Early Management of Acute Coronary Syndrome
|
|
|
- Shauna Patrick
- 5 years ago
- Views:
Transcription
1 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial oxygen supply and demand à myocardial ischemia/infarction Unstable angina Non- ST- segment elevation myocardial infarction (NSTEMI) ST- segment elevation myocardial infarction (STEMI) >780,000 patients with ACS annually in U.S. ~25-40% STEMI In U.S., median age at presentation 68 yo Male- to- female ratio 3:2 STEMI Ischemic symptoms c/w ACS Persistent ST elevations on ECG Subsequent + cardiac biomarkers ACS definitions NSTE- ACS Ischemic symptoms c/w ACS Absence of persistent ST elevations on ECG With or w/o ischemic ECG changes (ST depression, transient ST elevations, T wave inversions) Unstable angina* Negative biomarkers of myocardial necrosis NSTEMI* Positive biomarkers of myocardial necrosis *UA/NSTEMI indistinguishable early on b/c troponin may not be positive for hours




2 Third universal definition of myocardial infarction Cardiac biomarkers JACC Vol. 50, No. 7, 2007 Pathogenesis of ACS Coronary artery disease (CAD) with plaque rupture/erosion most common Other non- atherosclerotic etiologies include spontaneous coronary artery dissection, embolism, arteritis Excessive myocardial oxygen demand with stable flow- limiting coronary lesion Non- coronary supply- demand mismatch (hypotension, anemia, hypertension, tachycardia, aortic stenosis, pulmonary embolism, heart failure)








3 Nature Reviews Cardiology 2016;13: Stable CAD Acute coronary syndrome Stable angina Unstable angina NSTEMI STEMI Non- occlusive thrombus Occlusive thrombus Photos from Davies MJ. Heart 2000;83: NSTEMI STEMI Murray S. Br J Cardiol 2010;17:129-32

 GI (GERD, esophageal spasm, PUD, pancreatitis) Musculoskeletal (costochrondritis, cervical radiculopathy) Psychiatric (anxiety, somatoform disorders) Other (sickle cell crisis, herpes")
4 Clinical presentation Chest discomfort (tightness, pressure, heaviness) at rest or for a prolonged period (>10min) Unstable angina: rest pain, new angina, or worsening of preexisting angina Radiation to back, neck, jaw, arms Associated with shortness of breath, diaphoresis, dizziness, syncope, nausea, vomiting, weakness Women, elderly, patients with diabetes less likely to experience chest pain Differential diagnosis Non- ischemic cardiovascular chest pain Aortic dissection Expanding aortic aneurysm Pericarditis Pulmonary embolism Non- cardiovascular pain Pulmonary (pneumonia, pneumothorax, pleuritis) GI (GERD, esophageal spasm, PUD, pancreatitis) Musculoskeletal (costochrondritis, cervical radiculopathy) Psychiatric (anxiety, somatoform disorders) Other (sickle cell crisis, herpes zoster) Applying Classification of Recommendation and Level of Evidence


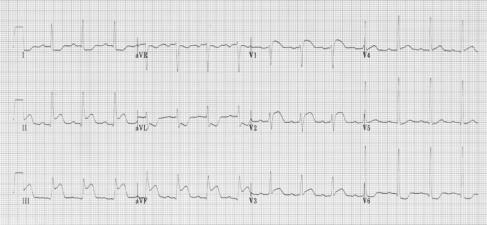
5 Initial evaluation 1) What is the likelihood this is ACS? 2) What is the likelihood of adverse clinical outcomes? Early hospital care Is this a STEMI? BMJ 2002;324:831
 Isolated posterior MI less")



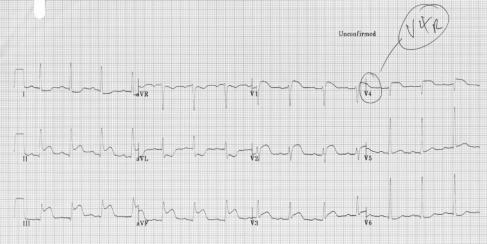
6 Posterior lead ECG Posterior infarct occurs in 15-20% of STEMIs (typically inferior or lateral infarction) Isolated posterior MI less common (3-11%), often missed b/c electrographically silent High suspicion for ACS but non- diagnostic standard ECG Can help differentiate anterior wall ischemia from posterior STEMI Right ventricular infarct complicates up to 40% of inferior STEMIs STE in V4R most sensitive for RV infarction Patients are preload sensitive AVOID nitroglycerin and other preload- reducing agents Treat with aggressive fluid resuscitation Right- sided ECG

7 Call interventional cardiology for STEMI! Reperfusion therapy for STEMI


8 Fibrinolysis Keeley et al. Lancet 2003; 361: So it s not a STEMI


9 Rationale for early risk stratification in NSTE- ACS Useful for selection of site of care (cardiac ICU, step- down unit, observation unit) Helpful to determine medical therapy and need for early invasive strategy Provides prognostic information

10 When to forego formal early risk stratification in NSTE- ACS Patients with any of the following should proceed to urgent coronary angiography: Cardiogenic shock Heart failure Recurrent/persistent angina despite intensive medical therapy Unstable ventricular arrhythmias Ischemia- guided vs. early invasive strategy for NSTE- ACS Ischemia- guided Avoid routine early invasive procedure Plan for noninvasive evaluation to detect severe ischemia at low level of stress Some pts stabilize, may not need angiography Avoids procedural risk/cost Invasive evaluation if Medical therapy failed Ischemia on stress test High clinical risk Early invasive Coronary angiography up front Rapidly risk stratify based on knowledge of coronary anatomy Earlier revascularization Earlier hospital discharge Optimal timing inconclusive W/in 24 hrs vs within hrs, latter may allow antithrombotic therapy to stabilize plaque


11 TACTICS- TIMI 18: Invasive vs conservative strategies in NSTE- ACS 2220 pts with UA/NSTEMI Cannon CP et al. NEJM 2001;344: Routine vs selective invasive strategy in NSTE- ACS: 5 year outcomes

12 Antithrombotic therapy in ACS Antiplatelet therapy Gurbel and Tantry. JACC Heart Fail. 2014;2(1):1-14 Aspirin
 NEJM 2001;345:494-502 Clopidogrel + ASA and fibrinolysis for STEMI 3491 pts w/ STEMI undergoing lysis CV death, MI, urgent revascularization (%) ClOpidogrel and Metoprolol in Myocardial")
13 12,562 pts w/ NSTE- ACS CV death/mi/stroke Relative risk 0.80 (95% CI , p<0.001) NEJM 2001;345: Clopidogrel + ASA and fibrinolysis for STEMI 3491 pts w/ STEMI undergoing lysis CV death, MI, urgent revascularization (%) ClOpidogrel and Metoprolol in Myocardial Infarction Trial (COMMIT) 45,852 pts randomized w/in 24h of acute MI 93% STEMI or new LBBB 2x2 factorial design: Up to 15 mg IV à 200 mg po metoprolol daily vs. placebo Clopidogrel + ASA vs. ASA alone Lancet 2005; 366:

14 TRITON- TIMI 38: Prasugrel vs clopidogrel in patients with ACS pts (~10,000 w/ NSTE- ACS, ~3500 w/ STEMI) scheduled to have PCI CV death/mi/stroke Major bleeding Wiviott SD et al. N Engl J Med 2007;;357: TRILOGY ACS: Prasugrel vs clopidogrel for ACS w/o revascularization 7243 pts <75 yo w/ NSTE- ACS medically managed Roe et al. NEJM 2012;367: PLATO: Ticagrelor vs clopidogrel in patients w/ ACS pts, ~11,000 w/ NSTE-ACS, ~7000 w/ STEMI CV death/mi/stroke (%) HR 0.84 (95% CI , p<0.001) HR 0.84 (95% CI , p<0.001) Wallentin L et al. N Engl J Med 2009;;361:
 have")


15 Early trials NSTEMI Glycoprotein IIbIIIa inhibitors STEMI More recent trials in NSTE- ACS patients treated w/ invasive strategy (EARLY ACS, ACUITY TIMING) have shown increased bleeding without ischemic benefit for routine upstream GPIIbIIIa use vs. delayed provisional use after angiography Am J Med 2000;109: N Engl J Med 2009;360: JAMA 2007;297(6): NSTE- ACS Guideline recommendations: antiplatelet therapy Guideline recommendations: antiplatelet therapy STEMI (undergoing primary PCI)
:1-14 Unfractionated Heparin Advantages Multiple sites of action in coagulation cascade (IIa,Xa) Long history of successful clinical use Readily monitored by aptt and ACT Very inexpensive")
16 Anticoagulant therapy Gurbel and Tantry. JACC Heart Fail. 2014;2(1):1-14 Unfractionated Heparin Advantages Multiple sites of action in coagulation cascade (IIa,Xa) Long history of successful clinical use Readily monitored by aptt and ACT Very inexpensive Disadvantages Indirect thrombin inhibitor Requires AT for activation Does not inhibit clot- bound thrombin Nonspecific binding to: Plasma proteins Endothelial cells (variable anticoagulation level) Inhibited by platelet factor 4 reduced effect in ACS Causes platelet aggregation Risk of HIT Hirsh J, et al: Circulation 2001;;103: % of composition


17 Benefit of heparins vs placebo in NSTE- ACS Enoxaparin vs. UFH for NSTE- ACS Meta- analysis of ESSENCE and TIMI 11B trials Death/MI/urgent revascularization at day 43 Mainly conservative management, no P2Y12 inhibitor TIMI 11B ESSENCE OVERALL N UFH (%) Enox (%) % 18% 16% 14% 12% 10% 8% 6% 4% 2% 0% B B Day OR % p ( ) UFH ENOX Enox Better Odds Ratio UFH Better Antman EM et al. Circulation 1999;100: SYNERGY: enoxaparin vs. UFH 10,027 patients w/ NSTE- ACS planned for early invasive management % p= Enox (4992) UFH (4982) p= d Death / MI TIMI Major Bleed The Synergy Investigators: JAMA 2004;292:45-54
18 Summary: heparins Enoxaparin and UFH equally efficacious in NSTE- ACS Patients managed w/ conservative strategy may have fewer MACE with enoxaparin (ESSENCE, TIMI 11B) For patients undergoing early invasive strategy, UFH may be preferable due to increased bleeding with enoxaparin (SYNERGY) Do not switch between enoxaparin and UFH (SYNERGY) Direct Thrombin Inhibitors Inhibits soluble and fibrinbound thrombin Inhibits thrombin-induced platelet aggregation No platelet activation No HIT Advantages Disadvantages Short t 1/2 (20 min) Needs continuous infusion No antidote Cost Predictable anticoagulant response ACUITY: Bivalirudin for NSTE- ACS Moderate- to high- risk patients with UA or NSTEMI undergoing an invasive strategy (N = 13,819) Moderate- to high- risk ACS Aspirin in all;; Clopidogrel dosing and timing per local practice R UFH or enox + GP IIb/IIIa n=4,603 Bivalirudin + GP IIb/IIIa n=4,604 Bivalirudin alone n=4,612 Angiography within 72 h Medical management PCI CABG Stone GW, et al: Am Heart J 2004;; 148:
 7.7% 7.3% 1.07 (0.92-1.23) 5.3% 5.7% 0.93 (0.78-1.10) <.001.")
19 ACUITY: Primary End Point Measures Primary EP UFH/Enox + GPI vs Bivalirudin + GPI Risk ratio ±95% CI Bival + GPI UFH/Enox + GPI RR (95% CI) p value (noninferior) (superior) Net clinical outcome Ischemic composite Major bleeding Upper boundary non-inferiority 11.8% 11.7% 1.01 ( ) 7.7% 7.3% 1.07 ( ) 5.3% 5.7% 0.93 ( ) < < Bivalirudin + GPI better UFH/Enox + GPI better N Engl J Med 2006;; 355: ACUITY: Primary End Point Measures Primary EP UFH/Enox + GPI vs Bivalirudin alone Risk ratio ±95% CI Bival alone UFH/Enox + GPI RR (95% CI) p value (noninferior) (superior) Net clinical outcome Ischemic composite Major bleeding Upper boundary non-inferiority 10.1% 11.7% 0.86 ( ) 7.8% 7.3% 1.08 ( ) 3.0% 5.7% 0.53 ( ) < <.001 < Bivalirudin better UFH/Enox + GPI better N Engl J Med 2006;; 355: HORIZONS- AMI: Bivalirudin in primary PCI for AMI 20 % Heparin + GPI (N=1802) RR = 0.76 P sup = RR = 0.60 P sup endpoint 1 endpoint Bivalirudin (N=1800) RR = 0.99 P sup = Net adverse clinical events Major bleeding* MACE** * Non- CABG ** MACE = Death, re- MI, TVR or stroke Stone GW et al: NEJM 2008;; 358:
20 Summary: bivalirudin Bivalirudin has similarly efficacy but less bleeding as UFH/enoxaparin with or without GPIIbIIIa inhibition in NSTE- ACS pts w/ mod- high risk treated w/ an invasive strategy Bivalirudin has similar efficacy but less bleeding in pts w/ STEMI undergoing primary PCI Not studied in pts managed w/ conservative strategy, so not for use in this population Fondaparinux Advantages Synthetic heparin pentasaccharide that exclusively neutralizes factor X SC administration once daily Fixed dose Predictable response No antigenicity Disadvantages Difficult to monitor (no aptt or ACT) Long half- life Catheter thrombosis during PCI Simoons ML: J Am Coll Cardiol 2004;;43: Yusuf S: N Engl J Med 2066;; 354: OASIS- 5: comparison of fondaparinux and enoxaparin in ACS Death, MI, or Refractory Ischemia Major Bleeding % 6 HR: 1.01 (95% CI, ) % HR: 0.52 (95% CI, ) 4 5 p< Fondaparinux 3 3 Enoxaparin 2 2 Enoxaparin 1 1 Fondaparinux Days Days 30 Day and 6 Month Results Event Fondaparinux Enoxaparin p value Mortality (30 day) 2.9% 3.5% 0.02 Mortality (6 mo) 5.8% 6.5% % thrombus on catheter (in fondaparixux group) if no UFH given Yusuf S: et al: N Engl J Med 2006:354:


21 Summary: fondaparinux Fondaparinux is a reasonable option for patients w/ NSTE- ACS managed with a conservative strategy Fondaparinux might be better if increased bleeding risk If pt on fondaparinux undergoes PCI, need to switch to another anticoagulant to avoid catheter thrombosis NSTE- ACS Guideline recommendations: anticoagulants STEMI Guideline recommendations: anticoagulants


22 84 pts treated for 1 year w/ beta- blockers after MI to prevent one death ClOpidogrel and Metoprolol in Myocardial Infarction Trial (COMMIT) 45,852 pts randomized w/ 24h of acute MI 93% STEMI or LBBB 2x2 factorial design: Up to 15 mg IV à 200 mg po metoprolol daily vs. placebo Clopidogrel + ASA vs. ASA alone Fewer reinfarctions and fewer VF BUT more cardiogenic shock, especially with initial hemodynamic instability (first 24 h) Moderate late benefit after relative stability Lancet 2005; 366: Guideline recommendations: beta- blockers NSTEMI Initiate oral beta- blockers w/in first 24 hrs in the absence of HF, low output state, risk for cardiogenic shock, or other contraindications (Class I, LOE A) Use metoprolol succinate, carvedilol, or bisoprolol in pts w/ stabilized HF and reduced EF (Class I, LOE C) Reasonable to continue beta- blockers w/ normal LV function in NSTE- ACS (Class IIa, LOE C) STEMI Beta blockers should be continued during/after hospitalization in all STEMI pts w/o contraindications (Class 1, LOE B) Pts w/ initial contraindications during first 24h after STEMI should be reevaluated for subsequent eligibility (Class I, LOE C)
23 MIRACL: effects of atorvastatin on recurrent ischemic events in NSTE- ACS 15 Placebo (n = 1548) LDL-C 135 mg/dl (3.5 mmol/l) 17.4% 14.8% 16% RRR Cumulative Incidence*, % 10 5 Atorvastatin 80 mg (n = 1538) LDL-C 72 mg/dl (1.9 mmol/l) RR = 0.84 (95% CI , p=0.048) Time Since Randomization, weeks *Death (any cause), nonfatal MI, resuscitated cardiac arrest, worsening angina with new objective evidence and urgent rehospitalization. Schwartz GG et al. JAMA. 2001;;285: PROVE IT: Intensive vs. moderate lipid lowering w/ statins after ACS 4162 patients w/ ACS (one- third w/ STEMI) Death, MI, UA rehosp, revasc, or stroke % Pravastatin 40 mg (n = 1548) 95 mg/dl (2.5 mmol/l) Atorvastatin 80 mg (n = 2099) 62 mg/dl (1.6 mmol/l) 26.3% 16% RRR 22.4% 35% LDL reduction (P =.005) Months of Follow-up Cannon CP et al. N Engl J Med. 2004;;350: % proportional reduction in 30d mortality à 4.8 deaths/1000 pts avoided Circulation 1998;97:
 ACEI should be used in all NSTE- ACS patients with LVEF <40 or in")
24 Effect of ACE Inhibitors on Mortality in Patients with CHF Garg R and Yusuf S. JAMA 1995;273: Guideline recommendations: statins and ACEI Initiate or continue high- intensity statin if no contraindications (Class I, LOE A) ACEI should be used in all NSTE- ACS patients with LVEF <40 or in those with HTN, DM, or stable CKD unless contraindicated (Class I, LOE A) ACEI w/in 24 hours for STEMI pts w/ anterior infarct, HF, or EF <40 unless contraindicated (Class I, LOE A) ACEI reasonable for all pts w/ STEMI and no contraindications (Class IIa, LOE A) ARBs are recommended if pt cannot tolerate ACEI (Class I, LOE A) Conclusions ACS is a spectrum of clinical conditions most commonly due to atherosclerosis and plaque rupture Early recognition and risk stratification key for selection of appropriate treatment Cornerstones of early management include antiplatelet therapy, anticoagulation, and revascularization Beta- blockers, statins, and ACEI/ARB also important components of early ACS treatment
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
AIMS: CHEST PAIN. Causes of chest pain. Causes of chest pain: Cardiac causes: Acute coronary syndromes pericarditis thoracic aortic dissection
 CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
CHEST PAIN Dr Susan Hertzberg Emergency Department Prince of Wales Hospital AIMS: To identify causes of chest pain in patients presenting to the ED. To identify and risk stratify patients presenting with
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
COPYRIGHT. Harvard Medical School
 Agenda New Rapid Rule Out Strategy General Guidelines and Therapies Assessing Patient Risk Timing of Catheterization Navigating Anticoagulant/Antiplatelet Choices Newer Choices and new data The Future
Agenda New Rapid Rule Out Strategy General Guidelines and Therapies Assessing Patient Risk Timing of Catheterization Navigating Anticoagulant/Antiplatelet Choices Newer Choices and new data The Future
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION?
 SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Is there a real need for new agents to optimize efficacy/safety balance
 Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI
 Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
NSTEACS Case Presentation
 NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Heart disease is the leading cause of death
 ACS AND ANTIPLATELET MANAGEMENT: UPDATED GUIDELINES AND CURRENT TRIALS Christopher P. Cannon, MD,* ABSTRACT Acute coronary syndrome (ACS) is an important cause of morbidity and mortality in the US population
ACS AND ANTIPLATELET MANAGEMENT: UPDATED GUIDELINES AND CURRENT TRIALS Christopher P. Cannon, MD,* ABSTRACT Acute coronary syndrome (ACS) is an important cause of morbidity and mortality in the US population
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department
: Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department") ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
From STEMIs to Stents: Updates in PCI practice
 From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Is Cangrelor hype or hope in STEMI primary PCI?
 Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY
 2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary
 Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Clopidogrel and ASA after CABG for NSTEMI
 Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Optimal antithrombotic therapy:
 Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Management of Acute Coronary Syndromes
 Management of Acute Coronary Syndromes Objectives 1. To outline the approach in managing a patient who presents with an acute coronary syndrome focusing on anti- thrombotic agents. Jenny Chiu, BScPhm,
Management of Acute Coronary Syndromes Objectives 1. To outline the approach in managing a patient who presents with an acute coronary syndrome focusing on anti- thrombotic agents. Jenny Chiu, BScPhm,
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
Anticoagulation therapy in acute coronary syndromes according to current guidelines
 Acute management of ACS Anticoagulation therapy in acute coronary syndromes according to current guidelines Marcin Grabowski, Marcin Leszczyk, Andrzej Cacko, Krzysztof J. Filipiak, Grzegorz Opolski 1 st
Acute management of ACS Anticoagulation therapy in acute coronary syndromes according to current guidelines Marcin Grabowski, Marcin Leszczyk, Andrzej Cacko, Krzysztof J. Filipiak, Grzegorz Opolski 1 st
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN
 What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics
 Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology