Pathophysiology of ACS
|
|
|
- Spencer Gallagher
- 6 years ago
- Views:
Transcription

1 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS

2 NSTEMI vs STEMI
3 VANQWISH Boden et al N Engl J Med 1998;338: patients randomized to either invasive or conservative management, defined as medical therapy and noninvasive testing, with subsequent invasive management if indicated by the development of spontaneous or inducible ischemia, within 72 hours of the onset of a non Q-wave infarction. Results The number of patients who died at hospital discharge was significantly higher in the invasive-strategy group (36 vs. 15 patients, P=0.004), Overall mortality during follow-up did not differ significantly. Conclusions Most patients with non Q-wave MI do not benefit from routine, early invasive management consisting of coronary angiography and revascularization.
4 FRISC II Outcome at 1 Year N= 2,457 Swedish ACS patients conservative invasive Lancet 2000;356:9-16

5 Platelet adhesion Platelet aggregation Adhesive proteins fibrinogen vwf GPIIb/IIIa inhibitors
6 N= 29,570 pts in 6 randomized, double-blind placebo-controlled trials of GPIIb/IIIa antagonists in the management of ACS diabetics Roffi et al. Eur Heart J 2002;23,
 elevation) The The")

7 2006;295: N=2,022 N=2,022 high high risk risk ACS ACS patients patients (unstable (unstable angina angina with with EKG abnormalities EKG abnormalities or or troponin troponin elevation) elevation) The The primary primary end end point point was was a a composite composite of of death, death, myocardial myocardial infarction, infarction, or or urgent urgent target target vessel vessel revascularization revascularization
8 Oral Anti-platelet Agents Sites of Action

9 GP IIb/IIIa inhibitor
10 CAPRIE - Primary Endpoints* N= 19,185 patients with atherosclerotic disease Cumulative Event Rate (%) % Overall Risk Reduction p= % 5.33% Aspirin Clopidogrel * MI, Ischemic Stroke, or Vascular Death Months of Follow-Up
11 MI/Stroke/CV Death Within 30 Days Cumulative Hazard Rate * In addition to other standard therapies. 0 Placebo + ASA* Clopidogrel + ASA* Days of Follow-Up The CURE Trial Investigators. N Engl J Med. 2001;345: % Relative Risk Reduction P = N = 12,562
12 Major Bleeding by ASA Dose ASA Dose Clopidogr el + ASA* Placebo + ASA* <100 mg 2.6% 2.0% mg 3.5% 2.3% >200 mg 4.9% 4.0%
13 Mortality (%) COMMIT: Effect of Clopidogrel on Death in Hospital Placebo + ASA: 1846 deaths (8.1%) Clopidogrel + ASA: 1728 deaths (7.5%) 7% (SE3) relative risk reduction (2P=.03) Time (d Since Randomization [ 28 d) Adapted with permission from COMMIT Collaborative Group. Lancet. 2005;366:
14 CLARITY TIMI TIMI 28: Primary Endpoint Occluded Artery (or Death/MI Through Angio/HD) Occluded Artery or Death/MI (%) % Odds Reduction 15.0 n=1752 n=1739 Clopidogrel 21.7 Placebo Odds Ratio: 0.64 (95% CI, ) P= Clopidogrel Better Placebo Better Sabatine MS et al N Engl J Med 2005;352:
 Metoprolol: 1776 deaths (7.7%) % dead 1% (SE 3) relative risk reduction (2P=0.")
15 COMMIT: Effects of metoprolol on death Placebo: 1798 deaths (7.8%) Metoprolol: 1776 deaths (7.7%) % dead 1% (SE 3) relative risk reduction (2P=0.7) Days since randomisation
16 COMMIT: Effects of metoprolol on cardiogenic shock by Killip class Baseline Metoprolol Placebo Odds ratio & 95% CI Killip class (22,927) (22,922) Metop. better I 611 (3.5%) 487 (2.8%) II 362 (7.9%) 296 (6.5%) Placebo better III 155 (16.2%) 100 (10.4%) ALL 1141 (5.0%) 888 (3.9%) -29% SE 5 (2P < )

 Maximum (max) platelet aggregation in")

17 Enhanced Platelet Activation on UFH Unstable angina patients Samples drawn before and after heparin infusion Light transmission aggregometry (0.625 μm) Maximum (max) platelet aggregation in PRP from volunteers after adding saline, UFH, enoxaparin, or argatroban Xiao and Theroux Circulation 1998;97:


18 Should we inhibit thrombin directly or indirectly? Indirect Inhibition Direct Inhibition Heparin binding site Active site Fibrin/ogen binding site Anti-Xa:Anti-IIa ratio Hirudin Argatroban Bivalent versus univalent
 target ACT > 225 sec Bivalirudin 0.75 mg/kg initial bolus, 1.75 mg/kg-hr during PCI Provisional GP IIb/IIIa (abciximab or eptifibatide) abciximab: 0.")
19 REPLACE-2 2 Trial Design Bivalirudin vs Heparin + GP IIb/IIIa During PCI N ~ 6000 Patients: Urgent or Elective PCI Randomization - double blind, triple dummy Heparin 65 U/kg initial bolus Planned GP IIb/IIIa (abciximab or eptifibatide) target ACT > 225 sec Bivalirudin 0.75 mg/kg initial bolus, 1.75 mg/kg-hr during PCI Provisional GP IIb/IIIa (abciximab or eptifibatide) abciximab: 0.25 mg/kg bolus, μg/kg-min (max 10 μg/min) x 12 hrs eptifibatide: : 180 μg/kg double bolus, 2.0 μg/kg-min x hrs Quadruple Endpoint at 30 Days
20 Primary Quadruple Endpoint Death, MI, URev, Maj Bld (%) Odds Ratio = ( ) 10.0 Heparin+ GP IIb/IIIa (n=3008) p = Bivalirudin (n=2994) Heparin superiority boundary Heparin Better Bivalirudin Better Heparin + GP IIb/IIIa non-inferiority boundary = Odds Ratio & 95% CI 1

21 Prospective, Randomized Comparison of Heparin Plus IIb/IIIa Inhibition and Bivalirudin With or Without IIb/IIIa Inhibition in Patients with Acute Coronary Syndromes 21
22 Study Design First Randomization Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,800) Moderatehigh risk ACS Aspirin in all Clopidogrel dosing and timing per local practice R* UFH or Enoxaparin + GP IIb/IIIa Bivalirudin + GP IIb/IIIa Bivalirudin Alone Angiography within 72h Medical management PCI CABG *Stratified by pre-angiography thienopyridine use or administration ACUITY Design. Stone GW et al. AHJ 2004;148:764 75
23 Canada (26) USA (246) ACUITY Enrollment 13,819 pts randomized at 448 centers in 17 countries (4) Norway Sweden (6) (5) Denmark (4) Netherlands Finland (3) (5) Belgium Poland (1) (12) UK Germany (66) (8) France Austria (4) Italy (15) (25) Spain (4) New Zealand (17) Australia

24 Primary Endpoint Measures (ITT) UFH/Enoxaparin + GPI vs. Bivalirudin Alone UFH/Enoxaparin+GPI (N=4603) Bivalirudin alone (N=4612) 30 day events (%) P NI < P Sup = % 10.1% P NI = P Sup = % 7.8% P NI < P Sup < % 3.0% Net clinical outcome Ischemic composite Major bleeding
25 Net Clinical Outcome Composite UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone Risk ratio ±95% CI Bival Alone UFH/Enox + IIb/IIIa RR (95% CI) P P int Age <65 (n=5051) Age 65 (n=4164) 7.8% 12.9% 9.2% 14.7% 0.86 ( ) 0.88 ( ) Men (n=6444) Women (n=2771) 9.5% 11.6% 10.9% 13.5% 0.87 ( ) 0.86 ( ) Diabetes (n=2585) No diabetes (n=6630) 10.8% 9.8% 13.7% 10.9% 0.79 ( ) 0.90 ( ) CrCl 60 (n=6993) CrCl <60 (n=1644) 8.9% 16.1% 10.4% 16.8% 0.86 ( ) 0.96 ( ) US (n=5224) OUS (n=3991) 10.6% 9.5% 11.8% 11.5% 0.90 ( ) 0.82 ( ) Bivalirudin alone better UFH/Enox + IIb/IIIa better
26 Net Clinical Outcome Composite UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone Risk ratio ±95% CI Bival Alone UFH/Enox + IIb/IIIa RR (95% CI) P P int Biomarkers (CK/Trop) Elevated (n=5368) Normal (n=3841) 12.2% 7.1% 13.3% 9.4% 0.92 ( ) 0.75 ( ) ST Deviation Yes (n=3197) No (n=6008) 13.0% 8.6% 13.7% 10.6% 0.96 ( ) 0.81 ( ) TIMI Risk Score Low (0-2) (n=1291) Intermed (3-4) (n=4407) High (5-7) (n=2449) Pre Thienopyridine Yes (n=5192) No (n=4023) 6.4% 10.2% 0.63 ( ) % 10.2% 0.92 ( ) % 15.2% 0.92 ( ) % 11.3% 12.2% 11.1% 0.76 ( ) 1.02 ( ) < Bivalirudin alone better UFH/Enox + IIb/IIIa better
27 Study Design Second Randomization Moderate-high risk unstable angina or NSTEMI undergoing an invasive strategy (N = 13,819) Moderatehigh risk ACS (n=13,819) UFH or Enoxaparin Routine upstream GPI in all pts R GPI started in CCL for PCI only R Bivalirudin Routine upstream GPI in all pts GPI started in CCL for PCI only Routine upstream GPI in all pts (4,605) VS. Deferred GPI for PCI only (n=4,602) UFH, Enoxaparin, or Bivalirudin Aspirin in all Clopidogrel dosing and timing per local practice Bivalirudin Alone (n=4,612) ACUITY Design. Stone GW et al. AHJ 2004;148:764 75
 15 10 5 Routine Upstream IIb/IIIa (N=4605) Estimate 7.1% 7.9% 0.14 7.")
28 Ischemic Composite Endpoint Upstream IIb/IIIa vs. Selective IIb/IIIa vs. Bivalirudin alone Cumulative Events (%) Routine Upstream IIb/IIIa (N=4605) Estimate 7.1% 7.9% % P (log rank) Deferred PCI IIb/IIIa (n=4602) Bivalirudin alone (N=4612) Days from Randomization
29 Major Bleeding Endpoint Upstream IIb/IIIa vs. Selective IIb/IIIa vs. Bivalirudin alone Cumulative Events (%) Routine Upstream IIb/IIIa (N=4605) Estimate P 6.1% (log rank) 4.9% % Deferred PCI IIb/IIIa (n=4602) Bivalirudin alone (N=4612) < Days from Randomization
30 ST Elevation Myocardial Infarction (STEMI) 8 6 Relationship Between Time to Reperfusion and Mortality: GUSTO-IIb 6.4 p= day mortality (%) < > 91 N: Berger et al. Circulation 1999;100:14 Time to PTCA (minutes)
31 Myocardial viability (%) Wavefront Theory of Myocardial Loss Transmural necrosis (%) min 3h 6h 24h 96h 0 3h 6h 24h Duration of occlusion Time post-occlusion 0 Reimer et al Circulation 1977;56:786-94
32 ASA vs Placebo in ISIS-II: II: Odds of Vascular Death Astrological Gemini/Libra (n=1442) Birthsign All Others (n=7157) Odds ratio and 95% CI Play of chance Unrecognized randomization error True effect Prior MI Yes No Diabetic Yes No Sex Male Female Age < Systolic BP < Heart Rate < EKG BBB IMI AMI ST ALL PATIENTS (9.4 vs 11.8% mortality) 23% When in a trial with a clearly positive result many subgroups are considered, false negative results in some particular subgroups must be expected It is clear that the best estimate of the real effect is given by the overall results derived from all subgroups combined. Modified from: ISIS-2 Lancet 1988 Aug 13;2(8607): ASA better 1 Placebo better 1.5
33 19 Randomized Trials of PCI vs Lysis N = 5,066 12% 10% 10.0% Lysis PCI Event rate 8% 6% 4% 2% 0% p= % 6.7% p= % 7.2% p< % Death Death (excl shock) Reinfarction Keeley, Grines; Lancet 2003

34 19 Randomized Trials of PCI vs Lysis N = 5,066 3% Lysis PCI 2.2% Event rate 2% 1% 1.3% P< p= % 0% 0.08% Hemorrhagic stroke Total stroke Keeley, Grines; in press
35 DANAMI-2: Patient Flow ST- elevation MI (n=1,900) Randomize 100 mg accelerated t-pat PCI (+ stent)
36 DANAMI-2 DENMARK 5.4 mill. inhabitants 5 PCI centers 24 referral hospitals 62% of the Danish population Transport distance up to 95 US miles (mean 35 miles) 100 US miles
37 DANAMI-2: Primary Results Death / MI / Stroke (%) 16% 12% 8% 4% 14% Combined P= RRR 45% 8% 16% 12% 8% 4% Transfer Sites 14% P=0.002 RRR 40% 9% 16% 12% 8% 4% Non-Transfer Sites 12% P=0.048 RRR 45% 7% 0% Lytic 0% Primary PCI 0% Lytic Primary PCI Lytic Primary PCI
38 Early Presenting Patients: Primary PCI vs Fibrinolytics 20% Lytic (STK) Transfer for PCI 10% Prehosp t-pa PCI 30-d Mortality (%) 15% 10% 5% P< d Mortality (%) 8% 6% 4% 2% P= P= % <3 hr (n=551) >3 hr (n=299) PRAGUE-2 0% <2 hr (n=460) >2 hr (n=374) CAPTIM Widimsky P, et al. Eur Heart J. 2003;24(1): Steg PG, et al. Circulation. 2003;108(23):

39 Gersh, Stone, White, Holmes JAMA 2005;293:
40 The Evolution of Optimal Myocardial Infarction Therapy Eisenhower Cheney Year: Therapy: Morphine Angioplasty/Stent Heparin Heparin Warfarin Aspirin Atropine Abciximab Clopidogrel β-blocker Statin Bed Rest: 7 Weeks < 2 Days Expected Mortality: 30% < 5%
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC
 Mitchell W. Krucoff, MD, FACC") Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Timing of Anti-Platelet Therapy for ACS (EARLY-ACS & ACUITY) Mitchell W. Krucoff, MD, FACC Professor, Medicine/Cardiology Duke University Medical Center Director, Cardiovascular Devices Unit Duke Clinical
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI
 Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Direct Thrombin Inhibitors for PCI Pharmacology: Role of Bivalirudin in High-Risk PCI Charles A. Simonton MD, FACC, FSCAI Sanger Clinic Medical Director Clinical Innovation and Research Carolinas Heart
Is there a real need for new agents to optimize efficacy/safety balance
 Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Anticoagulation in acute coronary syndrome Is there a real need for new agents to optimize efficacy/safety balance Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI
 HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
Bivalirudin should be indicated for all patients with STEMI. Adnan Kastrati Deutsches Herzzentrum, Munich, Germany
 Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI. ISAR-REACT 4 Trial
 Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
Is the role of bivalirudin established?
 Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
Is the role of bivalirudin established? Rob Henderson Consultant Cardiologist Trent Cardiac Centre Nottingham University Hospitals Conflicts of Interest: None Declarations: Member NICE Unstable Angina
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department
: Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department") ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Jonathan D. Marmur, MD, FACC Professor of Medicine Director, Cardiac Catheterization and Interventional Cardiology. State University of New York
 STEMI Management 2007 Jonathan D. Marmur, MD, FACC Professor of Medicine i Director, Cardiac Catheterization and Interventional Cardiology Health Science Center at Brooklyn State University of New York
STEMI Management 2007 Jonathan D. Marmur, MD, FACC Professor of Medicine i Director, Cardiac Catheterization and Interventional Cardiology Health Science Center at Brooklyn State University of New York
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Clopidogrel When For What For How Long. T Benjanuwattra Chiang Mai Heart Cent
 Clopidogrel When For What For How Long T Benjanuwattra Chiang Mai Heart Cent Evidence Based Medicine I don t want to put you to sleep But want you to be fully alert Atherothrombosis: A Generalized and
Clopidogrel When For What For How Long T Benjanuwattra Chiang Mai Heart Cent Evidence Based Medicine I don t want to put you to sleep But want you to be fully alert Atherothrombosis: A Generalized and
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
Otamixaban for non-st-segment elevation acute coronary syndrome
 Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Timing of angiography for high- risk ACS
 Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
From STEMIs to Stents: Updates in PCI practice
 From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
From STEMIs to Stents: Updates in PCI practice Arnold Seto, MD, MPA Assistant Clinical Professor, UC-Irvine and Long Beach VA Director of Interventional Cardiology Research Hospitalizations in the U.S.
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Patient characteristics Intervention Comparison Length of followup
 ANTICOAGULANT CHAPTER Low Molecular Weight Heparins compared with Unfractionated Heparin Ref ID: 1903 Reference Antman EM, McCabe CH, Gurfinkel EP et al. Enoxaparin prevents death and cardiac ischemic
ANTICOAGULANT CHAPTER Low Molecular Weight Heparins compared with Unfractionated Heparin Ref ID: 1903 Reference Antman EM, McCabe CH, Gurfinkel EP et al. Enoxaparin prevents death and cardiac ischemic
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION?
 SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
SHOULD BETA BLOCKERS BE USED ROUTINELY IN POST MI PATIENTS WITH PRESERVED LV FUNCTION? Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Optimal antithrombotic therapy:
 Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Scottish Medicines Consortium
 Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
Scottish Medicines Consortium bivalirudin, 250mg powder for concentrate for solution for injection or infusion (Angiox ) No. (516/08) The Medicines Company UK Ltd 07 November 2008 The Scottish Medicines
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
ST-Elevation MI: Update on Bivalirudin and DES
 ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
ST-Elevation MI: Update on Bivalirudin and DES George D. Dangas, MD, FACC, FSCAI, FAHA Professor of Medicine Director, Cardiovascular Innovation Mount Sinai Medical Center, New York, NY Disclosure Research
Is Cangrelor hype or hope in STEMI primary PCI?
 Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company
 SMC No. (638/10) The Medicines Company") bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
 Judd E. Hollander, MD Professor, Clinical Research Director, Department of Emergency Medicine University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania OBJECTIVES: 1. Discuss the concept
Judd E. Hollander, MD Professor, Clinical Research Director, Department of Emergency Medicine University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania OBJECTIVES: 1. Discuss the concept
STEMI: Newer Aspects in Pharmacological Treatment
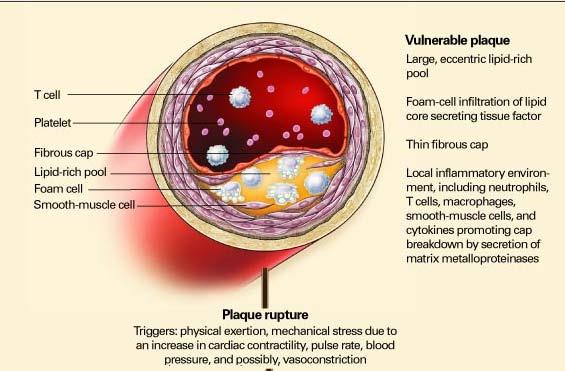
 CHAPTER 14 STEMI: Newer Aspects in Pharmacological Treatment P. C. Manoria, Pankaj Manoria Introduction ST elevation myocardial infarction (STEMI) commonly results from disruption of a vulnerable plaque
CHAPTER 14 STEMI: Newer Aspects in Pharmacological Treatment P. C. Manoria, Pankaj Manoria Introduction ST elevation myocardial infarction (STEMI) commonly results from disruption of a vulnerable plaque
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY
 2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
2007 ACC/AHA GUIDELINES FOR THE MANAGEMENT OF NSTE-ACS: OPTIMAL ANTICOAGULATION AND ANTIPLATELET THERAPY Charles V. Pollack, Jr., MA, MD, FACEP, FAAEM, FAHA Professor and Chairman, Department of Emergency
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN
 What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
10 Steps to Managing Non-ST Elevation ACS
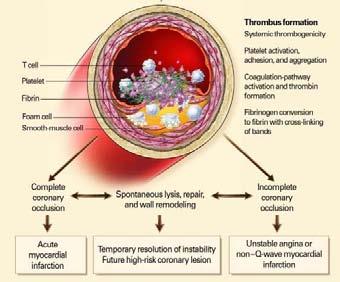
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
Disclosure. Financial disclosure: National Advisory Board & Research Grant from Boehringer-Ingelheim
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute
 Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib!
 Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
Anti-platelet Therapies in Cardiovascular Disease: From Stable CAD to ACS and Afib! Roxana Mehran, MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Research support
C.R.E.D.O. Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial
 Prospective Randomized Double Blind Placebo Controlled Trial") Clopidogrel for the Reduction of Events During Observation Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial From Steinhubl et al, JAMA 2002;228:2411-20
Clopidogrel for the Reduction of Events During Observation Multicenter Multinational (USA, Canada) Prospective Randomized Double Blind Placebo Controlled Trial From Steinhubl et al, JAMA 2002;228:2411-20
ESC 2012: Klinisch relevante Neuigkeiten beim ACS
 Kardiologie-Kreis KH Barmherzige Schwestern Linz, 2.10.2012 ESC 2012: Klinisch relevante Neuigkeiten beim ACS 30 Minuten Priv.- Doz. Dr. Hannes Alber REHA ZENTRUM MÜNSTER UNIV.- KLINIK f. INNERE MED. III
Kardiologie-Kreis KH Barmherzige Schwestern Linz, 2.10.2012 ESC 2012: Klinisch relevante Neuigkeiten beim ACS 30 Minuten Priv.- Doz. Dr. Hannes Alber REHA ZENTRUM MÜNSTER UNIV.- KLINIK f. INNERE MED. III
Chronic kidney disease (CKD) is frequently encountered
 is frequently encountered") AHA Scientific Statement Pharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary Syndrome A Scientific Statement From the American Heart Association Jeffrey B. Washam, PharmD,
AHA Scientific Statement Pharmacotherapy in Chronic Kidney Disease Patients Presenting With Acute Coronary Syndrome A Scientific Statement From the American Heart Association Jeffrey B. Washam, PharmD,
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
NSTEACS Case Presentation
 NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
After acute coronary syndromes patients continue to have recurrent ischemic events despite revascularization and dual antiplatelet therapy
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
MULTIcentre evaluation of Single high-dose. acute myocardial infarction study
 MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes
 European Heart Journal (00) 3, 1441 1448 doi:10.1053/euhj.00.3160, available online at http://www.idealibrary.com on Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes Gradient of benefit
European Heart Journal (00) 3, 1441 1448 doi:10.1053/euhj.00.3160, available online at http://www.idealibrary.com on Platelet glycoprotein IIb/IIIa inhibition in acute coronary syndromes Gradient of benefit
Direct Thrombin Inhibitors and Gp 2b/3a Receptor Blockers in the Cardiac Cath Lab. Eric J Dippel, MD FACC
 Midwest Cardiovascular Research Foundation Direct Thrombin Inhibitors and Gp 2b/3a Receptor Blockers in the Cardiac Cath Lab Eric J Dippel, MD FACC Plaque Rupture Stable Angina Unstable Angina Non Q-wave
Midwest Cardiovascular Research Foundation Direct Thrombin Inhibitors and Gp 2b/3a Receptor Blockers in the Cardiac Cath Lab Eric J Dippel, MD FACC Plaque Rupture Stable Angina Unstable Angina Non Q-wave
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Do We Need Platelet Function Assays?
 Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Prof. Jindřich Špinar, MD
 Prof. Jindřich Špinar, MD Head of the Internal Cardiology dpt., University Hospital Brno Focuses on clinical cardiology, acute and chronic heart failure, ischemic heart gisease, hypertension Vice head
Prof. Jindřich Špinar, MD Head of the Internal Cardiology dpt., University Hospital Brno Focuses on clinical cardiology, acute and chronic heart failure, ischemic heart gisease, hypertension Vice head
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),