An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction. Disclosures
|
|
|
- Alexandra Chandler
- 5 years ago
- Views:
Transcription
1 An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction R. Scott Wright, MD, FACC, FESC, FAHA, Professor of Medicine Mayo Clinic Fall Managed Care Forum November Disclosures Consulting Roche/Genentech, Sanofi-Regeneron Updated August


2 ACS is driven by platelet thrombosis 2

3 Why are platelets so important in ACS? The final culprit that triggers the syndrome and obstructs coronary blood flow, producing clinical symptoms Platelet activation triggers a cascade that likely promotes vasospasm and further platelet thrombosis a vicious cycle 3

4 Options for platelet blockade The platelets have multiple receptors that activate with exposure to tissue factor or thrombus. Clinicians have multiple pathways to target with pharmacotherapy Multiple drug therapy gets to be expensive especially in the long-term 4

5 What are we certain of in 2013? Use of aspirin is strongly associated with risk reduction and improvement in survival Aspirin remains the single most cost effective therapy in ACS. Adding a second anti-platelet agent is now the standard of care in ACS Rx. 5
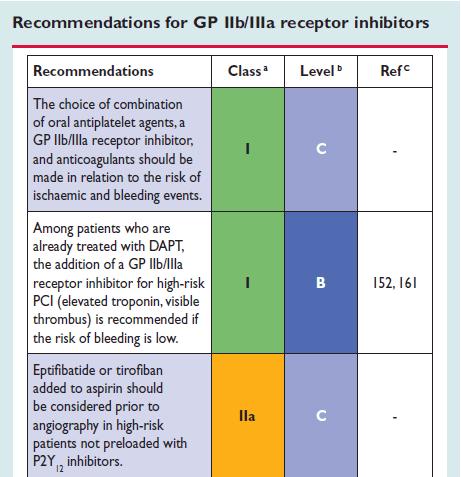
6 Class I and Class IIa Recommendations for Initial Management of UA/NSTEMI Diagnosis of UA/NSTEMI is likely or definite ASA (class I, LOE: A) Clopidogrel if ASA intolerant (class I, LOE: A) Select management strategy Initial conservative strategy or unknown Invasive strategy Initiate anticoagulant therapy (class I, LOE: A) Acceptable options include Enoxaparin or UFH (class I, LOE: A) Fondaparinux (class I, LOE: B)* Enoxaparin or fondaparinux preferred over other GP IIb/IIIa inhibitors (class IIa, LOE: B) Initiate anticoagulant therapy (class I, LOE: A) Acceptable options include Enoxaparin or UFH (class I, LOE: A) Bivalirudin (class I, LOE: B) Initiate clopidogrel (class I, LOE: B) Or Initiate Ticagrelor (Class I, LOE:C) CABG: maintenance ASA (class I, LOE: A) Wright et al: Circ 123, 2011 PCI: add 2nd antiplatelet agent (class I, LOE: A) P2Y12 (class I, LOE: B) or GP IIb/IIIa inhibitor (class I, LOE: A) (IV eptifibatide or tirofiban preferred) Next step per triage decision at angiography PCI: class I: Clopidogrel (if not begun precath) (LOE: A) or Prasurgrel (LOE: B) or Selectively, GP IIb/IIIa inhibitor (if not begun precath) (LOE: A) Rx: D/C GP IIb/IIIa inhibitors if begun and give clopidogrel per conservative strategy 6

7 Challenges facing management of non-st ACS in 2013 and beyond Single therapy with aspirin is no longer the standard of care every patient needs at least two oral anti-platelet agents DAPT Triple anti-platelet therapy should be used in some patients but should it be reserved for the cath lab with PCI and perhaps for certain high risk subsets prior to PCI? Selection of which agents to use for DAPT and TAPT remain a challenge 7


8 P2Y 12 Inhibitor Therapy Clopidogrel is established therapy with proven efficacy and is approved for: Medical management Invasive management Prasugrel is proven and approved for: Invasive management Stent thrombosis Ticagrelor is proven and approved for: Medical Invasive management
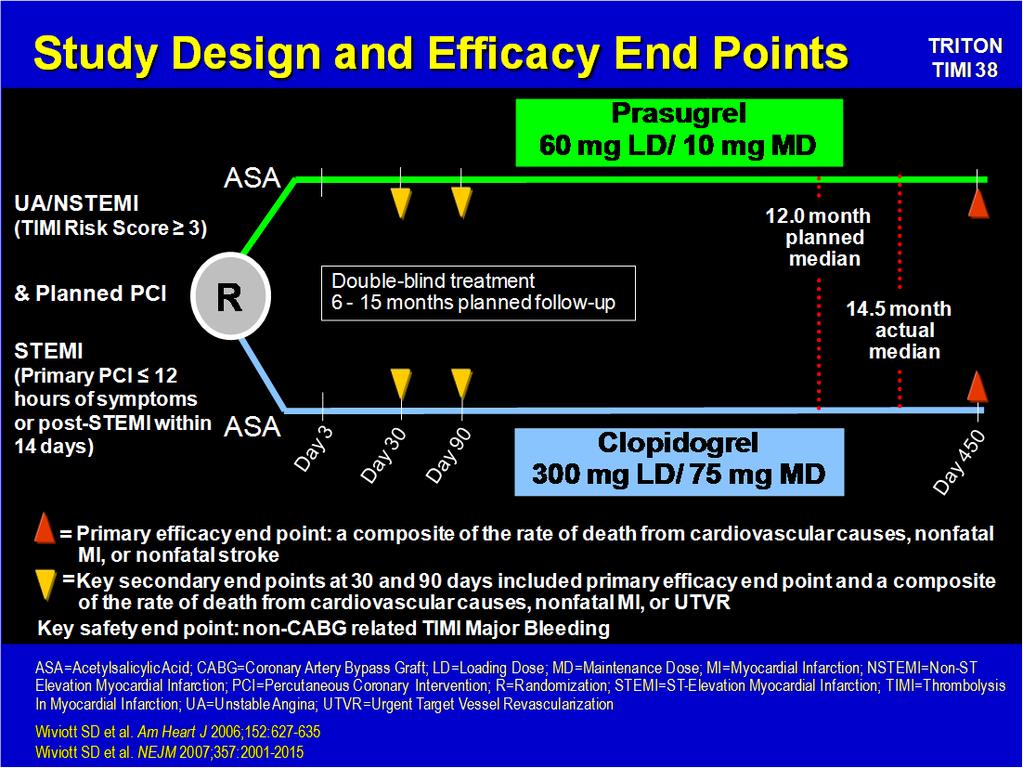
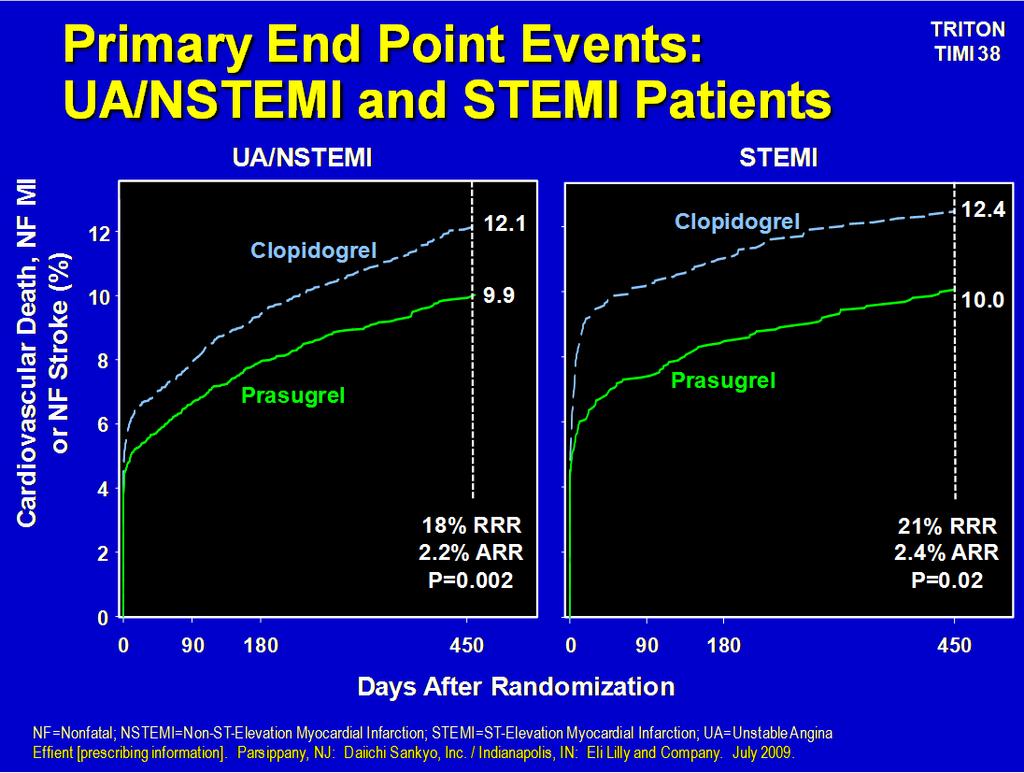
9 Challenges facing management of non-st ACS in 2013 and beyond DAPT with aspirin and clopidogrel is proven therapy in non-stemi for those being managed conservatively or invasively DAPT with aspirin and prasugrel is reserved only for those undergoing PCI DAPT with ticagrelor is effective for patients undergoing PCI but what about those managed conservatively? Clopidogrel vs Prasugrel TRITON TIMI 38 Trial Population tested Non-STEMI undergoing PCI STEMI undergoing PCI Head to head comparison for efficacy and safety in patients undergoing PCI
10 10

11 What about use of Prasugrel in those without PCI? Trilogy Trial Population tested Non-STEMI not undergoing PCI Head to head comparison for efficacy and safety in patients being managed medicaly
12 Study Design 9326 patients in 8 regions, 52 countries (Primary: 7243 patients < 75 years old) Medically Managed UA/NSTEMI Patients Randomization Stratified by: Age, Country, Prior Clopidogrel Treatment (Primary analysis cohort Age < 75 years) Median Time to Enrollment = 4.5 Days Medical Management Decision 72 hrs (No prior clopidogrel given) 4% of total Medical Management Decision 10 days (Clopidogrel started 72 hrs in-hospital OR on chronic clopidogrel) 96% of total Clopidogrel mg LD + 75 mg MD Prasugrel 1 30 mg LD + 5 or 10 mg MD Clopidogrel 1 75 mg MD Prasugrel 1 5 or 10 mg MD Minimum Rx Duration: 6 months; Maximum Rx Duration: 30 months Primary Efficacy Endpoint: CV Death, MI, Stroke 1. All patients were on aspirin, and low-dose aspirin (< 100 mg) was strongly recommended. For patients < 60 kg or 75 years, 5 mg MD of prasugrel was given. Adapted from Chin CT et al. Am Heart J 2010;160:16-22.e1. Roe Mt et al NEJM 2012 Primary Efficacy Endpoint and TIMI Major Bleeding Through 30 Months (Age < 75 years; 7243) Endpoint (%) HR (95% CI): 0.91 (0.79, 1.05) P = 0.21 HR (95% CI): 1.31 (0.81, 2.11) P = 0.27 Roe MT et al NEJM
13 Dual anti-platelet therapy in NSTEMI There are many reasons why NSTEMI patients are not referred for PCI Some NSTEMI patients may have type II infarcts rather than type I Co-morbidities like renal failure may influence a decision for PCI. What about enriching the analyzed cohort for CAD using prerandomization coronary angiography? DAPT benefit without PCI CURE was enriched for subjects not undergoing urgent or early PCI Selection bias clearly impacts who is referred for angiography vs who is not referred for angiography The diagnosis of MI was based upon CK-MB elevation in CURE Small changes in ctnt or I in recent trials thus enriching these trials with Type II infarcts (infarcts likely not due to plaque rupture) 13
 Notes: 1. Non-obstructive = 30 - <50% stenosis 2.")

: 0.77 (0.61, 0.98) 16.3% vs 16.7% P = 0.")
14 Baseline Characteristics: Angiographic Results (>50% Stenosis) Notes: 1. Non-obstructive = 30 - <50% stenosis 2. LM disease - 6.2% of subjects Primary Efficacy Endpoint to 30 Months (Age < 75 years) Angio N=3085 No Angio N= % vs 14.9% P = HR (95% CI): 0.77 (0.61, 0.98) 16.3% vs 16.7% P = HR (95% CI): 1.01 (0.84, 1.20) P interaction =
 9.2% vs 10.6% P = 0.989 HR (95% CI): 1.00 (0.79, 1.")
: 0.30 (0.13,0.71) 2.2% vs 2.0% P = 0.933 HR (95% CI): 1.03 (0.")
15 Myocardial Infarction Angio No Angio 7.2% vs 10.3% P = HR (95% CI): 0.74 (0.55, 1.00) 9.2% vs 10.6% P = HR (95% CI): 1.00 (0.79, 1.26) P interaction = 0.12 Stroke Angio No Angio 0.6% vs 2.4% P = HR (95% CI): 0.30 (0.13,0.71) 2.2% vs 2.0% P = HR (95% CI): 1.03 (0.58,1.83) P interaction =
 P interaction = 0.65 1.6% vs 1.5% P = 0.851 HR (95% CI): 0.92 (0.47, 1.83) P interaction = 0.16 What have we learned with Prasugrel?")
16 TIMI Major Bleeding Angio No Angio 2.7% vs 1.4% P = HR (95% CI): 1.84 (0.93, 3.63) TIMI Major or Minor Bleeding Angio: No Angio: HR (95% CI): HR (95% CI): 1.68 (1.00, 2.83) 1.42 (0.83, 2.41) P interaction = % vs 1.5% P = HR (95% CI): 0.92 (0.47, 1.83) P interaction = 0.16 What have we learned with Prasugrel? It is effective and superior to clopidogrel in patients undergoing PCI The data do not support extending its label to the medically managed ACS patient Prasugrel may have superior efficacy in diabetic patients 16
17 Clopidogrel vs Ticagrelor PLATO Trial Population tested Non-STEMI/STEMI undergoing medical management Non-STEMI/STEMI undergoing PCI Head to head comparison for efficacy and safety 17
18 Primary End-Point MI CV Death 18
19 30 Days Stent Thrombosis 1 Year 19
20 P2Y 12 Inhibitor Therapy Clopidogrel is established therapy with proven efficacy and is approved for: Medical management Invasive management Prasugrel is proven and approved for: Invasive management Stent thrombosis Ticagrelor is proven and approved for: Medical Invasive management Oral Anti-platelet agents Are there issues or unique properties of these agents that allow us to tailor their use? CYP 2C19 issue Bleeding risks? Concurrent aspirin dosing concerns? Onset of anti-platelet action?
21 Oral Anti-platelet agents Are there issues or unique properties of these agents that allow us to tailor their use? CYP 2C19 issue Bleeding risks? Concurrent aspirin dosing concerns? Onset of anti-platelet action? FDA Warning on Clopidogrel March 12, 2010 The FDA issued a boxed warning about the diminished effectiveness of clopidogrel in patients with impaired ability to convert the drug into its active form. Should we consider off label use of Prasugrel to protect patients from this concern? 21

22 Clopidogrel A Pro-drug 15% of absorbed clopidogrel is activated by the Liver via several CYP450 isoenzymes Of these isoenzymes, CYP2C19 is responsible for 45% of the first step of activation. 22
23 CYP2C19 Variants Variants of CYP2C19 are responsible for the variability in clopidogrel active metabolite bioavailability CYP2C19*2 encodes a nonfunctional protein CYP2C19*3, *4, *5, *8 also exist ETHNICITY and CYP2C19*2 Distribution of CYP2C19*2 varies by ethnicity Chinese 50% have it African American 34% Caucasian 25% Hispanic 19% 23
24 Impact of CYP2C19*2 Multiple studies support an association between this allele variant and increased risk of CV events. The increase in risk ranges from 53% to 500% (OR 1.5 to 5.0) Mechanism of Action and Metabolic Pathways for Clopidogrel, Prasugrel and Ticagrelor CYP1A2 CYP2B6 CYP2C19 CYP2B6 CYP2C9 CYP2C19 CYP3A4 Active intestinal absorption P-gp (ABCB1) H 3 C S H COOCH 3 N CI Clopidogrel Esterases Inactive metabolites (85% of clopidogrel dose) O O N O S F Prasugrel O S Esterases O S H COOCH 3 N CI 2-oxo-clopidogrel O N F R CYP3A CYP2B6 CYP2D6 CYP2C9 CYP2C19 H COOCH 3 HOOC HS Pharmacologically active metabolite of clopidogrel HOOC HS O N F R P2Y 12 receptor banding Lancet, 2010 N N N N S HO N OH O OH Ticagrelor F F Inhibition of platelet activation


25 Recommendations for Additional Management of Antiplatelet and Anticoagulant Therapy-Table 4 Wright et al: Circ 123,

26 DAPT - Aspirin and a Glycoprotein IIb/IIIa inhibitor Timing and Role of intravenous anti-platelet therapy CAPTURE, PURSUIT and PRSIM-Plus established the benefit of IV 2b/3a antagonist therapy use when started upstream from the cath as a second anti-platelet agent Should this be updated in light of new evidence? Is there a continued role for 2b/3a agents? ACS 2b or ROUTINE USE SELECTIVE USE UFH or LMWH or Bivalirudin Plus IIb/IIIa Agent not PURSUIT Prism Plus Tactics TIMI 18 Ictus UFH or LMWH or Bivalirudin Decision on Invasive 2b? Strategy Angiography Initiate IIb/IIIa Agent PCI (Capture) 26
27 Advantages ROUTINE USE All are on Rx Benefit observed without invasive Rx (PURSUIT) Single Bolus of Eptifibatide SELECTIVE USE Cost effective ($) Risk of bleeding Use only in higher risk patients Disadvantages ROUTINE USE Bleeding Cost ($$$) Complicate referral to surgery SELECTIVE USE Delayed benefit in higher risk patients (potentially) benefit if routine Rx reduces risk of recurrent ischemia or urgent revasc. 27
28 Routine versus Selective Use of IIb/IIIa agents EARLY ACS Trial 9492 patients w/ ACS undergoing invasive strategy Primary EP (Superiority) 30 day rate of Death, MI, Recurrent ischemia requiring PCI or PCIrelated thrombotic occlusion Secondary EP Death or 30 d ACUITY Trial 9207 patients w/acs (moderate to high risk) undergoing invasive strategy Primary EP (non-inferiority) 30 day rate of Death, MI or unplanned revascularization Secondary EP s: Composite ischemia, major bleeding Routine versus Selective Use of IIb/IIIa agents EARLY ACS Trial 9492 patients w/ ACS undergoing invasive strategy Primary EP (Superiority) 30 day rate of Death, MI, Recurrent ischemia requiring PCI or PCIrelated thrombotic occlusion Secondary EP Death or 30 d ACUITY Trial 9207 patients w/acs (moderate to high risk) undergoing invasive strategy Primary EP (non-inferiority) 30 day rate of Death, MI or unplanned revascularization Secondary EP s: Composite ischemia, major bleeding 28
29 EARLY ACS Trial NEJM 2009;360: EARLY ACS Trial NEJM 2009;360:
 undergoing invasive strategy Primary EP (non-inferiority) 30 day rate of")
30 Routine versus Selective Use of IIb/IIIa agents EARLY ACS Trial 9492 patients w/ ACS undergoing invasive strategy Primary EP (Superiority) 30 day rate of Death, MI, Recurrent ischemia requiring PCI or PCIrelated thrombotic occlusion Secondary EP Death or 30 d ACUITY Trial 9207 patients w/acs (moderate to high risk) undergoing invasive strategy Primary EP (non-inferiority) 30 day rate of Death, MI or unplanned revascularization Secondary EP s: Composite ischemia, major bleeding ACUITY Trial JAMA 2007;297:
31 ACUITY Trial JAMA 2007;297: Routine versus Selective Use of IIb/IIIa agents - Summary No Benefit to Routine Use of these agents prior to PCI in all patients EARLY ACS Trial 9492 patients w/ ACS undergoing invasive strategy Primary EP (Superiority) 30 day rate of Death, MI, Recurrent ischemia requiring PCI or PCIrelated thrombotic occlusion Secondary EP Death or 30 d ACUITY Trial 9207 patients w/acs (moderate to high risk) undergoing invasive strategy Primary EP (non-inferiority) 30 day rate of Death, MI or unplanned revascularization Secondary EP s: Composite ischemia, major bleeding 31




32 Recommendations for Antiplatelet Therapy-Table 2 Wright et al: Circ 123, Recommendations for Antiplatelet Therapy-Table 2 Wright et al: Circ 123,

33

34 ACC 2012 Guidelines July
35 Oral Anti-platelet agents Are there issues or unique properties of these agents that allow us to tailor their use? CYP 2C19 issue Bleeding risks? Concurrent aspirin dosing concerns? Onset of anti-platelet action? P2Y 12 Inhibitor Therapy Clopidogrel Prasugrel Ticagrelor Post PCI Yes Yes Yes Med Rx Yes No Yes Loading 600 mg 60 mg 180 mg Dose Daily 75 mg 10 mg 90 mg Dose % Platelet inhib 50-60% 60-70% 85-90% Aspirin Dose mg mg < 100 mg (Daily) Cost (daily) $0.33 $6.50 $




36 Recommendations for Antiplatelet Therapy-Table 2 Wright et al: Circ 123, Recommendations for Antiplatelet Therapy Wright et al: Circ 123,

37 Oral Anti-platelet agents Are there issues or unique properties of these agents that allow us to tailor their use? CYP 2C19 issue Bleeding risks? Concurrent aspirin dosing concerns? Onset of anti-platelet action?
38 CYP2C19 Variants Variants of CYP2C19 are responsible for the variability in clopidogrel active metabolite bioavailability CYP2C19*2 encodes a non-functional protein CYP2C19*3, *4, *5, *8 also exist ETHNICITY and CYP2C19*2 Distribution of CYP2C19*2 varies by ethnicity Chinese 50% have it African American 34% Caucasian 25% Hispanic 19%

39 Impact of CYP2C19*2 Multiple studies support an association between this allele variant and increased risk of CV events. The increase in risk ranges from 53% to 500% (OR 1.5 to 5.0) Recommendations for Additional Management of Antiplatelet and Anticoagulant Therapy-Table 4 Wright et al: Circ 123,
40 Optimal Dosing of Aspirin and Clopidogrel If both of these drugs are helpful, then higher doses might work even more, right? If you are not confused, then you are not thinking properly Bernard Gersh, ACC
41 Efficacy and Safety Outcomes for the Aspirin Dose Comparison Aspirin dose High (n=8,624) Low (n=8,639) Adjusted HR (95% CI) P CV death, MI, or stroke 356 (4.1%) 366 (4.2%) 0.98 ( ) 0.76 CV death, MI, stroke, or recurrent ischaemia 381 (4.4%) 417 (4.8%) 0.92 ( ) 0.23 CV death 156 (1.8%) 173 (2.0%) 0.90 ( ) 0.35 MI 196 (2.3%) 202 (2.4%) 0.97 ( ) 0.80 Stroke 37 (0.4%) 29 (0.3%) 1.26 ( ) 0.36 Recurrent ischaemia 31 (0.4%) 56 (0.7%) 0.56 ( ) Total mortality 160 (1.9%) 185 (2.1%) 0.86 ( ) 0.18 CURRENT-defined major bleed 128 (1.5%) 110 (1.3%) 1.18 ( ) 0.20 CURRENT-defined severe bleed 92 (1.1%) 76 (0.9%) 1.22 ( ) 0.20 TIMI-defined major bleed 79 (0.9%) 62 (0.7%) 1.29 ( ) 0.13 Fatal bleed 10 (0.1%) 9 (0.1%) 1.12 ( ) 0.80 Intracranial bleed 4 (0.05%) 3 (0.03%) 1.34 ( ) 0.70 Red-cell transfusion 2 units 100 (1.2%) 86 (1.0%) 1.19 ( ) 0.24 CABG-related bleed 8 (0.1%) 8 (0.1%) 0.99 ( ) 0.99 Haemoglobin drop 50 g/l 43 (0.5%) 34 (0.4%) 1.27 ( ) 0.30 Minor bleed 433 (5.0%) 370 (4.3%) 1.18 ( ) Events before PCI MI or stroke 23 (0.3%) 21 (0.2%) 1.09 ( ) 0.78 MI 21 (0.2%) 21 (0.2%) 0.99 ( ) 0.98 Stroke 2 (0.02%) 0 (0.0%) CURRENT-defined major bleed 8 (0.1%) 5 (0.1%) 1.58 ( ) 0.42 CURRENT-defined severe bleed 5 (0.1%) 2 (0.02%) 2.48 ( ) 0.28 TIMI-defined major bleed 4 (0.05%) 2 (0.02%) 1.98 ( ) 0.43 Events after PCI CV death, MI, or stroke 333 (3.9%) 345 (4.0%) 0.97 ( ) 0.68 CV death, MI, stroke, or recurrent ischaemia 342 (4.0%) 374 (4.3%) 0.92 ( ) 0.24 CV death 156 (1.8%) 173 (2.0%) 0.91 ( ) 0.38 MI 175 (2.0%) 181 (2.1%) 0.97 ( ) 0.75 Stroke 35 (0.4%) 29 (0.3%) 1.21 ( ) 0.45 Recurrent ischaemia 15 (0.2%) 34 (0.4%) 0.44 ( ) Total mortality 160 (1.9%) 185 (2.1%) 0.87 ( ) 0.20 CURRENT-defined major bleed 120 (1.4%) 105 (1.2%) 1.14 ( ) 0.32 CURRENT-defined severe bleed 87 (1.0%) 74 (0.9%) 1.18 ( ) 0.30 TIMI-defined major bleed 75 (0.9%) 60 (0.7%) 1.25 ( ) Major Outcomes at 30 Days, According to Dose of Clopidogrel Double dose n=12,520 Standard dose n=12,566 Hazard ratio (95% CI) P No. % No. % Primary outcome: death from cardio ( ) 0.30 vascular causes, myocardial infarction, or stroke Secondary outcomes Death from cardiovascular causes, ( ) 0.25 myocardial infarction, stroke, or recurrent ischemia Death from cardiovascular causes ( ) 0.57 Myocardial infarction ( ) 0.09 Stroke ( ) 0.95 Recurrent ischemia ( ) 0.72 Death from any cause ( ) 0.61 Safety outcome: bleeding Major Study criteria ( ) 0.01 Requiring RBC transfusion 2 U ( ) 0.01 CABG related ( ) 0.53 Severe ( ) 0.04 Leading to decrease in ( ) 0.13 hemoglobin level 5 g/dl Symptomatic intracranial ( ) 0.53 Fatal ( ) 0.85 TIMI criteria ( ) 0.03 Minor ( ) 0.01 NEJM 363:934,

42




43 Recommendations for Antiplatelet Therapy-Table 2 Wright et al: Circ 123, Anti-platelet therapy Practical thoughts Dual anti-platelet therapy for one year in post-acs patients is the gold standard -- Evidence suggests that clopidogrel works well and that the others are slightly better with higher bleeding risks -- Some centers use Ticagrelor for one month, then switch to clopidogrel not FDA Approved or established by trial evidence
44 Anti-platelet therapy Practical thoughts Patient adherence to DAPT for the first year after ACS is critical -- More efforts must be given to promote adherence -- Discontinuation of DAPT triggers some recurrent ACS events Use of aspirin after year-1 is usually adequate and is the Guideline based expectation Anti-platelet therapy Practical thoughts Guidelines are just that Guidelines The science evolves be prepare to alter strategy Decisions often need to be tailored to individual patient needs Remain vigilant for safety concerns
45 Anti-platelet therapy the Future? What are the future directions new therapies will take? Is it reasonable to develop new antiplatelet agents? Current therapies are very effective Can we afford new therapies? Bleeding risks less or more? A Tethering (transient adhesion) B Stable adhesion Platelet GP Ib/V/IX Platelet GP VI GP Ib/V/IX GP Ia/IIa GP Ib/V/IX VWF VWF Fibrinogen Collagen Subendothelium Subendothelium C Activation Thrombin ADP TXA 2 EPI Serotonin Platelet Release of TXA 2 ADP D Aggregation GP IIa/IIIa Fibrinogen VWF Platelet GP IIa/IIIa GP VI GP Ib/V/IX GP Ia/IIa GP VI GP Ib/V/IX GP Ia/IIa Platelet VWF Collagen VWF Collagen Subendothelium Kiefer and Becker: Circ 120:2488, 2009 Subendothelium

46 Investigational Inhibitors of Platelet Adhesion Receptor/ target and agent VWF GP Ib/V/IX GP VI Structure Company Status in development AjvW-2 Murine monoclonal antibody Ajinomoto Preclinical AJW200 Human monoclonal antibody Ajinomoto Preclinical R9.3 Oligonucleotide aptamer Academic Preclinical R9.14 Oligonucleotide aptamer Academic Preclinical ARC1779 Oligonucleotide aptamer Archemix Phase II clinical trial R9 557 Inhibitory peptide Academic Preclinical Monoclonal antibody K.U. Leuven Research and Development Preclinical 6B4 JAQ1 Monoclonal antibody Academic Preclinical OM2 Monoclonal antibody Otsuka Pharmaceutical Preclinical Soluble GPVI inhibitor Small inhibitory antibody decoy Academic Preclinical EXP3179 Angiotensin II type 1 receptor metabolite Merck Preclinical 2-I Recombinant protein inhibitor Academic Preclinical GP Ia/IIa Small molecule Synthetic I domain allosteric inhibitors inhibitor Academic Preclinical Collagen AAPP Recombinant protein inhibitor Otsuka Pharmaceutical Preclinical TGX-221 Isoform specific enzyme inhibitor Academic Preclinical PI3K Kiefer and Becker: Circ 120:2488,
47 Class I and Class IIa Recommendations for Initial Management of UA/NSTEMI Diagnosis of UA/NSTEMI is likely or definite ASA (class I, LOE: A) Clopidogrel if ASA intolerant (class I, LOE: A) Select management strategy Initial conservative strategy or unknown Initiate anticoagulant therapy (class I, LOE: A) Acceptable options include Enoxaparin or UFH (class I, LOE: A) Fondaparinux (class I, LOE: B)* Enoxaparin or fondaparinux preferred over other GP IIb/IIIa inhibitors (class IIa, LOE: B) Initiate clopidogrel (class I, LOE: B) Or Initiate Ticagrelor (Class I, LOE:C) Invasive strategy Initiate anticoagulant therapy (class I, LOE: A) Acceptable options include Enoxaparin or UFH (class I, LOE: A) Bivalirudin (class I, LOE: B) PCI: add 2 nd antiplatelet agent (class I, LOE: A) P2Y12 (class I, LOE: B) or GP IIb/IIIa inhibitor (class I, LOE: A) (IV eptifibatide or tirofiban preferred) Next step per triage decision at angiography Wright et al: Circ 123, 2011 CABG: maintenance ASA (class I, LOE: A) PCI: class I: Clopidogrel (if not begun precath) (LOE: A) or Prasurgrel (LOE: B) or Selectively, GP IIb/IIIa inhibitor (if not begun precath) (LOE: A) Rx: D/C GP IIb/IIIa inhibitors if begun and give clopidogrel per conservative strategy
Disclosures. Research consulting with: Sanofi-Regeneron Pfizer The Medicines Company Astra Zeneca
 Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
INDIVIDUALIZED MEDICINE
 CENTER FOR INDIVIDUALIZED MEDICINE Clopidogrel Pharmacogenetics Can We Impact Clinical Practice? Michael E. Farkouh, MD, MSc Peter Munk Cardiac Centre University of Toronto Naveen Pereira MD Mayo Clinic
CENTER FOR INDIVIDUALIZED MEDICINE Clopidogrel Pharmacogenetics Can We Impact Clinical Practice? Michael E. Farkouh, MD, MSc Peter Munk Cardiac Centre University of Toronto Naveen Pereira MD Mayo Clinic
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Do We Need Platelet Function Assays?
 Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
Session Objectives. Clopidogrel Resistance. Clopidogrel (Plavix )
") Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Clopidogrel Use in ACS and PCI: Clinical Trial Update
 Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor
 Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Anticoagulation Update David J. Moliterno, MD
 David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies.
 INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies. José G. Díez, MD, FACC, FSCAI Associate Professor of Medicine, Baylor College of Medicine Hall Garcia
INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies. José G. Díez, MD, FACC, FSCAI Associate Professor of Medicine, Baylor College of Medicine Hall Garcia
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
P 2 Y 12 Receptor Inhibitors
 P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
Prasugrel: Son of Clopidogrel or Distant Cousin? Disclosures. Objectives
 Prasugrel: Son of Clopidogrel or Distant Cousin? By John J. Bon, Pharm.D., BCPS Lead Clinical Pharmacist, Critical Care Summa Health System Disclosures I have no actual or potential conflict of interest
Prasugrel: Son of Clopidogrel or Distant Cousin? By John J. Bon, Pharm.D., BCPS Lead Clinical Pharmacist, Critical Care Summa Health System Disclosures I have no actual or potential conflict of interest
New antiplatelets in NSTEMI. Overview: dual anti-platelet oral therapy
 Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs
 Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ. Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον?
 ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ ΕΡΕΥΝΗΤΙΚΟ ΚΕΝΤΡΟ ΑΘΗΡΟΘΡΟΜΒΩΣΗΣ Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον? Αλέξανδρος Δ. Τσελέπης, MD, PhD Καθηγητής Βιοχηµείας - Κλινικής Χηµείας Disclosures
ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ ΕΡΕΥΝΗΤΙΚΟ ΚΕΝΤΡΟ ΑΘΗΡΟΘΡΟΜΒΩΣΗΣ Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον? Αλέξανδρος Δ. Τσελέπης, MD, PhD Καθηγητής Βιοχηµείας - Κλινικής Χηµείας Disclosures
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI
 Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary
 Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Dual Oral Antiplatelet Therapy for ACS: Improving Standards of Care to Optimize Outcomes
 Agenda Welcome and Introduction Pathophysiology of ACS Is Aspirin Enough? Overview of Antiplatelet Agents Clopidogrel Prasugrel Ticagrelor New Guideline Recommendations for Dual Antiplatelet Therapy in
Agenda Welcome and Introduction Pathophysiology of ACS Is Aspirin Enough? Overview of Antiplatelet Agents Clopidogrel Prasugrel Ticagrelor New Guideline Recommendations for Dual Antiplatelet Therapy in
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Relationships Relevant to this Presentation
 Relationships Relevant to this Presentation Research grants/contracts to DCRI NHLBI, ACC, AHA, sanofi-aventis, Lilly, Daiichi- Sankyo, GSK, TMC, BMS, Astra, J&J, BI, Portola, Novartis, Merck, Regado Consulting
Relationships Relevant to this Presentation Research grants/contracts to DCRI NHLBI, ACC, AHA, sanofi-aventis, Lilly, Daiichi- Sankyo, GSK, TMC, BMS, Astra, J&J, BI, Portola, Novartis, Merck, Regado Consulting
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants
 Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Is there a real need for new agents to optimize efficacy/safety balance
 Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute
 Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Thrombosis Research active studies
 Thrombosis Research active studies A Pharmacodynamic Study Comparing Prasugrel Versus Ticagrelor in Patients With Coronary Artery Disease Undergoing PCI With CYP2C19 Loss-of-function Genotypes: A Feasibility
Thrombosis Research active studies A Pharmacodynamic Study Comparing Prasugrel Versus Ticagrelor in Patients With Coronary Artery Disease Undergoing PCI With CYP2C19 Loss-of-function Genotypes: A Feasibility
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
Update on Antiplatelet Therapy
 Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Optimal Duration of Dual Anti- Platelet Therapy. December 19, 2015
 Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
COME ORIENTARSI TRA I NUOVI. Maria Rosa Conte H. Mauriziano Torino
 COME ORIENTARSI TRA I NUOVI ANTIPIASTRINIC I Maria Rosa Conte H. Mauriziano Torino Sulle sponde del Ticino- Novara 10 maggio 2013 NEW ORAL ANTIPLATET AGENT PRASUGREL TICAGRELOR (Cangrelor) Death/ MI/
COME ORIENTARSI TRA I NUOVI ANTIPIASTRINIC I Maria Rosa Conte H. Mauriziano Torino Sulle sponde del Ticino- Novara 10 maggio 2013 NEW ORAL ANTIPLATET AGENT PRASUGREL TICAGRELOR (Cangrelor) Death/ MI/
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS. Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands
 DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
DOUBLE or TRIPLE ANTI-TROMBOTIC THERAPY in ACS Maarten L Simoons Thoraxcenter - Erasmus MC Rotterdam - The Netherlands RECENT DEVELOPMENTS Better anti-platelet agents: Prasugrel and Ticagrelor to replace
Scottish Medicines Consortium
 Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Impact of CYP2C19 and ABCB1 SNPs on outcomes with ticagrelor versus clopidogrel in acute coronary syndromes: a PLATO genetic substudy
 Impact of CYP2C19 and ABCB1 SNPs on outcomes with ticagrelor versus clopidogrel in acute coronary syndromes: a PLATO genetic substudy Lars Wallentin, Stefan James, Robert F Storey, Martin Armstrong, Bryan
Impact of CYP2C19 and ABCB1 SNPs on outcomes with ticagrelor versus clopidogrel in acute coronary syndromes: a PLATO genetic substudy Lars Wallentin, Stefan James, Robert F Storey, Martin Armstrong, Bryan
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis Alaide Chieffo
 Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Antiplatelet Therapy. Briain Mac Neill
 Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Optimal medical therapy in patients with stable CAD
 Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Robert Storey. Sheffield, United Kingdom
 Antiplatelet in ACS Moving beyond clopidogrel Robert Storey Professor of Cardiology, Department of Cardiovascular Science, University of Sheffield and Academic Director and Honorary Consultant Cardiologist,
Antiplatelet in ACS Moving beyond clopidogrel Robert Storey Professor of Cardiology, Department of Cardiovascular Science, University of Sheffield and Academic Director and Honorary Consultant Cardiologist,
Selective use of platelet glycoprotein IIb/IIIa inhibition
 20 years clinical use of GP IIb/IIIa receptor antagonists: What have we learned and where to go? EBAC ACCREDITED EDUCATIONAL PROGRAMME HELD DURING THE ESC CONGRESS 2014 Selective use of platelet glycoprotein
20 years clinical use of GP IIb/IIIa receptor antagonists: What have we learned and where to go? EBAC ACCREDITED EDUCATIONAL PROGRAMME HELD DURING THE ESC CONGRESS 2014 Selective use of platelet glycoprotein
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France
 Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
Antithrombotic treatment in ACS: what do the guidelines say? Nicolas Danchin, HEGP, Paris France Disclosures Research grants: Astra-Zeneca, Merck, Novartis, Pfizer, sanofi-aventis, Servier, The MedCo Fees
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation?
 What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
European Heart Journal 2015 doi: /eurheartj/ehv320
 European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type