PRN Medications. Indications & Use. Bindu Swaroop, MD Associate Clinical Professor Department of Medicine
|
|
|
- Tabitha Lee
- 5 years ago
- Views:
Transcription


1 PRN Medications Indications & Use Bindu Swaroop, MD Associate Clinical Professor Department of Medicine
2 Objectives Identify which prn medications are appropriate for inclusion in admission orders Identify contraindications and adverse effects associated with common prn medications Known when to evaluate the patient prior to ordering or the nurse giving a prn medication 2
3 Common Uses Pain Sleep Cardiovascular: Hypertension Sedatives: ETOH withdrawal, agitation Pulmonary: Nebulizers, Mucolytics GI: Bowels, Heartburn, Constipation 3
4 Case Vignette HPI: 61 year old male admitted for chest pain and acute ETOH intoxication. He also complains of hematemesis during his most recent drinking binge. PMHx: AVNRT, Hepatitis C, insomnia, depression, COPD Meds: combivent inhaler bid, ibuprofen 600mg po tid prn EKG on admission reveals bpm 4
5 Case Vignette He is admitted to the medicine service with the following prn orders: -Ativan 2mg IV q4hr prn withdrawal -Albuterol neb q6h prn, Atrovent neb q6hr prn -Acetaminophen 650mg q4hr prn pain -Ibuprofen 600mg po tid prn pain 5
6 Case Vignette That night the patient subsequently requests pain medication for his chest pain. Since ibuprofen is ordered prn the night float instructs the nurse to give this to the patient. The patient still complains of pain later that night, and the night float writes an order for Morphine sulfate 2mg IVP q4hr prn pain. Are these appropriate meds to give to the patient? What other alternatives could have been given? 6
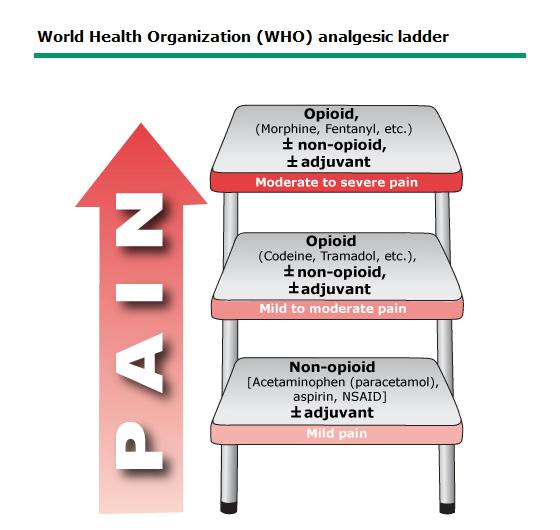
7
8 Analgesics Oral Pain Severity SC/IM/IV Pain Severity Adverse Effects Non- Opiods Acetaminophen mg Mild Ketorolac 30-60mg Moderate Caution in hepatic or renal impairment Opiods Ibuprofen mg Tramadol mg Mild Mild to Moderate PUD, GI bleed, renal toxicity Norco (5-10mg hydrocodone/325 mg acetaminophen) Moderate Morphine Moderate to Severe Constipation, Ileus, n/v, respiratory depression, urinary retention Percocet (5mg oxycodone /325mg) Moderate Dilaudid Severe Caution Hepatic or Renal Impairment 8 Morphine IR Moderate Fentanyl (ICU) Severe
9 Case Vignette The next day his BP has risen to 170/105. He is given hydralazine 10mg IVP by the team with a drop in his BP to 125/ What is likely contributing to the rise in BP? 4. What side effects could occur from lowering the BP too much? 5. How else could this patient have been treated? 9
10 Hypertension Treatment- Inpatient Goal: -To identify and treat the underlying cause -Prevent end-organ damage Common Causes: Rebound Inadequate dosing Drug Interactions ETOH withdrawal Hypoxemia, respiratory distress Pain, Anxiety Autonomic response: urinary retention, constipation, SCI 10
11 Hypertension- Inpatient Management Approach to evaluating the patient: -Determine patient s baseline -Confirm accuracy, both arms, cuff size -Screen for the underlying cause -Determine if hypertensive emergency or urgency is present 11
12 Hypertension Treatment Hypertensive Urgency -SBP >180 or DBP >120 -gradual reduction of BP to 160/110 over hours -use ORAL meds *There is no proven benefit from rapid reduction of blood pressure in patients with severe asymptomatic hypertension 12
13 Hypertensive Emergency -evidence of end-organ damage -Immediate reduction of MAP: by 10 to 20 percent in the first hour then a further 5 to 15 percent over the next 23hrs -Use PARENTERAL agents (drips only, not IVP) -Transfer to ICU (There are exceptions: Aortic Dissection, Neurologic Emergencies, etc.) 13
14 Inpatient BP Management- Where s the Evidence? Intravenous Hydralazine for Blood Pressure Management in the Hospitalized Patient: Its Use is Often Unjustified Patrick Campbell, M.D., William L. Baker, Pharm.D., et.al Journal for American Society of Hypertension 94 patients (mean age, 69yrs, 89% with chronic hypertension) who received 201 intravenous hydralazine doses Baseline BP was 175/82 ± 25/16 mmhg and following hydralazine was reduced by 24/9 Only 2% of patients had evidence of an urgent hypertensive condition but 8% had adverse effects (hypotension) 48% of the doses were ordered between 11 pm and 7am. The internal medicine service ordered 52% of the intravenous hydralazine doses Seven (7.5%) patients were evaluated by a physician prior to hydralazine administration and 17 (18%) were evaluated post-dosing 14
15 Inpatient BP Management- Where s the Evidence? An Update on Inpatient Hypertension Management R. Neal Axon; Mason Turner; Ryan Buckley et.al Current Cardiology Reports; November 2015 most instances of elevated BP observed in the hospital are asymptomatic and may not require urgent action available evidence suggests a tendency for inpatient providers to overreact to asymptomatic elevated BP offering little benefit and risking potential harm Practice patterns, outcomes, and end-organ dysfunction for patients with acute severe hypertension: The Studying the Treatment of Acute hypertension (STAT) Registry N.Katz MD a. Joel M. GoreMD b. Alpesh Amin MD c et.al American Heart Journal, October institution, US registry of consecutive patients with acute severe hypertension (>180 SBP or >110 DBP)treated with IV meds in ICU or ED found marked variability in practice patterns and outcomes. This heterogeneity in care, along with high mortality and readmission rates, also highlights the importance of further investigation for this understudied clinical condition. 15


16 44% of respondents indicated that they would treat acutely elevated BP in an asymptomatic patient. The strong preference of trainees for hydralazine for hypertensive urgency in non intensive-care-unit patients is curious given that there do not appear to be any randomized controlled clinical trials with this medication for this indication.

17 Inpatient HTN Management There is no RCT evidence demonstrating that antihypertensive drugs reduce mortality or morbidity in patients with hypertensive emergencies There is insufficient RCT evidence to determine which drug or drug class is most effective in reducing mortality and morbidity. Although physicians commonly treat acute hypertension in hospitalized patients, we can find no consensus recommendation supporting the practice. 17 reasonable to limit the use of parenteral therapy to situations in which acute target organ damage is suspected and not as a standing prn order targeted to elevated BP above a threshold level.
18 Hypertension Clinical Pearls Hypertensive treatment rarely requires immediate treatment in the middle of the night Avoid prn use of rapid acting agents (can precipitate ischemic events) For patients with sustained HTN, primary team should initiate treatment with long acting regimen 18
19 Case Vignette Later that night the patient requests something for sleep and receives Benadryl 25mg po, written as qhs prn per night float. On day three of admission he develops urinary retention with a PVR of 300cc. A foley catheter is placed. You review his chart and notice a prior urology note indicating the patients prostate size on DRE is 50g. What could be contributing to the urinary retention? What other alternatives could have been used for his insomnia? 19
20 Hypnotics Benadryl 25mg-50mg Temazepam (Restoril) 15-30mg (geriatric 7.5mg) Trazodone (unlabeled use) 25-50mg Zolpidem (Ambien) 5-10mg Beers high severity Beers high severity Okay in elderly Beers High Severity (avoid chronic use) Anti-cholinergic effects (confusion, dry mouth, urinary retention; caution in pts with glaucoma and BPH Same AE as any benzo; contraindicated in glaucoma caution in those with falls risk, hepatic or renal impairment Hypotension, increased bleeding risk if on NSAID s or warfarin, priapism, serotonin syndrome, caution post-mi or with h/o seizures HA, dizziness, somnloence; in elderly similar effects to benzo (derlium, fall, fractures) Melatonin Melatonin Agonist (Ramelteon) 20 Safe, Well Tolerated Tolerated No evidence of benefit; may help in certain subgroup of patients Somnolence; caution in hepatic impairment
21 Case Vignette He remains hospitalized due to social issues including homelessness. On day 6 of admission you are called by the nurse due to the patient falling in his room. You evaluate his gait and notice he is unsteady in addition to being more somnolent than usual. What could be contributing to the fall and gait impairment? 21
22 Sedatives Ativan: common use in ETOH withdrawal -AE include sedation, respiratory depression -Caution in those with acute angle glaucoma, sleep apnea, respiratory issues, hepatic/renal impairment, h/o drug abuse or falls risk Anti-Psychotics: Typical (Haldol) & Atypical (Seroquel, Risperidone) -anti-cholinergic side effects, QT prolongation -careful in dementia related psychosis (increased risk of death compared to placebo) 22
23 Case Vignette A review indicates the patient has continued to receive Ativan despite no further evidence of withdrawal due to complaints of anxiety and insomnia. A review of his chart reveals he was previously on mirtazapine but this medication had not been continued on admission. During rounds, it is noted that the tachycardia noted on admission has recurred. On exam he is also noted to have a unilateral, fixed, dilated pupil. What else could be contributing to the tachycardia? What is causing the anisocoria? 23
24 Review- Case Vignette HPI: 59 year old male admitted for chest pain and acute ETOH intoxication. He also complains of hematemesis during his most recent drinking binge. PMHx: AVNRT, Hepatitis C, insomnia, depression, COPD Meds: combivent inhaler bid, ibuprofen 600mg po tid prn EKG on admission reveals bpm 24
25 Review- Case Vignette He is admitted to the medicine service with the following prn orders: -Ativan 2mg IV q4hr prn withdrawal -Albuterol neb q6h prn, Atrovent neb q6hr prn -Acetaminophen 650mg q4hr prn pain -Ibuprofen 600mg po tid prn pain 25
26 Pulmonary Nebulizers: Albuterol (max dose 3mL q4hours): can cause tachycardia, arrhythmia, caution in patients with ischemia Atrovent: anti-cholinergic side effects; caution in those with glaucoma, BPH Mucolytics: Mucomyst: can cause bronchospasm; use minutes after bronchodilator administration 26


27 Nebulizer Associated Anisocoria 27
28 Case Vignette The patient subsequently complains of diarrhea the next day. Stool studies are sent, and the intern orders lomotil prn for loose stools. Is this an appropriate order? 28
29 Gastrointestinal Heartburn: Maalox (aluminum dioxide, magnesium hydroxide) or Maalox plus AE: constipation, cramps, fecal discoloration; aluminum intoxication Use with caution in renal impairment: hypophosphatemia or hypermagnesemia long list of drug interactions Must be administered one hour apart from other oral meds Diarrhea: do not use in those with C. diff colitis Loperamide (Immodium): caution in hepatic impairment Lomotil (diphenoxylate/atropine): anti-cholinergic side effects Constipation: see mini-lecture on residency website 29
30 Case Vignette The patient subsequently does well and is discharged. Upon discharging the patient, you order the following outpatient medication regimen: Ibuprofen 600mg po tid prn Norco 2 tabs q6hr prn Combivent inhaler q4hr prn Benadryl 25mg po qhs prn Librium taper Are these appropriate orders? 30
31 Summary For all PRN orders, know the correct dosage, common adverse effects and contraindications Check the next day to see if your patient actually received any of the PRN meds Convert frequently administered PRN meds into standing orders Don t just put in PRN orders to save night float the trouble of getting called Evaluate underlying cause or condition requiring use of a PRN med and treat accordingly Don t forget the importance of medication reconciliation! 31
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice
 Opioid of choice") PATIENT CONTROLLED ANALGESIA (PCA) PLAN Allergies: Medication Selection: morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice HYDROmorphone (Dilaudid ) 6 mg/ 30 ml (0.2 mg/ml) fentanyl 300 mcg/ 30 ml (10 mcg/ml)
PATIENT CONTROLLED ANALGESIA (PCA) PLAN Allergies: Medication Selection: morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice HYDROmorphone (Dilaudid ) 6 mg/ 30 ml (0.2 mg/ml) fentanyl 300 mcg/ 30 ml (10 mcg/ml)
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients
 Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Guidelines for Management and Prevention of Delirium In Geriatric Trauma Patients Objectives: Provide a guideline for recognizing and managing delirium in geriatric trauma patients. Provide a template
Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD
 Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD Chairman, Department of Behavioral Health NYU Winthrop Hospital Associate Professor of Psychiatry and
Integrated Care of Patients on Constant Observation in a General Hospital Setting Aaron Pinkhasov, MD Chairman, Department of Behavioral Health NYU Winthrop Hospital Associate Professor of Psychiatry and
WHS POSTOPERATIVE POWERPLAN CHANGES
 Medications simplified and standardized to improve safety and effectiveness in the management of pain, itching, nausea/vomiting. Management: o The Anesthesiologist will continue to manage pain in the PACU.
Medications simplified and standardized to improve safety and effectiveness in the management of pain, itching, nausea/vomiting. Management: o The Anesthesiologist will continue to manage pain in the PACU.
* * FORM REV. 02/2019 Page 1 of 4. TNKASE (tenecteplase) / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:
 / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:") 1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
ENT THYROIDECTOMY/PARATHYROIDECTOMY POST OP ADMIT PLAN - Phase: Begin Immediately/PACU
 - Phase: Begin Immediately/PACU Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Pt Status:
- Phase: Begin Immediately/PACU Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Pt Status:
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
ENT THYROIDECTOMY/PARATHYROIDECTOMY POST OP PLAN - Phase: Begin Immediately/PACU
 - Phase: Begin Immediately/PACU PHYSICIAN S Diagnosis Weight Allergies Laboratory Calcium Level STAT Outpatient/PACU, T;N PTH Intact STAT Outpatient/PACU, T;N 1 of 7 - Phase: When Patient Arrives to Room
- Phase: Begin Immediately/PACU PHYSICIAN S Diagnosis Weight Allergies Laboratory Calcium Level STAT Outpatient/PACU, T;N PTH Intact STAT Outpatient/PACU, T;N 1 of 7 - Phase: When Patient Arrives to Room
GERIATRICS 101. Victoria L. Braund, MD, FACP, CMD. Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston
 GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
GERIATRICS 101 Victoria L. Braund, MD, FACP, CMD Director, Division of Geriatrics, NorthShore Medical Director, Symphony of Evanston LET S REVIEW Medicare Hospice Pain mgmt. Bowel business Delirium Sleep
SEDATIVE-HYPNOTIC AGENTS
 SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
PAIN PODCAST SHOW NOTES:
 PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
What to do when you are called to see a patient with... PAIN. Susan Merel, MD Division of General Internal Medicine July 2018
 What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
Tricyclic Antidespressants: Actions
 Introductory Clinical Pharmacology Chapter 24 Antidepressant Drugs Tricyclic Antidespressants: Actions Increase sensitivity in postsynaptic alpha (α)-adrenergic, serotonin receptors Decrease sensitivity
Introductory Clinical Pharmacology Chapter 24 Antidepressant Drugs Tricyclic Antidespressants: Actions Increase sensitivity in postsynaptic alpha (α)-adrenergic, serotonin receptors Decrease sensitivity
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
LBVA NIGHT FLOAT GUIDE FOR INTERNS
 LBVA NIGHT FLOAT GUIDE FOR INTERNS NIGHTFLOAT Basic Principles. 1 Common Crosscover Pages 1 Running a Rapid Response or Code Blue 4 Nightly Schedule 4 Passcodes.. 4 Basic Pain Management Guide..... 5 Electrolyte
LBVA NIGHT FLOAT GUIDE FOR INTERNS NIGHTFLOAT Basic Principles. 1 Common Crosscover Pages 1 Running a Rapid Response or Code Blue 4 Nightly Schedule 4 Passcodes.. 4 Basic Pain Management Guide..... 5 Electrolyte
Standardized Nurse Activated Protocols (SNAPs)
") SNAPs by presenting complaint/problem help nurses initiate care before the patient is seen by a physician. SNAPs should be approved by ED team consensus If patient unstable in any way, immediately notify
SNAPs by presenting complaint/problem help nurses initiate care before the patient is seen by a physician. SNAPs should be approved by ED team consensus If patient unstable in any way, immediately notify
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
1. Attending Physician: Dr Syn Pager: Cell: Co-Morbidities:
 BARIATRIC SURGERY IMMEDIATE POST-OP PLAN (Includes Post Op Day 1) Denotes order requirement Antibiotic administered in the OR at: 1. Attending Physician: Dr Syn Pager: 740-6545 Cell: 438-9415 2. To remain
BARIATRIC SURGERY IMMEDIATE POST-OP PLAN (Includes Post Op Day 1) Denotes order requirement Antibiotic administered in the OR at: 1. Attending Physician: Dr Syn Pager: 740-6545 Cell: 438-9415 2. To remain
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC
 Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC By 2020, the cost of falls is estimated to be 30 billion per year. Fall Prevention: National Patient Safety Goal Focus on falls: older adults,
Margaret Knight PhD, PMHCNS-BC Catherine Coakley MS, RN-BC By 2020, the cost of falls is estimated to be 30 billion per year. Fall Prevention: National Patient Safety Goal Focus on falls: older adults,
EPIDURAL / INTRATHECAL POST-OP PLAN
 EPIDURAL / INTRATHECAL POST-OP PLAN Diagnosis Weight PHYSICIAN S Allergies Patient Care Vital Signs Per Unit Standards, PLUS check and record RR q1h x 12, then q2h x 6, until 24h following narcotic administration.
EPIDURAL / INTRATHECAL POST-OP PLAN Diagnosis Weight PHYSICIAN S Allergies Patient Care Vital Signs Per Unit Standards, PLUS check and record RR q1h x 12, then q2h x 6, until 24h following narcotic administration.
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
UMC Health System Patient Label Here. PHYSICIAN ORDERS Diagnosis
 COPD PLAN UMC Health System PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Vital Signs Per Unit Standards Daily Weight Patient Activity Up Ad Lib/Activity as Tolerated Assist as Needed Bedrest
COPD PLAN UMC Health System PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Vital Signs Per Unit Standards Daily Weight Patient Activity Up Ad Lib/Activity as Tolerated Assist as Needed Bedrest
OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN
 OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Patient Discharge Anticipated in 24 Hour (Patient Discharge Anticipated in 24 Hours) Patient
OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Patient Discharge Anticipated in 24 Hour (Patient Discharge Anticipated in 24 Hours) Patient
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Children with Hypertension in ED
 Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Children with Hypertension in ED By Prof. Sanaa AK Helmy Professor of Anesthesia, Intensive Care and Pain Management, Faculty of Medicine, Cairo University Vice-chairman of the Egyptian Society of Emergency
Immodium / loprarmide
 Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
IS ATIVAN LIKE KLONOPIN
 IS ATIVAN LIKE KLONOPIN Is Ativan Like Klonopin How will ativan make me feel How can you get addicted to ativan Ativan wellbutrin lexapro interaction Can i take ativan day after drinking Daily ativan for
IS ATIVAN LIKE KLONOPIN Is Ativan Like Klonopin How will ativan make me feel How can you get addicted to ativan Ativan wellbutrin lexapro interaction Can i take ativan day after drinking Daily ativan for
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Drug Review Rozerem (ramelteon)
") Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
Drug Review Rozerem (ramelteon) Introduction 1 Ramelteon is a melatonin receptor agonist with affinity for MT 1 and MT 2 and selectivity over the MT 3 receptor. The activity at the MT 1 and MT 2 receptors
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine)
") Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
Nursing Process Focus: Patients Receiving Chlorpromazine (Thorazine) Potential Nursing Diagnoses Ineffective Therapeutic Regimen Management Risk for Activity Intolerance, related to side effect of drug
OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN
 OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN PHYSICIAN S Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards Patient Activity Up Ad Lib/Activity as Tolerated Bedrest STRICT Bedrest Up to
OB/GYN POSTPARTUM VAGINAL DELIVERY PLAN PHYSICIAN S Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards Patient Activity Up Ad Lib/Activity as Tolerated Bedrest STRICT Bedrest Up to
A UMC Health System Performance Improvement Initiative for use in all units where cardiac/surgical patients are admitted.
 A UMC Health System Performance Improvement Initiative for use in all units where cardiac/surgical patients are admitted Denotes guideline requirement Attending Physician: Resident/Fellow: Allergies_ Diagnosis:
A UMC Health System Performance Improvement Initiative for use in all units where cardiac/surgical patients are admitted Denotes guideline requirement Attending Physician: Resident/Fellow: Allergies_ Diagnosis:
LYSIS OF ADHESIONS POST-OP PLAN - Phase: PACU Phase
 - Phase: PACU Phase PHYSICIAN S Diagnosis Weight Allergies Communication Place Device at Bedside Confirm there are 3 x Aliquots of 0.2% Ropivacaine. 2 x Medfusion Infusion pumps. Confirm 3 x PF Aliquots
- Phase: PACU Phase PHYSICIAN S Diagnosis Weight Allergies Communication Place Device at Bedside Confirm there are 3 x Aliquots of 0.2% Ropivacaine. 2 x Medfusion Infusion pumps. Confirm 3 x PF Aliquots
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
A Geriatrician s Perspective on Successful Aging. Ariel Green, MD, MPH Assistant Professor of Medicine
 A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
A Geriatrician s Perspective on Successful Aging Ariel Green, MD, MPH Assistant Professor of Medicine 1 Disclosures Johns Hopkins Clinical Research Scholars Program American College of Cardiology Foundation
Chitra Fernando, MD March 18, 2008
 Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
SANDOMIGRAN (pizotifen malate)
") SANDOMIGRAN (pizotifen malate) S N CH 3 Pizotifen. COOH CH OH CH 2 COOH MALATE DESCRIPTION Pizotifen is a cycloheptathiophene derivative structurally related to cyproheptadine and the tricyclic antidepressants.
SANDOMIGRAN (pizotifen malate) S N CH 3 Pizotifen. COOH CH OH CH 2 COOH MALATE DESCRIPTION Pizotifen is a cycloheptathiophene derivative structurally related to cyproheptadine and the tricyclic antidepressants.
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs
 Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
ATIVAN OVERDOSE BRAIN DAMAGE
 ATIVAN OVERDOSE BRAIN DAMAGE Ativan Overdose Brain Damage Ativan how many mg Ativan hardly knee replacement parts Using ativan prior to a procedure code Ativan for end of life care Can ativan be used to
ATIVAN OVERDOSE BRAIN DAMAGE Ativan Overdose Brain Damage Ativan how many mg Ativan hardly knee replacement parts Using ativan prior to a procedure code Ativan for end of life care Can ativan be used to
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Pharmacology. Definitions. Pharmacology Definitions 8/20/2013. Drug:
 Pharmacology Medications and their potential implications in physical therapy Definitions Drug: Any substance that alters physiologic function in the organism, regardless of whether the effect is beneficial
Pharmacology Medications and their potential implications in physical therapy Definitions Drug: Any substance that alters physiologic function in the organism, regardless of whether the effect is beneficial
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
How to Manage Insomnia with and without medications
 How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
ATIVAN YES OR NO TAROT CARD
 ATIVAN YES OR NO TAROT CARD Ativan Yes Or No Tarot Card Ativan oral onset time Does ativan help with ibs Klonopin along with ativan for alcohol detox at home depot Tylenol and ativan at same time Ativan
ATIVAN YES OR NO TAROT CARD Ativan Yes Or No Tarot Card Ativan oral onset time Does ativan help with ibs Klonopin along with ativan for alcohol detox at home depot Tylenol and ativan at same time Ativan
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach)
") Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
Fall Prevention in Hospice (A pharmacologic and nonpharmacologic approach) Chinenye Emereole, Pharm.D. Clinical Pharmacist Hospice Pharmacy Solutions Objectives Assess and identify hospice patients who
Sedative-Hypnotics. Sedative Agents (General Considerations)
") Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Hospice High Dollar Medications and Possible Alternatives
 Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage
Hospice High Dollar Medications and Possible Alternatives Ly M. Dang, PharmD LDang@HospicePharmacySolutions.com Director of Pharmacy Operations Hospice Pharmacy Solutions Topics of Discussion Hospice Coverage
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Treatment of Alcohol and Opiate Withdrawal
 Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Nursing Process Focus: Patients Receiving Salmeterol (Serevent)
") Prior to administration: Assess for presence/history of chronic asthma, exercise induced asthma, acute asthma attacks, and acute upper airway obstruction. Assess respiratory rate and lung sounds, pulse
Prior to administration: Assess for presence/history of chronic asthma, exercise induced asthma, acute asthma attacks, and acute upper airway obstruction. Assess respiratory rate and lung sounds, pulse
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
RP PERCOCET STREET VALUE
 RP 5 325 PERCOCET STREET VALUE Rp 5 325 Percocet Street Value Max dose of percocet a day Urgent care percocet bothell wa 98012 directions I need a substitute for percocet 10/325 percocet Percocet constipation
RP 5 325 PERCOCET STREET VALUE Rp 5 325 Percocet Street Value Max dose of percocet a day Urgent care percocet bothell wa 98012 directions I need a substitute for percocet 10/325 percocet Percocet constipation
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Richard Senysyzn, MD Psychiatry for Adults 1260 River Acres Drive New Braunfels, TX , Fax. (888)
") ADHD Evaluation Intake Form Patient Contact Information Patient Name: Date of Birth: Age: Last First MI Address: Email address: Contact phone number: Emergency Contact/Number/Relationship: Pharmacy: Primary
ADHD Evaluation Intake Form Patient Contact Information Patient Name: Date of Birth: Age: Last First MI Address: Email address: Contact phone number: Emergency Contact/Number/Relationship: Pharmacy: Primary
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Atrovent Administration
 Atrovent Administration ICEMA Training 2007 Sherri Shimshy RN OBJECTIVES Describe the pharmacology of Atrovent Identify the indications for use of Atrovent in the Adult Population Identify the indications
Atrovent Administration ICEMA Training 2007 Sherri Shimshy RN OBJECTIVES Describe the pharmacology of Atrovent Identify the indications for use of Atrovent in the Adult Population Identify the indications
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Physician s Order Form. Physician s Order Form. Telemetry/Progressive Care Orders. Continued on next page. >>>>>>> Continued on next page.
 DATE: TIME: DATE TIME INTRAVENOS FLID and MEDICATION Status: Admit to Telemetry Admit to Progressive Care nit Transfer to Progressive Care nit Note: Discontinue Previous Orders Transfer to Telemetry nit
DATE: TIME: DATE TIME INTRAVENOS FLID and MEDICATION Status: Admit to Telemetry Admit to Progressive Care nit Transfer to Progressive Care nit Note: Discontinue Previous Orders Transfer to Telemetry nit
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy
 START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
START, STOPP, Beers Oh My! Navigating the World of Geriatric Pharmacy Jessica DiLeo, PharmD Kate Murphy, PharmD OBJECTIVES Identify pharmacodynamic and pharmacokinetic parameters that may influence treatment
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Procedure: Laser Transurethral Resection of Prostate or Transurethral Resection of Prostate
 Laser Transurethral Resection Of Prostate Or Transurethral Resection Of Prostate Post-Operative Plan Patient Label Here A UMC Health System Performance Improvement Initiative for use in all units where
Laser Transurethral Resection Of Prostate Or Transurethral Resection Of Prostate Post-Operative Plan Patient Label Here A UMC Health System Performance Improvement Initiative for use in all units where
Hip Hemiarthroplasty Post Op Version 2 4/20/17
 Patient Name: Diagnosis: Allergies with reaction type: Hip Hemiarthroplasty Post Op Version 2 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro PCU ICU General
Patient Name: Diagnosis: Allergies with reaction type: Hip Hemiarthroplasty Post Op Version 2 4/20/17 Patient Placement General Diagnosis/Procedure: Preferred Location/Unit Ortho/Neuro PCU ICU General
Orthopedic Admission Hip Fracture Version 2 1/25/2017
 Patient Name: Initial each page and Sign/Date/Time last page Diagnosis: Allergies with reaction type: Orthopedic Admission Hip Fracture Version 2 1/25/2017 Patient Placement Patient Status If the physician
Patient Name: Initial each page and Sign/Date/Time last page Diagnosis: Allergies with reaction type: Orthopedic Admission Hip Fracture Version 2 1/25/2017 Patient Placement Patient Status If the physician
USUAL DOSE OF XANAX. Usual Dose Of Xanax
 USUAL DOSE OF XANAX Usual Dose Of Xanax Withdrawal what symptoms xanax from Compared valium to xanax.5 Valium vs vs xanax ativan Gocce mg 0 xanax 25 quante Melatonin between and xanax interactions Lb xanax
USUAL DOSE OF XANAX Usual Dose Of Xanax Withdrawal what symptoms xanax from Compared valium to xanax.5 Valium vs vs xanax ativan Gocce mg 0 xanax 25 quante Melatonin between and xanax interactions Lb xanax
Nuts for Neuro and why I hate EMR
 Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Policy REVISED: 6/30/2016 3:30 PM. Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016
 Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Title: Antihypertensive Treatment for Severe Hypertension During Pregnancy Applies To: ObGyn Responsible Department: ObGyn Revised: June 30, 2016 Policy POLICY STATEMENT: Pregnant or postpartum patients
Reducing the risk of patient harm: A focus on opioids
 Reducing the risk of patient harm: A focus on opioids New York State Partnership for Patients (NYSPFP) Initiative Regional Educational Session November 2013 1 Disclosure Matthew Fricker, Matthew Grissinger,
Reducing the risk of patient harm: A focus on opioids New York State Partnership for Patients (NYSPFP) Initiative Regional Educational Session November 2013 1 Disclosure Matthew Fricker, Matthew Grissinger,
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Conflict of Interest. Background. Objectives. Adverse Events 10/20/2015
 Utilizing a Structured Pain Management Approach in Total Hip and Total Knee Arthroplasty Jennifer Watson, Medication Safety Pharmacist Gina Anderson-Malum, Total Joint Specialist, Bone & Joint Center Conflict
Utilizing a Structured Pain Management Approach in Total Hip and Total Knee Arthroplasty Jennifer Watson, Medication Safety Pharmacist Gina Anderson-Malum, Total Joint Specialist, Bone & Joint Center Conflict
Lorazepam Tablets, USP
 Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Beta Blockade. Andre P. Marshall, PGY2 8/14/09 VANDERBILT SURGERY
 Beta Blockade Andre P. Marshall, PGY2 8/14/09 Beta Blockade Who are the Betas anyway? When, why, and how do we block them? The Beta Receptor B 1 : cardiac chronotropic and inotropic B 2 : bronchodilation,
Beta Blockade Andre P. Marshall, PGY2 8/14/09 Beta Blockade Who are the Betas anyway? When, why, and how do we block them? The Beta Receptor B 1 : cardiac chronotropic and inotropic B 2 : bronchodilation,
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ
 PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Based on 2014 SOGC Guidelines
 Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
Based on 2014 SOGC Guidelines 22nd Edition 2015 1 ICH + gestational hypertension by far the biggest cause of direct maternal deaths New stats coming in 2013 OCR 22nd Edition 2015 2 Diastolic 90 mmhg is
PRESCRIBING ALERT
 www.empr.com PRESCRIBING ALERT Dear Healthcare Professional, At MPR we strive to bring you important drug information in a concise and timely fashion. In keeping with this goal, we are pleased to bring
www.empr.com PRESCRIBING ALERT Dear Healthcare Professional, At MPR we strive to bring you important drug information in a concise and timely fashion. In keeping with this goal, we are pleased to bring
Basics of Benzodiazepine Use Disorder. DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic