INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies.
|
|
|
- Moses Robbins
- 5 years ago
- Views:
Transcription



1 INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies. José G. Díez, MD, FACC, FSCAI Associate Professor of Medicine, Baylor College of Medicine Hall Garcia Cardiology at Baylor College of Medicine Senior Research Scientist Texas Heart Institute Houston, TX
2 Acute Coronary Syndromes Progression and Stages Opportunities for Treatment Onset of NSTE-ACS -Initial recognition and management in the ED by first responders or ED personnel -Risk stratification -Immediate management Hospital Management -Medication -Conservative versus invasive strategy -Special groups -Preparation for discharge Management Prior to NSTE-ACS Secondary Prevention/ Long-Term Management
3 Acute Coronary Syndromes (stages - scenarios) Presentation Ischemic Discomfort ACS Working Dx ECG No ST Elevation NSTE-ACS ST Elevation Cardiac Biomarker UA NSTEMI* STEMI* Final Dx Unstable Angina Myocardial Infarction NQMI QwMI Noncardiac Etiologies

4 Spectrum of Pathologic and Clinical ST-Segment Elevation Acute Myocardial Infarction (STEMI) and Non-STEMI Acute Coronary Syndromes. Anderson JL, Morrow DA. N Engl J Med 2017;376:
5 TIMI Risk Score TIMI Risk Score* for NSTE-ACS All-Cause Mortality, New or Recurrent MI, or Severe Recurrent Ischemia Requiring Urgent Revascularization Through 14 d After Randomization, % *The TIMI risk score is determined by the sum of the presence of 7 variables at admission; 1 point is given for each of the following variables: 65 y of age; 3 risk factors for CAD; prior coronary stenosis 50%; ST deviation on ECG; 2 anginal events in prior 24 h; use of aspirin in prior 7 d; and elevated cardiac biomarkers.
6 GRACE Risk Model Nomogram To convert serum creatinine level to micromoles per liter, multiply by 88.4.
7 Algorithm for Management of Patients With Definite or Likely NSTE-ACS NSTE-ACS: Definite or Likely Ischemia-Guided Strategy Early Invasive Strategy Initiate DAPT and Anticoagulant Therapy 1. ASA (Class I; LOE: A) 2. P2Y 12 inhibitor (in addition to ASA) (Class I; LOE: B) : Clopidogrel or Ticagrelor 3. Anticoagulant: UFH (Class I; LOE: B) or Enoxaparin (Class I; LOE: A) or Fondaparinux (Class I; LOE: B) Initiate DAPT and Anticoagulant Therapy 1. ASA (Class I; LOE: A) 2. P2Y 12 inhibitor (in addition to ASA) (Class I; LOE: B): Clopidogrel or Ticagrelor 3. Anticoagulant: UFH (Class I; LOE: B) or Enoxaparin (Class I; LOE: A) or Fondaparinux (Class I; LOE: B) or Bivalirudin (Class I; LOE: B) Can consider GPI in addition to ASA and P2Y 12 inhibitor in high-risk (e.g., troponin positive) pts (Class IIb; LOE: B) Eptifibatide Tirofiban Medical therapy chosen based on cath findings Therapy Effective Therapy Ineffective


8 EARLY INVASIVE STRATEGY
9 Factors Associated With Appropriate Selection of Early Invasive Strategy or Ischemia-Guided Strategy in Patients With NSTE-ACS Immediate invasive (within 2 h) Ischemiaguided strategy Early invasive (within 24 h) Delayed invasive (within h) Refractory angina Signs or symptoms of HF or new or worsening mitral regurgitation Hemodynamic instability Recurrent angina or ischemia at rest or with low-level activities despite intensive medical therapy Sustained VT or VF Low-risk score (e.g., TIMI [0 or 1], GRACE [<109]) Low-risk Tn-negative female patients Patient or clinician preference in the absence of high-risk features None of the above, but GRACE risk score >140 Temporal change in Tn (Section 3.4) New or presumably new ST depression None of the above but diabetes mellitus Renal insufficiency (GFR <60 ml/min/1.73 m²) Reduced LV systolic function (EF <0.40) Early postinfarction angina PCI within 6 mo Prior CABG GRACE risk score ; TIMI score 2


10 Meta-Analysis of Trials Comparing an Early Invasive vs. Conservative Strategy for NSTE-ACS N=8,375 Weighted mean follow-up 23.7 months Bavry AA, et al. JACC 2006;48: P=0.001 P=0.012 P< % 17% 31% INV CONS 5 0 All cause Mort. Nonfatal MI Rehosp UA NNT 62 NNT 66 NNT 11


")


11 Optimal Strategy for UA/NSTEMI FAST-MI ICTUS VANQWISH Conservative N= TIMACS (Low Risk) MATE TIMI IIIB N=3112 ELISA-3 TIMACS (High Risk) ISAR-COOL VINO Invasive N=10489 RITA-3 TRUCS TACTICS- TIMI 18 FRISC II Modified 2010 from Cannon, C. Cardiology Rounds 2003;7 (4) 1-6.


12 EuroIntervention 2013;9:54-61 Early or late intervention in high-risk non-st-elevation acute coronary syndromes: results of the ELISA-3 trial 2013 EuroIntervention. All rights reserved.

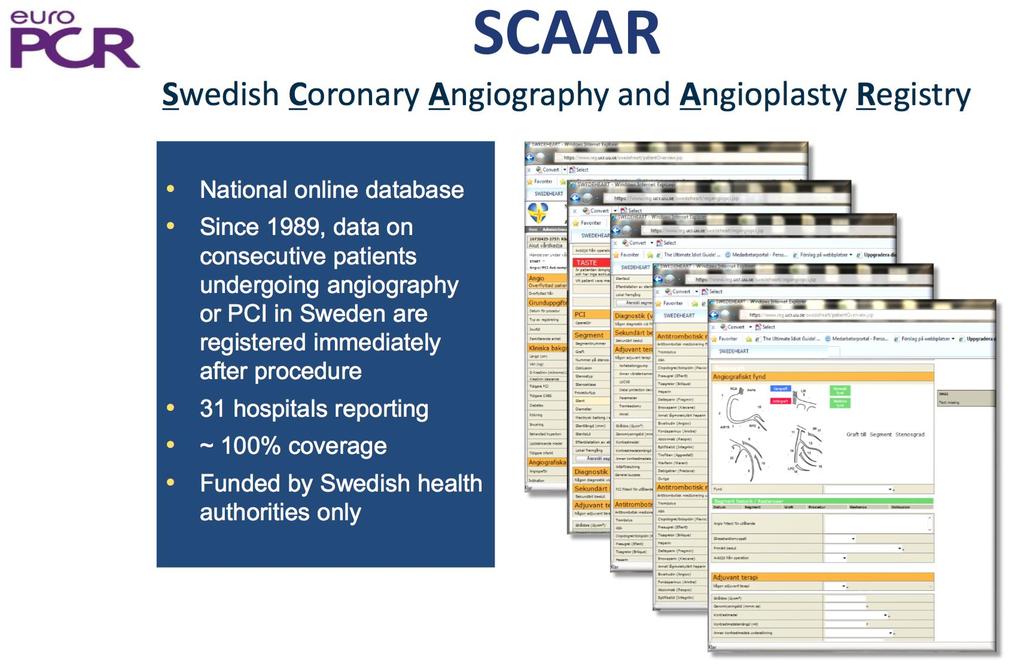
13 EuroIntervention 2015;11-online publish-ahead-of-print November 2015 Invasive strategies and outcomes for non-st-segment elevation acute coronary syndromes: a twelve-year experience from SWEDEHEART 2015 EuroIntervention. All rights reserved.

14

15 Wallentin, L. Eur Heart J :ehp296v1-296; doi: /eurheartj/ehp296
16


17 The Most Plausible Mechanism Of Aspirin In Reducing Risks Of Cardiovascular Disease Aspirin irreversibly acetylates the active site of cyclooxygenase, which is required for the production of thromboxane A2, a powerful promoter of platelet aggregation Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action of aspirin like drugs. Nat New Biol. 1971;231:232-5.

18 Second International Study of Infarct Survival ISIS-2 Collaborative Croup Lancet Aug 13;332:


19 SUMMARY OF TRIALS OF ANTITHROMBOTIC IN UA/NSTEMI Patients with event (%) Risk ratio (95% CI) P-value Trials N Active Placebo ASA vs placebo % Death or MI 5-day to 2-year endpoint Lewis et al (VA) Cairns et al Theroux et al RISC group All ASA vs placebo UFH + ASA vs ASA Theroux et al week endopoint 0.40 RISC group ATACS group Gurfinkel et al All UFH vs ASA LMWH + ASA vs ASA Gurfinkel et al week endopoint NA FRISC group All hep. or LMWH vs ASA GPIIb/IIIa anta + UFH vs UFH CAPTURE day endopoint PARAGON PRISM-PLUS PRISM* PURSUIT All GPIIb/IIIa vs UFH # Braunwald et al ACC/AHA Practice Guidelines
 3A4 enzyme system ADP ADP GPllb/llla (Fibrinogen receptor) Activation Collagen thrombin TXA 2 ASA COX TXA 2 COX (cyclo-oxygenase) ADP (adenosine")
20 The active metabolite exerts its antiplatelet effect by noncompetitive inhibition of the platelet ADP receptor subtype P2Y 12 CLOPIDOGREL C Clopidogrel: An inactive prodrug requires in vivo conversion in the liver by the cytochrome P450 (CYP) 3A4 enzyme system ADP ADP GPllb/llla (Fibrinogen receptor) Activation Collagen thrombin TXA 2 ASA COX TXA 2 COX (cyclo-oxygenase) ADP (adenosine diphosphate) TXA 2 (thromboxane A 2 ) Jarvis B, Simpson K. Drugs 2000; 60:
 Clopidogrel + Aspirin (n=6259) 20% Relative Risk Reduction P <.001 N=12,562 0.02 0.")
21 Cumulative Hazard Rate CURE Study: Primary End Point: MI/Stroke/CV Death Placebo + Aspirin (n=6303) Clopidogrel + Aspirin (n=6259) 20% Relative Risk Reduction P <.001 N=12, Months of Follow-up Yusuf S, et al. N Engl J Med. 2001;345:
22 Cumulative Hazard Rate PCI-CURE Study: CV Death or MI From Randomization Median time to PCI Placebo + Aspirin (n=1345) 12.6% 8.8% 31% Relative Risk Reduction Clopidogrel + Aspirin (n=1313) P= Days of Follow-up Mehta SR, et al. Lancet. 2001;358:






23 CREDO: 1-Year Primary Outcome Death, MI, or stroke (%) RRR=27% P=0.02 Placebo n=1,063 Clopidogrel n=1, % 8.5% Months Steinhubl S et al: JAMA 2002;288:
24
 Sabatine MS, et al.")

25 Percentage with endpoint (%) Clarity TIMI 28: CV Death, MI, RI Urg Revasc (n= 3491) Sabatine MS, et al. N Engl J Med. 2005;352:1179. Placebo 20% Clopidogrel Odds Ratio 0.80 (95% CI ) P= days

26 Schematic of different therapeutic options for inhibition of platelet P2Y12 receptor. José Luis Ferreiro, and Dominick J. Angiolillo Circ Cardiovasc Interv. 2012;5:
27 TRITON TIMI 38 - Main Trial Design ACS (STEMI or UA/NSTEMI) & Planned PCI ASA N= 13,608 Double-blind CLOPIDOGREL 300 mg LD/ 75 mg MD PRASUGREL 60 mg LD/ 10 mg MD Duration of therapy: 6-15 months 1 o endpoint: CV death, MI, Stroke 2 o endpoint: Stent Thrombosis Safety endpoints: TIMI major bleeds, Life-threatening bleeds 27 Wiviott SD, Antman EM et al AHJ 2006
28 Endpoint (%) TRITON TIMI 38 Main Trial: Primary Results CV Death / MI / Stroke Clopidogrel Prasugrel HR 0.81 ( ) P= TIMI Major NonCABG Bleeds Days Prasugrel Clopidogrel HR 1.32 ( ) P= Wiviott SD, Braunwald E, McCabe CH et al NEJM2007
29 CV Death, MI, Stroke (%) TRITON-TIMI Clopidogrel clopidogrel prasugrel P=0.002 Prasugrel P< P= HR 0.81 ( ) Days NNT= TIMI major bleed P=0.01 Life threatening Caveats: Warning - Weight < 60 kg, Age > 75, h/o CVA, need for CABG Wiviott et al. New Engl J Med 2007;357: No data long term therapy, uses other than ACS. TIMI major or minor
30

31
32 PLATO study design NSTE-ACS (moderate-to-high risk) STEMI (if primary PCI) Clopidogrel-treated or -naive; randomised within 24 hours of index event (N=18,624) Clopidogrel (n=9291) If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor (n=9333) 180 mg loading dose, then 90 mg bid maintenance; (additional 90 mg pre-pci) 6 12-month exposure Primary endpoint: CV death + MI + Stroke Primary safety endpoint: Total major bleeding
33 K-M estimated rate (% per year) K-M estimated rate (% per year) PLATO main endpoints 13 Primary efficacy endpoint: D/Mi/CVA 15 Primary safety endpoint: Bleeding Clopidogrel Ticagrelor Ticagrelor Clopidogrel HR 0.84 (95% CI ), p= HR 1.04 (95% CI ), p= No. at risk Ticagrelor Clopidogrel ,333 9,291 Months Months Caveats: Rhythm disorders, dyspnea, 8,628 8,460 8,219 6,743 5,161 4,147 9,235 7,246 6,826 6,545 5,129 8,521 8,362 8,124 6,743 5,096 4,047 9,186 7,305 6,930 6,670 5,209 CrCl, uric acid, not to be used in h/o CVA. 3,783 3,433 3,841 3,479 Wallentin et al., New Eng J Med. 2009;361:

34
35 Efficacy in reducing the rates of definite and probable stent thrombosis of new drugs/approaches tested in large-scale clinical trials. José Luis Ferreiro, and Dominick J. Angiolillo Circ
36
37
38

39

40
41
42
 should be given for at least 1 month ACS after BMS BMS/DES/ACB/MD implantation (unless the patient 12 is months at increased risk for bleeding); then it should be given for a minimum of 2")
43 ACC/AHA/SCAI 2005 guideline update for PCI Update No ACS DES - 12, first generation New generation 6, 3 months Class I In patients who have undergone Update PCI: clopidogrel (75 mg daily) should be given for at least 1 month ACS after BMS BMS/DES/ACB/MD implantation (unless the patient 12 is months at increased risk for bleeding); then it should be given for a minimum of 2 weeks), 3 months after sirolimus stent implantation, and Update 2009 and months after paclitaxel stent implantation, and ideally up to 12 ACS-DES months in patients 12 M, who STEMI are not at > high 15 months risk of bleeding. New DES SHORTER? 2016 LONGER - DAPT trial 30 months Smith S et al. Circulation. 2005;113:
44
45
46 Benefit of switching dual antiplatelet therapy after acute coronary syndrome: the TOPIC (timing of platelet inhibition after acute coronary syndrome) randomized study Cuisset T, Deharo P, Quilici J, et al. EHJ 2017, May 16 Aims to evaluate the benefit of switching dual antiplatelet therapy (DAPT) from aspirin plus a newer P2Y12 blocker to aspirin plus clopidogrel 1 month after ACS. Methods and results open-label, randomized trial. patients admitted with ACS requiring coronary intervention, on aspirin and a newer P2Y12 blocker and without adverse event at 1 month, were assigned to switch to aspirin and clopidogrel (switched DAPT) or continuation of their drug regimen (unchanged DAPT). The primary outcome was a composite of cardiovascular death, urgent revascularization, stroke and bleeding as defined by the Bleeding Academic Research Consortium (BARC) classification 2 at 1 year post ACS. Six hundred and forty five patients: 322 patients in the switched DAPT and 323 in the unchanged DAPT group. The primary endpoint occurred in 43 (13.4%) patients in the switched DAPT group and in 85 (26.3%) patients in the unchanged DAPT (HR 95%CI 0.48 ( ), P < 0.01). No significant differences were reported on ischaemic endpoints, BARC 2 bleeding occurred in 13 (4.0%) patients in the switched DAPT and in 48 (14.9%) in the unchanged DAPT group (HR 95%CI 0.30 ( ), P < 0.01). Conclusion A switched DAPT is superior to an unchanged DAPT strategy to prevent bleeding complications without increase in ischaemic events following ACS.

47 Balancing Ischemic and Bleeding Risk
48 JACC: Cardiovascular Interventions Volume 10, Issue 11, June 2017 Outcomes in Patients Undergoing Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction Via Radial Access Anticoagulated With Bivalirudin Versus Heparin A Report From the National Cardiovascular Data Registry Jovin et al.

49 Six Initial Assessment and Management Decisions Pertaining to Patients Presenting with Chest Pain and a Possible Acute Coronary Syndrome. Anderson JL, Morrow DA. N Engl J Med 2017;376:
50 Oral Chronic Anticoagulation? Choose wisely, choose carefully BMS vs DES Triple combination: 3 6 months INR 2.0 WOEST (Lancet 2013) 50
51 Antiplatelet Strategies in ACS: Conclusions Dual antiplatelet therapy indicated for at least 1 year after ACS and/or PCI CURE, PCI CURE, CREDO Potential benefit beyond 1 year in patients with prior ischemic events CHARISMA High Risk, PEGASUS Potential benefit beyond 1 year in patients with DES registry data, DAPT New Agents: Prasugrel, Ticagrelor, Elinogrel, Vorapaxar

52 Thank you! 52
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
COPYRIGHT. Harvard Medical School
 Agenda New Rapid Rule Out Strategy General Guidelines and Therapies Assessing Patient Risk Timing of Catheterization Navigating Anticoagulant/Antiplatelet Choices Newer Choices and new data The Future
Agenda New Rapid Rule Out Strategy General Guidelines and Therapies Assessing Patient Risk Timing of Catheterization Navigating Anticoagulant/Antiplatelet Choices Newer Choices and new data The Future
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Timing of angiography for high- risk ACS
 Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
P 2 Y 12 Receptor Inhibitors
 P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
New antiplatelets in NSTEMI. Overview: dual anti-platelet oral therapy
 Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants
 Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction. Disclosures
 An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction R. Scott Wright, MD, FACC, FESC, FAHA, Professor of Medicine Mayo Clinic Fall Managed Care Forum November 2013 3098590-1
An Update on Oral Anti-platelet therapy in patients with non-st Myocardial Infarction R. Scott Wright, MD, FACC, FESC, FAHA, Professor of Medicine Mayo Clinic Fall Managed Care Forum November 2013 3098590-1
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in Patients with Non-ST Elevation ACS
 Angioplasty to Blunt the rise Of troponin in Acute coronary syndromes Randomized for an immediate or Delayed intervention A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in
Angioplasty to Blunt the rise Of troponin in Acute coronary syndromes Randomized for an immediate or Delayed intervention A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary
 Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Disclosures. Research consulting with: Sanofi-Regeneron Pfizer The Medicines Company Astra Zeneca
 Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Acute Coronary Syndromes: Review and Update
 Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Update on Antiplatelet Therapy
 Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
Update on Antiplatelet Therapy Christine Ibarra Pharm.D. PGY-1 Baptist Hospital of Miami Objectives Explain the role of antiplatelettherapy in prevention of cardiovascular events Appreciate differences
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
NSTEACS Case Presentation
 NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας. A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο
 Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs
 Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
UPDATE ACUTE CORONARY SYNDROMES. Dr. Wayne Tymchak April 7, 2017
 UPDATE ACUTE CORONARY SYNDROMES Dr. Wayne Tymchak April 7, 2017 Spontaneous Rupture Unstable Angina Myocardial Infarction Classification: Acute Coronary Syndromes Ischemic Discomfort Non-ST ST Unstable
UPDATE ACUTE CORONARY SYNDROMES Dr. Wayne Tymchak April 7, 2017 Spontaneous Rupture Unstable Angina Myocardial Infarction Classification: Acute Coronary Syndromes Ischemic Discomfort Non-ST ST Unstable
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Antiplatelet Therapy. Briain Mac Neill
 Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Antiplatelet Therapy Briain Mac Neill Galway University Hospital & National University of Ireland Galway Milestones in ACS Management Anti-Thrombin Rx Heparin LMWH Bivalirudin Anti-Platelet Rx Aspirin
Προβληματισμοι στην χρηση αντιαιμοπεταλιακων στα οξέα ισχαιμικά σύνδρομα
 Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta
 Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
11/3/11. James M. Kirshenbaum, MD, FACC
 James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
Optimal medical therapy in patients with stable CAD
 Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Optimal medical therapy in patients with stable CAD Robert Storey Professor of Cardiology, University of Sheffield and Academic Director and Honorary Consultant Cardiologist, Cardiology and Cardiothoracic
Angioplastica coronarica nel paziente anziano ad alto rischio emorragico
 Attualità in Cardiologia Aprilia, Enea Hotel 22 ottobre 2011 Angioplastica coronarica nel paziente anziano ad alto rischio emorragico Fabrizio Tomai, MD, FACC, FESC Dept. of Cardiovascular Sciences - Interventional
Attualità in Cardiologia Aprilia, Enea Hotel 22 ottobre 2011 Angioplastica coronarica nel paziente anziano ad alto rischio emorragico Fabrizio Tomai, MD, FACC, FESC Dept. of Cardiovascular Sciences - Interventional
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Acute Coronary Syndromes: Selective vs Early Invasive Strategies
 Acute Coronary Syndromes: Selective vs Early Invasive Strategies WilliamE.Boden,MD,FACCandVipulGupta,MBBS,MPH Division of Cardiovascular Medicine, University at Buffalo Schools of Medicine and Public Health,
Acute Coronary Syndromes: Selective vs Early Invasive Strategies WilliamE.Boden,MD,FACCandVipulGupta,MBBS,MPH Division of Cardiovascular Medicine, University at Buffalo Schools of Medicine and Public Health,
Antiplatelet in diabetics: strong but incomplete umbrella
 Antiplatelet in diabetics: strong but incomplete umbrella Seung-Whan Lee, MD. Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Global Projections for the Number
Antiplatelet in diabetics: strong but incomplete umbrella Seung-Whan Lee, MD. Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Global Projections for the Number
USING EVIDENCE AND GUIDELINES - TREAT YOUR PATIENTS Non-ST-segment elevation acute coronary syndrome
 USING EVIDENCE AND GUIDELINES - TREAT YOUR PATIENTS Non-ST-segment elevation acute coronary syndrome Zaza Iakobishvili, MD, PhD Department of Cardiology Rabin Medical Center Petah Tikva RISK STRATIFICATION
USING EVIDENCE AND GUIDELINES - TREAT YOUR PATIENTS Non-ST-segment elevation acute coronary syndrome Zaza Iakobishvili, MD, PhD Department of Cardiology Rabin Medical Center Petah Tikva RISK STRATIFICATION