while the absence of LGE-CMR may reduce the need for ICD implantation in patients with NIDM who are at low risk for future VF/VT or SCD.
|
|
|
- Meagan Horton
- 5 years ago
- Views:
Transcription
1 Midwall replacement fibrosis with late gadolinium enhancement LGE-CMR imaging as an independent predictor of mortality and utility of Cardiovascular Magnetic Resonance Image One-third of all patients with heart failure(hf) have nonischemic dilated cardiomyopathy (NIDM). Five-year mortality from NIDM is as high as 20% with sudden cardiac death (SCD) as the cause in 30% of the deaths. Currently, the LVEF is used as the main criteria to risk stratify patients requiring an implantable cardioverter defibrillator (ICD) to prevent SCD. However, LVEF does not necessarily reflect myocardial propensity for electrical instability leading to ventricular tachycardia (VT) or ventricular fibrillation (VF). Due to the differential risk in various subgroups of patients for arrhythmic death, it is important to identify appropriate patients for ICD implantation so that we can optimize healthcare resources and avoid the complications of ICDs in individuals who are unlikely to benefit. NIDCM is identified by progressive dilatation of the LV associated with the absence of obstructive CAD. Histopathologic studies have associated NIDCM with myocardial inflammation and fibrosis, which may be secondary to prior viral infection, toxins, iron overload, or other causes. In single-center experiences, the absence of infarct-appearing LGE of the myocardium excludes CAD as the cause of LV dysfunction. (McCrohon 2003) Occasionally, a more specific diagnosis of NIDCM can be reached by observing patchy or linear midwall enhancement that does not follow a coronary artery territory. Ventricular arrhythmia is a frequent cause of SCD in patients with NIDCM with a depressed LVEF. (Bardy2005) The risk of SCD in this population has been shown to be reduced with the implantation of an ICD. The severity of transmural involvement of LGE in patients with NIDCM has been linked with ventricular arrhythmias and may become a risk-stratifying tool in this population.(nazarian 2005) Memon et al. performed a systematic search and review of clinical trials of NIDM and the use of ICDs and cardiac magnetic resonance imaging(cmr) with late gadolinium enhancement (LGE-CMR) for risk stratification. LGE-CMR identifies patients with NIDM who are at high risk for SCD and enables optimized patient selection for ICD placement,
2 while the absence of LGE-CMR may reduce the need for ICD implantation in patients with NIDM who are at low risk for future VF/VT or SCD. (Memon 2016) LGE-CMR is a predictor of adverse cardiovascular outcomes in patients with NICM. However, these findings are limited by single-center studies, small sample sizes, and low event rates. Kuruvilla et al. performed a meta-analysis to evaluate the prognostic role of LGE-CMR imaging in patients with NICM. PubMed, Cochrane CENTRAL, and EMBASE were searched for studies looking at the prognostic value of LGE-CMR in patients with NICM. The primary end points included all-cause mortality, HF hospitalization, and a composite end point of SCD or aborted SCD. Pooling of odds ratios was performed using a random-effect model, and annualized event rates were assessed. Data were included from 9 studies with a total of 1488 patients and a mean follow-up of 30 months. Patients had a mean age of 52 years, 67% were men, and the average LVEF was 37% on CMR. LGE was present in 38% of patients. Patients with LGE-CMR had increased overall mortality, HF hospitalization, and SCD/aborted SCD compared with those without LGE-CMR. The annualized event rates for mortality were 4.7% for LGE-CMR + subjects versus 1.7% for LGE-CMR - subjects (P=0.01), 5.03% versus 1.8% for HF hospitalization, and 6.0% versus 1.2% for SCD/aborted SCD. They concluded that LGE-CMR in patients with NICM is associated with increased risk of all-cause mortality, HF hospitalization, and SCD. Detection of LGE-CMR has excellent prognostic characteristics and may help guide risk stratification and management in patients with NICM. (Kuruvilla 2014) Risk stratification of patients with NIDC is primarily based on LVEF. Superior prognostic factors may improve patient selection for ICDs and other management decisions. Prospective, longitudinal study of 472 patients with NIDC referred to a UK center for CMR between November 2000 and December 2008 after presence and extent of midwall replacement fibrosis were determined. Patients were followed up through December Primary end point was all-cause mortality. Secondary end points included cardiovascular mortality or cardiac transplantation; an arrhythmic composite of SCD or aborted SCD (appropriate ICD shock, nonfatal VF, or S-VF); and a composite of HF death, HF hospitalization, or cardiac transplantation. Assessment of midwall fibrosis with LGE-CMR imaging provided independent prognostic information beyond LVEF in patients with NIDC.
3 The role of LGE-CMR in the risk stratification of NIDC requires further investigation. (Gulati 2013) Neilan et al studies sought to determine whether the extent of late gadolinium enhancement (LGE-CMR) can provide additive prognostic information in patients with a NIDC with an indication for ICD therapy for the primary prevention of SCD. Data suggest that the presence of LGE-CMR is a strong discriminator of events in patients with NIDC. Limited data exist on the role of LGE-CMR quantification. The extent of LGE-CMR and clinical follow-up were assessed in 162 patients with NIDC prior to ICD insertion for primary prevention of SCD. LGE-CMR extent was quantified using both the standard deviation-based (2-SD) method and the full-width half-maximum (FWHM) method. They al studied 162 patients with NIDC (65% male; mean age: 55 years LVEF: 26 ± 8% and followed up for major adverse cardiac events (MACE), including cardiovascular death and appropriate ICD therapy, for a mean of 29 ± 18 months. Annual MACE rates were substantially higher in patients with LGE-CMR (24%) than in those without LGE-CMR (2%). By univariate association, the presence and the extent of LGE-CMR demonstrated the strongest associations with MACE; LGE extent, HR: 1.15 per 1% increase in volume of LGE-CMR. Multivariate analyses showed that LGE-CMR extent was the strongest predictor in the best overall model for MACE, and a 7-fold hazard was observed per 10% LGE extent after adjustments for patient age, sex, and LVEF. LGE-CMR quantitation by 2-SD and FWHM both demonstrated robust prognostic association, with the highest MACE rate observed in patients with LGE involving >6.1% of LV myocardium. They concluded that LGE-CMR extent may provide further risk stratification in patients with NIDC with a current indication for ICD implantation for the primary prevention of SCD. Strategic guidance on ICD therapy by cardiac magnetic resonance in patients with NIDC warrants further study. ( Neilan 2013) Figure 1 Table 1 Sequence name Sequence function

4 Cine SSFP or fast gradient echo T1-weighted black blood T2-weighted black blood Inversion recovery late enhancement Myocardial structure and function Myocardial fat imaging Tissue edema Late gadolinium enhancement T2* Myocardial iron content Typical CMR sequences for evaluation of cardiomyopathies Table 2 CMR approach to cardiomyopathies Sequences
5 The application of CMR in the diagnostic evaluation of cardiomyopathy of unknown origin has been identified as an appropriate use of this technology (Hendel 2006). The unique features of CMR, including exceptional temporal and spatial resolution, tissue characterization, perfusion analysis, and ability to image in any tissue plane, make it an ideal tool for use in this clinical setting. Cardiomyopathy sequencing protocols have been published to standardize and streamline the approach to the clinical scan( An experienced staff can perform a thorough study within 30 minutes and provide a multimodality cardiac survey to help the clinician determine therapies that may ultimately improve patient outcomes. Mordi et al. studied the incremental prognostic value of global circumferential strain (GCS), as measured using CMR tagging, in addition to baseline clinical characteristics, LVEF, and LGE-CMR, in the prediction of MACE in an unselected cohort of patients. LVEF is a powerful predictor of mortality and is used for guiding treatment decisions. It is, however, subject to limitations. The value of GCS measured by CMR tagging in patients with suspected cardiac disease has not been fully explored despite its being considered as the gold standard noninvasive method of assessment of LV deformation. They prospectively evaluated data from 539 consecutive patients referred for CMR who underwent a CMR protocol that included cine imaging, tagging, and LGE. The primary endpoint was the prevalence of MACE, defined as a composite of all-cause mortality, HF-related hospitalization, and aborted SCD. MACE occurred in 62 of 539 patients (11.5%) over a mean follow-up period of 2.2 years. History of coronary heart disease (CHD) and β-blocker use were both significant clinical predictors of adverse outcomes. All 3 CMR parameters were significant multivariate predictors of the primary outcome when added to significant clinical predictors (LVEF, hazard ratio [HR]: 0.96 [95% confidence interval [CI]: 0.94 to 0.99; p = 0.005]; presence of LGE, HR: 2.07 [95% CI: 1.03 to 4.14; p = 0.04]; GCS, HR: 1.11 [95% CI: 1.02 to 1.21; p = 0.041]). Global chi-square increased significantly with the addition of both LGE-CMR, and GCS. Both the presence of LGE-CMR and reduced GCS had independent prognostic value in the overall cohort. Patients with LVEF 35% but LGE-CMR present and reduced GCS had a poor outcome similar to that in those with LVEF <35%. The authors found, in a large-scale cohort of patients, that GCS, in addition to clinical variables, LVEF, and LGE-CMR, had incremental independent prognostic value. This measure could
6 provide further risk stratification, especially in patients with mild LV impairment. (Mordi 2015) Current risk stratification for SCD in (NIDC relies on LV dysfunction, a poor marker of ventricular electrical instability. Contrast- LGE-CMR has the ability to accurately identify and quantify ventricular myocardial fibrosis To evaluate the impact of the presence and amount of myocardial fibrosis on arrhythmogenic risk prediction in NIDC Perazzolo Marra et al studied 137 consecutive patients with angiographically proven NIDC were enrolled for this study. All patients were followed up for a combined arrhythmic end point including sustained S-VT, appropriate ICD intervention, VF, and SCD. LV-LGE was identified in 76 (55.5%) patients. During a median follow-up of 3 years, the combined arrhythmic end point occurred in 22 (16.1%) patients: 8 (5.8%) S-VT, 9 (6.6%) appropriate ICD intervention, either against VF (n = 5; 3.6%) or VT (n = 4; 2.9%), 3 (2.2%) aborted SCD, and 2 (1.5%) died suddenly. Kaplan-Meier analysis revealed a significant correlation between the LV-LGE presence (not the amount and distribution) and malignant arrhythmic events. In univariate Cox regression analysis, LV-LGE (hazard ratio [HR] 4.17; 95% confidence interval [CI] ; P =.005) and LBBB (HR 2.43; 95% CI ; P =.048) were found to be associated with arrhythmias. In multivariable analysis, the presence of LGE was the only independent predictor of arrhythmias. The authors concluded that LV-LGE is a powerful and independent predictor of malignant arrhythmic prognosis, while its amount and distribution do not provide additional prognostic value. Contrastenhanced MCR may contribute to identify candidates for ICD therapy not fulfilling the current criteria based on LVEF.( Perazzolo Marra 2014) Ventricular tachycardia in patients with cardiomyopathy originates in scar tissue. Intramural or epicardial scar may result in ineffective ablation if mapping and ablation are limited to the endocardium. Njeim et al. investigate whether preprocedural CMR is beneficial in patients with failed endocardial VT ablations in determining an appropriate ablation strategy. A CMR was performed in 20 patients with a failed ablation procedure and cardiomyopathy (NIDCM n = 12, ischemic n = 8). A subsequent ablation strategy was determined by a LGE-CMR and an epicardial subxyphoid access was planned only in patients with epicardial or intramural free-wall scar. CMRs were performed in all patients with or without an ICD. The location of
7 scar tissue in the CMR predicted the origin of VT in all patients. In 9/20 patients an epicardial procedure was performed based on the result of the CMR. An endocardial procedure was performed in the remaining 11 patients who had either endocardial or septal scarring and one patient in whom the CMR only showed artifact. Five patients remained inducible postablation and 4 patients had VT recurrence within a follow-up period of 17 ± 22 months. All of the latter patients had an intramural scar pattern. They concluded that Imaging with CMR prior to VT ablation in patients with previously failed endocardial ablation procedures is beneficial in identifying an ablation strategy, helps to focus on an area of interest intraprocedurally, and provides valuable outcomes information. (Njeim 2016) Dweck et al studied the prognostic significance of midwall and infarct patterns of LGE-CMR in aortic stenosis. Myocardial fibrosis occurs in aortic stenosis as part of the hypertrophic response. It can be detected by LGE-CMR, which is associated with an adverse prognosis in a range of other cardiac conditions.between January 2003 and October 2008, consecutive patients with moderate or severe aortic stenosis undergoing CMR with administration of gadolinium contrast were enrolled into a registry. Patients were categorized into absent, midwall, or infarct patterns of LGE-CMR by blinded independent observers. Patient followup was completed using patient questionnaires, source record data, and the National Strategic Tracing Service. A total of 143 patients (age 68 ± 14 years; 97 male) were followed up for 2.0 ± 1.4 years. Seventy-two underwent aortic valve replacement, and 27 died (24 cardiac, 3 sudden cardiac deaths). Compared with those with no LGE-CMR (n = 49), univariate analysis revealed that patients with midwall fibrosis (n = 54) had an 8-fold increase in allcause mortality despite similar aortic stenosis severity and CAD burden. Patients with an myocardial infarct pattern (n = 40) had a 6-fold increase. Midwall fibrosis (hazard ratio: 5.35; 95% confidence interval: 1.16 to 24.56; p = 0.03) and LVEF (hazard ratio: 0.96; 95% confidence interval: 0.94 to 0.99; p = 0.01) were independent predictors of all-cause mortality by multivariate analysis. Midwall replacement fibrosis with late gadolinium enhancement LGE-CMR imaging was an independent predictor of mortality in patients with moderate and severe aortic stenosis. It has incremental prognostic value to ejection fraction and may provide a useful method of risk stratification. (Dweck 2011) Figure 2 Figure 1

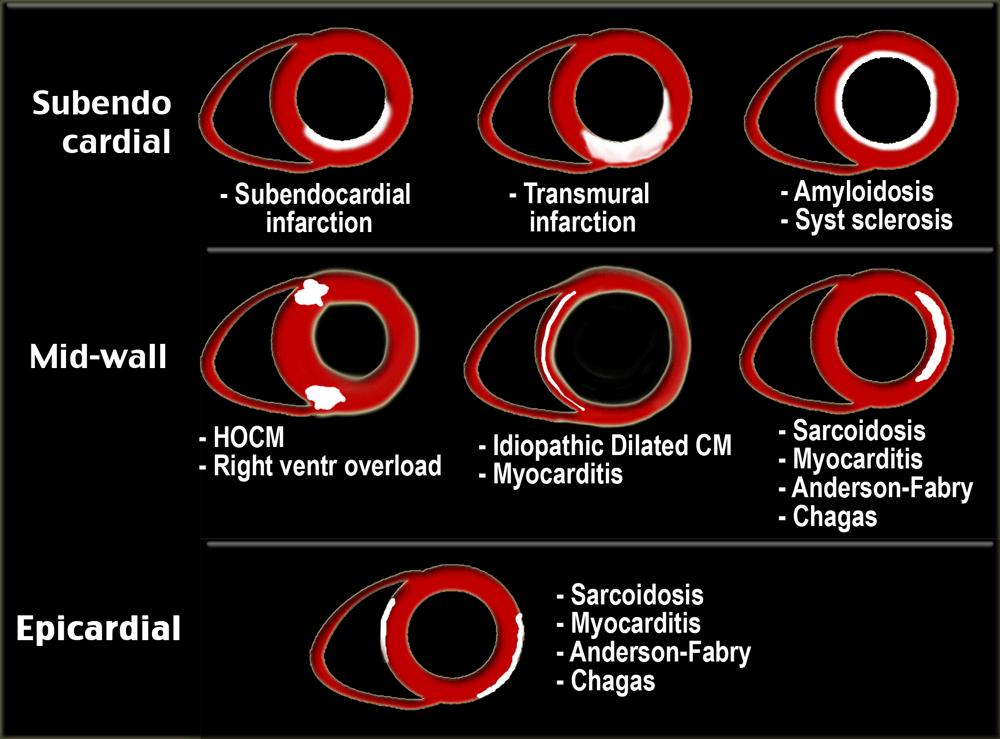
8 A pattern-based approach to assessment of delayed enhancement in NIDC using CMR imaging. (Cummings 2009; Karamitsos2009)


9 Figure 2 Several patterns of LGE-CMR can be observed in patients with severe aortic stenosis, from a no LGE, to b infarct-like replacement fibrosis with subendocardial scar, or c f midwall fibrosis. The arrows indicate the presence of LGE.
10 Figure 3


11 NIDM Cardiac Magnetic Resonance features

12

13

14 Summary Determination of exact etiology of cardiomyopathy can be difficult but remains important for both treatment and prognosis. CMR imaging allows comprehensive assessment of patients suspected to have NIDM and is therefore being increasingly used in diagnosis and follow-up of these patients. CMR offers a comprehensive assessment of HF patients and is now the gold standard imaging technique to assess myocardial anatomy, regional and global function, and viability. Furthermore, it allows assessment of perfusion and acute tissue injury (edema and necrosis), whereas in nonischemic HF, fibrosis, infiltration, and iron overload can be detected. LGE-CMR extent may provide further risk stratification in patients with NIDC with a current indication for ICD implantation for the primary prevention of SCD. Conclusions CMR has become one of the most accurate techniques (the gold standard) in quantification volumes, mass, study of the right ventricle, serial assessment of biventricular structure, size, and function (anatomy, LV/RV volumes, global and regional systolic
15 function, mass and the most complete in the diagnosis of ischemic diseases, NIDM (differentiation of ischemic versus NIDM), determination of the location and extent of acute (including no-reflow regions) and chronic myocardial necrosis, viability assessment before revascularization (LGE or low-dose dobutamine, determination of the area at risk in patients with acute myocardial infarction and the salvageable area post-revascularization with percutaneous coronary intervention, identification of the presence and quantification of the extent of inducible ischemia (vasodilator perfusion or high-dose dobutamine stress CMR), ARVC/D, LV noncompaction, HCM, Anderson-Fabry disease, cardiac sarcoidosis, amyloidosis, iron overload cardiomyopathy, evaluation of suspected anomalous coronary origins (MR coronary angiography) and others congenital diseases, patients with technically limited images from echocardiogram, Discordant information that is clinically significant from prior tests and assessment of mechanical dyssynchrony before resynchronization therapy and risk stratify patients requiring an ICD. Finally, in patients with structural heart disease and previously failed endocardial VT ablation procedures, preprocedural cardiac MRIs are helpful in identifying an ablation strategy, even in patients with previously implanted ICDs References
16 1. Bardy GH, Lee KL, Mark DB, et al. Amiodarone or implantable cardioverterdefibrillator for congestive heart failure. N Engl J Med. 2005; 352: Cummings KW et al. A Pattern-based Approach to Assessment of Delayed Enhancement in Nonischemic Cardiomyopathy at MR Imaging. Radiographics; January February 2009; 29: Dweck MR, Joshi S, Murigu T, et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis.j Am Coll Cardiol Sep 13;58(12): Gulati A, Jabbour A, Ismail TF, et al. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. JAMA Mar 6;309(9): Hendel RC, Patel MR, Kramer CM, et al. ACCF/ACR/ SCCT/SCMR/ASNC/ NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48: Karamitsos TD, Francis JM, Myerson S, Selvanayagam JB, Phil D, Neubauer S. The Role of Cardiovascular Magnetic Resonance Imaging in Heart Failure. J. Am. Coll. Cardiol. 2009; 54(15): Kuruvilla S, Adenaw N, Katwal AB, Lipinski MJ, Kramer CM, Salerno M. Late gadolinium enhancement on cardiac magnetic resonance predicts adverse cardiovascular outcomes in nonischemic cardiomyopathy: a systematic review and meta-analysis. Circ Cardiovasc Imaging Mar;7(2): McCrohon JA, Moon JC, Prasad SK, et al. Differentiation of heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-enhanced cardiovascular magnetic resonance. Circulation. 2003;108:54 59.
17 9. Memon S, Ganga HV, Kluger J.Late Gadolinium Enhancement in Patients with Nonischemic Dilated Cardiomyopathy.Pacing Clin Electrophysiol Jul;39(7): doi: /pace doi: /pace Mordi I, Bezerra H, Carrick D, Tzemos N. The Combined Incremental Prognostic Value of LVEF, Late Gadolinium Enhancement, and Global Circumferential Strain Assessed by CMR.JACC Cardiovasc Imaging May;8(5): Nazarian S, Bluemke DA, Lardo AC, et al. Magnetic resonance assessment of the substrate for inducible ventricular tachycardia in nonischemic cardiomyopathy. Circulation. 2005;112: Neilan TG, Coelho-Filho OR, Danik SB, et al. CMR quantification of myocardial scar provides additive prognostic information in nonischemic cardiomyopathy.jacc Cardiovasc Imaging Sep;6(9): Njeim M, Yokokawa M, Frank L, Crawford T, Good, Morady F, Bogun F. Value of Cardiac Magnetic Resonance Imaging in Patients With Failed Ablation Procedures for Ventricular Tachycardia. J Cardiovasc Electrophysiol Feb;27(2): Perazzolo Marra M, De Lazzari M, Zorzi A, et al.impact of the presence and amount of myocardial fibrosis by cardiac magnetic resonance on arrhythmic outcome and sudden cardiac death in nonischemic dilated cardiomyopathy.heart Rhythm May;11(5):
Advanced MR Imaging in Myocarditis
 Naeem Merchant MD FRCP Professor of Medicine Department of Radiology Department of Cardiac Sciences Cumming School of Medicine University of Calgary Advanced MR Imaging in Myocarditis The Lake Louise Criteria
Naeem Merchant MD FRCP Professor of Medicine Department of Radiology Department of Cardiac Sciences Cumming School of Medicine University of Calgary Advanced MR Imaging in Myocarditis The Lake Louise Criteria
Role of CMR in heart failure and cardiomyopathy
 Role of CMR in heart failure and cardiomyopathy Hajime Sakuma Department of Radiology, Mie University Late gadolinium enhancement (LGE) LGE MRI can demonstrate site of necrosis, fibrosis or deposition
Role of CMR in heart failure and cardiomyopathy Hajime Sakuma Department of Radiology, Mie University Late gadolinium enhancement (LGE) LGE MRI can demonstrate site of necrosis, fibrosis or deposition
Cardiac MRI: Cardiomyopathy
 Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD I do not have any relevant financial relationships with any commercial interests Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD Duke University Medical
Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD I do not have any relevant financial relationships with any commercial interests Cardiac MRI: Cardiomyopathy Laura E. Heyneman, MD Duke University Medical
What s New in Cardiac MRI
 What s New in Cardiac MRI Katie M. Hawthorne, MD Director, Cardiac MRI Main Line Health Philadelphia Cardiovascular Summit November 18, 2017 Cardiac MRI: Disclosure 2 Disclosures No financial disclosures
What s New in Cardiac MRI Katie M. Hawthorne, MD Director, Cardiac MRI Main Line Health Philadelphia Cardiovascular Summit November 18, 2017 Cardiac MRI: Disclosure 2 Disclosures No financial disclosures
Why Cardiac MRI? Presented by:
 Why Cardiac MRI? Presented by: Lisa G. Carkner, MD, FACC 1 Disclosures I have no financial disclosures Objectives Review basic principles of Cardiac MRI. What patient characteristics do I need to consider
Why Cardiac MRI? Presented by: Lisa G. Carkner, MD, FACC 1 Disclosures I have no financial disclosures Objectives Review basic principles of Cardiac MRI. What patient characteristics do I need to consider
Newly Diagnosed Heart Failure patient: When to Order an MRI and Why
 Newly Diagnosed Heart Failure patient: When to Order an MRI and Why Jennifer Dickerson MD Assistant Professor of Clinical Internal Medicine Director, The Ohio State University Echocardiography Laboratory
Newly Diagnosed Heart Failure patient: When to Order an MRI and Why Jennifer Dickerson MD Assistant Professor of Clinical Internal Medicine Director, The Ohio State University Echocardiography Laboratory
Imaging and heart failure
 Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
Imaging and heart failure Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston, St Jude, BMS imaging, GE Healthcare,
CT for Myocardial Characterization of Cardiomyopathy. Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea
 CT for Myocardial Characterization of Cardiomyopathy Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea Cardiomyopathy Elliott P et al. Eur Heart J 2008;29:270-276 The European Society
CT for Myocardial Characterization of Cardiomyopathy Byoung Wook Choi, Yonsei University Severance Hospital, Seoul, Korea Cardiomyopathy Elliott P et al. Eur Heart J 2008;29:270-276 The European Society
Cardiac Stress MRI: Detection of Ischemia. Disclosures: Dobutamine Stress MR. April 28, 2018
 Cardiac MRI: Detection of Ischemia Cardiac MRI in Today s Clinical Practice Foundations of Cardiovascular Magnetic Resonance Daniel C. Lee, MD, MSc Assistant Professor of Medicine and Radiology Co-Director,
Cardiac MRI: Detection of Ischemia Cardiac MRI in Today s Clinical Practice Foundations of Cardiovascular Magnetic Resonance Daniel C. Lee, MD, MSc Assistant Professor of Medicine and Radiology Co-Director,
Cardiac magnetic resonance imaging in rheumatoid arthritis: promising or misleading? Sophie Mavrogeni MD FESC
 Cardiac magnetic resonance imaging in rheumatoid arthritis: promising or misleading? Sophie Mavrogeni MD FESC Onassis Cardiac Surgery Center Athens Greece Nothing to disclose Financial disclosure Cardiac
Cardiac magnetic resonance imaging in rheumatoid arthritis: promising or misleading? Sophie Mavrogeni MD FESC Onassis Cardiac Surgery Center Athens Greece Nothing to disclose Financial disclosure Cardiac
Summary, conclusions and future perspectives
 Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
Summary, conclusions and future perspectives Summary The general introduction (Chapter 1) of this thesis describes aspects of sudden cardiac death (SCD), ventricular arrhythmias, substrates for ventricular
Midwall Fibrosis and 5-Year Outcome In Patients With Moderate and Severe Aortic Stenosis Brief Title: Midwall fibrosis in aortic stenosis
 Midwall Fibrosis and 5-Year Outcome In Patients With Moderate and Severe Aortic Stenosis Brief Title: Midwall fibrosis in aortic stenosis Vassilios S Vassiliou, MD 1,2,3, Aris Perperoglou, PhD 4, Claire
Midwall Fibrosis and 5-Year Outcome In Patients With Moderate and Severe Aortic Stenosis Brief Title: Midwall fibrosis in aortic stenosis Vassilios S Vassiliou, MD 1,2,3, Aris Perperoglou, PhD 4, Claire
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure
 Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure Wojciech Zareba Postinfarction patients with left ventricular dysfunction are at increased risk
Implantable Cardioverter Defibrillator Therapy in MADIT II Patients with Signs and Symptoms of Heart Failure Wojciech Zareba Postinfarction patients with left ventricular dysfunction are at increased risk
Cardiac MRI: Clinical Application to Disease
 Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
علم االنسان ما لم يعلم
 In the name of Allah, the Beneficiate, the Merciful ق ال هللا تعالي: 5 الدى علم بالق لم 4 علم االنسان ما لم يعلم سورة العلق It is He (Allah), Who has taught by the pen He has taught man which he did not
In the name of Allah, the Beneficiate, the Merciful ق ال هللا تعالي: 5 الدى علم بالق لم 4 علم االنسان ما لم يعلم سورة العلق It is He (Allah), Who has taught by the pen He has taught man which he did not
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Cardiac Imaging. Kimberly Delcour, DO, FACC. Mahi Ashwath, MD, FACC, FASE. Director, Cardiac CT. Director, Cardiac MRI
 Cardiac Imaging Kimberly Delcour, DO, FACC Director, Cardiac CT Mahi Ashwath, MD, FACC, FASE Director, Cardiac MRI Cardiac Imaging Discuss the clinical applications of and indications for: Cardiac CT Nuclear
Cardiac Imaging Kimberly Delcour, DO, FACC Director, Cardiac CT Mahi Ashwath, MD, FACC, FASE Director, Cardiac MRI Cardiac Imaging Discuss the clinical applications of and indications for: Cardiac CT Nuclear
Ventricular Tachycardia Ablation. Saverio Iacopino, MD, FACC, FESC
 Ventricular Tachycardia Ablation Saverio Iacopino, MD, FACC, FESC ü Ventricular arrhythmias, both symptomatic and asymptomatic, are common, but syncope and SCD are infrequent initial manifestations of
Ventricular Tachycardia Ablation Saverio Iacopino, MD, FACC, FESC ü Ventricular arrhythmias, both symptomatic and asymptomatic, are common, but syncope and SCD are infrequent initial manifestations of
DELAYED ENHANCEMENT IMAGING IN CHILDREN
 NASCI 38 TH ANNUAL MEENG, SEATLE October 3-5, 21 1. DELAYED ENHANCEMENT IN CHILDREN Shi-Joon Yoo, MD Lars Grosse-Wortmann, MD University of Toronto Canada -1. 1. 1. Magnitude image Magnitude images -1.
NASCI 38 TH ANNUAL MEENG, SEATLE October 3-5, 21 1. DELAYED ENHANCEMENT IN CHILDREN Shi-Joon Yoo, MD Lars Grosse-Wortmann, MD University of Toronto Canada -1. 1. 1. Magnitude image Magnitude images -1.
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Πρόληψη του ΑΚΘ σε ασθενείς με μη-ισχαιμική μυοκαρδιοπάθεια:
 Πρόληψη του ΑΚΘ σε ασθενείς με μη-ισχαιμική μυοκαρδιοπάθεια: Νεώτερα δεδομένα στη διαστρωμάτωση κινδύνου Εμμ. Μ. Κανουπάκης MD, PhD, FESC Πανεπιστημιακό Νοσοκομείο Ηρακλείου NIDCM Presence of LV dilatation
Πρόληψη του ΑΚΘ σε ασθενείς με μη-ισχαιμική μυοκαρδιοπάθεια: Νεώτερα δεδομένα στη διαστρωμάτωση κινδύνου Εμμ. Μ. Κανουπάκης MD, PhD, FESC Πανεπιστημιακό Νοσοκομείο Ηρακλείου NIDCM Presence of LV dilatation
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy
 Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Advanced Imaging MRI and CTA
 Advanced Imaging MRI and CTA Who and why may benefit. Matthew W. Martinez, M.D. FACC Lehigh Valley Health Network Director, Cardiovascular Imaging Learning Objectives Review basics of CMR and CTA Review
Advanced Imaging MRI and CTA Who and why may benefit. Matthew W. Martinez, M.D. FACC Lehigh Valley Health Network Director, Cardiovascular Imaging Learning Objectives Review basics of CMR and CTA Review
Evaluation of Sum Absolute QRST Integral as a Clinical Marker for Ventricular Arrhythmias. Markus Kowalsky Group 11
 Evaluation of Sum Absolute QRST Integral as a Clinical Marker for Ventricular Arrhythmias Markus Kowalsky Group 11 Selected Paper Ventricular arrhythmia is predicted by sum absolute QRST integral but not
Evaluation of Sum Absolute QRST Integral as a Clinical Marker for Ventricular Arrhythmias Markus Kowalsky Group 11 Selected Paper Ventricular arrhythmia is predicted by sum absolute QRST integral but not
Original Article Fragmented QRS as a Predictor of Appropriate Implantable Cardioverter-defibrillator Therapy
 4 Original Article Fragmented QRS as a Predictor of Appropriate Implantable Cardioverter-defibrillator Therapy Sirin Apiyasawat, Dujdao Sahasthas, Tachapong Ngarmukos, Pakorn Chandanamattha, Khanchit Likittanasombat
4 Original Article Fragmented QRS as a Predictor of Appropriate Implantable Cardioverter-defibrillator Therapy Sirin Apiyasawat, Dujdao Sahasthas, Tachapong Ngarmukos, Pakorn Chandanamattha, Khanchit Likittanasombat
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
Cardiac MRI: Clinical Application to Disease
 Cardiac MRI: Clinical Application to Disease Stacy Rissing, MD! Cardiothoracic imaging, Indiana University! Outline Imaging planes Disease findings Pulse sequences used for each indication Pathophysiology
Cardiac MRI: Clinical Application to Disease Stacy Rissing, MD! Cardiothoracic imaging, Indiana University! Outline Imaging planes Disease findings Pulse sequences used for each indication Pathophysiology
The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease
 The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease G.P. Spanos, MSc, Phd Head of CardioVascular Imaging Tomographia Diagnostic Center Cardiovascular magnetic
The role of Magnetic Resonance Imaging in the diagnosis of viability & Coronary Artery Disease G.P. Spanos, MSc, Phd Head of CardioVascular Imaging Tomographia Diagnostic Center Cardiovascular magnetic
Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures?
 Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center
 CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
CMR Perfusion and Viability A STICH Out of Time? Sung A Chang Department of Internal Medicine, Division of Cardiology, Sungkyunkwan University School of Medicine, Samsung Medical Center Can Imaging Improve
ICD THERAPIES: are they harmful or just high risk markers?
 ICD THERAPIES: are they harmful or just high risk markers? Konstantinos P. Letsas, MD, PhD, FESC LAB OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL ATHENS ICD therapies are common In a meta-analysis
ICD THERAPIES: are they harmful or just high risk markers? Konstantinos P. Letsas, MD, PhD, FESC LAB OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL ATHENS ICD therapies are common In a meta-analysis
A Light in the Dark: Cardiac MRI and Risk Mitigation. J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED)
") A Light in the Dark: Cardiac MRI and Risk Mitigation J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED) Dr. Mikolich has NO financial disclosures relative to
A Light in the Dark: Cardiac MRI and Risk Mitigation J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED) Dr. Mikolich has NO financial disclosures relative to
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες
 Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Εμφύτευση απινιδωτών για πρωτογενή πρόληψη σε ασθενείς που δεν περιλαμβάνονται στις κλινικές μελέτες Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides
 Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
Cardiac Devices CRT,ICD: Who is and is not a Candidate? Who Decides Colette Seifer MB(Hons) FRCP(UK) Associate Professor, University of Manitoba, Cardiologist, Cardiac Sciences Program, St Boniface Hospital
ADVANCED CARDIOVASCULAR IMAGING. Medical Knowledge. Goals and Objectives PF EF MF LF Aspirational
 Medical Knowledge Goals and Objectives PF EF MF LF Aspirational Know the basic principles of magnetic resonance imaging (MRI) including the role of the magnetic fields and gradient coil systems, generation
Medical Knowledge Goals and Objectives PF EF MF LF Aspirational Know the basic principles of magnetic resonance imaging (MRI) including the role of the magnetic fields and gradient coil systems, generation
Late Gadolinium Enhancement by Cardiac Magnetic Resonance Imaging and Major Adverse Coronary Events
 Pacific University CommonKnowledge School of Physician Assistant Studies College of Health Professions Summer 8-12-2017 Late Gadolinium Enhancement by Cardiac Magnetic Resonance Imaging and Major Adverse
Pacific University CommonKnowledge School of Physician Assistant Studies College of Health Professions Summer 8-12-2017 Late Gadolinium Enhancement by Cardiac Magnetic Resonance Imaging and Major Adverse
CLINICAL STUDY. remain incomplete and novel non-invasive strategies are needed in order to effectively identify high-risk HCM patients.
 CLINICAL STUDY Quantitative Differentiation of LV Myocardium with and without Layer-Specific Fibrosis Using MRI in Hypertrophic Cardiomyopathy and Layer-Specific Strain TTE Analysis Nobusada Funabashi,
CLINICAL STUDY Quantitative Differentiation of LV Myocardium with and without Layer-Specific Fibrosis Using MRI in Hypertrophic Cardiomyopathy and Layer-Specific Strain TTE Analysis Nobusada Funabashi,
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D.
 PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
PVCs: Do they cause Cardiomyopathy? Raed Abu Sham a, M.D. Cardiologist and Electrophysiologist No conflict of interest related to this presentation Objectives 1. PVCs are benign. What is the Evidence?
1. LV function and remodeling. 2. Contribution of myocardial ischemia due to CAD, and
 1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
1 The clinical syndrome of heart failure in adults is commonly associated with the etiologies of ischemic and non-ischemic dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertensive heart disease,
Prevention of sudden cardiac death: With an emphasis on sudden cardiac death from ventricular arrhythmias
 Prevention of sudden cardiac death: With an emphasis on sudden cardiac death from ventricular arrhythmias The Toronto ACS Summit Toronto, March 1, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology
Prevention of sudden cardiac death: With an emphasis on sudden cardiac death from ventricular arrhythmias The Toronto ACS Summit Toronto, March 1, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology
Ventricular Tachycardia Substrate. For the ablationist. Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia
 Ventricular Tachycardia Substrate For the ablationist Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia Two Attitudes of Ventricular Tachycardia Ablation 1 2C:\Documents
Ventricular Tachycardia Substrate For the ablationist Stanley Tung, MD FRCPC Arrhythmia Service/St Paul Hospital University of British Columbia Two Attitudes of Ventricular Tachycardia Ablation 1 2C:\Documents
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia
 The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
The Therapeutic Role of the Implantable Cardioverter Defibrillator in Arrhythmogenic Right Ventricular Dysplasia By Sandeep Joshi, MD and Jonathan S. Steinberg, MD Arrhythmia Service, Division of Cardiology
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE
 A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
A Square Peg in a Round Hole: CRT IN PAEDIATRICS AND CONGENITAL HEART DISEASE Adele Greyling Dora Nginza Hospital, Port Elizabeth SA Heart November 2017 What are the guidelines based on? MADIT-II Size:
Usefulness of Delayed Enhancement by Magnetic Resonance Imaging in Hypertrophic Cardiomyopathy as a Marker of Disease and Its Severity
 Usefulness of Delayed Enhancement by Magnetic Resonance Imaging in Hypertrophic Cardiomyopathy as a Marker of Disease and Its Severity G.D.Aquaro, MD Fondazione G.Monasterio Regione Toscana/CNR Pisa, Italy
Usefulness of Delayed Enhancement by Magnetic Resonance Imaging in Hypertrophic Cardiomyopathy as a Marker of Disease and Its Severity G.D.Aquaro, MD Fondazione G.Monasterio Regione Toscana/CNR Pisa, Italy
Detection and Assessment of MI: Use of Imaging Methods. Robert O. Bonow, M.D.
 Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. No Relationships to Disclose Expert Consensus Document
Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. No Relationships to Disclose Expert Consensus Document
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro
 Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro Jerónimo Farré MD, Madrid, ES AF: the kingdom of wishful thinking In AF we
Progression of atrial fibrillation: can we prevent it? Early catheter ablation will stop progression of atrial fibrillation pro Jerónimo Farré MD, Madrid, ES AF: the kingdom of wishful thinking In AF we
Defibrillation threshold testing should no longer be performed: contra
 Defibrillation threshold testing should no longer be performed: contra Andreas Goette St. Vincenz-Hospital Paderborn Dept. of Cardiology and Intensive Care Medicine Germany No conflict of interest to disclose
Defibrillation threshold testing should no longer be performed: contra Andreas Goette St. Vincenz-Hospital Paderborn Dept. of Cardiology and Intensive Care Medicine Germany No conflict of interest to disclose
Journal of the American College of Cardiology Vol. 37, No. 2, by the American College of Cardiology ISSN /01/$20.
 Journal of the American College of Cardiology Vol. 37, No. 2, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)01133-5 Coronary
Journal of the American College of Cardiology Vol. 37, No. 2, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)01133-5 Coronary
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
CMR stress Perfusion: what's new?
 CMR stress Perfusion: what's new? John P. Greenwood Professor of Cardiology, Leeds University, UK Consultant Cardiologist Leeds Teaching Hospitals NHS Trust, UK CMR: multi-parametric CMR: multi-parametric
CMR stress Perfusion: what's new? John P. Greenwood Professor of Cardiology, Leeds University, UK Consultant Cardiologist Leeds Teaching Hospitals NHS Trust, UK CMR: multi-parametric CMR: multi-parametric
General Cardiovascular Magnetic Resonance Imaging
 2 General Cardiovascular Magnetic Resonance Imaging 19 Peter G. Danias, Cardiovascular MRI: 150 Multiple-Choice Questions and Answers Humana Press 2008 20 Cardiovascular MRI: 150 Multiple-Choice Questions
2 General Cardiovascular Magnetic Resonance Imaging 19 Peter G. Danias, Cardiovascular MRI: 150 Multiple-Choice Questions and Answers Humana Press 2008 20 Cardiovascular MRI: 150 Multiple-Choice Questions
THE NEW PLACE OF CARDIAC MRI IN AERONAUTICAL FITNESS
 88 th ASMA ANNUAL SCIENTIFIC MEETING DENVER - CO April 30- May 4, 2017 THE NEW PLACE OF CARDIAC MRI IN AERONAUTICAL FITNESS S. BISCONTE (1), J. MONIN (2), N. HUIBAN (3), G. GUIU (2), S. NGUYEN (1), O.
88 th ASMA ANNUAL SCIENTIFIC MEETING DENVER - CO April 30- May 4, 2017 THE NEW PLACE OF CARDIAC MRI IN AERONAUTICAL FITNESS S. BISCONTE (1), J. MONIN (2), N. HUIBAN (3), G. GUIU (2), S. NGUYEN (1), O.
Current Indications for Cardiac MRI: What You See is What You Get?
 Current Indications for Cardiac MRI: What You See is What You Get? Javier Ganame, MD, PhD, FASE No disclosures Cardiology Update, Niagara, Sept 24th, 2016 The Ideal Diagnostic Technique Easy to apply Accurate
Current Indications for Cardiac MRI: What You See is What You Get? Javier Ganame, MD, PhD, FASE No disclosures Cardiology Update, Niagara, Sept 24th, 2016 The Ideal Diagnostic Technique Easy to apply Accurate
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy
 The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
The Role of Ventricular Electrical Delay to Predict Left Ventricular Remodeling With Cardiac Resynchronization Therapy Results from the SMART-AV Trial Michael R. Gold, MD, PhD, Ulrika Birgersdotter-Green,
Cardiac MRI: Appropriateness. Scott Mattson, DO, FACC Lutheran Medical Group Fort Wayne, IN
 Cardiac MRI: Appropriateness Scott Mattson, DO, FACC Lutheran Medical Group Fort Wayne, IN Approaches to Appropriateness The indication The patient The scanner and technologists The interpreting physician
Cardiac MRI: Appropriateness Scott Mattson, DO, FACC Lutheran Medical Group Fort Wayne, IN Approaches to Appropriateness The indication The patient The scanner and technologists The interpreting physician
Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία
 Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία Θεόδωρος. Καραμήτσος MD PhD Honorary Consultant in Cardiology University of Oxford Centre for Clinical Magnetic Resonance
Φαινόμενο No-Reflow. Απεικόνιση με CMR, κλινική συσχέτιση και προγνωστική σημασία Θεόδωρος. Καραμήτσος MD PhD Honorary Consultant in Cardiology University of Oxford Centre for Clinical Magnetic Resonance
Silvia G Priori MD PhD
 The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
The approach to the cardiac arrest survivor Silvia G Priori MD PhD Molecular Cardiology, IRCCS Fondazione Salvatore Maugeri Pavia, Italy AND Leon Charney Division of Cardiology, Cardiovascular Genetics
Synopsis of Management on Ventricular arrhythmias. M. Soni MD Interventional Cardiologist
 Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
Importance of CRT team for optimization of the results: a European point of view
 Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Importance of CRT team for optimization of the results: a European point of view Matteo Bertini, MD, PhD Arcispedale S. Anna Azienda Ospedaliero-Universitaria Cona-Ferrara No conflict of interest to declare
Myocardial viability testing. What we knew and what is new
 Myocardial viability testing. What we knew and what is new Dr B K S Sastry, MD, DM. CARE Hospitals, Hyderabad What is Viability Viability Dysfunctional myocardium subtended by diseased coronary arteries
Myocardial viability testing. What we knew and what is new Dr B K S Sastry, MD, DM. CARE Hospitals, Hyderabad What is Viability Viability Dysfunctional myocardium subtended by diseased coronary arteries
Cardial MRI; Approaching the Level of Gold Standard for Viability Assessment
 Cardial MRI; Approaching the Level of Gold Standard for Viability Assessment 용환석 고려대학교구로병원영상의학과 Viability Hibernating myocardium a state of myocardial hypocontractility during chronic hypoperfusion, in
Cardial MRI; Approaching the Level of Gold Standard for Viability Assessment 용환석 고려대학교구로병원영상의학과 Viability Hibernating myocardium a state of myocardial hypocontractility during chronic hypoperfusion, in
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Management of Syncope in Heart Failure. University of Iowa
 Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
A Light in the Dark: Cardiac MRI and Risk Mitigation. J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED)
") A Light in the Dark: Cardiac MRI and Risk Mitigation J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED) Dr. Mikolich has NO financial disclosures relative to
A Light in the Dark: Cardiac MRI and Risk Mitigation J. Ronald Mikolich MD Professor of Internal Medicine Northeast Ohio Medical University (NEOMED) Dr. Mikolich has NO financial disclosures relative to
Novel Approaches to VT Management Glenn M Polin MD
 Novel Approaches to VT Management Glenn M Polin MD Medical Director, Electrophysiology Laboratory John Ochsner Heart and Vascular Institute New Orleans, LA Disclosures Pfizer Speaker Bureau Bristol Myers
Novel Approaches to VT Management Glenn M Polin MD Medical Director, Electrophysiology Laboratory John Ochsner Heart and Vascular Institute New Orleans, LA Disclosures Pfizer Speaker Bureau Bristol Myers
Map-Guided Ablation of Non-ischemic VT. Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN
 Map-Guided Ablation of Non-ischemic VT Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN nothing Declaration of Interest Catheter Ablation of Non-ischemic VT Sarcoidosis, 13, 6%
Map-Guided Ablation of Non-ischemic VT Takashi Nitta Cardiovascular Surgery, Nippon Medical School Tokyo, JAPAN nothing Declaration of Interest Catheter Ablation of Non-ischemic VT Sarcoidosis, 13, 6%
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy
 Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Primary prevention of SCD with the ICD in Nonischemic Cardiomyopathy Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: Consulting and Clinical Trials Medtronic
Prof. Samir Morcos Rafla Alexandria Univ. Cardiology Dept.
 Obesity as a risk factor for Atrial Fibrillation Prof. Samir Morcos Rafla Alexandria Univ. Cardiology Dept. CardioAlex 2010 smrafla@hotmail.com 1 Obesity has reached epidemic proportions in the United
Obesity as a risk factor for Atrial Fibrillation Prof. Samir Morcos Rafla Alexandria Univ. Cardiology Dept. CardioAlex 2010 smrafla@hotmail.com 1 Obesity has reached epidemic proportions in the United
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Secondary prevention of sudden cardiac death
 Secondary prevention of sudden cardiac death Balbir Singh, MD, DM; Lakshmi N. Kottu, MBBS, Dip Card, PGPCard Department of Cardiology, Medanta Medcity Hospital, Gurgaon, India Abstract All randomised secondary
Secondary prevention of sudden cardiac death Balbir Singh, MD, DM; Lakshmi N. Kottu, MBBS, Dip Card, PGPCard Department of Cardiology, Medanta Medcity Hospital, Gurgaon, India Abstract All randomised secondary
Risk Stratification of Sudden Cardiac Death
 Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Risk Stratification of Sudden Cardiac Death Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC USA Disclosures: None Sudden Cardiac Death A Major Public Health Problem > 1/2 of
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Cardiomyopathy. Cardiomyopathies HOCM. Hypertrophic Obstructive Cardiomyopathy. Systolic Anterior Movement (SAM) of Mitral Valve (Venturi Effect) Cine
 of Mitral Valve (Venturi Effect) Cine") Jens Bremerich Radiology University Hospital Basel Hypertrophic Obstructive Cine VENC Cine (5m/s) Modified Bernoulli Equation: P (in mmhg) = 4 x (Vmax)2 Vmax= 4.2 m/s, P = 70mm Hg Hydrodynamica 738 HOCM
Jens Bremerich Radiology University Hospital Basel Hypertrophic Obstructive Cine VENC Cine (5m/s) Modified Bernoulli Equation: P (in mmhg) = 4 x (Vmax)2 Vmax= 4.2 m/s, P = 70mm Hg Hydrodynamica 738 HOCM
Update on use of cardiac MRI in ARVC/D. Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology
 Update on use of cardiac MRI in ARVC/D Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology Outline Background Diagnosis Characteristic imaging findings Genetics of ARVC Genotype phenotype
Update on use of cardiac MRI in ARVC/D Stefan L. Zimmerman, MD Johns Hopkins University Department of Radiology Outline Background Diagnosis Characteristic imaging findings Genetics of ARVC Genotype phenotype
Radiologic Assessment of Myocardial Viability
 November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
Risk prediction in inherited conditions Laminopathies
 Risk prediction in inherited conditions Laminopathies Karim Wahbi Cochin hospital, Paris karim.wahbi@aphp.fr Risk prediction in laminopathies Current approach for risk stratification A new score to predict
Risk prediction in inherited conditions Laminopathies Karim Wahbi Cochin hospital, Paris karim.wahbi@aphp.fr Risk prediction in laminopathies Current approach for risk stratification A new score to predict
Echocardiography for the Electrophysiologist: Day-to-day practice. Emmanuel Fares, MD
 Echocardiography for the Electrophysiologist: Day-to-day practice Emmanuel Fares, MD EP and pacing service, Department of Cardiovascular Medicine, Cairo University Agenda Role of echo in arrhythmia management:
Echocardiography for the Electrophysiologist: Day-to-day practice Emmanuel Fares, MD EP and pacing service, Department of Cardiovascular Medicine, Cairo University Agenda Role of echo in arrhythmia management:
Long-Term Prognosis in Recipients of Implantable Cardioverter-Defibrillators for Secondary Preventions in Taiwan A Multicenter Registry Study
 Mini Forum for EPS Acta Cardiol Sin 2014;30:22 28 Long-Term Prognosis in Recipients of Implantable Cardioverter-Defibrillators for Secondary Preventions in Taiwan A Multicenter Registry Study Tze-Fan Chao,
Mini Forum for EPS Acta Cardiol Sin 2014;30:22 28 Long-Term Prognosis in Recipients of Implantable Cardioverter-Defibrillators for Secondary Preventions in Taiwan A Multicenter Registry Study Tze-Fan Chao,
Myocardial Scar Visualized by Cardiovascular Magnetic Resonance Imaging Predicts Major Adverse Events in Patients With Hypertrophic Cardiomyopathy
 Journal of the American College of Cardiology Vol. 56, No. 11, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.05.007
Journal of the American College of Cardiology Vol. 56, No. 11, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2010.05.007
27-year-old professionnal rugby player: asymptomatic
 27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
27-year-old professionnal rugby player: asymptomatic Benefits and limits of cardiac MRI in the young athlete with a suspected heart disease. Philippe PAULE Service de Cardiologie, HIA Clermont Tonnerre,
that number is extremely high. It s 16 episodes, or in other words, it s 14, one-four, ICD shocks per patient per day.
 Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Doctor Karlsner, Doctor Schumosky, ladies and gentlemen. It s my real pleasure to participate in this session on controversial issues in the management of ventricular tachycardia and I m sure that will
Do All Patients With An ICD Indication Need A BiV Pacing Device?
 Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Do All Patients With An ICD Indication Need A BiV Pacing Device? Muhammad A. Hammouda, MD Electrophysiology Laboratory Department of Critical Care Medicine Cairo University Etiology and Pathophysiology
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Pathophysiology of Coronary Microvascular Dysfunction
 Pathophysiology of Coronary Microvascular Dysfunction Cheol Woong Yu, MD, PhD Cardiology Department Division of Internal Medicine Korea University Anam Hospital. Etiologies of Chest Pain without obstructive
Pathophysiology of Coronary Microvascular Dysfunction Cheol Woong Yu, MD, PhD Cardiology Department Division of Internal Medicine Korea University Anam Hospital. Etiologies of Chest Pain without obstructive
Cardiovascular Imaging Stress Echo
 Cardiovascular Imaging Stress Echo Theodora A Zaglavara, MD, PhD Cardiac Imaging Department INTERBALKAN MEDICAL CENTER Thessaloniki GREECE Evolution of Stress Echo: From Innovation to a Widely Established
Cardiovascular Imaging Stress Echo Theodora A Zaglavara, MD, PhD Cardiac Imaging Department INTERBALKAN MEDICAL CENTER Thessaloniki GREECE Evolution of Stress Echo: From Innovation to a Widely Established
MEDICAL POLICY SUBJECT: MICROVOLT T-WAVE ALTERNANS
 MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Indications for catheter ablation in 2010: Ventricular Tachycardia
 Indications for catheter ablation in 2010: Ventricular Tachycardia Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology Laboratories Ospedale San Raffaele, IRCCS, Milan, Italy Europace
Indications for catheter ablation in 2010: Ventricular Tachycardia Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology Laboratories Ospedale San Raffaele, IRCCS, Milan, Italy Europace
Non-Invasive Ablation of Ventricular Tachycardia
 Non-Invasive Ablation of Ventricular Tachycardia Dr Shaemala Anpalakhan Newcastle upon Tyne Hospitals NHS Foundation Trust Freeman Road, Newcastle Upon Tyne, NE7 7DN Contact: shaemala@doctors.org.uk Introduction
Non-Invasive Ablation of Ventricular Tachycardia Dr Shaemala Anpalakhan Newcastle upon Tyne Hospitals NHS Foundation Trust Freeman Road, Newcastle Upon Tyne, NE7 7DN Contact: shaemala@doctors.org.uk Introduction
What Every Physician Should Know:
 What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
What Every Physician Should Know: The Canadian Heart Rhythm Society estimates that, in Canada, sudden cardiac death (SCD) is responsible for about 40,000 deaths annually; more than AIDS, breast cancer
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease
 The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
The implantable cardioverter defibrillator is not enough: Ventricular Tachycardia Catheter Ablation in Patients with Structural Heart Disease Paolo Della Bella, MD Arrhythmia Department and Clinical Electrophysiology
Apical Hypertrophic Cardiomyopathy With Hemodynamically Unstable Ventricular Arrhythmia Atypical Presentation
 Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
Cronicon OPEN ACCESS Hemant Chaturvedi* Department of Cardiology, Non-Invasive Cardiology, Eternal Heart Care Center & research Institute, Rajasthan, India Received: September 15, 2015; Published: October
Public Statement: Medical Policy Statement:
 Medical Policy Title: Cardioverter- ARBenefits Approval: 09/7/2011 Defibrillators Effective Date: 01/01/2012 Document: ARB0096 Revision Date: Code(s): C1721, C1722, C1777, C1882, C1895, C1896 and C1899
Medical Policy Title: Cardioverter- ARBenefits Approval: 09/7/2011 Defibrillators Effective Date: 01/01/2012 Document: ARB0096 Revision Date: Code(s): C1721, C1722, C1777, C1882, C1895, C1896 and C1899
Atrial fibrillation (AF) is a disorder seen
 is a disorder seen") This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,