The ictal interictal continuum
|
|
|
- Alexis Catherine Lee
- 6 years ago
- Views:
Transcription
, Irving Institute for Clinical and Translational")
1 The ictal interictal continuum Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY Disclosures: Research Support: Columbia University Clinical Translational Science Award (CTSA), Irving Institute for Clinical and Translational Research
2 Case history CC: 69 yo Woman p/w unresponsiveness PMHx: SAH s/p right MCA clipping 17 yrs prior to admission, LRE, HTN OSH ER: BP 210/11, HR 80, NIHSS 21, no commands, R eye did not doll, L did not cross midline, left hemiparesis Transferred for possible ia-tpa NICU: on arrival 2 nd GTC seizure, CTA normal, LP unremarkable Convulsions stopped with LRZ 6 mg fdph 1.5 gm but remained comatose


3 Emergent ceeg Loaded with Valproic Acid 30 mg/kg EEG post clinically successfully treated GCSE 20-48% electrographic seizures 14% NCSE Most without any clinical signs DeLorenzo Epil 1998, Treiman NEJM 1998
4 Seizures stopped but ceeg showed PLEDs plus: periodic discharges with superimposed rhythmic slowing No change in mental status

5 PLEDs plus: periodic discharges with superimposed rhythmic slowing Neuronal damage from ictal-interictal patterns? Chong & Hirsch, 2005 PLEDs- Plus

 may occur with PLEDs Snodgrass 1989, Baykan 2000,")
6 Are PEDs ictal? Pro Reversible confusional state akin to NCSE during PLEDs in the elderly Terzano 1986 Glc metabolism: local increase during PLEDs similar to seizure pattern on FDG-PET Handforth 1994 CBF: increase during PLEDs on SPECT, reversed with successful treatment Assal 2001; Bozkurt 2002 EPC (focal motor status epilepticus) may occur with PLEDs Snodgrass 1989, Baykan 2000, Kuroiwa 1980 Contra May have benign clinical courses with longstanding PEDs Chronic PLEDs Westmoreland 1986 or BIPLEDs Fushimi 2003
7 Ictal-interictal continuum and focal nonconvulsive seizures: Patient with encephalitis and RSE Irregular 2 Hz generalized periodic discharges superimposed on diffuse rhythmic 2 Hz delta activity. GPDs-plus = ictal-interictal continuum


8 Ictal-interictal continuum and focal nonconvulsive seizures: Patient with encephalitis and RSE NCSZ from left posterior Irregular 2 Hz generalized periodic discharges superimposed on diffuse rhythmic 2 Hz delta activity. GPDs-plus = ictal-interictal continuum NCSZ from right temporal
9 What do PEDs mean? Controversial if PEDs ictal but definitely predictors of electrographic seizures Predictors of electrographic seizures: Coma on exam: 56% of comatose pts vs. 12% Young age: 36% of pts <18 yo vs. 17% of pts > 18. Epilepsy in the past medical history: 41% vs. 16%, or remote risk factors for szs Convulsive seizures prior to monitoring: 43% of pts with vs. 12% Periodic discharges (PLEDs or GPEDs) or Suppression-burst Oculomotor abnl s: nystag, hippus or eye deviation Cardiac or respiratory arrest Sepsis Varelas Neurology 2003; Husain JNNP 2003, Claassen 2004; Oddo CCM 2009 Incidence of seizures in the acute setting of PLEDs 58% to 100% Pohlmann-Eden et al., 1996
10 PEDs and seizures Claassen, Neurology 2004



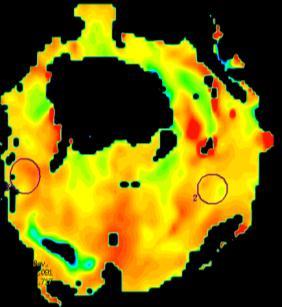
11 Technetium- 99m-HMAPO SPECT: R TL increased blood flow PLEDs plus: periodic discharges with superimposed rhythmic slowing


12 Ictal 99mHMPAO SPECT: Prolonged focal SE that progressed to PLEDs SPECT during and after PLEDs in alcoholic patient post GTC seizure Donaire JNNP 2006 Assal 2001

13 Levetiracetam 1000 mg BID AED serum levels: VPA 114 ug/ml, DPH 14 ug/ml, free DPH 3.1 ug/ml EEG: isolated epileptiform discharges Mental status improved slowly, discharged to subacute rehab 2 wks after presentation on DPH, VPA, and LEV
14 Done! Successful rehabilitation: she was tapered off all AEDs for a secondary cognitive deterioration and returned to her neurological baseline Happy ending, but


15 One month later presented to OSH with recurrent CPSE Restarted DPH, LEV, VPA but unresponsive NCSE Midazolam load of 14 mg and drip up to 0.4 mg/kg/hr


16 EEG on midazolam gtt PLEDs plus: with superimposed rhythmic slowing and fast activity





")





17 MRI during the ictal interictal continuum: restricted diffusion, increased CBF & CBV, decreased mean transit time (MTT) DWI: restricted diffusion R TL MTT CBF CBV ADC: minimal changes MDZ gtt 1 mg/kg/hr VPA (goal level ug/ml)




18 DWI ADC Imaging ictal patterns Decrease ADC/increased DWI after CPSE & seizures Hippocampal formation Cortical areas adjacent to the primary pathology Posterior part/pulvinar of the thalamus Szabo 2005, Kim 2001, Farina 2004 MR perfusion: increased perfusion in region of decreased diffusion Szabo 2005 Initial DWI shows diffuse, gyriform cortical hyperintensities Lansberg 99 5 months later diffuse low signal intensities ASL Detre 1996 Chu 01


19 Suppression burst Wean off MDZ without recurrent seizures. PLEDs persisted for almost 2 wks.














20 MRI during the ictal interictal continuum: almost complete resolution of the previously noted changes DWI MTT CBF CBV ADC
21 Benzodiazepine Trial for the Diagnosis of Non-Convulsive Status Epilepticus. Monitoring: EEG, pulse ox, BP, ECG, respiratory rate, with dedicated nurse. Antiepileptic Drug Trial: Sequential small doses of rapidly-acting short-duration benzodiazepine such as midazolam at 1mg/dose. Between doses, repeated clinical and EEG assessment. Trial is stopped after any of the following: o Persistent resolution of the EEG pattern (and exam repeated) o Definite clinical improvement o Respiratory depression, hypotension, or other adverse effect o A maximum dose is reached (such as 0.2 mg/kg midazolam, though higher may be needed if on chronic benzodiazepines) o Test is considered positive if there is resolution of the potentially ictal EEG pattern AND either an improvement in the clinical state or the appearance of previously-absent normal EEG patterns (eg. posterior dominant alpha rhythm). If EEG improves but patient does not, the result is equivocal.
22 Due to thrombocytopenia VPA stopped Recurrence of NCSE -> Phenobarbital started Neuro: encephalopathic While weaning phenobarbital started on LTG Left > right facial twitching developed with PLEDs proper Benzodiazepine trial: 1 mg midazolam repeated doses of (total of 4 mg) -> facial twitching resolved and PLEDs gone but otherwise no neuro improvement = Equivocal Serial NSE levels throughout hospital course did not correlate with EEG activity








23 FDG-PET: decreased metabolism in the right temporal lobe Phenobarbital discontinued. Discharged to NH 1 month after admission on TPM, DPH, and LEV
24 Outcome: 2 months after discharge continuing to improve in an active rehabilitation program Interactive able to recognize family members moves all four extremities mobilized to a chair undergoing ventilator weaning
25 Criteria for Nonconvulsive Seizure Any pattern lasting > 10 secs satisfying any one of these 3 primary criteria: Primary Criteria: 1. Repetitive generalized or focal spikes, sharp-waves, spike-and-wave or sharp-and-slow wave complexes at >3/sec 2. Repetitive generalized or focal spikes, sharp waves, spike-and-wave or sharp-and-slow wave complexes at <3/sec and secondary criterion 3. Sequential rhythmic, periodic, or quasi-periodic waves at > 1/sec and unequivocal evolution in frequency (gradually increasing or decreasing by at least 1/sec, e.g. from 2 to 3/sec), morphology, or location (gradual spread into or out of a region involving at least 2 electrodes). Evolution in amplitude alone not sufficient Change in sharpness without other change in morphology not adequate Secondary criterion: After administration of a rapidly-acting AED: Significant improvement in clinical state or appearance of previously-absent normal EEG patterns (such as a posterior dominant rhythm) Not satisfactory: resolution of the epileptiform discharges leaving diffuse slowing without clinical improvement and without appearance of previouslyabsent normal EEG patterns Chong et al, 2005 modification of Young et al 1996
26 Strategies to support treatment decisions for patients in the ictal-interictal continuum: determine similarities to seizures 1. EEG signature: Classify into PLEDs plus (low amplitude rhythmic discharge ) and PLEDs proper (Reiher 91) 2. Physiologic measurements Benzodiazepine trial CBF and CBV (SPECT, CT perfusion, MR perfusion imaging, arterial spin labeling) Cerebral metabolism (PET scanning) Multimodality monitoring (PbtO2, hemodex for CBF, microdialysis for glutamate and GABA) 3. Quantify neuronal injury Imaging studies (ADC, MR spectroscopy) Serum markers (neuron specific enolase) Microdialysis endpoints (LPR, glycerol)
27 Practical approach to patients with PEDs: 1. Investigate the cause: this may be guided by specific PED pattern (history, MRI, CSF, angio, brain biopsy) 2. Conventional AED prophylaxis for seizures: Levetiracetam (alternatives: oxcarbazepine, CBZ, DPH, VPA, TPM, GBP); at this point should not use civ AEDs for PEDs without seizures 3. May do benzo trial to determine ictal nature 4. Continue ceeg monitoring for potential nonconvulsive seizures or status epilepticus. 5. Long-term treatment: individualize based on other EEG findings (e.g. epil discharges) and underlying brain injury Acute PLEDs that resolved without seizures -> taper AEDs/one month after acute illness. Acute PLEDs with seizures: AED treatment for 3-12 months Consider DPH, phenobarbital, and benzos may adversely affect motor recovery after stroke (Camilo and Goldstein, 2004).


28 SIRPIDs: Stimulus-Induced Rhythmic, Periodic or Ictal Discharges Staff enter s Sti m Prevalence: 22% (33/150) consecutive ceeg patients Hirsch Epilepsia 2004 and 2007
29 Acknowledgements Depart. of Biomedical Informatics Adler Perotte, MD Samantha Kleinberg, PhD David Albers, PhD George Hripcsak, MD, MS Division Critical Care Neurology J Michael Schmidt, PhD Stephan A. Mayer, MD NICU Fellows NICU nurses Neurology residents Department of Neurosurgery E Sander Connolly, MD Neurosurgery residents Comprehensive Epilepsy Center Bin Tu, MD EEG Technicians Epilepsy attendings Epilepsy fellows
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Electroencephalography. Role of EEG in NCSE. Continuous EEG in ICU 25/05/59. EEG pattern in status epilepticus
 EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
EEG workshop. Epileptiform abnormalities. Definitions. Dr. Suthida Yenjun
 EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
EEG workshop Epileptiform abnormalities Paroxysmal EEG activities ( focal or generalized) are often termed epileptiform activities EEG hallmark of epilepsy Dr. Suthida Yenjun Epileptiform abnormalities
Mapping of the brain in unconscious patients Quantitative EEG
 Mapping of the brain in unconscious patients Quantitative EEG Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures:
Mapping of the brain in unconscious patients Quantitative EEG Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures:
Case report. Epileptic Disord 2005; 7 (1): 37-41
: 37-41") Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Status Epilepticus: The good, the bad, the ugly
 Status Epilepticus: The good, the bad, the ugly Emily J. Gilmore, MD, MS Assistant Professor Division of Neurocritical Care and Emergency Neurology, and Epilepsy (CCEEG) Yale New Haven Hospital/Yale School
Status Epilepticus: The good, the bad, the ugly Emily J. Gilmore, MD, MS Assistant Professor Division of Neurocritical Care and Emergency Neurology, and Epilepsy (CCEEG) Yale New Haven Hospital/Yale School
Continuous EEG: A Standard in Canada?
 Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
Continuous EEG: A Standard in Canada? Victoria McCredie MBChB Neurointensivist Sunnybrook Health Sciences Centre Critical Care Canada Forum 28 th October 2015 No conflicts of interest to disclose. Outline
Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study
 http://escholarship.umassmed.edu/neurol_bull Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study Jane Louie and Jaishree Narayanan
http://escholarship.umassmed.edu/neurol_bull Does Neurological Examination Change With Resolution of PLEDs on EEG in Non-Anoxic Patients: A Prospective Observational Study Jane Louie and Jaishree Narayanan
02/08/53. ** Thanks you to. Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi
 ** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
ICU EEG Monitoring: When and Why
 ICU EEG Monitoring: When and Why Lawrence J. Hirsch, MD Professor of Clinical Neurology Director of Clinical Neurophysiology Neurological Institute Columbia University New York, New York Disclosures Name
ICU EEG Monitoring: When and Why Lawrence J. Hirsch, MD Professor of Clinical Neurology Director of Clinical Neurophysiology Neurological Institute Columbia University New York, New York Disclosures Name
Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke
 in remote stroke") Original article Epileptic Disord 2007; 9 (2): 164-9 Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke José F. Téllez-Zenteno 1, Sylaja N. Pillai 2, Michael D. Hill 2, Neelan
Original article Epileptic Disord 2007; 9 (2): 164-9 Chronic PLEDs with transitional rhythmic discharges (PLEDs-plus) in remote stroke José F. Téllez-Zenteno 1, Sylaja N. Pillai 2, Michael D. Hill 2, Neelan
Generalized seizures, generalized spike-waves and other things. Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke
 Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
NEUROIMAGING IN EPILEPSY
 ASN ANNUAL MEETING: NEUROIMAGING FOR PRECISION MEDICINE AND HEALTH NEUROIMAGING IN EPILEPSY Gregory Kapinos, MD, MS, FASN Neurologist, Neurointensivist, ICU EEG specialist & Neuroimager Assistant Professor,
ASN ANNUAL MEETING: NEUROIMAGING FOR PRECISION MEDICINE AND HEALTH NEUROIMAGING IN EPILEPSY Gregory Kapinos, MD, MS, FASN Neurologist, Neurointensivist, ICU EEG specialist & Neuroimager Assistant Professor,
Common EEG pattern in critical care
 Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
0 56 BiPLEDS 3 (L:2, O:1), 9
, 9") Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
Seizure 18 (2009) Contents lists available at ScienceDirect. Seizure. journal homepage:
 Contents lists available at ScienceDirect. Seizure. journal homepage:") Seizure 18 (2009) 38 42 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Non-convulsive status epilepticus; the rate of occurrence in a general hospital
Seizure 18 (2009) 38 42 Contents lists available at ScienceDirect Seizure journal homepage: www.elsevier.com/locate/yseiz Non-convulsive status epilepticus; the rate of occurrence in a general hospital
Outline. What is a seizure? What is epilepsy? Updates in Seizure Management Terminology, Triage & Treatment
 Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Outline Updates in Seizure Management Terminology, Triage & Treatment Joseph Sullivan, MD! Terminology! Videos of different types of seizures! Diagnostic evaluation! Treatment options! Acute! Maintenance
Scope. EEG patterns in Encephalopathy. Diffuse encephalopathy. EEG in adult patients with. EEG in diffuse encephalopathy
 Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
EEG IN FOCAL ENCEPHALOPATHIES: CEREBROVASCULAR DISEASE, NEOPLASMS, AND INFECTIONS
 246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
246 Figure 8.7: FIRDA. The patient has a history of nonspecific cognitive decline and multiple small WM changes on imaging. oligodendrocytic tumors of the cerebral hemispheres (11,12). Electroencephalogram
ORIGINAL CONTRIBUTION. Frequency and Predictors of Nonconvulsive Seizures. continuous electroencephalographic
 ORIGINAL CONTRIBUTION Frequency and Predictors of Nonconvulsive Seizures During Continuous Electroencephalographic Monitoring in Critically Ill Children Nathalie Jette, MD, MSc; Jan Claassen, MD; Ronald
ORIGINAL CONTRIBUTION Frequency and Predictors of Nonconvulsive Seizures During Continuous Electroencephalographic Monitoring in Critically Ill Children Nathalie Jette, MD, MSc; Jan Claassen, MD; Ronald
Complex partial status epilepticus is an unrecognised feature in SESA syndrome: new insights into its pathophysiology
 Original article Epileptic Disord 2007; 9 (2): 134-9 Complex partial status epilepticus is an unrecognised feature in SESA syndrome: new insights into its pathophysiology José L. Fernández-Torre 1, José
Original article Epileptic Disord 2007; 9 (2): 134-9 Complex partial status epilepticus is an unrecognised feature in SESA syndrome: new insights into its pathophysiology José L. Fernández-Torre 1, José
Status epilepticus: news and perspectives
 Status epilepticus: news and perspectives LOREDANA LUCA MD, PHD EMERGENCY COUNTY HOSPITAL PIUS BRINZEU CLINIC OF ANAESTHESIA AND INTENSIVE CARE TIMISOARA, ROMANIA Objectives History Definition of status
Status epilepticus: news and perspectives LOREDANA LUCA MD, PHD EMERGENCY COUNTY HOSPITAL PIUS BRINZEU CLINIC OF ANAESTHESIA AND INTENSIVE CARE TIMISOARA, ROMANIA Objectives History Definition of status
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Nonconvulsive status epilepticus (NCSE) is defined as prolonged or recurrent
 is defined as prolonged or recurrent") Nonconvulsive status epilepticus (NCSE) is defined as prolonged or recurrent electrographic seizure activity lasting more than 30 minutes without prominent motor (i.e. convulsive) clinical symptoms. 1
Nonconvulsive status epilepticus (NCSE) is defined as prolonged or recurrent electrographic seizure activity lasting more than 30 minutes without prominent motor (i.e. convulsive) clinical symptoms. 1
CHAIR SUMMIT 7TH ANNUAL #CHAIR2014. Master Class for Neuroscience Professional Development. September 11 13, Westin Tampa Harbour Island
 #CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Clinical Case Challenge: Seizure Emergency
#CHAIR2014 7TH ANNUAL CHAIR SUMMIT Master Class for Neuroscience Professional Development September 11 13, 2014 Westin Tampa Harbour Island Sponsored by #CHAIR2014 Clinical Case Challenge: Seizure Emergency
Periodic lateralized epileptiform discharges: association with seizures
 Seizure 2000; 9: 402 406 doi: 10.1053/seiz.2000.0435, available online at http://www.idealibrary.com on Periodic lateralized epileptiform discharges: association with seizures BETÜL BAYKAN, DEMET KINAY,
Seizure 2000; 9: 402 406 doi: 10.1053/seiz.2000.0435, available online at http://www.idealibrary.com on Periodic lateralized epileptiform discharges: association with seizures BETÜL BAYKAN, DEMET KINAY,
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology
 A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
The Theraputic Role of Hypothermia
 The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
4/12/2016. Seizure description Basic EEG ICU monitoring Inpatient Monitoring Elective admission for continuous EEG monitoring Nursing s Role
 Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Challenges In Treatment of NCSE NCSE. Definition 22/07/56
 Challenges In Treatment of NCSE Anannit Visudtibhan, MD. Division of Neurology, Department of Pediatrics, Faculty of Medicine-Ramathibodi Hospital NCSE Definition & Classification Diagnosis Issues in specific
Challenges In Treatment of NCSE Anannit Visudtibhan, MD. Division of Neurology, Department of Pediatrics, Faculty of Medicine-Ramathibodi Hospital NCSE Definition & Classification Diagnosis Issues in specific
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus
 Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
9/18/16. Setting: Community ED, 30k admissions per year Time: Friday night, 11pm. CC: Syncope
 William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
William A. Knight IV MD, FACEP Associate Professor Emergency Medicine & Neurosurgery University of Cincinnati September 21, 2016 (William.knight@uc.edu) ED as the Front Door Spectrum of care with Endovascular
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
give lorazepam Page 1 UC SF First known description of status epilepticus (Sakikku cuneiform, ca. 700 B.C) NEUROCRITICAL CARE PROGRAM
 NEUROCRITICAL CARE PROGRAM") Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
Update on Neurocritical Care J. Claude Hemphill III, MD, MAS Special Thanks to: Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University Disclosures Research Support: NIH/NINDS Stock
Disclosures 2/10/2017. RAIN 2017 Difficult Cases Session. Patient MC, Original Diagnosis, 9/2006. MRI 9/5/06, pre-op
 Disclosures RAIN 2017 Difficult Cases Session Clinical trials research funding support from: Novartis Genentech/Roche Merck NEUROLOGY AND NEUROLOGICAL SURGERY Jennifer L. Clarke, MD, MPH Associate Professor
Disclosures RAIN 2017 Difficult Cases Session Clinical trials research funding support from: Novartis Genentech/Roche Merck NEUROLOGY AND NEUROLOGICAL SURGERY Jennifer L. Clarke, MD, MPH Associate Professor
The EEG in focal epilepsy. Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center
 The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI)
") Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI) Poster No.: C-1086 Congress: ECR 014 Type: Scientific Exhibit Authors: J. AELLEN, E. Abela, R. Kottke, E. Springer,
Hemodynamic patterns of status epilepticus detected by susceptibility weighted imaging (SWI) Poster No.: C-1086 Congress: ECR 014 Type: Scientific Exhibit Authors: J. AELLEN, E. Abela, R. Kottke, E. Springer,
ESETT OUTCOMES. Investigator Kick-off Meeting Robert Silbergleit, MD
 ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
ESETT OUTCOMES Investigator Kick-off Meeting Robert Silbergleit, MD Primary objective The primary objective is to determine the most effective and/or the least effective treatment of benzodiazepinerefractory
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Medically Refractory Epilepsy with a Temporal Lobe Lesion Steven Ellis, MD Neurophysiology Fellow, PGY-5 UT Health San Antonio History No history of febrile seizures, meningitis, encephalitis, or head
Medically Refractory Epilepsy with a Temporal Lobe Lesion Steven Ellis, MD Neurophysiology Fellow, PGY-5 UT Health San Antonio History No history of febrile seizures, meningitis, encephalitis, or head
Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain Tumors
 Neurocrit Care (2012) 16:109 113 DOI 10.1007/s12028-011-9626-4 ORIGINAL ARTICLE Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain
Neurocrit Care (2012) 16:109 113 DOI 10.1007/s12028-011-9626-4 ORIGINAL ARTICLE Phenytoin, Levetiracetam, and Pregabalin in the Acute Management of Refractory Status Epilepticus in Patients with Brain
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
9/16/2018. Recognizing & Managing Seizures in Pediatric TBI. Objectives. Definitions and Epidemiology
 Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Recognizing & Managing Seizures in Pediatric TBI UW Medicine EMS & Trauma 2018 Conference September 17 and 18, 2018 Mark Wainwright MD PhD Herman and Faye Sarkowsky Professor of Neurology Division Head,
Post-anoxic status epilepticus and EEG patterns
 Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
B(I)RD Watching: A Way to Stratify Seizure Risk?
RD Watching: A Way to Stratify Seizure Risk?") B(I)RD Watching: A Way to Stratify Seizure Risk? Current Literature In Clinical Science Brief Potentially Ictal Rhythmic Discharges in Critically Ill Adults. Yoo JY, Rampal N, Petroff OA, Hirsch LJ, Gaspard
B(I)RD Watching: A Way to Stratify Seizure Risk? Current Literature In Clinical Science Brief Potentially Ictal Rhythmic Discharges in Critically Ill Adults. Yoo JY, Rampal N, Petroff OA, Hirsch LJ, Gaspard
Idiopathic epilepsy syndromes
 1 Idiopathic epilepsy syndromes PANISRA SUDACHAN, M.D. Pe diatric Neuro lo gis t Pediatric Neurology Department Pras at Neuro lo gic al Institute Epilepsy course 20 August 2016 Classification 2 1964 1970
1 Idiopathic epilepsy syndromes PANISRA SUDACHAN, M.D. Pe diatric Neuro lo gis t Pediatric Neurology Department Pras at Neuro lo gic al Institute Epilepsy course 20 August 2016 Classification 2 1964 1970
Cardiac and Autonomic Functions in Epilepsy
 Cardiac and Autonomic Functions in Epilepsy June 23 rd, 2012 Stephan Schuele, MD, MPH Northwestern University, Feinberg School of Medicine Northwestern Memorial Hospital Partners Against Mortality in Epilepsy
Cardiac and Autonomic Functions in Epilepsy June 23 rd, 2012 Stephan Schuele, MD, MPH Northwestern University, Feinberg School of Medicine Northwestern Memorial Hospital Partners Against Mortality in Epilepsy
EEG in the ICU. Quiz. March Teneille E. Gofton
 EEG in the ICU Quiz March 2012 Teneille E. Gofton Quiz The next several slides will show 15 subhairline EEGs. Choose the best possible answer in each scenario. Your score and solutions will be provided
EEG in the ICU Quiz March 2012 Teneille E. Gofton Quiz The next several slides will show 15 subhairline EEGs. Choose the best possible answer in each scenario. Your score and solutions will be provided
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Presenter Disclosure
 Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Potential Future studies
 Potential Future studies John P Betjemann, Daniel H Lowenstein, Status Epilepticus in adults The Lancet Neurology, Volume 14, Issue 6, 2015, 615 624 Add another treatment to midazolam AEDs available in
Potential Future studies John P Betjemann, Daniel H Lowenstein, Status Epilepticus in adults The Lancet Neurology, Volume 14, Issue 6, 2015, 615 624 Add another treatment to midazolam AEDs available in
Case #1. Inter-ictal EEG. Difficult Diagnosis Pediatrics. 15 mos girl with medically refractory infantile spasms 2/13/2010
 Difficult Diagnosis Pediatrics Joseph E. Sullivan M.D. Assistant Professor of Clinical Neurology & Pediatrics Director, UCSF Pediatric Epilepsy Center University of California San Francisco Case #1 15
Difficult Diagnosis Pediatrics Joseph E. Sullivan M.D. Assistant Professor of Clinical Neurology & Pediatrics Director, UCSF Pediatric Epilepsy Center University of California San Francisco Case #1 15
Case reports functional imaging in epilepsy
 Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Antiepileptic treatment for anti-nmda receptor encephalitis: the need for video-eeg monitoring
 Clinical commentary with video sequences Epileptic Disord 2013; 15 (2): 166-70 Antiepileptic treatment for anti-nmda receptor encephalitis: the need for video-eeg monitoring Nese Dericioglu, Atay Vural,
Clinical commentary with video sequences Epileptic Disord 2013; 15 (2): 166-70 Antiepileptic treatment for anti-nmda receptor encephalitis: the need for video-eeg monitoring Nese Dericioglu, Atay Vural,
Metabolic Correlates of the Ictal-Interictal Continuum: FDG-PET During Continuous EEG
 Neurocrit Care (2016) 24:324 331 DOI 10.1007/s12028-016-0245-y ORIGINAL ARTICLE Metabolic Correlates of the Ictal-Interictal Continuum: FDG-PET During Continuous EEG Aaron F. Struck 1 M. Brandon Westover
Neurocrit Care (2016) 24:324 331 DOI 10.1007/s12028-016-0245-y ORIGINAL ARTICLE Metabolic Correlates of the Ictal-Interictal Continuum: FDG-PET During Continuous EEG Aaron F. Struck 1 M. Brandon Westover
Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination
 & ASEAN Neurological Association (ASNA) EEG Certification Examination") Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography
Asian Epilepsy Academy (ASEPA) & ASEAN Neurological Association (ASNA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography
Status Epilepticus: A refresher. Objectives
 Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Acute Management of Seizures
 Acute Management of Seizures KURT HECOX M.D. PH.D. CHIEF OF PEDIATRIC NEUROLOGY BAUMAN ENDOWED CHAIR IN PEDIATRIC EPILEPSY Outline Management Principles Categorizing the event Key elements to the history
Acute Management of Seizures KURT HECOX M.D. PH.D. CHIEF OF PEDIATRIC NEUROLOGY BAUMAN ENDOWED CHAIR IN PEDIATRIC EPILEPSY Outline Management Principles Categorizing the event Key elements to the history
Developmental Changes Including Neonatal EEG. Gregory L. Holmes, MD
 Developmental Changes Including Neonatal EEG Gregory L. Holmes, MD A A + B =: B + A.Dravet Syndrome B.Menkes syndrome C.West syndrome D.Ohtahara shyndrome The Difficult Delivery 1 day old male transferred
Developmental Changes Including Neonatal EEG Gregory L. Holmes, MD A A + B =: B + A.Dravet Syndrome B.Menkes syndrome C.West syndrome D.Ohtahara shyndrome The Difficult Delivery 1 day old male transferred
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
True Epileptiform Patterns (and some others)
") True Epileptiform Patterns (and some others) a) What is epileptiform b) Some possible surprises c) Classification of generalized epileptiform patterns An epileptiform pattern Interpretative term based
True Epileptiform Patterns (and some others) a) What is epileptiform b) Some possible surprises c) Classification of generalized epileptiform patterns An epileptiform pattern Interpretative term based
Non epileptiform abnormality J U LY 2 7,
 Non epileptiform abnormality S U D A J I R A S A K U L D E J, M D. C H U L A L O N G KO R N C O M P R E H E N S I V E E P I L E P S Y C E N T E R J U LY 2 7, 2 0 1 6 Outline Slow pattern Focal slowing
Non epileptiform abnormality S U D A J I R A S A K U L D E J, M D. C H U L A L O N G KO R N C O M P R E H E N S I V E E P I L E P S Y C E N T E R J U LY 2 7, 2 0 1 6 Outline Slow pattern Focal slowing
Management of acute seizure and status epilepticus
 Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi Hospital Sunday August 27 10.00-10.45 Bangsan Objectives Acute repetitive seizure Status epilepticus
Management of acute seizure and status epilepticus Apisit Boongird, MD Division of Neurology Ramathibodi Hospital Sunday August 27 10.00-10.45 Bangsan Objectives Acute repetitive seizure Status epilepticus
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Introduction to EEG del Campo. Introduction to EEG. J.C. Martin del Campo, MD, FRCP University Health Network Toronto, Canada
 Introduction to EEG J.C. Martin, MD, FRCP University Health Network Toronto, Canada What is EEG? A graphic representation of the difference in voltage between two different cerebral locations plotted over
Introduction to EEG J.C. Martin, MD, FRCP University Health Network Toronto, Canada What is EEG? A graphic representation of the difference in voltage between two different cerebral locations plotted over
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Classification of Seizures. Generalized Epilepsies. Classification of Seizures. Classification of Seizures. Bassel F. Shneker
 Classification of Seizures Generalized Epilepsies Bassel F. Shneker Traditionally divided into grand mal and petit mal seizures ILAE classification of epileptic seizures in 1981 based on clinical observation
Classification of Seizures Generalized Epilepsies Bassel F. Shneker Traditionally divided into grand mal and petit mal seizures ILAE classification of epileptic seizures in 1981 based on clinical observation
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity
 Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Advanced Neuroimaging for Acute Stroke
 Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
Advanced Neuroimaging for Acute Stroke E. Bradshaw Bunney, MD, FACEP Professor Department Of Emergency Medicine University of Illinois at Chicago Swedish American Belvidere Hospital Disclosures FERNE Board
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM
 ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
Asian Epilepsy Academy (ASEPA) EEG Certification Examination
 EEG Certification Examination") Asian Epilepsy Academy (ASEPA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography (EEG) in the Asian Oceanian region
Asian Epilepsy Academy (ASEPA) EEG Certification Examination EEG Certification Examination Aims To set and improve the standard of practice of Electroencephalography (EEG) in the Asian Oceanian region
Disclosures. What is Status Epilepticus? Purpose of Today s Discussion. Nothing to Disclose. How do I recognize Status Epilepticus?
 Disclosures Nothing to Disclose Neurologic Emergencies SID W. ATKINSON MD Chief, Division of Child Neurology, and Developmental Pediatrics Purpose of Today s Discussion Understand 2 Neurologic Emergencies
Disclosures Nothing to Disclose Neurologic Emergencies SID W. ATKINSON MD Chief, Division of Child Neurology, and Developmental Pediatrics Purpose of Today s Discussion Understand 2 Neurologic Emergencies
CASE REPORT. Abstract. Introduction. Case Report. Masato Kadoya, Hiroyuki Onoue, Akiko Kadoya, Katsunori Ikewaki and Kenichi Kaida
 CASE REPORT Refractory Status Epilepticus Caused by Anti-NMDA Receptor Encephalitis that Markedly Improved Following Combination Therapy with Rituximab and Cyclophosphamide Masato Kadoya, Hiroyuki Onoue,
CASE REPORT Refractory Status Epilepticus Caused by Anti-NMDA Receptor Encephalitis that Markedly Improved Following Combination Therapy with Rituximab and Cyclophosphamide Masato Kadoya, Hiroyuki Onoue,
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
Seizures Seizures & Status Epilepticus Seizures are episodes of disturbed brain activity that cause changes in attention or behavior. Donna Lindsay, MN RN, CNS-BC, CCRN, CNRN Neuroscience Clinical Nurse
ENCEPHALOPATHY RECOGNIZING METABOLIC AND ANOXIC CHANGES
 ENCEPHALOPATHY RECOGNIZING METABOLIC AND ANOXIC CHANGES ENCEPHALOPATHY Encephalopathy is a general term that means brain disease, damage, or malfunction. The major symptom of encephalopathy is an altered
ENCEPHALOPATHY RECOGNIZING METABOLIC AND ANOXIC CHANGES ENCEPHALOPATHY Encephalopathy is a general term that means brain disease, damage, or malfunction. The major symptom of encephalopathy is an altered
Beyond the Basics in EEG Interpretation: Throughout the Life Stages
 Beyond the Basics in EEG Interpretation: Throughout the Life Stages Steve S. Chung, MD, FAAN Chairman, Neuroscience Institute Director, Epilepsy Program Banner University Medical Center University of Arizona
Beyond the Basics in EEG Interpretation: Throughout the Life Stages Steve S. Chung, MD, FAAN Chairman, Neuroscience Institute Director, Epilepsy Program Banner University Medical Center University of Arizona
Epilepsy Currents and Pearls. Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento
 Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Epilepsy Currents and Pearls Eniko Nagy-Wilde, MD Medical Director of Epilepsy and Clinical Neurophysiology Sutter Medical Center, Sacramento No disclosures Presenter Disclosure Information Learning Objectives
Status Epilepticus. Ednea Simon, MD Swedish Pediatric Neuroscience Center
 Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
Status Epilepticus Ednea Simon, MD Swedish Pediatric Neuroscience Center 1 Status Epilepticus Status epilepticus (SE) is a condition resulting either from failure of the mechanisms responsible for seizure
Sleep in Epilepsy. Kurupath Radhakrishnan,
 Sleep in Epilepsy Kurupath Radhakrishnan, Retired Senior Professor (Emeritus), R. Madavan Nayar Center for Comprehensive Epilepsy Care, Retired Director, Sree Chitra Tirunal Institute for Medical Sciences
Sleep in Epilepsy Kurupath Radhakrishnan, Retired Senior Professor (Emeritus), R. Madavan Nayar Center for Comprehensive Epilepsy Care, Retired Director, Sree Chitra Tirunal Institute for Medical Sciences
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES. Mr. Johnson. Seizures at 29 Years of Age. Dileep Nair, MD Juan Bulacio, MD
 Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
EEG WORKSHOP Nonepileptiform Abnormalities
 EEG WORKSHOP Nonepileptiform Abnormalities Kamornwan Katanyuwong MD Chiangmai University Hospital EST: 20th July 2010 EEG reading Age Background Epileptiform Non epileptiform Activation procedure normal
EEG WORKSHOP Nonepileptiform Abnormalities Kamornwan Katanyuwong MD Chiangmai University Hospital EST: 20th July 2010 EEG reading Age Background Epileptiform Non epileptiform Activation procedure normal
RAPID BEDSIDE NEUROLOGIC ASSESSMENT. Stephan A. Mayer, MD, FCCM Director, Neurocritical Care Mount Sinai Health System
 RAPID BEDSIDE NEUROLOGIC ASSESSMENT Stephan A. Mayer, MD, FCCM Director, Neurocritical Care Mount Sinai Health System Classic Neurological Examination 1. Mental Status 2. Cranial Nerves 3. Motor Exam
RAPID BEDSIDE NEUROLOGIC ASSESSMENT Stephan A. Mayer, MD, FCCM Director, Neurocritical Care Mount Sinai Health System Classic Neurological Examination 1. Mental Status 2. Cranial Nerves 3. Motor Exam
Ambulatory non-convulsive status epilepticus evolving into a malignant form
 Original article Epileptic Disord 2012; 14 (1): 41-50 Ambulatory non-convulsive status epilepticus evolving into a malignant form José L Fernández-Torre 1,2,3, Peter W Kaplan 4, Mariano Rebollo 5, Agustín
Original article Epileptic Disord 2012; 14 (1): 41-50 Ambulatory non-convulsive status epilepticus evolving into a malignant form José L Fernández-Torre 1,2,3, Peter W Kaplan 4, Mariano Rebollo 5, Agustín
Pediatric Thrombectomy
 Pediatric Thrombectomy Translating adult standard of care to pediatric patients DATE: September 16, 2016 PRESENTED BY: Ittai Bushlin MD, PhD and Adrienne McDougal, RN Objectives: Review acute management
Pediatric Thrombectomy Translating adult standard of care to pediatric patients DATE: September 16, 2016 PRESENTED BY: Ittai Bushlin MD, PhD and Adrienne McDougal, RN Objectives: Review acute management
Presurgical Evaluation before Epilepsy Surgery
 Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Epilepsy. Annual Incidence. Adult Epilepsy Update
 Adult Epilepsy Update Annual Incidence J. Layne Moore, MD, MPH Associate Professor Department of Neurology and Pharmacy Director, Division of Epilepsy The Ohio State University Used by permission Health
Adult Epilepsy Update Annual Incidence J. Layne Moore, MD, MPH Associate Professor Department of Neurology and Pharmacy Director, Division of Epilepsy The Ohio State University Used by permission Health
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011
 Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011 Sudha Kilaru Kessler M.D. Assistant Professor of Neurology and Pediatrics Children s Hospital of Philadelphia University of Pennsylvania
Pediatric Continuous EEG Monitoring: Case Presentation December 5, 2011 Sudha Kilaru Kessler M.D. Assistant Professor of Neurology and Pediatrics Children s Hospital of Philadelphia University of Pennsylvania
Can t Stop the Seizing!
 Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Prescribing and Monitoring Anti-Epileptic Drugs
 Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Prescribing and Monitoring Anti-Epileptic Drugs Mark Granner, MD Clinical Professor and Vice Chair for Clinical Programs Director, Iowa Comprehensive Epilepsy Program Department of Neurology University
Positron Emission Tomography Imaging in Brain Injured Patients
 Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
Positron Emission Tomography Imaging in Brain Injured Patients Paul Vespa, MD Professor Director of Neurocritical Care UCLA Brain Injury Research Center Outline Clinical Context of imaging Practical issues
PRESURGICAL EVALUATION. ISLAND OF COS Hippocrates: On the Sacred Disease. Disclosure Research-Educational Grants. Patients with seizure disorders
 PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
Localization a quick look
 Localization a quick look Covering the basics Differential amplifiers Polarity convention 10-20 electrode system Basic montages: bipolar and referential Other aspects of displaying the EEG Localization
Localization a quick look Covering the basics Differential amplifiers Polarity convention 10-20 electrode system Basic montages: bipolar and referential Other aspects of displaying the EEG Localization