit, Evaluation Governance Improving access to clinical and research resources Present evidence relevant to patient care and facilitate clinicians access to knowledge base Integration with EMR Point-of-care patient-specific guidance in convenient clinician friendly format.
77 Next Stage Eval Type Explore Feasibility, Reliability, safety informally More Formal Test of components Tests in Actual use; External reviewers Large Clinical trial,? RCT Post- Implementation surveillance Stage Early Design And develop Intermed Development More Mature System Wider Implementation
78 Clinical Decision Support Systems What are Clinical decision support systems? Why do we need them? How can they be put to use? Do they work? What can de done to make this one work in a wider environment? Is there a role for National and International Organisations?
79 79 Is there a role for National and International Organisations? Ensure availability of standard clinically acceptable formats for representing CDS knowledge and interventions Ensure availability of communitywide approaches to procuring and distributing CDS Ensure availability of methods to remove or mitigate against policy, legal and financial barriers to implementation. Ensure availability of best practice guidance for implementation Ensure availability of standards and a process to collect data on, learn from, and share national CDS experience Ensure availability of a system to use EHR data systematically to advance knowledge through validated health service research methods

80 Georges Clemenceau French journalist, physician and statesman. He served as Prime Minister from 1906 to 1909 and from 1917 to War is too serious a matter to entrust to military men. Health Informatics?
81 THANK YOU DEVAKA FERNANDO 9/22/ Healthcare Information and Management Systems Society 81
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes
 PRESS RELEASE Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes Dublin, Ireland (15 June 2012) Sanofi presented results
PRESS RELEASE Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes Dublin, Ireland (15 June 2012) Sanofi presented results
04-Sep-17. INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification
 PROF MERLIN THOMAS DIAttitude Study INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification 13% immediately 41% of patients
PROF MERLIN THOMAS DIAttitude Study INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification 13% immediately 41% of patients
= AUDIO. Managing Diabetes for Improved Cardiovascular Health. An Important Reminder. Mission of OFMQ 8/18/2015. Jimmi Norris MS, RN, CDE
 Managing Diabetes for Improved Cardiovascular Health Jimmi Norris MS, RN, CDE An Important Reminder For audio, you must use your phone: Step 1: Call (866) 906 0123. Step 2: Enter code 2071585#. Step 3:
Managing Diabetes for Improved Cardiovascular Health Jimmi Norris MS, RN, CDE An Important Reminder For audio, you must use your phone: Step 1: Call (866) 906 0123. Step 2: Enter code 2071585#. Step 3:
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Welcome and Introduction
 Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Diabetes Mellitus Aeromedical Considerations. Aviation Medicine Seminar Bucharest, Romania. 11 th to 15 th November 2013
 Diabetes Mellitus Aeromedical Considerations Aviation Medicine Seminar Bucharest, Romania. 11 th to 15 th November 2013 Metabolic, Nutritional or Endocrine disorders Applicants with metabolic, nutritional
Diabetes Mellitus Aeromedical Considerations Aviation Medicine Seminar Bucharest, Romania. 11 th to 15 th November 2013 Metabolic, Nutritional or Endocrine disorders Applicants with metabolic, nutritional
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE. Type 2 diabetes: the management of type 2 diabetes (update)
") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Type 2 diabetes: the management of type 2 diabetes (update) 1.1 Short title Type 2 diabetes (update) 2 Background a) The National
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Type 2 diabetes: the management of type 2 diabetes (update) 1.1 Short title Type 2 diabetes (update) 2 Background a) The National
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
WILL YOU USE HBA1C TO SCREEN & MONITOR DIABETES? Dr. Amany Mousa
 WILL YOU USE HBA1C TO SCREEN & MONITOR DIABETES? Dr. Amany Mousa Diabetes is clinically well defined by glycation of proteins 1. True 2. false So far, diabetes has been defined as a clinical condition
WILL YOU USE HBA1C TO SCREEN & MONITOR DIABETES? Dr. Amany Mousa Diabetes is clinically well defined by glycation of proteins 1. True 2. false So far, diabetes has been defined as a clinical condition
UK launch of once-daily tablet from Janssen provides new option to improve blood glucose control for thousands of people with Type 2 diabetes 1
 PRESS RELEASE 24 th February, 2014 UK launch of once-daily tablet from Janssen provides new option to improve blood glucose control for thousands of people with Type 2 diabetes 1 London, 24 February 2014
PRESS RELEASE 24 th February, 2014 UK launch of once-daily tablet from Janssen provides new option to improve blood glucose control for thousands of people with Type 2 diabetes 1 London, 24 February 2014
Glucose Control: Does it lower CV risk?
 Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
The United Kingdom Prospective
 Professional issues The UKPDS: a nursing perspective Marilyn Gallichan Article points 1The UKPDS followed up more than 5000 patients from 23 centres for a median of 10 years. 2The findings provide a powerful
Professional issues The UKPDS: a nursing perspective Marilyn Gallichan Article points 1The UKPDS followed up more than 5000 patients from 23 centres for a median of 10 years. 2The findings provide a powerful
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Diabetes Prevention & Management of Complications
 Diabetes Prevention & Management of Complications Dr Ketan Dhatariya Consultant in Diabetes and Endocrinology NNUH The Planet is Changing IFCC (mmol/mol) = (current value (%) * 10.93) - 23.50 (reported
Diabetes Prevention & Management of Complications Dr Ketan Dhatariya Consultant in Diabetes and Endocrinology NNUH The Planet is Changing IFCC (mmol/mol) = (current value (%) * 10.93) - 23.50 (reported
Diabetes Mellitus Type 2 Evidence-Based Drivers
 This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Information for people with diabetes. diabetes. glossary of. terms
 Information for people with diabetes i diabetes glossary of terms Diabetes is a common condition, which most people have some understanding of, but when you listen to people talk about it, you may feel
Information for people with diabetes i diabetes glossary of terms Diabetes is a common condition, which most people have some understanding of, but when you listen to people talk about it, you may feel
QOF Indicator DM013:
 QOF Indicator DM013: The percentage of patients with diabetes, on the register, who have a record of a dietary review by a suitably competent professional in the preceding 12 months Note: the bold signposts
QOF Indicator DM013: The percentage of patients with diabetes, on the register, who have a record of a dietary review by a suitably competent professional in the preceding 12 months Note: the bold signposts
Team-Based Decision Support in Diabetes Outcomes and Costs
 Team-Based Decision Support in Diabetes Outcomes and Costs Session 89, 8:30 a.m. February 13, 2019 Gary Ozanich, Ph.D. - College of Informatics, Northern Kentucky University 1 Conflict of Interest Gary
Team-Based Decision Support in Diabetes Outcomes and Costs Session 89, 8:30 a.m. February 13, 2019 Gary Ozanich, Ph.D. - College of Informatics, Northern Kentucky University 1 Conflict of Interest Gary
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Why Do We Care About Prediabetes?
 Why Do We Care About Prediabetes? Complications of Diabetes Diabetic Retinopathy Leading cause of blindness in adults 1,2 Diabetic Nephropathy Leading cause of Kidney failure Stroke 2- to 4-fold increase
Why Do We Care About Prediabetes? Complications of Diabetes Diabetic Retinopathy Leading cause of blindness in adults 1,2 Diabetic Nephropathy Leading cause of Kidney failure Stroke 2- to 4-fold increase
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181)
") Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Long-Term Care Updates
 Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
The DIABETES CHALLENGE IN PAKISTAN FIFTH NATIONAL ACTION PLAN
 1. INTRODUCTION The DIABETES CHALLENGE IN PAKISTAN FIFTH NATIONAL ACTION PLAN 2014 2018 UNITE AGAINST DIABETES STOP RISING TREND Diabetes is a significant and growing challenge globally that affects individuals,
1. INTRODUCTION The DIABETES CHALLENGE IN PAKISTAN FIFTH NATIONAL ACTION PLAN 2014 2018 UNITE AGAINST DIABETES STOP RISING TREND Diabetes is a significant and growing challenge globally that affects individuals,
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
EFFECTIVE SHARE CARE AGREEMENT. FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY
 Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
Barns Medical Practice Service Specification: Diabetes
 Barns Medical Practice Service Specification: Diabetes DEVELOPED June 2017 REVIEW DATE June 2019 Introduction Diabetes mellitus is a life-long progressive condition that can be controlled but not cured.
Barns Medical Practice Service Specification: Diabetes DEVELOPED June 2017 REVIEW DATE June 2019 Introduction Diabetes mellitus is a life-long progressive condition that can be controlled but not cured.
Evidence Briefing for NHS Bradford and Airedale. Physical health monitoring for people with schizophrenia or other serious mental illness
 Evidence Briefing for NHS Bradford and Airedale Physical health monitoring for people with schizophrenia or other serious mental illness The NICE clinical guideline on schizophrenia 1 recommends that GPs
Evidence Briefing for NHS Bradford and Airedale Physical health monitoring for people with schizophrenia or other serious mental illness The NICE clinical guideline on schizophrenia 1 recommends that GPs
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Technology appraisal guidance Published: 26 June 2013 nice.org.uk/guidance/ta288
 Dapagliflozin in combination therapy for treating type 2 diabetes Technology appraisal guidance Published: 26 June 2013 nice.org.uk/guidance/ta288 NICE 2018. All rights reserved. Subject to Notice of rights
Dapagliflozin in combination therapy for treating type 2 diabetes Technology appraisal guidance Published: 26 June 2013 nice.org.uk/guidance/ta288 NICE 2018. All rights reserved. Subject to Notice of rights
National Paediatric Diabetes Audit
 National Paediatric Diabetes Audit Parent and Carers Report 2014-15 Commissioned by the Healthcare Quality Improvement Partnership Managed by the Royal College of Paediatrics and Child Health 2 National
National Paediatric Diabetes Audit Parent and Carers Report 2014-15 Commissioned by the Healthcare Quality Improvement Partnership Managed by the Royal College of Paediatrics and Child Health 2 National
Isolated Post-challenge Hyperglycemia: Concept and Clinical Significance
 CLINICAL PRACTICE Isolated Post-challenge Hyperglycemia: Concept and Clinical Significance John MF. Adam*, Daniel Josten** ABSTRACT The American Diabetes Association has strongly recommended that fasting
CLINICAL PRACTICE Isolated Post-challenge Hyperglycemia: Concept and Clinical Significance John MF. Adam*, Daniel Josten** ABSTRACT The American Diabetes Association has strongly recommended that fasting
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Horizon Scanning Technology Summary. Liraglutide for type 2 diabetes. National Horizon Scanning Centre. April 2007
 Horizon Scanning Technology Summary National Horizon Scanning Centre Liraglutide for type 2 diabetes April 2007 This technology summary is based on information available at the time of research and a limited
Horizon Scanning Technology Summary National Horizon Scanning Centre Liraglutide for type 2 diabetes April 2007 This technology summary is based on information available at the time of research and a limited
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE. AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY. sul Paziente ad alto rischio CV*
 CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
COMMUNITY HEALTH NEEDS ASSESSMENT IMPLEMENTATION STRATEGY
 2016 COMMUNITY HEALTH NEEDS ASSESSMENT IMPLEMENTATION STRATEGY Table of Contents Introduction... 2 Executive summary... 2 University Care System s mission, vision, and values... 2 Description of the health
2016 COMMUNITY HEALTH NEEDS ASSESSMENT IMPLEMENTATION STRATEGY Table of Contents Introduction... 2 Executive summary... 2 University Care System s mission, vision, and values... 2 Description of the health
Moving to an A1C-Based Screening & Diagnosis of Diabetes. By Prof.M.Assy Diabetes&Endocrinology unit
 Moving to an A1C-Based Screening & Diagnosis of Diabetes By Prof.M.Assy Diabetes&Endocrinology unit is the nonenzymatic glycated product of the hemoglobin beta-chain at the valine terminal residue. Clin
Moving to an A1C-Based Screening & Diagnosis of Diabetes By Prof.M.Assy Diabetes&Endocrinology unit is the nonenzymatic glycated product of the hemoglobin beta-chain at the valine terminal residue. Clin
Diabetes. Ref HSCW 024
 Diabetes Ref HSCW 024 Why is it important? Diabetes is an increasingly common, life-long, progressive but largely preventable health condition affecting children and adults, causing a heavy burden on health
Diabetes Ref HSCW 024 Why is it important? Diabetes is an increasingly common, life-long, progressive but largely preventable health condition affecting children and adults, causing a heavy burden on health
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME QOF indicator area: Diabetes Briefing paper Potential output: Recommendations
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME QOF indicator area: Diabetes Briefing paper Potential output: Recommendations
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Community Based Diabetes Prevention
 Community Based Diabetes Prevention Melanie Davies Professor of Diabetes Medicine Outline NIHR Programme Grant proposal and update to progress The Vascular Check programme HbA1c debate Algorithm to detect
Community Based Diabetes Prevention Melanie Davies Professor of Diabetes Medicine Outline NIHR Programme Grant proposal and update to progress The Vascular Check programme HbA1c debate Algorithm to detect
Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease
 Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease Authored by Paul Zimmet and Richard Nesto on behalf of the Global Partnership for Effective Diabetes Management.
Case study: Adult with uncontrolled type 2 diabetes of long duration and cardiovascular disease Authored by Paul Zimmet and Richard Nesto on behalf of the Global Partnership for Effective Diabetes Management.
Pre-diabetes. Dr Neel Basudev. GPSI Lambeth DICT, Diabetes Lead Lambeth CCG
 Pre-diabetes Dr Neel Basudev GPSI Lambeth DICT, Diabetes Lead Lambeth CCG The Prevention of Diabetes Where has this come from? Pre-diabetes mellitus (PDM) Term introduced by Tommy G. Thompson (Health &
Pre-diabetes Dr Neel Basudev GPSI Lambeth DICT, Diabetes Lead Lambeth CCG The Prevention of Diabetes Where has this come from? Pre-diabetes mellitus (PDM) Term introduced by Tommy G. Thompson (Health &
Diabetes: Staying Two Steps Ahead. The prevalence of diabetes is increasing. What causes Type 2 diabetes?
 Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
Focus on CME at the University of University Manitoba of Manitoba : Staying Two Steps Ahead By Shagufta Khan, MD; and Liam J. Murphy, MD The prevalence of diabetes is increasing worldwide and will double
In keeping with the Scottish Diabetes Group criteria, use should be restricted to those who:
 Advice Statement 009-18 July 2018 Advice Statement What is the clinical and cost effectiveness of Freestyle Libre flash glucose monitoring for patients with diabetes mellitus treated with intensive insulin
Advice Statement 009-18 July 2018 Advice Statement What is the clinical and cost effectiveness of Freestyle Libre flash glucose monitoring for patients with diabetes mellitus treated with intensive insulin
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Optimizing Postpartum Maternal Health to Prevent Chronic Diseases
 Optimizing Postpartum Maternal Health to Prevent Chronic Diseases Amy Loden, MD, FACP, NCMP Disclosures Research: None Financial: none applicable to this presentation PRIUM QEssentials Market Research
Optimizing Postpartum Maternal Health to Prevent Chronic Diseases Amy Loden, MD, FACP, NCMP Disclosures Research: None Financial: none applicable to this presentation PRIUM QEssentials Market Research
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home
 Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes
 HARVARD MEDICAL SCHOOL How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes Richard W. Grant MD MPH Endocrine Society Beta Cell meeting January 9-10, 2009 Outline Background Observed
HARVARD MEDICAL SCHOOL How Doctors Choose Medicines when Treating Patients with Type 2 Diabetes Richard W. Grant MD MPH Endocrine Society Beta Cell meeting January 9-10, 2009 Outline Background Observed
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar. Simon Kane March 2016
 GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar Simon Kane March 2016 Objectives History and definitions Definition and Australian data Pathophysiology and prevalence Rationale
GESTATIONAL DIABETES for GP Obstetric Shared Care Accreditation Seminar Simon Kane March 2016 Objectives History and definitions Definition and Australian data Pathophysiology and prevalence Rationale
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Pre-diabetes: Information for primary care practitioners
 Pre-diabetes: Information for primary care practitioners Michelle Barker 2005 Important Messages This booklet is based on three key messages for patients. 1. Pre-diabetes is a serious condition with a
Pre-diabetes: Information for primary care practitioners Michelle Barker 2005 Important Messages This booklet is based on three key messages for patients. 1. Pre-diabetes is a serious condition with a
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
What if we could prescribe information that supported patients to understand and own their diabetes?
 Briefing Paper Project Information Prescriptions Date /0/05 From Amy Rylance, Head of Healthcare Professional Engagement Page of Introduction: Our Reaching People with Diabetes through Healthcare Professionals
Briefing Paper Project Information Prescriptions Date /0/05 From Amy Rylance, Head of Healthcare Professional Engagement Page of Introduction: Our Reaching People with Diabetes through Healthcare Professionals
NICE offer to STPs: CVD prevention
 NICE offer to STPs: CVD prevention Zoe Girdis Regional Technical Adviser South of England and Channel Islands NICE support for STPs Based on the best available evidence of what works and is costeffective,
NICE offer to STPs: CVD prevention Zoe Girdis Regional Technical Adviser South of England and Channel Islands NICE support for STPs Based on the best available evidence of what works and is costeffective,
Copyright 2017 by Sea Courses Inc.
 Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
NICE Indicator Programme. Consultation on proposed amendments to current QOF indicators
 NICE Indicator Programme Consultation on proposed amendments to current QOF s Consultation dates: 18 July to 1 August 2018 This document outlines proposed amendments to a small number of QOF s in the diabetes
NICE Indicator Programme Consultation on proposed amendments to current QOF s Consultation dates: 18 July to 1 August 2018 This document outlines proposed amendments to a small number of QOF s in the diabetes
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes
 in combination with basal insulin for type 2 diabetes") Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Liraglutide (Victoza) in combination with basal insulin for type 2 diabetes May 2011 This technology summary is based on information available at the time of research and a limited literature search. It
Metformin is the only drug. Sustained release metformin where standard metformin is not tolerated. Julie Brake
 Sustained release metformin where standard metformin is not tolerated Julie Brake Article points 1. Few people will continue taking medication while experiencing side effects. 2. Hypoglycaemia does not
Sustained release metformin where standard metformin is not tolerated Julie Brake Article points 1. Few people will continue taking medication while experiencing side effects. 2. Hypoglycaemia does not
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes
 Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
GUIDELINES FOR DYSLIPIDEMIA MANAGEMENT AND EDUCATION THROUGH NOVA SCOTIA DIABETES CENTRES
 GUIDELINES FOR DYSLIPIDEMIA MANAGEMENT AND EDUCATION THROUGH NOVA SCOTIA DIABETES CENTRES Prepared by DCPNS Action Committee Dr. Lynne Harrigan Brenda Cook Peggy Dunbar Bev Harpell with the assistance
GUIDELINES FOR DYSLIPIDEMIA MANAGEMENT AND EDUCATION THROUGH NOVA SCOTIA DIABETES CENTRES Prepared by DCPNS Action Committee Dr. Lynne Harrigan Brenda Cook Peggy Dunbar Bev Harpell with the assistance