Management of Glucose in the Preterm Infant. Charles A. Stanley, MD Division of Endocrinology Children s Hospital of Philadelphia
|
|
|
- Timothy Fleming
- 5 years ago
- Views:
Transcription
1 Management of Glucose in the Preterm Infant Charles A. Stanley, MD Division of Endocrinology Children s Hospital of Philadelphia
2 Disclosures Charles Stanley, MD I have no relevant financial relationships to disclose or conflicts of interest to resolve. I will not discuss any unapproved or offlabel, experimental or investigational use of a product or device.
3 The Problem Too little glucose: risk of seizures, permanent brain damage, liability suits

4 The Elephant and The Blind Men Endo Neo
 is issued by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) to encourage Research Project Grant (R01)")

5 The Journal of Pediatrics Volume 155, Issue 5, November 2009, Pages Marvin Cornblath, 2000 NICHD RFA, PA , December, Studies in Neonatal Hypoglycemia. This funding opportunity announcement (FOA) is issued by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) to encourage Research Project Grant (R01) applications from institutions and organizations to propose studies related to basic, applied and translational research in neonatal hypoglycemia. While much progress has been made in understanding the causes and mechanisms of altered neonatal glucose homeostasis, major gaps remain. Through this FOA, the NICHD is hoping to fill-in such knowledge gaps, which may lead to better monitoring and treatment strategies for altered neonatal glucose homeostasis. Concerns about neonatal hypoglycemia driven by malpractice worries.

6 1954-First recognition of importance of hypoglycemia in infants

7 McQuarrie 1954
8 Idiopathic Hypoglycemia: Concerns in Irreparable brain damage 2. Delayed diagnosis 3. Inadequate (early) therapy 4. Etiology 5. Genetic?
9 How have we been doing since the time that Idiopathic Hypoglycemia of Infancy was Not Great!: described in 1953? For neonates with HI (the most common form of congenital hypoglycemia): 1. 30% of infants with focal HI who required pancreatectomy were not detected before discharge from nursery 2. 50% of diazoxide-responsive HI cases are not detected during the neonatal period. 3. Rates of neurodevelopmental delay in infants with congenital HI are too high (25-50% of cases). Risk of lawsuits for poor outcomes associated with hypoglycemia remains a concern
10 Points to cover Use of critical sample for specific diagnosis Three different types of hypoglycemia in neonates: 1. transient/developmental in normal neonates 2. peri-natal stress/prolonged hyperinsulinism 3. permanent/genetic forms (especially, HI) Focal vs Diffuse forms of congenital hyperinsulinism Hypoglycemia and normal newborns
11 (1) Permanent hypoglycemia in neonates: Hyperinsulinism (HI) is the most common cause. CHOP series (156 cases) Glycogenoses 4% 19% ß-Oxidation defects and Hypopituitarism 34% HI needing surgery Transient HI 26% 17% HI diazoxide responsive
 Treatment: diazoxide surgery (98% PX if diffuse, local excision if focal) NB.")
12 Congenital Hyperinsulinism (HI) Incidence ~1 in 20,000 LGA birthweight common Increased glucose utilization (GIR up to mg/kg/min) Recessive or dominant (9 loci) Treatment: diazoxide surgery (98% PX if diffuse, local excision if focal) NB. Never use steroids for treatment of hypoglycemia!
13 Use of Critical Samples to Define Specific Etiology Fasting Hypoglycemia Acidemia No Acidemia Lactate Ketones FFA Ketones FFA Ketones G-6-Pase F-1,6-Pase PCase Ethanol Normal Ketotic Hypo GSD 3,6,9,0 GH-def Cortisol-def FAO def Hyperinsulinism Cong Hypopit SGA/birth asphyxia? Neonates DOL1 Glycemic response to glucagon

14 Hypoketonemia: a diagnostic feature of hyperinsulinemic-hypoglycemia normals Congenital HI
15 Plasma Insulin (µu/ml) Hypoketonemia better for diagnosing HI than insulin level. Insulin vs ß-Hydroxybutyrate at Blood Glucose < 50 mg/dl mmol/l Hyperinsulinism Controls µu/ml Plasma ß-Hydroxybutyrate (mmol/l)

16 Beta-hydroxybutyrate bedside monitoring Finger-stick enzymatic assay for BOB Range 0-6 mmol/l Accuracy ± 0.5 mmol/l Expected levels Well-fed: <0.1 mmol/l Hypoglycemia: >2.5 mmol/l
17 Diagnosis of Hyperinsulinism: Glycemic Response to Glucagon x HI. Fasting controls Hypoglycemic controls
18 Congenital Hyperinsulinism Recessive or Dominant Inheritance
19 Congenital Hyperinsulinism: Genes glucose leucine amino acids pyruvate MCT1 GK + GDH glutamate mechanism unclear: SCHAD HNF4a UCP2 diazoxide + K ATP channel SUR1 & KIR6.2 ATP ATP Insulin Ca K + - tolbutamide depolarization - calcium channel + somatostatin
20 Focal HI Clinically identical to recessive, diffuse KATP-HI 40-70% of severe congenital HI cases Diazoxide unresponsive Surgical pancreatectomy required 2-hit mechanism: Clonal LOH for maternal 11p UPD for a recessive paternal KATP-channel mutation

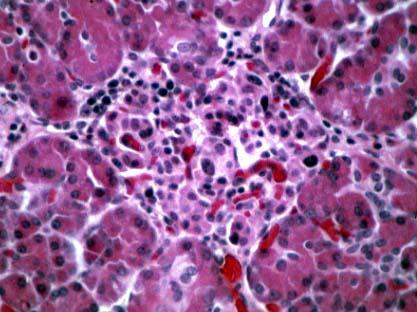

21 HISTOLOGIC FORMS OF HYPERINSULINISM Diffuse form Focal form

22 CHOP HI Center
23 Imaging focal HI by 18F-DOPA PET scan (Positron Emission Tomography) Usual imaging methods don t work in focal HI (MRI, CT, Echo, catheterization) 18F-DOPA concentrated in beta-cells to form an image of focal lesion in the PET scan 18F-DOPA custom-made for PET scans in UPenn cyclotron under FDA investigational IND

24 Focal HI 18 F-DOPA PET Scan

")
25 18 F-DOPA PET: Focal HI in Infant with Ectopic Lesions in Jejunum 10 min post injection 60 min post injection focal lesion in head of pancreas (small arrows show ectopic lesions in jejunum)


26 Interpreting Glucose Levels: Glucose Treatment Targets 100 good 70 caution 50 danger 30 Data from Cryer, et al.
27 Criteria for management of hyperinsulinism and other forms of hypoglycemia Cure of Focal HI: able to fast keeping BS >70 mg/dl for 18 hr OR ketones > 2.5 mm before BS <50 mg/dl Prolonged Hypoglycemia (Day 2 up to several weeks) Good control (e.g., diazoxide Rx in HI): same Birth asphyxia, IUGR, other peri-natal stresse Mechanism: hyperinsulinism Permanent Adequate Hypoglycemias control of presenting hypoglycemia in neonates for discharge: able to fast through 2+ feeds keeping BS >70 mg/dl (i.e., Genetic hyperinsulinism(s) minimum 8-10 hr) Panhypopituitarism Fatty acid oxidation defects


28 CHOP HI Center
 Prolonged Hypoglycemia (Day 2 up to several weeks) Mechanism: hyperinsulinism Permanent Hypoglycemias presenting in neonates Genetic hyperinsulinism(s)")
29 (2) Transient Neonatal Hypoglycemia (Day 1) High risk related to delayed feeding Mechanism: speculative (immaturities in hepatic ketogenesis Birth asphyxia, IUGR, & gluconeogenesis, other peri-natal stresse insulin suppression until hours) Prolonged Hypoglycemia (Day 2 up to several weeks) Mechanism: hyperinsulinism Permanent Hypoglycemias presenting in neonates Genetic hyperinsulinism(s) Panhypopituitarism Fatty acid oxidation defects
30 Plasma Glucose Distribution Prior to 1 st Feed at 8 hr of Age
31 Incidence of Hypoglycemia before 1 st Feed at 8hr old (BS < 30 mg/dl) (Lubchenko & Bard, Pediatrics,1971)
32 Evolution of Transient Neonatal Hypoglycemia: Frequency of Plasma Glucose < 50 mg/dl Day 1 vs Day 2-3 (Lubchenko & Bard, Pediatrics,1971) Term AGA All Others Before 1 st feed at 8 hr of age 29 % 50 % Day 2-3 of life 0 % 1 %


33 Lack of ketogenic response to hypoglycemia in both AGA and SGA neonates on Day 1. Stanley CA, Baker L. Pediatrics normals Stanley CA, Anday EK, Baker L, Delivoria- Papadopolous M. Pediatrics Congenital HI
34 On Day 1: Ketogenesis is suppressed in both normal and SGA neonates. (Haymond et al. NEJM 1974)
35 Glucose, Total Ketones (mm) Hawdon, et al. Arch Dis Child 1992 Hypoketonemia in Term Neonates during 1 st week Day of Life 72 mg/dl glucose ketones
36 Etiology of Transient Hypoketotic Hypoglycemia in Normal Neonates: Immaturities of Fasting Adaptation Hepatic Gluconeogenesis: PEP-CK activity absent Matures by hr Hepatic Ketogenesis CPT-1 (&?HMG-CoA synthase) absent Expression activated by long-chain fatty acids (colostrum) Matures by hr Insulin secretion Incomplete suppression at low BS? Persistent HK1, MCT1 expression Implication: All infants born with at least two strikes!
37 (3) Prolonged Neonatal Hypoglycemia (Day 2 up to several weeks) Transient Hypoglycemia (Day 1) High risk related to delayed feeding Mechanism: immaturities in hepatic ketogenesis and gluconeogenesis, insulin suppression until hours Birth asphyxia, SGA, maternal hypertension, other peri-natal stresses Mechanism: hyperinsulinism Permanent Hypoglycemias presenting in neonates Genetic hyperinsulinism(s) Panhypopituitarism Fatty acid oxidation defects
38 Plasma Glucose Distribution Prior to 1 st Feed at 8 hr of Age
39 Incidence of Hypoglycemia before 1 st Feed at 8hr old (BS < 20 mg/dl)
40 Maternal preeclampsia appears to be a risk factor for prolonged hypoglycemia in SGA neonates during 1 st 24 hr (open circles). Wright LL, Stanley CA, Anday EK, Baker L. The effect of early feeding on plasma glucose levels in SGA infants. Clin Pediatr. 1983;22:539-41
41 Prolonged Hyperinsulinism in Perinatal Stress Hypoglycemia Collins JE, Leonard JV. Hyperinsulinism in asphyxiated and small-for-dates infants with hypoglycaemia. Lancet 1984;ii: Collins JE, Leonard JV, Teale D, Marks V, Williams DM, Kennedy CR, Hall MA. Hyperinsulinaemic hypoglycaemia in small for dates babies. Archives of Disease in Childhood 1990; 65: Hoe FM, Thornton PS, Wanner LA, Steinkrauss L, Simmons RA, Stanley CA. Clinical features and insulin regulation in infants with a syndrome of prolonged neonatal hyperinsulinism. J Pediatr 2006; 148:
42 Characteristics of 26 neonates with peri-natal stress HI Frequency P value (vs US newborns 2000) Male 81% Risk factors Maternal hypertension 12% 0.3 Prematurity 23% 0.1 SGA 27% 0.01 LGA 8% Perinatal stress 35% Cesarean delivery 62% < No risk factors 19% Hoe FM, Thornton PS, Wanner LA, Steinkrauss L, Simmons RA, Stanley CA. Clinical features and insulin regulation in infants with a syndrome of prolonged neonatal hyperinsulinism. J Pediatr. 2006;148:
43 Features of prolonged neonatal hyperinsulinism (median, range) Age of initial hypoglycemia Age at diagnosis of hyperinsulinism Maximum glucose infusion rate Treatment Required: Frequent feeding only Diazoxide Treatment Continuous feeding Age resolution documented 1 day (0 to 168 days) 13 days (2 to 180 days) 12 mg/kg/min (0 to 19 mg/kg/min) 5 neonates 19 neonates 2 neonates 181 days (18 to 403 days) Hoe FM, Thornton PS, Wanner LA, Steinkrauss L, Simmons RA, Stanley CA. Clinical features and insulin regulation in infants with a syndrome of prolonged neonatal hyperinsulinism. J Pediatr. 2006;148:
44 Perinatal-Stress HI: Evidence of Hyperinsulinism that Spontaneously Resolves (n = 24, m±sem) Resolution of Perinatal Stress Hyperinsulinism At Diagnosis After Resolution Insulin (µu/ml) 6.2± ±0 BOB (mm) 0.8± ±0.1 FFA 0.6± ±0.2 Glucagon response (mg/dl) 40±3 11±3
45 Perinatal-Stress HI: Acute Insulin Responses (AIR) (resembles GK-HI;?overexpression of HK1) (n = 11, m±sem) Perinatal-Stress 0.2 ± 0.5 Calcium Leucine Glucose Tolbutamide 2 ± 1 29 ± 6 23 ± 5 GK-HI (3) ,80 ND KATP-HI (6) 22 ± 4 5 ± 2 14 ± ± 1 GDH-HI (5) -4 ± 2 73 ± 21 Normals (6) 0.1 ± ± ± 17 2 ± 3 42 ± 9 53 ± 12
 ins454a mut 45 1.1 1.2 0.")
46 Functional Properties of GK-HI & GK-MODY Mutations & Effect of HK1 Expression HK1 plus GK Heterozygous ins454a mutation Hexokinase 1 (HK1) ins454a mut
47 Diurnal glucose profiles in severe (child 1) & mild (child 2) GCK-HI (Mean plasma glucose 50±2 vs. 63±1 mg/dl, P < ) Child 1 Child
48 Prolonged hypoglycemia in neonates: Perinatal stress hyperinsulinism *** Associated with SGA, birth asphyxia, toxemia* Common: 10% of SGA have hypoglycemic beyond 1 week of age Glucose requirement up to mg/kg/min Spontaneous remission, but can last up to 3 months No benefit from glucocorticoids Usually responds well to diazoxide Rx Mechanism uncertain, but resembles GK-HI *Collins & Leonard, Lancet 1984; ADC 1990 ** Palotto, et al *** Hoe, et al J Pediatr
49 The Elephant and The Blind Men Endo Neo
50 Neonatal hypoglycemia Hypoglycemia Day 1 Day 2+ no risk factors asymptomatic risk factors or symptomatic breast fed all others feed re-check IV dextrose re-check keep glucose > 70 workup if can t fast > 12 hr feed re-check IV dextrose re-check keep glucose > 70 workup if can t fast > 12 hr
51 Neonatal hypoglycemia take-home messages Need to be specific about type and mechanism After Day 1, Hyperinsulinism is the most frequent cause (peri-natal stress or genetic) Ketones are suppressed in neonatal hypoglycemia Glucose thresholds should be same as in older children (treatment target is to keep BS > 70 mg/dl) For medically-unresponsive hyperinsulinism, an experienced team approach is important to find & cure potential focal HI lesion
52 end
53 Glucose Thresholds Physiologically normal is mg/dl Therapeutic target for hypoglycemia is to keep BS > 70 mg/dl End-point for provocative fasting test is BS < 50 mg/dl Same for newborns as older children/adults
54 Phenotypes of Congenital Hyperinsulinism genetics Sensitivity to stimuli / inhibitors diazoxide protein leucine calcium exercise KATP KATP GDH GCK SCHAD MCT1 HNF4a UCP2 rec dom dom dom rec dom dom dom Peri-natal stress - NO yes yes NO yes ? yes + -? - yes yes? - -?

55
56 Brain Metabolism (%) Fasting Systems in Normal Child 100 glycogenolysis ketogenesis 0 gluconeogenesis Time 30 hr
57 Brain Metabolism (%) Fasting Systems: AGA Neonate on Day Time 30 hr
58 Case of Neonatal Hypoglycemia: 3 wk old WM referred to Endo clinic for possible hypoglycemia Term pregnancy, mild maternal pre-eclampsia, BW 3.8 kg DOL 2 hypothermic, lethargic, BS 35 mg/dl (breast fed); repeat BS 45; discharged on DOL3 DOL 4 at home, not nursing, lethargic in morning, seizure In ER BS 10 mg/dl; admitted Hosp #2, IV dextrose for 3 days, prefeed BS mg/dl; discharged to Endo clinic in 1-2 weeks 3 wk old, Endo clinic, admitted to Hosp #3 HI documented (suspected perinatal-stress transient HI); hypoglycemia persists, Rx diazoxide; at discharge 1 week later able to fast 16 hr with BS > 70 mg/dl 3 mon old, trial off diazoxide: HI not resolved; probable genetic HI; diazoxide restarted (still on at age 2 yr); development 3-6 mon delayed
59 Categories of hypoglycemia in neonates Transient Hypoglycemia (Day 1) High risk related to delayed feeding Mechanism: immaturities in hepatic ketogenesis and gluconeogenesis, insulin suppression until hours Prolonged Hypoglycemia (Day 2 up to several weeks) Birth asphyxia, IUGR, other peri-natal stresse Mechanism: hyperinsulinism Permanent Hypoglycemias presenting in neonates Genetic hyperinsulinism(s) Panhypopituitarism Fatty acid oxidation defects
60 Plasma Fuels (mmol/l) Fasting fuels in a normal child 4 ß-hydroxybutyrate 3 2 FFA glucose Length of Fast (hr) lactate
61 Metabolic fuels at time of hypoglycemia: 1 st postnatal fast in normal neonates (mmol/l, m±sd) (Stanley, Anday, Baker, Delivoria-Papadopolous. Pediatr 1979)
62 Plasma Insulin (µu/ml) Plasma Insulin in Children with Hyperinsulinism HI patients controls Plasma Glucose (mg/dl)
63 Congenital Hyperinsulinism Autosomal Dominant Inheritance
64 Congenital hyperinsulinism paradigm hypoglycemia fasting 1-2 days test hyperinsulinism NH 3 / acyl-carn / AIR tests 4-7 days endocrinologist 4-7 days (-) diazoxide trial focal / diffuse K ATP octreotide trial (-) 1-2 days PET radiologists (+) GDH GCK SCHAD dom K ATP other? geneticist focal surgery 65% 35% surgeon pathologist diffuse local resection 98% pancreatectomy

65 CHOP Hyperinsulinism Center
66 Canada Curaca o Hawaii Iran Iceland Japan Turkey
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA
 NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
NEONATAL HYPOGLYCEMIA HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS NEONATAL HYPOGLYCEMIA? Glucose concentration low enough to cause signs and symptoms of impaired brain
Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Patient Demographics 5/12/2016
 Patient Demographics 5/12/2016") Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Pediatric Endocrine Nursing Society May 14, 2016 Enyo Dzata, MSN, CRNP Congenital Hyperinsulinism Center Division
Beyond the Naked Eye: A Case Presentation on a Rare Form of Congenital Hyperinsulinism (HI) Pediatric Endocrine Nursing Society May 14, 2016 Enyo Dzata, MSN, CRNP Congenital Hyperinsulinism Center Division
55 Years of Idiopathic Hypoglycemia in Infants
 55 Years of Idiopathic Hypoglycemia in Infants A historical perspective on McQuarrie s Presidential Address to the 63 rd Meeting of the American Pediatric Society. Charles A. Stanley, MD LWPES President
55 Years of Idiopathic Hypoglycemia in Infants A historical perspective on McQuarrie s Presidential Address to the 63 rd Meeting of the American Pediatric Society. Charles A. Stanley, MD LWPES President
Overview. o Limitations o Normal regulation of blood glucose o Definition o Symptoms o Clinical forms o Pathophysiology o Treatment.
 Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia
Pål R. Njølstad MD PhD KG Jebsen Center for Diabetes Research University of Bergen, Norway Depertment of Pediatrics Haukeland University Hospital Broad Institute of Harvard & MIT Cambridge, MA, USA Hypoglycemia
Learning Objectives. At the conclusion of this module, participants should be better able to:
 Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Learning Objectives At the conclusion of this module, participants should be better able to: Treat asymptomatic neonatal hypoglycemia with buccal dextrose gel Develop patient-specific approaches to intravenous
Neonatal Hypoglycaemia
 Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Neonatal Hypoglycaemia Dr Shubha Srinivasan Paediatric Endocrinologist The Children s Hospital at Westmead Hypoglycaemia and the Brain CSF glucose is 2/3 that of plasma Intracerebral glucose 1/3 that of
Controversies in Neonatal Hypoglycemia PAC / LAC CONFERENCE, JUNE 1 ST 2017
 Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Controversies in Neonatal Hypoglycemia PRIYA JEGATHEESAN, MD PAC / LAC CONFERENCE, JUNE 1 ST 2017 Disclosure I have no conflicts of interest to disclose Objectives Review Recommendations from different
Neonatal Hypoglycemia
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Neonatal Hypoglycemia. These podcasts are designed to give medical students an overview of key topics in pediatrics.
W1A- Cases I Learned From
 W1A- Cases I Learned From David H Adamkin, MD Professor of Pediatrics Director, Division of Neonatology Director of Nutritional Research Rounsavall Chair of Neonatal Medicine Co-Director of Neonatal Fellowship
W1A- Cases I Learned From David H Adamkin, MD Professor of Pediatrics Director, Division of Neonatology Director of Nutritional Research Rounsavall Chair of Neonatal Medicine Co-Director of Neonatal Fellowship
Challenging diagnosis of congenital hyperinsulinism in two infants of diabetic mothers with rare pathogenic KCNJ11 and HNF4A gene variants
 Huerta-Saenz et al. International Journal of Pediatric Endocrinology (2018) 2018:5 https://doi.org/10.1186/s13633-018-0060-7 CASE REPORT Open Access Challenging diagnosis of congenital hyperinsulinism
Huerta-Saenz et al. International Journal of Pediatric Endocrinology (2018) 2018:5 https://doi.org/10.1186/s13633-018-0060-7 CASE REPORT Open Access Challenging diagnosis of congenital hyperinsulinism
Diazoxide-responsive Hyperinsulinism
 Diazoxide-responsive Hyperinsulinism Linda Boyajian, CRNP Diva D. De León-Crutchlow, MD, MSCE Congenital Hyperinsulinism Center The Children s Hospital of Philadelphia Picture courtesy of Dr. Colin Hawkes
Diazoxide-responsive Hyperinsulinism Linda Boyajian, CRNP Diva D. De León-Crutchlow, MD, MSCE Congenital Hyperinsulinism Center The Children s Hospital of Philadelphia Picture courtesy of Dr. Colin Hawkes
History of Hyperinsulinism (HI) in Pediatrics and Overview of Diagnostic/Therapeutic Algorithm. Charles A. Stanley, MD CHOP HI Center
 in Pediatrics and Overview of Diagnostic/Therapeutic Algorithm. Charles A. Stanley, MD CHOP HI Center") History of Hyperinsulinism (HI) in Pediatrics and Overview of Diagnostic/Therapeutic Algorithm Charles A. Stanley, MD CHOP HI Center Discovery of Hypoglycemia January, 1922 (? by J.B. Collip) In the Beginning
History of Hyperinsulinism (HI) in Pediatrics and Overview of Diagnostic/Therapeutic Algorithm Charles A. Stanley, MD CHOP HI Center Discovery of Hypoglycemia January, 1922 (? by J.B. Collip) In the Beginning
Congenital hyperinsulinism
 SWISS SOCIETY OF NEONATOLOGY Winner of the Case of the Year Award 2012 Congenital hyperinsulinism FEBRUARY 2012 2 Morgillo D, Berger TM, Caduff JH, Barthlen W, Mohnike K, Mohnike W, Neonatal and Pediatric
SWISS SOCIETY OF NEONATOLOGY Winner of the Case of the Year Award 2012 Congenital hyperinsulinism FEBRUARY 2012 2 Morgillo D, Berger TM, Caduff JH, Barthlen W, Mohnike K, Mohnike W, Neonatal and Pediatric
PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team
 Cook Children s 1 PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team Cook Children s 2 Co-Chair: Charles Stanley
Cook Children s 1 PES Recommendations for Evaluation and Management of Hypoglycemia in Neonates, Infants, and Children Paul S. Thornton On behalf of the Team Cook Children s 2 Co-Chair: Charles Stanley
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری
 بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
بنام خدا هیپوگلیسمی درنوزادان و گاالکتوزمی دکتر انتظاری Serum glucose< 35 mg/dl 1-3 hr of life < 40 mg/dl 3-24 hr < 45 mg/dl after 24 hr 10% NL newborns can t maintain BS>30 if delayed feeding >3-6 hrs
7/11/2018. Oral Dextrose Gel Treatment for Newborns with Hypoglycemia Reduces NICU Admissions DISCLOSURE. Objectives
 Gaps in Knowledge, Competence, Performance, or Patient Outcomes DISCLOSURE The content of this presentation does not relate to any product of a commercial entity; therefore, I have no relationships to
Gaps in Knowledge, Competence, Performance, or Patient Outcomes DISCLOSURE The content of this presentation does not relate to any product of a commercial entity; therefore, I have no relationships to
Hypoglycemia in congenital hyperinsulinism
 How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
How a normal body works: Our body is constantly at work. Our cells need a source of energy, and this source of energy is called glucose. The process is quite simple; think of it like an assembly line.
Surgery in Congenital Hyperinsulinismless. Winfried Barthlen
 Surgery in Congenital Hyperinsulinismless may be more Winfried Barthlen congenital hyperinsulinism - very rare (1:40.000) - uncontrolled insulin secretion - life threatening hypoglycemia symptoms - unconsciousness,
Surgery in Congenital Hyperinsulinismless may be more Winfried Barthlen congenital hyperinsulinism - very rare (1:40.000) - uncontrolled insulin secretion - life threatening hypoglycemia symptoms - unconsciousness,
Cook Children s Hyperinsulinism Center
 Cook Children s Hyperinsulinism Center Dear friends and colleagues, It is my privilege to present Cook Children s Hyperinsulinism Center, one of only two of its kind in the country. At Cook Children s,
Cook Children s Hyperinsulinism Center Dear friends and colleagues, It is my privilege to present Cook Children s Hyperinsulinism Center, one of only two of its kind in the country. At Cook Children s,
Managing Congenital Hyperinsulinism in the Neonatal Period Vall d Hebron Hospital s Approach and Experience
 Managing Congenital Hyperinsulinism in the Alejandro Vargas Pieck Miquel Gussinyer Canadell María Clemente León Diego Yeste Fernández Universidad Autónoma de Barcelona Antonio Carrascosa Lezcano The first
Managing Congenital Hyperinsulinism in the Alejandro Vargas Pieck Miquel Gussinyer Canadell María Clemente León Diego Yeste Fernández Universidad Autónoma de Barcelona Antonio Carrascosa Lezcano The first
Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia
 Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Neonatal Nursing Education Brief: Evidence-Based Update: Using Glucose Gel to Treat Neonatal Hypoglycemia http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/
Cook Children s HI Center. Paul Thornton Medical Director Cook Children s Hyperinsulinism Center
 Cook Children s HI Center Paul Thornton Medical Director Cook Children s Hyperinsulinism Center Formed in Oct 2010 Cook Children s HI Center Mission: To provide excellence in medical care to patients with
Cook Children s HI Center Paul Thornton Medical Director Cook Children s Hyperinsulinism Center Formed in Oct 2010 Cook Children s HI Center Mission: To provide excellence in medical care to patients with
THE IMPORTANCE OF GENETICS WHEN TREATING HYPERINSULINISM
 THE IMPORTANCE OF GENETICS WHEN TREATING HYPERINSULINISM HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS HYPERINSULINISM? The leading cause of hypoglycemia in infants and
THE IMPORTANCE OF GENETICS WHEN TREATING HYPERINSULINISM HEATHER MCKNIGHT-MENCI, MSN, CRNP CHILDREN S HOSPITAL OF PHILADELPHIA WHAT IS HYPERINSULINISM? The leading cause of hypoglycemia in infants and
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children
 National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
National Metabolic Biochemistry Network Guidelines for the investigation of hypoglycaemia in infants and children Aim To provide guidance on the biochemical investigation of hypoglycaemia in infants and
Paediatric Hypoglycaemia and the Laboratory. AACB Webinar, 8 th April 2015 Tina Yen
 Paediatric Hypoglycaemia and the Laboratory AACB Webinar, 8 th April 2015 Tina Yen Synopsis Definition and classification Newborn and Neonatal Hypoglycaemia Transient Persistant Hypoglycaemia in infants
Paediatric Hypoglycaemia and the Laboratory AACB Webinar, 8 th April 2015 Tina Yen Synopsis Definition and classification Newborn and Neonatal Hypoglycaemia Transient Persistant Hypoglycaemia in infants
Remission in Non-Operated Patients with Diffuse Disease and Long-Term Conservative Treatment.
 5th Congenital Hyperinsulinism International Family Conference Milan, September 17-18 Remission in Non-Operated Patients with Diffuse Disease and Long-Term Conservative Treatment. PD Dr. Thomas Meissner
5th Congenital Hyperinsulinism International Family Conference Milan, September 17-18 Remission in Non-Operated Patients with Diffuse Disease and Long-Term Conservative Treatment. PD Dr. Thomas Meissner
Hyperglycaemia. Clinical presentation. Definition of hyperglycaemia. Approach to the problem
 Hyperglycaemia 1 Clinical presentation Hyperglycaemia is usually picked up incidentally on routine blood glucose assessment or in response to finding glycosuria. It may be noted as part of the workup of
Hyperglycaemia 1 Clinical presentation Hyperglycaemia is usually picked up incidentally on routine blood glucose assessment or in response to finding glycosuria. It may be noted as part of the workup of
Hypoglycaemia of the neonate. Dr. L.G. Lloyd Dept. Paediatrics
 Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Hypoglycaemia of the neonate Dr. L.G. Lloyd Dept. Paediatrics Why is glucose important? It provides 60-70% of energy needs Utilization obligatory by red blood cells, brain and kidney as major source of
Neurodevelopmental Risk?
 Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Normal Newborn During transitional hypoglycemia normal newborns have an enhanced ketogenic response to fasting. Newborn brains have enhanced capability to use ketone bodies for fuel Allows newborns to
Neonatal Hypoglycemia. Presented By : Kamlah Olaimat 25\7\2010
 Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Neonatal Hypoglycemia Presented By : Kamlah Olaimat 25\7\2010 Definition The S.T.A.B.L.E. Program defines hypoglycemia as: Glucose delivery or availability is inadequate to meet glucose demand (Karlsen,
Re-Evaluating Transitional Neonatal Hypoglycemia : Mechanism and Implications for Management
 Re-Evaluating Transitional Neonatal Hypoglycemia : Mechanism and Implications for Management Charles A. Stanley, MD 1, Paul J. Rozance, MD 2, Paul S. Thornton, MB, BCh 3, Diva D. De Leon, MD 1, Deborah
Re-Evaluating Transitional Neonatal Hypoglycemia : Mechanism and Implications for Management Charles A. Stanley, MD 1, Paul J. Rozance, MD 2, Paul S. Thornton, MB, BCh 3, Diva D. De Leon, MD 1, Deborah
By: Dr. Doaa Khater Yassin, MM and M.D Paed Sr. specialist of Pediatrics SQUH
 By: Dr. Doaa Khater Yassin, MM and M.D Paed Sr. specialist of Pediatrics SQUH Born SGA with birth weight of 2.4 kg, had IUGR Hospitalized at the age of 2 month with severe dehydration Diagnosed as DKA
By: Dr. Doaa Khater Yassin, MM and M.D Paed Sr. specialist of Pediatrics SQUH Born SGA with birth weight of 2.4 kg, had IUGR Hospitalized at the age of 2 month with severe dehydration Diagnosed as DKA
The Surgeon General s Call to Action and the
 Case of the Month Pamela Heaberlin, MS, RN, NNP-BC Section Editor 2.3 HOURS Continuing Education Congenital Hyperinsulinism Exclusive Human Milk and Breastfeeding Taryn M. Edwards, MSN, CRNP, NNP-BC ;
Case of the Month Pamela Heaberlin, MS, RN, NNP-BC Section Editor 2.3 HOURS Continuing Education Congenital Hyperinsulinism Exclusive Human Milk and Breastfeeding Taryn M. Edwards, MSN, CRNP, NNP-BC ;
Newborn Hypoglycemia
 Newborn Hypoglycemia Self Learning Module Developed by the Interprofessional Education and Research Committee of the Champlain Maternal Newborn Regional Program (CMNRP) 2013 TABLE OF CONTENTS Definition....3
Newborn Hypoglycemia Self Learning Module Developed by the Interprofessional Education and Research Committee of the Champlain Maternal Newborn Regional Program (CMNRP) 2013 TABLE OF CONTENTS Definition....3
A novel case of compound heterozygous congenital hyperinsulinism without high insulin levels
 Brady et al. International Journal of Pediatric Endocrinology (2015) 2015:16 DOI 10.1186/s13633-015-0012-4 CASE REPORT Open Access A novel case of compound heterozygous congenital hyperinsulinism without
Brady et al. International Journal of Pediatric Endocrinology (2015) 2015:16 DOI 10.1186/s13633-015-0012-4 CASE REPORT Open Access A novel case of compound heterozygous congenital hyperinsulinism without
Case 1. Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Faculty Financial Disclosures 3/8/2018
 Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Shawnte R. James, MD, FAAP Assistant Professor Newborn Medicine Hospitalist Emory University School of Medicine Department of Pediatrics
Managing Neonatal Hypoglycemia: Can formula supplementation be avoided? Shawnte R. James, MD, FAAP Assistant Professor Newborn Medicine Hospitalist Emory University School of Medicine Department of Pediatrics
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn Committee Child Health Standards
NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn Committee Child Health Standards
PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS. A17/S(HSS)/a Congenital hyperinsulinism service (Children)
/a Congenital hyperinsulinism service (Children)") A17/S(HSS)/a 2013/14 NHS STANDARD CONTRACT FOR CONGENITAL HYPERINSULINISM SERVICE (CHILDREN) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner
A17/S(HSS)/a 2013/14 NHS STANDARD CONTRACT FOR CONGENITAL HYPERINSULINISM SERVICE (CHILDREN) PARTICULARS, SCHEDULE 2- THE SERVICES, A- SERVICE SPECIFICATIONS Service Specification No. Service Commissioner
Not Your Typical Case of Ketotic Hypoglycemia
 Not Your Typical Case of Ketotic Hypoglycemia Linda Steinkrauss, RN, MSN, CPNP Objectives By the end of this session, attendees should be able to: 1. Discuss the difference between idiopathic ketotic hypoglycemia
Not Your Typical Case of Ketotic Hypoglycemia Linda Steinkrauss, RN, MSN, CPNP Objectives By the end of this session, attendees should be able to: 1. Discuss the difference between idiopathic ketotic hypoglycemia
Summary of Changes: References/content updated to reflect most current standards of practice.
 Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
Alaska Native Medical Center: Mother Baby Unit Guideline: Neonatal Hypoglycemia Subject: Neonatal Hypoglycemia REVISION DATE: Jan 2015,12/2011, 02/2009, 11, 2007, 07/2007,04/2001, 04/1999 REPLACES: NSY:
How Un It is: The Conundrum of What to Do for Transient Neonatal Hypoglycemia
 How Un It is: The Conundrum of What to Do for Transient Neonatal Hypoglycemia Jeffrey R. Kaiser, MD, MA Kenneth V. and Eleanor M. Hatt Professor of Neonatal Medicine Division of Neonatal-Perinatal Medicine
How Un It is: The Conundrum of What to Do for Transient Neonatal Hypoglycemia Jeffrey R. Kaiser, MD, MA Kenneth V. and Eleanor M. Hatt Professor of Neonatal Medicine Division of Neonatal-Perinatal Medicine
PRACTICE GUIDELINES WOMEN S HEALTH PROGRAM
 C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
C Title: NEWBORN: HYPOGLYCEMIA IN NEONATES BORN AT 35+0 WEEKS GESTATION AND GREATER: DIAGNOSIS AND MANAGEMENT IN THE FIRST 72 HOURS Authorization Section Head, Neonatology, Program Director, Women s Health
An interesting case of recurrent seizures. By Dr S.Murugarajan Final yr DNB pg Dr Kannan HOD Railway hospital, Perambur.
 An interesting case of recurrent seizures By Dr S.Murugarajan Final yr DNB pg Dr Kannan HOD Railway hospital, Perambur. Chief complaints A 6 months old male infant, 1 st born of second degree consanguineous
An interesting case of recurrent seizures By Dr S.Murugarajan Final yr DNB pg Dr Kannan HOD Railway hospital, Perambur. Chief complaints A 6 months old male infant, 1 st born of second degree consanguineous
Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359
 Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Chair of Paediatric Clinical Governance Governance
Guideline for the Prevention and Management of Neonatal Hypoglycaemia GL359 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Chair of Paediatric Clinical Governance Governance
Deb Cobie Judy Evans Professionally Approved By Dr Saravanan Consultant Lead for Risk Management June 2009
 TREATMENT OF NEONATAL HYPOGLYCAEMIA Developed in response to: Contributes to CQC Standards No CLINICAL GUIDELINES Register No: 04219 Status: Public Intrapartum NICE Guidelines RCOG guideline C5a Consulted
TREATMENT OF NEONATAL HYPOGLYCAEMIA Developed in response to: Contributes to CQC Standards No CLINICAL GUIDELINES Register No: 04219 Status: Public Intrapartum NICE Guidelines RCOG guideline C5a Consulted
Linda Boyajian, RN, MSN, CRNP Congenital Hyperinsulinism Center Children s Hospital of Philadelphia
 Linda Boyajian, RN, MSN, CRNP Congenital Hyperinsulinism Center Children s Hospital of Philadelphia Congenital Hyperinsulinism refers to a variety of congenital disorders in which hypoglycemia is caused
Linda Boyajian, RN, MSN, CRNP Congenital Hyperinsulinism Center Children s Hospital of Philadelphia Congenital Hyperinsulinism refers to a variety of congenital disorders in which hypoglycemia is caused
Intrapartum and Postpartum Management of the Diabetic Mother and Infant
 Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Intrapartum and Postpartum Management of the Diabetic Mother and Infant Intrapartum Management Women with gestational diabetes who maintain normal glucose levels during pregnancy on diet and exercise therapy
Guidelines for the Prevention and Management of Hypoglycaemia
 ASHFORD & ST PETER S HOSPITALS NHS TRUST CHILDREN S SERVICES Guidelines for the Prevention and Management of Hypoglycaemia 1. The Care Plan for Prevention of Hypoglycaemia on Labour Ward and the Postnatal
ASHFORD & ST PETER S HOSPITALS NHS TRUST CHILDREN S SERVICES Guidelines for the Prevention and Management of Hypoglycaemia 1. The Care Plan for Prevention of Hypoglycaemia on Labour Ward and the Postnatal
Use of Lanreotide (long acting Somatostatin analogue) in Congenital Hyperinsulinism (CHI)
 in Congenital Hyperinsulinism (CHI)") Use of Lanreotide (long acting Somatostatin analogue) in Congenital Hyperinsulinism (CHI) Dr Pratik Shah Clinical Research fellow in Hyperinsulinism Clinical Molecular Genetics Unit Institute of Child
Use of Lanreotide (long acting Somatostatin analogue) in Congenital Hyperinsulinism (CHI) Dr Pratik Shah Clinical Research fellow in Hyperinsulinism Clinical Molecular Genetics Unit Institute of Child
Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number:
 This is an official Northern Trust policy and should not be edited in any way Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number: NHSCT/10/293 Target audience: Midwifery,
This is an official Northern Trust policy and should not be edited in any way Prevention and Management of Hypoglycaemia of the Breastfed Newborn Reference Number: NHSCT/10/293 Target audience: Midwifery,
Neonatal hypoglycemia Sharon Straussman and Lynne L. Levitsky
 Neonatal hypoglycemia Sharon Straussman and Lynne L. Levitsky Pediatric Endocrine Unit, Massachusetts General Hospital, Boston, Massachusetts, USA Correspondence to Lynne L. Levitsky, MD, Chief, Pediatric
Neonatal hypoglycemia Sharon Straussman and Lynne L. Levitsky Pediatric Endocrine Unit, Massachusetts General Hospital, Boston, Massachusetts, USA Correspondence to Lynne L. Levitsky, MD, Chief, Pediatric
Case Reports. Diffuse Type Hyperinsulinaemic Hypoglycaemia of Infancy: Case Report of Management without Pancreatectomy
 HK J Paediatr (new series) 2014;19:252-256 Case Reports Diffuse Type Hyperinsulinaemic Hypoglycaemia of Infancy: Case Report of Management without Pancreatectomy THY TAN, KL NG Abstract Key words Congenital
HK J Paediatr (new series) 2014;19:252-256 Case Reports Diffuse Type Hyperinsulinaemic Hypoglycaemia of Infancy: Case Report of Management without Pancreatectomy THY TAN, KL NG Abstract Key words Congenital
Heartland Genetics and Newborn Screening Collaborative Conference
 Heartland Genetics and Newborn Screening Collaborative Conference Laurel K. Willig, MD Assistant Medical Director for the Center for Pediatric Genomic Medicine and Joshua E. Petrikin, MD Director of Neonatal
Heartland Genetics and Newborn Screening Collaborative Conference Laurel K. Willig, MD Assistant Medical Director for the Center for Pediatric Genomic Medicine and Joshua E. Petrikin, MD Director of Neonatal
Neonatal Hypoglycaemia Guidelines
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad
 Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Gestational Diabetes Mellitus Dr. Fawaz Amin Saad Senior Consultant OB/GYN, Al-Hayat Medical Center, Doha, Qatar DISCLOSURE OF CONFLICT OF INTEREST I am a full-time Employee at Al-Hayat Medical Center.
Diagnosis and treatment of hyperinsulinaemic hypoglycaemia and its implications for paediatric endocrinology
 Demirbilek et al. International Journal of Pediatric Endocrinology (2017) 2017:9 DOI 10.1186/s13633-017-0048-8 REVIEW Diagnosis and treatment of hyperinsulinaemic hypoglycaemia and its implications for
Demirbilek et al. International Journal of Pediatric Endocrinology (2017) 2017:9 DOI 10.1186/s13633-017-0048-8 REVIEW Diagnosis and treatment of hyperinsulinaemic hypoglycaemia and its implications for
Nottingham Neonatal Service Guideline
 Title: Screening and Management of Neonatal Hypoglycaemia Version: 10 Ratification Date: Review Date: Jan 2023 Approval: Nottingham Neonatal Service Clinical Guideline Meeting Author: Shalini Ojha 1, Lara
Title: Screening and Management of Neonatal Hypoglycaemia Version: 10 Ratification Date: Review Date: Jan 2023 Approval: Nottingham Neonatal Service Clinical Guideline Meeting Author: Shalini Ojha 1, Lara
Paediatric Clinical Chemistry
 Paediatric Clinical Chemistry Dr N Oosthuizen Dept Chemical Pathology UP 2011 Paediatric biochemistry The child is not a miniature adult Physiological development Immature organ systems Growing individual
Paediatric Clinical Chemistry Dr N Oosthuizen Dept Chemical Pathology UP 2011 Paediatric biochemistry The child is not a miniature adult Physiological development Immature organ systems Growing individual
Alvaro Serrano Russi MD University of Iowa Hospitals and Clinics
 Retrospective Analysis of the Region 4 Post Analytical Tool and Confirmatory Testing for Long Chain Fatty Acid Oxidation Disorders Screened in the State of Iowa Alvaro Serrano Russi MD University of Iowa
Retrospective Analysis of the Region 4 Post Analytical Tool and Confirmatory Testing for Long Chain Fatty Acid Oxidation Disorders Screened in the State of Iowa Alvaro Serrano Russi MD University of Iowa
Research Article A Novel Algorithm in the Management of Hypoglycemia in Newborns
 International Pediatrics, Article ID 935726, 5 pages http://dx.doi.org/10.1155/2014/935726 Research Article A Novel Algorithm in the Management of Hypoglycemia in Newborns Swapna Naveen, Chikati Rosy,
International Pediatrics, Article ID 935726, 5 pages http://dx.doi.org/10.1155/2014/935726 Research Article A Novel Algorithm in the Management of Hypoglycemia in Newborns Swapna Naveen, Chikati Rosy,
Hyperinsulinaemic Hypoglycaemia
 Review 157 Hyperinsulinaemic Hypoglycaemia Authors V. B. Arya 1, Z. Mohammed 1, O. Blankenstein 2, P. De Lonlay 3, K. Hussain 1 Affiliations Key words congenital hyperinsulinism hyperinsulinaemic hypoglycaemia
Review 157 Hyperinsulinaemic Hypoglycaemia Authors V. B. Arya 1, Z. Mohammed 1, O. Blankenstein 2, P. De Lonlay 3, K. Hussain 1 Affiliations Key words congenital hyperinsulinism hyperinsulinaemic hypoglycaemia
Clinical Study An Evaluation of Growth Hormone and IGF-1 Responses in Neonates with Hyperinsulinaemic Hypoglycaemia
 International Endocrinology Volume 2013, Article ID 638257, 5 pages http://dx.doi.org/10.1155/2013/638257 Clinical Study An Evaluation of Growth Hormone and IGF-1 Responses in Neonates with Hyperinsulinaemic
International Endocrinology Volume 2013, Article ID 638257, 5 pages http://dx.doi.org/10.1155/2013/638257 Clinical Study An Evaluation of Growth Hormone and IGF-1 Responses in Neonates with Hyperinsulinaemic
ANATOMY OF A METABOLIC CRISIS: FAOD-style. Mark S. Korson, MD Tufts Medical Center Boston, MA
 ANATOMY OF A METABOLIC CRISIS: FAOD-style Mark S. Korson, MD Tufts Medical Center Boston, MA NORMAL PHYSIOLOGY Anabolic Eating well Calories eaten > body s needs BRAIN uses GLUCOSE MUSCLE uses GLUCOSE
ANATOMY OF A METABOLIC CRISIS: FAOD-style Mark S. Korson, MD Tufts Medical Center Boston, MA NORMAL PHYSIOLOGY Anabolic Eating well Calories eaten > body s needs BRAIN uses GLUCOSE MUSCLE uses GLUCOSE
Diabetes in Pregnancy. L.Sekhavat MD
 Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
Diabetes in Pregnancy L.Sekhavat MD Diabetes in Pregnancy Gestational Diabetes Pre-gestational diabetes (overt) Insulin dependent (type1) Non-insulin dependent (type 2) Definition Gestational diabetes
Glucose Metabolism in The NICU. Reese H. Clark, MD Pediatrix Medical Group
 Glucose Metabolism in The NICU Reese H. Clark, MD Pediatrix Medical Group Objectives To discuss the physiology of glucose metabolism To review the derivation of the definition of hypoglycemia To identify
Glucose Metabolism in The NICU Reese H. Clark, MD Pediatrix Medical Group Objectives To discuss the physiology of glucose metabolism To review the derivation of the definition of hypoglycemia To identify
LRI Children s Hospital
 LRI Children s Hospital Hypoglycaemia in Infants & Children (not for use in the NNU or for Children diagnosed with diabetes) Staff relevant to: Clinical staff working within the UHL Children s Hospital.
LRI Children s Hospital Hypoglycaemia in Infants & Children (not for use in the NNU or for Children diagnosed with diabetes) Staff relevant to: Clinical staff working within the UHL Children s Hospital.
Week 3, Lecture 5a. Pathophysiology of Diabetes. Simin Liu, MD, ScD
 Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
Neonatal Diabetes. Objectives. Conflicts of Interest Disclosure. No conflicts of interest related to the content of this presentation
 Neonatal Diabetes Shannon Abernethy BSN, RN, CPN Pediatric Nurse Navigator Bon Secours Virginia Medical Group Pediatric Endocrinology and Diabetes Associates 1 Objectives Identify and define neonatal diabetes
Neonatal Diabetes Shannon Abernethy BSN, RN, CPN Pediatric Nurse Navigator Bon Secours Virginia Medical Group Pediatric Endocrinology and Diabetes Associates 1 Objectives Identify and define neonatal diabetes
4/23/2015. Linda Steinkrauss, MSN, PNP. No conflicts of interest
 Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
Linda Steinkrauss, MSN, PNP No conflicts of interest 1 5 year old African-American female presented to our Endocrinology Clinic with hypoglycemia Abnormal chromosomes Duplication of 11q13.5-11p14.1 affecting
THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals
 Br. J. Anaesth. (1981), 53, 131 THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals J. C. STANLEY In this paper, the glucose-fatty acid cycle
Br. J. Anaesth. (1981), 53, 131 THE GLUCOSE-FATTY ACID-KETONE BODY CYCLE Role of ketone bodies as respiratory substrates and metabolic signals J. C. STANLEY In this paper, the glucose-fatty acid cycle
CARE OF THE NEWBORN HYPOGLYCAEMIA
 CARE OF THE NEWBORN HYPOGLYCAEMIA Background Definition A true blood glucose of less than 2.6 mmol/l venous sample. Neonatal hypoglycaemia is commonly defined as a true blood glucose of less than 2.6 mmol/l
CARE OF THE NEWBORN HYPOGLYCAEMIA Background Definition A true blood glucose of less than 2.6 mmol/l venous sample. Neonatal hypoglycaemia is commonly defined as a true blood glucose of less than 2.6 mmol/l
ARTICLE. Experience With Intravenous Glucagon Infusions as a Treatment for Resistant Neonatal Hypoglycemia
 ARTICLE Experience With Intravenous Glucagon Infusions as a Treatment for Resistant Neonatal Hypoglycemia Robin E. Miralles, MB, BCh, MRCPCH; Abhay Lodha, MD, DM; Max Perlman, MB, FRCPC; Aideen M. Moore,
ARTICLE Experience With Intravenous Glucagon Infusions as a Treatment for Resistant Neonatal Hypoglycemia Robin E. Miralles, MB, BCh, MRCPCH; Abhay Lodha, MD, DM; Max Perlman, MB, FRCPC; Aideen M. Moore,
Permanent neonatal diabetes mellitus. Case Report
 Rawal Medical Journal An official publication of Pakistan Medical Association Rawalpindi Islamabad branch Established 1975 Volume 36 Number 4 October - December 2011 Case Report Permanent neonatal diabetes
Rawal Medical Journal An official publication of Pakistan Medical Association Rawalpindi Islamabad branch Established 1975 Volume 36 Number 4 October - December 2011 Case Report Permanent neonatal diabetes
What is symptomatic? Neonatal hypoglycemia: how low can you go? Hypoglycemia and MRI. Conflicts. What s the problem? Hypoglycemia and MRI
 Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Neonatal hypoglycemia: how low can you go? Kristi Watterberg, MD Professor of Pediatrics, UNM What is symptomatic? Jitteriness Cyanosis Poor feeding Weak, high-pitched cry Seizures Apnea Lethargy, low
Prevention and Management of Hypoglycaemia
 Prevention and Management of Hypoglycaemia Use for ALL babies on the Labour Ward, Postnatal Ward & Transitional Care. This guideline is based on the BAPM Hypoglycaemia Guideline 2017. This guideline should
Prevention and Management of Hypoglycaemia Use for ALL babies on the Labour Ward, Postnatal Ward & Transitional Care. This guideline is based on the BAPM Hypoglycaemia Guideline 2017. This guideline should
Advances in the diagnosis and management of hyperinsulinemic hypoglycemia
 Advances in the diagnosis and management of hyperinsulinemic hypoglycemia Ritika R Kapoor, Chela James and Khalid Hussain* SUMMARY Hyperinsulinemic hypoglycemia (HH) is a consequence of unregulated insulin
Advances in the diagnosis and management of hyperinsulinemic hypoglycemia Ritika R Kapoor, Chela James and Khalid Hussain* SUMMARY Hyperinsulinemic hypoglycemia (HH) is a consequence of unregulated insulin
Hormonal Regulations Of Glucose Metabolism & DM
 Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
RECENTLY, WE AND others described an unusual form
 0013-7227/01/$03.00/0 The Journal of Clinical Endocrinology & Metabolism 86(8):3724 3728 Printed in U.S.A. Copyright 2001 by The Endocrine Society Acute Insulin Responses to Leucine in Children with the
0013-7227/01/$03.00/0 The Journal of Clinical Endocrinology & Metabolism 86(8):3724 3728 Printed in U.S.A. Copyright 2001 by The Endocrine Society Acute Insulin Responses to Leucine in Children with the
Hormonal regulation of. Physiology Department Medical School, University of Sumatera Utara
 Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Vishwanath Pattan Endocrinology Wyoming Medical Center
 Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Fatty Acid Oxidation Disorders- an update. Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London
 Fatty Acid Oxidation Disorders- an update Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London An update. Overview of metabolism Clinical presentation and outcome Diagnostic
Fatty Acid Oxidation Disorders- an update Fiona Carragher Biochemical Sciences, GSTS Pathology St Thomas Hospital, London An update. Overview of metabolism Clinical presentation and outcome Diagnostic
Diabetes mellitus. Diabetes mellitus - 1. Diabetes mellitus Lecture from pathological physiology
 Diabetes mellitus Lecture from pathological physiology Oliver Rácz, 2007-2018 Šafárik University, Košice, Slovakia In cooperation with F. Ništiar, (immunology) A. Chmelárová, (biochemistry) D. Kuzmová,
Diabetes mellitus Lecture from pathological physiology Oliver Rácz, 2007-2018 Šafárik University, Košice, Slovakia In cooperation with F. Ništiar, (immunology) A. Chmelárová, (biochemistry) D. Kuzmová,
Staff at the Nottingham Children s Hospital. Guidelines process; paediatric endocrinology team
 Hypoglycaemia Title of Guideline Contact Name and Job Title (author) Hypoglycaemia in infants and children: aetiology, investigation and treatment Dr. Hoong-Wei Gan ST6 Paediatric Endocrinology & Diabetes
Hypoglycaemia Title of Guideline Contact Name and Job Title (author) Hypoglycaemia in infants and children: aetiology, investigation and treatment Dr. Hoong-Wei Gan ST6 Paediatric Endocrinology & Diabetes
A novel mutation of ABCC8 gene in a patient with diazoxide-unresponsive congenital hyperinsulinism
 Case report Park Korean JS, J et Pediatr al. Congenital 2016;59(Suppl hyperinsulinism 1):S116-120with a novel mutation of ABCC8 pissn 1738-1061 eissn 2092-7258 Korean J Pediatr A novel mutation of ABCC8
Case report Park Korean JS, J et Pediatr al. Congenital 2016;59(Suppl hyperinsulinism 1):S116-120with a novel mutation of ABCC8 pissn 1738-1061 eissn 2092-7258 Korean J Pediatr A novel mutation of ABCC8
Paul Hofman. Professor. Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland
 Professor Paul Hofman Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland 9:25-9:50 Endocrine and Metabolic Consequences of Being Born Preterm
Professor Paul Hofman Paediatrician Endocrinologist Liggins Institute, The University of Auckland, Starship Children Hospital, Auckland 9:25-9:50 Endocrine and Metabolic Consequences of Being Born Preterm
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016, Last Revised July 2018 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn
NEONATAL CLINICAL PRACTICE GUIDELINE 1.0 PURPOSE AND INTENT Title: Approval Date: March 2016, Last Revised July 2018 Approved by: Neonatal Patient Care Teams, HSC & SBH Women s Health Maternal Newborn
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Congenital hyperinsulinism (HI) is the leading cause of
 is the leading cause of") ORIGINAL ARTICLE High Risk of Diabetes and Neurobehavioral Deficits in Individuals With Surgically Treated Hyperinsulinism Katherine Lord, Jerilynn Radcliffe, Paul R. Gallagher, N. Scott Adzick, Charles
ORIGINAL ARTICLE High Risk of Diabetes and Neurobehavioral Deficits in Individuals With Surgically Treated Hyperinsulinism Katherine Lord, Jerilynn Radcliffe, Paul R. Gallagher, N. Scott Adzick, Charles
Clinical Director for Women s and Children s Directorate
 TREATMENT OF NEONATAL HYPOGLYCAEMIA IN THE HIGH RISK INFANT CLINICAL GUIDELINES Register No: 12025 Status: Public Developed in response to: Intrapartum NICE Guidelines RCOG guideline Contributes to CQC
TREATMENT OF NEONATAL HYPOGLYCAEMIA IN THE HIGH RISK INFANT CLINICAL GUIDELINES Register No: 12025 Status: Public Developed in response to: Intrapartum NICE Guidelines RCOG guideline Contributes to CQC
Glucose Homeostasis. Liver. Glucose. Muscle, Fat. Pancreatic Islet. Glucose utilization. Glucose production, storage Insulin Glucagon
 Glucose Homeostasis Liver Glucose Glucose utilization Glucose production, storage Insulin Glucagon Muscle, Fat Pancreatic Islet Classification of Diabetes Type 1 diabetes Type 2 diabetes Other types of
Glucose Homeostasis Liver Glucose Glucose utilization Glucose production, storage Insulin Glucagon Muscle, Fat Pancreatic Islet Classification of Diabetes Type 1 diabetes Type 2 diabetes Other types of
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting
 Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting Kristin Lindstrom, MD Division of Genetics and Metabolism Phoenix Children s Hospital AzAAP Pediatrics in the Red
Work-Up and Initial Management of Common Metabolic Emergencies in the Inpatient Setting Kristin Lindstrom, MD Division of Genetics and Metabolism Phoenix Children s Hospital AzAAP Pediatrics in the Red
2018 Standard of Medical Care Diabetes and Pregnancy
 2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
2018 Standard of Medical Care Diabetes and Pregnancy 2018 Standard of Medical Care Diabetes and Pregnancy Marjorie Cypress does not have any relevant financial relationships with any commercial interests
Management of Pregestational and Gestational Diabetes Mellitus
 Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
Background and Prevalence Management of Pregestational and Gestational Diabetes Mellitus Pregestational Diabetes - 8 million women in the US are affected, complicating 1% of all pregnancies. Type II is
Long-term treatment with Lanreotide in CHI
 Long-term treatment with Lanreotide in CHI Oliver Blankenstein Institute for Experimental Paediatric Endocrinology Charité-Universitätsmedizin Berlin U N I V E R S I T Ä T S M E D I Z I N B E R L I N 5
Long-term treatment with Lanreotide in CHI Oliver Blankenstein Institute for Experimental Paediatric Endocrinology Charité-Universitätsmedizin Berlin U N I V E R S I T Ä T S M E D I Z I N B E R L I N 5
Gestational Diabetes. Gestational Diabetes:
 Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Gestational Diabetes Detection and Management Steven Gabbe, MD The Ohio State University Medical Center Gestational Diabetes: Detection and Management Learning Objectives: At the conclusion of this presentation,
Timing and tempo of first year growth in relation to cardiovascular and metabolic risk profile in early adulthood
 Note: for non-commercial purposes only Timing and tempo of first year growth in relation to cardiovascular and metabolic risk profile in early adulthood Anita Hokken-Koelega Professor of Pediatric Endocrinology
Note: for non-commercial purposes only Timing and tempo of first year growth in relation to cardiovascular and metabolic risk profile in early adulthood Anita Hokken-Koelega Professor of Pediatric Endocrinology
Evaluation of Maternal and Neonatal Risk factors for Neonatal Hypoglycemia
 Evaluation of Maternal and Neonatal Risk factors for Neonatal Hypoglycemia Najla I. Ayoub MBChB, MRCP, DCH* Basil M. Hanoudi MBChB, CABP* Monir H Naif MBChB* Abstract: Background; Hypoglycemia is the most
Evaluation of Maternal and Neonatal Risk factors for Neonatal Hypoglycemia Najla I. Ayoub MBChB, MRCP, DCH* Basil M. Hanoudi MBChB, CABP* Monir H Naif MBChB* Abstract: Background; Hypoglycemia is the most
Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when
 is a rare inherited disorder that occurs when") CPT2 Deficiency Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when the last step in the entry of fats into sac-like bodies called mitochondria is blocked.
CPT2 Deficiency Carnitine palmitoyl transferase 2 deficiency (CPT2) is a rare inherited disorder that occurs when the last step in the entry of fats into sac-like bodies called mitochondria is blocked.
DIABETES WITH PREGNANCY
 DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal
DIABETES WITH PREGNANCY Prof. Aasem Saif MD,MRCP(UK),FRCP (Edinburgh) Maternal and Fetal Risks Diabetes in pregnancy is associated with risks to the woman and to the developing fetus. Maternal and Fetal