March 31, 2016 Orlando, FL. ENT Procedures Jose C. Mercado, PA-C, MMS, DFAAPA
|
|
|
- Basil Owen
- 6 years ago
- Views:
Transcription



1 March 31, 2016 Orlando, FL ENT Procedures Jose C. Mercado, PA-C, MMS, DFAAPA Updated 12/03/2015




2 ENT Procedures Workshop Clear Instruction Live Demonstration Hands-On Practice Learn by doing Removal Foreign Body (Nose) Control Posterior Epistaxis Peritonsillar Abscess Control Anterior Epistaxis Fine Needle Aspiration Auricular Hematoma
3 Introduction There are multiple methods and techniques available to successfully complete all the topics presented in this workshop. Some are based on patient request, available equipment or supervising physician s preference. The goal of this workshop is to correctly demonstrate the most common methods and give participants time for hands on training.
4 ENT Procedures Workshop Learning Objectives Discuss indications for and practice removal nasal foreign body. Discuss indications for and practice control anterior epistaxis. Discuss indications for and practice control posterior epistaxis. Discuss indications for and practice fine needle aspiration. Discuss indications for and practice peritonsillar abscess drainage. Discuss indications for drainage auricular hematoma and practice splinting.

5 Removal Foreign Body (Nose) Purulent unilateral nasal discharge, especially in children Usually lodge on the floor of anterior or middle third Figure. A: Fiberoptic nasal endoscopy shows the mass in the left anterior nasal cavity. B: Coronal CT shows the area of attenuation in the left inferior turbinate. C: Photograph shows the broken mass. D: Following removal of the mass, the passageway is clear. Mercado, JC, Goldberg SG, Recurrent purulent rhinorrhea in an otherwise healthy woman Ear Nose Throat J Jun;83(6):381-2
6 Removal Foreign Body (Nose) Good visualization: headlamp & nasal speculum Alligator forceps should be used to remove cloth, cotton, or paper Other hard FB are more easily grasped using bayonet forceps, Kelly clamps, or they may be rolled out by getting behind it using an ear curette, single skin hook, or right angle ear hook Spray topical anesthetic and decongestant prior to initiating procedure. Practice mannequins available to practice removal of nasal foreign bodies technique.




7 Task: Removal Foreign Body Nose Indications: Unilateral purulent nasal discharge 1. Explain Procedure. Apply topical anesthetic & decongestant BILATERALLY. 2. Good visualization with use of bright headlight & nasal speculum. Mercado Alligator forceps should be used to remove cloth, cotton, or paper. Other hard FB are more easily grasped using bayonet forceps, Kelly clamps, or they may be rolled out by getting behind it using an ear curette, single skin hook, or right angle ear hook Mercado 2013 Mercado Perform flexible fiberoptic endoscopy to check for infection, bleeding and additional foreign bodies. Mercado 2013
8 Control Anterior Epistaxis


9 Control Anterior Epistaxis Control anterior epistaxis in office. Apply direct manual pressure for at least 10 minutes Mercado 2011 Mercado 2011

10 Anterior vs. Posterior Kiesslebach s Plexus or Little s Area is most common site of anterior nosebleeds. Woodruff s Plexus is most common site for posterior nose bleeds and may represent a lesion. Sphenopalatine artery is generally the source of severe posterior nosebleeds. Epistaxis
11 Etiology of Epistaxis Local Trauma /Nose picking or blowing / surgery Dry air / Irritants Topical medications (steroids) Foreign body Tumor Systemic Bleeding disorders Hereditary hemorrhagic telangiectasia Drugs (anticoagulants) Hypertension



12 Direct Manual Pressure NO NO YES Mercado 2011 Mercado 2011 Mercado 2011

13 Control Anterior Epistaxis Spray or apply topical anesthetic with decongestant. Reapply direct manual pressure an additional 10 minutes. Mercado 2011

14 Control Anterior Epistaxis Once bleeding has subsided, identify site of nosebleed. Mercado 2011
 Caution bilateral cauterization as may result in septal perforation.")
15 Control Anterior Epistaxis Control bleeding with silver nitrate cauterization. (start from outside in) Caution bilateral cauterization as may result in septal perforation. Mercado 2011


16 Control Anterior Epistaxis Lubricate naris with Vaseline or Neosporin ointment. Let sit for minutes to ensure hemostasis is achieved. Keep cotton in nares for at least 1 hour to prevent staining. Avoid sneezing, forceful nose blowing, nose picking, etc. Follow up 2 weeks as recauterization may be necessary. Post chemical cauterization stain day 1 Post chemical cauterization stain day 4 Mercado Mercado

17 Anterior Nasal Packing Nasal packing Absorbable gelfoam Vaseline gauze Nasal tampon Anterior packing Mercado 2011




18 Anterior Nasal Packing Nasal packing Vaseline gauze is inserted along floor of naris to form a tight seal.


19 Anterior Nasal Packing Nasal packing Nasal tampon expands in nasal cavity to form a tight seal. Do not allow packing to moisten until in position. Removal may cause re-bleeding. Mercado 2011 Mercado 2011

20 Anterior Nasal Tampon Insert nasal tampon horizontally. Lubricate with Neosporin but DO NOT moisten! Secure ties to cheek. Mercado 2011 Practice mannequins available to practice anterior nasal packing technique.

21 Anterior Nasal Packing Anterior nasal packing Easy to insert and remove due to self-lubricating hydrocolloid fabric and ultra-low profile. Packing quickly conforms to nasal anatomy and provides gentle and even compression to areas of epistaxis. Mercado 2011


22 Anterior Nasal Packing Soak dressing to hydrate Gel Knit hydrocolloid fabric in sterile water for 30 seconds. Insert Rapid Rhino horizontally. Inflate balloon only with air. Tape pilot cuff to side of face. Mercado 2011 Mercado 2011


23 Which of the following is correct? A B
24 Control Posterior Epistaxis
25 Anterior vs. Posterior Epistaxis Kiesslebach s Plexus or Little s Area is most common site of anterior nosebleeds. Woodruff s Plexus is most common site for posterior nose bleeds and may represent a lesion. Sphenopalatine artery is generally the source of severe posterior nosebleeds. Posterior tend to be more difficult to control and may suggest an underlying etiology.
26 Etiology of Epistaxis Local Trauma (Nose picking or blowing) Dry air / Irritants Topical medications (steroids) Foreign body Tumor / polyp Surgery Systemic Hypertension Coagulopathies Hereditary hemorrhagic telangiectasia Drugs (anticoagulants)
27 Control Posterior Epistaxis Control Hypertension Identify Coagulopathy Treat with FFP, transfusions, etc PT, PTT, INR Coumadin toxicity - Vitamin K Posterior Packing Endoscopic Cauterization Arterial Embolization (Interventional Radiology)

28 Posterior Nasal Packing Topical anesthetic & decongestant Posterior nasal packing Foley catheter Double balloon device

29 Posterior Packing Epistaxis 1. Thoroughly soak in sterile water for 30 seconds. 2. Insert Rapid Rhino into the patient s nostril parallel to the septal floor, or following along the superior aspect of the hard palate, until the blue indicator ring is inside the opening of the nostril. 3. Using a 20 cc syringe, slowly inflate the posterior (green stripe) balloon first with air only inside the patient s nose.

30 Posterior Packing Epistaxis 4. Inflate second balloon with air. 5. Allow the patient to sit for minutes prior to discharge. Swelling in the nasal anatomy will reduce and the balloons may need to be inflated more to avoid movement of the device. Don t forget prophylaxis antibiotics! 6. To remove packing, deflate balloons hours later.


31 Additional Treatments Endoscopic Cauterization B. Ghorayeb, MD Arterial Embolization Koh E et al. AJR 2000;174:


32 Practice mannequins available to practice posterior nasal packing technique. Summary Epistaxis Direct Pressure Embolization Chemical Cauterization Mercado 2011 Thermal Cauterization Nasal packing

33 Task: Control Anterior Epistaxis Indications: Anterior persistent nosebleed in office 1. Apply direct manual pressure for at least 10 minutes. 2. Spray or apply topical anesthetic with decongestant. Reapply direct manual pressure an additional 10 minutes Mercado Once bleeding has subsided, identify site of nosebleed 4. Control bleeding with silver nitrate cauterization. (start from outside in) Mercado Lubricate naris with Vaseline or Neosporin ointment. Keep cotton in nares for at least 1 hour to prevent staining. 6. Let sit for minutes to ensure hemostasis is achieved. Mercado 2011 Avoid sneezing, forceful nose blowing, nose picking, etc. Follow up 2 weeks as re-cauterization may be necessary. Mercado 2011
34 Task: Control Epistaxis Indications: Persistent anterior or posterior nosebleed despite cauterization 1. Thoroughly soak in sterile water for 30 seconds. 2. Insert nasal pack into the patient s nostril parallel to the septal floor, or following along the superior aspect of the hard palate, until the blue indicator ring is inside the opening of the nostril. 3. Using a 20 cc syringe, slowly inflate the posterior (green stripe) balloon first with air only inside the patient s nose. 4. Inflate second balloon with air. 5. Allow the patient to sit for minutes prior to discharge. Swelling in the nasal anatomy will reduce and the balloons may need to be inflated more to avoid movement of the device. Don t forget prophylaxis antibiotics! 6. To remove packing, deflate balloons hours later.
35 Fine Needle Aspiration



36 Site Selection Common sites include thyroid and parotid glands as well as lymph nodes. Mercado 2011 Mercado 2011 Mercado 2011
37 Anesthesia For superficial aspirates, clean technique suffices for cleansing of the skin surface. Local anesthetic may or may not be used. If more than two or three attempts are anticipated, this is recommended. However, be certain not to contaminate the lesion with a large volume of anesthetic. Also, make attempts not to directly interfere with the ability to palpate and localize the lesion. For deep aspirates, sterile technique is required for cleansing of the skin and local anesthetic is usually required.
38 Fine Needle Aspiration Use a 3, 5, 10 or 20 ml syringe. Use of a Syringe Pistol is optional. Needle should be at least 1 ½ inch or appropriate length and be 22 to 25 gauge. Single end label clear glass slides (for preparation of direct smears). Fixative to preserve fixed slides (either Cytology spray fixative, Saccomanno fixative or 95% ethyl alcohol in coplin jar). Mercado 2011

39 Fine Needle Aspiration Palpate and identify mass or lesion. Clean topically with alcohol. Stabilize the mass with non-dominant hand. Insert needle through the skin with a quick motion. Mercado 2011 Mercado 2011

40 Fine Needle Aspiration Advance through the subcutaneous tissue into the mass. Aim needle toward the center of small masses but toward the periphery of larger masses as the center may be necrotic. A noticeable difference in the consistency of the tissue should be noted when the needle penetrates the mass. With the needle in the mass, the needle tip should be moved in short motions initially to loosen cells within the mass. Pull back on plunger to create negative pressure. Fowler 2011
41 Fine Needle Aspiration Without releasing pressure, withdraw the needle within the target slightly then reinsert at a slightly different angle. Repeat maneuver several times before complete withdrawal. May also perform a corkscrew action before withdrawal. If blood or material appears in the hub of the needle, the aspiration should be stopped. Release negative pressure before withdrawing the needle, negative pressure must be released to prevent suction of the material into the barrel of the syringe when the needle exits the skin. Fowler 2011
42 Preparing Slides Transfer specimen from needle hub to slides. Gently and evenly spread specimen between two slides before fixing. Allow to air dry before closing slide holder. Mercado 2011 Mercado 2011

43 Fine Needle Aspiration Aspiration techniques vary widely based on personal preference, and specific clinical circumstances. Goal is to collect adequate cellular material for cytologic evaluation. Practice mannequins available to palpate and practice technique.





44 Task: Fine Needle Aspiration Indications: Obtain histopathologic diagnosis of suspected neoplasms 1. Explain Procedure. Prepare supplies 2. Palpate and identify mass or lesion. Mercado Clean topically with alcohol. Mercado Stabilize the mass with non-dominant hand. Insert needle through the skin with a quick motion. Mercado Transfer specimen to slides and either fix or immediately submerge in alcohol. Mercado 2011
45 Peritonsillar Abscess
 CT Scan with contrast")
46 Peritonsillar Abscess History Severe Odynophagia Dysphagia Physical Fever Unilateral edema Hot Potato Voice Elevated white count (CBC) CT Scan with contrast Fowler 2011


47 Peritonsillar Abscess Strong clinical suspicion without obvious physical findings. Mercado 2011 Mercado 2011
48 Mercado 2011 Equipment needed Hurricaine spray Lidocaine w/ epi Tongue Blade Scalpel Headlight Suction setup Long tonsil clamp Culturette
49 Peritonsillar Abscess Management options Needle aspiration Incision and Drainage Quinsy tonsillectomy Choice will depend on site and location of abscess. Smaller, deep abscess are sometimes easier to reach with large bore needle. Both have similar success rates (Needle Aspiration 90-95% vs. I and D %)

50 Peritonsillar Abscess Peritonsillar Abscess


51 Needle Aspiration Mercado 2011 Mercado 2011

52 Incision and Drainage Incision & Drainage with #15 blade Mercado 2011 Blunt Dissection with curved hemostat Mercado 2011 Mercado 2011

53 Peritonsillar Abscess Discharge instruction : Penicillin based antibiotics 7-10 days. Oral prednisone (medrol dose pack). In-office follow up 2 weeks. Mercado 2014 Possible tonsillectomy. Practice mannequins available to practice drainage of PTA.

54 Peritonsillar Abscess Mercado 2014 Practice mannequins available to simulate PTA and practice needle aspiration technique.


 over area of")
. 5.")


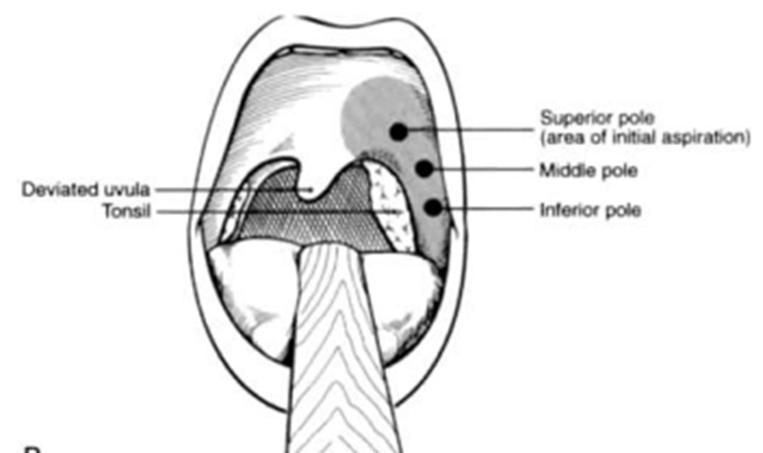
55 Task: Drainage Peritonsillar Abscess Indications: Drainage peritonsillar abscess >1cm. 1. Explain Procedure. Prepare supplies and locate landmarks 2. Apply topical anesthetic, inject local anesthetic. Mercado Insert large bore needle with guard (optional) over area of greatest fluctuance (imaging). Mercado Aspirate pus (release pressure when with drawing). 5. Perform incision at the point of maximum protrusion, usually between the uvula and the second upper molar tooth. Mercado Perform blunt dissection with curved hemostat. Treat with PCN based antibiotics and oral steroids. Mercado 2011 Johnson RF, Stewart MG, Wright CG. An evidence-based review of the treatment of peritonsillar abscess. Otolaryngol Head Neck Surg. 2003;128(3):




56 Auricular Hematoma Acute auricular hematoma is common after blunt trauma to the side of the head. A network of vessels provides a rich blood supply to the ear, and the ear cartilage receives its nutrients from the overlying perichondrium. Prompt management of hematoma includes drainage and prevention of reaccumulation. Several articles recommend drainage within 5 days to prevent irreversible cartilage thickening. However, authors have had great results draining up to 10 days provided there is fluctuance. The mechanism of hematoma drainage has been debated. To date, no randomized controlled trials have addressed this issue. Mercado 2013 Fowler 2013 Mercado 2013


57 Auricular Hematoma If left untreated, an auricular hematoma can result in complications such as perichondritis, infection, and necrosis. Cauliflower ear may result from long-standing loss of blood supply to the ear cartilage and formation of neocartilage from disrupted perichondrium. The goal of treatment is to completely evacuate subperichondrial blood and to prevent its reaccumulation and associated deformity. Mercado 2011




58 Auricular Hematoma Methods of applying pressure to area of hematoma include 1. compression dressing 2. external splinting Ballenger's Otorhinolaryngology: Head and Neck Surgery Mercado 2013

59 Equipment Mercado Anesthesia 2. 10cc syringe drain hematoma 3. Aquaplast 4. Hot water 160 F 5. Bandage scissors 6. Betadine prep 7. Gauze 8. 0 silk straight needle (needle driver)

 Cut to shape and size of area to")
 Cut oval or kidney shape for")
60 Auricular Hematoma Prepare 1/16inch thick Aquaplast by making pattern on OPPOSITE ear. a) Cut to shape and size of area to compress on anterior surface. b) Cut oval or kidney shape for posterior surface. Mercado 2013 Mercado 2013 Mercado 2013

61 Auricular Hematoma Pearls for working with Aquaplast. Make pattern on OPPOSITE ear. Fine tune on OPPOSITE ear before working on inured ear. Use good bandage scissors Cut round smooth edges Mercado 2013
62 Auricular Hematoma 1. Place patient in sitting position with head supported. 2. Inject 1% lidocaine with or without epinephrine RING BLOCK technique.
 Mercado 2013")
63 Auricular Hematoma Evacuate hematoma (incision & drainage or 18ga needle aspiration) Mercado 2013


64 Auricular Hematoma Prepare non-adherent gauze pad or petroleum gauze the shape of the Aquaplast so they project 1-2 mm BEYOND margins Mercado 2013 Mercado 2013


65 Auricular Hematoma Immerse Aquaplast in hot water (160F) until it becomes transparent. Place splint over site (Aquaplast will NOT burn underlying skin) and allow to conform to ear surface as it cools. Repeat process for posterior splint. Mercado 2013 Mercado 2013


66 Auricular Hematoma 9. After placement of gauze pads between the splints and the skin surface secure with two or three through and through 0 silk on a straight needle to snuggly compress splint dressing to hematoma in sandwich fashion. Mercado 2013 Mercado 2013 Mercado 2013 Mercado 2013


67 Auricular Hematoma 10. Discharge on oral antibiotics (cephalaxin) and follow up 7-10 days for removal of sutures. Mercado 2013 Mercado 2013

:116-20 Giles WC, Iverson KC, King JD, Hill FC, Woody EA, Bouknight AL.")
:2097-9 Greywoode JD, Pribitkin EA, Krein H.")
68 References Fowler 2013 Fowler 2013 Fowler 2013 Biedenbach P, Steehler KW, Anon JB, Management of Auricular Hematoma using Aquaplast Pressure Dressing. Operative Tech in Otolaryngology HNS, vol 8, No 2, 1997: Mudry A, Pirsig W. Auricular hematoma and cauliflower deformation of the ear: from art to medicine. Otol Neurotol. Jan 2009;30(1): Giles WC, Iverson KC, King JD, Hill FC, Woody EA, Bouknight AL. Incision and drainage followed by mattress suture repair of auricular hematoma. Laryngoscope. Dec 2007;117(12): Greywoode JD, Pribitkin EA, Krein H. Management of auricular hematoma and the cauliflower ear. Facial Plast Surg. Dec 2010;26(6):451-5.v






69 Task: Drain Auricular Hematoma Indications: Drainage hematoma within 5-10 days to prevent irreversible cartilage 1. Explain Procedure. Prepare supplies thickening. 2. Prepare 1/16inch thick Aquaplast by making pattern on OPPOSITE ear. Mercado Inject anesthesia (ring block). Mercado Drain hematoma. 5. Immerse Aquaplast in hot water (160 F) until it becomes transparent. Then mold over site. Mercado Prepare non-adherent gauze pad or petroleum gauze the shape of the Aquaplast so they project 1-2 mm BEYOND margins Mercado 2013 Mercado After placement of gauze pads between the splints and the skin surface secure with two or three through and through 0 silk on a straight needle to snuggly compress splint dressing to hematoma in sandwich fashion. Mercado 2013 Mercado 2013 Mercado 2013

70 Station 1 Epistaxis Removal FB Screen Station 4 Auricular Hematoma Station 1 Station 4 Station 2 PTA Projector Speaker Station 2 Station 3 Station 3 FNA Proctors
71 ENT Procedures Workshop Evaluations Score cards will be used for admission to workshops and attendance. Credit will only be awarded for completed score cards. Name Session On scale of 1 through 5 with 5 being most likely Scale Were learning objectives met? 2. Was instruction free of commercial bias? 3. Was there adequate instruction before practice? 4. Was there adequate supervision during practice? 5. Were training aids useful/realistic in learning skill? 6. How likely are you to perform these skills in future 7. Did this training improve your skills? Comments:
72 ENT Procedures Workshop Score Card Name Session Removal Nasal FB Control Anterior Epistaxis Control Posterior Epistaxis Perform FNA Drain PTA Drain & splint auricular hematoma Comments Rotate and complete each station. Go/No Go for internal use only. Completion of workshop is NOT contingent on pass/fail. Task Go No Go Proctor Name Proctor Signature
ENT Procedures Workshop
 March 19, 2015 Newport Beach, CA ENT Procedures Jose C. Mercado, PA-C, MMS, DFAAPA Updated 01/24/2015 ENT Procedures Workshop Clear Live Hands On Instruction Demonstration Practice Learn by doing Removal
March 19, 2015 Newport Beach, CA ENT Procedures Jose C. Mercado, PA-C, MMS, DFAAPA Updated 01/24/2015 ENT Procedures Workshop Clear Live Hands On Instruction Demonstration Practice Learn by doing Removal
Flexible Fiberoptic Exam
 Flexible Fiberoptic Exam True Vocal Cords abducted True Vocal Cords adducted *Fiberoptic endoscopy, image is true. Cerumen Removal Position Patient -Explain Procedure Visualize Canal/Landmarks Determine
Flexible Fiberoptic Exam True Vocal Cords abducted True Vocal Cords adducted *Fiberoptic endoscopy, image is true. Cerumen Removal Position Patient -Explain Procedure Visualize Canal/Landmarks Determine
NONGYNECOLOGICAL CYTOLOGY FINE NEEDLE ASPIRATION SPECIMENS
 NONGYNECOLOGICAL CYTOLOGY FINE NEEDLE ASPIRATION SPECIMENS I. Purpose Fine needle aspiration of mass lesions is commonly utilized in the detection and characterization of a variety of malignant diseases.
NONGYNECOLOGICAL CYTOLOGY FINE NEEDLE ASPIRATION SPECIMENS I. Purpose Fine needle aspiration of mass lesions is commonly utilized in the detection and characterization of a variety of malignant diseases.
Chapter 6 Epistaxis. What You Need. Página 1 de 6.
 Página 1 de 6 Chapter 6 Epistaxis Epistaxis is a common problem; although the vast majority of cases are trivial, some may present as life-threatening problems because of hypotension or aspiration of blood.
Página 1 de 6 Chapter 6 Epistaxis Epistaxis is a common problem; although the vast majority of cases are trivial, some may present as life-threatening problems because of hypotension or aspiration of blood.
EPISTAXIS. Nasal Trauma, and other emergencies. Marc A. Tewfik MDCM, MSc, FRCSC
 EPISTAXIS Nasal Trauma, and other emergencies Marc A. Tewfik MDCM, MSc, FRCSC Assistant Professor, McGill University Otolaryngology-Head & Neck Surgery DISCLOSURES Speaker/Consultant Merck Novartis MEDA
EPISTAXIS Nasal Trauma, and other emergencies Marc A. Tewfik MDCM, MSc, FRCSC Assistant Professor, McGill University Otolaryngology-Head & Neck Surgery DISCLOSURES Speaker/Consultant Merck Novartis MEDA
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Nosebleed (Epistaxis)
") 2015 WebMD, LLC. All rights reserved. Nosebleed (Epistaxis) Nosebleed Overview Nosebleed Causes Nosebleeds in Children Nosebleed Symptoms When to Seek Medical Care Nosebleed Diagnosis Nosebleed Self-Care
2015 WebMD, LLC. All rights reserved. Nosebleed (Epistaxis) Nosebleed Overview Nosebleed Causes Nosebleeds in Children Nosebleed Symptoms When to Seek Medical Care Nosebleed Diagnosis Nosebleed Self-Care
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
Introduction 4/17/2017. Otology Workshop; Advanced Ryan Marovich, MPAS, PA-C J. Andrew Clark, PA-C Updated 12/03/2015
 March 31, 2016 Orlando, FL Otology Workshop; Advanced Ryan Marovich, MPAS, PA-C J. Andrew Clark, PA-C Updated 12/03/2015 Otology Workshop; Advanced Clear Instruction Live Demonstration Hands On Practice
March 31, 2016 Orlando, FL Otology Workshop; Advanced Ryan Marovich, MPAS, PA-C J. Andrew Clark, PA-C Updated 12/03/2015 Otology Workshop; Advanced Clear Instruction Live Demonstration Hands On Practice
Implanting an Adult Rat with the Single-Channel Epoch Transmitter for Recording Electrocardiogram in the Type II electrode configuration.
 Implanting an Adult Rat with the Single-Channel Epoch Transmitter for Recording Electrocardiogram in the Type II electrode configuration. Recommended Surgical Tools A. Scalpel handle B. Scalpel blade (#15)
Implanting an Adult Rat with the Single-Channel Epoch Transmitter for Recording Electrocardiogram in the Type II electrode configuration. Recommended Surgical Tools A. Scalpel handle B. Scalpel blade (#15)
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
ATI Skills Modules Checklist for Central Venous Access Devices
 For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
For faculty use only Educator s name Score Date ATI Skills Modules Checklist for Central Venous Access Devices Student s name Date Verify order Patient record Assess for procedure need Identify, gather,
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 5 Basic Surgical Procedures Key Points 2 5.1 Wound Management Many important procedures can be performed under local anesthesia and do not require a surgical specialist
Surgical Care at the District Hospital 1 5 Basic Surgical Procedures Key Points 2 5.1 Wound Management Many important procedures can be performed under local anesthesia and do not require a surgical specialist
Endoscopy. Pulmonary Endoscopy
 Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
ENTs: Not-So-Easy Emergencies
 Focus on CME at the University of Manitoba ENTs: Not-So-Easy Emergencies F. Gigi Osler, BScMed, MD, FRCSP(C) Presented at CME for Family Physicians: ENT Day, University of Manitoba (October 2003). Epistaxis
Focus on CME at the University of Manitoba ENTs: Not-So-Easy Emergencies F. Gigi Osler, BScMed, MD, FRCSP(C) Presented at CME for Family Physicians: ENT Day, University of Manitoba (October 2003). Epistaxis
Benign vs. Cancer. Oculofacial Biopsy. Evolution of skin cancer. Richard E. Castillo, OD, DO
 Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
Objectives. Urgent Care in the Family Practice Setting. Disclosures. Urgent Care in the Family Practice Setting. Tanya A.
 Urgent Care in the Family Practice Setting Tanya A. Tupick DO Pennsylvania Osteopathic Family Physicians Society August 3 rd 2018 Disclosures Dr. Tupick has provided no disclosures. Objectives Goals and
Urgent Care in the Family Practice Setting Tanya A. Tupick DO Pennsylvania Osteopathic Family Physicians Society August 3 rd 2018 Disclosures Dr. Tupick has provided no disclosures. Objectives Goals and
INFORMATION REGARDING YOUR NASAL SURGERY
 INFORMATION REGARDING YOUR NASAL SURGERY This document contains information about the following aspects of nasal surgery: Pre-op information: How to prepare for surgery. Procedure: Wat is done during surgery.
INFORMATION REGARDING YOUR NASAL SURGERY This document contains information about the following aspects of nasal surgery: Pre-op information: How to prepare for surgery. Procedure: Wat is done during surgery.
BP and Heart Rate by Telemetry
 BP and Heart Rate by Telemetry Version: 1 Modified from: Butz et al. Physiol Genomics. 2001 Mar 8;5(2):89-97. Edited by: Dr. Lynette Bower, UC Davis Summary Reagents and Materials Protocol Reagent Preparation
BP and Heart Rate by Telemetry Version: 1 Modified from: Butz et al. Physiol Genomics. 2001 Mar 8;5(2):89-97. Edited by: Dr. Lynette Bower, UC Davis Summary Reagents and Materials Protocol Reagent Preparation
Commen Nose Diseases
 Commen Nose Diseases Symptoms List: Nasal obstruction. Nasal discharge: Anterior (Rhinorrhea). Posterior (Postnasal discharge). Epistaxis. Hyposmia and Anosmia. Headache. Snoring. Nasal Obstruction Definition:
Commen Nose Diseases Symptoms List: Nasal obstruction. Nasal discharge: Anterior (Rhinorrhea). Posterior (Postnasal discharge). Epistaxis. Hyposmia and Anosmia. Headache. Snoring. Nasal Obstruction Definition:
Chest Tube Thoracostomy
 Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Sterile Technique & IJ/Femoral Return Demonstration
 Sterile Technique & IJ/Femoral Return Demonstration Sterile Technique Description: This is a return demonstration checklist used to evaluate participants in the simulated hands on skills portions for certification
Sterile Technique & IJ/Femoral Return Demonstration Sterile Technique Description: This is a return demonstration checklist used to evaluate participants in the simulated hands on skills portions for certification
How to use the Control-Cric to perform a surgical cricothyrotomy
 TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
Patient Information Publications Warren Grant Magnuson Clinical Center National Institutes of Health
 Warren Grant Magnuson Clinical Center National Institutes of Health What is a subcutaneous injection? A subcutaneous injection is given in the fatty layer of tissue just under the skin. A subcutaneous
Warren Grant Magnuson Clinical Center National Institutes of Health What is a subcutaneous injection? A subcutaneous injection is given in the fatty layer of tissue just under the skin. A subcutaneous
Table of Contents. Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings
 Table of Contents Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings Dialysis Port Care Know What Type of Vascular Access You Have. Fistula: An artery in your forearm
Table of Contents Dialysis Port Care Chemotherapy Port Care G-Tube Care Colostomy Bags Wound Dressings Dialysis Port Care Know What Type of Vascular Access You Have. Fistula: An artery in your forearm
LESSON ASSIGNMENT. Emergency Surgical Procedures. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
CHEST DRAIN PROTOCOL
 CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
Ultrasound-guided FNA Biopsy. American Thyroid Association 2017
 Ultrasound-guided FNA Biopsy American Thyroid Association 2017 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University Disclosures: No relevant
Ultrasound-guided FNA Biopsy American Thyroid Association 2017 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University Disclosures: No relevant
B. PURPOSE The purpose of this policy is to define the workflow and process involved with the procurement of Fine Needle Aspirations.
 RUTLAND REGIONAL MEDICAL CENTER Page 1 of 9 DEPARTMENT: Laboratory - Cytology EFFECTIVE DATE: 8/3/2011 /Allison Yelton ENDORSED BY: Keith Leblanc APPROVED BY: Tony M Masuck, MD APPROVED DATE: 5/27/216
RUTLAND REGIONAL MEDICAL CENTER Page 1 of 9 DEPARTMENT: Laboratory - Cytology EFFECTIVE DATE: 8/3/2011 /Allison Yelton ENDORSED BY: Keith Leblanc APPROVED BY: Tony M Masuck, MD APPROVED DATE: 5/27/216
Procedures/Risks:central venous catheter
 Procedures/Risks:central venous catheter Central Venous Catheter Placement Procedure: Placement of the central venous catheter will take place in the Interventional Radiology Department (IRD) at The Ohio
Procedures/Risks:central venous catheter Central Venous Catheter Placement Procedure: Placement of the central venous catheter will take place in the Interventional Radiology Department (IRD) at The Ohio
2017 Coding and Reimbursement Survival Guide
 2017 Coding and Reimbursement Survival Guide Chapter 14: Otolaryngology CPT 2017: Latest CPT Edition Offers New Code for Injection Laryngoplasty Changes could impact your reimbursement. The New Year is
2017 Coding and Reimbursement Survival Guide Chapter 14: Otolaryngology CPT 2017: Latest CPT Edition Offers New Code for Injection Laryngoplasty Changes could impact your reimbursement. The New Year is
Initial placement 24FR Pull PEG kit REORDER NO:
 Initial placement 24FR Pull PEG kit REORDER NO: 00710805 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 24FR Pull PEG kit is
Initial placement 24FR Pull PEG kit REORDER NO: 00710805 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 24FR Pull PEG kit is
Initial placement 20FR Guidewire PEG kit REORDER NO:
 Initial placement 20FR Guidewire PEG kit REORDER NO: 00710802 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 20FR Guidewire
Initial placement 20FR Guidewire PEG kit REORDER NO: 00710802 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 20FR Guidewire
BOCL-01: Bonding Materials Checklist
 Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Surgery/Integumentary System ( )
") 10030 The provider inserts a catheter through the skin using imaging to view the fluid. He then drains the fluid from the soft tissue in cases such as abscess, hematoma, seroma, lymphocele, or cyst. Imaging
10030 The provider inserts a catheter through the skin using imaging to view the fluid. He then drains the fluid from the soft tissue in cases such as abscess, hematoma, seroma, lymphocele, or cyst. Imaging
AACE/ACE Advanced Neck Ultrasound Training Course
 AACE/ACE Advanced Neck Ultrasound Training Course Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University No Disclosures Goals of FNA Obtain
AACE/ACE Advanced Neck Ultrasound Training Course Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel School of Medicine at Dartmouth University No Disclosures Goals of FNA Obtain
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Procedures in the ED. MCEP Straight Talk Most $$$ ED CPT Codes (not including E&M codes) EKGs X-rays Ultrasounds.
 EKGs X-rays Ultrasounds.") Procedures in the ED Most $$$ ED CPT Codes (not including E&M codes) 93010 Electrocardiogram report 31500 Insert emergency airway 36556 Insert non-tunnel CV cath 92950 Heart/lung resuscitation CPR 12001
Procedures in the ED Most $$$ ED CPT Codes (not including E&M codes) 93010 Electrocardiogram report 31500 Insert emergency airway 36556 Insert non-tunnel CV cath 92950 Heart/lung resuscitation CPR 12001
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
CAREFULLY READ ALL INSTRUCTIONS PRIOR TO USE
 CAREFULLY READ ALL INSTRUCTIONS PRIOR TO USE INDICATIONS FOR USE The LATERA Absorbable Nasal Implant is indicated for supporting upper and lower lateral nasal cartilage. CAUTION: Federal law restricts
CAREFULLY READ ALL INSTRUCTIONS PRIOR TO USE INDICATIONS FOR USE The LATERA Absorbable Nasal Implant is indicated for supporting upper and lower lateral nasal cartilage. CAUTION: Federal law restricts
EPISTAXIS. Rory Attwood MBChB,FRCS Department of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch
 EPISTAXIS Rory Attwood MBChB,FRCS Department of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch EPISTAXIS Bleeding from the nose Age Incidence Children Elderly
EPISTAXIS Rory Attwood MBChB,FRCS Department of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch EPISTAXIS Bleeding from the nose Age Incidence Children Elderly
NECK MASS. Clinical history and examination: Document detail history of mass. Imaging: US or CT of neck
 ENT ENT Referral Referral Guidelines Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment
ENT ENT Referral Referral Guidelines Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment
Title: EZ-IO. Effective Date: January SOG Number: EMS Rescinds:
 S O G Title: EZ-IO Effective Date: January 2010 SOG Number: EMS - 25 Rescinds: Scope: Providers Authorized are AIC s in the following certifications EMT-I and EMT-P who have been trained and cleared by
S O G Title: EZ-IO Effective Date: January 2010 SOG Number: EMS - 25 Rescinds: Scope: Providers Authorized are AIC s in the following certifications EMT-I and EMT-P who have been trained and cleared by
SOP: Urinary Catheter in Dogs and Cats
 SOP: Urinary Catheter in Dogs and Cats These SOPs were developed by the Office of the University Veterinarian and reviewed by Virginia Tech IACUC to provide a reference and guidance to investigators during
SOP: Urinary Catheter in Dogs and Cats These SOPs were developed by the Office of the University Veterinarian and reviewed by Virginia Tech IACUC to provide a reference and guidance to investigators during
Injection Techniques Principles and Practice. Introduction. Learning Objectives 5/18/2015. Richard E. Castillo, OD, DO
 Injection Techniques Principles and Practice Richard E. Castillo, OD, DO Administering injections is considered a routine clinic activity Safety demands knowledge of: Anatomy & Physiology Pharmacology
Injection Techniques Principles and Practice Richard E. Castillo, OD, DO Administering injections is considered a routine clinic activity Safety demands knowledge of: Anatomy & Physiology Pharmacology
General Practitioner Assessment of the Inside and Outside of the Nose. Chris Thomson Otolaryngologist Head and Neck Surgeon
 General Practitioner Assessment of the Inside and Outside of the Nose Chris Thomson Otolaryngologist Head and Neck Surgeon Nasal problems are very common in General practice but the nose is a difficult
General Practitioner Assessment of the Inside and Outside of the Nose Chris Thomson Otolaryngologist Head and Neck Surgeon Nasal problems are very common in General practice but the nose is a difficult
Airway/Breathing. Chapter 5
 Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Airway/Breathing Chapter 5 Airway/Breathing Introduction Skillful, rapid assessment and management of airway and ventilation are critical to preventing morbidity and mortality. Airway compromise can occur
Functional Endoscopic Sinus Surgery
 WHAT IS FUNCTIONAL ENDOSCOPIC SINUS SURGERY (FESS)? The nasal telescope has greatly changes the evaluation and treatment of rhino-sinusitis. This instrument, which provides a view of the structures in
WHAT IS FUNCTIONAL ENDOSCOPIC SINUS SURGERY (FESS)? The nasal telescope has greatly changes the evaluation and treatment of rhino-sinusitis. This instrument, which provides a view of the structures in
Summary Report for Individual Task Perform a Surgical Cricothyroidotomy Status: Approved
 Report Date: 12 Jul 2011 Summary Report for Individual Task 081-833-3005 Perform a Surgical Cricothyroidotomy Status: Approved DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited.
Report Date: 12 Jul 2011 Summary Report for Individual Task 081-833-3005 Perform a Surgical Cricothyroidotomy Status: Approved DISTRIBUTION RESTRICTION: Approved for public release; distribution is unlimited.
Ophthalmology Wet Lab Notes - Kimberly Hsu, DVM, MSc, DACVO
 Ophthalmology Wet Lab Notes - Kimberly Hsu, DVM, MSc, DACVO If you have questions, please do not hesitate to call Dr. Hsu at Eye Care for Animals, St. Charles at 630-444-0393 or email at stcharlesinfo@eyecareforanimals.com
Ophthalmology Wet Lab Notes - Kimberly Hsu, DVM, MSc, DACVO If you have questions, please do not hesitate to call Dr. Hsu at Eye Care for Animals, St. Charles at 630-444-0393 or email at stcharlesinfo@eyecareforanimals.com
All bedside percutaneously placed tracheostomies
 Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Page 1 of 5 Scope: All bedside percutaneously placed tracheostomies Population: All ICU personnel Outcomes: To standardize and outline the steps necessary to safely perform a percutaneous tracheostomy
Detecting a sinus perforation.
 Extractions and the Sinus Dentistry s Black Hole. Detecting a sinus perforation. How to know when you have a small perforation? Need: Adequate light (headlight preferred) Small suction tip (2 mm diameter)
Extractions and the Sinus Dentistry s Black Hole. Detecting a sinus perforation. How to know when you have a small perforation? Need: Adequate light (headlight preferred) Small suction tip (2 mm diameter)
ENT Referral Guidelines
 ENT Referral Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment of patients with cancerous
ENT Referral Guidelines Austin Health ENT Clinic holds fortnightly multidisciplinary meetings with Plastics/ Maxillary Facial and Oncology units to discuss and plan the treatment of patients with cancerous
Complex Exodontia. Jone Kim, DDS, MS
 Complex Exodontia Jone Kim, DDS, MS Diplomate, American Board of Oral & Maxillofacial Surgery Lecturer, UCLA School of Dentistry, Dept. of Oral & Maxillofacial Surgery Principle of Complex Exodontia Principle
Complex Exodontia Jone Kim, DDS, MS Diplomate, American Board of Oral & Maxillofacial Surgery Lecturer, UCLA School of Dentistry, Dept. of Oral & Maxillofacial Surgery Principle of Complex Exodontia Principle
Aspira* Peritoneal Drainage Catheter
 Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Successful IV Starts Revised February 2014
 Successful IV Starts Revised February 2014 Why Intravenous Therapy? Used for access to the body s circulation Indications: Administer fluids, blood, medications, and nutrition Obtain laboratory specimens
Successful IV Starts Revised February 2014 Why Intravenous Therapy? Used for access to the body s circulation Indications: Administer fluids, blood, medications, and nutrition Obtain laboratory specimens
Nosebleeds are divided into two types, depending on whether the bleeding is coming from the front or back of the nose.
 Nosebleeds Anatomy and Physiology The nose is an area of the body that contains many tiny blood vessels or arterioles that can break easily. One of every seven people will develop a nosebleed some time
Nosebleeds Anatomy and Physiology The nose is an area of the body that contains many tiny blood vessels or arterioles that can break easily. One of every seven people will develop a nosebleed some time
Infusion Skills Competency Checklist To be used at annual skills fair or at any other time for IV Competency
 Employee Profile Infusion Skills Checklist Last Name First Name Middle Initial Employee Number Employee Discipline Check one: RN LPN Per state specific LPN Practice Acts Direct Supervisor s Name: Date
Employee Profile Infusion Skills Checklist Last Name First Name Middle Initial Employee Number Employee Discipline Check one: RN LPN Per state specific LPN Practice Acts Direct Supervisor s Name: Date
Nasal Surgery. Types of Surgery. This handout explains different types of nasal surgery and what to expect.
 Nasal Surgery This handout explains different types of nasal surgery and what to expect. Types of Surgery Septoplasty is a surgery done to straighten the septum. The septum is made of bone and cartilage.
Nasal Surgery This handout explains different types of nasal surgery and what to expect. Types of Surgery Septoplasty is a surgery done to straighten the septum. The septum is made of bone and cartilage.
Management of epistaxis in general practice. Dennis Pashen, Maurice Stevens. (Australian Family Physician, Vol 31, No 8, August 2002)
") Management of epistaxis in general practice Dennis Pashen, Maurice Stevens (Australian Family Physician, Vol 31, No 8, August 2002) Background. The vast majority of cases of epistaxis can be managed successfully
Management of epistaxis in general practice Dennis Pashen, Maurice Stevens (Australian Family Physician, Vol 31, No 8, August 2002) Background. The vast majority of cases of epistaxis can be managed successfully
LESSON ASSIGNMENT. Urinary System Diseases/Disorders. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 4 Urinary System Diseases/Disorders LESSON ASSIGNMENT Paragraphs 4-1 through 4-8. LESSON OBJECTIVES After completing this lesson, you should be able to: 4-1. Identify the purposes
LESSON ASSIGNMENT LESSON 4 Urinary System Diseases/Disorders LESSON ASSIGNMENT Paragraphs 4-1 through 4-8. LESSON OBJECTIVES After completing this lesson, you should be able to: 4-1. Identify the purposes
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
Skin Integrity and Wound Care
 Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Edintrak II Endoscopic decompression of intermetatarsal nerve. Operative technique
 Edintrak II Endoscopic decompression of intermetatarsal nerve Operative technique Endoscopic decompression of intermetatarsal nerve Table of contents Introduction 3 Operative technique 4 This publication
Edintrak II Endoscopic decompression of intermetatarsal nerve Operative technique Endoscopic decompression of intermetatarsal nerve Table of contents Introduction 3 Operative technique 4 This publication
Policy x.xxx. Issued: Artificial Airways and Airway Care. ABC Home Medical Company Policy & Procedure Manual. A. Tracheostomy Tubes ( trach tubes)
") A. Tracheostomy Tubes ( trach tubes) A tracheotomy is a surgical procedure whereby an opening is cut into the trachea of the patient for the purpose of inserting a tube (trach tube). The trach tube allows
A. Tracheostomy Tubes ( trach tubes) A tracheotomy is a surgical procedure whereby an opening is cut into the trachea of the patient for the purpose of inserting a tube (trach tube). The trach tube allows
If viewing a printed copy of this policy, please note it could be expired. Got to to view current policies.
 If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Code: D: PC-5555 Entity: Fairview Pharmacy Services
If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Code: D: PC-5555 Entity: Fairview Pharmacy Services
PRODUCTS FOR THE DIFFICULT AIRWAY. Courtesy of Cook Critical Care
 PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
PRODUCTS FOR THE DIFFICULT AIRWAY Courtesy of Cook Critical Care EMERGENCY CRICOTHYROTOMY Thyroid Cartilage Access Site Cricoid Cartilage Identify the cricothyroid membrane between the cricoid and thyroid
NASAL FRACTURES. Andrew H. Murr, MD FACS Professor Chief of Service Department of Otolaryngology/ Head and Neck Surgery San Francisco General Hospital
 NASAL FRACTURES Andrew H. Murr, MD FACS Professor Chief of Service Department of Otolaryngology/ Head and Neck Surgery San Francisco General Hospital Roger Boles, M.D. Endowed Chair in Otolaryngology Education
NASAL FRACTURES Andrew H. Murr, MD FACS Professor Chief of Service Department of Otolaryngology/ Head and Neck Surgery San Francisco General Hospital Roger Boles, M.D. Endowed Chair in Otolaryngology Education
Susan G. Komen 3-Day. Medical Team Blister Protocol. Randy Pearson, MD, FAAFP, FACSM Dr. Jennifer A. Saam, DPM
 Susan G. Komen 3-Day Medical Team Blister Protocol Randy Pearson, MD, FAAFP, FACSM Dr. Jennifer A. Saam, DPM Blisters happen because of friction. Most common problem on the Komen 3-Day. Caused by friction
Susan G. Komen 3-Day Medical Team Blister Protocol Randy Pearson, MD, FAAFP, FACSM Dr. Jennifer A. Saam, DPM Blisters happen because of friction. Most common problem on the Komen 3-Day. Caused by friction
Taking nose, throat and skin swabs. Clinical Skills
 Clinical Skills Taking nose, throat and skin swabs Carole Loveridge (Lecturer in Women s Health) Aims and Objectives Aims and Objectives The aim of this module is to facilitate learning regarding the purpose
Clinical Skills Taking nose, throat and skin swabs Carole Loveridge (Lecturer in Women s Health) Aims and Objectives Aims and Objectives The aim of this module is to facilitate learning regarding the purpose
M A H O M E W O R K # 2 P a g e Outpatient surgery is generally limited to procedures requiring less than 60
 M A 2 0 5 H O M E W O R K # 2 P a g e 1 NAME: DATE: CHAPTER 42 Assisting with Minor Surgery True/False: 1. Outpatient surgery is generally limited to procedures requiring less than 60 minutes to perform.
M A 2 0 5 H O M E W O R K # 2 P a g e 1 NAME: DATE: CHAPTER 42 Assisting with Minor Surgery True/False: 1. Outpatient surgery is generally limited to procedures requiring less than 60 minutes to perform.
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
This information was created and reviewed through a partnership with the UAMS Patient and Family Advisory Councils.
 Tracheostomy Care You have a: Cuffed Tracheostomy Cuffless Tracheostomy What is a tracheostomy? A tracheostomy (sometimes called a trach rhymes with cake ) is a small opening, or stoma, in your throat.
Tracheostomy Care You have a: Cuffed Tracheostomy Cuffless Tracheostomy What is a tracheostomy? A tracheostomy (sometimes called a trach rhymes with cake ) is a small opening, or stoma, in your throat.
DISCOVER NEW HORIZONS IN FLUID DRAINAGE. Bringing Safety and Convenience to Fluid Drainage Management
 DISCOVER NEW HORIZONS IN FLUID DRAINAGE Bringing Safety and Convenience to Fluid Drainage Management DRAIN ASEPT Pleural and Peritoneal Drainage Catheter System 600mL or 1,000mL Evacuated Drainage Bottle
DISCOVER NEW HORIZONS IN FLUID DRAINAGE Bringing Safety and Convenience to Fluid Drainage Management DRAIN ASEPT Pleural and Peritoneal Drainage Catheter System 600mL or 1,000mL Evacuated Drainage Bottle
How to Change a. Foley catheter. Patient Education Rehabilitation Nursing. Step-by-step instructions for the caregiver
 Patient Education How to Change a Foley Catheter Step-by-step instructions for the caregiver This handout gives step-bystep instructions for changing a Foley catheter, which is a tube in your bladder to
Patient Education How to Change a Foley Catheter Step-by-step instructions for the caregiver This handout gives step-bystep instructions for changing a Foley catheter, which is a tube in your bladder to
This information will help you care for your tracheostomy while you re in the hospital and at home.
 PATIENT & CAREGIVER EDUCATION Caring for Your Tracheostomy This information will help you care for your tracheostomy while you re in the hospital and at home. Your Trachea Your trachea (windpipe) is part
PATIENT & CAREGIVER EDUCATION Caring for Your Tracheostomy This information will help you care for your tracheostomy while you re in the hospital and at home. Your Trachea Your trachea (windpipe) is part
Tips for Successful Venipuncture
 Page 1 of 5 Patient Positioning Have patient lie or sit down. Never draw blood on a patient who is standing. Make the patient as comfortable as you possibly can. Always watch and ask patient if he/she
Page 1 of 5 Patient Positioning Have patient lie or sit down. Never draw blood on a patient who is standing. Make the patient as comfortable as you possibly can. Always watch and ask patient if he/she
INSTRUCTIONS FOR PREPARING AND GIVING AN INJECTION OF ENBREL POWDER
 INSTRUCTIONS FOR PREPARING AND GIVING AN INJECTION OF ENBREL POWDER Introduction The following instructions explain how to prepare and inject Enbrel powder for injection. Please read the instructions carefully
INSTRUCTIONS FOR PREPARING AND GIVING AN INJECTION OF ENBREL POWDER Introduction The following instructions explain how to prepare and inject Enbrel powder for injection. Please read the instructions carefully
ASSESSMENT AND CARE Monitor for the following and remove catheter if there is: redness, pain, swelling, firm tissue, exudates, bleeding or leakage.
 POLICY An Indwelling subcutaneous catheter may be inserted when an infant requires regular subcutaneous injections (At least one subcutaneous injection per day). SUPPORTIVE DATA In the NICU medications
POLICY An Indwelling subcutaneous catheter may be inserted when an infant requires regular subcutaneous injections (At least one subcutaneous injection per day). SUPPORTIVE DATA In the NICU medications
Note: This CareKit does not replace expert medical care. Be Prepared
 Note: This CareKit does not replace expert medical care. Be Prepared EMS #: 9-1-1 Poison Control #: 800.222.1222 Take a first aid course. Learn CPR and first aid for choking. Before you give first aid,
Note: This CareKit does not replace expert medical care. Be Prepared EMS #: 9-1-1 Poison Control #: 800.222.1222 Take a first aid course. Learn CPR and first aid for choking. Before you give first aid,
NASHVILLE EAR, NOSE &THROAT CLINIC STEPHEN A. MITCHELL, M.D., F.A.C.S MITCHELL K. SCHWABER, M.D. STEVEN ENRICH, M.D. MATTHEW SPEYER. M.D., P.C.
 N A S H V I L L E ENT C L I N I C NASHVILLE EAR, NOSE &THROAT CLINIC STEPHEN A. MITCHELL, M.D., F.A.C.S MITCHELL K. SCHWABER, M.D. STEVEN ENRICH, M.D. MATTHEW SPEYER. M.D., P.C. WHAT TO EXPECT AFTER SEPTOPLASTY
N A S H V I L L E ENT C L I N I C NASHVILLE EAR, NOSE &THROAT CLINIC STEPHEN A. MITCHELL, M.D., F.A.C.S MITCHELL K. SCHWABER, M.D. STEVEN ENRICH, M.D. MATTHEW SPEYER. M.D., P.C. WHAT TO EXPECT AFTER SEPTOPLASTY
INGROWING TOE NAIL REQUIREMENTS A. Instruments to be autoclaved and packed B. Disposables C. Solutions PROCEDURE
 INGROWING TOE NAIL Pages with reference to book, From 21 To 23 Irfan Daudi ( Department of Surgery, Aga Khan University of Health Sciences, Stadium Road, Karachi. ) The condition of in growing toe nail
INGROWING TOE NAIL Pages with reference to book, From 21 To 23 Irfan Daudi ( Department of Surgery, Aga Khan University of Health Sciences, Stadium Road, Karachi. ) The condition of in growing toe nail
Critical ENT Skills and Procedures in the Emergency Department
 Critical ENT Skills and Procedures in the Emergency Department Jorge L. Falcon-Chevere, MD a, *, Laureano Giraldez, MD b, Jose O. Rivera-Rivera, MD a, Tito Suero-Salvador, MD a KEYWORDS Ear laceration
Critical ENT Skills and Procedures in the Emergency Department Jorge L. Falcon-Chevere, MD a, *, Laureano Giraldez, MD b, Jose O. Rivera-Rivera, MD a, Tito Suero-Salvador, MD a KEYWORDS Ear laceration
EndoBlade Soft Tissue Release System
 Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System
 WHITE PAPER Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System Jerome Hester, MD Chief Medical Officer SinuSys Corporation Palo Alto, California USA Introduction Establishment
WHITE PAPER Treatment of Maxillary Sinusitis Using the SinuSys Vent-Os Sinus Dilation System Jerome Hester, MD Chief Medical Officer SinuSys Corporation Palo Alto, California USA Introduction Establishment
PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY
 PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
PATIENT CENTERED MEDICINE - 1 GOALS & OUTCOMES: PCM1 Physical Exam Skills Session: Head and Neck FACILITATOR & STUDENT COPY 1. To introduce the applied anatomy relevant for the examination of the head
Effective Date: Approved by: Laboratory Executive Director, Ed Hughes (electronic signature)
") 1 Policy #: 406 (PLH-406-02) Effective Date: NA Reviewed Date: 2/1/2008 Subject: VENIPUNCTURE PROCEDURE Approved by: Laboratory Executive Director, Ed Hughes (electronic signature) Approved by: Laboratory
1 Policy #: 406 (PLH-406-02) Effective Date: NA Reviewed Date: 2/1/2008 Subject: VENIPUNCTURE PROCEDURE Approved by: Laboratory Executive Director, Ed Hughes (electronic signature) Approved by: Laboratory
Meniscus cartilage replacement with cadaveric
 Technical Note Meniscal Allografting: The Three-Tunnel Technique Kevin R. Stone, M.D., and Ann W. Walgenbach, R.N.N.P., M.S.N. Abstract: This technical note describes an improved arthroscopic technique
Technical Note Meniscal Allografting: The Three-Tunnel Technique Kevin R. Stone, M.D., and Ann W. Walgenbach, R.N.N.P., M.S.N. Abstract: This technical note describes an improved arthroscopic technique
Epistaxis in children: approach and management. Jacques Viljoen. (CME, Nov/Dec 2003, Vol 21, No 11.) Epidemiology
 Epidemiology") Epistaxis in children: approach and management Jacques Viljoen (CME, Nov/Dec 2003, Vol 21, No 11.) Nose bleeds can be intimidating for the child, the parents and the doctor alike. Epistaxis (Greek for
Epistaxis in children: approach and management Jacques Viljoen (CME, Nov/Dec 2003, Vol 21, No 11.) Nose bleeds can be intimidating for the child, the parents and the doctor alike. Epistaxis (Greek for
Head and Neck Examination
 Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
How to Do a Subacromial Shoulder Injection
 How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
How to Do a Subacromial Shoulder Injection UCSF Primary Care Sports Medicine Conference 2018 Carlin Senter, MD Associate Professor Co-Director UCSF Sports Concussion Program Primary Care Sports Medicine
Education for Self Administration of Intravenous Therapy HOME IV THERAPY PICC. Portacath
 HOME IV THERAPY PICC Portacath Who To contact Cardio-Respiratory Integrated Specialist Services (CRISS) Office hours 0800 1630 hours Ph: 364 0167 Weekends and after hours, phone Christchurch Hospital operator
HOME IV THERAPY PICC Portacath Who To contact Cardio-Respiratory Integrated Specialist Services (CRISS) Office hours 0800 1630 hours Ph: 364 0167 Weekends and after hours, phone Christchurch Hospital operator
RAPID RHINO With CMC Technology. Moisture matters. Naturally derived, exclusive CMC technology designed to create a moist environment.
 RAPID RHINO With CMC Technology Moisture matters. Naturally derived, exclusive CMC technology designed to create a moist environment. PN 83763 Rev. A CMC Brochure_final.indd 1 1/19/217 4:38:18 PM The RAPID
RAPID RHINO With CMC Technology Moisture matters. Naturally derived, exclusive CMC technology designed to create a moist environment. PN 83763 Rev. A CMC Brochure_final.indd 1 1/19/217 4:38:18 PM The RAPID
Case Presentation and Discussion on Posterior Neck Mass. Martin Joseph S. Cabahug
 Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
(SKILLS/HANDS-ON) Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC
 Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC") (SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
(SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Transfemoral Amputation
 Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma
Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma