Mitochondrial Disease & its Anesthetic Considerations. Stephen Okoth BSN, SRNA (Sr.) York College of PA/Wellspan Health NAP
|
|
|
- Dana Craig
- 6 years ago
- Views:
Transcription

1 Mitochondrial Disease & its Anesthetic Considerations tephen Okoth BN, RNA (r.) York College of PA/Wellspan Health NAP
2 Objectives Discuss the structure of the Mitochondrion Discuss the main function of the Mitochondrion Detecting and Diagnosing mitochondrial diseases Treatment of mitochondrial diseases Anesthetic considerations for patients with mitochondrial diseases Case Review

3 Endosymbiotic theory

4 Mitochondrion
5 Mitochondrial vs. Nucleic DNA The mitochondrial genome is circular, whereas the nuclear genome is linear The mitochondrial genome is built of 16,569 DNA base pairs, whereas the nuclear genome is made of 3.3 billion DNA base pairs. The mitochondrial genome contains 37 genes that encode 13 proteins, 22 trnas, and 2 rrnas. The small mitochondrial genome are unable to produce all of the proteins needed for functionality; thus, mitochondria rely heavily on imported nuclear gene products.


6 Mitochondrial import pathways for precursor proteins. tephan Kutik et al. J Cell Biol 2007;179: The Rockefeller University Press
7 Mitochondrial Gene Inheritance

8 Fission vs. Fussion
9 Function Energy production in the form of ATP Thermogenesis torage and Regulation of Calcium Ions Apoptosis Cholesterol and Neurotransmitter Metabolism Detoxification of Ammonia

10 Cellular Respiration

11 ATP Production Ref:

12 Oxidative phosphorylation Ref:
13 Mitochondrial diseases clinical and biochemical disorders resulting from dysfunction of the mitochondria. First clinically described in 1960 This results in a lack of cellular energy to perform various functions and in the accumulation of byproducts that impair or destroy the cell itself They can be caused by mutation of genes encoded by either nuclear DNA or mitochondrial DNA (mtdna) Mitochondrial disorders may present at any age. There is an estimated incidence of 1 in 4000 live births suffering from mitochondrial disease in the United tates. These diseases have varying etiologies and are often very difficult to classify

14 Clinical Manifestation
15 igns and ymptoms loss of motor control diabetes muscle weakness and pain respiratory complications gastro-intestinal disorders and swallowing difficulties poor growth cardiac disease liver disease seizures visual/hearing problems lactic acidosis developmental delays susceptibility to infection.
16 Classifying the diseases cientists have discovered over 40 different mitochondrial diseases. Early on diseases would be classed by clinical syndrome e.g CPEO: chronic progressive external ophthalmoplegia MELA: mitochondrial encephalopathy with lactid acidosis and stroke like episodes MERRF: myoclonic epilepsy with ragged red fibers LHON: Leber hereditary optic neuropathy
17 Classifying the diseases Genocopies Phenocopies diseases that are caused by the same mutation but which may not look the same clinically different mutations in mtdna and ndna can lead to the same diseases. primary mitochondrial disease: a mutation in the mitochondria causes the organelle to malfunction and produce symptoms. secondary mitochondrial disease: genetic alteration is present, but does not produce any symptoms of disease until an external environmental force triggers mitochondrial dysfunction.
18 Causes of Mitochondrial diseases The major cause of the disease is gene inheritance. Either nucleic or mitochondrial genes The other cause is mitochondrial toxins. Various agents including commonly used drugs have been found to be toxic to the mitochondria.
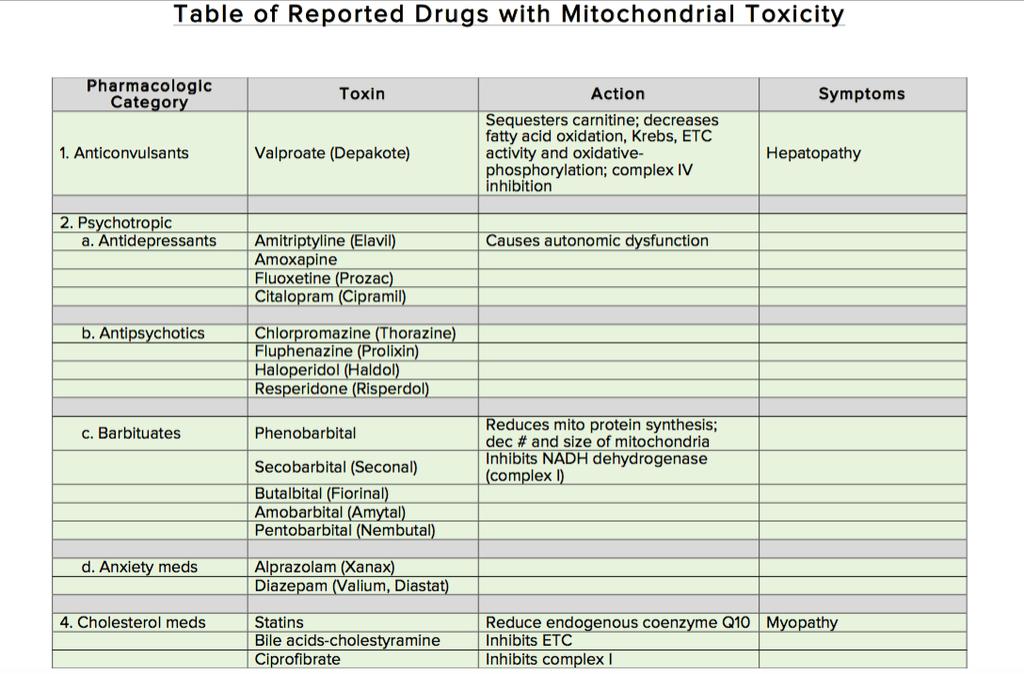
19 Mitochondrial toxins

20 Mitochondrial toxins
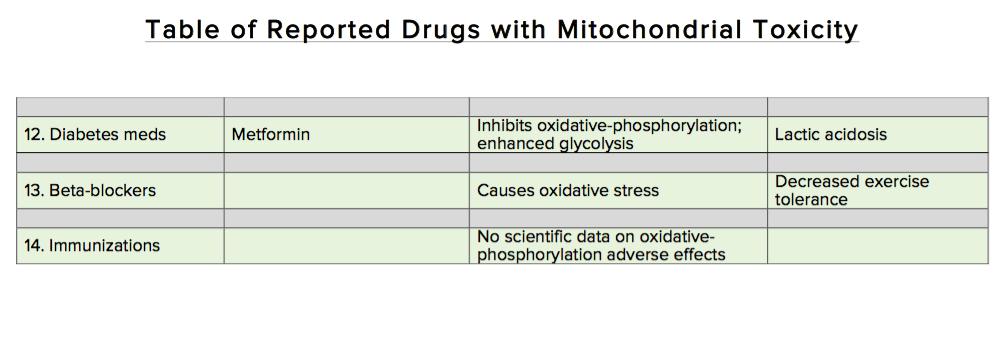
21 Mitochondrial Toxins
22 Diagnosing Mitochondrial diseases are difficult to diagnose. Referral to an appropriate research center is critical. Combination of clinical observations, laboratory evaluation, cerebral imaging, and muscle biopsies are used to aid diagnosis. A single blood or urine lab test with normal results does not rule out or confirm a 100% diagnosis of mitochondrial disease. Genetic testing can be done to assess for known mutations

23 Who knew..
24 Muscle Biopsy When treated with a dye that stains mitochondria red, muscles affected by mitochondrial disease often show ragged red fibers muscle cells (fibers) that have excessive abnormal mitochondria. Other stains can detect the absence of essential mitochondrial enzymes in the muscle. It is also possible to extract mitochondrial proteins from the muscle and measure their activity.

25 Ragged Red Fibers
26 Treating mitochondrial disease There is no definitive cure for mitochondrial diseases Therapy is aimed at alleviating symptoms, maintaining optimal health, using preventive measures to mitigate symptom worsening during times of physiologic stress, and avoiding mitochondrial toxins. The use of antioxidant supplements aimed at reducing reactive oxygen species that are produced in increased amounts in this disease.

27 Exercise Training
28 Anesthetic Considerations The heterogeneity of the diseases makes it very difficult to have the one perfect anesthetic. The lack of clinical trials investigating the effects of anesthetic agents in patients with mitochondrial disease has limited the anesthetists ability to deliver the perfect anesthetic. Adverse effects on mitochondrial function of many agents used in anesthesia have been documented in vitro, but there are few reports of adverse events in vivo. The theoretical effects of any agent need to be considered in the general context of any one patient s medical history.

29 Clinical Trials
30 Clinical Trial
31 Pre-op Evaluation Multi-system involvement in these disorders necessitates a thorough pre op evaluation including family history. Determine degree of neurological and musculoskeletal compromise. Careful cardiac assessment including EKG and echocardiography. Renal and Hepatic function All clinical manifestations of MD, including seizures, arrhythmias, cardiac dysfunction, myopathy, and endocrinopathies, can be worsened by trauma, illness, or surgical stress. Duration of NPO status

32 Local, regional or general?
33 Pre Medication Avoid lactated ringers solution which could increase lactate load. Avoid respiratory depressants, patients have inadequate response to hypoxia or hypercapnia.

34 Induction ensitivity to induction agents Ketamine and barbiturates inhibit complex I Etomidate inhibits complex I and complex II Propofol has been shown to be most problematic as it inhibits complex I and IV as well as disrupting fatty acid transport. Conflicting opinions however persist on single dose use.
35 PRI Propofol-related infusion syndrome (PRI) is a rare yet often fatal syndrome that has been observed in critically ill patients receiving propofol for sedation. Doses greater than 4mg/kg/hr for durations longer than 48 hours place a patient at risk for PRI. PRI is characterized by severe unexplained metabolic acidosis, arrhythmias, acute renal failure, rhabdomyolysis, hyperkalemia, and cardiovascular collapse. The exact pathophysiology of PRI remains to be determined, but is thought to be related to impaired tissue metabolism. Risk factors for developing PRI include sepsis, severe cerebral injury, and high propofol doses. Early recognition of the manifestations is the key to managing PRI. If is suspected, propofol should be discontinued and an alternative sedative agent initiated. General measures to support cardiac and renal function should be initiated promptly in patients with suspected PRI.
36 Muscle Relaxation There is conflicting evidence on the use of muscle relaxants. It is generally thought that there could be an increased sensitivity to non depolarizing muscle relaxants. uccinylcholine has been used successfully but is often avoided as these patients are thought to have a susceptibility to MH and could be subject to hyperkalemia if they are inactive.
37 Analgesia Beneficial in minimizing oxygen demand However impaired respiratory control necessitates that opioids are used with caution. Remifentanil is thought to have less effect on mitochondrial energetics than fentanyl which is preferred over morphine L.A s have been shown to inhibit complex I & acylcarnitine transferase. Lidocaine<ropivicaine<bupivacaine
38 Intra-op Monitor blood glucose especially in long cases. Less tolerance to hypoxia Maintain normothermia. Hypothermia further depresses mitochondrial activity. Keep patient hydrated
39 Emergence May not be a good candidate for deep extubation Consider leaving on ventilator or going to PACU on ventilator if far from baseline.
40 Post-Op Crucial period for these patients Exacerbation of mitochondrial disease may not be immediate. Warrants patients to be monitored longer Do not transfer from OR to stage 2 recovery.
41 Case Review 46 year old male pt kg BMI 22.6 scheduled for vascular access port. PMH: recent diagnosis of genetically associated mitochondrial disease, industrial injury that required transplantation of toes to right hand. PH: appendectomy, tonsillectomy, depression, chronic pain, GERD, left heart catheterization Allergies: Penicillin
42 Case review cont d Patient states he has been feeling progressively weak and fatigued since July work up done for lymes dz, adrenal insufficiency and myasthenia gravis all negative. Pt muscle biopsy in 2009 which showed no pathology. Meds: L-carnitine, L-arginine, vit c, vit d3, riboflavin, duloxetine, ubiquinone, dextrose 30mg po q morning,
43 What did we do? witched patient s IV fluids from LR to 0.9% N which was already running in the pre operative area. Checked patients blood glucose in pre op. Made anesthesiologist and surgeon aware of concerns with patient s disease process.
44 Anesthesia plan Upon deliberation, consensus was reached to perform a MAC anesthetic Anesthesia start time at 17:15 due to delay in surgeons other cases Midazolam 2mg, ketamine 20mg, precedex infusion 1mcg/kg bolus then started infusion (total 98mcg), fentanyl 35mcg. Anesthesia stop time 18:13. BP s, HR 70 s NR No untoward events. Intra op. Pt. was discharged home later that evening.

45
46 References Alberts, B., Johnson, A., Lewis, J., Raff, M., Roberts, K., & Walter, P. (2002). Molecular Biology Of The Cell (4th Edition ed.). New York, New York: Garland cience. Chial, H., & Craig, J. (2008). mtdna and Mitochondrial Diseases. Nature Education, 1 (1), 217. Chinnery, P. (2000). Mitochondrial Disorders Overview. GeneReviews. Cooper, G. (2000). The Cell: A Molecular Approach (2nd Edition ed.). underland, MA: inauer Associates. Cooper, M., & Fox, R. (2003). Anesthesia for corrective spinal surgery in a patient with leigh disease. Anesthesia & Analgesia, 97 (5), El-Hattab, A., & caglia, F. (2016, March). Mitochondrial Cytopathies. Cell Calcium. Finsterer, J., & egall, L. (2010). Drugs interfering with mitochondrial disorders. Drug and Chemical Toxicology, 33 (2), Finsterer, J., Haberler, C., & chmiedel, J. (2005). Deterioration of kearns-sayre syndrome following articaine administration for local anesthetic. Clinical Neuropharmacology. Hall, J., & Guyton, A. (2011). Guyton and Hall Textbook of Medical Physiology (12th ed.). Philadelphia: aunders Elsevier. Koenig, M. (2008). Presentation and Diagnosis of Mitochondrial Disease in Children. Pediatric Neurology, 38 (5), Krane, E., & Williamson, J. (2011). Anesthesia for Patients with Mitochondrial Disease.
47 References Kuhlbrandt, W. (2015). tructure and function of mitochondrial membrane protein complexes. BMC Biology, 13. Mtaweh, H., Bayir, H., Kochanek, P., & Bell, M. (2014). Effect of a single dose of propofol and lack of dextrose administration in a child with mitochondrial disease. Journal of Child Neurology, 29 (8), NP40-NP46. Niezgoda, J., & Morgan, P. (2013). Anesthetic Considerations in Patients with Mitochondrial Defects. Pediatric Anesthesia, 23 (9), Parikh,., aneto, R., Falk, M., Anselm, I., Cohen, B., & Haas, R. (2009). A modern approach to the treatment of mitochondrial disease. Current Treatments in Neurology, 11 (6), Rivera-Cruz, B. (2013). Mitochondrial Diseases and Anesthesia: a Literature Review of Current Opinions. AANA Journal, 81 (3), cheffler, I. (2007). Mitochondria (2nd ed.). Hoboken: Wiley. irrs,., Duncan, P., & O'Riley, M. (2010). Anesthetic Considerations in Mitochondrial Diseases. Retrieved March 1, 2016, from United Mitochondrial Disease Foundation: UMDF. (n.d.). understanding mitochondrial disease. Retrieved February 17, 2016, from United Mitochondrial Disease Foundation: umdf.org Wallace, J., & Perndt, H. (1998). Anesthesia and mitochondrial disease. Paediatric Anesthesia,
Anesthesia and Mitochondrial Cytopathies Bruce H. Cohen, MD, John Shoffner, MD, Glenn DeBoer, MD United Mitochondrial Disease Foundation, 1998
 Introduction Anesthesia and Mitochondrial Cytopathies Bruce H. Cohen, MD, John Shoffner, MD, Glenn DeBoer, MD United Mitochondrial Disease Foundation, 1998 This article will outline some basic aspects
Introduction Anesthesia and Mitochondrial Cytopathies Bruce H. Cohen, MD, John Shoffner, MD, Glenn DeBoer, MD United Mitochondrial Disease Foundation, 1998 This article will outline some basic aspects
Presentation and investigation of mitochondrial disease in children
 Presentation and investigation of mitochondrial disease in children Andrew Morris Willink Unit, Manchester Mitochondrial function Carbohydrate Fat Respiratory chain Energy Mitochondria are the product
Presentation and investigation of mitochondrial disease in children Andrew Morris Willink Unit, Manchester Mitochondrial function Carbohydrate Fat Respiratory chain Energy Mitochondria are the product
Nutritional Interventions in Primary Mitochondrial Disorders
 Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
Nutritional Interventions in Primary Mitochondrial Disorders Carolyn J Ellaway MBBS PhD FRACP CGHGSA Genetic Metabolic Disorders Service Sydney Children s Hospital Network Disciplines of Child and Adolescent
MITOCHONDRIAL DISEASE. Amel Karaa, MD Mitochondrial Disease Program Massachusetts General Hospital
 MITOCHONDRIAL DISEASE Amel Karaa, MD Mitochondrial Disease Program Massachusetts General Hospital Disclosures & Disclaimers United Mitochondrial Disease Foundation Research Grant North American Mitochondrial
MITOCHONDRIAL DISEASE Amel Karaa, MD Mitochondrial Disease Program Massachusetts General Hospital Disclosures & Disclaimers United Mitochondrial Disease Foundation Research Grant North American Mitochondrial
MYOCLONIC EPILEPSY WITH RAGGED RED FIBERS (MERRF) By- Promie Faruque
 By- Promie Faruque") MYOCLONIC EPILEPSY WITH RAGGED RED FIBERS (MERRF) By- Promie Faruque PHYSIOLOGY -MERRF is a rare panethnic mitochondrial disease which is caused by mutations in the mtdna -It mainly affects the muscle
MYOCLONIC EPILEPSY WITH RAGGED RED FIBERS (MERRF) By- Promie Faruque PHYSIOLOGY -MERRF is a rare panethnic mitochondrial disease which is caused by mutations in the mtdna -It mainly affects the muscle
An Introduction to mitochondrial disease.
 9 th September 2017 An Introduction to mitochondrial disease. Dr Andy Schaefer Consultant Neurologist and Clinical Lead NHS Highly Specialised Rare Mitochondrial Disease Service and Wellcome Trust Centre
9 th September 2017 An Introduction to mitochondrial disease. Dr Andy Schaefer Consultant Neurologist and Clinical Lead NHS Highly Specialised Rare Mitochondrial Disease Service and Wellcome Trust Centre
Metabolic Precautions & ER Recommendations
 Metabolic Precautions & ER Recommendations * To whom correspondence Sumit Parikh, should MD be addressed Center for Pediatric Neurology Cleveland Clinic Cleveland, OH UMDF 2010 The catabolic state Entering
Metabolic Precautions & ER Recommendations * To whom correspondence Sumit Parikh, should MD be addressed Center for Pediatric Neurology Cleveland Clinic Cleveland, OH UMDF 2010 The catabolic state Entering
Mitochondrial Disease: Navigating Clinical Uncertainties, Patient Misinformation & Urban Myths
 PBLD 2015 SPA Mitochondrial Disease: Navigating Clinical Uncertainties, Patient Misinformation & Urban Myths Moderators: Thomas Romanelli, M.D., Aaron Broman, MD Institution: Vanderbilt University/Monroe
PBLD 2015 SPA Mitochondrial Disease: Navigating Clinical Uncertainties, Patient Misinformation & Urban Myths Moderators: Thomas Romanelli, M.D., Aaron Broman, MD Institution: Vanderbilt University/Monroe
The presentation based on Propofol infusion syndrome Ne-Hooi Will Loh, MBBS EDIC FRCA FFICM Priya Nair, MBBS FRCA FFICM Contin Educ Anaesth Crit Care
 The presentation based on Propofol infusion syndrome Ne-Hooi Will Loh, MBBS EDIC FRCA FFICM Priya Nair, MBBS FRCA FFICM Contin Educ Anaesth Crit Care Pain (2013) 13 (6): 200-202 Risk factors Severe head
The presentation based on Propofol infusion syndrome Ne-Hooi Will Loh, MBBS EDIC FRCA FFICM Priya Nair, MBBS FRCA FFICM Contin Educ Anaesth Crit Care Pain (2013) 13 (6): 200-202 Risk factors Severe head
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Malignant Hyperthermia: What the ICU Needs to Know
 Malignant Hyperthermia: What the ICU Needs to Know Objectives 1. Compare the pathophysiology of malignant hyperthermia (MH) with presenting signs/symptoms in a critical care environment. 2. Identify critical,
Malignant Hyperthermia: What the ICU Needs to Know Objectives 1. Compare the pathophysiology of malignant hyperthermia (MH) with presenting signs/symptoms in a critical care environment. 2. Identify critical,
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy
 Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Awake regional versus general anesthesia in preterms and ex-preterm infants for herniotomy Department of Anaesthesia University Children s Hospital Zurich Switzerland Epidemiology Herniotomy needed in
Respiratory Depression
 Respiratory Depression H. William Gottschalk, D.D.S. Fellow, Academy of General Dentistry Fellow, American Dental Society of Anesthesiology Diplomate, American Board of Dental Anesthesiology Diplomate,
Respiratory Depression H. William Gottschalk, D.D.S. Fellow, Academy of General Dentistry Fellow, American Dental Society of Anesthesiology Diplomate, American Board of Dental Anesthesiology Diplomate,
Neurogenic Muscle Weakness, Ataxia, and Retinitis Pigmentosa (NARP) Genetic Testing Policy
 Genetic Testing Policy") Neurogenic Muscle Weakness, Ataxia, and Retinitis Pigmentosa (NARP) Genetic Testing Policy Procedure(s) addressed by this policy: Procedure Code(s) MT-ATP6 Targeted Mutation Analysis 81401 Whole Mitochondrial
Neurogenic Muscle Weakness, Ataxia, and Retinitis Pigmentosa (NARP) Genetic Testing Policy Procedure(s) addressed by this policy: Procedure Code(s) MT-ATP6 Targeted Mutation Analysis 81401 Whole Mitochondrial
General anesthesia. No single drug capable of achieving these effects both safely and effectively.
 General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General anesthesia General anesthesia is essential to surgical practice, because it renders patients analgesic, amnesia, and unconscious reflexes, while causing muscle relaxation and suppression of undesirable
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
Childhood Obesity: Anesthetic Implications
 Childhood Obesity: Anesthetic Implications The Changing Practice of Anesthesia 2015 UCSF Department of Anesthesia and Perioperative Care Marla Ferschl, MD Associate Professor of Anesthesia University of
Childhood Obesity: Anesthetic Implications The Changing Practice of Anesthesia 2015 UCSF Department of Anesthesia and Perioperative Care Marla Ferschl, MD Associate Professor of Anesthesia University of
Seizures Emergency Treatment
 Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL USE OF PROPOFOL (DIPRIVAN) FOR VENTILATOR MANAGEMENT
 FOR VENTILATOR MANAGEMENT") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL I. PURPOSE: To provide guidelines for the administration of Propofol, which is an anesthetic agent, indicated for the continuous intravenous
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOL I. PURPOSE: To provide guidelines for the administration of Propofol, which is an anesthetic agent, indicated for the continuous intravenous
Chapter 25. General Anesthetics
 Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Chapter 25 1. Introduction General anesthetics: 1. Analgesia 2. Amnesia 3. Loss of consciousness 4. Inhibition of sensory and autonomic reflexes 5. Skeletal muscle relaxation An ideal anesthetic: 1. A
Anesthetic concerns when paralyzing is not an option. By: Ashley Evick, BSN, SRNA
 Anesthetic concerns when paralyzing is not an option By: Ashley Evick, BSN, SRNA Introduction Neuromuscular blockade is utilized in many of the surgeries performed today. There are two types of neuromuscular
Anesthetic concerns when paralyzing is not an option By: Ashley Evick, BSN, SRNA Introduction Neuromuscular blockade is utilized in many of the surgeries performed today. There are two types of neuromuscular
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Role of IONM in reducing the incidence and severity in pediatric patients with AIS
 Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
Role of IONM in reducing the incidence and severity in pediatric patients with AIS Mohamed Nassef M.D PGY 2 ANESTHESIA McMaster University DEC 9, 2015 Objectives: Literature Review on neurological complications
SWISS SOCIETY OF NEONATOLOGY. Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant
 SWISS SOCIETY OF NEONATOLOGY Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant July 2001 2 Wagner B, Intensive Care Unit, University Children s Hospital
SWISS SOCIETY OF NEONATOLOGY Prolonged arterial hypotension due to propofol used for endotracheal intubation in a newborn infant July 2001 2 Wagner B, Intensive Care Unit, University Children s Hospital
Hypotension after induction, corrected with 20 mg ephedrine x cc LR EBL 250cc Urine output:
 Terry C. Wicks, CRNA, MHS Catawba Valley Medical Center Hickory, North Carolina 63 y.o., 5 2, 88 kg female for hand assisted laparoscopic tranversecolectomy Co-morbidities include: Hypertension controlled
Terry C. Wicks, CRNA, MHS Catawba Valley Medical Center Hickory, North Carolina 63 y.o., 5 2, 88 kg female for hand assisted laparoscopic tranversecolectomy Co-morbidities include: Hypertension controlled
REVIEW ARTICLE Mitochondrial disorders and general anaesthesia: a case series and review
 British Journal of Anaesthesia 100 (4): 436 41 (2008) doi:10.1093/bja/aen014 Advance Access publication February 19, 2008 REVIEW ARTICLE Mitochondrial disorders and general anaesthesia: a case series and
British Journal of Anaesthesia 100 (4): 436 41 (2008) doi:10.1093/bja/aen014 Advance Access publication February 19, 2008 REVIEW ARTICLE Mitochondrial disorders and general anaesthesia: a case series and
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
What is MH? Malignant Hyperthermia (MH)! Malignant Hyperthermia (MH) Malignant Hyperthermia (MH) ! The underlying physical mechanismintracellular
! Malignant Hyperthermia (MH) Malignant Hyperthermia (MH) ! The underlying physical mechanismintracellular") 10/2/13 What is MH? Libby Morse BSN RN CPAN An inherited disorder of skeletal muscle triggered in susceptible humans in most instances by inhalation agents and/ or succinylcholine, resulting in hypermetabolism,
10/2/13 What is MH? Libby Morse BSN RN CPAN An inherited disorder of skeletal muscle triggered in susceptible humans in most instances by inhalation agents and/ or succinylcholine, resulting in hypermetabolism,
Childhood mitochondrial encephalomyopathies: clinical course, diagnosis, neuroimaging findings, mtdna mutations and outcome in six children
 Lu and Huang Italian Journal of Pediatrics 2013, 39:60 ITALIAN JOURNAL OF PEDIATRICS CASE REPORT Open Access Childhood mitochondrial encephalomyopathies: clinical course, diagnosis, neuroimaging findings,
Lu and Huang Italian Journal of Pediatrics 2013, 39:60 ITALIAN JOURNAL OF PEDIATRICS CASE REPORT Open Access Childhood mitochondrial encephalomyopathies: clinical course, diagnosis, neuroimaging findings,
variant led to a premature stop codon p.k316* which resulted in nonsense-mediated mrna decay. Although the exact function of the C19L1 is still
 157 Neurological disorders primarily affect and impair the functioning of the brain and/or neurological system. Structural, electrical or metabolic abnormalities in the brain or neurological system can
157 Neurological disorders primarily affect and impair the functioning of the brain and/or neurological system. Structural, electrical or metabolic abnormalities in the brain or neurological system can
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
DEEP SEDATION TEST QUESTIONS
 Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery
 Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Anesthetic Techniques in Endoscopic Sinus and Skull Base Surgery Martha Cordoba Amorocho, MD Iuliu Fat, MD Supplement to Cordoba Amorocho M, Fat I. Anesthetic techniques in endoscopic sinus and skull base
Kurt Baker-Watson, MD Associate Professor
 Kurt Baker-Watson, MD Associate Professor Anesthetics Previous types, complications, satisfaction, familial history of complications, acute and chronic pain issues Airway Dentition/dental appliances, temporomandibular
Kurt Baker-Watson, MD Associate Professor Anesthetics Previous types, complications, satisfaction, familial history of complications, acute and chronic pain issues Airway Dentition/dental appliances, temporomandibular
Mitochondrial Diseases
 Mitochondrial Diseases Simon Heales SWIM Conference Taunton, November 29 th 2018 Respiratory Failure Cardiomyopathy Optic Atrophy / Retinitis Pigmentosa Seizures / Developmental delay Liver Failure Deafness
Mitochondrial Diseases Simon Heales SWIM Conference Taunton, November 29 th 2018 Respiratory Failure Cardiomyopathy Optic Atrophy / Retinitis Pigmentosa Seizures / Developmental delay Liver Failure Deafness
Chapter 8 Mitochondria and Cellular Respiration
 Chapter 8 Mitochondria and Cellular Respiration Cellular respiration is the process of oxidizing food molecules, like glucose, to carbon dioxide and water. The energy released is trapped in the form of
Chapter 8 Mitochondria and Cellular Respiration Cellular respiration is the process of oxidizing food molecules, like glucose, to carbon dioxide and water. The energy released is trapped in the form of
REQUISITION FORM NOTE: ALL FORMS MUST BE FILLED OUT COMPLETELY FOR SAMPLE TO BE PROCESSED. Last First Last First
 #: DEPARTMENT OF NEUROLOGY COLUMBIA COLLEGE OF PHYSICIANS & SURGEONS Room 4-420 630 West 168th Street, New York, NY 10032 Telephone #: 212-305-3947 Fax#: 212-305-3986 REQUISITION FORM NOTE: ALL FORMS MUST
#: DEPARTMENT OF NEUROLOGY COLUMBIA COLLEGE OF PHYSICIANS & SURGEONS Room 4-420 630 West 168th Street, New York, NY 10032 Telephone #: 212-305-3947 Fax#: 212-305-3986 REQUISITION FORM NOTE: ALL FORMS MUST
The Organism as a system
 The Organism as a system PATIENT 1: Seven-year old female with a history of normal development until age two. At this point she developed episodic vomiting, acidosis, epilepsy, general weakness, ataxia
The Organism as a system PATIENT 1: Seven-year old female with a history of normal development until age two. At this point she developed episodic vomiting, acidosis, epilepsy, general weakness, ataxia
THIAMINE TRANSPORTER TYPE 2 DEFICIENCY
 THIAMINE TRANSPORTER TYPE 2 DEFICIENCY WHAT IS THE THIAMINE TRANSPORTER TYPE 2 DEFICIENCY (hthtr2)? The thiamine transporter type 2 deficiency (hthtr2) is a inborn error of thiamine metabolism caused by
THIAMINE TRANSPORTER TYPE 2 DEFICIENCY WHAT IS THE THIAMINE TRANSPORTER TYPE 2 DEFICIENCY (hthtr2)? The thiamine transporter type 2 deficiency (hthtr2) is a inborn error of thiamine metabolism caused by
Prevention and Treatment Patrick Levelle, MD
 Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
The following criteria must be met in order to obtain pediatric clinical privileges for pediatric sedation.
 Pediatric Sedation Sedation of children is different from sedation of adults. Sedatives are generally administered to gain the cooperation of the child. The ability of the child to cooperate depends on
Pediatric Sedation Sedation of children is different from sedation of adults. Sedatives are generally administered to gain the cooperation of the child. The ability of the child to cooperate depends on
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center
 buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center PMH: hypertension, hyperlipidemia, asthma, hypothyroidism
buteykobreathing.co.nz Melanie Kalmanowicz, MD Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center PMH: hypertension, hyperlipidemia, asthma, hypothyroidism
Chapter 004 Procedural Sedation and Analgesia
 Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Robert Barski. Biochemical Genetics St James s University Hospital, Leeds. MetBioNet IEM Introductory Training
 Robert Barski Biochemical Genetics St James s University Hospital, Leeds Lactate is produced as the fate of anaerobic metabolism of pyruvate. It is an important intermediary metabolite especially with
Robert Barski Biochemical Genetics St James s University Hospital, Leeds Lactate is produced as the fate of anaerobic metabolism of pyruvate. It is an important intermediary metabolite especially with
The laboratory investigation of lactic acidaemia. J Bonham/T Laing
 The laboratory investigation of lactic acidaemia J Bonham/T Laing Reference range Typical ranges for blood lactate are: Newborn 0.3-2.2 mmol/l Nielsen J et al1 1994 1-12mo 0.9-1.8 mmol/l Bonnefont et al
The laboratory investigation of lactic acidaemia J Bonham/T Laing Reference range Typical ranges for blood lactate are: Newborn 0.3-2.2 mmol/l Nielsen J et al1 1994 1-12mo 0.9-1.8 mmol/l Bonnefont et al
Gaucher disease 3/22/2009. Mendelian pedigree patterns. Autosomal-dominant inheritance
 Mendelian pedigree patterns Autosomal-dominant inheritance Autosomal dominant Autosomal recessive X-linked dominant X-linked recessive Y-linked Examples of AD inheritance Autosomal-recessive inheritance
Mendelian pedigree patterns Autosomal-dominant inheritance Autosomal dominant Autosomal recessive X-linked dominant X-linked recessive Y-linked Examples of AD inheritance Autosomal-recessive inheritance
Dr. Gavin Parker PINCHER CREEK AB 140
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Gavin Parker PINCHER CREEK AB 140 MALIGNANT HYPERTHERMIA Malignant
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Gavin Parker PINCHER CREEK AB 140 MALIGNANT HYPERTHERMIA Malignant
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED
 ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
ANESTHETIZING DISEASED PATIENTS: URINARY; NEUROLOGICAL; TRAUMATIZED Lyon Lee DVM PhD DACVA Patients with Urinary Tract Diseases General considerations Three main factors to consider in anesthetizing urinary
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
The mitochondrion and its disorders
 100 PRACTICAL NEUROLOGY H O W T O U N D E R S T A N D I T The mitochondrion and its disorders Patrick F. Chinnery Department of Neurology, Regional Neurosciences Centre, Newcastle General Hospital and
100 PRACTICAL NEUROLOGY H O W T O U N D E R S T A N D I T The mitochondrion and its disorders Patrick F. Chinnery Department of Neurology, Regional Neurosciences Centre, Newcastle General Hospital and
Core Safety Profile. Pharmaceutical form(s)/strength: Solution for Injection CZ/H/PSUR/0005/002 Date of FAR:
/strength: Solution for Injection CZ/H/PSUR/0005/002 Date of FAR:") Core Safety Profile Active substance: Rocuronium bromide Pharmaceutical form(s)/strength: Solution for Injection P-RMS: CZ/H/PSUR/0005/002 Date of FAR: 31.05.2012 4.3 Contraindications Hypersensitivity
Core Safety Profile Active substance: Rocuronium bromide Pharmaceutical form(s)/strength: Solution for Injection P-RMS: CZ/H/PSUR/0005/002 Date of FAR: 31.05.2012 4.3 Contraindications Hypersensitivity
SEDATION FOR SMALL PROCEDURES
 SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
SEDATION FOR SMALL PROCEDURES Sinno Simons Erasmus MC Sophia Children s Hospital Rotterdam, the Netherlands s.simons@erasmusmc.nl SEDATION in newborns How and when How to evaluate How to dose Why to use
Children s of Alabama. Birmingham, Alabama
 Preoperative Evaluation of Pediatric Patients Heather Rankin, CRNA, MSN Children s of Alabama Birmingham, Alabama Objectives Define NPO guidelines Review history assessment Review system assessment Review
Preoperative Evaluation of Pediatric Patients Heather Rankin, CRNA, MSN Children s of Alabama Birmingham, Alabama Objectives Define NPO guidelines Review history assessment Review system assessment Review
ANAPHYLAXIS IN ANESTHESIA
 ANAPHYLAXIS IN ANESTHESIA Content I. Definition II. Epidemiology III. Etiology IV. Recognition V. Diagnosis VI. Observation and follow up VII.Drugs Definition Prophylaxis : protection Anaphylaxis : against
ANAPHYLAXIS IN ANESTHESIA Content I. Definition II. Epidemiology III. Etiology IV. Recognition V. Diagnosis VI. Observation and follow up VII.Drugs Definition Prophylaxis : protection Anaphylaxis : against
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Patterns of Single-Gene Inheritance Cont.
 Genetic Basis of Disease Patterns of Single-Gene Inheritance Cont. Traditional Mechanisms Chromosomal disorders Single-gene gene disorders Polygenic/multifactorial disorders Novel mechanisms Imprinting
Genetic Basis of Disease Patterns of Single-Gene Inheritance Cont. Traditional Mechanisms Chromosomal disorders Single-gene gene disorders Polygenic/multifactorial disorders Novel mechanisms Imprinting
Mitochondrial Implications in Coronary Heart Disease. (Pre-Ischemia)
") Mitochondrial Implications in Coronary Heart Disease (Pre-Ischemia) Arteriosclerotic Vascular Disease (ASVD) ASVD is the build up of plaque along arterial walls. Plaque is composed of cholesterol, fat,
Mitochondrial Implications in Coronary Heart Disease (Pre-Ischemia) Arteriosclerotic Vascular Disease (ASVD) ASVD is the build up of plaque along arterial walls. Plaque is composed of cholesterol, fat,
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Biochemistry of cellular organelles
 Kontinkangas, L101A Biochemistry of cellular organelles Lectures: 1. Membrane channels; 2. Membrane transporters; 3. Soluble lipid/metabolite-transfer proteins; 4. Mitochondria as cellular organelles;
Kontinkangas, L101A Biochemistry of cellular organelles Lectures: 1. Membrane channels; 2. Membrane transporters; 3. Soluble lipid/metabolite-transfer proteins; 4. Mitochondria as cellular organelles;
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Hompes Method Lesson 29 Organic Acids Part One
 Hompes Method Lesson 29 Organic Acids Part One Health for the People Ltd not for reuse without expressed permission Organic Acids - Introduction The ultimate tool for laboratory evaluations in nutritional
Hompes Method Lesson 29 Organic Acids Part One Health for the People Ltd not for reuse without expressed permission Organic Acids - Introduction The ultimate tool for laboratory evaluations in nutritional
Metabolic diseases of the liver
 Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Satisfactory Analgesia Minimal Emesis in Day Surgeries. (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone
 A Randomized Control Trial Comparing Morphine and Hydromorphone") Satisfactory Analgesia Minimal Emesis in Day Surgeries (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone HARSHA SHANTHANNA ASSISTANT PROFESSOR ANESTHESIOLOGY MCMASTER UNIVERSITY
Satisfactory Analgesia Minimal Emesis in Day Surgeries (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone HARSHA SHANTHANNA ASSISTANT PROFESSOR ANESTHESIOLOGY MCMASTER UNIVERSITY
Enteral Tube Feeding in Paediatric Mitochondrial Diseases
 www.nature.com/scientificreports Received: 6 April 2017 Accepted: 23 November 2017 Published: xx xx xxxx OPEN Enteral Tube Feeding in Paediatric Mitochondrial Diseases Han Som Choi & Young-Mock Lee We
www.nature.com/scientificreports Received: 6 April 2017 Accepted: 23 November 2017 Published: xx xx xxxx OPEN Enteral Tube Feeding in Paediatric Mitochondrial Diseases Han Som Choi & Young-Mock Lee We
Committee to Review Adverse Effects of Vaccines An Institute of Medicine Workshop on the Safety of Vaccines. Mitochondrial Disorders
 Committee to Review Adverse Effects of Vaccines An Institute of Medicine Workshop on the Safety of Vaccines Mitochondrial Disorders Bruce H. Cohen, MD Cleveland Clinic August 26, 2009 special thanks to
Committee to Review Adverse Effects of Vaccines An Institute of Medicine Workshop on the Safety of Vaccines Mitochondrial Disorders Bruce H. Cohen, MD Cleveland Clinic August 26, 2009 special thanks to
HOPE. ENERGY. LIFE. MitoFIRST Handbook An Introductory Guide HOPE. ENERGY. LIFE. HOPE. ENERGY. LIFE. HOPE. ENERGY. LIFE. HOPE. ENERGY. LIFE.
 HOPE. ENERGY. LIFE MitoFIRST Handbook An Introductory Guide Focus on Information, Resources, Support, and Treatments ABOUT UMDF The United Mitochondrial Disease Foundation is redefining hope for families
HOPE. ENERGY. LIFE MitoFIRST Handbook An Introductory Guide Focus on Information, Resources, Support, and Treatments ABOUT UMDF The United Mitochondrial Disease Foundation is redefining hope for families
7 Medical Genetics. Hemoglobinopathies. Hemoglobinopathies. Protein and Gene Structure. and Biochemical Genetics
 SESSION 7 Medical Genetics Hemoglobinopathies and Biochemical Genetics J a v a d F a s a J a m s h i d i U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 Hemoglobinopathies
SESSION 7 Medical Genetics Hemoglobinopathies and Biochemical Genetics J a v a d F a s a J a m s h i d i U n i v e r s i t y o f M e d i c a l S c i e n c e s, N o v e m b e r 2 0 1 7 Hemoglobinopathies
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient
 Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Cardiovascular Effects of Anesthesia for Cesarean Delivery in the Cardiac Patient Katherine W. Arendt, M.D. Associate Professor of Anesthesiology Mayo Clinic, Rochester, Minnesota Cardiac Problems in Pregnancy
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
The Challenging Pediatric Cardiac Patient. Edmund Jooste
 The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
Anaesthetic Plan And The Practical Conduct Of Anaesthesia. Dr.S.Vashisht Hillingdon Hospital
 Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Anaesthetic Plan And The Practical Conduct Of Anaesthesia Dr.S.Vashisht Hillingdon Hospital Anaesthetic Plan Is based on Age / physiological status of the patient (ASA) Co-morbid conditions that may be
Problem Based Learning. Problem. Based Learning
 Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Problem 2013 Based Learning Problem Based Learning Your teacher presents you with a problem in anesthesia, our learning becomes active in the sense that you discover and work with content that you determine
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
PAAQS Reference Guide
 Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Q. 1 Patient's Date of Birth (DOB) *Required Enter patient's date of birth PAAQS Reference Guide Q. 2 Starting Anesthesiologist *Required Record the anesthesiologist that started the case Q. 3 Reporting
Airway management problem during anaesthesia. Airway management problem in ICU / HDU. Airway management problem occurring in the Emergency Department
 4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
4th National Audit Project of the Royal College of Anaesthetists: Major Complications of Airway Management in the UK Please select one form from the list below Airway management problem during anaesthesia
Ketofol: risky or revolutionary: CPD article IV
 Ketofol: risky or revolutionary: CPD article IV Abstract Ketofol, a sedative/analgesic combination of ketamine and propofol, which can be administered as a mixture in the same syringe or independently,
Ketofol: risky or revolutionary: CPD article IV Abstract Ketofol, a sedative/analgesic combination of ketamine and propofol, which can be administered as a mixture in the same syringe or independently,
A study of 133 Chinese children with mitochondrial respiratory chain complex I deficiency
 Clin Genet 2015: 87: 179 184 Printed in Singapore. All rights reserved Short Report 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd CLNCAL GENETCS doi: 10.1111/cge.12356 A study of 133 Chinese
Clin Genet 2015: 87: 179 184 Printed in Singapore. All rights reserved Short Report 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd CLNCAL GENETCS doi: 10.1111/cge.12356 A study of 133 Chinese
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Chapter 18. Skeletal Muscle Relaxants (Neuromuscular Blocking Agents)
") Chapter 18 Skeletal Muscle Relaxants (Neuromuscular Blocking Agents) Uses of Neuromuscular Blocking Facilitate intubation Surgery Agents Enhance ventilator synchrony Reduce intracranial pressure (ICP)
Chapter 18 Skeletal Muscle Relaxants (Neuromuscular Blocking Agents) Uses of Neuromuscular Blocking Facilitate intubation Surgery Agents Enhance ventilator synchrony Reduce intracranial pressure (ICP)
Procedural Sedation and Analgesia in the ED
 Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
HYDROGEN ION HOMEOSTASIS
 ACID BASE BALANCE 1 HYDROGEN ION HOMEOSTASIS Free H + ions are present in very minute quantity in the blood (is around 1 in 3 million of Na + concentration) H + ion concentration is 0.00004 meq/l Na +
ACID BASE BALANCE 1 HYDROGEN ION HOMEOSTASIS Free H + ions are present in very minute quantity in the blood (is around 1 in 3 million of Na + concentration) H + ion concentration is 0.00004 meq/l Na +
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY
 ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
ETIOLOGY AND PATHOGENESIS OF HYPOXIC-ISCHEMIC ENCEPHALOPATHY HYPOXIC-ISCHEMIC ENCEPHALOPATHY Hypoxic-İschemic Encephalopathy Encephalopathy due to hypoxic-ischemic injury [Hypoxic-ischemic encephalopathy
BOTULINUM TOXIN AND INTRATHECAL BACLOFEN. Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018
 BOTULINUM TOXIN AND INTRATHECAL BACLOFEN Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018 INJECTABLES MEDICAL MANAGEMENT OF SPASTICITY Leonard, J In: Botulinum toxin: 2009 A protein and
BOTULINUM TOXIN AND INTRATHECAL BACLOFEN Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018 INJECTABLES MEDICAL MANAGEMENT OF SPASTICITY Leonard, J In: Botulinum toxin: 2009 A protein and
Diagnosis and management of mitochondrial disease: a consensus statement from the Mitochondrial Medicine Society
 American College of Medical Genetics and Genomics SYSTEMATIC REVIEW Diagnosis and management of mitochondrial disease: a consensus statement from the Mitochondrial Medicine Society Sumit Parikh, MD 1,
American College of Medical Genetics and Genomics SYSTEMATIC REVIEW Diagnosis and management of mitochondrial disease: a consensus statement from the Mitochondrial Medicine Society Sumit Parikh, MD 1,
Chapter 18 Neuromuscular Blocking Agents Study Guide and Application Exercise
 Chapter 18 Neuromuscular Blocking Agents Study Guide and Application Exercise 1. Read chapter 2. Review objectives (p.305) 3. Review key terms and definitions (p.305) Add: Cholinesterase inhibitor Vagal
Chapter 18 Neuromuscular Blocking Agents Study Guide and Application Exercise 1. Read chapter 2. Review objectives (p.305) 3. Review key terms and definitions (p.305) Add: Cholinesterase inhibitor Vagal
Sedation in Children
 CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Training Syllabus CLINICAL SYLLABUS
 Training Syllabus CLINICAL SYLLABUS SYLLABUS FOR TRAINING IN CLINICAL PAEDIATRIC METABOLIC MEDICINE Updated July 2006 This syllabus is intended as a guide. Whilst the training should be comprehensive,
Training Syllabus CLINICAL SYLLABUS SYLLABUS FOR TRAINING IN CLINICAL PAEDIATRIC METABOLIC MEDICINE Updated July 2006 This syllabus is intended as a guide. Whilst the training should be comprehensive,