Status Epilepticus: The good, the bad, the ugly
|
|
|
- Joshua Mills
- 5 years ago
- Views:
Transcription
1 Status Epilepticus: The good, the bad, the ugly Emily J. Gilmore, MD, MS Assistant Professor Division of Neurocritical Care and Emergency Neurology, and Epilepsy (CCEEG) Yale New Haven Hospital/Yale School of Medicine Latin American Workshop Havana, Cuba November 14 th -15 th 2016
2
3

4

5



6 Trinka et al, Report of the ILAE Task Force on Classification of Status Epilepticus 2015
7 Status Epilepticus (SE) Convulsive SE Nonconvulsive SE Prominent Prominent Motor Motor Features Features Without Without Prominent Prominent Motor Motor Features Features (Subtle) (Subtle) Generalized Generalized With With and and Without Without Impairment Impairment in in Consciousness Consciousness Convulsive SE Nonconvulsive SE Ictal-Interictal Continuum Prominent Motor Features Focal Focal with with impaired impaired consciousness consciousness (ie (ie aphasia aphasia only) only) Often Often excludes excludes EPC EPC Generalized Generalized and and Focal Focal Without Prominent Motor Features (Subtle) < 3 hz Non-Evolving Periodic or Rhythmic Activity Generalized With and Without Impairment in Consciousness Without Prominent Motor Features Focal with impaired consciousness (ie aphasia only) Often With Impairment of Consciousness Often excludes EPC Generalized and Focal Generalized and Focal < <3 3 hz hz Non-Evolving Non-Evolving Periodic Periodic or or Rhythmic Rhythmic Activity Activity Ictal-Interictal Continuum Without Without Prominent Prominent Motor Motor Features Features Often Often With With Impairment Impairment of of Consciousness Consciousness Generalized Generalized and and Focal Focal

8 Time is Brain
9 Time is Brain The longer generalized SE persists, the harder it is to control Neuronal damage is primarily caused by continuous excitatory activity, not systemic complications. Systemic complications, may exacerbate neuronal damage. Every seizure counts in terms of making SE, especially convulsive, more difficult to control and for causing neuronal damage.
10 The SE Continuum Continuous seizure activity for > 5 min or recurrent episodes without recovery in between episodes Established Status Epilepticus Status epilepticus unresponsive to initial standard antiepileptic medications (1 of patients with SE st and one 2 nd line therapy) 1 Occurs in 23-43% 2 Refractory Status Epilepticus Seizures continuing despite additional AEDs and/or after the initial continuous infusion of anesthetic agents Super-Refractory Status Epilepticus 1. Bleck TP. Refractory status epilepticus. Curr Opin Crit Care 2005; 11: Rossetti AO. Management of Refractory Status Epilepticus in Adults. Lancet Neurol. 2011; 10:
11 CSE: The Good CSE Other; 6.00% Anoxia; 4.00% Prominent Motor Features Generalized Metabolic; 4.00%?Focal with impaired consciousness Excludes EPC Tumor; 6.00% Stroke; 5.00% AED noncompliance; 29.00% Trauma; 6.00% Refractory epilepsy; 6.00% CNS infection; 8.00% Ethanol-related; 26.00% Lowenstein DH, Alldredge BK. Status epilepticus at an urban public hospital in the 1980s. Neurology 1993;43:
12 Epidemiology of SE Incidence /100,000 depending on population 3 million of SE/yr 70% GCSE (75% Overt) More than half of patients will not have had a prior seizure Half of patients will have an acute symptomatic etiology SE is the initial presentation of new onset seizure disorder in 1/3 of cases DeLorenzo et al Neurology 1996

13
14 Beyond Benzos: Evidence Free Zone Brophy GM. Et al NCC Clobazam Probably Class IIb, level C
15 My hospital has a status epilepticus management protocol? A. B. C. Yes No Don t know st nd rd We now have high level data to support the use of specific 1, 2 and 3 line agents in the management of status epilepticus? D. E. F. Yes No Don t know

16 AES Status Epilepticus Treatment Algorithm, Epil Currents 2016
17
18 American Epilepsy Soc. Status Epilepticus Guidelinewww.aesnet.org; Epil Currents 2016 For initial therapy: IM midaz, IV loraz or IV diaz should be used Although IV phenobarb effective, its slower rate of administration positions it as an alternative initial therapy rather than a drug of choice. For pre-hospital or if above 3 benzos not avail, rectal diaz, nasal midaz and buccal midaz are reasonable alternatives (level B) For second therapy: No clear choice. Reasonable options include fosphenytoin (level U), VPA (level B) and LEV (level U) For third therapy: no clear choice: can repeat second line or use thiopental, midaz, pentobarb or propofol, all w/ continuous EEG monitoring


19 First 10 min:
20 American Epilepsy Soc. Status Epilepticus Guidelinewww.aesnet.org; Epil Currents 2016 For initial therapy: IM midaz, IV loraz or IV diaz should be used (level A, 4 RCTs) Although IV phenobarb effective, its slower rate of administration positions it as an alternative initial therapy rather than a drug of choice. For pre-hospital or if above 3 benzos not avail, rectal diaz, nasal midaz and buccal midaz are reasonable alternatives (level B) For second therapy: No clear choice. Reasonable options include fosphenytoin (level U), VPA (level B) and LEV (level U) For third therapy: no clear choice: can repeat second line or use thiopental, midaz, pentobarb or propofol, all w/ continuous EEG monitoring
21 Neurocritical Care Society (2012) Lacosamide?
22 10-30 min
23 Established Status Epilepticus Treatment Trial (ESETT) Multicenter, randomized, allocation concealed, Bayesian adaptive, Phase III comparative effectiveness trial. The ESE treatment trial is designed to determine the most effective and/or the least effective treatment of ESE among patients older than two years by comparing three arms: fosphenytoin (fpht) levetiracetam (LVT), and valproic acid (VPA). The primary outcome measure is cessation of clinical seizure activity and improving mental status, without serious adverse effects or further intervention at 60 min after administration of study drug.
24 NCSE: The BAD NCSE Without Prominent Motor Features (Subtle) Other; 6.00% Anoxia; 4.00% Metabolic; 4.00% With and Without Impairment in Consciousness (ie aphasia only) Generalized and Focal Tumor; 6.00% Stroke; 5.00% AED noncompliance; 29.00% Trauma; 6.00% Refractory epilepsy; 6.00% CNS infection; 8.00% Ethanol-related; 26.00% Lowenstein DH, Alldredge BK. Status epilepticus at an urban public hospital in the 1980s. Neurology 1993;43:
25 Pathways to Badness 0.5 NONCONVULSIVE SEIZURES: Prevalence in critically ill adults w/ primary neuro diagnosis
26 Risk factors for nonconvulsive seizures and NCSE Husain et al JNNP 2003: 48 urgent EEGs for possible NCSE; positive in 12; 3 risk factor identified: Severely impaired mental status Oculomotor abnormalities Nystagmus Sustained eye deviation Hippus Remote risk factors for epilepsy Claassen et al Neurology 2004: 570 consecutive patients undergoing continuous EEG monitoring
27 Independent predictors of CEEG-documented seizures 1. Coma on neuro exam at start of CEEG 56% of 97 comatose patients vs. 12% of 473 other. 2. Age < 18 years 36% of 75 patients <18 y.o. vs. 17% of 495 pts > Past medical history of epilepsy 41% of 68 patients w/ PMH epil vs. 16% of 502 w/out. 4. Convulsive seizures prior to monitoring 43% of 134 patients with vs. 12% of 436 w/out. 5. Periodic discharges (PLEDs or GPEDs) or Suppresion-burst Claassen 2004
28 Definition and Diagnosis of NCSE Focal or generalized spikes, sharp waves, or sharp-and-slow complexes at frequencies >3 Hz Focal or generalized spikes, sharp waves, or sharp-and-slow complexes at frequencies <3 Hz or rhythmic activity >0.5Hz and ONE of the following: EEG AND clinical improvement after an IV trial of an AED Subtle clinical ictal phenomena during the EEG pattern Typical spatiotemporal evolution, including incrementing onset (increase in voltage and change in frequency), or evolution in pattern (change in frequency >1 Hz or change in location), or decrementing termination (voltage or frequency) But for how long? Unified EEG terminology and criteria for nonconvulsive status epilepticus. Beniczky S, Hirsch LJ, Kaplan PW, Pressler R, Bauer G, Aurlien H, Brøgger JC, Trinka E Epilepsia Sep;54 Suppl 6:28-9.
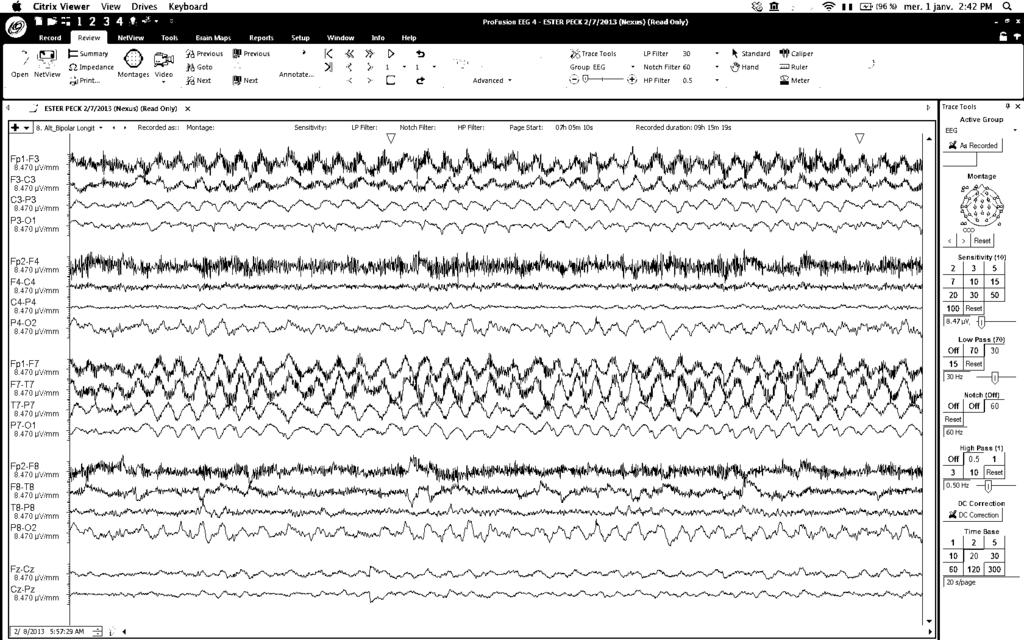
29 83 year old woman with a PMH of remote ischemic stroke x 2 with aphasia/mild RHP (able to walk with cane), dementia and LRE who resents from an OSH where she had been seizing for 5 days despite ginger titration of AEDs and Ativan pushes. On arrival, she was not intubated, but was unresponsive with episodes of R gaze preference, R arm extension, lasting about a minute and occurring every 5-6 minutes. AEDS: Levetiracetam 1000 mg bid, phenytoin 200 mg bid (had been 300 mg bid), Ativan (received 7-1 mg IVP in the last 24 hours) Other meds: Coumadin, metoprolol, risperdone, sertraline, methocarbamol PHT level 6


30 CT
31 EEG:
32 EEG:

33 EEG:
34 EEG (Summary): Frequent seizures arising from the L temporal-occipital region, spreading over the entire L hemisphere and at times to the R hemisphere. Occurring 10/hr No clear clinical correlate Diagnosis: Focal seizures with impaired consciouness
35 What would you do next?
36 Outcome Patient was DNR/DNI on arrival - > family changed to DNR Loaded with Levetiracetam 2500 mg IV, VPA 30 mg/kg x 2 (level returned at 140) but seizures persisted at 5-6/hr. Loaded with Vimpat 400 mg IV after which her seizures stopped. She was placed on LVT 1000 mg IV q8, Vimpat 150 mg IV q6, PHT 200 mg q12, VPA 900 mg q12. Her admission UA/Uctx was positive for pansensitive Ecoli (> 100k). PHT and LVT were weaned off over the subsequent 5 days, her mental status improved, she passed a swallow evaluation and was discharged back to her long-term care nursing facility after a 2 week hospital stay.
37 Take Home Message In the elderly, being aggressive with anesthetics is associated with worse outcome Engage the family in goals of care discussions early without being overly pessimistic so as not to fall off the self-fulfilling prophecy cliff. If you are going to use non-sedating AEDs, you have to use therapeutic doses Have a low threshold to evaluate for occult infection patients with seizures often meet SIRS criteria
38 Anti-seizure Medication Trial for the Diagnosis of Non-Convulsive Status Epilepticus Patients: Rhythmic or periodic focal or generalized epileptiform discharges on EEG with neurological impairment. Monitoring: EEG, pulse ox, BP, ECG, respiratory rate, with dedicated nurse. Antiepileptic Drug Trial: Sequential small doses of rapidly-acting short-duration benzodiazepine such as midazolam at 1mg/dose, or a non-sedating IV AED. (lev, lacos, fpht/pht, vpa). Between doses, repeated clinical and EEG assessment. Trial is stopped after any of the following: opersistent resolution of the EEG pattern (and exam repeated) odefinite clinical improvement orespiratory depression, hypotension, or other adverse effect oa maximum dose is reached (such as 0.2 mg/kg midazolam, though higher may be needed if on chronic benzodiazepines) otest is considered positive if there is resolution of the potentially ictal EEG pattern AND either an improvement in the clinical state or the appearance of previously-absent normal EEG patterns (eg. posterior dominant alpha rhythm). If EEG improves but patient does not, the result is equivocal ( possible NCSE )
39 Do patients wake up after treating NCSE? If so, when? Beth Israel Deaconess, Boston Of 68 patients with seizures on EEG in an ICU, excluding post-arrest, 38 (56%) improved in alertness, including 25/52 comatose patients Improvement not immediate, but often same day 21/38 responders survived vs 1/30 of others Didn t use anesthetics Drislane et al, Aug 2008
40 The Ugly (PART 1): RSE and SRSE
41 American Epilepsy Soc. Status Epilepticus Guidelinewww.aesnet.org; Epil Currents 2016 For initial therapy: IM midaz, IV loraz or IV diaz should be used (level A, 4 RCTs) Although IV phenobarb effective, its slower rate of administration positions it as an alternative initial therapy rather than a drug of choice. For pre-hospital or if above 3 benzos not avail, rectal diaz, nasal midaz and buccal midaz are reasonable alternatives (level B) For second therapy: No clear choice. Reasonable options include fosphenytoin (level U), VPA (level B) and LEV (level U) For third therapy: no clear choice: can repeat second line or use thiopental, midaz, pentobarb or propofol, all w/ continuous EEG monitoring
42 > 30 min
43 The Ugly (PART 2): IIC IIC < 3 hz Non-Evolving Periodic or Rhythmic Activity Without Prominent Motor Features Often With Impairment of Consciousness Generalized and Focal

44 Dividing EEG patterns in encephalopathic or comatose patients into a strict dichotomy of ictal or not ictal is not only extremely difficult, but can be misleading to clinicians and therefore potentially.
45 The ictal-interictal continuum (IIC) Interictal: <1 Hz Ictal: clinical correlate; evolving; or >2.5 Hz IIC: Typically between 1 and 2.5 Hz, fluctuating, and either rhythmic (RDA), periodic (PDs), or both (PD+R or RDA+S); much less commonly SW (spikewave or sharp-wave) Note that this includes triphasic waves Might also include frequent nonconvulsive seizures occupying ~50% of a recording
46 Value of benzo trial for possible NCSE Hopp JL et al, The Neurologist 2011 (U. Maryland) 62 patients with benzo trial for impaired consciousness with epileptiform pattern potentially consistent with NCSE Examined immediately and for 1 hour 85% of all patients had improvement in EEG 22 (35%) had improved consciousness within an hour, and all 22 survived and had good functional outcome 40 (65%) did not respond clinically, and only 14 of those 40 (35%) recovered consciousness EEG response w/out clinical improvement also correlated w/ modestly higher chance of awakening prior to discharge than having no EEG response, but less strongly, and no correlation with survival
47 Response rates to anticonvulsant trials in patients with triphasic wave EEG patterns of uncertain significance O Rourke D, et al, for the CCEMRC, Neurocrit Care institutions (Yale, Columbia, MGH), retrospective, N=64 w/ TW pattern who got benzo trial for possible NCSE 72% had metabolic derangement or infection Excluded postanoxia and those with definite status epilepticus (clinical or on EEG) Response: resolution of EEG and either unequivocal improvement in encephalopathy or appearance of previously absent normal EEG patterns Divided into immediate (<2 hours) or delayed Benzo trials: 83% loraz, mean dose 2.5 mg; 17% midaz, mean 4 mg Non-benzo trials: 69% levetiracetam, 44% pht, 7% lacos, 4% vpa
 and 19/45 trials with nonsedating AEDs (42%; 7% immed, 20% delayed but definite, 16% delayed and possible).")
48 Response rates to anticonvulsant trials in patients with triphasic wave EEG patterns of uncertain significance O Rourke D, Chen, PM Westover MB, and CCEMRC, Neurocrit Care 2015 Positive response in 10/53 benzo trials (19%, all immediate) and 19/45 trials with nonsedating AEDs (42%; 7% immed, 20% delayed but definite, 16% delayed and possible). Overall 34% definite positive response and 11% possible No difference in metabolic status in responders and nonresponders No difference in benzo doses between responders and nonresponders Complications of trial: one only: bradycardia, then PEA arrest after load of fospht; recovered. Suggests these trials are useful and that many patients with metabolic encephalopathy and triphasic waves have an AED responsive condition.
49 Case. #2 84 y.o. woman with atrial fibrillation, congestive heart failure, recent right middle cerebral artery stroke for which she underwent mechanical thrombectomy at an outside hospital. Hospital course was complicated by septic shock with multiorgan failure re-quiring dialysis, tracheostomy and feeding tube. Continuous EEG showed unequivocal nonconvulsive status epilepticus, successfully treated. She was discharged to rehab, awake and able to follow simple commands. Soon after arriving in rehab, she became less interactive It was felt that AEDs were the culprit so they were decreased. When she did not improve, she was transferred to Yale Initial EEG: GPDs at Hz, fluctuating
")
50 (a) 6 hours (b) (c)
51 Case, continued Lorazepam led to marked improvement in EEG, including improved background and including appearance of sleep spindles; no immediate clinical change Gradually awoke over next 48 hours w/ no return of nonconvulsive seizures, interictal-ictal continuum or periodic discharges. No major metabolic or other medical changes over that time period.
52 Practical Treatment Points: IIC The dichotomy between ictal and interictal may not exist in many patients. The most common continuum patterns are between 1 and 2.5 Hz. IV anti-seizure medication trials work. Now that we know what to call these patterns, we can study them need randomized trial. Reliable biomarkers of seizure-induced neuronal injury are needed to approach these patients more rationally.
53 Conclusions Many of these cases are often complicated. Intractable conditions can be challenging especially with sparse evidence-based guidance. Early treatment is critical, and the identification of an underlying etiology dictates both continued treatment and prognosis. Aggressiveness of treatment may be controversial, but timely EEG is useful for diagnosis, management, optimizing treatment response, as well as for determining prognosis. Treatment should not be relegated to the nihilistic fate of a self-fulfilling prophecy, especially in younger patients without widespread irreversible brain injury.
54 Future Directions: SE Which AEDs work best? What are cost-effective approach for the early identification and treatment of seizures and status epilepticus? What are the effects of prolonged EEG monitoring on outcomes? What is the effect of early use of anesthetics, their associated complications as well as optimal depth and duration of treatment of RSE and SRSE? When should immunotherapy be started? Can we develop dry electrode EEG devices that can be easily applied without a trained EEG technologist? What are the mechanisms of epileptogenesis in this heterogeneous groups of patients with acute symptomatic seizures?
55 Future Directions: IIC Are these patterns surrogate markers for more severely injured brain? Do they lead to secondary neuronal injury via excessive metabolic demand, excitotoxicity, or other mechanisms? Do they always warrant treatment or at least prophylaxis? Should our goal be to decrease burden or make them go away completely? How long should we treat? Are these patterns associated with the development of epilepsy and long term functional and cognitive outcomes?
56 Thanks Questions.
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
ESETT OUTCOMES. Investigator Kick-off Meeting Robert Silbergleit, MD
 ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
Electroencephalography. Role of EEG in NCSE. Continuous EEG in ICU 25/05/59. EEG pattern in status epilepticus
 EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology
 A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
Continuous EEG: A Standard in Canada?
 Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
The ictal interictal continuum
 The ictal interictal continuum Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures: Research Support: Columbia
The ictal interictal continuum Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures: Research Support: Columbia
Generalized seizures, generalized spike-waves and other things. Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke
 Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Status Epilepticus: A refresher. Objectives
 Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Periodic discharges and prognostic significance Pedersen GL et al, Clin Nphys 2013 (Denmark)
") Periodic discharges and prognostic significance Pedersen GL et al, Clin Nphys 2013 (Denmark) 102 patients w/ PDs vs 102 age, gender and etiology matched controls, using ACNS nomenclature and read blinded
Periodic discharges and prognostic significance Pedersen GL et al, Clin Nphys 2013 (Denmark) 102 patients w/ PDs vs 102 age, gender and etiology matched controls, using ACNS nomenclature and read blinded
Status Epilepticus. Ednea Simon, MD Swedish Pediatric Neuroscience Center
 Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain Tumors
 Neurocrit Care (2012) 16:109 113 DOI 10.1007/s12028-011-9626-4 ORIGINAL ARTICLE Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain
Neurocrit Care (2012) 16:109 113 DOI 10.1007/s12028-011-9626-4 ORIGINAL ARTICLE Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain
Simple Protocol & Bayesian Design: Established Status Epilepticus Treatment Trial (ESETT)
") Simple Protocol & Bayesian Design: Established Status Epilepticus Treatment Trial (ESETT) Jaideep Kapur on behalf of ESETT invertigator University of Virginia Status epilepticus is a condition resulting
Simple Protocol & Bayesian Design: Established Status Epilepticus Treatment Trial (ESETT) Jaideep Kapur on behalf of ESETT invertigator University of Virginia Status epilepticus is a condition resulting
Management of acute seizure and status epilepticus
 Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi Hospital Sunday August 27 10.00-10.45 Bangsan Objectives Acute repetitive seizure Status epilepticus
Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi Hospital Sunday August 27 10.00-10.45 Bangsan Objectives Acute repetitive seizure Status epilepticus
Potential Future studies
 Potential Future studies John P Betjemann, Daniel H Lowenstein, Status Epilepticus in adults The Lancet Neurology, Volume 14, Issue 6, 2015, 615 624 Add another treatment to midazolam AEDs available in
Potential Future studies John P Betjemann, Daniel H Lowenstein, Status Epilepticus in adults The Lancet Neurology, Volume 14, Issue 6, 2015, 615 624 Add another treatment to midazolam AEDs available in
Challenges In Treatment of NCSE NCSE. Definition 22/07/56
 Challenges In Treatment of NCSE Anannit Visudtibhan, MD. Division of Neurology, Department of Pediatrics, Faculty of Medicine-Ramathibodi Hospital NCSE Definition & Classification Diagnosis Issues in specific
Challenges In Treatment of NCSE Anannit Visudtibhan, MD. Division of Neurology, Department of Pediatrics, Faculty of Medicine-Ramathibodi Hospital NCSE Definition & Classification Diagnosis Issues in specific
Outline. What is a seizure? What is epilepsy? Updates in Seizure Management Terminology, Triage & Treatment
 Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium. Management of acute seizure settings from infancy to adolescence
 Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Seizure 18 (2009) Contents lists available at ScienceDirect. Seizure. journal homepage:
 Contents lists available at ScienceDirect. Seizure. journal homepage:") Seizure 18 (2009) 38 42 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Non-convulsive status epilepticus; the rate of occurrence in a general hospital
Seizure 18 (2009) 38 42 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Non-convulsive status epilepticus; the rate of occurrence in a general hospital
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
EEG workshop. Epileptiform abnormalities. Definitions. Dr. Suthida Yenjun
 EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Classification of Status Epilepticus: A New Proposal Dan Lowenstein, M.D. University of California, San Francisco
 Classification of Status Epilepticus: A New Proposal Dan Lowenstein, M.D. University of California, San Francisco for the ILAE Taskforce for Classification of Status Epilepticus: Eugen Trinka, Hannah Cock,
Classification of Status Epilepticus: A New Proposal Dan Lowenstein, M.D. University of California, San Francisco for the ILAE Taskforce for Classification of Status Epilepticus: Eugen Trinka, Hannah Cock,
Management of acute seizure and status epilepticus. Apisit Boongird, MD Division of Neurology Ramathibodi hospital
 Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi hospital Outlines Seizure cluster/ Acute repetitive seizures Status epilepticus Seizure cluster
Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi hospital Outlines Seizure cluster/ Acute repetitive seizures Status epilepticus Seizure cluster
Stop the Status: Improving Outcomes in Pediatric Epilepsy Syndromes. Michelle Welborn, PharmD ICE Alliance
 Stop the Status: Improving Outcomes in Pediatric Epilepsy Syndromes Michelle Welborn, PharmD ICE Alliance Overview Seizures and Epilepsy Syndromes Seizure Emergencies Febrile Seizures Critical Population
Stop the Status: Improving Outcomes in Pediatric Epilepsy Syndromes Michelle Welborn, PharmD ICE Alliance Overview Seizures and Epilepsy Syndromes Seizure Emergencies Febrile Seizures Critical Population
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Can t Stop the Seizing!
 Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Status epilepticus: news and perspectives
 Status epilepticus: news and perspectives LOREDANA LUCA MD, PHD EMERGENCY COUNTY HOSPITAL PIUS BRINZEU CLINIC OF ANAESTHESIA AND INTENSIVE CARE TIMISOARA, ROMANIA Objectives History Definition of status
Status epilepticus: news and perspectives LOREDANA LUCA MD, PHD EMERGENCY COUNTY HOSPITAL PIUS BRINZEU CLINIC OF ANAESTHESIA AND INTENSIVE CARE TIMISOARA, ROMANIA Objectives History Definition of status
Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination
 & ASEAN Neurological Association (ASNA) EEG Certification Examination") Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography
Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography
NEUROIMAGING IN EPILEPSY
 ASN ANNUAL MEETING: NEUROIMAGING FOR PRECISION MEDICINE AND HEALTH NEUROIMAGING IN EPILEPSY Gregory Kapinos, MD, MS, FASN Neurologist, Neurointensivist, ICU EEG specialist & Neuroimager Assistant Professor,
ASN ANNUAL MEETING: NEUROIMAGING FOR PRECISION MEDICINE AND HEALTH NEUROIMAGING IN EPILEPSY Gregory Kapinos, MD, MS, FASN Neurologist, Neurointensivist, ICU EEG specialist & Neuroimager Assistant Professor,
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Common EEG pattern in critical care
 Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016
 Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016 Outline Definition of status epilepticus Classification of status epilepticus Treatment of status
Treatment of Status Epilepticus SUDA JIRASAKULDEJ, MD KING CHULALONGKORN MEMORIAL HOSPITAL AUGUST 21, 2016 Outline Definition of status epilepticus Classification of status epilepticus Treatment of status
SAGE-547 for super-refractory status epilepticus
 NIHR Innovation Observatory Evidence Briefing: April 2017 SAGE-547 for super-refractory status epilepticus NIHRIO (HSRIC) ID: 10866 NICE ID: 8456 Status epilepticus is a single epileptic seizure lasting
NIHR Innovation Observatory Evidence Briefing: April 2017 SAGE-547 for super-refractory status epilepticus NIHRIO (HSRIC) ID: 10866 NICE ID: 8456 Status epilepticus is a single epileptic seizure lasting
WHOLE LOTTA SHAKIN GOIN ON
 WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
11/1/2018 STATUS EPILEPTICUS DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS. November is National Epilepsy Awareness Month
 STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Case report. Epileptic Disord 2005; 7 (1): 37-41
: 37-41") Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
ORIGINAL CONTRIBUTION. Frequency and Predictors of Nonconvulsive Seizures. continuous electroencephalographic
 ORIGINAL CONTRIBUTION Frequency and Predictors of Nonconvulsive Seizures During Continuous Electroencephalographic Monitoring in Critically Ill Children Nathalie Jette, MD, MSc; Jan Claassen, MD; Ronald
ORIGINAL CONTRIBUTION Frequency and Predictors of Nonconvulsive Seizures During Continuous Electroencephalographic Monitoring in Critically Ill Children Nathalie Jette, MD, MSc; Jan Claassen, MD; Ronald
8/27/2017. Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience. Definition SE. Definition SE. Epidemiology CSE. Classification of SE
 Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience Definition SE Traditional : Prolonged seizure lasting 30 mins or series of seizure without full recovery to baseline lasting 30 mins
Super-Refractory Status Epilepticus 2014 Pediatric Chula Experience Definition SE Traditional : Prolonged seizure lasting 30 mins or series of seizure without full recovery to baseline lasting 30 mins
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Epilepsy Currents and Pearls. Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento
 Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM
 ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
Asian Epilepsy Academy (ASEPA) EEG Certification Examination
 EEG Certification Examination") Asian Epilepsy Academy (ASEPA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography (EEG) in the Asian Oceanian region
Asian Epilepsy Academy (ASEPA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography (EEG) in the Asian Oceanian region
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Supplementary Online Content
 Supplementary Online Content Hocker SE, Britton JW, Mandrekar JN, Wijdicks EFM, Rabinstein AA. Predictors of outcome in refractory status epilepticus. Arch Neurol. Published online October 8, 2012. doi:10.1001/archneurol.2012.1697.
Supplementary Online Content Hocker SE, Britton JW, Mandrekar JN, Wijdicks EFM, Rabinstein AA. Predictors of outcome in refractory status epilepticus. Arch Neurol. Published online October 8, 2012. doi:10.1001/archneurol.2012.1697.
Post-anoxic status epilepticus and EEG patterns
 Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Is pentobarbital safe and efficacious in the treatment of super-refractory status epilepticus: a cohort study
 Pugin et al. Critical Care 2014, 18:R103 RESEARCH Open Access Is pentobarbital safe and efficacious in the treatment of super-refractory status epilepticus: a cohort study Deborah Pugin 1, Brandon Foreman
Pugin et al. Critical Care 2014, 18:R103 RESEARCH Open Access Is pentobarbital safe and efficacious in the treatment of super-refractory status epilepticus: a cohort study Deborah Pugin 1, Brandon Foreman
David Dredge, MD MGH Child Neurology CME Course September 9, 2017
 David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
NICIS Paris, June Review of Status epilepticus care
 NICIS Paris, June 19 2015 Review of Status epilepticus care Andrea O. Rossetti Département des Neurosciences Cliniques Lausanne, Switzerland Disclosure UCB pharma, SAGE Research support Several medications
NICIS Paris, June 19 2015 Review of Status epilepticus care Andrea O. Rossetti Département des Neurosciences Cliniques Lausanne, Switzerland Disclosure UCB pharma, SAGE Research support Several medications
Status Epilepticus. Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital. Pediatrics
 Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus
 Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
Talk outline. Some definitions. Emergency epilepsy now what? Recognising seizure types. Dr Richard Perry. Management of status epilepticus
 Emergency epilepsy now what? Dr Richard Perry Imperial College NHS Trust Imperial College Talk outline Recognising seizure types Management of status epilepticus Some definitions Epileptic seizure A clinical
Emergency epilepsy now what? Dr Richard Perry Imperial College NHS Trust Imperial College Talk outline Recognising seizure types Management of status epilepticus Some definitions Epileptic seizure A clinical
Tonic Upward Eyeball Deviation Mimicking Non-Convulsive Occipital Lobe Status Epilepticus That Was Induced by Hydrocephalus
 Min-Hee Woo, et al. Hydrocephalus Mimicking Status Epilepticus 49 Case Report Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Tonic Upward Eyeball Deviation Mimicking Non-Convulsive Occipital
Min-Hee Woo, et al. Hydrocephalus Mimicking Status Epilepticus 49 Case Report Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Tonic Upward Eyeball Deviation Mimicking Non-Convulsive Occipital
The Management of Refractory Status Epilepticus: An Update
 Epilepsia, 47(Suppl. 1):35 40, 2006 Blackwell Publishing, Inc. C International League Against Epilepsy The Management of Refractory Status Epilepticus: An Update Daniel H. Lowenstein Department of Neurology,
Epilepsia, 47(Suppl. 1):35 40, 2006 Blackwell Publishing, Inc. C International League Against Epilepsy The Management of Refractory Status Epilepticus: An Update Daniel H. Lowenstein Department of Neurology,
Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011
 Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011 Sudha Kilaru Kessler M.D. Assistant Professor of Neurology and Pediatrics Children s Hospital of Philadelphia University of Pennsylvania
Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011 Sudha Kilaru Kessler M.D. Assistant Professor of Neurology and Pediatrics Children s Hospital of Philadelphia University of Pennsylvania
02/08/53. ** Thanks you to. Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi
 ** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study
 http://escholarship.umassmed.edu/neurol_bull Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study Jane Louie and Jaishree Narayanan
http://escholarship.umassmed.edu/neurol_bull Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study Jane Louie and Jaishree Narayanan
0 56 BiPLEDS 3 (L:2, O:1), 9
, 9") Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
Proposed practical working definitions of NORSE, FIRES, related syndromes, and Status Epilepticus (SE) of different severities: consensus panel
 of different severities: consensus panel") Proposed practical working definitions of NORSE, FIRES, related syndromes, and Status Epilepticus (SE) of different severities: consensus panel 5 April 2017 Hotel Imlauer Salzburg Austria Objective To
Proposed practical working definitions of NORSE, FIRES, related syndromes, and Status Epilepticus (SE) of different severities: consensus panel 5 April 2017 Hotel Imlauer Salzburg Austria Objective To
Epilepsy and Epileptic Seizures
 Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
4/12/2016. Seizure description Basic EEG ICU monitoring Inpatient Monitoring Elective admission for continuous EEG monitoring Nursing s Role
 Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Scope. EEG patterns in Encephalopathy. Diffuse encephalopathy. EEG in adult patients with. EEG in diffuse encephalopathy
 Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
ADVERSE EVENT REPORTING. Catherine Dillon, CCRP
 ADVERSE EVENT REPORTING Catherine Dillon, CCRP Reporting Adverse Events Adverse Events (AEs) are... any untoward medical occurrence in a subject that was not previously identified which does not necessarily
ADVERSE EVENT REPORTING Catherine Dillon, CCRP Reporting Adverse Events Adverse Events (AEs) are... any untoward medical occurrence in a subject that was not previously identified which does not necessarily
Successful Use of Therapeutic Hypothermia for Refractory Nonconvulsive Status Epilepticus
 Successful Use of Therapeutic Hypothermia for Refractory Nonconvulsive Status Epilepticus Do-Hyung Kim 1, Hye-hoon Kang 1, Minjung Kim 1, Tae-Won Yang 2, Oh-Young Kwon 1, Jung Sook Yeom 3, Bong Su Kang
Successful Use of Therapeutic Hypothermia for Refractory Nonconvulsive Status Epilepticus Do-Hyung Kim 1, Hye-hoon Kang 1, Minjung Kim 1, Tae-Won Yang 2, Oh-Young Kwon 1, Jung Sook Yeom 3, Bong Su Kang
High-dose midazolam infusion for refractory status epilepticus
 High-dose midazolam infusion for refractory status epilepticus Andres Fernandez, MD Hector Lantigua, MD Christine Lesch, PharmD Belinda Shao, BA Brandon Foreman, MD J. Michael Schmidt, PhD Lawrence J.
High-dose midazolam infusion for refractory status epilepticus Andres Fernandez, MD Hector Lantigua, MD Christine Lesch, PharmD Belinda Shao, BA Brandon Foreman, MD J. Michael Schmidt, PhD Lawrence J.
Emergency Management of Paediatric Status Epilepticus. Dr. Maggie Yau Department of Paediatrics Prince of Wales Hospital
 Emergency Management of Paediatric Status Epilepticus Dr. Maggie Yau Department of Paediatrics Prince of Wales Hospital Definition (ILAE 2015) After t1 failure of the mechanisms responsible for seizure
Emergency Management of Paediatric Status Epilepticus Dr. Maggie Yau Department of Paediatrics Prince of Wales Hospital Definition (ILAE 2015) After t1 failure of the mechanisms responsible for seizure
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012
 Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
ESETT ELIGIBILITY OVERVIEW. James Chamberlain, MD
 ESETT ELIGIBILITY OVERVIEW James Chamberlain, MD Eligibility Age Convulsive Status Benzos Not excluded Eligibility Age 2 years to < 18 years (Pediatric) 18 years to 65 years (Adult) > 65 years (Geriatric)
ESETT ELIGIBILITY OVERVIEW James Chamberlain, MD Eligibility Age Convulsive Status Benzos Not excluded Eligibility Age 2 years to < 18 years (Pediatric) 18 years to 65 years (Adult) > 65 years (Geriatric)
Challenges in idiopathic/ genetic epilepsy syndromes
 Herlev and Gentofte Hospital Department of Pediatrics Indsæt h af objekt 1. Højrek vælg Gitt 2. Sæt kr tegnehjæ 3. Vælg O Challenges in idiopathic/ genetic epilepsy syndromes g Navn menuen Sidefod tår
Herlev and Gentofte Hospital Department of Pediatrics Indsæt h af objekt 1. Højrek vælg Gitt 2. Sæt kr tegnehjæ 3. Vælg O Challenges in idiopathic/ genetic epilepsy syndromes g Navn menuen Sidefod tår
Guidelines for the Evaluation and Management of Status Epilepticus
 Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy, Rodney Bell, Jan Claassen, Brian Alldredge, Thomas P. Bleck, Tracy Glauser, Suzette M. LaRoche, James J. Riviello,
Guidelines for the Evaluation and Management of Status Epilepticus Gretchen M. Brophy, Rodney Bell, Jan Claassen, Brian Alldredge, Thomas P. Bleck, Tracy Glauser, Suzette M. LaRoche, James J. Riviello,
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults. Contents
 Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
Status Epilepticus And Prolonged Seizures: Guideline For Management In Adults Classification: Clinical guideline Lead Author: Rajiv Mohanraj, Consultant Neurologist Additional author(s): Matt Jones, Consultant
2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg
 in adults and children > 40 kg") Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
Yale New Haven Health Department of Pharmacy, Department of Neurology 2016 Treatment Algorithm for Generalized Convulsive Status Epilepticus (SE) in adults and children > 40 kg Guideline, YNHHS Original
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
5/23/14. Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments
 Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
Febrile seizures: Who need further workup? Afebrile seizures: Who needs imaging? Status epilepticus: Most effective treatments Andi Marmor, MD, MSEd Associate Professor, Pediatrics University of California,
8/27/2017. Management of Status Epilepticus & Super-Refractory SE Definition SE. Definition SE. Epidemiology CSE. Classification of SE
 Management of Status Epilepticus & Super-Refractory SE 2017 TAYARD DESUDCHIT MD. HEAD, DIV. OF PED. NEUROLOGY FACULTY OF MEDICINE CHULALONGKORN U. Definition SE Traditional : Prolonged seizure lasting
Management of Status Epilepticus & Super-Refractory SE 2017 TAYARD DESUDCHIT MD. HEAD, DIV. OF PED. NEUROLOGY FACULTY OF MEDICINE CHULALONGKORN U. Definition SE Traditional : Prolonged seizure lasting
Response Rates to Anticonvulsant Trials in Patients with Triphasic-Wave EEG Patterns of Uncertain Significance
 Response Rates to Anticonvulsant Trials in Patients with Triphasic-Wave EEG Patterns of Uncertain Significance Deirdre O'Rourke, Massachusetts General Hospital Patrick M. Chen, Massachusetts General Hospital
Response Rates to Anticonvulsant Trials in Patients with Triphasic-Wave EEG Patterns of Uncertain Significance Deirdre O'Rourke, Massachusetts General Hospital Patrick M. Chen, Massachusetts General Hospital
ICU EEG Monitoring: When and Why
 ICU EEG Monitoring: When and Why Lawrence J. Hirsch, MD Professor of Clinical Neurology Director of Clinical Neurophysiology Neurological Institute Columbia University New York, New York Disclosures Name
ICU EEG Monitoring: When and Why Lawrence J. Hirsch, MD Professor of Clinical Neurology Director of Clinical Neurophysiology Neurological Institute Columbia University New York, New York Disclosures Name
Prescribing and Monitoring Anti-Epileptic Drugs
 Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Seizures Emergency Treatment
 Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Status Epilepticus in Children. Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech
 Status Epilepticus in Children Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech Status epilepticus (SE) presents in a multitude of forms, dependent on etiology and patient age
Status Epilepticus in Children Azhar Daoud Professor of Child Neurology Jordan Univ of science and Tech Status epilepticus (SE) presents in a multitude of forms, dependent on etiology and patient age
EEG in the ICU. Quiz. March Teneille E. Gofton
 EEG in the ICU Quiz March 2012 Teneille E. Gofton Quiz The next several slides will show 15 subhairline EEGs. Choose the best possible answer in each scenario. Your score and solutions will be provided
EEG in the ICU Quiz March 2012 Teneille E. Gofton Quiz The next several slides will show 15 subhairline EEGs. Choose the best possible answer in each scenario. Your score and solutions will be provided
The Theraputic Role of Hypothermia
 The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
The diagnostic dilemma of non-convulsive status epilepticus in sporadic Creutzfeldt-Jakob disease
 Journal of Epileptology 2017 25 53 58 10.1515/joepi-2017-0001 53 The diagnostic dilemma of non-convulsive status epilepticus in sporadic Creutzfeldt-Jakob disease Matthias Wittstock 1, Uwe Walter 1, Daniela
Journal of Epileptology 2017 25 53 58 10.1515/joepi-2017-0001 53 The diagnostic dilemma of non-convulsive status epilepticus in sporadic Creutzfeldt-Jakob disease Matthias Wittstock 1, Uwe Walter 1, Daniela
Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke
 in remote stroke") Original article Epileptic Disord 2007; 9 (2): 164-9 Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke José F. Téllez-Zenteno 1, Sylaja N. Pillai 2, Michael D. Hill 2, Neelan
Original article Epileptic Disord 2007; 9 (2): 164-9 Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke José F. Téllez-Zenteno 1, Sylaja N. Pillai 2, Michael D. Hill 2, Neelan
Management of Complex Febrile Seizures
 Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Management of Complex Febrile Seizures An 13 month old girl presents to the ED after having a shaking episode at home. Mom describes shaking of both arms and legs, lasting 20 minutes. The child has no
Presenter Disclosure
 Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Intracranial Studies Of Human Epilepsy In A Surgical Setting
 Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Status Epilepticus. G. Bryan Young, MD, FRCPC. Department of Clinical Neurological Sciences, University of Western Ontario, London, Ontario, Canada
 1 Status Epilepticus G. Bryan Young, MD, FRCPC Department of Clinical Neurological Sciences, University of Western Ontario, London, Ontario, Canada Contact information: Dr. G. B. Young, Room B10-106, University
1 Status Epilepticus G. Bryan Young, MD, FRCPC Department of Clinical Neurological Sciences, University of Western Ontario, London, Ontario, Canada Contact information: Dr. G. B. Young, Room B10-106, University
Refractory Status Elipticus
 Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
EEG WORKSHOP Nonepileptiform Abnormalities
 EEG WORKSHOP Nonepileptiform Abnormalities Kamornwan Katanyuwong MD Chiangmai University Hospital EST: 20th July 2010 EEG reading Age Background Epileptiform Non epileptiform Activation procedure normal
EEG WORKSHOP Nonepileptiform Abnormalities Kamornwan Katanyuwong MD Chiangmai University Hospital EST: 20th July 2010 EEG reading Age Background Epileptiform Non epileptiform Activation procedure normal
Status epilepticus (SE) is a condition that commonly
 is a condition that commonly") Status Epilepticus in the Pediatric Emergency Department Joshua Goldstein, MD Status epilepticus (SE) is a common childhood condition often seen by emergency physicians. It occurs at a frequency of between
Status Epilepticus in the Pediatric Emergency Department Joshua Goldstein, MD Status epilepticus (SE) is a common childhood condition often seen by emergency physicians. It occurs at a frequency of between
NMDOH digital library; keywords searched: pre-hospital, benzodiazepine, emergency medical technician, treatment of seizures, status epilepticus.
 Background Literature Review and Recommendations Administration of Benzodiazepines by EMT -I in the pre-hospital setting EMS Bureau Protocol Review Steering Committee Status epilepticus is a recognized
Background Literature Review and Recommendations Administration of Benzodiazepines by EMT -I in the pre-hospital setting EMS Bureau Protocol Review Steering Committee Status epilepticus is a recognized
Status epilepticus. Dr FL Chow
 Status epilepticus Dr FL Chow Terms Seizure paroxysmal event due to abnormal excessive neuronal activity in brain Epilepsy recurrent seizures due to chronic, underlying process; epilepsy syndromes Classification
Status epilepticus Dr FL Chow Terms Seizure paroxysmal event due to abnormal excessive neuronal activity in brain Epilepsy recurrent seizures due to chronic, underlying process; epilepsy syndromes Classification
Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity
 Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity Seizures in the School Setting Meghan Candee, MD MS Assistant
Measures have been taken, by the Utah Department of Health, Bureau of Health Promotions, to ensure no conflict of interest in this activity Seizures in the School Setting Meghan Candee, MD MS Assistant