HIMSS Davies Enterprise Award Submission
|
|
|
- Roberta Fisher
- 6 years ago
- Views:
Transcription
1 HIMSS Davies Enterprise Award Submission Applicant Organization: St. Clair Hospital Organization s Address: 1000 Bower Hill Road, Pittsburgh, PA, Submitter s Name: Richard J. Schaeffer Submitter s Title: VP and CIO Submitter s rich.schaeffer@stclair.org Core Item/Clinical Value: EHR support for organizational initiatives, including diabetes, C.diff, and pneumonia vaccine administration Executive Summary: St. Clair continually seeks opportunities to improve quality, reduce cost, and provide a positive patient experience. Consistent with this commitment, St. Clair Hospital is enrolled in Highmark s QualityBlue Pay-for-Performance program. Participation in this program assists the organization to approach challenging clinical improvements with a more focused effort, centered on improving quality, improving patient satisfaction and implementing evidence - based practices. Powered by tools within the EHR, improved clinical value was realized in the following areas: improved diabetes care, a reduction in C.diff infections, and improvements in the administration of pneumonia vaccine. Background Knowledge: St. Clair Hospital is a 328-bed independent, acute care facility that provides advanced, high quality health care to more than 480,000 residents of southwestern Pennsylvania. Our mission is to provide highly-valued, service oriented healthcare to our community across the hospital s main campus and five outpatient centers. The selected quality initiatives represented welldocumented risks to our patients and worthy of directed efforts at improvement. Leveraging tools within the EHR could help us achieve success in improving the care provided to our patients. Local Problem and Intended Improvement: 1. Diabetes The American Diabetes Association recently reported that diabetes is not only the 7 th leading cause of death, but over 9% of the US population has the disease. Accordingly, a self-assessment of the St. Clair experience related to diabetes care was conducted. In 2011, twenty-eight (28%) of patients had a primary diagnosis of diabetes. Several key improvements were desired, including data analysis to identify the rate of patients with hyperglycemia and severe hypoglycemia events, the identification of the percent of diabetic patients who, either prior to discharge or within 90 days of the hospital admission, received a hemoglobin A1C (HbA1c), and the implementation of evidence-based, standardized order sets and protocols. Diabetes is typically a secondary diagnosis, and patients with diabetes are managed across multiple nursing units. 1
2 2. Healthcare Infection Prevention In recent years, the CDC has reported that C.diff infections are at an all time high nationally, and have been linked to 14,000 annual deaths nationally. In 2011, the Hospital observed an undesirable upward trend in the frequency of C. diff infections. In an effort to address this potentially devastating condition, efforts were focused on reduction strategies. These included an improvement of the rate of C.diff per 10,000 patient days, as well as the use of protocols that restrict and reduce the overall use of antibiotics. To further drive the rate down, for FY2014, the Hospital established an organizational goal around C.diff reduction and tied it to the Hospital s organizational achievement award. Three levels of performance were established with the maximum target was set at 55 infections. 3. Pneumonia The CDC reports that more than 5,000 patient deaths occur as a result of pneumococcal infections and these infections are the sixth leading cause of death in the country. A significant number of these deaths were preventable had the patient received a pneumococcal vaccination. Beyond the CMS Core Measure requiring hospitals to report pneumococcal vaccination rates, St. Clair Hospital recognized this issue to be a major health care concern and sought an improvement in the number of patients discharged who were screened for pneumococcal vaccine status and received pneumococcal vaccine prior to discharge, if indicated. Design and Implementation: For each initiative, clinical improvement teams were established. Membership included physician champions, clinical leadership, quality, IT and bedside clinical staff. Members were selected based on knowledge, expertise and skill related to the specific goals that needed to be accomplished. All goals were assigned to the most appropriate team member and included accountability for achieving the desired outcome. Once this structure was established, assessments were conducted related to the current situation and the development of an action plan for improvement. For the St. Clair Diabetes protocol, our HIS team had to hardwire the clinical decision support into the EHR. First, the Diabetes Risk Assessment was added to the Patient Profile tab. Next, the electronic search and auto-population of diabetes history functionality was added. Finally, an automatic order was added to the system to schedule a HbA1c test if no record of a HbA1c test in the last three months is part of the patient s medical history. Our approach was to minimize unnecessary alerts that lead to alert fatigue. The selected diabetic process uses a question and answer dialog rather than leaning on an alert and provider reaction. Within the Patient Profile process, the nurse completes the Diabetes Risk Assessment, which automatically pulls in history of diabetes and history of A1C results. How Health IT Was Utilized: 2



3 Diabetes: To successfully pursue improved care for the population of diabetes patients, the EHR must first assist clinicians in identifying these patients using analytics to generate the Monthly Diabetes Report shown below. For example, a key focus for improvement was identifying patients who experienced blood glucose levels of greater than 180 mg/dl or less than 40 mg/dl. At the time of the admission, the EHR searches for a previously documented history of diabetes. For a positive history, the system then searches the patient s record for a documented Hemoglobin A1C result filed within the last 3 months. If the system finds none, the EHR interacts with the clinician by inquiring if an order is needed and, if yes, proceeds to place the order as depicted in the flow diagram below. Below, the top portion of the screen shot show the system finding the diabetes history and auto-selecting the Yes radio button during the Diabetes Risk Assessment. Likewise, the A1C test 3


4 within 3 months is also found, and again, the appropriate radio button is auto-selected for the nurse. In this screen shot, the search for the A1C within the last 3 months is unsuccessful and the auto-order of the test is entered. 4


5 To better communicate with care providers, the Hemoglobin A1C result is retrieved and added to the patient s discharge instructions via the Transition of Care Record. This document is available via the patient portal and patients are encouraged to take these instructions with them when they visit the next care provider. In addition, those providers able to access the EHR, can view this document online. Diabetes - Capturing Undiagnosed Patients For the process of identifying new diabetic patients, screening criteria was put in place early on in the patient s stay, as shown in the diagram below. Once identified, it is essential to ensure that these patients receive critical survival skills and appropriate follow up education. To support the key focus for improvement, identifying patients with blood glucose levels greater than 180 mg/dl or less than 40 mg/dl is conducted through the use of logic based on specific criteria, as shown in the flow diagram below. The EHR first searches for a filed blood 5

6 glucose result. Exceptions are built in to this logic so that patients with a known history of diabetes or those patients receiving medications known to increase blood glucose levels, are eliminated. Following this inclusion/exclusion criteria, only those patients with a possible new diabetes diagnosis remain. At this point, an order for a Hemoglobin A1C is generated. Once the Hemoglobin A1C result is filed, those patients with a result greater than 6.5 are pulled onto the Potential Diabetes Risk list, and are then referred to appropriate clinicians for review as diagramed in the workflow below. 6


7 The Subcutaneous Insulin Order Set shown below preselects orders for Outpatient Diabetes Education and Nutritional Counseling. 7


8 This is done so that the order will cross over to the Discharge Orders Reconciliation for the physician to address if the patient will need further education upon discharge. Once selected on the Discharge Orders Reconciliation, it will send an automatic referral to the Diabetes Center to contact the patient. Diabetes - Patient Glycemic Control New for 2014, a goal to improve the time between obtaining blood glucose levels and the delivery of meal trays was defined. A system report was designed based on each unit s meal delivery time. Care providers are then able to prioritize tray delivery based on the last BGM documented. Tray delivery is not to occur for those patients who have not yet had a blood glucose level obtained. The EHR also provides clinicians with ongoing 7-day trending reports for blood glucose levels and any insulin coverage required. Finally, all efforts were supported by revised protocols and 8
 rate was established.")
9 electronic order sets that were developed with evidence-based sliding scale orders and referrals for outpatient diabetes self-management education. Healthcare Infection Prevention In 2012, a targeted goal of 5% reduction in the C. diff infection (CDI) rate was established. Process goals included a coordinated and enhanced antibiotic stewardship and earlier identification and isolation of C. diff patients. In support of this goal, the EHR and the electronic infection prevention program, Theradoc, were utilized to define key data elements. These included the identification of healthcare-facility onset cases (HO), community onset cases (CO) and community onset, healthcare-facility associated cases (CO-HCFA). In addition, the system provided a report of Defined Daily Dose (DDD) for quinolones and cephalosporins. Using Theradoc s Infection Control assistant module daily, the St. Clair infection preventionists perform daily surveillance (Monday through Friday). Theradoc generates reports of patients with positive C.diff result in the designated timeframe. Here is an example of a real time microbiology report. 9


10 Patients with positive C.diff results are moved by the Infection Preventionist to the Infection Worklist. The Worklist serves as Infection Prevention's electronic worksheet of patients with potential Health-care associated infection. The Infection Preventionist can expand C.diff patient entry on the Infection Work List to access the Theradoc Infection Worksheet. Using the Worksheet, the Infection Preventionist can classify C.diff patient as healthcare associated or community acquired C.diff infection based on current CDC healthcare associated infection definitions. Theradoc interfaces with the EHR system (Allscripts SCM) to recover clinical symptoms to meet criteria such as temperature and 10
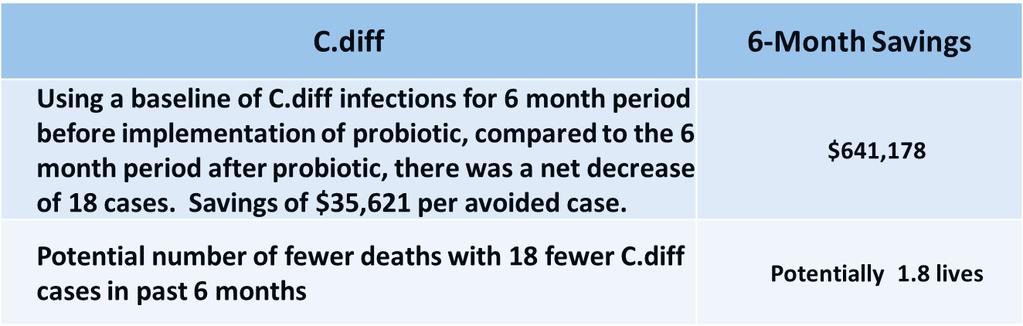
11 complete blood count (CBC.) The Infection Prevention also uses SCM to research nursing and physician progress notes for further information to meet criteria. The Infection Preventionist can pull reports of healthcare-associated infections identified in the Infection Report Context of Theradoc, for mandatory reporting to the CDC s National Healthcare Safety Network (NHSN) system. The reports are used for Infection Prevention Committees, Leadership, and frontline staff to identify trends and gaps so that interventions can be implemented to prevent C.diff infections. Introduction of Probiotic Treatment Based on current literature, including the November 2012 Annals of Internal Medicine, which concluded there is some evidence that probiotic prophylaxis results in large reduction in CDAD, the Pharmacy team members recommended the use of probiotics for patients receiving the known antibiotic-culprits for acquiring an HO episode of C. diff. As a result, further changes were added to key antibiotic order sets. Once the decision was made to implement the probiotic protocol, it was essential that the EHR deliver this capability seamlessly. This required several rounds of discussion to find the middle ground between the Pharmacy team members who advocated alert messages being triggered for the automatic order, and physician leadership who was not in favor of an extra click every time an antibiotic was ordered. Needless to say a compromise was reached and the probiotic auto-order is now a standard part of antibiotic ordering. Once the antibiotic is ordered, the EHR automatically enters the order for the probiotic. In the workflow shown below, the logic running behind the order entry screen determines if the medication is an antibiotic, and if so, examines whether it is an antiviral, antifungal, antimalarial, antituberculosis, or anthelmintic. It then compares the med to an exclusion list and further examines the patient type, patient age, the duration of the medication therapy, the ANC lab results, and potential probiotic duplication. If all criteria are met, the probiotic is autoordered. 11

12 Pneumonia: In January, 2011, 95% of patients were screened for vaccine status and administration, if appropriate. It was determined that the organization should strive for near 100% compliance. Evidence-based order sets were implemented. One year later, the number rose to 98%, closing the gap. However, more improvements were required. During the admission process, nurses reported that it was often difficult to ascertain whether the patient had received the vaccine in the past. Functionality within the EHR was designed to search the patient s past medical history. If the patient has no vaccine history documented, the EHR alerts the nurse to that fact and begins to assist the nurse in assessing whether the patient is appropriate to receive the vaccine. The EHR now searches for any chronic condition (as defined by the CDC) and asks the nurse to validate this information. Depending on that validation, an order for the pneumococcal vaccine is automatically placed, if appropriate. Once administered using bedside, bar-coded technology, the EHR automatically updates the vaccine history, facilitating ease of retrieval should the patient be admitted in the future. As the workflow in the diagram depicts, the logic embedded behind the scenes in the EHR performs the heavy lifting of searching the various sections of the patient s electronic chart to find evidence of a prior vaccine. 12

13 In addition, health issues are accessed to determine whether chronic or immunocompromising conditions are present and the appropriate radio button is autoselected. The Hospital s protocol rules are applied to appropriately select whether the vaccine should be ordered. By following the Protocol Rules flowchart below, the factors involved in determining the autoorder, and the sequence of decisions, can be seen. If it is determined that the patient should receive the vaccine, and the patient refuses, the nurse has the opportunity to record that. If the routine determines that the vaccine should not be ordered, the nurse cannot override and process the order. Finally, upon charting of the vaccine administration, an entry is recorded in the patient s health issues list. All of these automated portions of the workflow save the nurse time, and ultimately enable an efficient process. 13

14 Value/Derived Outcomes: Diabetes: The EHR was designed to provide results to the Diabetes Team, identifying those patients who experienced hyperglycemic episodes of greater than 180 mg/dl and severe hypoglycemia less than 70 mg/dl. In March, 2011, the incidence of hyperglycemia was 659 per 1,000 patient days. Hypoglycemia incidence was 55 per 1,000 patient days. It was clear that there was room for improvement. With physician engagement, a standardi zed, evidence-based subcutaneous order set was implemented, accompanied by a revised hypoglycemia protocol. Three years later, in March, 2014, the rate of hyperglycemic episodes dropped to 416 per 1,000 patient days. A refocus of hypoglycemia resulted in revised data collection for severe hypoglycemia, now defined as a blood sugar less than 40 mg/dl. In 2014, the rate of severe hypoglycemic episodes fell from 4.6 to a low of 1.86 per 1,000 patient days. The search for an HbA1c result with the last 90 days was conducted and reviewed. If the outcome was that there was no result, auto-ordering an HbA1C was triggered. Since the 2011 timeframe, this has consistently exceeded the established goal of 90%. Finally, time frames from the last blood glucose reading to meal delivery time have been reduced to less than the targeted goal of 30 minutes or less, with the one exception being a 33 minute average in March Healthcare Infection Prevention: In 2012, positive outcomes were realized. The rate of HO-CDI reduction exceeded the targeted goal of a 5%. In 2013, at 61 cases of HO-CDI, the rate remained within the targeted range. However, beginning in fiscal 2014, the Hospital established the stretch goal of reducing the number of infection to 55 or less per year. During the first three (3) months, the Hospital was well off the pace to achieve the goal and additional actions had to be identified and implemented. After getting off to such a bad start, the Hospital was not successful in achieving the stretch goal of 55 or less infections for the 12-month period. However, over the final 6 months of the period, the rate of infection was well below the pace necessary to stay below 55, and leads to optimism for the next 12 months. The use of probiotics is still considered an evolving subject of 14


15 study as a mechanism for the prevention of C.diff, and it is therefore difficult to draw a direct correlation between its use and the decreased rate of infection. However, the implementation of the auto-ordering feature of the EHR was identified as a key intervention, and the rate of C.diff infection did decrease thereafter. Pneumonia: In January, 2010, 95% of patients were screened for their current vaccine status and administered the vaccine if appropriate. In January, 2013, 100% of patients met the measure. This has been sustained with little fluctuation. 15
16 Lessons Learned: Although it may seem that there is organizational consensus, and a level of urgency surrounding the implementation of clinical decision support, in the case auto-ordering the probiotic, different stakeholders were firm in their views on exactly how it should be implemented. For example, pharmacy advocated a detailed alert to be presented to the physician. Physician leadership was firm in their belief an alert box was unnecessary. Expecting clinicians to readily adopt and apply a new best practice, will have only limited success. To achieve the desired adoption, it must be hardwired into the EHR so that it happens automatically. The use of probiotics has been advocated for some time, but the compliance was inconsistent until it became an automatic function of the EHR. Improvement can be achieved on particular quality measures, and despite having the same solutions in place and functioning as expected, there are variables that arise that erode the gains, and new solutions have to be put in place to recover the gains. Identification of chronic disease patients is fundamental to many quality initiatives and yet these cohorts are not always pre-defined in the EHR. Without a disease registry module, the chronic disease patient lists must be created in the EHR. Specific for diabetic identification and treatment o Not every newly diagnosed diabetic patient is ordered insulin. Listen to the front line staff. They identified the gap in the order sets for protocol IV fluids. o Establishing systems to support patients continued use of their insulin pumps during hospitalization is challenging. Champions must increase staff awareness and confidence with implementing intervention of initiating IV fluids with dextrose or adding them to existing fluids. o Collecting data related to monitoring time between blood glucose measurement and tray delivery is a challenge. It is expected the EHR s elapsed time feature will help to further automate this task and provide analytic reporting. Financial Considerations: The Diabetes program required the following capital/staff investments totaling $68,513: o Lab procedures (Glycohemoglobin A1C- One per Admission)- $12,557 o Total labor costs (meeting time, lab time, HIS team) was calculated to total $54,286 to implement IT and execute the diabetic protocols. o Over 1400 education packets were developed and distributed to staff ($1,671) The reduction of hospital acquired infections represents significant potential return on investment through cost avoidance and avoiding CMS Value Based Purchasing penalties. 16
17 17
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Creating a reminder for GSK vaccines in Allscripts Professional EHR
 Vaccine reminders Ensure timely and appropriate vaccine orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient care. Alerts
Vaccine reminders Ensure timely and appropriate vaccine orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient care. Alerts
Gaps In Successful EHR Implementations: The Challenges & Successes Of Providers In The Marketplace
 Gaps In Successful EHR Implementations: The Challenges & Successes Of Providers In The Marketplace A White Paper By Credible Behavioral Health, Inc. October 2016 Contents I. Introduction... 3 Ii. Findings
Gaps In Successful EHR Implementations: The Challenges & Successes Of Providers In The Marketplace A White Paper By Credible Behavioral Health, Inc. October 2016 Contents I. Introduction... 3 Ii. Findings
The MetroHealth System. Creating the HIT Organizational Culture at MetroHealth. Creating the HIT Organizational Culture
 CASE STUDY CASE STUDY The MetroHealth System Optimizing Health Information Technology to Increase Vaccination Rates The MetroHealth System in Cleveland, Ohio, was the first safety-net health care system
CASE STUDY CASE STUDY The MetroHealth System Optimizing Health Information Technology to Increase Vaccination Rates The MetroHealth System in Cleveland, Ohio, was the first safety-net health care system
Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes
 Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
QUALITY IMPROVEMENT TOOLS
 QUALITY IMPROVEMENT TOOLS QUALITY IMPROVEMENT TOOLS The goal of this section is to build the capacity of quality improvement staff to implement proven strategies and techniques within their health care
QUALITY IMPROVEMENT TOOLS QUALITY IMPROVEMENT TOOLS The goal of this section is to build the capacity of quality improvement staff to implement proven strategies and techniques within their health care
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care
 Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
SAGE. Nick Beard Vice President, IDX Systems Corp.
 SAGE Nick Beard Vice President, IDX Systems Corp. Sharable Active Guideline Environment An R&D consortium to develop the technology infrastructure to enable computable clinical guidelines, that will be
SAGE Nick Beard Vice President, IDX Systems Corp. Sharable Active Guideline Environment An R&D consortium to develop the technology infrastructure to enable computable clinical guidelines, that will be
Reach Out to Patients for Better Disease Management
 CASE STUDY Reach Out to Patients for Better Disease Management Logansport Memorial Hospital How automated reminders led to a higher compliance rate for overdue labs by diabetic patients. Quick Summary
CASE STUDY Reach Out to Patients for Better Disease Management Logansport Memorial Hospital How automated reminders led to a higher compliance rate for overdue labs by diabetic patients. Quick Summary
Systematic Improvement of Diabetes Care in the Inpatient Setting
 Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Success Story Systematic Improvement of Diabetes Care in the Inpatient Setting EXECUTIVE SUMMARY Texas Children s Hospital is improving the care delivery of its patients with diabetes, one of the most
Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital:
 Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital: Eugenio H. Zabaleta, Ph.D. Clinical Chemist OhioHealth Mansfield Hospital Reducing Readmissions and Improving Outcomes at
Reducing Readmissions and Improving Outcomes at OhioHealth Mansfield Hospital: Eugenio H. Zabaleta, Ph.D. Clinical Chemist OhioHealth Mansfield Hospital Reducing Readmissions and Improving Outcomes at
Section #3: Process of Change
 Section #3: Process of Change This module will: Describe a model of change that supported the development and implementation of a palliative care program in long term care. Describe strategies that assisted
Section #3: Process of Change This module will: Describe a model of change that supported the development and implementation of a palliative care program in long term care. Describe strategies that assisted
Report Reference Guide
 Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Quality Improvement through HIT
 Quality Improvement through HIT What is quality in healthcare? Safe Effective Patientcentered Timely Efficient Equitable Overview Reinforce a vision for using HIT to improve quality Share our approach
Quality Improvement through HIT What is quality in healthcare? Safe Effective Patientcentered Timely Efficient Equitable Overview Reinforce a vision for using HIT to improve quality Share our approach
CHI Franciscan. Matt Levi Director Virtual Health Services. March 31, 2015
 CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
CHI Franciscan Matt Levi Director Virtual Health Services March 31, 2015 Reflection / 2 Agenda Introduction and background Matt Levi Director of Franciscan Health System Virtual Health Katie Farrell Manager
Understanding the Dialysis Event Protocol and Avoiding Common Reporting Mistakes Alicia Shugart, MA
 Understanding the Dialysis Event Protocol and Avoiding Common Reporting Mistakes Alicia Shugart, MA Public Health Analyst Topics Dialysis Event Protocol Collecting data Reporting a numerator and denominator
Understanding the Dialysis Event Protocol and Avoiding Common Reporting Mistakes Alicia Shugart, MA Public Health Analyst Topics Dialysis Event Protocol Collecting data Reporting a numerator and denominator
P R O J E C T B U L L E T I N - F A L L I N T H I S I S S U E U P D A T E S F O R
 D I A B E T E S O B E S I T Y & N U T R I T I O N S T R A T E G I C C L I N I C A L N E T W O R K ( D O N S C N ) I N T H I S I S S U E U P D A T E S F O R P R O V I N C I A L D I A B E T E S I N P A T
D I A B E T E S O B E S I T Y & N U T R I T I O N S T R A T E G I C C L I N I C A L N E T W O R K ( D O N S C N ) I N T H I S I S S U E U P D A T E S F O R P R O V I N C I A L D I A B E T E S I N P A T
Report Reference Guide. THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1
 Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
NAVIFY Tumor Board NAVIFY
 NAVIFY Tumor Board Make the most informed personalized treatment decisions possible by leveraging innovative technologies and the latest scientific and clinical data WHAT S INSIDE Key Takeaways NAVIFY
NAVIFY Tumor Board Make the most informed personalized treatment decisions possible by leveraging innovative technologies and the latest scientific and clinical data WHAT S INSIDE Key Takeaways NAVIFY
CareLink. software REPORT REFERENCE GUIDE. Management Software for Diabetes
 CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
GLYCEMIC CONTROL SURVEY
 GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
Infection Control: Meeting the Challenge
 22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Infection Control: Meeting the Challenge Wednesday, June 5, 2:30 pm The data demands placed on Infection Control departments have significantly
Creating an alert for GSK vaccines in e-mds EHR
 Immunization Alerts in e-mds Ensure timely and appropriate immunization orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient
Immunization Alerts in e-mds Ensure timely and appropriate immunization orders and administration Keeping track of patient vaccination requirements is an important aspect in the delivery of ongoing patient
ZERO SUICIDE DATA ELEMENTS WORKSHEET
 ZERO SUICIDE DATA ELEMENTS WORKSHEET Description and Instructions This worksheet is intended to assist health and behavioral health care organizations in developing a data-driven, quality improvement approach
ZERO SUICIDE DATA ELEMENTS WORKSHEET Description and Instructions This worksheet is intended to assist health and behavioral health care organizations in developing a data-driven, quality improvement approach
How to Integrate Peer Support & Navigation into Care Delivery
 How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
How to Integrate Peer Support & Navigation into Care Delivery Andrew Bertagnolli, PhD Care Management Institute Why Integrate Peer Support into the Care Delivery Pathway? Improved health Increased feelings
Participants in the Program
 Type 2 Diabetes Performance Improvement Initiative: Chart Reviews Participants in the Program 318 clinicians have registered 192 have started the program 126 have started their initial chart review 26
Type 2 Diabetes Performance Improvement Initiative: Chart Reviews Participants in the Program 318 clinicians have registered 192 have started the program 126 have started their initial chart review 26
Knowledge to Practice; Applying New Skills
 Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
Knowledge to Practice; Applying New Skills Linda R. Greene, RN, BS, MPS,CIC UR Highland Hospital Rochester, NY linda_greene@urmc.rochester.edu Kim M. Delahanty, RN, BSN, PHN,MBA/HCM,CIC UCSD Health System
Prevention of Excessive Anticoagulation from Warfarin STARTER PACK WEBINAR #1
 Prevention of Excessive Anticoagulation from Warfarin STARTER PACK WEBINAR #1 Why is it important to reduce the incidence of excessive INRs? What is Excessive Anticoagulation? No national definition No
Prevention of Excessive Anticoagulation from Warfarin STARTER PACK WEBINAR #1 Why is it important to reduce the incidence of excessive INRs? What is Excessive Anticoagulation? No national definition No
C. Difficile Testing Protocol
 C. Difficile Testing Protocol Caroline Donovan, RN, BSN, ONC- Infection Control Practitioner Abegail Pangan, RN, MSN, CIC- Infection Control Practitioner U.S. NEWS & WORLD REPORT 2017 2018 RANKINGS Acute
C. Difficile Testing Protocol Caroline Donovan, RN, BSN, ONC- Infection Control Practitioner Abegail Pangan, RN, MSN, CIC- Infection Control Practitioner U.S. NEWS & WORLD REPORT 2017 2018 RANKINGS Acute
LOUISIANA MEDICAID PROGRAM ISSUED: 02/01/12 REPLACED: 02/01/94 CHAPTER 5: PROFESSIONAL SERVICES SECTION 5.1: COVERED SERVICES PAGE(S) 6
 6") Diabetes Education Management Training Diabetes self management training (DSMT) is a collaborative process through which recipients with diabetes gain knowledge and skills needed to modify behavior and
Diabetes Education Management Training Diabetes self management training (DSMT) is a collaborative process through which recipients with diabetes gain knowledge and skills needed to modify behavior and
Diabetes Quality Improvement Initiative
 Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
Diabetes Quality Improvement Initiative Community Care of North Carolina 2300 Rexwoods Drive, Ste. 100 Raleigh, NC 27607 (919) 745-2350 www.communitycarenc.org 2007 Background The Clinical Directors of
Blood Pressure Management: A Journey in Quality Improvement Phil E. Yphantides, M.D.
 Blood Pressure Management: A Journey in Quality Improvement Phil E. Yphantides, M.D. Medical Director, Urgent Care Hypertension and Diabetes Physician Champion Sharp Rees-Stealy Medical Group San Diego,
Blood Pressure Management: A Journey in Quality Improvement Phil E. Yphantides, M.D. Medical Director, Urgent Care Hypertension and Diabetes Physician Champion Sharp Rees-Stealy Medical Group San Diego,
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Statit pimd Client Panel. Guy March, Product Lead, Midas+ Statit
 Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
Statit pimd Client Panel Guy March, Product Lead, Midas+ Statit Statit pimd/ppr Statit Software Started ~25 years ago Currently serving 650 hospitals Guy March Working with Statit QC products for over
Over 425 Members Strong
 Quality Measurement 101: The Basics Camille Smith, MSW, MSPH Director, Member Education Karen Johnson, MS Senior Director, Quality Measurement October 8, 2015 2:00pm-3:00pm ET Over 425 Members Strong 2
Quality Measurement 101: The Basics Camille Smith, MSW, MSPH Director, Member Education Karen Johnson, MS Senior Director, Quality Measurement October 8, 2015 2:00pm-3:00pm ET Over 425 Members Strong 2
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Topics in Inpatient Glycemic Control
 Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
RESULTS REPORTING MANUAL. Hospital Births Newborn Screening Program June 2016
 RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
RESULTS REPORTING MANUAL Hospital Births Newborn Screening Program June 2016 CONTENTS GETTING STARTED... 1 Summary... 1 Logging In... 1 Access For New Hires... 2 Reporting Parental Refusals... 3 Adding
NDoc Reference for the July 2012 Patient Demographic Enhancements
 Summary: This document provides a summary of the patient demographic enhancements incorporated in the July 2012 Update, including changes to the entry of patient names, the charting of patient address
Summary: This document provides a summary of the patient demographic enhancements incorporated in the July 2012 Update, including changes to the entry of patient names, the charting of patient address
August 29, Dear Dr. Berwick:
 August 29, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 445-G Washington, DC 20201 Re: Proposed
August 29, 2011 Donald Berwick, MD Administrator Centers for Medicare & Medicaid Services U.S. Department of Health and Human Services 200 Independence Avenue, SW Room 445-G Washington, DC 20201 Re: Proposed
the rural primary care practice guide to Creating Interprofessional Oral Health Networks
 the rural primary care practice guide to Creating Interprofessional Oral Health Networks November 2017 2 purpose and background 3 getting started: developing a plan 4 activities and ideas for consideration
the rural primary care practice guide to Creating Interprofessional Oral Health Networks November 2017 2 purpose and background 3 getting started: developing a plan 4 activities and ideas for consideration
Costs and Limitations
 Costs and Limitations For Certified Healthcare IT EHR EMR Version 10.0 07/14/2017 Penn Medical Informatics Systems, Inc Costs and Limitations for EyeDoc EMR Version 10.0 Capability and Description 2014
Costs and Limitations For Certified Healthcare IT EHR EMR Version 10.0 07/14/2017 Penn Medical Informatics Systems, Inc Costs and Limitations for EyeDoc EMR Version 10.0 Capability and Description 2014
Successful Immunization Program For Health Care Workers and Residents in Long Term Care. By Vicky S Lyman, RN, BSN, ICP, WCC
 Successful Immunization Program For Health Care Workers and Residents in Long Term Care By Vicky S Lyman, RN, BSN, ICP, WCC OBJECTIVES 1. Learn Strategies to increase Health Care Workers Influenza vaccination
Successful Immunization Program For Health Care Workers and Residents in Long Term Care By Vicky S Lyman, RN, BSN, ICP, WCC OBJECTIVES 1. Learn Strategies to increase Health Care Workers Influenza vaccination
ACO Congress Conference Pre Session Clinical Performance Measurement
 ACO Congress Conference Pre Session Clinical Performance Measurement Lynne Rothney-Kozlak, MPH Interim VP, ACO Collaborative (Independent Consultant) October 25, 2010 Agenda for Presentation 1. The Framework
ACO Congress Conference Pre Session Clinical Performance Measurement Lynne Rothney-Kozlak, MPH Interim VP, ACO Collaborative (Independent Consultant) October 25, 2010 Agenda for Presentation 1. The Framework
Palliative Care Quality Improvement Program (QIP) Measurement Specifications
 Measurement Specifications") Palliative Care Quality Improvement Program (QIP) 2017-18 Measurement Specifications Developed by: QIP Team Contact: palliativeqip@partnershiphp.org Published on: October 6, 2017 Table of Contents Program
Palliative Care Quality Improvement Program (QIP) 2017-18 Measurement Specifications Developed by: QIP Team Contact: palliativeqip@partnershiphp.org Published on: October 6, 2017 Table of Contents Program
COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012
 COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012 INTRODUCTION/HISTORY OF PROJECT Colon cancer is easily treated and often cured when caught in the early stages. Yet, it remains the
COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012 INTRODUCTION/HISTORY OF PROJECT Colon cancer is easily treated and often cured when caught in the early stages. Yet, it remains the
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home
 Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Arts Administrators and Healthcare Providers
 Arts Administrators and Healthcare Providers Table of Contents Part One: Creating Music and Programs 2 Preparing to Start a Program 2 Finding Funding 2 Selecting Partner Arts Organizations or Healthcare
Arts Administrators and Healthcare Providers Table of Contents Part One: Creating Music and Programs 2 Preparing to Start a Program 2 Finding Funding 2 Selecting Partner Arts Organizations or Healthcare
BETTER WAYS TO PAY FOR CANCER CARE Creating Win-Win-Win Approaches for Oncologists, Cancer Patients, and Payers
 BETTER WAYS TO PAY FOR CANCER CARE Creating Win-Win-Win Approaches for Oncologists, Cancer Patients, and Payers Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform Physicians
BETTER WAYS TO PAY FOR CANCER CARE Creating Win-Win-Win Approaches for Oncologists, Cancer Patients, and Payers Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform Physicians
Summary Transforming healthcare for women and newborns
 Summary Transforming healthcare for women The Women s Strategic Plan 2016-2020 The Women s Declaration For more than 160 years, the Women s has led the advocacy and advancement of women s health and wellbeing
Summary Transforming healthcare for women The Women s Strategic Plan 2016-2020 The Women s Declaration For more than 160 years, the Women s has led the advocacy and advancement of women s health and wellbeing
Using Analytics for Value-Based Care
 Using Analytics for Value-Based Care John Cuddeback, MD, PhD Elizabeth Ciemins, PhD, MPH, MA AMGA Northwest Regional Meeting February 3, 2017 Seattle A Fundamental Change Is Underway Fee for Service MIPS
Using Analytics for Value-Based Care John Cuddeback, MD, PhD Elizabeth Ciemins, PhD, MPH, MA AMGA Northwest Regional Meeting February 3, 2017 Seattle A Fundamental Change Is Underway Fee for Service MIPS
16 th Annual IHA Stakeholders Meeting Session 2C
 16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
16 th Annual IHA Stakeholders Meeting Session 2C September 19, 2017 Hilton Los Angeles Airport Thank you to our Content Partner: Medication Adherence AppleCare Pharmacy Programs Confidential and proprietary.
Patricia Bax, RN, MS August 17, Reaching New York State Tobacco Users through Opt-to-Quit
 Patricia Bax, RN, MS August 17, 2015 Reaching New York State Tobacco Users through Opt-to-Quit Good Afternoon! Welcome Roswell Park Cessation Services and Opt-to-Quit Overview Featured Site: Stony Brook
Patricia Bax, RN, MS August 17, 2015 Reaching New York State Tobacco Users through Opt-to-Quit Good Afternoon! Welcome Roswell Park Cessation Services and Opt-to-Quit Overview Featured Site: Stony Brook
The Emerging Zero Suicide Paradigm Reducing Suicide for Those in Care. Julie Goldstein Grumet, PhD Mike Hogan, PhD August 28, 2014
 The Emerging Zero Suicide Paradigm Reducing Suicide for Those in Care Julie Goldstein Grumet, PhD Mike Hogan, PhD August 28, 2014 Moderator and Presenters Sarah A. Bernes, MPH, MSW Research Associate,
The Emerging Zero Suicide Paradigm Reducing Suicide for Those in Care Julie Goldstein Grumet, PhD Mike Hogan, PhD August 28, 2014 Moderator and Presenters Sarah A. Bernes, MPH, MSW Research Associate,
2017 CMS Web Interface Reporting
 2017 CMS Web Interface Reporting Measure Specification Review May 18, 2017 Sherry Grund, Telligen Mary Schrader, Telligen Medicare Shared Savings Program and Next Generation ACO Model DISCLAIMER This presentation
2017 CMS Web Interface Reporting Measure Specification Review May 18, 2017 Sherry Grund, Telligen Mary Schrader, Telligen Medicare Shared Savings Program and Next Generation ACO Model DISCLAIMER This presentation
A Framework for Optimal Cancer Care Pathways in Practice
 A to Guide Care Cancer Care A for Care in Practice SUPPORTING CONTINUOUS IMPROVEMENT IN CANCER CARE Developed by the National Cancer Expert Reference Group to support the early adoption of the A to Guide
A to Guide Care Cancer Care A for Care in Practice SUPPORTING CONTINUOUS IMPROVEMENT IN CANCER CARE Developed by the National Cancer Expert Reference Group to support the early adoption of the A to Guide
EmergencyKT: New Onset Diabetes, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg %
 EmergencyKT: New Onset, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg % Obtain: CBCD EP1 VBG Serum Ketone Hemoglobin A1c (for follow up) UA β-hcg (female at risk for pregnancy)
EmergencyKT: New Onset, Non-DKA Definition: ED patient with newly discovered hyperglycemia, >200 mg % Obtain: CBCD EP1 VBG Serum Ketone Hemoglobin A1c (for follow up) UA β-hcg (female at risk for pregnancy)
EHR Hospital Communication: September 7, 2016
 Page1 Please post / share this communication within 24 hours in your department/unit. Remember: Many answers/clarifications on EHR processes can be accessed through the EHR Intranet site or EHR Learning
Page1 Please post / share this communication within 24 hours in your department/unit. Remember: Many answers/clarifications on EHR processes can be accessed through the EHR Intranet site or EHR Learning
Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System
 Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System Tarush Kothari, MD, MPH Physician Informaticist, Northwell Health Laboratories Assistant Professor in Pathology and
Standardizing Detection of Acute Kidney Injury in an Integrated Delivery Health System Tarush Kothari, MD, MPH Physician Informaticist, Northwell Health Laboratories Assistant Professor in Pathology and
OneTouch Reveal Web Application. User Manual for Healthcare Professionals Instructions for Use
 OneTouch Reveal Web Application User Manual for Healthcare Professionals Instructions for Use Contents 2 Contents Chapter 1: Introduction...4 Product Overview...4 Intended Use...4 System Requirements...
OneTouch Reveal Web Application User Manual for Healthcare Professionals Instructions for Use Contents 2 Contents Chapter 1: Introduction...4 Product Overview...4 Intended Use...4 System Requirements...
Improved IPGM: Demonstrating the Value to both Patients and Hospitals
 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Mirus Metrics Process Companion
 Mirus Metrics Process Companion Contents Getting Started... 1 Executive Summary... 2 Key Functions... 3 Glossary... 4 Care Revenue... 5 Performance... 7 Planning (Mandatory Assessments)... 13 Planning
Mirus Metrics Process Companion Contents Getting Started... 1 Executive Summary... 2 Key Functions... 3 Glossary... 4 Care Revenue... 5 Performance... 7 Planning (Mandatory Assessments)... 13 Planning
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. November 12, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
USING THE WEBEX Q&A FEATURE
 USING THE WEBEX Q&A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions below to use the Q&A
USING THE WEBEX Q&A FEATURE All lines are placed on mute to block out background noises. However, you can send in questions to the panelists via the Q&A button. Follow the directions below to use the Q&A
Member-centered cancer care In Georgia
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Member-centered cancer care In Georgia Ira Klein, MD, MBA, FACP GASCO Annual Meeting September 5, 2015 > One
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Member-centered cancer care In Georgia Ira Klein, MD, MBA, FACP GASCO Annual Meeting September 5, 2015 > One
Executive Director Position Announcement August, 2018
 Executive Director Position Announcement August, 2018 Overview This is an excellent opportunity for a seasoned nonprofit leader with a proven ability to positively engage people to lead an organization
Executive Director Position Announcement August, 2018 Overview This is an excellent opportunity for a seasoned nonprofit leader with a proven ability to positively engage people to lead an organization
FY 2018 PERFORMANCE PLAN
 Home-Delivered Meals AAA/ADSD Rachel Coates x1727 & Helen King x1734 Program Purpose Enhance nutrition and socialization for home-bound adults age 60 and older and their caregivers, and persons with disabilities,
Home-Delivered Meals AAA/ADSD Rachel Coates x1727 & Helen King x1734 Program Purpose Enhance nutrition and socialization for home-bound adults age 60 and older and their caregivers, and persons with disabilities,
DRUG ORDERING & DISPENSING:
 STUDY DRUG: List the study drugs that will be used at your site based on your hospital formulary 1. Insulin Humulin R 2. Insulin Humalog 3. Insulin Lantus DRUG SUPPLY & STORAGE: Since study drugs are not
STUDY DRUG: List the study drugs that will be used at your site based on your hospital formulary 1. Insulin Humulin R 2. Insulin Humalog 3. Insulin Lantus DRUG SUPPLY & STORAGE: Since study drugs are not
Treating Emergency Room Opioid Withdrawal with Buprenorphine
 Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
Treating Emergency Room Opioid Withdrawal with Buprenorphine Monday, February 11th (3:45pm 4:30pm) Room W314B Christine Bucago, Advanced Practice Clinical Leader (Nursing), CAMH Jane Paterson, Director,
2017 Diabetes. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
About the Highmark Foundation
 About the Highmark Foundation The Highmark Foundation, created in 2000 as an affiliate of Highmark Inc., is a charitable organization and a private foundation that supports initiatives and programs aimed
About the Highmark Foundation The Highmark Foundation, created in 2000 as an affiliate of Highmark Inc., is a charitable organization and a private foundation that supports initiatives and programs aimed
10/25/2018. Welcome TPCA Lead the Way with Advanced Care Management. Introductions
 Welcome TPCA Lead the Way with Advanced Care Management Introductions Let s get to know a little about each other! What emr do you use? NextGen, GE Centricity, ecw, Athena, Allscripts, emds, other: How
Welcome TPCA Lead the Way with Advanced Care Management Introductions Let s get to know a little about each other! What emr do you use? NextGen, GE Centricity, ecw, Athena, Allscripts, emds, other: How
New Approach to Reducing Adverse Drug Events Anticoagulants Insulin Opioids
 New Approach to Reducing Adverse Drug Events Anticoagulants Insulin Opioids October 9, 2013 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association NYSPFP
New Approach to Reducing Adverse Drug Events Anticoagulants Insulin Opioids October 9, 2013 A partnership of the Healthcare Association of New York State and the Greater New York Hospital Association NYSPFP
This evaluation was funded by the Centers for Disease Control and Prevention
 Preventing Older Adult Falls: Evaluating the integration of Clinical Falls Prevention and the Electronic Health Record American Evaluation Association 2016 Meeting October 29, 2016 This evaluation was
Preventing Older Adult Falls: Evaluating the integration of Clinical Falls Prevention and the Electronic Health Record American Evaluation Association 2016 Meeting October 29, 2016 This evaluation was
Pandemic Flu Plan. Revision #7, September Reviewed: 5/06, 7/06, 9/06, 2/07, 12/08, 09/09 Revised: 6/06, 8/06, 9/06, 2/07, 03/09, 09/09
 Pandemic Flu Plan Revision #7, September 2009 Reviewed: 5/06, 7/06, 9/06, 2/07, 12/08, 09/09 Revised: 6/06, 8/06, 9/06, 2/07, 03/09, 09/09 Revision #7, May, 2009 Page 2 of 152 Disclaimer: This plan was
Pandemic Flu Plan Revision #7, September 2009 Reviewed: 5/06, 7/06, 9/06, 2/07, 12/08, 09/09 Revised: 6/06, 8/06, 9/06, 2/07, 03/09, 09/09 Revision #7, May, 2009 Page 2 of 152 Disclaimer: This plan was
Texas ereferral Project with Lonestar Circle of Care, NextGen, Alere Wellbeing and University of Texas at Austin Update Date: October 2014
 ereferral Project Summary Please describe the purpose / goals for your ereferral project. Give a description of the health care provider/system, why/how they were selected, and other relevant information.
ereferral Project Summary Please describe the purpose / goals for your ereferral project. Give a description of the health care provider/system, why/how they were selected, and other relevant information.
Riding the Current: Upstream and Downstream Approaches to Implement Adult Immunization Strategies
 Riding the Current: Upstream and Downstream Approaches to Implement Adult Immunization Strategies Paul Nguyen Community Health Partnership Connie Chung-Bohling California Department of Public Health Session
Riding the Current: Upstream and Downstream Approaches to Implement Adult Immunization Strategies Paul Nguyen Community Health Partnership Connie Chung-Bohling California Department of Public Health Session
Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services?
 the future of diabetes services?") Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services? Dr PARIJAT DE DUK Clinical Champion Clinical Lead for Diabetes & Endocrinology, Sandwell & West
Sandwell & West Birmingham integrated community care diabetes model (DICE) the future of diabetes services? Dr PARIJAT DE DUK Clinical Champion Clinical Lead for Diabetes & Endocrinology, Sandwell & West
LEVEL OF CARE GUIDELINES: PEER SUPPORT SERVICES OPTUM IDAHO MEDICAID
 OPTUM IDAHO LEVEL OF CARE GUIDELINES: PEER SUPPORT SERVICES IDAHO MEDICAID LEVEL OF CARE GUIDELINES: PEER SUPPORT SERVICES OPTUM IDAHO MEDICAID Guideline Number: BH803IDPSS_012017 Effective Date: July,
OPTUM IDAHO LEVEL OF CARE GUIDELINES: PEER SUPPORT SERVICES IDAHO MEDICAID LEVEL OF CARE GUIDELINES: PEER SUPPORT SERVICES OPTUM IDAHO MEDICAID Guideline Number: BH803IDPSS_012017 Effective Date: July,
2017 Davies Award. Kressly Pediatrics Case Studies SUSAN J. KRESSLY, MD, FAAP
 2017 Davies Award Kressly Pediatrics Case Studies SUSAN J. KRESSLY, MD, FAAP Who We Are Founded in 2004 by Dr. Kressly with a clear vision: 3 Board Certified Pediatricians Susan J. Kressly, MD Karen W.
2017 Davies Award Kressly Pediatrics Case Studies SUSAN J. KRESSLY, MD, FAAP Who We Are Founded in 2004 by Dr. Kressly with a clear vision: 3 Board Certified Pediatricians Susan J. Kressly, MD Karen W.
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
POPULATION TRACKER - DREAMED USER GUIDE
 POPULATION TRACKER - DREAMED USER GUIDE November 2018 IFU-0011 05 TABLE OF CONTENTS TABLE OF CONTENTS GENERAL INFORMATION... 1 Product Description... 1 Glooko Intended Use... 1 DreaMed Intended Use...
POPULATION TRACKER - DREAMED USER GUIDE November 2018 IFU-0011 05 TABLE OF CONTENTS TABLE OF CONTENTS GENERAL INFORMATION... 1 Product Description... 1 Glooko Intended Use... 1 DreaMed Intended Use...
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0
 Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
Solutions for Language Services in Healthcare
 Solutions for Language Services in Healthcare We improve communication between patients and providers to enhance patient care and reduce cost, while improving patient outcomes. InDemand partners with today
Solutions for Language Services in Healthcare We improve communication between patients and providers to enhance patient care and reduce cost, while improving patient outcomes. InDemand partners with today
Healthcare Personnel Safety Component. Healthcare Personnel Vaccination Module Influenza Vaccination Summary. Outpatient Dialysis Facilities
 Healthcare Personnel Safety Component Healthcare Personnel Vaccination Module Influenza Vaccination Summary Outpatient Dialysis Facilities National Center for Emerging and Zoonotic Infectious Diseases
Healthcare Personnel Safety Component Healthcare Personnel Vaccination Module Influenza Vaccination Summary Outpatient Dialysis Facilities National Center for Emerging and Zoonotic Infectious Diseases
Real World Patients: The Intersection of Real World Evidence and Episode of Care Analytics
 PharmaSUG 2018 - Paper RW-05 Real World Patients: The Intersection of Real World Evidence and Episode of Care Analytics David Olaleye and Youngjin Park, SAS Institute Inc. ABSTRACT SAS Institute recently
PharmaSUG 2018 - Paper RW-05 Real World Patients: The Intersection of Real World Evidence and Episode of Care Analytics David Olaleye and Youngjin Park, SAS Institute Inc. ABSTRACT SAS Institute recently
EXHIBIT 3: ASSESSMENT TABLE GUIDANCE DOCUMENT
 EXHIBIT 3: ASSESSMENT TABLE GUIDANCE DOCUMENT Programs seeking initial or renewal of accreditation with ABPTRFE demonstrate the extent to which they are achieving their mission by completing Exhibit 3:
EXHIBIT 3: ASSESSMENT TABLE GUIDANCE DOCUMENT Programs seeking initial or renewal of accreditation with ABPTRFE demonstrate the extent to which they are achieving their mission by completing Exhibit 3:
Leonard Wonnenberg, PA-C May 18, 2016
 Using EHR to Establish a Workflow Process for Referring Patients to Diabetes Self- Management/Chronic Disease Self-Management Programs Leonard Wonnenberg, PA-C May 18, 2016 Horizon Proprietary = Data +
Using EHR to Establish a Workflow Process for Referring Patients to Diabetes Self- Management/Chronic Disease Self-Management Programs Leonard Wonnenberg, PA-C May 18, 2016 Horizon Proprietary = Data +
EHR Developer Code of Conduct Frequently Asked Questions
 EHR Developer Code of Conduct Frequently Asked Questions General What is the purpose of the EHR Developer Code of Conduct? EHR Association (the Association) members have a long tradition of working with
EHR Developer Code of Conduct Frequently Asked Questions General What is the purpose of the EHR Developer Code of Conduct? EHR Association (the Association) members have a long tradition of working with
Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children s Hospital
 Improving Preventative Care in Pediatrics through Health and Technology: A Davies Story Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children
Improving Preventative Care in Pediatrics through Health and Technology: A Davies Story Session #206, March 8, 2018 Susan J. Kressly, MD, FAAP, Kressly Pediatrics Dr. Jacques Orces, D.O., Nicklaus Children
Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff
 QUILLEN ETSU PHYSICIANS Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff Task List The functionality of the Task List tab is the same, but the appearance has been slightly changed.
QUILLEN ETSU PHYSICIANS Allscripts Version 11.2 Enhancements Front Desk and Medical Records Staff Task List The functionality of the Task List tab is the same, but the appearance has been slightly changed.
Identifying Hypertension and Diabetes by Mastering IT
 Click to edit Master title style Identifying Hypertension and Diabetes by Mastering IT Bruce Maki, MA M-CEITA / Altarum Institute Gregory Makris, MD M-CEITA / Altarum Institute 6/16/2015 1 1 Altarum Institute
Click to edit Master title style Identifying Hypertension and Diabetes by Mastering IT Bruce Maki, MA M-CEITA / Altarum Institute Gregory Makris, MD M-CEITA / Altarum Institute 6/16/2015 1 1 Altarum Institute
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions
 Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Great Lakes Partners for Patients: Hospital Improvement Innovation Network - Encyclopedia of Measures Frequently Asked Questions Contents Great Lakes Partners for Patients: Hospital Improvement Innovation
Quality Payment Program: A Closer Look at the Proposed Rule for Year 3
 Quality Payment Program: A Closer Look at the Proposed Rule for Year 3 Sandy Swallow and Michelle Brunsen August 21, 2018 1 This material was prepared by Telligen, the Medicare Quality Innovation Network
Quality Payment Program: A Closer Look at the Proposed Rule for Year 3 Sandy Swallow and Michelle Brunsen August 21, 2018 1 This material was prepared by Telligen, the Medicare Quality Innovation Network
Welcome to CareLink Pro
 Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
HEALTHSTREAM LIVING LABS IN ACTION
 HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
HEALTHSTREAM LIVING LABS IN ACTION A CONVERSATION WITH: Mitchel T. Heflin MD, MHS Associate Professor of Medicine, Duke University School of Medicine Eleanor McConnell PhD, RN, GCNS-BC Associate Professor,
MedStar St. Mary s Hospital Pioneers In Quality Presentation. Presenter: Elizabeth Ballard, MSN, RN and Dawn Yeitrakis MS, RN, CEN
 MedStar St. Mary s Hospital Pioneers In Quality Presentation Presenter: Elizabeth Ballard, MSN, RN and Dawn Yeitrakis MS, RN, CEN 1 MedStar St. Mary's Hospital (MSMH) Mission & Vision Our Mission MedStar
MedStar St. Mary s Hospital Pioneers In Quality Presentation Presenter: Elizabeth Ballard, MSN, RN and Dawn Yeitrakis MS, RN, CEN 1 MedStar St. Mary's Hospital (MSMH) Mission & Vision Our Mission MedStar
FAMILY & CHILDREN S SERVICES STRATEGIC PLAN
 2014-2019 FAMILY & CHILDREN S SERVICES STRATEGIC PLAN WHO WE ARE Family & Children s Services is a leading provider of behavioral health care and family services for people of all ages in Tulsa and surrounding
2014-2019 FAMILY & CHILDREN S SERVICES STRATEGIC PLAN WHO WE ARE Family & Children s Services is a leading provider of behavioral health care and family services for people of all ages in Tulsa and surrounding
Agenda. Immunization Registry Reporting in Community Health Centers. Presented by: Ben Pierson Program Manager Health Information Exchange
 Immunization Registry Reporting in Community Health Centers Presented by: Ben Pierson Program Manager Health Information Exchange Agenda Introduction About OCHIN Vaccination support in EHR Immunization
Immunization Registry Reporting in Community Health Centers Presented by: Ben Pierson Program Manager Health Information Exchange Agenda Introduction About OCHIN Vaccination support in EHR Immunization
Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model
 1 Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model OneCity Health Webinar January 13, 2016 Overview of presentation 2 Approach to care model development Project overview
1 Approved Care Model for Project 3gi: Integration of Palliative Care into the PCMH Model OneCity Health Webinar January 13, 2016 Overview of presentation 2 Approach to care model development Project overview