I have no financial disclosures
|
|
|
- Bethanie Stephens
- 5 years ago
- Views:
Transcription

1 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1

2 6 Y/O male presents with vomiting and abdominal pain for past couple of days Felt warm Had been feeling tired prior to vomiting Clothes look looser on him Appears distressed Alert and somewhat anxious Noted tachypnea RR: 30 HR: 170, BP: 85/45 Cool extremities Diffuse abdominal pain Dry mucous membranes 2
3 Vomiting: Viral illness Appendicitis Other GI illness Sepsis Dehydrated IV obtained : 20 cc/kg bolus Labs: glucose: 497 Bicarb:5 Lactate: 5, ph:7.01 WBC:25K,HB:15 3
4 DKA New onset? Per 2014 International Society for Pediatric and Adolescent Diabetes guidelines, pediatric DKA will be defined as patients < 18 YO(cared for by pediatric services) with presenting serum glucose of > 200, venous ph < 7.30 or serum bicarbonate of < 15 with presence of ketones in either the blood and urine. 4
5 Polyuria, polydipsia, polyphagia Weight loss Fatigue Nausea/ vomiting Abdominal pain (paralytic ileus) Fruity odor to breath Hyperventilation (Kussmaul resp.) Evidence dehydration-hr, cap refill, turgor Mental status- altered, coma The clinical disturbances seen in kids in DKA are manifestations of loss of normal hormonal control of: 1. carbohydrate metabolism 2. protein metabolism 3. Fat metabolism 5
6 Hyperglycemia Acidosis Increased K (however low actual stores) Lactic acidosis Pseudohyponatremia 6
7 Dehydration: most DKA are about 10% dehydrated Kussmaul breathing Electrolyte abnormalities Mental status changes: Cerebral edema Cerebral edema is the most devastating and overt form of cerebral injury in DKA (CIDKA), accounting for up to 90% of pediatric DKA deaths. 3,4 Thoughts that there potential contributing mechanisms for CIDKA.inflammation and vasogenic factors 7

 are at highest risk of developing overt cerebral edema.")
8 The figure is excerpted from Dr. Elliot Krane s publication and indicates that the peak onset of cerebral edema is oft 6-18 hours after initiation of treatment. These data were confirmed by Glaser et al in Case control studies indicate that pediatric patients receiving sodium bicarbonate in the early phases of DKA, those presenting with severe acidosis and dehydration and those whose corrected serum sodium decrease during treatment (Glaser et al 2001, Durward et al 2011) are at highest risk of developing overt cerebral edema. Hyperglycemia raises osmolality of ECF Lowers serum sodium by dilution As insulin corrects hyperglycemia, serum sodium should rise Failure of serum sodium to rise appropriately may be sign of increased risk for cerebral edema 8
9 For each 100 mg /dl increase in blood glucose, serum Na+ will measure 1.6 meq/dl lower If glucose is 497,serum sodium may be 132 for our patient on lab results All pts in DKA are potassium depleted Insulin and correction of acidosis will drive K+ back into cells Serum K+ levels will drop Almost all pts will require K+ replacement Close monitoring is needed 9
10 Prevent depletion of RBC 2,3 DPG which will improve tissue oxygenation as acidosis is resolving May be useful in patients with anemia, CHF, pneumonia, hypoxia Phosphate therapy increased 2,3 DPG in treated group at 48 hrs. (N/S) Glucose and acidosis rates of correction were not improved Treated group had significantly lower plasma ionized calcium Tetany has been reported in pediatric patients given all replacement as KPO4 Fisher and Kitabihi
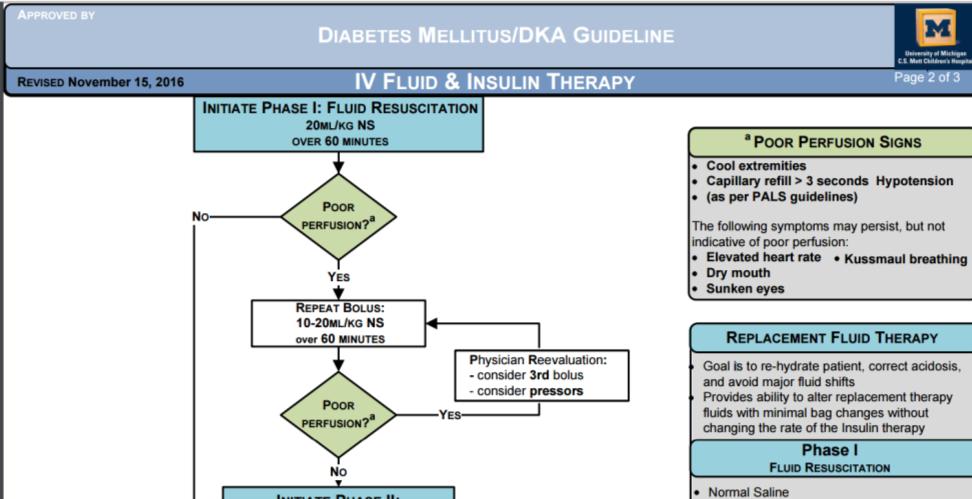
11 Correct dehydration IV Fluids Stop catabolism/ restore normoglycemia Insulin Correct electrolytes replacement (Na, Cl, K, phos) Correct acidosis/ reverse ketosis Insulin and IVF, Avoid complications of treatment Establish IV (2 if possible). Labs venous blood gas with electrolytes, CBC, Comp, Magnesium, Phosphorus, HgbA1C. Fluid bolus with isotonic fluids NS - 20ml/kg. Consider repeat 20 ml/kg ONLY if hemodynamics (especially blood pressures) are unstable. Goal of fluid resuscitation is to assure perfusion and restore blood pressure NOT to normalize HR and mentation. NO insulin bolus. NO sodium bicarbonate UNLESS patient hypotensive or in cardiopulmonary arrest. 11
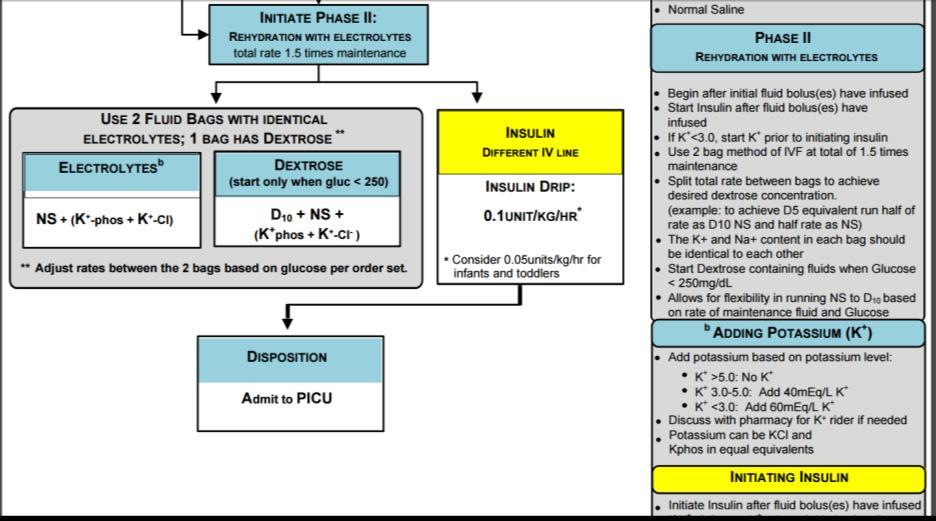
12 Very important to monitor Q1 hour neuro checks in initial resuscitation Cerebral edema is a most worrisome outcome/presentation If concern for neuro status: consider 3%saline bolus (5cc/kg) Recheck blood glucose (hourly) Goal glucose mg/dl. Start/continue insulin infusion DO NOT bolus insulin Regular Humulin Insulin at 0.1 units/kg/hour. Consider start at 0.05 units/kg/hr in infants or toddlers < 3yo with new onset DKA or in patients demonstrating extreme insulin sensitivity. IV fluids with electrolytes at 1.5 x Maintenance 12
 and Bag #2 at 50% of ordered fluid rate (0.75 x Maintenance) If Glucose between 100 119, run Bag #2 at 100% or ordered fluid rate (1.")
13 Infusion rates: If Glucose > 250 run Bag #1 at 100% of ordered fluid rate (1.5 x Maintenance) If Glucose between , run Bag #1 at 50% of ordered fluid rate (0.75 x Maintenance) and Bag #2 at 50% of ordered fluid rate (0.75 x Maintenance) If Glucose between , run Bag #2 at 100% or ordered fluid rate (1.5 x Maintenance) 13


14 Insulin infusion is NOT to be discontinued while the patient is in DKA. For patients with rapidly dropping glucose, dextrose content should be increased so that infusion can be maintained. If, after dextrose concentration is increased, glucose remains low, consider dropping infusion to 0.05 U/kg/hr but all attempts should be made NOT to stop the infusion until DKA is resolved. 14
15 15


16 Treated with above protocol guidelines Time for correction? Up to 24 hours 16


17 In children with diabetes Risk 1-10/100 person years Poor metabolic control/history of DKA Psychiatric disorders Peripubertal and adolescent girls Unstable family situation Pump therapy failure Patients are told to check all three sites Do nut disconnect pump unless sure they are in DKA TROUBLESHOOTING: 1. TUBING 2. INFUSION SET 3.NEEDLE 4.PUMP 17

18 Recognition of DKA Rehydration is important Insulin helps to restore catabolic state and not stopped until DKA resolved Careful monitoring of electrolytes and replacement Risk of Cerebral edema is most concerning 18

19 Koves,IH,Leu,MG et al; Improving Care for Pediatric Diabetic Ketoacidosis. Pediatrics 2014;134;e848 Glaser N,Barnett,P et al; Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Risk factors for cerebral edema in children with diabetic acidosis. N Engl J Med 2001;344(4): Wolfsdorf JI,Allgrove J,Craig ME,etal; ISPAD Clinical practice Consensus Guideline 2014 Compendium: Diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes 2014(suppl20): Dunger DB,Sperling MA et al; Predicting Cerebral edema during diabetic ketoacidosis. N Engl J Med. 2001;344 (4) Decourcey DD, Steil GM,etal; Increasing use of hypertonic saline over mannitol in the treatment of symptomatic cerebral edema in pediatric diabetic ketoacidosis: an 11-year Retrospective Analysis of Mortality. Pediatric Critical Care Medicine 2013:14(7)
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
Nothing to disclose. Disclosure
 Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Clinical Guideline DKA
 Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017
 CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Pediatric Diabetic Ketoacidosis Guidelines
 Pediatric Diabetic Ketoacidosis Guidelines For new onset diabetes in a pediatric patient NOT in DKA (see criteria below) These guidelines may not be appropriate Consult endocrine and pediatric admit resident
Pediatric Diabetic Ketoacidosis Guidelines For new onset diabetes in a pediatric patient NOT in DKA (see criteria below) These guidelines may not be appropriate Consult endocrine and pediatric admit resident
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital
 George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital Disclosure Statement of Financial Interest I, George Ford MD MS, DO NOT have a financial interest/arrangement
George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital Disclosure Statement of Financial Interest I, George Ford MD MS, DO NOT have a financial interest/arrangement
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
11 year-old female with altered mental status in the setting of diabetic ketoacidosis
 11 year-old female with altered mental status in the setting of diabetic ketoacidosis Katie O Sullivan, M.D. Fellow Adult/Pediatric Endocrinology University of Chicago Thursday, January 23 rd, 2014 Chief
11 year-old female with altered mental status in the setting of diabetic ketoacidosis Katie O Sullivan, M.D. Fellow Adult/Pediatric Endocrinology University of Chicago Thursday, January 23 rd, 2014 Chief
Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY
 Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY Outline Definitions and Pathophysiology of DKA Clinical Presentation/Diagnosis Treatment Process Monitoring in Hospital
Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY Outline Definitions and Pathophysiology of DKA Clinical Presentation/Diagnosis Treatment Process Monitoring in Hospital
MEDICAL VIDEO REVIEW. Mary Frey, RN Katie Kroeger, RN Brad Sobolewski, MD, MEd
 MEDICAL VIDEO REVIEW DKANovember 25, 2014 Mary Frey, RN Katie Kroeger, RN Brad Sobolewski, MD, MEd DISCLAIMER Privileged & Confidential This document is covered under the attorney-client privilege. This
MEDICAL VIDEO REVIEW DKANovember 25, 2014 Mary Frey, RN Katie Kroeger, RN Brad Sobolewski, MD, MEd DISCLAIMER Privileged & Confidential This document is covered under the attorney-client privilege. This
DIABETIC KETOACIDOSIS MANAGEMENT PLAN:
 DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
DIABETIC KETOACIDOSIS MANAGEMENT PLAN: 1. Assessment (weight, blood glucose level (BGL), blood pressure (BP), heart rate (HR), respiratory rate (RR), temperature, history & examination) 2. Resuscitation
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
DIABETES MELLITUS. IAP UG Teaching slides
 DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
DKA/HHS Pathway Phase 1 (Adult) Insulin Potassium Bicarbonate
 Insulin Potassium Bicarbonate") Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
LRI Children s Hospital
 LRI Children s Hospital Diabetic Ketoacidosis (DKA) Management in Children Staff relevant to: Medical & Nursing staff working within the UHL Children s Hospital. Team approval date: March 2017 Version:
LRI Children s Hospital Diabetic Ketoacidosis (DKA) Management in Children Staff relevant to: Medical & Nursing staff working within the UHL Children s Hospital. Team approval date: March 2017 Version:
Chapter Goal. Learning Objectives 9/12/2012. Chapter 25. Diabetic Emergencies
 Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
diabetes in adults Metabolic complications of
 Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Diabetic Emergencies. Chapter 15
 Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Diabetic Emergencies Chapter 15 Diabetes- is a disorder of glucose metabolism or difficulty metabolizing carbohydrates, fats and proteins Full name is diabetes mellitus which refers to the presence of
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
CCRN/PCCN Review Course May 30, 2013
 A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
Diabetic Ketoacidosis (DKA) v4.0: Links and Clinical Tools
 v4.0: Links and Clinical Tools") Diabetic Ketoacidosis (DKA) v4.0: Exclusion and Inclusion Criteria Pathway Overview DKA Risk Assessment ICU Admission Criteria Cerebral Edema Where Should the Child be Managed? PHASE 1: Early Electrolyte
Diabetic Ketoacidosis (DKA) v4.0: Exclusion and Inclusion Criteria Pathway Overview DKA Risk Assessment ICU Admission Criteria Cerebral Edema Where Should the Child be Managed? PHASE 1: Early Electrolyte
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology
 Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts:
 Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts: Insulin s function in the body. The basics of diabetes
Objectives / Learning Targets: The learner who successfully completes this course will be able to demonstrate understanding of the following concepts: Insulin s function in the body. The basics of diabetes
DIABETES AND PREGNANCY. CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor
 DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
DKA: Tripping on Acidosis
 DKA: Tripping on Acidosis Grace Chan Oei, MD, MA Attending Physician, Division of Pediatric Critical Care, Loma Linda University Children s Hospital Assistant Professor of Pediatrics, Loma Linda University
DKA: Tripping on Acidosis Grace Chan Oei, MD, MA Attending Physician, Division of Pediatric Critical Care, Loma Linda University Children s Hospital Assistant Professor of Pediatrics, Loma Linda University
Diabetic Ketoacidosis (DKA)
") Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Diabetic Emergencies. Goals. Diabetic Ketoacidosis (DKA) 11/6/2008. James Hardy, MD
 11/6/2008. James Hardy, MD") Diabetic Emergencies James Hardy, MD Assistant Clinical Professor Department of Emergency Medicine, UCSF Goals DKA and Hyperosmolar hyperglycemic state (HHS) Treatment guidelines (Peds vs Adult) Interesting
Diabetic Emergencies James Hardy, MD Assistant Clinical Professor Department of Emergency Medicine, UCSF Goals DKA and Hyperosmolar hyperglycemic state (HHS) Treatment guidelines (Peds vs Adult) Interesting
Pediatric Intensive Care Unit (PICU) Pediatric Diabetic Ketoacidosis (DKA) Admission Order Set
 Pediatric Diabetic Ketoacidosis (DKA) Admission Order Set") Discontinue all previous orders Weight: kg DKA admit order set is for initial management Ongoing management required based on frequent reassessment of TFI, fluid balance and lab results. Admit to PICU
Discontinue all previous orders Weight: kg DKA admit order set is for initial management Ongoing management required based on frequent reassessment of TFI, fluid balance and lab results. Admit to PICU
Wk 10. Management of Clients with Diabetes Mellitus
 Wk 10. Management of Clients with Diabetes Mellitus 2. Acute complications of DM 1) Hyperglycemia and diabetic ketoacidosis Hyperglycemia: glycogenolysis gluconeogenesis 1) Etiology and Risk Factors Taking
Wk 10. Management of Clients with Diabetes Mellitus 2. Acute complications of DM 1) Hyperglycemia and diabetic ketoacidosis Hyperglycemia: glycogenolysis gluconeogenesis 1) Etiology and Risk Factors Taking
For The Management Of. Diabetic Ketoacidosis
 Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Type I diabetes mellitus. Dr Laurence Lacroix
 mellitus Dr Laurence Lacroix 26.03.2014 1 DEFINITION: Group of diseases characterized by a disorder of glucose homeostasis with high levels of blood glucose resulting from defects in : o insulin production
mellitus Dr Laurence Lacroix 26.03.2014 1 DEFINITION: Group of diseases characterized by a disorder of glucose homeostasis with high levels of blood glucose resulting from defects in : o insulin production
Diabetic Emergencies in Pregnancy. Brian A. Mason, MS, MD
 Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
Assessment of the Patient with Endocrine Dysfunction. Objective. Endocrine. Endocrine Facts. Physical Assessment 10/3/2013
 Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
Objective Endocrine Jennifer MacDermott, MS, RN, ACNS BC, NP C, CCRN Clinical Nurse Specialist Surgical Intensive Care Unit Identify abnormal assessment finding sin a patient with endocrine dysfunction.
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter
 Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Chapter 16 Nutrition, Fluids and Electrolytes, and Acid-Base Balance Nutrition Nutrients Water o Functions Promotes metabolic processes Transporter for nutrients and wastes Lubricant Insulator and shock
Paediatric diabetic ketoacidosis
 Simon Steel FRCA Shane M Tibby MRCP Key points Diabetic ketoacidosis (DKA) is the leading cause of morbidity and mortality in children with diabetes. Cerebral oedema is the most common cause of death and
Simon Steel FRCA Shane M Tibby MRCP Key points Diabetic ketoacidosis (DKA) is the leading cause of morbidity and mortality in children with diabetes. Cerebral oedema is the most common cause of death and
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DIABETIC KETOACIDOSIS
 DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
DIABETIC KETOACIDOSIS
 DIABETIC KETOACIDOSIS MODULE: ENDOCRINOLOGY / METABOLIC TARGET: ALL PAEDIATRIC TRAINEES; NURSING STAFF BACKGROUND: DKA occurs when a relative or absolute lack of insulin leads to the inability to metabolise
DIABETIC KETOACIDOSIS MODULE: ENDOCRINOLOGY / METABOLIC TARGET: ALL PAEDIATRIC TRAINEES; NURSING STAFF BACKGROUND: DKA occurs when a relative or absolute lack of insulin leads to the inability to metabolise
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA
 The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA Introduction When a mentally altered patient arrives on the scene at any veterinary
The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA Introduction When a mentally altered patient arrives on the scene at any veterinary
Blood Glucose Monitoring
 Blood Glucose Monitoring What is Glucose? A simple sugar that enters the diet as part of sucrose, lactose, or maltose Part of a polysaccharide called dietary starch Most of the body s energy comes from
Blood Glucose Monitoring What is Glucose? A simple sugar that enters the diet as part of sucrose, lactose, or maltose Part of a polysaccharide called dietary starch Most of the body s energy comes from
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
Canada has one of the highest
 Daniel L. Metzger, MD, FAAP, FRCPC Diabetic ketoacidosis in children and adolescents: An update and revised treatment protocol Standardized pediatric-specific treatment is required to ensure safe correction
Daniel L. Metzger, MD, FAAP, FRCPC Diabetic ketoacidosis in children and adolescents: An update and revised treatment protocol Standardized pediatric-specific treatment is required to ensure safe correction
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
TOO SWEET TOO STORMY. CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth. PRESENTOR: Dr. Abhinaya PG I (M.D Paeds)
") TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
Lynda Astbury Lead Diabetes Specialist Nurse
 Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Diabetic ketoacidosis and. adults. By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences
 IN THE NAME OF GOD Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences DKA AND HHS Diabetic ketoacidosis
IN THE NAME OF GOD Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences DKA AND HHS Diabetic ketoacidosis
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Institute of Maternal and Child Research, School of Medicine, University of Chile, Santiago,
 12/13/17 1 Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State: A Consensus Statement from the International Society for Pediatric and Adolescent Diabetes Joseph I. Wolfsdorf a, Nicole Glaser b,
12/13/17 1 Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State: A Consensus Statement from the International Society for Pediatric and Adolescent Diabetes Joseph I. Wolfsdorf a, Nicole Glaser b,
DKA TREATMENT PROTOCOL Barbara Davis Center for Childhood Diabetes, University of Colorado & Children s Hospital Colorado
 2018-2019 DKA TREATMENT PROTOCOL Barbara Davis Center for Childhood Diabetes, University of Colorado & Children s Hospital Colorado Diabetic ketoacidosis (DKA) is a life-threatening condition. One in 100
2018-2019 DKA TREATMENT PROTOCOL Barbara Davis Center for Childhood Diabetes, University of Colorado & Children s Hospital Colorado Diabetic ketoacidosis (DKA) is a life-threatening condition. One in 100
Adherence to pediatric diabetic ketoacidosis guidelines by community emergency departments providers
 Zee-Cheng et al. International Journal of Emergency Medicine (2017) 10:11 DOI 10.1186/s12245-017-0137-8 International Journal of Emergency Medicine ORIGINAL RESEARCH Open Access Adherence to pediatric
Zee-Cheng et al. International Journal of Emergency Medicine (2017) 10:11 DOI 10.1186/s12245-017-0137-8 International Journal of Emergency Medicine ORIGINAL RESEARCH Open Access Adherence to pediatric
Diabetic Ketoacidosis. Raed Abu Sham a, M.D
 Diabetic Ketoacidosis Raed Abu Sham a, M.D Type 1 DM Autoimmune destruction of the pancreatic islet cell Hallmark = lymphocytic infiltration of islets Progresses over years Leads to insulin deficiency
Diabetic Ketoacidosis Raed Abu Sham a, M.D Type 1 DM Autoimmune destruction of the pancreatic islet cell Hallmark = lymphocytic infiltration of islets Progresses over years Leads to insulin deficiency
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid and Electrolytes: Parenteral
 Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Presentation of Children with Diabetic Ketoacidosis in a Tertiary Pediatric Emergency Department in Costa Rica
 Research Article imedpub Journals http://www.imedpub.com Abstract Presentation of Children with Diabetic Ketoacidosis in a Tertiary Pediatric Emergency Department in Costa Rica Background: Children with
Research Article imedpub Journals http://www.imedpub.com Abstract Presentation of Children with Diabetic Ketoacidosis in a Tertiary Pediatric Emergency Department in Costa Rica Background: Children with
PEDIATRIC DIABETIC KETOACIDOSIS
 PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois EMSC Pediatric DKA Data Dictionary Confidential for QI purposes only AIM Statement: To provide safe and effective care
PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois EMSC Pediatric DKA Data Dictionary Confidential for QI purposes only AIM Statement: To provide safe and effective care
Elke Rudloff, DVM, DACVECC
 THE DIABETIC-KETOTIC DISASTER Elke Rudloff, DVM, DACVECC EMERGENCY AND CRITICAL CARE Hyperglycemic ketoacidosis is a syndrome that can cause severe illness and death. Serum hyperosmolarity, osmotic diuresis,
THE DIABETIC-KETOTIC DISASTER Elke Rudloff, DVM, DACVECC EMERGENCY AND CRITICAL CARE Hyperglycemic ketoacidosis is a syndrome that can cause severe illness and death. Serum hyperosmolarity, osmotic diuresis,
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Multiple c hoice q uestions
 Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
ADMIT DIABETIC KETOACIDOSIS (DKA) PLAN - Phase: Begin Immediately/Emergency Center
 PLAN - Phase: Begin Immediately/Emergency Center") - Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
- Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
Acid Base Balance. Professor Dr. Raid M. H. Al-Salih. Clinical Chemistry Professor Dr. Raid M. H. Al-Salih
 Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Acid Base Balance 1 HYDROGEN ION CONCENTRATION and CONCEPT OF ph Blood hydrogen ion concentration (abbreviated [H + ]) is maintained within tight limits in health, with the normal concentration being between
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
CETEP PRE-TEST For questions 1 through 3, consider the following scenario:
 CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Use this version only
 Integrated Care Pathway PAEDIATRIC DIABETIC KETOACIDOSIS (DKA) Use this version only Patient Label Details Ward: Consultant: Named Nurse: Date of Admission: Date of Discharge/Transfer: ALL STAFF TO WRITE
Integrated Care Pathway PAEDIATRIC DIABETIC KETOACIDOSIS (DKA) Use this version only Patient Label Details Ward: Consultant: Named Nurse: Date of Admission: Date of Discharge/Transfer: ALL STAFF TO WRITE
Journal of Pediatric Critical Care P - ISSN: E - ISSN: Year: 2017 Volume: 4 Issue: 4 DOI /
 Journal of Pediatric Critical Care P - ISSN: 2349-6592 E - ISSN: 2455-709 Year: 2017 Volume: 4 Issue: 4 DOI-10.21304/2017.0403.00212 Symposium Article The Clinical Management of Diabetic Ketoacidosis Asrar
Journal of Pediatric Critical Care P - ISSN: 2349-6592 E - ISSN: 2455-709 Year: 2017 Volume: 4 Issue: 4 DOI-10.21304/2017.0403.00212 Symposium Article The Clinical Management of Diabetic Ketoacidosis Asrar
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
IDS. Pediatric Donor Management
 IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
FREQUENCY OF DIABETIC KETOACIDOSIS IN DIABETIC PATIENTS
 Original Article IN DIABETIC PATIENTS Ghulam Abbas Sheikh 1, Dilshad Muhammad 2, Khalid Amin 3 1 Consultant Physician, Aziz Fatimah Hospitals, Faisalabad. 2 Senior Registrar, DHQ Hospital, Faisalabad.
Original Article IN DIABETIC PATIENTS Ghulam Abbas Sheikh 1, Dilshad Muhammad 2, Khalid Amin 3 1 Consultant Physician, Aziz Fatimah Hospitals, Faisalabad. 2 Senior Registrar, DHQ Hospital, Faisalabad.
Symposium. Clinical Management of Diabetic Ketoacidosis
 Symposium Asrar Rashid *, Sanjay Perkar **, Praveen Khilnani ***, Sarah Ehtisham **** DOI-10.21304/2017.0404.00212 *Sr Consultant Pediatric intensive care unit, **PICU specialist, ****Senior consultant
Symposium Asrar Rashid *, Sanjay Perkar **, Praveen Khilnani ***, Sarah Ehtisham **** DOI-10.21304/2017.0404.00212 *Sr Consultant Pediatric intensive care unit, **PICU specialist, ****Senior consultant
Salicylate (Aspirin) Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes
 Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes") Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Two of the most common metabolic emergencies
 CLINICAL DIFFERENTIATING BETWEEN AND Authors: Christy McDonald Lenahan, MSN, RN, FNP-BC, and Brenda Holloway, DNSc, MSN, RN, FNP-BC, Lafayette, LA, Mobile, AL Earn Up to 8.5 CE Hours. See page 270. Two
CLINICAL DIFFERENTIATING BETWEEN AND Authors: Christy McDonald Lenahan, MSN, RN, FNP-BC, and Brenda Holloway, DNSc, MSN, RN, FNP-BC, Lafayette, LA, Mobile, AL Earn Up to 8.5 CE Hours. See page 270. Two
Acid-Base Balance Workshop. Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli
 Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Management of Hyperglycemic Crises
 Management of Hyperglycemic Crises Guillermo E. Umpierrez, MD, CDE, FACP, FACE Professor of Medicine Director Clinical Research, Diabetes & Metabolism Center Emory University School of Medicine Chief,
Management of Hyperglycemic Crises Guillermo E. Umpierrez, MD, CDE, FACP, FACE Professor of Medicine Director Clinical Research, Diabetes & Metabolism Center Emory University School of Medicine Chief,