THE HEMODIALYSIS PRESCRIPTION: TREATMENT ADEQUACY GERALD SCHULMAN MD VANDERBILT UNIVERSITY MEDICAL SCHOOL NASHVILLE, TENNESSEE
|
|
|
- Bertha Moody
- 6 years ago
- Views:
Transcription
1 THE HEMODIALYSIS PRESCRIPTION: TREATMENT ADEQUACY GERALD SCHULMAN MD VANDERBILT UNIVERSITY MEDICAL SCHOOL NASHVILLE, TENNESSEE

2 THE DIALYSIS CYCLE /TIME

3 DESIGN OF THE NATIONAL COOPERATIVE DIALYSIS STUDY

4 REVISED NCDS RESULTS EXPRESSED AS Kt/V MORBIDITY, NOT MORTALITY

5 COMPARATIVE MORTALITY RATES
6 IMPLICATION OF US DIALYSIS MORTALITY RATE

7 IMPLICATION OF US DIALYSIS MORTALITY RATE
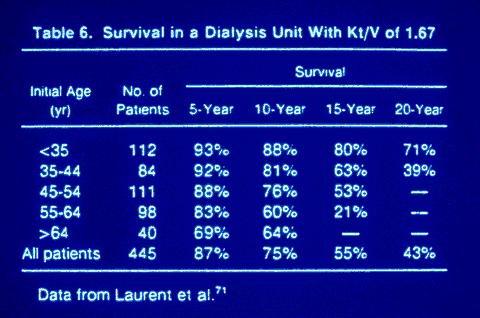
8 TASSIN EXPERIENCE

9 Kt/V AND MORTALITY
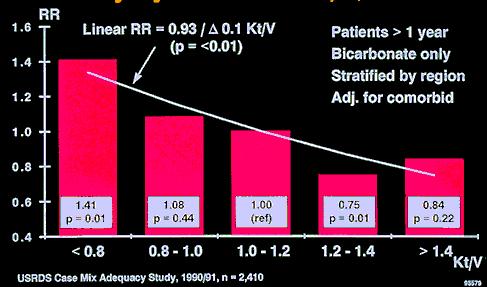
10 Kt/V & RISK OF MORTALITY 1.

11 Kt/V & MORTALITY: MINNESOTA EXPERIENCE

12 CHANGING TRENDS IN THERAPY

13 CHANGING TRENDS IN THERAPY

14 CHANGING TRENDS IN THERAPY

15 CHANGING TRENDS IN THERAPY
16
17 MEMBRANE FLUX: A POTENTIAL CONFOUNDING VARIABLE CHANGES IN Kt/V WERE IN PART ACCOMPLISHED BY USE OF HFM POTENTIAL BENEFITS OF HFM IMPROVED PROTEIN CATABOLIC RATE IMPROVED TG METABOLISM IMPROVED EPO RESPONSE IMPROVED BETA 2 -MICROGLOBULIN REMOVAL HOWEVER, BECAUSE OF LOW T D, THE FULL EFFECT OF HFM IS NOT EVIDENT. REMOVAL OF HIGH MW SUBSTANCES ARE ALSO TIME DEPENDENT.
18 INFLUENCE OF DOSE AND DIALYZER CHOICE ON NUTRITION High Ktt/V, Synthetic npcr High Kt/V, Cellulosic GOAL: HEMO-Kt/V>1.2 PD-Kt/V>2.1(week) Low Kt/v & Cellulosic DIALYSIS DOSE

19 ADEQUACY AND NUTRITIONAL STATUS

20 ADEQUACY AND ALBUMIN LEVEL
21 HEMODIALYSIS TIME: THE UNRESOLVED PARAMETER K D IS A MERE TECHNICAL ISSUE MINIMUM T D HAS ITS BASIS ROOTED IN PHYSIOLOGY SHORT TIME MAKES HEMODIALYSIS UNFORGIVING: EXCEPT FOR TASSIN, NO MODERN STUDIES HAS EXAMINED LONG (>5 HOURS) TIME AND OUTCOME
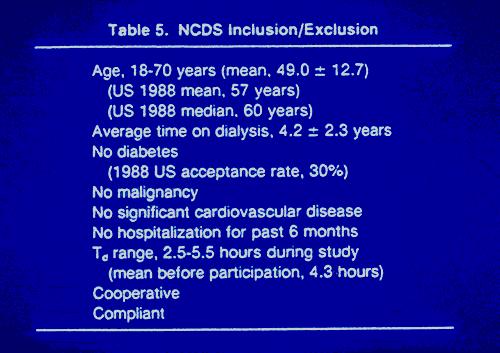
22 THE NCDS POPULATION
23 FACTORS RELATED TO DIALYSIS ADEQUACY HEMODIALYSIS RELATED FACTORS DOSE LOW MW SOLUTES HIGH MW SOLUTES DIALYSIS TIME MEMBRANE FLUX BIOCOMPATIBILTY REUSE PATIENT RELATED FACTORS NUTRITION ACIDOSIS CA x P BLOOD PRESSURE LIPIDS CARDIOVASCULAR MORBIDITY INFLAMMATION

24 ALTERNATIVES FOR THE HEMO STUDY
25 THE HEMODIALYSIS (HEMO) STUDY AN NIH-NIDDK SPONSORED RANDOMIZED, MULTI-CENTER CLINICAL TRIAL
26 THE CHOICE: OBJECTIVES OF THE HEMO STUDY In patients undergoing 3x/week maintenance hemodialysis, to determine whether higher dose, or high-flux membrane affect mortality (primary outcome), or morbidity (secondary outcome)

27 DOUBLE POOL KINETICS
28 THE RATE EQUATION

29 RATE EQUATION AS A FUNCTION OF TIME

30 RELATIONSHIP OF Kt/V SP TO Kt/V DP AND AS A FUNCTION OF REBOUND
31 THE DIALYSIS CYCLE /TIME
32 Standard dose ekt/v = 1.05 spkt/v 1.25 URR 65% Dose High dose ekt/v = 1.45 spkt/v 1.65 URR 75% Standard Dose Low Flux High Dose Low Flux Standard Dose High Flux High Dose High Flux
33 Flux Low-flux dialyzers: β 2 M clearance < 10 ml/min Flux comparison Standard Dose Low Flux Standard Dose High Flux High Dose Low Flux High Dose High Flux High-flux dialyzers: β 2 M clearance > 20 ml/min
34 Time to Death by Kt/V Group

35 Time to Death by Flux Group
36 Interactions of Treatments with Baseline Characteristics Did treatment effects differ between subgroups for seven pre-specified baseline factors? Age Gender Race Diabetes Years of dialysis Comorbidity Albumin
37 Predictors of Mortality by Cox Regression Predictor Variable Relative Risk 95% Confidence p-value High dose 0.96 (0.84, 1.09) 0.52 High flux 0.92 (0.81, 1.06) 0.24 Age (per 10 yrs increase) 1.44 (1.35, 1.54) <0.001 Gender (female) 0.86 (0.74, 0.99) 0.03 Race (African American) 0.76 (0.65, 0.89) Diabetes 1.24 (1.06, 1.45) <0.001 Years of dialysis 1.04 (1.02, 1.06) <0.001 Baseline serum albumin (per 0.5 g/dl increment) 0.51 (0.43, 0.62) Model also includes 2 other sig. variables: ICED, albumin x time Analysis stratified by clinical center <0.001
38 Time to Death by Kt/V Group Females (484 Deaths)
39 Time to Death by Flux Group Duration of Dialysis > 3.7 Years (298 Deaths)
40 HEMO STUDY SUMMARY 1) THE HIGHER DOSE OF HEMODIALYSIS THRICE WEEKLY DID NOT: IMPROVE SURVIVAL, REDUCE HOSPITALIZATIONS, OR MAINTAIN SERUM ALBUMIN 2) USE OF A HIGH FLUX MEMBRANE DID NOT: IMPROVE SURVIVAL, REDUCE HOSPITALIZATIONS, OR MAINTAIN SERUM ALBUMIN
41 HEMO STUDY SUMMARY 3) HOWEVER, EFFECTS MAY VARY AMONG CERTAIN SUBSETS OF PATIENTS: A) IN WOMEN, THE HIGHER DOSE OF DIALYSIS MAY BE ASSOCIATED WITH INCREASED SURVIVAL B) IN PATIENTS WITH > 3.7 YEARS ON DIALYSIS, USE OF A HIGH FLUX MEMBRANE MAY BE ASSOCIATED WITH INCREASED SURVIVAL C) THE RESULTS ON THESE SUBSETS SHOULD BE INTERPRETED CAUTIOUSLY AND BE FURTHER INVESTIGATED
42 ARE WE CONFOUNDING DETERMINATION OF ADEQUACY BY THE USE OF Kt/V? Kt/V Kt= AMOUNT OF DIALYSIS, A GOOD THING V= VOLUME~WEIGHT~MUSCLE MASS, A GOOD THING A GOOD THING/A GOOD THING
43 UREA VOLUME AND SURVIVAL 25L 45L 55L RELATIVE RISK OF DEATH
44 MINEFIELDS AVOIDED BY THE HEMO STUDY DESPITE ITS LENGTH, WE AVOIDED BEING ECLIPSED BY CHANGES IN COMMUNITY PRACTICE PATTERNS T D, Q B, Q D SIMILAR TO USRDS MEMBRANES SIMILAR STANDARD LEVEL Kt/V DELIVERED WAS BETTER OR EQUAL TO COMMUNITY PRACTICE THROUGHOUT THE STUDY. THE COMMUNITY RECOMMENDATIONS EXCEEDED HEMO STANDARD Kt/V FOR ONLY A SHORT TIME DOSE AND FLUX GOALS ACHIEVED MORTALITY NOT OVERESTIMATED ADEQUATELY POWERED WHAT WAS PILOTED IS WHAT WAS STUDIED
45 WHY THE HEMO STUDY WAS NEEDED RAPIDLY GROWING ESRD POPULATION 10 %/YEAR GROWTH RATE, COSTING $BILLIONS WORSENING COMORBIDITY MAJORITY TREATED BY HEMODIALYSIS US ANNUAL GROSS MORTALITY OF 21-23% OBSERVATIONAL AND CORRELATIONAL STUDIES DEMONSTRATING IMPROVED SURVIVAL FOLLOWING TREATMENT CHANGES HIGHER DOSE AS MEASURED BY Kt/V OR URR BIOCOMPATIBLE MEMBRANES REMOVAL OF HIGH MW SUBSTANCES (FLUX)

46 IMPLICATIONS OF THE HEMO STUDY ADAPTED FROM MUJAIS; ADEMEX STUDY

47 PLACES TO GO NEXT ADAPTED FROM MUJAIS; ADEMEX STUDY
48 LARGE MOLECULE REBOUND
49 MEMBRANE FLUX: A POTENTIAL CONFOUNDING VARIABLE CHANGES IN Kt/V WERE IN PART ACCOMPLISHED BY USE OF HFM POTENTIAL BENEFITS OF HFM IMPROVED PROTEIN CATABOLIC RATE IMPROVED TG METABOLISM IMPROVED EPO RESPONSE IMPROVED BETA 2 -MICROGLOBULIN REMOVAL HOWEVER, BECAUSE OF LOW T D, THE FULL EFFECT OF HFM IS NOT EVIDENT: REMOVAL OF HIGH MW SUBSTANCES ARE ALSO TIME DEPENDENT- LONGER TIMES ARE NECESSARY TO SHOW BENEFITS OF HFM
50 HEMODIALYSIS TIME: THE UNRESOLVED PARAMETER K D IS A MERE TECHNICAL ISSUE MINIMUM T D HAS ITS BASIS ROOTED IN PHYSIOLOGY SHORT TIME MAKES HEMODIALYSIS UNFORGIVING: EXCEPT FOR TASSIN, NO MODERN STUDIES HAS EXAMINED LONG (>5 HOURS) TIME AND OUTCOME
51 POTENTIAL PARAMETERS TO CONSIDER WITH NOCTURNAL AND DAILY HD
52 FACTORS THAT MAY INFLUENCE MORBIDITY AND SURVIVAL ON HEMODIALYSIS MEMBRANES: SYNTHETIC, FLUX DIALYSATE: SODIUM, BICARBONATE PHOSPHATE, Ca x P, Ca EPO DIALYSIS KINETICS DIALYSIS TIME NUTRITION ALTERNATE DIALYSIS SCHEDULES
53 ISSUES TO BE CONSIDERED DEFINTIONS OF THE MODALITIES INDIVIDUAL STUDIES OF EACH OF THE MODALITIES DAILY HEMODIALYSIS vs NOCTURNAL HEMODIALYSIS
54 ALTERNATIVES TO STANDARD HEMODIALSIS TREATMENTS SLOW LONG-DURATION HEMODIALYSIS THRICE WEEKLY; BIOINCOMPATIBLE MEMBRANE; 6-8 HOURS; Q B = ml/min; Kt/V>1.8 SHORT DURATION DAILY DIALYSIS 5-6 TIMES EACH WEEK; HIGH FLUX BIOCOMPATIBLE MEMBRANE ; HOURS; Q B >400 ml/min; Kt/V NOCTURNAL HEMODIALYSIS 5-7 TIMES EACH WEEK; BIOCOMPATIBLE MEMBRANE; 6-8 HOURS; Q B = ml/min; K
55 Elevated Serum Phosphorus Increases Mortality Risk1 US PTS 39%> 6.5 Relative Mortality Risk (RR) * Serum Phosphorus Quintile (mg/dl) 1.39** * P=0.03 ** P< (n=6407) 1. Adapted from Block GA, et al. Am J Kidney Dis. 1998;31:

56 SERUM PHOSPHORUS DURING DIALYSIS
57 NOCTURNAL HD AND PHOSPHATE CONTROL PHOSPHATE REMOVAL mmol P REMOVAL/SESSION P REMOVAL/WEEK CONVENTIONAL NOCTURNAL KI 1998; 53:
58 DIETARY PHOSPHATE INTAKE: CONVENTIONAL vs NOCTURNAL HD PHOSPHATE INTAKE mmol/day CONVENTIONAL NOCTURNAL CONVENTIONAL NOCTURNAL KI 1998; 53:
59 CONVENTIONAL HD vs NOCTURNAL HD: PHOSPHATE CONTROL PHOSPHATE LEVELS 2.1 mmol/l (~6 mg/dl) DECREASED TO 1.3 mmol/l (~3.9 mg/dl) WITH THE START OF NOCTURNAL HD BY THE 4th MONTH OF NOCTURNAL HD, NONE OF THE PATIENTS WERE USING PHOSPHATE BINDERS KI 1998; 53:
60 NOCTURNAL vs DAILY SHORT HEMODIALYSIS NOCTURNAL HD LONG TREATMENTS PHOSHATE CONTROL IMPROVED BLOOD PRESSURE CONTROL IMPROVED ALBUMIN IMPROVED HOME THERAPY DAILY SHORT HD SHORT TREATMENTS PHOSPHATE CONTROL NOT IMPROVED BLOOD PRESSURE CONTROL IMPROVED ALBUMIN IMPROVED HOME OR IN-CENTER THERAPY
61 PRINCIPLE BEHIND THE USE OF STANDARD Kt/V UREA IS REMOVED IN A MORE EFFICIENT MANNER AT THE SAME WEEKLY KT/V AS YOU INCREASE DIALYSIS FREQUENCY. REMOVAL OF LESS DIFFUSIBLE SOLUTES IS EVEN MORE EFFICIENT AT THE SAME WEEKLY KT/V.
62 STATUS OF DAILY DIALYSIS NO PROSPECTIVE STUDIES OF INCIDENT PATIENTS PATIENT SELECTION IS NOT RANDOM PATIENTS NUMBER IN THE 100 S NO STANDARDIZATION OF REGIMENS NO OUTCOME STUDIES NOCTURNAL vs DAILY ACCESS FUNCTION NOT COMPROMISED
63 THE DIALYSIS CYCLE /TIME

64 THE EFFECT OF FREQUENCY ON WEEKLY Kt/V As you increase the frequency, on the x axis here, and maintain the same time average BUN, the need for dialysis diminishes, the dose of dialysis expressed on a weekly basis is less.

65 RATIONALE FOR USING THE STANDARD Kt/V DEPNER

66 STANDARD Kt/V FOR A CONTINUOUS THERAPY, PEAK=MEAN

67 CONTINUOUS VS INTERMITTENT THERAPY

68 STANDARD WEEKLY Kt/V MODEL -CAPD -IHD -SDHD -NHHD
69 RELATIONSHIP BETWEEN WEEKLY AND STANDARD Kt/V MODALITY SHORT DAILY DIALYSIS NOCTURNAL HEMODIALYSIS WEEKLY Kt/V STANDARD Kt/V LEYPOLDT, SEMINAR DIAL, 2004
70 SUMMARY AND CONCLUSIONS MULTIPLE LINES OF EVIDENCE SUGGEST DAILY TREATMENTS IMPROVE: ADEQUACY BLOOD PRESSURE CONTROL HOSPITALIZTION RATE NUTRITION TRIALS OF THE MODALITIES ARE REQUIRED NOCTURNAL HD NEEDS TO BE INCLUDED IN SUCH TRIALS LACSON AND DIAZ BUXO:NHD FIRST, DHD SUBSEQUENTLY AM J KIDNEY DISEASE 2001; 38:

71 STANDARD Kt/V: A CONTINUOUS CLEARANCE EQUIVALENT DEPNER
72 PLACES TO GO NEXT DAILY/NOCTURNAL TREATMENT REGIMENS
73 THE REAL KEY TREATMENT VARIABLE AFTER DR. C RONCO

74 THE EYE OF GOD
Design Paper Design and Statistical Issues of the Hemodialysis (HEMO) Study
 Study") Design Paper Design and Statistical Issues of the Hemodialysis (HEMO) Study The HEMO Study Group,* Prepared by: Tom Greene, PhD, Gerald J. Beck, PhD, Jennifer J. Gassman, PhD, Frank A. Gotch, MD, John
Design Paper Design and Statistical Issues of the Hemodialysis (HEMO) Study The HEMO Study Group,* Prepared by: Tom Greene, PhD, Gerald J. Beck, PhD, Jennifer J. Gassman, PhD, Frank A. Gotch, MD, John
Hemodialysis Adequacy: A Complex and Evolving Paradigm. Balazs Szamosfalvi, MD Monday, 08/30/ :00-09:45
 Hemodialysis Adequacy: A Complex and Evolving Paradigm Balazs Szamosfalvi, MD Monday, 08/30/2010 09:00-09:45 Adequacy 1943-1970 Fresenius The patient survived the dialysis session Uremia improved Volume
Hemodialysis Adequacy: A Complex and Evolving Paradigm Balazs Szamosfalvi, MD Monday, 08/30/2010 09:00-09:45 Adequacy 1943-1970 Fresenius The patient survived the dialysis session Uremia improved Volume
There are no shortcuts to Dialysis
 There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
Effects of High-Flux Hemodialysis on Clinical Outcomes: Results of the HEMO Study
 J Am Soc Nephrol 14: 3251 3263, 2003 Effects of High-Flux Hemodialysis on Clinical Outcomes: Results of the HEMO Study ALFRED K. CHEUNG,* NATHAN W. LEVIN, TOM GREENE, LAWRENCE AGODOA, JAMES BAILEY, GERALD
J Am Soc Nephrol 14: 3251 3263, 2003 Effects of High-Flux Hemodialysis on Clinical Outcomes: Results of the HEMO Study ALFRED K. CHEUNG,* NATHAN W. LEVIN, TOM GREENE, LAWRENCE AGODOA, JAMES BAILEY, GERALD
3/21/2017. Solute Clearance and Adequacy Targets in Peritoneal Dialysis. Peritoneal Membrane. Peritoneal Membrane
 3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Ana Paula Bernardo. CHP Hospital de Santo António ICBAS/ Universidade do Porto
 Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Coming to a Home near You
 Home Dialysis i Coming to a Home near You John A. Sweeny NANT Annual National Symposium Tuesday March 8 th, 2011 Initial Home Hemodialysis Home HD was begun to reduce the cost of in-hospital HD in the
Home Dialysis i Coming to a Home near You John A. Sweeny NANT Annual National Symposium Tuesday March 8 th, 2011 Initial Home Hemodialysis Home HD was begun to reduce the cost of in-hospital HD in the
Dialysis Adequacy (HD) Guidelines
 Guidelines") Dialysis Adequacy (HD) Guidelines Peter Kerr, Convenor (Monash, Victoria) Vlado Perkovic (Camperdown, New South Wales) Jim Petrie (Woolloongabba, Queensland) John Agar (Geelong, Victoria) Alex Disney (Woodville,
Dialysis Adequacy (HD) Guidelines Peter Kerr, Convenor (Monash, Victoria) Vlado Perkovic (Camperdown, New South Wales) Jim Petrie (Woolloongabba, Queensland) John Agar (Geelong, Victoria) Alex Disney (Woodville,
All patients suitable for home dialysis should do PD first
 All patients suitable for home dialysis should do PD first 2008 BC Nephrology Day Conference October 2, 2008 Vancouver, British Columbia Robert S. Lockridge, Jr. M.D. Lynchburg Nephrology Physicians Associate
All patients suitable for home dialysis should do PD first 2008 BC Nephrology Day Conference October 2, 2008 Vancouver, British Columbia Robert S. Lockridge, Jr. M.D. Lynchburg Nephrology Physicians Associate
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
THE CURRENT PARADIGM of thrice-weekly
 Dose of Dialysis: Key Lessons From Major Observational Studies and Clinical Trials Rajiv Saran, MD, MS, Bernard J. Canaud, MD, Thomas A. Depner, MD, Marcia L. Keen, PhD, Keith P. McCullough, MS, Mark R.
Dose of Dialysis: Key Lessons From Major Observational Studies and Clinical Trials Rajiv Saran, MD, MS, Bernard J. Canaud, MD, Thomas A. Depner, MD, Marcia L. Keen, PhD, Keith P. McCullough, MS, Mark R.
Since its first application as a treatment for end-stage
 Dialysis Session Length ( t ) as a Determinant of the Adequacy of Dialysis Manjula Kurella and Glenn M. Chertow Several studies have shown an association between the hemodialysis session length (the t
Dialysis Session Length ( t ) as a Determinant of the Adequacy of Dialysis Manjula Kurella and Glenn M. Chertow Several studies have shown an association between the hemodialysis session length (the t
Patients and Machines. NANT Annual National Symposium Wednesday March 9 th, 2011
 Patients and Machines John A Sweeny John A. Sweeny NANT Annual National Symposium Wednesday March 9 th, 2011 Caroline Helm Caroline Helm was the first homepatient in the United States. She was a patient
Patients and Machines John A Sweeny John A. Sweeny NANT Annual National Symposium Wednesday March 9 th, 2011 Caroline Helm Caroline Helm was the first homepatient in the United States. She was a patient
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
The CARI Guidelines Caring for Australians with Renal Impairment. Blood urea sampling methods GUIDELINES
 Date written: November 2004 Final submission: July 2005 Blood urea sampling methods GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions are
Date written: November 2004 Final submission: July 2005 Blood urea sampling methods GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions are
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006") IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate
 Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Supplemental Quick Reference Guide
 Supplemental Quick Reference Guide How to use this Supplemental Quick Reference Guide This guide provides a 5-step method for considering a variety of frequencies and treatment lengths, based on achieving
Supplemental Quick Reference Guide How to use this Supplemental Quick Reference Guide This guide provides a 5-step method for considering a variety of frequencies and treatment lengths, based on achieving
Chapter Five Clinical indicators & preventive health
 Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)
![[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)](/thumbs/92/109602349.jpg "[1] Levy [3] (odds ratio) 5.5. mannitol. (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP)") [1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
[1] Levy [3] 183 174 (odds ratio) 5.5 Woodrow [1] 1956 1989 mannitol (renal dose) dopamine 1 µg/kg/min atrial natriuretic peptide (ANP) McCarthy [2] 1970 1990 insulin-like growth factor-1 (IGF-1) ANP 92
Hemodialysis is a life-sustaining procedure for the treatment of
 The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
Chapter IV. The USRDS Dialysis Morbidity and Mortality Study (Wave 1) Methods
 Methods") Annual Data Report USRDS Dialysis Morbidity and Mortality (Wave 1) Chapter IV The USRDS Dialysis Morbidity and Mortality Study (Wave 1) T he USRDS Dialysis Morbidity and Mortality Study is an observational
Annual Data Report USRDS Dialysis Morbidity and Mortality (Wave 1) Chapter IV The USRDS Dialysis Morbidity and Mortality Study (Wave 1) T he USRDS Dialysis Morbidity and Mortality Study is an observational
EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey
 EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof Ercan Ok Division
EFFECT OF ONLINE HAEMODIAFILTRATION ON ALL- CAUSE MORTALITY AND CARDIOVASCULAR OUTCOMES Ercan Ok, Izmir, Turkey Chair: Walter H. Hörl, Vienna, Austria Wojciech Zaluska, Lublin, Poland Prof Ercan Ok Division
Effect of the dialysis membrane on mortality of chronic
 Kidney International, Vol. 50 (1996), pp. 566 5 70 Effect of the dialysis membrane on mortality of chronic hemodialysis patients RAYMOND M. HAKIM, PHILIP J. HELD, DAVID C. STANNARD, ROBERT A. WOLFE, FRIEDRICH
Kidney International, Vol. 50 (1996), pp. 566 5 70 Effect of the dialysis membrane on mortality of chronic hemodialysis patients RAYMOND M. HAKIM, PHILIP J. HELD, DAVID C. STANNARD, ROBERT A. WOLFE, FRIEDRICH
Diacap. Constant performance resulting in high quality dialysis. Avitum
 Diacap Constant performance resulting in high quality dialysis Avitum B. Braun Avitum. Always with Passion. B. Braun is a leading international company in the healthcare market. With a long tradition stretching
Diacap Constant performance resulting in high quality dialysis Avitum B. Braun Avitum. Always with Passion. B. Braun is a leading international company in the healthcare market. With a long tradition stretching
Principal Equations of Dialysis. John A. Sweeny
 Principal Equations of Dialysis John A. Sweeny john@sweenyfamily.net 1 An Equation is Math: A statement that each of two statements are equal to each other. Y 2 = 3x 3 + 2x + 7 Chemistry: A symbolic expression
Principal Equations of Dialysis John A. Sweeny john@sweenyfamily.net 1 An Equation is Math: A statement that each of two statements are equal to each other. Y 2 = 3x 3 + 2x + 7 Chemistry: A symbolic expression
Achieving Equilibrium in ESRD Patients
 Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Dialysis Dose and Body Mass Index Are Strongly Associated with Survival in Hemodialysis Patients
 J Am Soc Nephrol 13: 1061 1066, 2002 Dialysis Dose and Body Mass Index Are Strongly Associated with Survival in Hemodialysis Patients FRIEDRICH K. PORT, VALARIE B. ASHBY, RAJNISH K. DHINGRA, ERIK C. ROYS,
J Am Soc Nephrol 13: 1061 1066, 2002 Dialysis Dose and Body Mass Index Are Strongly Associated with Survival in Hemodialysis Patients FRIEDRICH K. PORT, VALARIE B. ASHBY, RAJNISH K. DHINGRA, ERIK C. ROYS,
The CARI Guidelines Caring for Australians with Renal Impairment. Mode of dialysis at initiation GUIDELINES
 Date written: September 2004 Final submission: February 2005 Mode of dialysis at initiation GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: September 2004 Final submission: February 2005 Mode of dialysis at initiation GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Why Consider Home Dialysis? Empower the patient!
 Why Consider Home Dialysis? Empower the patient! Michael Kraus, MD FACP Professor of Clinical Medicine Indiana University School of Medicine Arguments against increased frequency home dialysis 1. Too small
Why Consider Home Dialysis? Empower the patient! Michael Kraus, MD FACP Professor of Clinical Medicine Indiana University School of Medicine Arguments against increased frequency home dialysis 1. Too small
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Status of the CKD and ESRD treatment: Growth, Care, Disparities
 Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
mean hemoglobin 11 g/dl (110 g/l) compared to patients with lower mean hemoglobin values (Table 20).
 compared to patients with lower mean hemoglobin values (Table 20).") S44 Figure 53 depicts the trend in Epoetin dosing from the 1998 study period to the 2003 study period, with an increasing mean weekly Epoetin dose (units/kg/wk) for patients prescribed Epoetin in lower
S44 Figure 53 depicts the trend in Epoetin dosing from the 1998 study period to the 2003 study period, with an increasing mean weekly Epoetin dose (units/kg/wk) for patients prescribed Epoetin in lower
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI
 HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Lesson #7: Quality Assessment and Performance Improvement
 ESRD Update: Transitioning to New ESRD Conditions for Coverage Student Manual Lesson #7: Quality Assessment and Performance Improvement Learning Objectives At the conclusion of this lesson, you will be
ESRD Update: Transitioning to New ESRD Conditions for Coverage Student Manual Lesson #7: Quality Assessment and Performance Improvement Learning Objectives At the conclusion of this lesson, you will be
PART FOUR. Metabolism and Nutrition
 PART FOUR Metabolism and Nutrition Advances in Peritoneal Dialysis, Vol. 22, 2006 Costas Fourtounas, Eirini Savidaki, Marilena Roumelioti, Periklis Dousdampanis, Andreas Hardalias, Pantelitsa Kalliakmani,
PART FOUR Metabolism and Nutrition Advances in Peritoneal Dialysis, Vol. 22, 2006 Costas Fourtounas, Eirini Savidaki, Marilena Roumelioti, Periklis Dousdampanis, Andreas Hardalias, Pantelitsa Kalliakmani,
Hemodiafiltration: principles and advantages over conventional HD. Rukshana Shroff Great Ormond Street Hospital for Children London, UK
 Hemodiafiltration: principles and advantages over conventional HD Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009
Hemodiafiltration: principles and advantages over conventional HD Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009
Prescriptions for Home Hemodialysis
 9 Prescriptions for Home Hemodialysis Robert Lockridge, MD 1 Tom Cornelis, MD 2 Carolyn van Eps, MBBS, PhD, FRACP 3 1 Lynchburg Nephrology Physicians, Lynchburg, Virginia, USA; 2 Department of Internal
9 Prescriptions for Home Hemodialysis Robert Lockridge, MD 1 Tom Cornelis, MD 2 Carolyn van Eps, MBBS, PhD, FRACP 3 1 Lynchburg Nephrology Physicians, Lynchburg, Virginia, USA; 2 Department of Internal
La relation dialyse et nutrition
 Nutrition en dialyse : controverses La relation dialyse et nutrition Charles Chazot, MD NephroCare Tassin-Charcot Sainte Foy Les Lyon, France HEMO study lessons (1) Dose Body weight flux Rocco, Kidney
Nutrition en dialyse : controverses La relation dialyse et nutrition Charles Chazot, MD NephroCare Tassin-Charcot Sainte Foy Les Lyon, France HEMO study lessons (1) Dose Body weight flux Rocco, Kidney
 IN THE NAME OF GOD Uremic toxins I. Small (< 500 D); water soluble Surrogate marker urea or sodium (ionic dialysance) Rapidly produced in intracellular fluid compartment Large variability in intra-patient
IN THE NAME OF GOD Uremic toxins I. Small (< 500 D); water soluble Surrogate marker urea or sodium (ionic dialysance) Rapidly produced in intracellular fluid compartment Large variability in intra-patient
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
NATIONAL QUALITY FORUM Renal EM Submitted Measures
 NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
NKF-DOQI CLINICAL PRACTICE GUIDELINES FOR HEMODIALYSIS ADEQUACY
 NKF-DOQI CLINICAL PRACTICE GUIDELINES FOR HEMODIALYSIS ADEQUACY 515 Acronyms and Abbreviations Abbreviation AAMI BUN EDW ESRD GFR HCFA HD HEMO NCDS NPCR PRU QALE RPA TCV TMP UFR UKM URR USRDS Term Association
NKF-DOQI CLINICAL PRACTICE GUIDELINES FOR HEMODIALYSIS ADEQUACY 515 Acronyms and Abbreviations Abbreviation AAMI BUN EDW ESRD GFR HCFA HD HEMO NCDS NPCR PRU QALE RPA TCV TMP UFR UKM URR USRDS Term Association
Adjusting hemodialysis dose - APPENDIX (6)
") Adjusting hemodialysis dose - APPENDIX 2014.06.10 1(6) Adjusting hemodialysis dose for protein catabolic rate Aarne J Vartia APPENDIX Main algorithm of the optimization procedure Qb and td are continuous
Adjusting hemodialysis dose - APPENDIX 2014.06.10 1(6) Adjusting hemodialysis dose for protein catabolic rate Aarne J Vartia APPENDIX Main algorithm of the optimization procedure Qb and td are continuous
Original Article. Introduction
 Nephrol Dial Transplant (2004) 19: 100 107 DOI: 10.1093/ndt/gfg418 Original Article Haemodialysis prescription, adherence and nutritional indicators in five European countries: results from the Dialysis
Nephrol Dial Transplant (2004) 19: 100 107 DOI: 10.1093/ndt/gfg418 Original Article Haemodialysis prescription, adherence and nutritional indicators in five European countries: results from the Dialysis
Incremental Hemodialysis
 The 25 th Budapest Nephrology School, 2018 Incremental Hemodialysis a story about Hemodialysis and the Residual Kidney Function - a fairy tale? Csaba Ambrus Szent Imre Teaching Hospital, Div. of Nephrology-Hypertension
The 25 th Budapest Nephrology School, 2018 Incremental Hemodialysis a story about Hemodialysis and the Residual Kidney Function - a fairy tale? Csaba Ambrus Szent Imre Teaching Hospital, Div. of Nephrology-Hypertension
Dialysis outcomes: can we do better?
 Dialysis outcomes: can we do better? Allan J. Collins, MD, FACP Professor of Medicine University of Minnesota Director, Chronic Disease Research Group Minneapolis Medical Research Foundation Director,
Dialysis outcomes: can we do better? Allan J. Collins, MD, FACP Professor of Medicine University of Minnesota Director, Chronic Disease Research Group Minneapolis Medical Research Foundation Director,
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001
 CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001") IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001 [Before completing please read instructions at the bottom of this page and on pages 4 and 5] PATIENT IDENTIFICATION MAKE
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001 [Before completing please read instructions at the bottom of this page and on pages 4 and 5] PATIENT IDENTIFICATION MAKE
FOUR. Clinical Indicators of Care
 Clinical Indicators of Care T FOUR The great questions of the time are not decided by speeches and majority decisions but by iron and blood. Otto von Bismarck, Speech to the Prussian Diet 78 ž 2000 ATLAS
Clinical Indicators of Care T FOUR The great questions of the time are not decided by speeches and majority decisions but by iron and blood. Otto von Bismarck, Speech to the Prussian Diet 78 ž 2000 ATLAS
chapter two clinical indicators and preventive care page
 chapter two clinical indicators and preventive care If you believe in magic don t bother to choose If it s jug band music or rhythm and blues Just go and listen it ll start with a smile It won t wipe off
chapter two clinical indicators and preventive care If you believe in magic don t bother to choose If it s jug band music or rhythm and blues Just go and listen it ll start with a smile It won t wipe off
Reprocessing dialysers for multiple uses: recent analysis of death risks for patients
 Nephrol Dial Transplant (2004) 19: 2823 2830 doi:10.1093/ndt/gfh460 Advance Access publication 17 August 2004 Original Article Reprocessing dialysers for multiple uses: recent analysis of death risks for
Nephrol Dial Transplant (2004) 19: 2823 2830 doi:10.1093/ndt/gfh460 Advance Access publication 17 August 2004 Original Article Reprocessing dialysers for multiple uses: recent analysis of death risks for
Haemodialysis. Online Clearance Monitoring Assuring the Desired Dose of Dialysis
 Haemodialysis Online Clearance Monitoring Assuring the Desired Dose of Dialysis Contents 1. Foreword 2. Dialysis dose 2.1 Standard methods of determination of the dialysis dose 2.1.1 Urea Reduction Ratio
Haemodialysis Online Clearance Monitoring Assuring the Desired Dose of Dialysis Contents 1. Foreword 2. Dialysis dose 2.1 Standard methods of determination of the dialysis dose 2.1.1 Urea Reduction Ratio
The Effect of High-Flux Hemodialysis on Dialysis-Associated Amyloidosis
 Renal Failure, 1:31-34, 2005 Copyright 2005 Taylor & Francis Inc. ISSN: 0886-022X print / 1525-6049 online DOI: 10.1081/JDI-200042868 Taylor & Francis Taylor 6. Francis Croup CLINICAL STUDY The Effect
Renal Failure, 1:31-34, 2005 Copyright 2005 Taylor & Francis Inc. ISSN: 0886-022X print / 1525-6049 online DOI: 10.1081/JDI-200042868 Taylor & Francis Taylor 6. Francis Croup CLINICAL STUDY The Effect
Hemodialysis: Techniques and Prescription
 CORE CURRICULUM IN NEPHROLOGY Hemodialysis: Techniques and Prescription T. Alp Ikizler, MD, and Gerald Schulman, MD INTRODUCTION HEMODIALYSIS (HD) is the routine renal replacement therapy for more than
CORE CURRICULUM IN NEPHROLOGY Hemodialysis: Techniques and Prescription T. Alp Ikizler, MD, and Gerald Schulman, MD INTRODUCTION HEMODIALYSIS (HD) is the routine renal replacement therapy for more than
Variable Included. Excluded. Included. Excluded
 Table S1. Baseline characteristics of patients included in the analysis and those excluded patients because of missing baseline serumj bicarbonate levels, stratified by dialysis modality. Variable HD patients
Table S1. Baseline characteristics of patients included in the analysis and those excluded patients because of missing baseline serumj bicarbonate levels, stratified by dialysis modality. Variable HD patients
Phil. J. Internal Medicine, 47: 19-23, Jan.-Feb., 2009
 Original Articles Assessment of Hemodialysis Adequacy 19 Phil. J. Internal Medicine, 47: 19-23, Jan.-Feb., 2009 ASSESSMENT OF HEMODIALYSIS ADEQUACY: IONIC DIALYSANCE IN COMPARISON TO STANDARD METHOD KT/V-MAKATI
Original Articles Assessment of Hemodialysis Adequacy 19 Phil. J. Internal Medicine, 47: 19-23, Jan.-Feb., 2009 ASSESSMENT OF HEMODIALYSIS ADEQUACY: IONIC DIALYSANCE IN COMPARISON TO STANDARD METHOD KT/V-MAKATI
You can sleep while I dialyze
 You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
Biochemical Analysis of End Stage Renal Disease Patients Following Regular Haemodialysis
 Original Research Biochemical Analysis of End Stage Renal Disease Patients Following Regular Haemodialysis Ipsita Dash 1,*, Suchitra Kumari 2 1 Tutor, 2 Assistant Professor, Dept. of Biochemistry, All
Original Research Biochemical Analysis of End Stage Renal Disease Patients Following Regular Haemodialysis Ipsita Dash 1,*, Suchitra Kumari 2 1 Tutor, 2 Assistant Professor, Dept. of Biochemistry, All
In-Center Hemodialysis Six Times per Week versus Three Times per Week
 Journal Club du 25 novembre 2010 In-Center Hemodialysis Six Times per Week versus Three Times per Week The FHN Trial Group N Engl J Med 2010 Frequent Hemodialysis Network Introduction fréquence? dose?
Journal Club du 25 novembre 2010 In-Center Hemodialysis Six Times per Week versus Three Times per Week The FHN Trial Group N Engl J Med 2010 Frequent Hemodialysis Network Introduction fréquence? dose?
I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY
 I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY GUIDELINE 1. INITIATION OF DIALYSIS 1.1 Preparation for kidney failure: Patients who reach chronic kidney disease (CKD) stage 4 (estimated
I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY GUIDELINE 1. INITIATION OF DIALYSIS 1.1 Preparation for kidney failure: Patients who reach chronic kidney disease (CKD) stage 4 (estimated
The Intact Nephron Hypothesis in Reverse: An Argument In Favor of Incremental Initiation Of Dialysis (With Residual Kidney Function)
") The Intact Nephron Hypothesis in Reverse: An Argument In Favor of Incremental Initiation Of Dialysis (With Residual Kidney Function) Thomas A. Golper MD, FACP, FASN Vanderbilt University Medical Center
The Intact Nephron Hypothesis in Reverse: An Argument In Favor of Incremental Initiation Of Dialysis (With Residual Kidney Function) Thomas A. Golper MD, FACP, FASN Vanderbilt University Medical Center
Aspetti nutrizionali nel paziente in emodialisi cronica
 Aspetti nutrizionali nel paziente in emodialisi cronica Enrico Fiaccadori enrico.fiaccadori@unipr.it Università degli Studi di Parma Agenda Diagnosis of protein-energy wasting (PEW) in ESRD on HD Epidemiology
Aspetti nutrizionali nel paziente in emodialisi cronica Enrico Fiaccadori enrico.fiaccadori@unipr.it Università degli Studi di Parma Agenda Diagnosis of protein-energy wasting (PEW) in ESRD on HD Epidemiology
CJASN epress. Published on July 1, 2010 as doi: /CJN
 CJASN epress. Published on July 1, 2010 as doi: 10.2215/CJN.02350310 Can Rescaling Dose of Dialysis to Body Surface Area in the HEMO Study Explain the Different Responses to Dose in Women versus Men? John
CJASN epress. Published on July 1, 2010 as doi: 10.2215/CJN.02350310 Can Rescaling Dose of Dialysis to Body Surface Area in the HEMO Study Explain the Different Responses to Dose in Women versus Men? John
Hemodiafiltration: practical points. Rukshana Shroff Great Ormond Street Hospital for Children London, UK
 Hemodiafiltration: practical points Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009 No benefit from increased
Hemodiafiltration: practical points Rukshana Shroff Great Ormond Street Hospital for Children London, UK Effectiveness of RRT modalities Mcfarlane, Seminars in dialysis, 2009 No benefit from increased
Clinical Performance Goals
 Clinical Performance Goals 2011-2012 Clinical Performance Goals 2011-2012 Table of Contents Table of Contents... 1 Health Care Quality Improvement Program... 2 Clinical Performance Measures... 6 Chapter
Clinical Performance Goals 2011-2012 Clinical Performance Goals 2011-2012 Table of Contents Table of Contents... 1 Health Care Quality Improvement Program... 2 Clinical Performance Measures... 6 Chapter
Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance
 Advances in Peritoneal Dialysis, Vol. 24, 2008 Rajesh Yalavarthy, Isaac Teitelbaum Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance Two indices of small-solute clearance, Kt/V urea and creatinine
Advances in Peritoneal Dialysis, Vol. 24, 2008 Rajesh Yalavarthy, Isaac Teitelbaum Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance Two indices of small-solute clearance, Kt/V urea and creatinine
Dialysis dose and frequency
 NDT Advance Access published December 14, 2004 Nephrol Dial Transplant (2004) 1 of 12 doi:10.1093/ndt/gfh550 Special Feature Dialysis dose and frequency Francesco Locatelli 1, Umberto Buoncristiani 2,
NDT Advance Access published December 14, 2004 Nephrol Dial Transplant (2004) 1 of 12 doi:10.1093/ndt/gfh550 Special Feature Dialysis dose and frequency Francesco Locatelli 1, Umberto Buoncristiani 2,
Adequacy of haemodialysis and nutrition in maintenance haemodialysis patients: clinical evaluation of a new on-line urea monitor
 Nephrol Dial Transplant (1996) 11: 1568-1573 Original Article IMephrology Dialysis Transplantation Adequacy of haemodialysis and nutrition in maintenance haemodialysis patients: clinical evaluation of
Nephrol Dial Transplant (1996) 11: 1568-1573 Original Article IMephrology Dialysis Transplantation Adequacy of haemodialysis and nutrition in maintenance haemodialysis patients: clinical evaluation of
Protocol. This trial protocol has been provided by the authors to give readers additional information about their work.
 Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: The FHN Trial Group. In-center hedialysis six times per week versus
Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: The FHN Trial Group. In-center hedialysis six times per week versus
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
M uch has been made of the excessive mortality experienced by dialysis patients in the United States. Even when adjusted for the severity of associ-
 Dialysis Survival in a Large Inner-City Facility: A Comparison to National Rates1 John C. Stivelman,2 J. Michael Soucie, Elizabeth S. Hall, and Edwin J. Macon J.C. Stivelman. ES. Hall. E.J. Macon, Department
Dialysis Survival in a Large Inner-City Facility: A Comparison to National Rates1 John C. Stivelman,2 J. Michael Soucie, Elizabeth S. Hall, and Edwin J. Macon J.C. Stivelman. ES. Hall. E.J. Macon, Department
Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University
 Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
Hypertension in Hemodialysis Patient Maher Fouad Ramzy; MD, FACP Professor of Renal Medicine, Cairo University Mechanism of HTN in HD patients Volume-dependent HTN ECV expansion. Volume-independent HTN
Geriatric Nutritional Risk Index, home hemodialysis outcomes 131
 Subject Index Aksys PHD system 113 Anemia, home outcomes 111, 172, 173 Automated peritoneal dialysis dialysis comparison 17, 18 selection factors 18, 19 telemedicine system 19 21 Blood pressure -peritoneal
Subject Index Aksys PHD system 113 Anemia, home outcomes 111, 172, 173 Automated peritoneal dialysis dialysis comparison 17, 18 selection factors 18, 19 telemedicine system 19 21 Blood pressure -peritoneal
Measurement of dialyzer clearance, dialysis time, and body size: Death risk relationships among patients
 Kidney International, Vol. 66 (24), pp. 277 284 Measurement of dialyzer clearance, dialysis time, and body size: Death risk relationships among patients EDMUND G. LOWRIE,ZHENSHENG LI,NORMA OFSTHUN, and
Kidney International, Vol. 66 (24), pp. 277 284 Measurement of dialyzer clearance, dialysis time, and body size: Death risk relationships among patients EDMUND G. LOWRIE,ZHENSHENG LI,NORMA OFSTHUN, and
Hemodialysis Adequacy 2006 Work Group Membership
 Hemodialysis Adequacy 2006 Work Group Membership Thomas A. Depner, MD University of California, Davis Sacramento, CA Work Group Co-Chairs John T. Daugirdas, MD University of Illinois Medical Center Chicago,
Hemodialysis Adequacy 2006 Work Group Membership Thomas A. Depner, MD University of California, Davis Sacramento, CA Work Group Co-Chairs John T. Daugirdas, MD University of Illinois Medical Center Chicago,
ad e quate adjective \ˈa-di-kwət\
 PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
Gender, low Kt/V, and mortality in Japanese hemodialysis patients: Opportunities for improvement through modifiable practices
 Original Articles Gender, low Kt/V, and mortality in Japanese hemodialysis patients: Opportunities for improvement through modifiable practices Naoki KIMATA, 1 Angelo KARABOYAS, 2 Brian A. BIEBER, 2 Ronald
Original Articles Gender, low Kt/V, and mortality in Japanese hemodialysis patients: Opportunities for improvement through modifiable practices Naoki KIMATA, 1 Angelo KARABOYAS, 2 Brian A. BIEBER, 2 Ronald
Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis
 IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
IAMHD HOME HEMODIALYSIS CLINICAL PRACTICE STANDARDS AND PROCEDURES Phosphate Management Guideline for Patients Receiving Extended Duration Hemodialysis PRINTED copies of Clinical Practice Standards and
Nutrition in end-stage renal disease
 Kidney International, Vol. 50 (1996), pp. 343 357 PERSPECTIVES IN CLINICAL NEPHROLOGY Nutrition in end-stage renal disease Despite substantial improvements in the science and technology of renal replacement
Kidney International, Vol. 50 (1996), pp. 343 357 PERSPECTIVES IN CLINICAL NEPHROLOGY Nutrition in end-stage renal disease Despite substantial improvements in the science and technology of renal replacement
Acid-base profile in patients on PD
 Kidney International, Vol. 6, Supplement 88 (23), pp. S26 S36 Acid-base profile in patients on PD SALIM MUJAIS Renal Division, Baxter Healthcare Corporation, McGaw Park, Illinois Acid-base profile in patients
Kidney International, Vol. 6, Supplement 88 (23), pp. S26 S36 Acid-base profile in patients on PD SALIM MUJAIS Renal Division, Baxter Healthcare Corporation, McGaw Park, Illinois Acid-base profile in patients
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
Malnutrition and inflammation in peritoneal dialysis patients
 Kidney International, Vol. 64, Supplement 87 (2003), pp. S87 S91 Malnutrition and inflammation in peritoneal dialysis patients PAUL A. FEIN, NEAL MITTMAN, RAJDEEP GADH, JYOTIPRAKAS CHATTOPADHYAY, DANIEL
Kidney International, Vol. 64, Supplement 87 (2003), pp. S87 S91 Malnutrition and inflammation in peritoneal dialysis patients PAUL A. FEIN, NEAL MITTMAN, RAJDEEP GADH, JYOTIPRAKAS CHATTOPADHYAY, DANIEL
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
METABOLISM AND NUTRITION WITH PD OBESITY. Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle
 METABOLISM AND NUTRITION WITH PD OBESITY Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 Body Size in Patients New to Dialysis United States Body Mass Index, kg/m2 33 31
METABOLISM AND NUTRITION WITH PD OBESITY Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 Body Size in Patients New to Dialysis United States Body Mass Index, kg/m2 33 31
Control of hyperphosphatemia is a major goal in patients
 ORIGINAL ARTICLES Phosphorus Clearance Using Two Hemodialyzers Placed in Parallel Mitchell H. Rosner, 1,2 Allen Helmandollar, 1 Ryan Evans, 1 Emaad Abdel-Rahman 1 Division of Nephrology, 1 University of
ORIGINAL ARTICLES Phosphorus Clearance Using Two Hemodialyzers Placed in Parallel Mitchell H. Rosner, 1,2 Allen Helmandollar, 1 Ryan Evans, 1 Emaad Abdel-Rahman 1 Division of Nephrology, 1 University of
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE
 PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
2009 Nephrology Conference Tuesday March
 The Renal Network, INC. 2009 Nephrology Conference Tuesday March 10 2009 Advances in Dialysis i Therapies Quo Vadis? Carolyn Cacho Bowman MD Assistant Professor of Medicine, Case School of Medicine Medical
The Renal Network, INC. 2009 Nephrology Conference Tuesday March 10 2009 Advances in Dialysis i Therapies Quo Vadis? Carolyn Cacho Bowman MD Assistant Professor of Medicine, Case School of Medicine Medical
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond
 PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
5. Comparison of continuous cyclic peritoneal dialysis (CCPD) with CAPD in treatment for patients with ESRD.
 with CAPD in treatment for patients with ESRD.") Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, Lawrence P, Wallace S, Vale L, Cody
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, Lawrence P, Wallace S, Vale L, Cody
Predictors of Patient Survival in Continuous Ambulatory Peritoneal Dialysis 10-Year Experience in 2 Major Centers in Tehran
 Dialysis Predictors of Patient Survival in Continuous Ambulatory Peritoneal Dialysis 10-Year Experience in 2 Major Centers in Tehran Monir Sadat Hakemi, 1 Mehdi Golbabaei, 2 Amirahmad Nassiri, 3 Mandana
Dialysis Predictors of Patient Survival in Continuous Ambulatory Peritoneal Dialysis 10-Year Experience in 2 Major Centers in Tehran Monir Sadat Hakemi, 1 Mehdi Golbabaei, 2 Amirahmad Nassiri, 3 Mandana
DIALYSIS THE VIEW FROM THE OTHER SIDE
 DIALYSIS THE VIEW FROM THE OTHER SIDE Myriam Farah, MD, FRCPC Fellow in Hemodialysis Division of Nephrology, University of British Columbia October 2011 OBJECTIVES 1. Identify the limitations of conventional
DIALYSIS THE VIEW FROM THE OTHER SIDE Myriam Farah, MD, FRCPC Fellow in Hemodialysis Division of Nephrology, University of British Columbia October 2011 OBJECTIVES 1. Identify the limitations of conventional
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital
 Renal Dialysis Centre Hong Kong Sanatorium & Hospital") Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
State Profile for FY 2018 for Dialysis Patients and Facilities - STATE SAMPLE
 Dear State Surveyor: State Profile for FY 2018 for Dialysis Patients and Facilities - STATE SAMPLE This report is designed to provide a comparative summary of treatment patterns and patient outcomes for
Dear State Surveyor: State Profile for FY 2018 for Dialysis Patients and Facilities - STATE SAMPLE This report is designed to provide a comparative summary of treatment patterns and patient outcomes for
Medication burden in CKD-5D: impact of dialysis modality and setting
 Clin Kidney J (2014) 7: 557 561 doi: 10.1093/ckj/sfu091 Advance Access publication 11 September 2014 Clinical Research Medication burden in CKD-5D: impact of dialysis modality and setting Kathrine Parker,
Clin Kidney J (2014) 7: 557 561 doi: 10.1093/ckj/sfu091 Advance Access publication 11 September 2014 Clinical Research Medication burden in CKD-5D: impact of dialysis modality and setting Kathrine Parker,
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
Early Estimation of High Peritoneal Permeability Can Predict Poor Prognosis for Technique Survival in Patients on Peritoneal Dialysis
 Advances in Peritoneal Dialysis, Vol. 22, 2006 Hidetomo Nakamoto, 1,2 Hirokazu Imai, 2 Hideki Kawanishi, 2 Masahiko Nakamoto, 2 Jun Minakuchi, 2 Shinichi Kumon, 2 Syuichi Watanabe, 2 Yoshhiko Shiohira,
Advances in Peritoneal Dialysis, Vol. 22, 2006 Hidetomo Nakamoto, 1,2 Hirokazu Imai, 2 Hideki Kawanishi, 2 Masahiko Nakamoto, 2 Jun Minakuchi, 2 Shinichi Kumon, 2 Syuichi Watanabe, 2 Yoshhiko Shiohira,