Glucose and CV disease
|
|
|
- Lester Robinson
- 5 years ago
- Views:
Transcription
1 Glucose and CV disease
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.

3
4
5
6 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
7 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
8


9 Diabetes-related complications in the USA, Acute myocardial infarction Adapted from Gregg EW, et al. N Engl J Med 2014;370: Presented at the American Diabetes Association 76 th Scientific Sessions, Session 3-CT-SY24. June , New Orleans, LA, USA.
10
11
12 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
13 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
14 Relative Risk A1C and Relative Risk of Microvascular Complications: DCCT Retinopathy Nephropathy Neuropathy Microalbuminuria A1C (%) DCCT, Diabetes Control and Complications Trial. 1. Adapted from Skyler JS. Endocrinol Metab Clin North Am. 1996;25: DCCT. N Engl J Med. 1993;329: DCCT. Diabetes. 1995;44:
15

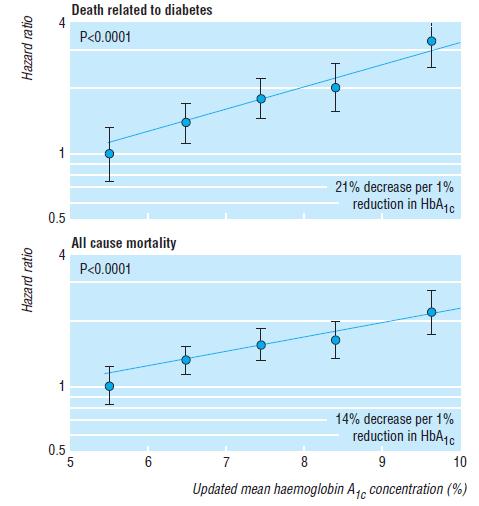
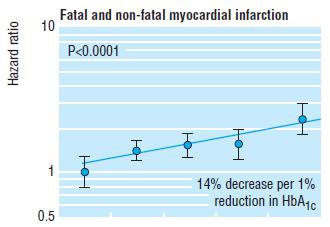
16 HbA1c predicts Coronary Heart Disease in Type 2 Diabetics 17
 Adjusted for age, sex, and ethnic group Stratton IM et al. BMJ 2000;321:405-412. Slide Source: ukpds Lipids Online www.lipidsonline.")
17 Incidence per 1000 Person Years (%) Incidence Rates of MI and Microvascular Endpoints by Mean Hemoglobin A 1c : UKPDS Myocardial Infarction 20 0 Microvascular Endpoints Updated Mean Hemoglobin A 1c Concentration (%) Adjusted for age, sex, and ethnic group Stratton IM et al. BMJ 2000;321: Slide Source: ukpds Lipids Online
18 2008
19
20 CV Death, MI, or Ischemic Stroke Rate of CVD, MI, or Ischemic Stroke Increases as Baseline HbA1c Increases* 12 Adj HR (95% CI) 10 9% 1.76 (1.48, 2.11) %-<9% 7%-<8% <7% 1.37 (1.14, 1.65) 1.14 (0.96, 1.35) Reference Months *Adjusted for age, gender, duration of DM, glomular filtration rate (GFR), established atherosclerosis vs primary prevention, and microalbumin:creatinine ratio (malb:cr) Cavender, MA, et al. American Heart Association Scientific Sessions. November 2013, data from SAVOR 21
21 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
22 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
23 DCCT: Reduction in Retinopathy NEJM Volume 329: Number 14;
24 DCCT: Reduction in Albuminuria Primary Prevention Secondary Intervention 34% RRR (p<0.04) 43% RRR (p=0.001) 56% RRR (p=0.01) Solid line = risk of developing microalbuminuria Dashed line = risk of developing macroalbuminuria RRR = relative risk reduction CI = confidence interval The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329: guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association ukpds
25 DCCT: Reduction in neuropathy The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329: ukpds

26 ukpds

27 Does tighter glycemic control offer CV benefits?
28 Cumulative incidence of non-fatal MI, stroke or death from CVD HbA 1C (%) DCCT/EDIC: glycaemic control reduces the risk of non-fatal MI, stroke or death from CVD in type 1 diabetes 9 Conventional treatment 8 Intensive treatment DCCT (intervention period EDIC (observational follow-up) Years % risk reduction in non-fatal MI, stroke or CVD death* (P = 0.02; 95% CI: 12 79%) Intensive treatment Conventional treatment 0.00 *Intensive vs conventional treatment DCCT (intervention period) EDIC (observational follow-up) Years Adapted from DCCT. N Engl J Med 1993; 329: DCCT/EDIC. JAMA 2002; 287: DCCT/EDIC. N Engl J Med 2005; 353:
29 3 major studies that are referred to, ADVANCE, ACCORD, VADT to provide answers All studies of Intensive glucose control vs looser glucose control All were in very high risk patients who had their diabetes for 8-11 years Either had documented vascular disease or Very high risk based on risk factors
30 3 major studies that are referred to, ADVANCE, ACCORD, VADT to provide answers All studies of Intensive glucose control vs looser glucose control All were in very high risk patients who had their diabetes for 8-11 years Either had documented vascular disease or Very high risk based on risk factors
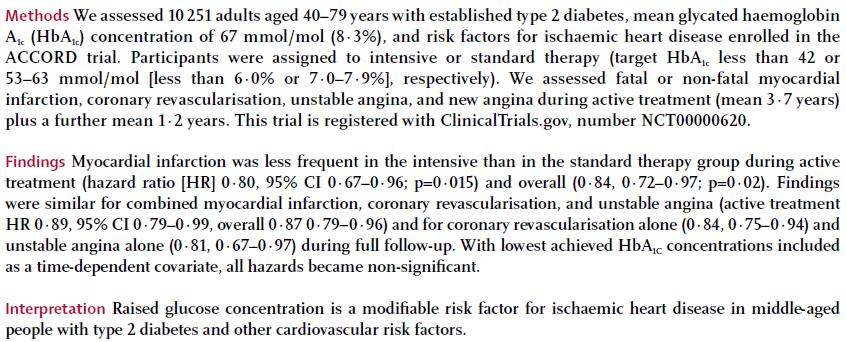
31 ACCORD 10,251 pts with T2DM + CV risk Average diabetes duration 10 yrs Median baseline A1c = 8.1% Intensive target <6.0% (actual 6.4%) Standard target 7-7.9% (actual 7.5%)
32 Mean A1c 7.5% Mean A1c 6.4%
33 Non-fatal MI, non-fatal CVA, death from CV causes ACCORD: Mean A1c 7.5% Mean A1c 6.4%
34 We ll discuss at much greater length HR 1.22, p =.04
35
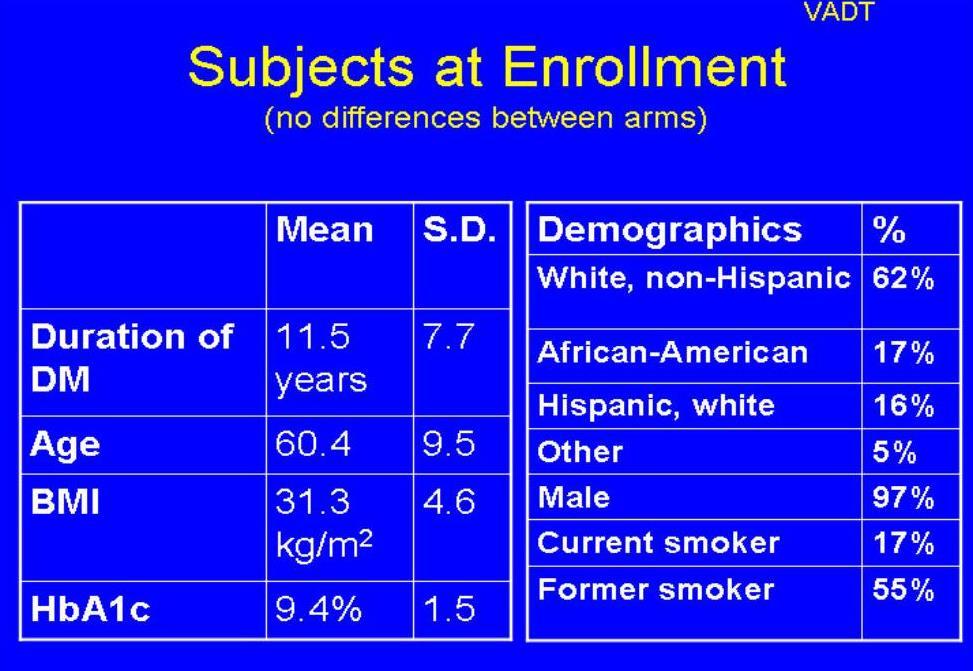
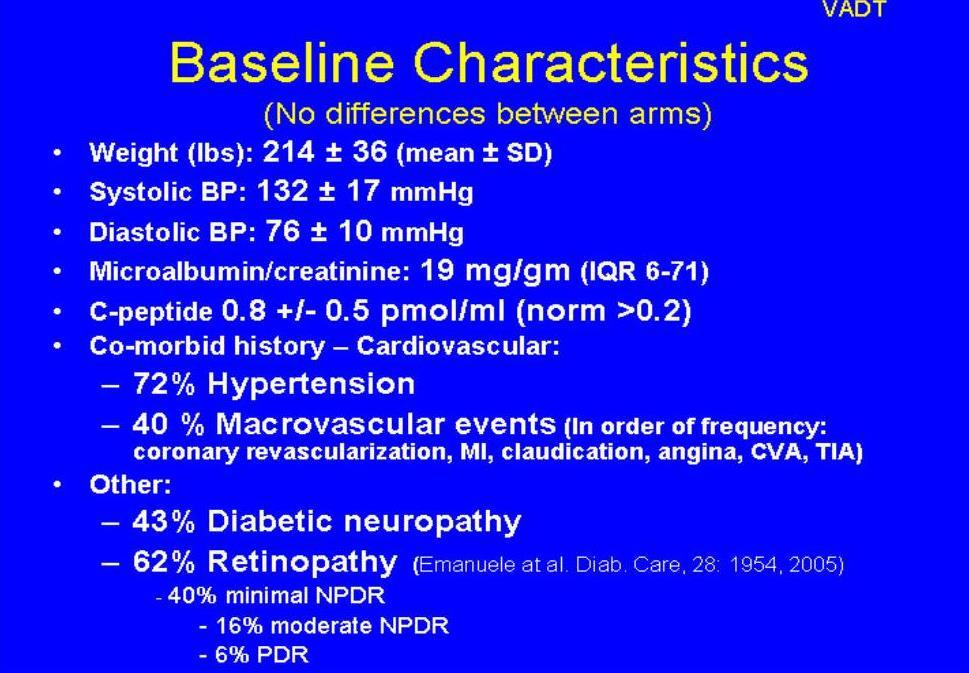
36 Mean A1c s 9.4% to 8.4% 9.4% to 6.9% VADT
37 And 6.9% 8.4% hazard ratio in the intensive-therapy group of 0.88 (95% confidence interval [CI], 0.74 to 1.05). VADT
38 Does VADT tell us anything?
39 VADT
40 Benefits of early vs late glycaemic intervention HbA 1c (%) Metabolic Memory = Glycaemic legacy 10 9 Estimated HbA 1c timecourse based on UKPDS data Enters VADT intensive treatment arm 8 7 Bad glycaemic legacy drives risk of complications HbA 1c time course in VADT 6 Ideal time-course of glycaemic control Time since diagnosis (years) UKPDS: United Kingdom Prospective Diabetes Study VADT: Veterans Affairs Diabetes Trial Adapted from Del Prato S. Diabetologia 2009;52:
41
42 P =.o3 VADT
43 NEJM Vol 358, No 24, June12, 2008: ACCORD heterogeneity
44
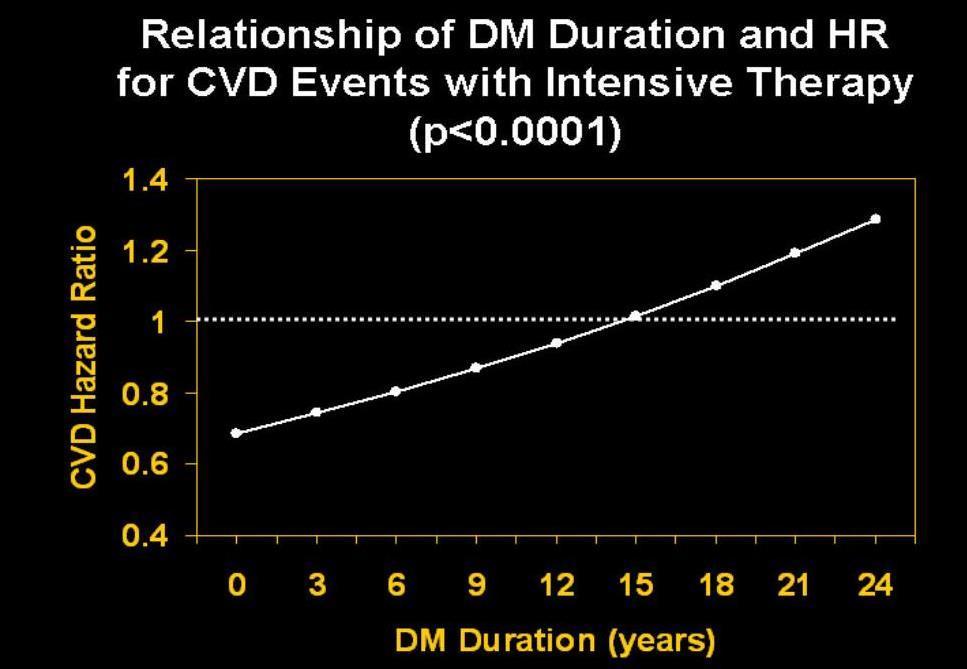
45 Early intervention! VADT
46 IS IT POSSIBLE TO PROVE THAT IMPROVED GLYCEMIC CONTROL CAN DECREASE CVD? ASSUME CVD event rate = 1.5% per year 25% risk reduction with intervention Alpha = 0.05 FOR 90% POWER Number 3 year study.28,000 5 year study.14, year study.6,800
47 Are there any studies looking at glucose control early in the course of the diabetes?

48 HbA 1c (%) HbA 1c 9 cross-sectional, median values 8 7 Conventional Intensive Mean difference.9% % upper limit of normal range Years from randomisation ukpds
49 % of patients with an event Myocardial Infarction (cumulative) 30% 20% 10% 0% Intensive p=0.052 fatal or non fatal myocardial infarction, sudden death 573 of 3867 patients (15%) Conventional Risk reduction 16% (95% CI: 0% to 29%) Years from randomisation ukpds
50
51 Proportion of patients with events overweight patients Myocardial Infarction Conventional (411) Intensive (951) Metformin (342) M v C p=0.010 M v I p= Years from randomisation RRR 31% ukpds

52 Abstract 1338
* HR 1.51 (CI: 1.25, 1.83)* HR 1.64 (CI: 1.40, 1.")
53 Delay in Treatment Intensification Increases the Risks of Cardiovascular Events in Patients with Type 2 Diabetes Compared to patients with HbA1c <7%, in patients with HbA1c 7%, a 12 month delay in receiving treatment intensification was associated with significantly increased risk: MI 67% STROKE 51% HF 64% CVE 62% HR 1.67 (CI: 1.39, 2.01)* HR 1.51 (CI: 1.25, 1.83)* HR 1.64 (CI: 1.40, 1.91)* HR 1.62 (CI: 1.46, 1.80)* MI= myocardial infarction, HF=Heart Failure, CVE= composite MI, Stroke & HF Retrospective cohort study (N = 105,477) from the United Kingdom Clinical Practice Research Datalink Not Proof of Cause and Effect * P <0.01 Adapted from Paul SK et al. Cardiovasc Diabetol Aug 7;14:100.
54 The earlier you start while the blood vessels are clean, the more benefit you expect from tighter glucose control
55 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
56 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
57
58 Diabetes and glucose How common is diabetes? Diabetes as a risk for CVD. Does A1c make a difference? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
59 Who died in ACCORD?
60 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers
61 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers

62
63 But when you adjust for glucose control.
64
65 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers

66
67 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers
68
69 What is it about this group of people that it wasn t possible to lower their A1c
70 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers
71 A1c s do not accurately describe glucose profiles in ALL people (Even excluding people with hemoglobinopathy, hemolysis, anemia, etc which are known to affect A1c)
72 Mr. R. R.
73 Mr. R. R.
74
75 Mr. F. S.
76 Mr. F. S.
77
78
79
80
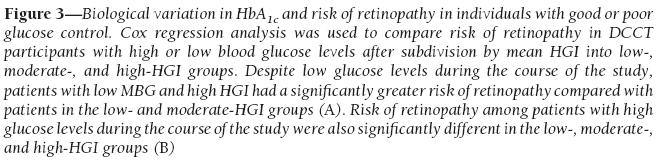
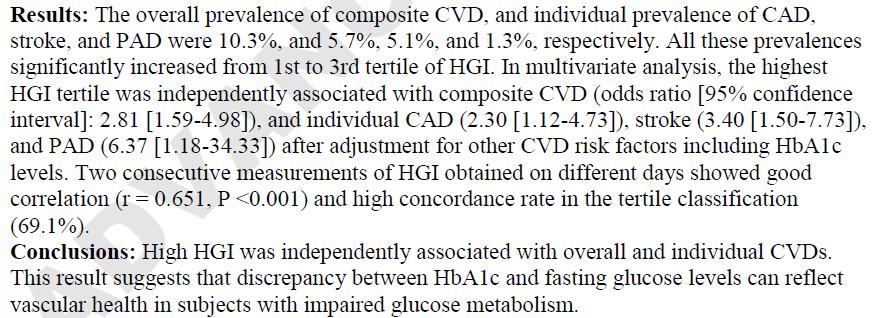
81 Hemoglobin Glycation Index (HGI) (Actual A1c) minus (Predicted A1c based on glucose values) Someone has a high HGI, (i.e., rapid glycator) if their glucoses are good but their A1c is high Someone has a low HGI, (i.e., slow glycator) if their glucoses are high but their A1c is low

82 Low HGI High HGI

83

84
85
86

87 High HGI Low HGI
88
89 Survivors High HGI Moderate HGI Low HGI Standard: dashed Intensive: solid
90 Mr. F. S
91

92
93
94 What does ACCORD really tell us? Tight glycemic control shows CV benefit after 5 years People who died had higher A1c s People who died were people in whom it was not possible to lower their A1c s People who died had a high Hemoglobin Glycation Index People who died tended not to be on beta blockers
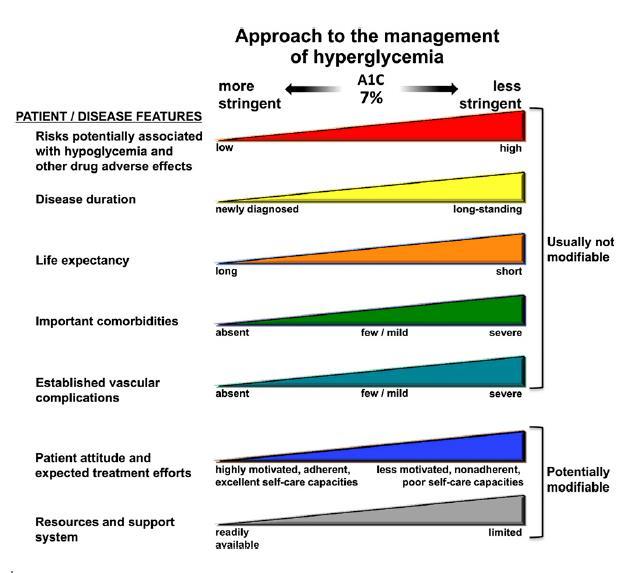
95
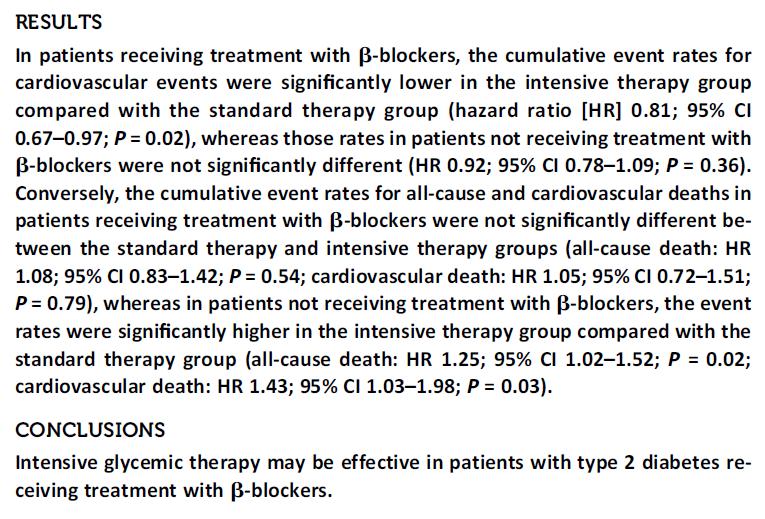
96 People on beta blockers had more events (not as surprise they had more disease) but being on intensive therapy lowered the event rate People not on beta blockers didn t have as many events (less disease) but intensive therapy did not lower the event rate
97 People on beta blockers had more events (not as surprise they had more disease) but being on intensive therapy did not increase the event rate People not on beta blockers didn t have as many events (less disease) but intensive therapy increased the event rate
98 Summary and Conclusions (1): Good glycemic control lowers risk of microvascular disease Aggressive glucose control early in the course of diabetes seems to be the best strategy Aggressive glucose control prior to the development of a large atherosclerotic burden seems to be best strategy This does not mean that if an individual has had their diabetes for a long period or has had a CV event that they won t benefit will take more time
99 Non-fatal MI, non-fatal CVA, death from CV causes NEJM Vol 358, No 24, June12, 2008
100 Non-fatal MI, non-fatal CVA, death from CV causes NEJM Vol 358, No 24, June12, 2008
101 Summary and Conclusions (2): A1c does not always tell the whole story. Look at the glucoses Look at the Pt s glucose meter!!! If A1c is high but glucoses are good, this patient is a rapid glycator with a high HGI. This is a higher risk patient There seems no gain in pushing his glucoses down further to lower his A1c It won t happen It would increase risk of hypoglycemia Concentrate on other risk factors
102 Summary and Conclusions (3): In people with vascular disease, beta blockers appear to be synergistic with tightening glucose control to lessen CV complications Protection for adrenergic stimulation from either Hypoglycemia? Further hyperinsulinemia????
103 Diabetes and glucose How common is diabetes? Why do we treat it? Does glycemic control predict complications? Does improving glucose control prevent complications? Does too tight glucose control cause death? Glucose vs glycation Hemoglobin Glycation Index What should our A1c target be?
104 Individualizing A1C Targets 2013 Consider % if: which must be balanced against the risk of hypoglycemia guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association
105
106 Hardin s suggestion for A1c target: Keep the above targets in mind, but Try to achieve the lowest A1c possible with the best balance of minimal highs and minimal lows The determination of best balance of minimal lows depends on risk of hypoglycemia and other general factors To do this, you must look at the meter and the logbook
107 Individualizing A1C Targets 2013 Consider % if: which must be balanced against the risk of hypoglycemia guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association
108 Individualizing A1C Targets 2013 Consider % if: which must be balanced against the risk of hypoglycemia guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association

 diabetes.")
109 Individualizing A1C Targets 2013 Consider % if: which must be balanced against the risk of hypoglycemia guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association
110
111
Glucose Control: Does it lower CV risk?
 Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Update on Diabetes. Ketan Dhatariya. Why it s Not Just About Glucose Lowering Any More. Consultant in Diabetes NNUH
 Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
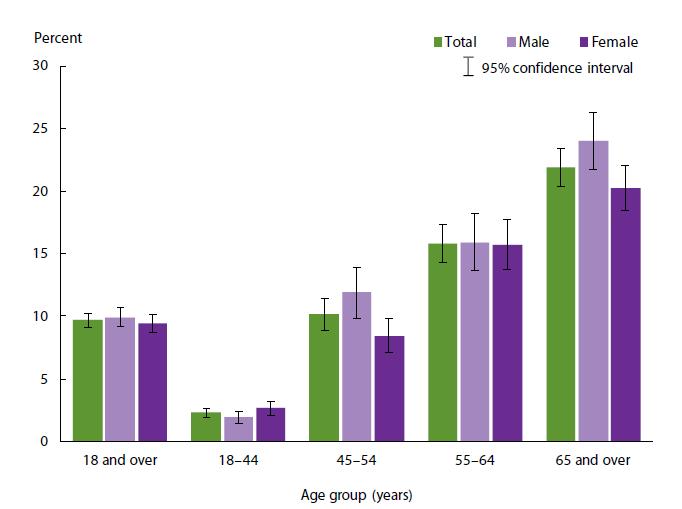
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Microvascular Complications in Diabetes:
 Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Microvascular Complications in Diabetes: Perspectives on Glycemic Control to Prevent Microvascular Complications Discussion Outline: Glycemia and Microvascular Compliations Clinical Trials - A Brief History
Copyright 2017 by Sea Courses Inc.
 Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE. AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY. sul Paziente ad alto rischio CV*
 CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
CONTROLLO GLICEMICO E RISCHIO CARDIOVASCOLARE AGOSTINO CONSOLI DMSI - Università d Annunzio CHIETI ITALY sul Paziente ad alto rischio CV* Does reducing hyperglycemia protect against cardiovascular risk?
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
DCCT Diabetes Control & Complications Trial
 DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,
DCCT Diabetes Control & Complications Trial A. Vinik MD, PhD, FCP, MACP, FACE, Καθηγητής και Αντιπρόεδρος για την Έρευνα, Ιατρική Σχολή Ανατολικής Βιρτζίνια, Κέντρο Ενδοκρινολογικών και Μεταβολικών Νοσημάτων,
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
ADVANCE Endpoints. Primary outcome. Secondary outcomes
 ADVANCE Trial-NEJM 11,140 type 2 patients with h/o microvascular or macrovascular disease or 1 vascular disease risk factor Control A1c to 6.5% vs standard tx Intensive arm received gliclazide XL 30 to
ADVANCE Trial-NEJM 11,140 type 2 patients with h/o microvascular or macrovascular disease or 1 vascular disease risk factor Control A1c to 6.5% vs standard tx Intensive arm received gliclazide XL 30 to
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Prevention of complications: are we winning or losing the battle. Naveed Sattar Professor of Metabolic Medicine
 Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
04-Sep-17. INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification
 PROF MERLIN THOMAS DIAttitude Study INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification 13% immediately 41% of patients
PROF MERLIN THOMAS DIAttitude Study INERTIA a failure to initiate or modify treatment in a timely manner in people whose health is likely to improve with this modification 13% immediately 41% of patients
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Glucose Control and Prevention of Cardiovascular Disease
 Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
Glucose Control and Prevention of Cardiovascular Disease Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Diabetes Update+, March
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Long-Term Care Updates
 Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Diabetes Mellitus Type 2 Evidence-Based Drivers
 This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
Type 2 diabetes affects an estimated 25.8 million
 Hosp Pharm 2014;49(8):697 701 2014 Thomas Land Publishers, Inc. www.hospital-pharmacy.com doi: 10.1310/hpj4908-697 Cardiovascular Therapeutics Diabetes and Cardiovascular Risk: Are Dipeptidyl Peptidase-4
Hosp Pharm 2014;49(8):697 701 2014 Thomas Land Publishers, Inc. www.hospital-pharmacy.com doi: 10.1310/hpj4908-697 Cardiovascular Therapeutics Diabetes and Cardiovascular Risk: Are Dipeptidyl Peptidase-4
Kidney and heart: dangerous liaisons. Luis M. RUILOPE (Madrid, Spain)
") Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus
 1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
1 Dissertation Title Page: Individualized Treatment Goals for Optimal Long-Term Health Outcomes among Patients with Type 2 Diabetes Mellitus Qian Shi, MPH, PhD candidate Department of Global Health Management
A nationwide population-based study. Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD
 The Association of Clinical Symptomatic Hypoglycemia with Cardiovascular Events and Total Death in Type 2 Diabetes Mellitus A nationwide population-based study Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD Taipei
The Association of Clinical Symptomatic Hypoglycemia with Cardiovascular Events and Total Death in Type 2 Diabetes Mellitus A nationwide population-based study Pai-Feng Hsu M.D. Shao-Yuan Chuang PhD Taipei
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
Metformin. Sulfonylurea. Thiazolidinedione. Insulin
 동아의대내분비내과박미경 Metformin Sulfonylurea Thiazolidinedione Insulin 요약 markers of inflammation (hs-crp, TNF-a) markers of impaired endothelial function (VFW, scams, tpa, PAI-1) LDL-C, fasting and postprandial
동아의대내분비내과박미경 Metformin Sulfonylurea Thiazolidinedione Insulin 요약 markers of inflammation (hs-crp, TNF-a) markers of impaired endothelial function (VFW, scams, tpa, PAI-1) LDL-C, fasting and postprandial
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Type 2 Diabetes. Treat to: limit complications maintain quality of life Improve survival
 Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Real World Evidence: From Efficacy to Effectiveness
 Real World Evidence: From Efficacy to Effectiveness Professor Kamlesh Khunti University of Leicester, UK Leicester Diabetes Centre at University Hospitals of Leicester NHS Trust, 2015. Not to be reproduced
Real World Evidence: From Efficacy to Effectiveness Professor Kamlesh Khunti University of Leicester, UK Leicester Diabetes Centre at University Hospitals of Leicester NHS Trust, 2015. Not to be reproduced
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies
 Ann. N.Y. Acad. Sci. ISSN 0077-8923 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES Issue: The Year in Diabetes and Obesity Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies Sophia
Ann. N.Y. Acad. Sci. ISSN 0077-8923 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES Issue: The Year in Diabetes and Obesity Cardiovascular outcomes in type 2 diabetes: the impact of preventative therapies Sophia
Management of Cardiovascular Disease in Diabetes
 Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Complications of Diabetes: Screening and Prevention. Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley
 Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
The metabolic memory. Antonio Ceriello
 The metabolic memory Antonio Ceriello : DCCT/EDIC - Long-term Microvascular Risk Reduction in Type 1 Diabetes A1C 12% 10% Intensive Retinopathy progression (incidence) Conventional 0.5 0.4 0.3 62% risk
The metabolic memory Antonio Ceriello : DCCT/EDIC - Long-term Microvascular Risk Reduction in Type 1 Diabetes A1C 12% 10% Intensive Retinopathy progression (incidence) Conventional 0.5 0.4 0.3 62% risk
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus
 Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Diabetes and the Heart
 Diabetes and the Heart By Samir Naim Assaad, MD, MRCP(UK), FRCP(Edin), FRCP(Lond) Professor of Medicine & Endocrinology University of Alexandria EGYPT Disclosure None, related to this presentation Road
Diabetes and the Heart By Samir Naim Assaad, MD, MRCP(UK), FRCP(Edin), FRCP(Lond) Professor of Medicine & Endocrinology University of Alexandria EGYPT Disclosure None, related to this presentation Road
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
DIABETES AND METABOLIC SYNDROME
 TRIALS NUMBER OF PARTICIPANTS NUMBER OF WOMEN PERCENTAGE OF WOMEN MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 48,508 20,091 41.4% 61.1 4.3 4/7 (57.1%) HR PROactive (Dormandy et al 61
TRIALS NUMBER OF PARTICIPANTS NUMBER OF WOMEN PERCENTAGE OF WOMEN MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 48,508 20,091 41.4% 61.1 4.3 4/7 (57.1%) HR PROactive (Dormandy et al 61
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
In general: Hypoglycemia is common in insulin treated diabetes, but may also occur in people on oral medications, especially sulfonylureas/glinides.
 1 2 3 In general: Hypoglycemia is common in insulin treated diabetes, but may also occur in people on oral medications, especially sulfonylureas/glinides. 4 Answer: b and c Many alcohol containing drinks
1 2 3 In general: Hypoglycemia is common in insulin treated diabetes, but may also occur in people on oral medications, especially sulfonylureas/glinides. 4 Answer: b and c Many alcohol containing drinks
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 ( ) 가천의대길병원내분비대사내과
 가천의대길병원내분비대사내과") 효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
1. How does the response to therapy compare in elderly versus middle age adults with diabetes in a randomized trial?
 Jeff D. Williamson, MD, MHS Chief, Geriatric Medicine Sticht Center on Aging 1. How does the response to therapy compare in elderly versus middle age adults with diabetes in a randomized trial? 2. Are
Jeff D. Williamson, MD, MHS Chief, Geriatric Medicine Sticht Center on Aging 1. How does the response to therapy compare in elderly versus middle age adults with diabetes in a randomized trial? 2. Are
Clinical outcomes of HbA1c standardisation
 Clinical outcomes of HbA1c standardisation Eric S. Kilpatrick Division Chief, Clinical Chemistry Sidra Medicine, Doha, Qatar Professor of Pathology & Laboratory Medicine, Weill Cornell Medicine-Qatar Honorary
Clinical outcomes of HbA1c standardisation Eric S. Kilpatrick Division Chief, Clinical Chemistry Sidra Medicine, Doha, Qatar Professor of Pathology & Laboratory Medicine, Weill Cornell Medicine-Qatar Honorary
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Diabetes outcomes Keystone 17 July 2014
 Diabetes outcomes Keystone 17 July 214 How diabetes outcomes have changed over the past 3 years JBN: 194,119.11 Date of Prep: June 214 Professor Philip Home Newcastle University How diabetes outcomes have
Diabetes outcomes Keystone 17 July 214 How diabetes outcomes have changed over the past 3 years JBN: 194,119.11 Date of Prep: June 214 Professor Philip Home Newcastle University How diabetes outcomes have
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
The New Diabetes Standard of Care: More Than Just Glycemic Control. Copyright
 CLINICAL Viewpoint The New Diabetes Standard of Care: More Than Just Glycemic Control Advancement in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
CLINICAL Viewpoint The New Diabetes Standard of Care: More Than Just Glycemic Control Advancement in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
Moving to an A1C-Based Screening & Diagnosis of Diabetes. By Prof.M.Assy Diabetes&Endocrinology unit
 Moving to an A1C-Based Screening & Diagnosis of Diabetes By Prof.M.Assy Diabetes&Endocrinology unit is the nonenzymatic glycated product of the hemoglobin beta-chain at the valine terminal residue. Clin
Moving to an A1C-Based Screening & Diagnosis of Diabetes By Prof.M.Assy Diabetes&Endocrinology unit is the nonenzymatic glycated product of the hemoglobin beta-chain at the valine terminal residue. Clin
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Sulfoniluree e glinidi: pro e contro
 Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor