Recurrent Diseases in the Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
|
|
|
- Abraham Heath
- 5 years ago
- Views:
Transcription
1 Recurrent Diseases in the Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
2
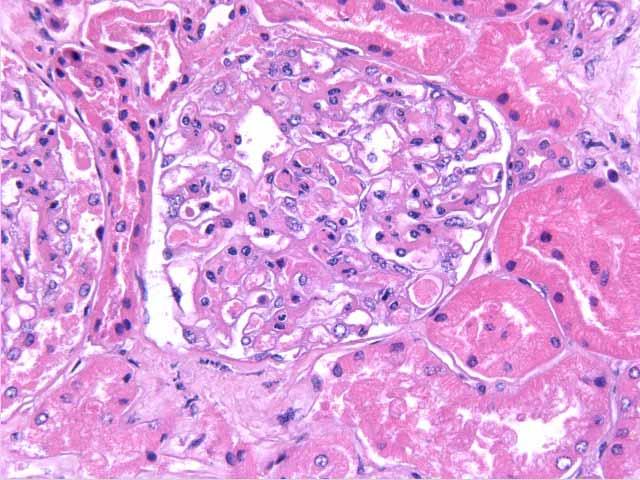
3 Case #1 21-year-old male, was on hemodialysis since September 2005 History of nephrotic range proteinuria and hematuria at the age of 3 Kidney biopsy (native): FSGS, treated with high dose steroids and Cytoxan Living-related kidney transplant 3/14/2006, Scr down to 1/7 mg/dl 3/27/06: On 6 mg TID of Prograf, Scr 2.0 mg/dl, urine protein/creat ratio 2.2, platelets 120,000 Transplant biopsy done
4
5
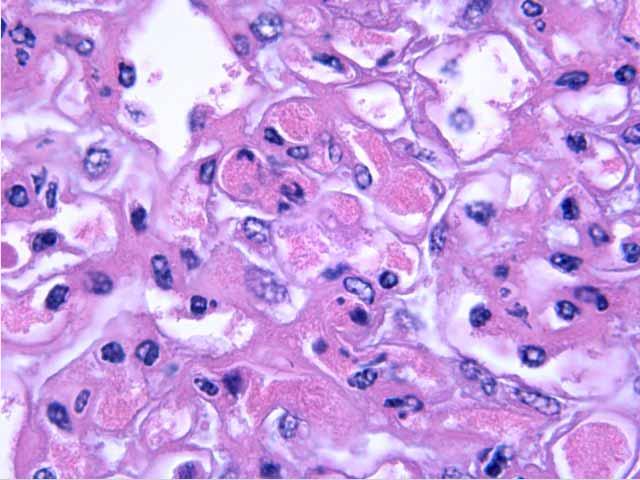
6 Case #1 Kidney biopsy: Small numbers of glomerular capillary platelet thrombi consistent with thrombotic microangiopathy Acute tubular necrosis No evidence for rejection Extensive visceral epithelial foot process effacement, most likely early recurrence of a sclerosing glomerulopathy
7 Case #1 Clinical course: Prograf dose decreased to a level around 4 (TAC 4 mg bid), also on MMF, prednisone Plasmapheresisx10 treatment Urine protein/creat ratio is down to 0.2, platelets >150,000 Repeat kidney biopsy 6/1/06: no rejection, no TMA, early FSGS Last clinic visit (17 months after surgery): on valsartan, lisinopril and spironolactone, Scr 1.7 mg/dl, urine prot/creat ratio: 4.5
8 Case #2 37 yo male, biopsy-proven FSGS, treated with high dose steroids, Cytoxan, azathioprine, and cyclosporine Started PD in January 2002 Received a CAD kidney in August never worked Transplant nephrectomy in October 2005 Second CAD kidney transplant on 11/30/2005
9 Case #2 1/30/06: urine protein/creat ratio: 5.8 Kidney biopsy 2/1/2006: Banff "Borderline changes", suspicious for early acute cellular rejection and mild mesangial proliferative glomerulopathy with significant effacement of the visceral epithelial foot processes as a background lesion for early FSGS
10 Case #2 Clinical course: Steroidsx3 (500 mg, IV) Plasmapheresisx10 Initial decrease in proteinuria to 1.7 g/d, then increased to 7.5 g/d Patient does not want to continue PE On Valsartan and ramipril, Scr mg/dl, protein/creatinine ratio: 11, kidney function worsened and started dialysis 14 months after surgery
11 Case #3 21 year old African American woman ESRD due to biopsy-proven lupus nephritis (class V) and h/o anti-cardiolipin antibody syndrome Living-unrelated kidney transplant from her husband ATS induction, on Neoral + Cellcept + Prednisone for maintenance
12 Case #3 Microscopic hematuria, proteinuria (2.7 g/day) and worsening kidney function (Scr 2.5 mg/d) Kidney biopsy: Focal proliferative GN with crescents and immune complexes (WHO class III, SLE) Solu-Medrol pulses (250 mg x 3), prednisone 60 mg/d
13 Case # 3 Severe herpes esophagitis and CMV infection ACE inhibitor, good blood pressure control, on 1000 mg twice a day Cellcept Returned to dialysis 8 years after transplantation
14 Recurrent Disease: Diagnosis Biopsy proven GN on native kidney Posttransplant proteinuria or hematuria or elevated creatinine Biopsy proven GN on kidney transplant
15 Risk of Graft Loss From Recurrent GN Recurrent GN 1505 patients with biopsy-proven GN from Australia ( ) The incidence of allograft loss due to recurrence at 10 years was 8.4% and increased overtime Most frequent causes of allograft loss at 10 years: 1. Chronic rejection, 2. Death with a functioning graft, 3. Recurrence Recurrence is more frequent than acute rejection as a cause of allograft loss during first 10 years after transplant Briganti EM, et al NEJM 2002
16
17
18 Recurrent GN in the Transplant The prevalence: 1.9%-31% in different series Higher prevalence in patients with ESRD due to biopsy-proven GN Higher recurrence: younger age, male gender, re-transplants, use of antilymphocytic serum for induction 1-8.4% of all graft failures are due to recurrent disease Recurrence is an important cause of allograft loss for those with ESRD due to GN
 Shimmura H, et al.")
19 Causes of Graft Loss (Living Kidney Transplantation from HLA- identical Sibling Donors) Shimmura H, et al. Int J Urol 2006

20 Causes of Graft Loss Shimmura H, et al. Int J Urol 2006
21 Recurrent GN in the Transplant Renal Allograft Disease Registry (RADR): 167 cases (3.4%) of recurrent and de novo diseases in 4913 renal transplants from 6 U.S. centers ( ) More men and a higher number of re-transplants in this group No difference according to the transplant type (LRD vs CAD) More graft failures (55% vs 25%, p<0.001) and shorter half-life in the recurrent disease group Hariharan S et al, Transplantation 1999
22 Recurrent GN in the Transplant (RADR Report) RADR findings: Recurrence FSGS (n= 57) 53% IgA nephropathy (n=22) 50% MPGN (n=18) 61% Membranous GN (n=16) 50% Diabetic nephropathy (n=19) 100% HUS/TTP (n=8) 100%
23 Risk Factors for Allograft Failure Cadaveric transplants Prolonged cold ischemia time (>20 hours) Elevated panel reactive antibody (>20%) The relative risk for graft failure because of recurrent and de novo disease was 1.9 The highest RR for graft failure: HUS/TTP (5.36), MPGN (2.37) and FSGS (2.25) Hariharan S et al, Transplantation 1999
24 A Prospective Study from RADR Recipients transplanted from /3216 (2.7%) with recurrent or de novo disease 853/3216 (26%) with prior native kidney biopsy, 36/853 (4.2) developed recurrence FSGS (7.4%), SLE (7.2%), MPGN (6.8%), and IgA (4.2%) Hussain SA et al, abstract #323, AST 2003

25 RECURRENT DISEASE AFTER KIDNEY TX: LITTLE PROGRESS IN 2 DECADES Sturdevant, M et al. WTC 2006, abstract#298
26 Recurrence After Transplantation Recurrence Graft Loss due to Rate Recurrence FSGS 20-50% 40-50% Anti-GBM disease 10-25% unusual Membranous GN 10-20% 50% IgA nephropathy 40-50% 6-33% Type I MPGN 20-30% 20-40% Type II MPGN 80-90% 10-20%
27 Recurrence After Transplantation Recurrence Graft Loss due Rate to Recurrence Henoch-Schönlein 15-35% 10-20% Lupus nephritis 1-25% Rare HUS 10-25% 50% Diabetic nephropathy 100% 5% Amyloidosis 2-33% 20% Wegener s 15-50% 10%
28 Choy BY, et al. Am J Transplant 2006
29
30 Recurrent FSGS Recurrence rate: 20-50% (difficult because of the focal nature of the distribution of lesions and possible sampling error) Graft loss: in ~50% of recurrent cases
31 Factors Contributing to Recurrence of FSGS Early onset (<15 years) of nephrotic syndrome Rapidly progressive FSGS in the native kidneys Race (more in African Americans), African- American kidney in a white recipient Diffuse mesangial proliferation on original kidney biopsy History of recurrence in a previous transplant
32 Factors Contributing to Recurrence of FSGS Circulating protein that alters glomerular capillary permeability? (Savin V, et al) Induction therapy with ALS (more with ATGAM) (Raafat R et al, Pediatr Nephrol 2000) Increased intra-graft NF-kappaB expression and intra-graft angiotensinogen gene expression (potential marker for recurrence?) (Schachter AD et al, Transplantation 2000) Patients with active FSGS or with posttx recurrence had oxidized plasma albumin-free radical involvement in FSGS Musante L, et al. J AM Soc Nephrol 2007
33 Recurrent FSGS NAPRTCS database, age year Clinical: malignant, diagnosis to dialysis is usually <3 years, nephrotic range proteinuria, ~75-80 % recurrence in the second graft Waiting 1-2 years between transplants Living-related vs cadaveric renal transplantation (controversial): Graft loss due to recurrent disease, no difference between LD (17%) or CAD (13.8%) grafts in NAPRTCS data Baum MA et al, Pediatr Transplantation 2002
34 Recurrent FSGS USRDS and US Scientific Renal Transplant Registry, ,414 patients in 19,259 adult primary renal transplant recipients Death-censored graft survival rates among FSGS patients Cibrik DM, Kaplan B, Campbell DA, Meier Kriesche H, AJT 2003
35 Recurrent FSGS Superior death-censored graft survival for FSGS patients who received a zero mismatch LD kidney vs HLA-mismatched CAD kidney Similar results in FSGS patients vs patients with other GN (zero mismatch LD kidney) Cibrik DM, Kaplan B, Campbell DA, Meier Kriesche H, AJT 2003
36 Five-year Death-censored Renal Allograft Survival (FSGS Vs Other GN)
37 Five-year Death-censored Renal Allograft Survival (FSGS)
38 Recurrent FSGS Limitations: retrospective, diagnosis of FSGS (biopsy-proven?), secondary causes of FSGS, incidence of recurrence Zero-mismatch LR transplant is NOT a risk factor for graft loss in FSGS, associated with significantly better death-censored renal allograft survival Cibrik DM, Kaplan B, Campbell DA, Meier Kriesche H, AJT 2003
39 Treatment for Recurrent FSGS 100 consecutive pediatric renal transplants 20 patients with FSGS, 8/20 (40%) with recurrence within 1 month of transplantation Plasmapheresis (mean: 24±17, range: 8-51 treatments to achieve a remission) in 5/6 pts One plasma volume was replaced with 5% albumin, 4 times per week then tapered when proteinuria decreased Greenstein SM et al, Pediatr Nephrol 2000
40 Treatment for Recurrent FSGS No prospective randomized studies Plasmapheresis ± dipyridamole (pre-or post transplant), 50% relapse after stopping plasmapheresis, nonresponders: sclerosis on biopsy, less effective in adults Pre-transplant plasmapheresis in children (retrospective data) Plasma protein adsorption High-dose cyclosporine, cyclophosphamide ACE inhibitors, NSAIDs, rapamycin use (Odama- Nwogu U et al, abstratc#55, AST 2003)
41 Pescovitz MD, Book BK, Sidner RA
42
43 FSGS and Transplantation There are not yet sufficient data for or against the use of prophylactic plasma exchange or other measure to prevent recurrent FSGS Native nephrectomy is not useful as a prevention
44 FSGS and Transplantation FSGS can recur in minutes after tx Massive proteinuria massive edema Posttx acute renal failure mimicking delayed graft function (DGF) Allograft biopsy-needed for diagnosis
45 FSGS and Transplantation Candidates with FSGS should be warned about the 30-50% risk of recurrence The risk of recurrence should not preclude transplantation Cadaveric versus LRD transplant (ethical issues) Should prior history of graft loss from recurrent FSGS be considered a relative contraindication to living donor transplantation (recurrence up to 80%)?
46 Recurrent IgA Nephropathy Recurrence rate: 40-60% Risk factors: -Younger age, HLA B35 and DR4 antigen -LRTx, high titers of serum IgA RF -Short interval between onset and ERSD -Glomerular crescents on original biopsy -Better donor/recipient HLA matching? -Greater number of rejections, previous h/o recurrence -IL-10 gene G-1082A polymorphism-worse outcome (Ivens K, et al ATC 2007, abstract#350)

47
48 Recurrent IgA Nephropathy Graft loss: 6-35% Clinical: microscopic hematuria ± proteinuria, worsening renal function, usually late recurrence, progression to ESRD is very slow Treatment: tonsillectomy (case reports from Japan), mycophenolate mofetil, high-dose fish oil, ACE inhibitors (WTC 2006 abstract#1790)
49 Recurrent Membranous Nephropathy (MN) Recurrence rate: 5%-42% Most cases are idiopathic, can be secondary to infectious agents (hepatitis B and C) or to SLE De novo MN is more frequent than recurrent MN Surveillance biopsies: 42% of patients developed histologic evidence of recurrence by 5 years, in most cases by 1-year post-tx. Minor clinical manifestations at diagnosis-mayo Clinic exp. Dabade TS, et al ATC 2007, abstract#351
50 Recurrent Membranous Nephropathy Graft loss: rare-30% Risk factors: male gender, rejection, HLAidentical living-related transplants Clinical: nephrotic range proteinuria, venous thrombosis of the allograft Treatment: Protein A immunoadsorption, pulse methylprednisolone and high-dose alternate day steroids, ACE inhibitors and MMF, early use of rituximab-mayo Clinic exp Cosio FG, et al ATC 2007, abstract#352
51 Recurrent MPGN Recurrence rate: % in type I, % in type II Graft loss: 40 % in type I, % in type II Risk factors: male gender, rapid progression to ESRD, massive proteinuria, identical LRD, recurrence on the first graft, HLA haplotype B8DR3 (Andresdottir et al, Transplantation 1997) *May mimic chronic allograft nephropathy
52 Recurrent MPGN Clinical: in secondary MPGN positive serology for hepatitis C ± cryoglobulinemia, low complement levels and rheumatoid factor, hematuria or proteinuria Treatment: Aspirin, steroids, cyclophosphamide, plasmapheresis is not useful

53 Rates of Graft Failure by Cause in the First 5 Years Post-Tx (per 100 patient-years) USRDS database, total n=140,109, MPGN=1,574 the rate of graft failure due to recurrent MPGN was more than 2-fold greater after TX in compared to TX in Kasiske, B, et al, WTC 2006, abstract#1765
54 Recurrent Lupus Nephritis (RLN) Recurrence rate: <10% in the literature Graft loss: reported rare Risk factors: active disease at the time of transplant (controversial), longer duration on dialysis before transplant (>25 weeks) Clinical: proteinuria, hematuria, and/or elevated serum creatinine, rarely extrarenal manifestations such as arthralgia, fever, skin rash and leukopenia
55
56
57
58
59 RLN-Vanderbilt Experience 50 SLE patients with at least 3 months of follow-up Induction with antithymocyte ab: 39 patients Immuno: AZA+pred (n=11), CsA (n=39), only 9 patients on CsA+MMF+pred Mean follow-up: 6.8±4.9 years; biopsy in 31 patients (62%) Recurrence rate: 52% of the patients biopsied, 30% of total patients One graft loss due to recurrent SLE Goral S et al, Transplantation 2003
60 RLN-Vanderbilt Experience Patient survival: 96% at 1 year, 82% at 5 years Graft survival: 87% at 1 year, 60% at 5 years No difference in graft survival between group 1 (RLN) and group 2 (no RLN) Graft survival was worse in patients who were biopsied compared to patients who never had any biopsies Worse outcome: one or more acute rejection and presence of chronic rejection Goral S et al, Transplantation 2003
 Kasiske, B et al, WTC 2006,")
61 Graft Failure Rates by Cause in the First 5 Years Post-Tx (per 100 patient-years) (USRDS database, total n=140,109, SLE=4,832) Kasiske, B et al, WTC 2006, abstract#1764
62 Recurrent Lupus Nephritis It is difficult to predict when RLN will occur after transplantation RLN can occur as early as 6 days after transplantation Surveillance biopsies might be helpful RLN may or may not have the same pattern as the original disease
63 Recurrent Lupus Nephritis Treatment: No definite treatment options (MMF), the impact of new immunosuppressive agents? Transplant kidney biopsy specimens from patients with history of ESRD due to SLE should be evaluated by both IF and EM in addition to LM (8 of 15 patients with RLN had mesangial LN)
64 Recurrent Diabetic Nephropathy Recurrence rate: up to 100% *Recurrence of GBM thickening and mesangial expansion 2 years beyond transplantation Reported as early as 2.5 years after transplant Graft loss: <5% in short-term,?predictor of graft loss Risk factors: suboptimal glycemic control (histological lesions are not observed in kidneypancreas recipients) Treatment: No studies
65 Recurrent Diabetic Nephropathy 58 patients; 74% had pretx-dm and 26% had posttx DM Biopsy proven diabetic nephropathy (done for clinical indications): 70% recurrent DN and 30% de novo DN De novo diabetic nephropathy at least as frequent as recurrent DN Bhalla V, Transplantation 2003
66 Recurrence of ANCA- Associated Vasculitis 35 patients with ANCA-associated vasculitis: microscopic polyangiitis (20 patients) and Wegener s granulomatosis (15 patients) The median time from diagnosis to transplantation: 25 months All patients in clinical remission 15 patients ANCA-positive at time of the transplant with 13 preemptive transplants Mean follow-up: 4.4±2.5 years Gera M, et al. Kidney Int 2007
67 Recurrence of ANCA-Associated Associated Vasculitis Antibody induction, steroids, mycophenolate mofetil, and tacrolimus Biopsy-proven AR in 6 recipients (23%) and BK nephropathy in 3 recipients (6%) Overall and death-censored graft survivals were 94 and 100%, respectively, 5 years posttransplantation Relapse of vasculitis in three of 35 patients (8.6% all nonrenal, reported up to 20% relapse rate in the literature-50% renal involvement) Gera M, et al. Kidney Int 2007
68 Recurrent Hemolytic Uremic Syndrome Recurrence rate: 13-50% Graft loss: 10-50% Risk factors: older age at onset of HUS, shorter interval between HUS onset and transplantation, LRDs, the use of calcineurin inhibitors (a meta-analysis, Ducloux D et al, Transplantation 1998) Clinical: microangiopathic hemolytic anemia, thrombocytopenia, worsening renal function *Sporadic HUS generally does not recur
69 Potential Problems for Identifying Recurrent GN in the Transplant No unified approach for patients with urinary abnormalities and increased serum creatinine after transplantation (histological vs clinical diagnosis) Primary disease is unknown for many patients Transplant biopsy is not routinely submitted for IF and EM examination
70 Potential Problems for Identifying Recurrent GN in the Transplant Interpretation of the biopsy: DIFFICULT, de novo vs recurrent-mpgn vs chronic rejection vs changes already present in the grafted kidney Most of the studies are small and retrospective with variable follow-up periods (mostly shortterm, inconsistent f/u) *No randomized, prospective studies for different treatment regimens (only case reports: MMF promising)
71 Recommendations The selection of recipients and donors should be no different for patients with GN from other candidates for kidney transplantation Potential recipients and donors should, however, be informed of the risk of recurrence
72 Post-Transplant GN- Recurrent or De Novo The best predictor factors that correlated with graft survival were: Proteinuria <3.5 g [relative risk (RR) = 0.24, p = 0.017] Serum creatinine below 2.0 mg/dl (RR = 0.06, p = 0.016) at the time of biopsy The use of angiotensin-converting enzyme inhibitors (ACEI) (RR = 0.12, p = 0.005). The use of ACEI markedly improved one-yr graft survival rates (92% vs. 47%, p < 0.001) Requiao-Moura LR, et al. Clin Transplant 2007
73 Challenges/Recommendations Awareness of recurrence Why do certain primary diseases affecting the native kidney recur? Obtain an exact diagnosis of primary disease Clarify the causes of prior graft loss Careful urinalysis in renal transplant recipients Early histological evaluation-low threshold for biopsy Prospective studies for specific treatments in individual diseases
74 Future Studies Prospective trials/registries: Recurrence rate Living donor vs. cadaver transplantation Various immunosuppressive protocols History of prior dialysis The recurrence rate for degree of HLA mismatch Identify risk factors for recurrence
75 Future Studies Selective prospective, interventional studies to prevent, delay recurrence and modify progression for individual diseases Prevention and treatment of FSGS with plasmapheresis Prevention of SLE and IgA nephritis with mycophenolate mofetil in renal transplant recipients Role of sirolimus in de novo HUS/TTP Management of HUS/TTP with plasmapheresis
76
77 Oxalosis Recurrence rate: early experience very high recurrence with allograft loss, now better results with: 1. Early transplantation (GFR 20 ml/min) 2. Aggressive preoperative dialysis 3. High urine flow after surgery 4. Simultaneous/sequential liver and kidney transplants Liver transplant followed by a kidney transplant (56): superior death-censored graft survival compared with patients who received a cadaveric or living-donor kidney transplant alone (134) (Cibrik DM et al, Transplantation 2002)
78 Amyloidosis Living-related kidney transplantation in 23 patients with ESRD due to amyloidosis, 47 controls Familial Mediterranean fever (FMF) in 16 patients and primary (idiopathic) in 7 transplant recipients Five- and 10-year actuarial graft survival rates were similar in both groups (79.35% vs 84.04% and 65.92% vs 56.61%, respectively ) Five- and 10-year actuarial patient survival rates also were similar (80% vs 94% and 68% vs 87%, respectively) Sherif AM et al, Am J Kidney Dis 2003
79 Amyloidosis Only one recurrence 10 years after transplantation (4.3%) Maintenance colchicine More GI problems and low blood pressure Sherif AM et al, Am J Kidney Dis 2003 Twenty of 30 patients (67%), biopsy confirmed recurrence after transplant (mostly well-matched LRDs) Ozdemir B et al, Tissue Antigens 2002
80 Vasculitis or Anti-GBM Disease 43 patients: Wegener's granulomatosis (n = 8), microscopic polyangiitis (n = 7), renal limited vasculitis (n = 18) and anti-gbm disease (n = 10) Average follow-up: 62+/-57 months No graft was lost due to recurrence of the underlying disease Patient and graft survival at 5 years after transplantation were 77% and 60% More malignancies Deegens JK et al, Clin Nephrol 2003
81 Recurrent Fibrillary GN Recurrence rate: up to 50 % 14 patients reported in the literature Clinical: benign course, prolonged graft survival is possible No evidence of systemic disease No definite treatment modality
82 Risk of Recurrent Disease 1. Should a kidney from a live donor be used if the recipient has an increased risk of recurrent disease? 2. Is there a greater chance that the recipient will lose the allograft from recurrent disease if a relative donor is used? 3. Will the same disease recipient has some day cause renal failure in the donor?
83 Kidney Transplantation In Patients With Lupus Nephritis Utilizing Modern Immunosuppression 29 patients with lupus nephritis (26 females and 3 males; 13 AA, 13 W, 2 Asians and 1 Hispanic) Transplanted between 1/2000 and 6/2005 Treated uniformly with antibody induction and the combination of tacrolimus, MMF and prednisone Three patients (11%) were treated for acute rejection Goral S, et al. WTC 2006, abstract.
84 Kidney Transplantation In Patients With Lupus Nephritis Utilizing Modern Immunosuppression Of 13 patients biopsied, only 2 had LM, IF and EM done, only one had recurrent lupus nephritis (5 years after the transplant) One-year graft and patient survival rates were 96% and 96%, respectively Three-year graft and patient survival rates were 88% and 88%, respectively Could this be due to uniform use of MMF in combination with tacrolimus in this population? The impact of this immunosuppressive combination on long-term survival and recurrence remains to be seen
Recurrent Diseases After Transplantation. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Recurrent Diseases After Transplantation Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History
Recurrent Diseases After Transplantation Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Many patients receiving renal allografts become identified simply
 Recurrent Disease in the Transplanted Kidney Jeremy B. Levy Many patients receiving renal allografts become identified simply as recipients of kidney transplantation. All subsequent events involving changes
Recurrent Disease in the Transplanted Kidney Jeremy B. Levy Many patients receiving renal allografts become identified simply as recipients of kidney transplantation. All subsequent events involving changes
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
Kidney Transplant Outcomes In Elderly Patients. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 28 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 28 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
Cases: CMV, HCV, BKV and Kidney Transplantation. Simin Goral, MD University of Pennsylvania Medical Center
 Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Pathology and Management of Chronic Allograft Dysfunction. Simin Goral, MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Pathology and Management of Chronic Allograft Dysfunction Simin Goral, MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Mission Impossible? PLAN To review the description of chronic
Pathology and Management of Chronic Allograft Dysfunction Simin Goral, MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Mission Impossible? PLAN To review the description of chronic
Lupus and Your Kidneys. Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia
 Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Chapter 8: ESRD Among Children, Adolescents, and Young Adults
 Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report. Renal Transplantation. Chronic Renal Insufficiency
 2005 Annual Report. Renal Transplantation. Chronic Renal Insufficiency") North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2006 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2006 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Literature Review: Transplantation July 2010-June 2011
 Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Long-term prognosis of BK virus-associated nephropathy in kidney transplant recipients
 Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function
 ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Chapter 6: Transplantation
 Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Lupus nephritis. Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic
 Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
Lupus nephritis Vladimir Tesar Department of Nephrology, General University Hospital, Prague, Czech Republic Disclosure of Interests Abbvie, Amgen, Baxter, Bayer, Boehringer-Ingelheim, Calliditas, Chemocentryx,
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Renal transplantation
 NEPHROLOGY 2008; 13, S37 S43 doi:10.1111/j.1440-1797.2008.00996.x Renal transplantation Date written: November 2006 Final submission: July 2007 Author: Nigel Toussaint GUIDELINES No recommendations possible
NEPHROLOGY 2008; 13, S37 S43 doi:10.1111/j.1440-1797.2008.00996.x Renal transplantation Date written: November 2006 Final submission: July 2007 Author: Nigel Toussaint GUIDELINES No recommendations possible
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Hasan Fattah 3/19/2013
 Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Use of mycophenolate mofetil in steroid-dependent and -resistant nephrotic syndrome
 Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Progress in Pediatric Kidney Transplantation
 Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
RECURRENT GLOMERULONEPHRITIS RISK OF RENAL ALLOGRAFT LOSS FROM RECURRENT GLOMERULONEPHRITIS. Data Collection
 RISK OF RENAL ALLOGRAFT LOSS FROM RECURRENT GLOMERULONEPHRITIS ESTHER M. BRIGANTI, M.B., B.S., M.CLIN.EPI., GRAEME R. RUSS, M.B., B.S., PH.D., JOHN J. MCNEIL, M.B., B.S., PH.D., ROBERT C. ATKINS, M.B.,
RISK OF RENAL ALLOGRAFT LOSS FROM RECURRENT GLOMERULONEPHRITIS ESTHER M. BRIGANTI, M.B., B.S., M.CLIN.EPI., GRAEME R. RUSS, M.B., B.S., PH.D., JOHN J. MCNEIL, M.B., B.S., PH.D., ROBERT C. ATKINS, M.B.,
RATIONALE. K Without therapy, ANCA vasculitis with GN is associated. K There is high-quality evidence for treatment with
 http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
Glomerular Disease. January 16, Katharine Dahl, MD
 Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel
 Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel Department of Pediatric Nephrology Pamukkale University School of Medicine IgA Nephropathy The most common cause of primary
Current treatment recommendations in children with IgA nephropathy Selçuk Yüksel Department of Pediatric Nephrology Pamukkale University School of Medicine IgA Nephropathy The most common cause of primary
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Effects of pretransplant plasmapheresis and rituximab on recurrence of focal segmental glomerulosclerosis in adult renal transplant recipients
 ORIGINAL ARTICLE Korean J Intern Med 2014;29:482-488 Effects of pretransplant plasmapheresis and rituximab on recurrence of focal segmental glomerulosclerosis in adult renal transplant recipients Hoon
ORIGINAL ARTICLE Korean J Intern Med 2014;29:482-488 Effects of pretransplant plasmapheresis and rituximab on recurrence of focal segmental glomerulosclerosis in adult renal transplant recipients Hoon
Overview. Evaluation of Potential Kidney Transplant Recipients. Projected Years of Life in Patients with ESRD
 Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Epidemiology of CKD in Children
 Epidemiology of CKD in Children Ali Düzova, M.D. Hacettepe University Faculty of Medicine Pediatric Nephrology and Rheumatology Unit Ankara CKD Course 03 June 2011, İstanbul Aim & Plan Causes of CKD in
Epidemiology of CKD in Children Ali Düzova, M.D. Hacettepe University Faculty of Medicine Pediatric Nephrology and Rheumatology Unit Ankara CKD Course 03 June 2011, İstanbul Aim & Plan Causes of CKD in
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
CKD in Other Organ Transplants
 CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Management of a Recipient with a Failed Kidney Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
2017 CST-Astellas Canadian Transplant Fellows Symposium. Management of Renal Dysfunction in Extra Renal Transplants
 2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
2017 CST-Astellas Canadian Transplant Fellows Symposium Management of Renal Dysfunction in Extra Renal Transplants Jeffrey Schiff, MD Dr. Jeffrey Schiff is an Assistant Professor of Medicine at the University
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of steroid therapy GUIDELINES
 Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
Specific management of IgA nephropathy: role of steroid therapy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES Steroid therapy may protect against progressive
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy
 International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Chapter 7: ESRD among Children, Adolescents, and Young Adults
 Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Post Transplant Immunosuppression: Consideration for Primary Care. Sameh Abul-Ezz, M.D., Dr.P.H.
 Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Chapter 12: Lupus nephritis Kidney International Supplements (2012) 2, ; doi: /kisup
 2, ; doi: /kisup") http://www.kidney-international.org chapter 12 & 2012 KDIGO Chapter 12: Lupus nephritis Kidney International Supplements (2012) 2, 221 232; doi:10.1038/kisup.2012.25 INTRODUCTION This chapter makes treatment
http://www.kidney-international.org chapter 12 & 2012 KDIGO Chapter 12: Lupus nephritis Kidney International Supplements (2012) 2, 221 232; doi:10.1038/kisup.2012.25 INTRODUCTION This chapter makes treatment
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
Kidney transplantation 2016: current status and potential challenges
 Kidney transplantation 2016: current status and potential challenges 15/12/2016 BVN-SBN : State-of-the-Art on Kidney Transplantation Patrick Peeters Ghent University Hospital, Belgium Challenges in 2016
Kidney transplantation 2016: current status and potential challenges 15/12/2016 BVN-SBN : State-of-the-Art on Kidney Transplantation Patrick Peeters Ghent University Hospital, Belgium Challenges in 2016
LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE
 & LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
& LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić