New Horizons in Kidney Transplant: Preventing Antibody-Mediated Rejection in Sensitized Patients
|
|
|
- Christine Tyler
- 5 years ago
- Views:
Transcription
1 New Horizons in Kidney Transplant: Preventing Antibody-Mediated Rejection in Sensitized Patients Denis Glotz, MD, PhD Saint-Louis Hospital Paris, France Robert A. Montgomery, MD, DPhil, FACS The Johns Hopkins Hospital Baltimore, Maryland In conjunction with the 2014 World Transplant Congress, July 26-31, 2014, in San Francisco, California.
2 Faculty Disclosures Denis Glotz, MD, PhD, has a financial interest/relationship or affiliation in the form of: Grant/Research Support from CSL Behring and Thermo Fisher Scientific Inc. Speakers Bureau participant with Alexion; F. Hoffmann-Roche; Sanofi; and Thermo Fisher Scientific Inc. This activity has been jointly sponsored by the University of New Mexico School of Medicine, Office of Continuing Medical Education, and PVI, PeerView Institute for Medical Education. This activity is supported by an unrestricted educational grant from Alexion Pharmaceuticals. This symposium is not part of the WTC official educational program and the sessions and content are not endorsed by WTC.
3 Faculty Disclosures Robert A. Montgomery, MD, DPhil, FACS, has a financial interest/relationship or affiliation in the form of: Consultant for ipierian Inc. Grant/Research Support from Alexion; Genzyme Corporation, a Sanofi company; and ViroPharma Incorporated, a wholly owned subsidiary of Shire, PLC. Scientific Advisory for Astellas Pharma US, Inc.; and Gambro. This activity has been jointly sponsored by the University of New Mexico School of Medicine, Office of Continuing Medical Education, and PVI, PeerView Institute for Medical Education. This activity is supported by an unrestricted educational grant from Alexion Pharmaceuticals. This symposium is not part of the WTC official educational program and the sessions and content are not endorsed by WTC.
4 Presentation 1: Antibody-Mediated Rejection: Clinical Phenotypes Photo Pending Denis Glotz, MD, PhD Saint-Louis Hospital Paris, France


5 Rejection Is an Antibody Process 1 CDC: complement-dependent cytotoxicity; Ig: immunoglobulin. 1. Taylor CJ et al. Transplantation. 1989;48:

6 Hyperacute Rejection 1 1. Courtesy of Denis Glotz, MD, PhD.

7 Patterns of Gene Expression 1 Rejection A : 50% graft loss Rejection B: Toxicity; infection Rejection C: CAN Rejection D: Normal CAN: chronic allograft nephropathy rejection type III. 1. Sarwal M et al. N Engl J Med. 2003;349:


8 Patterns of Gene Expression 1 AR: acute rejection; HLA: human leukocyte antigen: IL: interleukin; IFN: interferon; NK: natural killer. 1. Sarwal M et al. N Engl J Med. 2003;349:125-38

9 Laboratory Diagnosis of DSA: Luminex Assay 1 High sensitivity and specificity for HLA antibody detection Detects many more antibodies than are observed by the less sensitive and less specific CDC assay AMR: antibody-mediated rejection. 1. Chen G et al. Methods Mol Biol. 2013;1034:


10 Immunohistochemistry Versus Immunofluorescence 1 Kidney IF IHC IFV: immunofluorescence; IH: immunohistochemistry:. 1. Courtesy of Dominique Nochy.
11 AMR in Renal Transplant 1 Histological lesions ATN PTC, glomerulopathy, thrombosis Arteritis C4d+ DSA ATN: acute tubular necrosis; DSA: donor-specific antibody; PTC: peritubular capillaritis.. 1. Racusen LC et al. Am J Transplant Jun;3(6):
12 C4d Positivity in Various Treatment Centers Authors Biopsies/Pts Indication C4d+ (% Pt) Feucht /93 Renal failure 46% Lederer /218 Renal failure 46%-72% Regele /61 Renal failure 51% Bohmig /58 Renal failure 28% Nickeleit /265 Renal failure 35% Herzenberg /93 Rejection 37% Mauiyyedi /67 Renal failure 30% Regele /213 Renal failure 34% Sund /37 Protocol 30% Koo /48 Protocol 13% 1. Courtesy of Denis Glotz, MD, PhD.

13 AMR in KTRs: Biopsies for Cause 1 KTR: kidney transplant recipient. 1. Lefaucheur C et al. J Am Soc Nephrol :

14 AMR: An Evolutive Process 1 Bringing together the pieces of the puzzle Quantitation DSA pre-tx graft survival Histology and graft survival? MFI: mean fluorescence intensity. 1. Lefaucheur C et al. J Am Soc Nephrol :

15 Subclinical AMR Function Pathology Usefulness of Abs/screening biopsies+++ Ab: antibody.



16 Defining Subclinical AMR 1-3 Patient in a steady state: Stable GFR Evidence for Ab injury: glomerulitis+/ptc+ Evidence for Ab action in PTC: C4d+ Evidence for serologic Ab: DSA+ GFR: glomerular filtration rate. 1. Gloor J et al. Am J Transplant. 2007;7: Haas M et al. Am J Transplant. 2007;7: Lerut E at al. Translantation 2007;83:


17 Anti-HLA Antibodies and Late Allograft Loss 1 GFR: glomerular filtration rate. 1. Lee PC et al. Transplantation ;74(8):


18 Proteinuria is the Hallmark of Glomerular Injury 1 The relationship between HLA Ab and proteinuria in KTR developing DSA and NDSA a Control group never developed antibodies. NDSA: non donor-specific antibodies. 1. Fotheringham J et al. Transplantation ;91(9):991-6.


19 It All Starts With Proteinuria 1 egfr: estimated glomerular filtration rate. 1. Fotheringham J et al. Transplantation. 2011;15:
:2532-41.")
20 Presence of DSA Frequent in Late Biopsies For Cause 1 DSA distribution in pts undergoing late biopsies for clinical indication PRA: panel-reactive antibody. 1. Hidalgo LG et al. Am J Transplant. 2009;9(11):


21 Development of De Novo DSA Is Associated With Allograft Loss 1 Graft survival of patients with de novo DSA versus those without Time From Transplant, y 1. Wiebe C et al. Am J Transplant. 2012;12:

22 Nature History of Subclinical AMR 1 Evolution of chronic lesions in DSA+ patients according to time of screening biopsy a CG a Mean +/- SEM, data including nine additional screening biopsies performed at 3 y. CG: chronic glomerulopathy; IF: interstitial fibrosis; SEM: standard error of measurement; TA: tubular atrophy. 1. Loupe A et al. Am J Transplant. 2009; 9:
23 AMR Is the Leading Cause of Late Graft Failure 1 PVN 7% Missing data 5% Medical conditions 10% GN 13% ABMR AMR 47% Nonadherent 48% Adherent 52% Mixed 5% Probable AMR 13% 65% of subsequent failures could be attributed to AMR, probable AMR, or mixed; 48% were nonadherent GN: glomerulonephritis; PVN: polyomavirus nephropathy. 1. Sellarés J et al. Am J Transplant. 2012;12:
24 The Spectrum of Clinical Phenotypes 1 Hyperacute Acute Caused when high titers of DSA are present Happens within min to d Rare (due to crossmatching) Occurs in 5%-7% of KTRs Causes 20%-48% of acute-rejection episodes in presensitized crossmatched patients Manifests over days as a result of DSA Chronic Antibody mediated Characteristically seen as TG on kidney biopsy TG prevalence in protocol biopsies varies from 5% at 1 y to 20% at 5 y Manifestations Early stages: asymptomatic Advanced stages: nephrotic-range proteinuria Hypertension Allograft dysfunction; progression may be fairly rapid TG: transplant glomerulopathy. 1. Puttarajappa C et al. J Transplant.2012;2012:193724

25 80 DSA+ KTRs: 157 Protocol Biopsies 1 C4d status fluctuates during the first-year post-transplant, reflecting a dynamic process C4d = 3 C4d = 2 C4d = 1 C4d = 0 1. Loupy A et al. Am J Transplant. 2009;9:
26 Is Complement Necessary for Antibody-Mediated Lesions? 1 Specificity/sensitivity/positive predictive and negative predictive values for C4d Sensitivity = 0.69 Specificity = 0.83 PPV = 0.93 NPV = 0.44 C4d+ (n = 90) KTRs with preformed DSA (n = 80) Protocol biopsies at 3-mo and 1-y post-transplant (n = 157) C4d- (n = 67) Microvascular inflammation + (n = 84) Microvascular inflammation (n = 6) Microvascular inflammation + (n = 37) NPV: negative predictive value; PPV: positive predictive value. 1. Loupy A et al. Am J Transplant. 2011;11: Microvascular inflammation (n = 30)
27 Banff 2013: Inclusion of C4d- AMR and Antibody-Associated Arterial Lesions Full-blown acute AMR (acute AMR type 1) Acute AMR without evident complement deposition (acute AMR type 2) C4d-positive subclinical AMR (subclinical AMR type 1) Subclinical AMR without evident complement deposition (subclinical AMR type 2) C4d-positive chronic AMR (chronic AMR type 1) Chronic AMR without evident complement deposition (chronic AMR type 2) C4d staining without histologic evidence of rejection 1. Haas M et al. Am J Transplant. 2014;14:
28 Diagnostic Criteria for Acute AMR in KTR: Clinical Phenotypes: C4d+ vs C4d- 1 C4d+ Serological evidence DSA present Immunopathic evidence IF: diffuse-positive C4d in PTC IHC: diffuse of focal-positive C4d in PTC Histological evidence ATN-like changes and/or PTC and/or Glomerulitis and/or Thrombotic microangiopathy and/or Arterial fibrinoid necrosis and No evidence of chronic capillary injury a C4d- Serological evidence DSA present Immunopathic evidence Negative C4d staining and Endothelial activation, detected by increased mrna expression of endothelial genes and/or Evidence for glomerular and/or capillary endothelial cycling Histological evidence PTC and/or Glomerulitis and/or Thrombotic microenglopathy and/or Arterial fibrinoid necrosis and No evidence of chronic capillary injury a a Reduplication and/or multilayering of glomerular and PTC basement membranes. ATN: acute tubular necrosis; DSA: donor-specific antigen; IHC: Immunohistochemistry; IF: interstitial fibrosis; KTR: kidney transplant recipient; PTC: peritubular capillaritis.. 1. Mengel M et al. Transpl Int. 2012;25:
29 Diagnostic Criteria for Chronic AMR in KTR: Clinical Phenotypes: C4d+ vs C4d- 1 C4d+ C4d- Serological evidence DSA present Immunopathic evidence IF: diffuse-positive C4d in PTC IHC: diffuse of focal-positive C4d in PTC Histological evidence Transplant glomerulopathy and/or PTC basement membrane multilamination and/or IF with tubular atrophy and/or Fibrous intimal thickening of arteries Glomerulitis and/or capillaritis may accompany 1. Mengel M et al. Transpl Int. 2012;25: Serological evidence DSA present Immunopathic evidence Negative C4d staining and Endothelial activation, detected by increased mrna expression of endothelial genes and/or Evidence for glomerular and/or capillary endothelial cycling Histological evidence Transplant glomerulopathy and/or PTC basement membrane multilamination and/or IF with tubular atrophy and/or Fibrous intimal thickening of arteries Glomerulitis and/or capillaritis may accompany
30 Low Positive Predictive Value of DSA for AMR 1 Specificity/sensitivity/PPV/NPV for AMR Method N PPV Sensitivity (%) Specificity (%) CXM DSA ELISA DSA Luminex CXM: crossmatch. 1. Courtesy of Denis Glotz, MD, PhD.


31 Solid-Phase Assays for Antibodies 1 Complement-fixing C1q assay on the HLA SAB that combines sensitivity, specificity, and functional potential SAB: single-antigen bead. 1. Chen G et al. Hum Immunol. 2011;72:

32 Post Treatment DSA: Outcomes 1 DSA+/C1q+ = higher risk of graft loss 1. Loupy A et al. N Engl J Med. 2013;369:
33 Presentation 2: The Role of Complement Inhibition in Preventing and Treating AMR Robert A. Montgomery, MD, DPhil, FACS The Johns Hopkins Hospital Baltimore, Maryland
34 AMR: Pathogenesis of the Humoral Immune Response 1 Plasmablasts Plasma cells HLA antibody Clonal expansion T cell Complement activation Memory B cells LLPC Bone marrow LLPC: long-lived plasma cell. 1. Montgomery RA et al. Semin Immunol. 2011;23: Coagulative necrosis
35 AMR: Therapeutic Targets for Interrupting the Humoral Immune Response 1 Proteosomal Inhibitors HLA antibody IVIg and Plasmapheresis Anti-CD20 Clonal expansion Plasmablasts Plasma cells Splenectomy T-Cell ATG, Steroids Memory B cells Complement Inhibitors Complement Activation LLPC Bone marrow ATG: anti-thymocyte globulin; IVIg: intravenous immunoglobulin 1. Montgomery et al. Seminars in Immunology : Coagulative necrosis
36 Does Rituximab Prevent An Anamnestic Response 1 Made Antibody to Tetramer Antigen b Post-Transplant Antibody Production to Antigens With Elevated B-Cell Frequencies a Treated With Rituximab Yes No Yes 0 13 Χ 2 1= 16.2 P = No 10 3 Tetramers used to determine the frequencies of B cells with HLA specificities that are not producing soluble antibody Tetramers are available only for a limited number of HLA molecules a There was not detectable antibody to the tested tetramer antigen prior to transplantation. b Made antibody to the tetramer antigen after transplantation. 1. Zachary AA et al. Transplantation. 2013;95:
 met the primary endpoint in the rituximab group vs 57.9% (11/19) in the placebo group (P =.")
37 Placebo-Controlled, Randomized Trial of SOC ± Rituximab For Treatment of AMR 1 Primary endpoint: a composite criterion (graft loss or absence of improvement of renal function at d 12) Results: Among the 38 patients included with AMR, 52.6% (10/19) met the primary endpoint in the rituximab group vs 57.9% (11/19) in the placebo group (P =.744); there were no differences in SCr, proteinuria, and glomerulitis at 1, 6, or 12 mo SCr: serum creatinine. 1. Sautenet B et al American Transplant Congress (ATC 2013). Abstract 226.
38 Desensitization Protocol For +XM 1 FK506 (0.1 mg/kg/d) MMF (2 gm/d) Steroids ATG Anti-CD20 Continue FK506 Continue MMF (2 gm/d) Prednisone Taper Preoperative PP/IVIG TXP Postoperative PP/IVIG Goal Is a ( ) Cyto XM Goal Is a ( ) Flow XM ATG: anti-thymocyte globulin; MMF: mycophenolate mofetil. 1. Montgomery RA. Am J Transplant. 2010;10:
39 AMR in HLA-Incompatible Transplants 1 Type of AMR Incidence (%) Treatment Response Severe oliguric AMR 8.9% Not responsive to PP/IVIg/anti-CD20 AMR 15.8% Responds to PP/IVIg/anti-CD20 No AMR 75.3% No treatment beyond protocol CMR: cell-mediated rejection. 1. Orandi BJ et al. Am J Transplant In press.
40 PP/IVIg Treatment Protocol for Acute AMR 1 Anti-CD20 Steroid bolus or α-thymocyte globulin PP: single plasma volume exchange IVIg: 100 mg/kg following each PP treatment (CMV hyperimmune globulin) PP/IVIg PP/IVIg PP/IVIg PP/IVIg PP/IVIg AMR diagnosis CMV: cytomegalovirus. 1. Montgomery RA et al. Transplantation. 2000;70:
41 Severe Oliguric AMR and the Impact of Rescue Splenectomy 1 1. Locke JE et al. Am J Transplant. 2007;7:



42 Severe Oliguric AMR and the Impact of Rescue Splenectomy 1 1. Locke JE et al. Am J Transplant. 2007;7:


43 Classical Complement Pathway in Acute AMR in Sensitized KTRs 1 ECULIZUMAB a a FDA approved for PNH and ahus. ahus: atypical hemolytic uremic syndrome; DAF: decay-accelerating factor; PNH: paroxysmal nocturnal hemoglobinuria; Y-CVF, Yunnan-cobra venom factor. 1. Stegall MD et al. Nat Rev Nephrol. 2012;8:

44 Treatment Protocol for Severe Oliguric Acute AMR 1,2 Anti-CD20 Steroid bolus or α-thymocyte globulin Heparin D/C FK 506 PP/IVIg AMR diagnosis PP/IVIg PP/IVIg PP/IVIg PP/IVIg Eculizumab Eculizumab 1,200 mg 600 mg Splenectomy Eculizumab 600 mg Eculizumab 600 mg Eculizumab 600 mg 1. Locke JE et al. Am J Transplant. 2009;9: Iyer HS et al.curr Opin Nephrol Hypertens. 2013;22:

45 Graft Survival After Severe AMR By Intervention 1 1. Orandi BJ et al. Am J Transplant In press.

46 Transplant Glomerulopathy in Early Severe Oliguric AMR 1 Graft Loss/Died Missing CG: chronic glomerulopathy. 1. Orandi BJ et al. Am J Transplant In press.
47 Prevention Of AMR In Desensitized Patients With Eculizumab 1 PreTx BFXM <300 MESF <19,300 BFXM <200 MESF <10,000 STOP MESF 10, , , , ,200 STOP No post-transplant PP/biopsy/Ab levels at 4, 7, 14, 28, and 90 BFXM: B-cell flow cytometric crossmatch; MESF: molecules of equivalent soluble fluorochrome. 1. Stegall MD et al. Am J Transplant. 2011;11:
48 Prevention Of AMR In Desensitized Patients 1 Category Follow-up (mean mo + SD, range) Eculizumab (n = 26) ( ) Control (n = 51) ( ) Graft survival at 1 y (n, %) 16/16 (100) 49/51 (97) 1.00 AMR 3 mo (n, %) 2 (7.7) 21 (41).0031 Patients developing high DSA levels 3 mo a 13 (50) 22 (43).63 High DSA biopsies C4d+ (n, %) 13 (100) 20 (91).52 High DSA and C4d+ biopsies showing AMR (n, %) P N/A 2 (15) 20 (100) <.0001 Cellular rejection 3 mo (n, %) 1 (6.2) 1 (2).42 a B flow XM channel shift >350 at any time point in the first 3 mo. 1. Stegall MD et al. Am J Transplant. 2011;11:
49 Approaches to the Use of Eculizumab: Hopkins Versus Mayo Approach 1 Hopkins Approach Eculizumab along with PP (and splenectomy) used to rescue kidneys with severe AMR phenotype (8.9% occurs POD 5- POD 7) Rationale 75% of patients will not have AMR; this approach avoids the cost of treating them Protecting the kidney from complement-mediated damage while removing DSA might improve outcomes (reduce risk for immediate graft loss and TG) POD: postoperative day. 1. Courtesy of Robert A. Montgomery, MD, DPhil, FACS. Mayo Approach Eculizumab used as prophylaxis to reduce the incidence (from 41% to 7.7%; P =.003) and severity of early AMR Done without the use of posttransplant PP In some cases, remaining DSA disappears; in others it persists beyond the discontinuation of the agent, with many of these patients developing TG

50 AMR: C1 Esterase Inhibitor a Mechanistically Attractive Due To Proximal Complement Blockade 1 A FDA approved for hereditary angioedema. C1-INH: C1 esterase inhibitor; FDP: fibrin degradation product; HMWK: high molecular weight kininogen; IL: interleukin; KK: kallikrein; MASP: MBP-associated serine protease; MBP: mannosebinding protein; TNF: tumor necrosis factor; tpa: tissue plasminogen activator. 1. Levy J, O Donnell P. Expert Opin Investig Drugs. 2006;15:
51 Conclusions The rate of AMR after desensitization is 24.7%, of which 8.9% is severe and nonresponsive to standard therapy and 15.8% is not graft-threatening and is responsive to PP; both phenotypes at risk for TG Rituximab has an attractive mechanism and, when B-cell precursor rates are high, prevents anamnestic responses; however, this does not seem to translate into efficacy for the prevention or treatment of AMR Splenectomy is effective in rescuing kidneys with the severe AMR phenotype but does not protect against TG A combination of splenectomy, PP/IVIg, and eculizumab is good rescue therapy and appears to prevent TG in the severe AMR phenotype Eculizumab is very effective in reducing the rate of AMR in the first 3 mo after desensitization but, if high levels of DSA persist, there is a likelihood of chronic AMR/TG C1 esterase inhibitor provides more proximal complement blockade, and endogenous levels are depleted by PP
52 Panel Discussion: Review of Clinical Cases Denis Glotz, MD, PhD Saint-Louis Hospital Paris, France Robert A. Montgomery, MD, DPhil, FACS The Johns Hopkins Hospital Baltimore, Maryland

53 Prophylaxis of AMR: F.T.
54 F.T.: Transplant Status Potential living donor: sister Donor Status 4 MM: A24, B35, DR4, DQ8 Positive cytotoxic crossmatch T, IgG F.T. s Status 3 DSAs (MFI >15000): A24, DR4, DQ8
55 Patient Report Cytotox PRA: 93% vpra: 100% 1 donor /5 y
56 Prophylaxis of AMR: Treatment Considerations for F.T. IVIg high dose (Glotz, Jordan) PP/IVIg (Montgomery) acd20/ivig (Jordan) Bortezomib protocols (Woodle)
57 Prophylaxis of AMR: Desensitization Desensitization (1): lower cytotoxicity and obtain a negative cytotoxic crossmatch Desensitization (2): lower MFIs and negativate (as much as possible) the flow crossmatch
58 Prophylaxis of AMR: Desensitization (Cont d) Desensitization (1): lower cytotoxicity and obtain a negative cytotoxic crossmatch 6 monthly cures of IVIg high dose Desensitization (2): lower MFIs and negativate (as much as possible) the flow crossmatch 4 PP/IVIg sessions just before Tx
59 Prophylaxis of AMR Negative cytotoxic and flow crossmatches with low DSAs (<1,500) Transplantation, immediate function But AMR at day 10!
60 TT by C5 Inhibition: LD Tx HD Bx Bx Bx PP IVIg Cy 1. Courtesy of Denis Glotz, MD, PhD.

61 TT by C5 Inhibition: LD Tx (Cont d) 1. Courtesy of Denis Glotz, MD, PhD. Eculizumab
62 Kidney Transplantation Compared With Dialysis: Clinically Relevant Outcomes A systematic review of 110 studies (1,961,904 participants) with kidney failure Key findings Kidney transplantation was associated with» Reduced risk of mortality and cardiovascular events» Improved quality of life (vs chronic dialysis) Benefits of transplant (vs chronic dialysis) increased over time despite increased age and comorbidities of KTRs Results were consistent» For different dialysis modalities» For deceased and living donors» Across countries with differing health care systems Results confirm that kidney transplantation is the preferred modality of treatment for chronic kidney failure 1. Tonelli M et al. Am J Transplant. 2011;11:
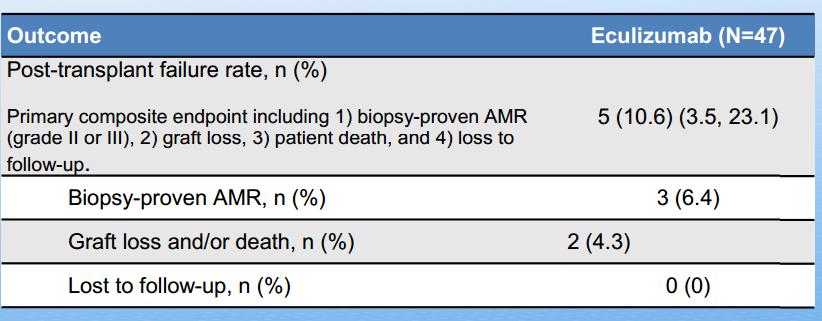
63 Preventing AMR in Sensitized Deceased-Donor KTRs 1 Open-label, single-arm, multicenter phase 2 trial: 9-wk preliminary results Primary endpoint: post-transplantation treatment failure rate at wk 9, defined by biopsy-proven AMR, graft loss, patient death, and/or loss to follow-up Ec 1,200 mg Ec 1,200 mg Ec 900 mg Ec 1,200 mg Ec 1,200 mg D 0 D 1, 7, 14, 28 Wk 5 Wk 7 Wk 9 Induction: rabbit ATG EC: eculizumab. Maintenance: prednisone, tacrolimus, mycophenolate 1. Glotz D et al. 16th Congress of the European Society for Organ Transplantation (ESOT 2013). Abstract 2071.
64 Preventing AMR in Sensitized Deceased-Donor KTRs 1 Outcome Post-transplant failure rate Primary composite endpoint including 1) biopsyproven AMR (grade II or III), 2) graft loss, 3) patient death, and 4) loss to follow-up. Eculizumab (N=47) n (%) 5 (10.6); (3.5, 23.1) Biopsy-proven AMR 3 (6.4) Graft loss and/or death 2 (4.3) Lost to follow-up 0 (0) Data from local laboratory instead of the central laboratory 1. Glotz D et al. ESOT Abstract 2071.
65
66 Thank You and Good Afternoon! Please remember to complete and submit your Post-Test and Evaluation for CME credit. Missed anything? Visit us at Download slides and Practice Aids Watch for the OnDemand version of this symposium PVI, PeerView Institute for Medical Education and University of New Mexico School of Medicine, Office of Continuing Medical Education, are responsible for the selection of this report s topics, the preparation of editorial content, and the distribution of this report. The preparation of PeerView reports is supported by educational grants subject to written agreements that clearly stipulate and enforce the editorial independence of PVI and University of New Mexico School of Medicine, Office of Continuing Medical Education. Our reports may contain references to unapproved products or uses of these products in certain jurisdictions. For approved prescribing information, please consult the manufacturer's product labeling. No endorsement of unapproved products or uses is made or implied by coverage of these products or uses in our reports. No responsibility is taken for errors or omissions in reports. Copyright , PeerView Press
Treatment of Chronic Antibody Mediated Rejection
 Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
HLA Part II: My Patient Has DSA, Now What?
 2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique. Mark D. Stegall Mayo Clinic, Rochester, MN
 Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
(Universal Activity Number H01- P) Please note: If you participated in the activity with UAN L01- P, you are
 Please note: If you participated in the activity with UAN L01- P, you are") CME Information Release Date: January 2, 2018 Expiration Date: January 2, 2019 UAN Live Release Date: June 12, 2016 Estimated Time to Complete this Activity: 1.25 hours Overview This article reviews the
CME Information Release Date: January 2, 2018 Expiration Date: January 2, 2019 UAN Live Release Date: June 12, 2016 Estimated Time to Complete this Activity: 1.25 hours Overview This article reviews the
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Methodist University Hospital, Transplant Institute Division of Transplantation, Department
Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management
 Curr Transpl Rep (2014) 1:78 85 DOI 10.1007/s40472-014-0012-y KIDNEY TRANSPLANTATION (ML HENRY, SECTION EDITOR) Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management Carrie
Curr Transpl Rep (2014) 1:78 85 DOI 10.1007/s40472-014-0012-y KIDNEY TRANSPLANTATION (ML HENRY, SECTION EDITOR) Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management Carrie
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Loupy A, Lefaucheur C, Vernerey D, et al. Complement-binding
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Loupy A, Lefaucheur C, Vernerey D, et al. Complement-binding
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New. Ramsey Hachem, MD March 28, 2017
 Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance
 ORIGINAL ARTICLE Port J Nephrol Hypert 2008; 22(1): 37-42 Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance Helena
ORIGINAL ARTICLE Port J Nephrol Hypert 2008; 22(1): 37-42 Peritubular capillaries C4d deposits in renal allograft biopsies and anti HLA I/II alloantibodies screening Incidence and clinical importance Helena
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients
 Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques
 Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques CAMR in 2010: natural history and perspectives Alexandre Loupy 1 Introduction 2 CAMR: the missing link 3 Natural history of CAMR
Le Rejet Humoral Chronique en 2010: Histoire naturelle et problématiques CAMR in 2010: natural history and perspectives Alexandre Loupy 1 Introduction 2 CAMR: the missing link 3 Natural history of CAMR
Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab
 ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation
 Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY
 2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk factor for graft loss
 http://www.kidney-international.org 2015 International Society of Nephrology see commentary on page 218 The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk
http://www.kidney-international.org 2015 International Society of Nephrology see commentary on page 218 The diffuse extent of peritubular capillaritis in renal allograft rejection is an independent risk
Dix ans de transplantation rénale Fonds Boussard
 Dix ans de transplantation rénale Fonds Boussard Groupe Spiesser A.T.N. Christophe Legendre, Hôpital Necker & Université Paris Descartes, Paris Fondation Day-Solvay Actualités Néphrologiques Jean Hamburger
Dix ans de transplantation rénale Fonds Boussard Groupe Spiesser A.T.N. Christophe Legendre, Hôpital Necker & Université Paris Descartes, Paris Fondation Day-Solvay Actualités Néphrologiques Jean Hamburger
Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes
 Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes INTRODUCTION In patients awaiting a transplant, having antibodies reactive to HLA antigens present
Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes INTRODUCTION In patients awaiting a transplant, having antibodies reactive to HLA antigens present
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients
 Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Utility of protocol kidney biopsies for de novo donor- specific antibodies
 Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation
 AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly Sensitized Renal Transplanted Patients
 BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting Antibody-Mediated Rejection
 Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Recognition and Management of Antibody-Mediated Rejection
 Recognition and Management of Antibody-Mediated Rejection Malcolm P. MacConmara, MB, BCh, BAO Emory University School of Medicine, Atlanta, Georgia Abstract Previously underdiagnosed and overshadowed by
Recognition and Management of Antibody-Mediated Rejection Malcolm P. MacConmara, MB, BCh, BAO Emory University School of Medicine, Atlanta, Georgia Abstract Previously underdiagnosed and overshadowed by
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Antibody Mediated Rejection in Heart Transplantation
 Antibody Mediated Rejection in Heart Transplantation 2012 Teresa De Marco, MD, FACC Professor of Medicine & Surgery Director Heart Failure and Pulmonary Hypertension Program Medical Director, Heart Transplantation
Antibody Mediated Rejection in Heart Transplantation 2012 Teresa De Marco, MD, FACC Professor of Medicine & Surgery Director Heart Failure and Pulmonary Hypertension Program Medical Director, Heart Transplantation
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS
 APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
Outcome of Subclinical Antibody-Mediated Rejection in Kidney Transplant Recipients with Preformed Donor-Specific Antibodies
 American Journal of Transplantation 2009; 9: 2561 2570 Wiley Periodicals Inc. C 2009 The Authors Journal compilation C 2009 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2009; 9: 2561 2570 Wiley Periodicals Inc. C 2009 The Authors Journal compilation C 2009 The American Society of Transplantation and the American Society of Transplant
Microcirculation Inflammation Associates With Outcome in Renal Transplant Patients With De Novo Donor-Specific Antibodies
 American Journal of Transplantation 2013; 13: 485 492 Wiley Periodicals Inc. Brief Communication C Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons
American Journal of Transplantation 2013; 13: 485 492 Wiley Periodicals Inc. Brief Communication C Copyright 2012 The American Society of Transplantation and the American Society of Transplant Surgeons
Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification
 Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
In-Depth Review. Desensitization Protocols and Their Outcome
 In-Depth Review Desensitization Protocols and Their Outcome Kwaku Marfo,* Amy Lu,* Min Ling* and Enver Akalin* Summary In the last decade, transplantation across previously incompatible barriers has increasingly
In-Depth Review Desensitization Protocols and Their Outcome Kwaku Marfo,* Amy Lu,* Min Ling* and Enver Akalin* Summary In the last decade, transplantation across previously incompatible barriers has increasingly
Desensitization for solid organ and hematopoietic stem cell transplantation
 Andrea A. Zachary Mary S. Leffell Desensitization for solid organ and hematopoietic stem cell transplantation Authors address Andrea A. 1 Zachary, Mary S. Leffell 1 1 Department of Medicine, Division of
Andrea A. Zachary Mary S. Leffell Desensitization for solid organ and hematopoietic stem cell transplantation Authors address Andrea A. 1 Zachary, Mary S. Leffell 1 1 Department of Medicine, Division of
Renal transplantation in sensitized recipients with positive luminex and negative CDC (complement-dependent cytotoxicity) crossmatches
 crossmatches") Transplant International ISSN 0934-0874 ORIGINAL ARTICLE Renal transplantation in sensitized recipients with positive luminex and negative CDC (complement-dependent cytotoxicity) crossmatches Kyu Ha Huh,
Transplant International ISSN 0934-0874 ORIGINAL ARTICLE Renal transplantation in sensitized recipients with positive luminex and negative CDC (complement-dependent cytotoxicity) crossmatches Kyu Ha Huh,
Medicine OBSERVATIONAL STUDY
 Medicine OBSERVATIONAL STUDY Clinical Significance of HLA-DQ Antibodies in the Development of Chronic Antibody-Mediated Rejection and Allograft Failure in Kidney Transplant Recipients Hyeyoung Lee, MD,
Medicine OBSERVATIONAL STUDY Clinical Significance of HLA-DQ Antibodies in the Development of Chronic Antibody-Mediated Rejection and Allograft Failure in Kidney Transplant Recipients Hyeyoung Lee, MD,
Diagnosis and Management of Acute and Chronic Humoral Rejection. Lars Pape
 Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis And Treatment Of Antibody Mediated Rejection Post Kidney And Kidney Pancreas Transplant RRCV CMG Renal and Transplant Service
 Diagnosis And Treatment Of Antibody Mediated Rejection Post Kidney And Kidney Pancreas Transplant RRCV CMG Renal and Transplant Service 1. Introduction Transplantation offers better survival and quality
Diagnosis And Treatment Of Antibody Mediated Rejection Post Kidney And Kidney Pancreas Transplant RRCV CMG Renal and Transplant Service 1. Introduction Transplantation offers better survival and quality
DSA Positive and then To biopsy or not?
 DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b
 Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b a John Hopkins University, Immunogenetics Laboratory, Baltimore, Maryland and b Cedars-Sinai
Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b a John Hopkins University, Immunogenetics Laboratory, Baltimore, Maryland and b Cedars-Sinai
3/6/2017. Treatment of Detected Antibodies. I have financial relationship(s) with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker
 with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker") Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function
 ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Since the first Banff meeting in 1991, the diagnosis and
 CLINICAL AND TRANSLATIONAL RESEARCH Acute Cellular Rejection: Impact of Donor-Specific Antibodies and C4d Michelle Willicombe, 1,5 Candice Roufosse, 2 Paul Brookes, 3 Adam G. McLean 1, Jack Galliford,
CLINICAL AND TRANSLATIONAL RESEARCH Acute Cellular Rejection: Impact of Donor-Specific Antibodies and C4d Michelle Willicombe, 1,5 Candice Roufosse, 2 Paul Brookes, 3 Adam G. McLean 1, Jack Galliford,
Cases: CMV, HCV, BKV and Kidney Transplantation. Simin Goral, MD University of Pennsylvania Medical Center
 Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Cases: CMV, HCV, BKV and Kidney Transplantation Simin Goral, MD University of Pennsylvania Medical Center Disclosures Grant support: Otsuka Pharmaceuticals, Astellas Pharma, Angion, AstraZeneca, and Kadmon
Treatment Update of Sensitized Pediatric Kidney Transplant Recipients: A Review
 RevIew Treatment Update of Sensitized Pediatric Kidney Transplant Recipients: A Review Hasan Otukesh, 1 Rozita Hoseini, 2 Nahid Rahimzadeh 3 Abstract Sensitization of recipients is an increasing problem
RevIew Treatment Update of Sensitized Pediatric Kidney Transplant Recipients: A Review Hasan Otukesh, 1 Rozita Hoseini, 2 Nahid Rahimzadeh 3 Abstract Sensitization of recipients is an increasing problem
23/10/2017. Panel Reactive Antibodies and Crossmatch by Flow Cytometry. Antibodies against. Renal transplantation. Antibody mediated rejection (AMR)
") Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
Interstitial Inflammation
 Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
Approach to Kidney Transplant in Sensitized Potential Transplant Recipients
 RevIew Approach to Kidney Transplant in Sensitized Potential Transplant Recipients Antoine Barbari, Souodod Abbas, Mahassen Jaafar Abstract More than one-third of patients on waiting lists for kidney transplant
RevIew Approach to Kidney Transplant in Sensitized Potential Transplant Recipients Antoine Barbari, Souodod Abbas, Mahassen Jaafar Abstract More than one-third of patients on waiting lists for kidney transplant
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy
 Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Risk Factors in Long Term Immunosuppressive Use and Advagraf. Daniel Serón Nephrology department Hospital Universitari Vall d Hebron
 Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham
 Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Living-Donor Kidney Transplant in T-Cell and B-Cell Flow Cytometry Crossmatch-Positive Patients
 ARTICLe Living-Donor Kidney Transplant in T-Cell and B-Cell Flow Cytometry Crossmatch-Positive Patients Soushi Terasaka, 1 Hidehisa Kitada, 1,3 Yasuhiro Okabe, 1 Sayako Kawanami, 1 Hiroshi Noguchi, 1 Kyoko
ARTICLe Living-Donor Kidney Transplant in T-Cell and B-Cell Flow Cytometry Crossmatch-Positive Patients Soushi Terasaka, 1 Hidehisa Kitada, 1,3 Yasuhiro Okabe, 1 Sayako Kawanami, 1 Hiroshi Noguchi, 1 Kyoko
RevIeWS. Sensitized renal transplant recipients: current protocols and future directions. James Gloor and Mark D. Stegall
 RevIeWS Sensitized renal transplant recipients: current protocols and future directions James Gloor and Mark D. Stegall Abstract The identification of suitable donor kidneys for transplant candidates with
RevIeWS Sensitized renal transplant recipients: current protocols and future directions James Gloor and Mark D. Stegall Abstract The identification of suitable donor kidneys for transplant candidates with
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Kidney Transplant. November 4 th, 2016
 Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
Kidney Transplant November 4 th, 2016 Brad West, MD, FACP Medical Director of Transplant Services, Memorial Medical Center Chairman Department of Nephrology, Springfield Clinic 1 Adjusted survival: 1993-1997
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT. 4th April 2014
 Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
OBJECTIVES. Phases of Transplantation and Immunosuppression
 Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
HLA Antibody Complement Based Assays. Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA
 Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA") HLA Antibody Complement Based Assays Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA Disclosure Neither presenter has any financial relationships related
HLA Antibody Complement Based Assays Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA Disclosure Neither presenter has any financial relationships related
2017 BANFF-SCT Joint Scientific Meeting. BARCELONA March 2017
 2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
Pros and cons for C4d as a biomarker
 review http://www.kidney-international.org & 2012 International Society of Nephrology Pros and cons for C4d as a biomarker Danielle Cohen 1, Robert B. Colvin 2, Mohamed R. Daha 3, Cinthia B. Drachenberg
review http://www.kidney-international.org & 2012 International Society of Nephrology Pros and cons for C4d as a biomarker Danielle Cohen 1, Robert B. Colvin 2, Mohamed R. Daha 3, Cinthia B. Drachenberg
Histopathological evaluation of renal allograft biopsies in Nepal: interpretation and significance
 Nepal Medical Association Building Exhibition Road, Kathmandu Journal of Pathology of Nepal (2012) Vol. 2, 172-179 Association of Clinical Pathologist of Nepal-2010 Journal of PATHOLOGY of Nepal www.acpnepal.com
Nepal Medical Association Building Exhibition Road, Kathmandu Journal of Pathology of Nepal (2012) Vol. 2, 172-179 Association of Clinical Pathologist of Nepal-2010 Journal of PATHOLOGY of Nepal www.acpnepal.com
The Banff Conferences on renal allograft pathology the latest 2013 report
 615245PSH0010.1177/2010105815615245Proceedings of Singapore HealthcareLoh research-article2015 Review Article PROCEEDINGS OF SINGAPORE HEALTHCARE The Banff Conferences on renal allograft pathology the
615245PSH0010.1177/2010105815615245Proceedings of Singapore HealthcareLoh research-article2015 Review Article PROCEEDINGS OF SINGAPORE HEALTHCARE The Banff Conferences on renal allograft pathology the
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients
 in LUNG TRANSPLANT Recipients") Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Darshana Dadhania 12 Fritz Diekmann 13 Klemens Budde 14 Fritz Lower 15 Babak J. Orandi 16 Ajda T. Rowshani 17 Lynn Cornell 18 Edward Kraus 19
 Received: 23 February 2018 Revised: 25 May 2018 Accepted: 31 May 2018 DOI: 10.1111/ajt.14979 ORIGINAL ARTICLE Banff survey on antibody mediated rejection clinical practices in kidney transplantation: Diagnostic
Received: 23 February 2018 Revised: 25 May 2018 Accepted: 31 May 2018 DOI: 10.1111/ajt.14979 ORIGINAL ARTICLE Banff survey on antibody mediated rejection clinical practices in kidney transplantation: Diagnostic
Open Access. Keywords: IVIg, acute rejection, proteinuria, alloantibody, post-transplant FSGS, glomerulonephritis.
 26 The Open Transplantation Journal, 2009, 3, 26-30 Open Access Heavy Proteinuria as a Manifestation of Acute Allograft Rejection Presenting Early after Kidney Transplantation: A Retrospective, Single-
26 The Open Transplantation Journal, 2009, 3, 26-30 Open Access Heavy Proteinuria as a Manifestation of Acute Allograft Rejection Presenting Early after Kidney Transplantation: A Retrospective, Single-
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation. Doctoral Thesis. Dr. Petra Gombos
 Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
ABO-incompatible kidney transplantation in elderly patients over 60 years of age
 Int Urol Nephrol (2012) 44:1563 1570 DOI 10.1007/s11255-012-0231-z NEPHROLOGY - ORIGINAL PAPER ABO-incompatible kidney transplantation in elderly patients over 60 years of age Junji Uchida Tomoaki Iwai
Int Urol Nephrol (2012) 44:1563 1570 DOI 10.1007/s11255-012-0231-z NEPHROLOGY - ORIGINAL PAPER ABO-incompatible kidney transplantation in elderly patients over 60 years of age Junji Uchida Tomoaki Iwai
Pre-transplant donor specific antibody and its clinical significance in kidney transplantation
 Original article Pre-transplant donor specific antibody and its clinical significance in kidney transplantation Duangtawan Thammanichanond, 1 Atiporn Ingsathit, 2,3 Tasanee Mongkolsuk, 1 Sasivimol Rattanasiri,
Original article Pre-transplant donor specific antibody and its clinical significance in kidney transplantation Duangtawan Thammanichanond, 1 Atiporn Ingsathit, 2,3 Tasanee Mongkolsuk, 1 Sasivimol Rattanasiri,
ABO Antibody Titer and Risk of Antibody-Mediated Rejection in ABO-Incompatible Renal Transplantation
 American Journal of Transplantation 2010; 10: 1247 1253 Wiley Periodicals Inc. C 2010 The Authors Journal compilation C 2010 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2010; 10: 1247 1253 Wiley Periodicals Inc. C 2010 The Authors Journal compilation C 2010 The American Society of Transplantation and the American Society of Transplant
Solid Organ Transplant
 Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Antibody-Mediated Rejection in the Lung Allograft. Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305
 Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Virtual Crossmatch in Kidney Transplantation
 Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
ABO. ABO ABO ABO ABO ABO ABO ABO ABO. Key words ABO. Alexandre ABO ABO. double filtration plasmapheresis, DFPP. antibody-mediated rejection, AMR
 ABO ABO ABO ABO ABO ABO ABO ABO ABO ABO.. ABO ABO. ABO. ABO ABO Key words ABO ABO A B antibody-mediated rejection, AMR Alexandre ABO double filtration plasmapheresis, DFPP ABO ABO n ABO n p-value R.....
ABO ABO ABO ABO ABO ABO ABO ABO ABO ABO.. ABO ABO. ABO. ABO ABO Key words ABO ABO A B antibody-mediated rejection, AMR Alexandre ABO double filtration plasmapheresis, DFPP ABO ABO n ABO n p-value R.....